


Mental health disorders contribute significantly to the global burden of disease in adolescents, with depression being one of the leading causes of mortality among this age group (World Health Organization, 2025). Between 2001 and 2020, the global prevalence of adolescents reporting clinically elevated levels of depressive symptoms has increased markedly from 24% to 37% (Shorey et al., Reference Shorey, Ng and Wong2022). Among Southeast Asian countries, Singapore reports one of the highest burdens and prevalence of mental health issues (Szücs et al., Reference Szücs, van der Lubbe, Arias de la Torre, Valderas, Hay, Bisignano, Morgan, Acharya, Adnani, Apostol, Aslam, Asri, Aung, Aurizki, Baig, Bermudez, Cenderadewi, Danpanichkul, Efendi and Ng2025). In particular, clinical levels of depressive symptoms are increasingly pervasive among the younger demographic, including children and adolescents. The mean age of depression onset has declined over the years, with a recent study reporting a fourfold increase in the incidence of depression among Singaporean youths between 2013 and 2018 (Tan et al., Reference Tan, Arvind, Lee, To, Paul, Leong and Shuen Sheng Fung2021). Depressive symptoms during childhood and adolescence are associated with a myriad of adverse outcomes, including academic difficulties, behavioral problems, and strained relationships with parents and peers (Branje et al., Reference Branje, Hale, Frijns and Meeus2010; Faust et al., Reference Faust, Baum and Forehand1985; Harrington, Reference Harrington2001; Wickersham et al., Reference Wickersham, Sugg, Epstein, Stewart, Ford and Downs2021). The early onset of depression during childhood and adolescence is also associated with more severe depression and poorer psychosocial functioning in adulthood (Liu et al., Reference Liu, Chen, Su, Fang, Srisurapanont, Hong, Hatim, Chua, Bautista and Si2015; Zisook et al., Reference Zisook, Lesser, Stewart, Wisniewski, Balasubramani, Fava, Gilmer, Dresselhaus, Thase, Nierenberg, Trivedi and Rush2007). Therefore, identifying and targeting risk factors for depressive disorders during early childhood is imperative for timely detection and intervention.
Prior cross-sectional and longitudinal research indicates that poorer language ability is a risk factor for heightened mental health problems across childhood and adolescence (e.g., Hentges et al., Reference Hentges, Devereux, Graham and Madigan2021; Koyuncu et al., Reference Koyuncu, Zabcı, Seçen Yazıcı, Sandıkçı, Çetin Kara and Doğangün2024; St Clair et al., Reference St Clair, Forrest, Yew and Gibson2019). Studies have examined this relationship through between-group comparisons of emotional problems among children with clinical language difficulties and their peers with typical language development (i.e., categorical approach) (e.g., Koyuncu et al., Reference Koyuncu, Zabcı, Seçen Yazıcı, Sandıkçı, Çetin Kara and Doğangün2024; Yew & O’Kearney, Reference Yew and O’Kearney2013). For example, meta-analytic evidence indicates that children with developmental language disorder (previously known as specific language impairment) are approximately twice as likely to experience clinical levels of internalizing problems as compared to their peers with typical language development (Yew & O’Kearney, Reference Yew and O’Kearney2013). Community-based cohort studies that assess language abilities on a continuum (i.e., dimensional approach) have also demonstrated an association between poorer language skills and increased internalizing problems (see Hentges et al., Reference Hentges, Devereux, Graham and Madigan2021 for a meta-analysis; Tamayo et al., Reference Tamayo, Wareham, Franken, McKean, Tiemeier and Jansen2023). Importantly, the association between language ability and emotional problems has been consistently demonstrated across both clinical and community samples (Hentges et al., Reference Hentges, Devereux, Graham and Madigan2021). Given the accumulating evidence on the association between poorer language abilities and emotional problems, greater attention to potential underlying mechanisms is warranted (Conti-Ramsden & Botting, Reference Conti-Ramsden and Botting2008; Salmon et al., Reference Salmon, O’Kearney, Reese and Fortune2016). Recent work has investigated mediating variables in the association between language difficulties and emotional problems (e.g., peer problems, emotion regulation, Forrest et al., Reference Forrest, Gibson, Halligan and St Clair2018; Helland et al., Reference Helland, Røysamb, Schjølberg, Øksendal and Gustavson2022). However, the mediating role of cognitive variables, such as children’s self-concept, remains unclear to date.
Self-concept as a mediating mechanism
Self-concept, often used interchangeably with the term “self-esteem,” is broadly defined as an individual’s perception of themselves, shaped by self-appraisals and evaluations from others (Shavelson et al., Reference Shavelson, Hubner and Stanton1976). Self-concept is a multi-dimensional construct comprising various domains, including social, academic, emotional, and physical competence (Marsh, Reference Marsh1986; Marsh & Shavelson, Reference Marsh and Shavelson1986). Notably, empirical research has highlighted the importance of distinguishing between self-concept and depression (Orth et al., Reference Orth, Robins and Roberts2008; Sowislo & Orth, Reference Sowislo and Orth2013). The strength of associations between self-concept and depression across past studies has demonstrated wide variability (Orth et al., Reference Orth, Robins and Roberts2008), which indicates that the two constructs are related but should still be treated as distinct.
The present study draws on two theoretical perspectives as a framework for understanding how early language ability may be prospectively linked to depressive symptoms through its influence on self-concept. First, cognitive models of psychopathology, such as the vulnerability model, suggest that self-concept plays a central role in the onset and maintenance of depression (Orth et al., Reference Orth, Robins, Trzesniewski, Maes and Schmitt2009; Sowislo & Orth, Reference Sowislo and Orth2013). A positive self-concept, involving enhanced views of the self, can support children’s psychological adjustment and facilitate the development of positive social relations (Chavez-Hernandez et al., Reference Chavez-Hernandez, Correa-Romero, Acosta-Rojas, Cardoso-Espindola, Padilla-Gallegos and Valadez-Figueroa2018). Conversely, persistent negative evaluations of the self may be a predisposing factor for depressive symptoms (Jacobs et al., Reference Jacobs, Reinecke, Gollan and Kane2008; Sowislo & Orth, Reference Sowislo and Orth2013). Additionally, competency-based models of depression (Cole, Reference Cole1990, Reference Cole1991) propose that children with lower competence across various domains of functioning may elicit negative appraisals from others, including parents, teachers, and peers. Such feedback can adversely affect children’s perceptions of the self (i.e., self-concept), which in turn may contribute to increased depressive symptoms. Considering that linguistic competence is a key domain for social evaluation in childhood and early adolescence (e.g., reading or speaking abilities), it has been theorized that children with poorer language abilities may be more susceptible to internalizing problems due to the development of negative self-perceptions (see Bornstein et al., Reference Bornstein, Hahn and Suwalsky2013).
Existing work examining the relationship between language ability and self-concept has largely taken a categorical approach, by comparing children with developmental language disorder and their peers with typical language development (Jerome et al., Reference Jerome, Fujiki, Brinton and James2002; Lindsay et al., Reference Lindsay, Dockrell, Letchford and Mackie2002; Lindsay & Dockrell, Reference Lindsay and Dockrell2012). Despite the clinical significance of findings from these studies, the extent to which variation in language ability relates to self-concept remains poorly understood. Prior research examining language ability from a dimensional perspective has shown that even in the absence of clinical language difficulties, children with poorer language ability tend to experience increased emotional problems (see Hentges et al., Reference Hentges, Devereux, Graham and Madigan2021). Therefore, considering language ability along a continuum may provide more nuanced insights into its associations with self-concept and subsequent emotional outcomes.
Research indicates that, during middle to late childhood, children with developmental language disorder may be at greater risk of poor self-concept compared to their peers with typical language development (Jerome et al., Reference Jerome, Fujiki, Brinton and James2002; Lindsay et al., Reference Lindsay, Dockrell, Letchford and Mackie2002). However, the evidence regarding the association between language ability and self-concept has been mixed, with other studies reporting no significant difference in self-concept between these groups (e.g., McAndrew, Reference McAndrew1999). Moreover, a longitudinal study following children with a history of developmental language disorder found that language ability assessed at ages 8 and 10 did not predict self-concept or internalizing problems during late adolescence (Lindsay & Dockrell, Reference Lindsay and Dockrell2012). These conflicting findings underscore the need for further investigation into how language ability is associated with self-concept, and whether this relationship may be specific to a particular developmental window.
As children transition from early to middle childhood, they become increasingly adept at evaluating their own competencies through social comparisons (Harter, Reference Harter1999). Middle childhood may therefore be a critical period during which children’s developing self-concepts are shaped by their language competence. Given that children with poorer language abilities often experience academic and social difficulties (Campisi et al., Reference Campisi, Serbin, Stack, Schwartzman and Ledingham2009; Mok et al., Reference Mok, Pickles, Durkin and Conti-Ramsden2014), these challenges – combined with the increased salience of peer comparisons within the school context – may exacerbate feelings of inadequacy and contribute to poorer self-concept (Jerome et al., Reference Jerome, Fujiki, Brinton and James2002). As such, poorer self-concept presents as a potential intermediary mechanism linking language difficulties to subsequent emotional problems. Consistent with the vulnerability model (Sowislo & Orth, Reference Sowislo and Orth2013), numerous studies have demonstrated that poorer self-concept is associated with increased levels of emotional problems among children and adolescents (e.g., de Jong et al., Reference de Jong, Sportel, de Hullu and Nauta2012; Spilt et al., Reference Spilt, van Lier, Leflot, Onghena and Colpin2014). In previous research that utilized global measures of self-concept, poorer self-concept following negative events was linked to increased depressive symptoms in children (Cohen et al., Reference Cohen, Young and Abela2012). Likewise, a study conducted with Hispanic adolescents revealed that poorer global self-concept was the strongest predictor of depressive symptoms, even after accounting for past feelings of depression (Robles-Piña et al., Reference Robles-Piña, Defrance and Cox2008). Taken together, existing studies highlight pertinent relationships among language ability, self-concept, and depressive symptoms. However, there remains a paucity of longitudinal research investigating whether self-concept mediates the association between early language ability and subsequent depressive symptoms.
Furthermore, insight into the potential domain-specificity and sex differences in these associations is lacking. Self-concept domains may be differentially related to early language ability and mental health outcomes (see Jerome et al., Reference Jerome, Fujiki, Brinton and James2002; Marsh et al., Reference Marsh, Parada and Ayotte2004). For instance, Marsh & colleagues (Reference Marsh, Parada and Ayotte2004) found that specific self-concept domains, such as better self-perceptions of emotional stability, were more strongly associated with internalizing symptoms, whereas domains related to physical appearance and physical ability showed comparatively weaker associations. Results from studies investigating the relationship between language ability and self-concept also differed depending on whether global- or domain-specific self-concept was assessed. Previous work has found that children with and without language difficulties showed no difference in overall (or global) self-concept (Cohen et al., Reference Cohen, Menna, Vallance, Barwick, Im and Horodezky1998; McAndrew, Reference McAndrew1999). However, when specific domains of self-concept were examined, children with language difficulties reported significantly poorer self-concept in the intellectual and school status domain as compared to their peers with typical language development (Cohen et al., Reference Cohen, Menna, Vallance, Barwick, Im and Horodezky1998). In light of the inconsistent evidence from existing studies, further research is needed to clarify the nature of the associations among children’s language ability, self-concept domains, and subsequent emotional outcomes.
The moderating role of child biological sex
Research has also documented sex differences in children’s self-concept and depressive symptoms (e.g., Weller et al., Reference Weller, Kloos, Kang and Weller2006; Wilgenbusch & Merrell, Reference Wilgenbusch and Merrell1999). A meta-analysis by Wilgenbusch et al., (Reference Wilgenbusch and Merrell1999) demonstrated that boys were more likely to report higher levels of overall self-concept than girls. In terms of specific domains, girls demonstrated higher self-concept in domains related to social competence, such as interpersonal relationships; boys showed higher levels of self-concept in domains concerning affective, academic, and physical competence. Prior work also indicates a sex difference in the emergence of depressive symptoms. Starting from early adolescence, girls are more likely than boys to experience an increase in depressive symptoms (Ge et al., Reference Ge, Conger and Elder2001). This sex difference persists during adulthood, with women being twice as likely as men to experience depression (Kuehner, Reference Kuehner2003; Salk et al., Reference Salk, Hyde and Abramson2017). Given the sex differences in the development of self-concept and depressive symptoms, child sex should be considered as a moderating variable when examining the indirect pathways from early language ability to subsequent depressive symptoms via self-concept domains.
Potential confounds in the associations among early language ability, self-concept, and depressive symptoms
Extensive research has established links between socioeconomic status (SES) and children’s language, cognitive, and socioemotional development (see Cooper & Stewart, Reference Cooper and Stewart2021 for a systematic review; Washbrook et al., Reference Washbrook, Gregg and Propper2014). SES is a multifaceted construct typically indexed by indicators such as income-based measures (e.g., monthly household income), parental occupation, and parental educational attainment (Ensminger & Fothergill, Reference Ensminger, Fothergill, Bornstein and Bradley2003). Maternal education attainment, in particular, is strongly associated with children’s developmental outcomes (Hoff & Laursen, Reference Hoff, Laursen and Bornstein2019; Magnuson et al., Reference Magnuson, Sexton, Davis-Kean and Huston2009). Studies have shown that children growing up in lower SES households are more likely to have poorer language development (Fernald et al., Reference Fernald, Marchman and Weisleder2013; Rodriguez & Tamis-LeMonda, Reference Rodriguez and Tamis-LeMonda2011), lower self-esteem (Doi et al., Reference Doi, Fujiwara, Isumi and Ochi2019; Orth, Reference Orth2018), and increased depressive symptoms (Joinson et al., Reference Joinson, Kounali and Lewis2017; Tracy et al., Reference Tracy, Zimmerman, Galea, McCauley and Stoep2008). Another significant factor associated with an increased risk for later anxiety and depressive disorders is internalizing problems during childhood (e.g., Goodwin et al., Reference Goodwin, Fergusson and Horwood2004; Roza et al., Reference Roza, Hofstra, van der Ende and Verhulst2003). Considering these factors jointly is thus crucial for determining whether the effects of children’s early language ability and self-concept on subsequent depressive symptoms are independent of lower SES and prior internalizing problems.
Understanding risk and protective factors for depressive symptoms within Singapore’s sociocultural context
Despite the growing literature on the relationship between children’s language ability and emotional problems, previous studies have been conducted predominantly in Western populations (e.g., St Clair et al., Reference St Clair, Forrest, Yew and Gibson2019; Tamayo et al., Reference Tamayo, Wareham, Franken, McKean, Tiemeier and Jansen2023; Westrupp et al., Reference Westrupp, Reilly, McKean, Law, Mensah and Nicholson2020). Further research across diverse sociocultural contexts is necessary to ascertain the generalizability of these findings. With the high prevalence of mental health problems among the younger demographic (Subramaniam et al., Reference Subramaniam, Vaingankar, Tan, Abdin, Chang, Tan, Samari, Archana, Chua, Lee, Tang, Lee, Chong and Verma2025), Singapore offers an understudied yet valuable context for investigating the risk and protective factors associated with depressive symptoms in preadolescence. Crucially, elucidating the pathways through which children’s early language ability contributes to subsequent depressive symptoms within Singapore’s sociocultural context may offer important insights into culturally informed processes underlying the development of psychopathology (see Causadias & Cicchetti, Reference Causadias and Cicchetti2018).
Several aspects of Singapore’s sociocultural landscape provide the backdrop for the present investigation. First, it is a linguistically diverse city-state that recognizes four official languages – English, Mandarin Chinese, Bahasa Melayu, and Tamil. In line with Singapore’s bilingual education policy, students learn English alongside one of the three heritage languages assigned based on their ethnic background (Dixon, Reference Dixon2005). English functions as the lingua franca and primary medium of instruction within the education system, making it the first and “working” language for Singaporeans (Chua, Reference Chua2011). Second, Singapore places considerable importance on providing accessible and high-quality education from early childhood. Reflecting this commitment, a 2023 survey reported that approximately 90% of children aged 3 to 4 were enrolled in preschool programs (Ministry of Social & Family Development, 2024), despite preschool education being non-compulsory. Government subsidies for lower-income families have also been progressively increased in recent years to encourage participation in early childhood education (Shafeeq, Reference Shafeeq2024). Additionally, Singaporean students pay only a nominal fee for primary school education in public schools, with fees remaining heavily subsidized beyond primary education (Ministry of Education, 2026). These policies help to ensure equitable access to education, regardless of socioeconomic conditions.
Lastly, children’s education and academic success are highly prioritized by parents in Singapore (Lowe & Ang, Reference Lowe and Ang2012). This is grounded in the broader societal view of education as a pathway to success, as well as interdependent socialization goals in Asian parenting where academic achievement is regarded as a means of honoring the family (Kim & Wong, Reference Kim, Wong, Kurasaki, Okazaki and Sue2002; Kyeong et al., Reference Kyeong, Yu, Tiemeier, Bakermans-Kranenburg and Setoh2025; Tan, Reference Tan2012). In contrast, European-American parenting goals may prioritize independence and the development of children’s self-esteem (e.g., Miller et al., Reference Miller, Wang, Sandel and Cho2002). In Singapore, the combination of strict parental expectations and the highly competitive educational environment (Lowe & Ang, Reference Lowe and Ang2012; Tan & Yates, Reference Tan and Yates2011) may place children under substantial academic, behavioral, and social pressures. With these factors distinguishing Singapore’s sociocultural context from that of Western populations, examining the pathways from early language ability to depressive symptoms in this Southeast Asian sample can advance a more culturally informed understanding of the underlying mechanisms.
The present study
The present study had two key aims. First, we sought to examine the mediating role of children’s self-concept domains in the relationship between their early language ability and severity of depressive symptoms during preadolescence. In line with previous studies (Jacobs et al., Reference Jacobs, Reinecke, Gollan and Kane2008; Lindsay et al., Reference Lindsay, Dockrell, Letchford and Mackie2002), we hypothesized that better language ability at ages 2 and 4 would be associated with better self-concept at age 8.5. In turn, this would predict less severe depressive symptoms at age 10. However, no a priori predictions pertaining to the independent mediating effects of each self-concept domain were formulated, as no studies have examined multi-dimensional self-concept in relation to both language ability and depressive symptoms. Next, we explored whether child biological sex would moderate the indirect effects of early language ability on subsequent depressive symptoms via the self-concept domains.
Method
Participants and procedure
Our study utilized data from a longitudinal pre-birth cohort in Singapore, Growing Up in Singapore Towards healthy Outcomes (GUSTO; Soh et al., Reference Soh, Tint, Gluckman, Godfrey, Rifkin-Graboi, Chan, Stunkel, Holbrook, Kwek, Chong, Saw, Sheppard, Chinnadurai, Ferguson-Smith, Goh, Biswas, Chia, Leutscher-Broekman, Shuter and Venkatesh2014). The study was designed to investigate the potential influence of epigenetic and developmental factors on children’s health and neurodevelopmental outcomes. Between 2009 and 2010, women in their first trimester of pregnancy were recruited from the National University Hospital and Kandang Kerbau (KK) Women’s and Children’s Hospital. Eligible mothers were Singaporean citizens or permanent citizens belonging to one of the three major ethnic groups in Singapore (i.e., Chinese, Malay, Indian) (see Soh et al., Reference Soh, Tint, Gluckman, Godfrey, Rifkin-Graboi, Chan, Stunkel, Holbrook, Kwek, Chong, Saw, Sheppard, Chinnadurai, Ferguson-Smith, Goh, Biswas, Chia, Leutscher-Broekman, Shuter and Venkatesh2014 for a detailed description of the inclusion and exclusion criteria). Mothers and their children underwent regular health and neuropsychological assessments from the antenatal period through adolescence, with data collection currently ongoing for the postnatal Year 15 follow-up. All assessments and questionnaires were administered by trained researchers in accordance with standardized study protocols. The GUSTO study was approved by the A*STAR Review Board (2020-011), National Healthcare Group Domain Specific Review Board (D/2009/00021; D/2014/00414), and SingHealth Centralized Institutional Review Board (2018/2767/D; 2019/2655/E). Written informed consent was obtained from participating mothers at recruitment, and children provided written assent for assessments from age 7 onwards.
A subsample of 473 children who have completed assessments of their language ability (2 and 4 years old), self-concept (8.5 years old), and depressive symptoms (10 years old) with data at two or more time points were included in this study. When children were aged 7, parents completed a questionnaire reporting on their child’s health and developmental concerns: “Has your child ever been seen by a doctor or been diagnosed for any of the following? [Medical condition].” Due to the double-barreled phrasing of the questionnaire items, it was not possible to determine whether the engagement of health professionals led to definitive clinical diagnoses of the medical conditions. As such, we chose not to exclude the children with parent-reported health and developmental concerns in the present study (n = 6 for autism spectrum disorder; n = 6 for hearing difficulties; n = 18 for speech and language difficulties; n = 8 for dyslexia). This inclusive sampling approach would also capture a wider range of early language abilities within the community sample. A sensitivity analysis excluding these children from the analytic sample was conducted (total n = 33, as some had more than one of the above-reported conditions), confirming that the inclusion of these children did not confound our main findings (see Supplement A for details).
Child sex, maternal education levels, and monthly household income did not differ significantly between the analytic sample and the excluded subsample from the larger GUSTO cohort, all ps > .05. There was a significant difference in ethnic composition between the two samples (χ 2 (2) = 7.16, p = .03, Cramer’s V = 0.07), with a higher proportion of Chinese and Malays and a lower proportion of Indians in the analytic sample (55.6% Chinese, 24.1% Malay, and 20.3% Indian in the excluded subsample). Table 1 presents the sociodemographic and language characteristics of the analytic sample. Language-group classifications were derived from caregiver-reported data on children’s language exposure at age 4 (available for 79.7% of the sample, see measures for detailed description). Consistent with Singapore’s three major ethnic groups and the use of English as the national lingua franca, the majority of children were exposed to (and consequently spoke) English and/or one of three heritage languages – Mandarin Chinese, Bahasa Melayu, or Tamil.
Sociodemographic and language characteristics of the analytic sample
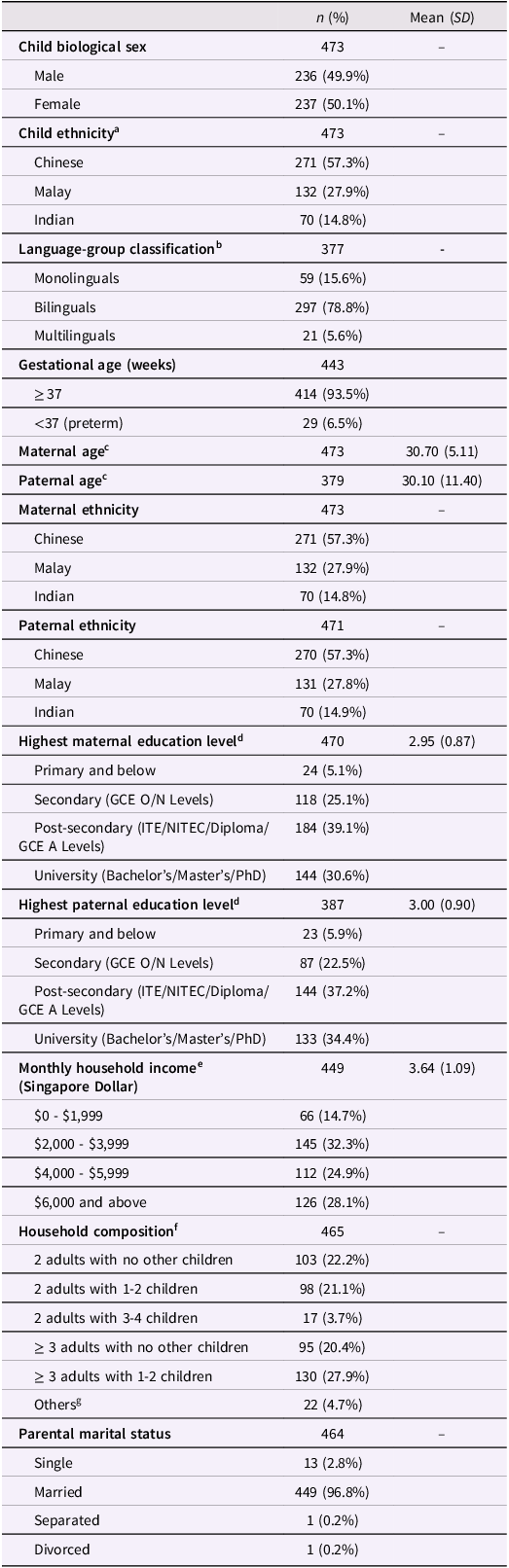
Table 1 Long description
The table presents sociodemographic and language characteristics of an analytic sample. It has 17 rows and 4 columns. The columns are labeled n (%), Mean (SD), and the rows are labeled with various sociodemographic and language characteristics. Row 1: Child biological sex, 473, -. Row 2: Male, 236, 49.9%. Row 3: Female, 237, 50.1%. Row 4: Child ethnicity, 473, -. Row 5: Chinese, 271, 57.3%. Row 6: Malay, 132, 27.9%. Row 7: Indian, 70, 14.8%. Row 8: Language-group classification, 377, -. Row 9: Monolinguals, 59, 15.6%. Row 10: Bilinguals, 297, 78.8%. Row 11: Multilinguals, 21, 5.6%. Row 12: Gestational age (weeks), 443, -. Row 13: >= 37, 414, 93.5%. Row 14: <37 (preterm), 29, 6.5%. Row 15: Maternal age, 473, 30.70 (5.11). Row 16: Paternal age, 379, 30.10 (11.40). Row 17: Maternal ethnicity, 473, -. Row 18: Chinese, 271, 57.3%. Row 19: Malay, 132, 27.9%. Row 20: Indian, 70, 14.8%. Row 21: Paternal ethnicity, 471, -. Row 22: Chinese, 270, 57.3%. Row 23: Malay, 131, 27.8%. Row 24: Indian, 70, 14.9%. Row 25: Highest maternal education level, 470, -. Row 26: Primary and below, 24, 5.1%. Row 27: Secondary (GCE O/N Levels), 118, 25.1%. Row 28: Post-secondary (ITE/NITEC/Diploma/GCE A Levels), 184, 39.1%. Row 29: University (Bachelor's/Master's/PhD), 144, 30.6%. Row 30: Highest paternal education level, 387, -. Row 31: Primary and below, 23, 5.9%. Row 32: Secondary (GCE O/N Levels), 87, 22.5%. Row 33: Post-secondary (ITE/NITEC/Diploma/GCE A Levels), 144, 37.2%. Row 34: University (Bachelor's/Master's/PhD), 133, 34.4%. Row 35: Monthly household income (Singapore Dollar), 449, 3.64 (1.09). Row 36: $0 - $1,999, 66, 14.7%. Row 37: $2,000 - $3,999, 145, 32.3%. Row 38: $4,000 - $5,999, 112, 24.9%. Row 39: $6,000 and above, 126, 28.1%. Row 40: Household composition, 465, -. Row 41: 2 adults with no other children, 103, 22.2%. Row 42: 2 adults with 1-2 children, 98, 21.1%. Row 43: 2 adults with 3-4 children, 17, 3.7%. Row 44: >= 3 adults with no other children, 95, 20.4%. Row 45: >= 3 adults with 1-2 children, 130, 27.9%. Row 46: Others, 22, 4.7%. Row 47: Parental marital status, 464, -. Row 48: Single, 13, 2.8%. Row 49: Married, 449, 96.8%. Row 50: Separated, 1, 0.2%. Row 51: Divorced, 1, 0.2%.
Note. n = number of participants with available data. Child biological sex was obtained from birth records. Monthly household income, parents’ age, maternal education level, and marital status were collected at recruitment. Paternal education level was collected at the 24- or 36-month visit. aChild ethnicity was derived from maternal ethnicity and coded categorically (1 = Chinese, 2 = Malay, 3 = Indian). bClassified as monolinguals if ≥ 85% exposure to one language, as bilinguals if exposure to two languages < 85%, and as multilinguals if exposure to three or more languages. cAge in decimal years is reported. dHighest education level was coded ordinally (1 = Primary and below to 4 = University). eMonthly household income was coded ordinally (1 = $0 - $1,999 to 4 = $6,000 and above). fReported by mothers at pregnancy week 11 visit; refers to the number of adults and children living in the child’s home (excluding the child). gHouseholds with 1 adult and 0–3 children, or ≥ 3 adults with 3–4 children.
Measures
Early language ability
Children’s early language ability was assessed using several well-established measures. The Bayley Scales of Infant and Toddler Development (BSID-3; Bayley, Reference Bayley2005) is a widely used assessment that enables a standardized approach to examining children’s cognitive, language, and motor development between the ages of 1 and 42 months. The receptive and expressive language subscales were administered by examiners during home visits when children were age 2. Items in the language subscales were adapted for administration in the three heritage languages – Mandarin Chinese, Bahasa Melayu, and Tamil. Translated items prioritized the intended item difficulty over semantic or structural equivalence (e.g., “shirt” was translated as the broader term “clothing” to better match the original item’s difficulty). Examiners were proficient in two or more of the languages relevant to the study and received training in administration and scoring beforehand. In line with the administration protocols, examiners identified the child’s dominant language prior to administration by asking parents and observing the child’s language use during a period of naturalistic interaction. While the BSID-3 was administered in the child’s dominant language, responses given in the non-dominant language, or a combination of both languages, were also accepted. The BSID-3 language scale has demonstrated excellent reliability for both expressive and receptive subscales (Bayley, Reference Bayley2005) and has adequate utility as a measure of general language ability in the GUSTO sample (Goh et al., Reference Goh, Tham, Magiati, Sim, Sanmugam, Qiu, Daniel, Broekman and Rifkin-Graboi2017).
The Peabody Picture Vocabulary Test (PPVT-4; Dunn & Dunn, Reference Dunn and Dunn2007) and the Comprehensive Test of Phonological Processing (CTOPP-2; Wagner et al., Reference Wagner, Torgesen, Rashotte and Pearson2013) were administered when children were age 4. Four CTOPP-2 subtests were administered to assess children’s phonological awareness: Blending Words, Elision, Sound Matching, and Phoneme Isolation. Children’s receptive vocabulary was assessed using the PPVT-4, which required them to point to one of four pictures that corresponded to a spoken target word. Both tests have good reliability (αs > 0.80; Dickens et al., Reference Dickens, Meisinger, Tarar, Wagner, Torgesen, Rashotte and Pearson2014; Dunn & Dunn, Reference Dunn and Dunn2007). A confirmatory factor analysis was performed to construct a latent language variable using test scores from the three measures of children’s vocabulary and phonological awareness, to be used in subsequent analyses. The measurement model for the latent language variable was just-identified (df = 0) and, by definition, had perfect global fit indices. We therefore evaluated the measurement model based on the factor loadings and residual variances. All indicators loaded significantly onto the latent language variable with positive residual variances, indicating the absence of Heywood cases. Standardized factor loadings and residual variances for the three indicators are shown in Table 2.
Measurement model results for the latent language variable
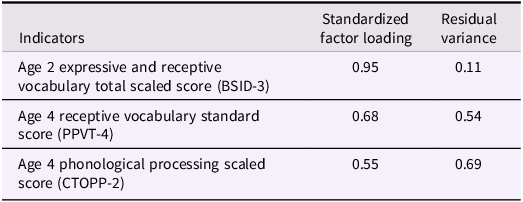
Table 2 Long description
A table with three rows and three columns. The columns are labeled Indicators, Standardized factor loading, and Residual variance. The rows are labeled as follows: Row 1: Age 2 expressive and receptive vocabulary total scaled score (BSID-3), 0.95, 0.11. Row 2: Age 4 receptive vocabulary standard score (PPVT-4), 0.68, 0.54. Row 3: Age 4 phonological processing scaled score (CTOPP-2), 0.55, 0.69.
Note. BSID-3 = Bayley Scales of Infant and Toddler Development, PPVT-4 = Peabody Picture Vocabulary Test, CTOPP-2 = Comprehensive Test of Phonological Processing. All three indicators loaded significantly onto the latent variable (ps < .001).
Self-concept domains
Children completed the Piers-Harris 2 (Piers & Herzberg, Reference Piers and Herzberg2002) at age 8.5. The Piers-Harris 2 is a 60-item measure assessing children’s self-concept across six domains: Behavioral Adjustment (e.g., “I behave badly at home.”), Intellectual and School Status (e.g., “I am good in my schoolwork.”), Physical Appearance and Attributes (e.g., “I am good looking.”), Freedom From Anxiety (e.g., “I am often afraid.”), Popularity (e.g., “It is hard for me to make friends.”), and Happiness and Satisfaction (e.g., “I am lucky.”). For each statement, children selected “yes” or “no,” and responses were scored as “0 = No” or “1 = Yes.” Total scores for each self-concept domain were derived by summing items within the subscale, where higher scores reflected better self-concept. All six domains showed adequate reliability in the sample (αs = 0.70 to 0.87).
Depressive symptoms
At age 10, children reported their depressive symptoms using the 28-item Children’s Depression Inventory 2 (CDI-2; Kovacs, Reference Kovacs2012). The CDI-2 is a commonly used screening instrument for the detection of depressive symptoms in children and adolescents. Children selected one of three statements which best describes how they have been feeling over the past two weeks (e.g., “I am sad once in a while,” “I am sad many times,” “I am sad all the time”), which corresponded to the scoring on a three-point Likert scale (0 = absent to 2 = always present). Scores were summed to derive a total depressive symptoms raw score. Raw scores were then converted into standardized T-scores according to child age and sex, with higher scores reflecting more severe depressive symptoms. The scale demonstrated good reliability in the sample (α = 0.87).
Covariates
Sociodemographic variables, including children’s biological sex, ethnicity, maternal education, and household income, were included as covariates. As previous research has shown that bilingual children were more likely to underperform relative to their monolingual peers on tasks assessing a single language (Bialystok & Feng, Reference Bialystok and Feng2008; Thordardottir et al., Reference Thordardottir, Rothenberg, Rivard and Naves2006), children’s language-group classification (monolingual vs. bilingual/multilingual) was included as a covariate to account for the influence of bilingual/multilingual status on early language ability. Language-group classification was derived from primary caregivers’ reports (typically mothers) of children’s language exposure at age 4, in response to the question: “Consider your child’s whole life. When you, your spouse and everybody else in your child’s life (also include teachers) talk to him/her, what percentage of each language is spoken to him/her?”. Children were classified as monolingual if they were exposed to a single language at least 85% of the time, bilingual if they were exposed to two languages (under 85% each), and multilingual if they were exposed to three or more languages. Due to the relatively small proportion of multilinguals in the sample (5.6%), we combined the bilingual and multilingual categories for analyses. Children’s internalizing problems at age 4 were also included as a covariate to control for emotional symptoms at baseline. Mothers reported on their children’s internalizing problems using the Child Behavior Checklist (Achenbach, Reference Achenbach1991), by indicating the extent to which their children exhibited symptoms of emotional reactivity, anxiety/depression, somatic complaints, and withdrawal on a three-point Likert scale (0 = not true to 2 = very true). T-scores were utilized in analyses, and there was good reliability in the sample (α = 0.88).
Analytic plan
Variance inflation factor (VIF) values of all independent variables were computed prior to the mediation analyses to rule out multicollinearity. All VIF values were below 5 (ranging from 1.06 to 2.10), indicating no multicollinearity (Kutner et al., Reference Kutner, Nachtsheim and Neter2004). To test our hypothesized model, we employed structural equation modeling (SEM) using Mplus 8 (Muthén & Muthén, Reference Muthén and Muthén1998–2017). Little’s (Reference Little1988) MCAR test indicated that data were not missing completely at random, χ2(188) = 320.49, p < .001. Hence, missing data were handled using full information maximum likelihood estimation to ensure unbiased parameter estimates in the main analyses (Enders & Bandalos, Reference Enders and Bandalos2001). In line with Hayes & Scharkow’s (Reference Hayes and Scharkow2013) guidelines, indirect effects were estimated using the bias-corrected bootstrap method with 5,000 samples. Statistical significance of mediation effects was determined if the 95% confidence interval (CI) of the indirect effect did not include zero (Preacher & Hayes, Reference Preacher and Hayes2008).
Next, we examined child sex as a potential moderator using multi-group SEM. Two multi-group models were estimated: a constrained model in which structural paths were constrained to be equal across sex groups, and an unconstrained model in which structural paths were allowed to vary across sex groups. A chi-square difference test was conducted to determine whether freeing the paths significantly improved the fit of the model. A significant difference in the model fit would indicate that the unconstrained model fits the data better than the constrained model (i.e., presence of sex differences in the mediating pathways). Finally, group differences in the indirect effects were tested using Wald tests of parameter constraints. We evaluated model fit using the Tucker–Lewis index (TLI), comparative fit index (CFI), root mean square error of approximation (RMSEA), and standardized root mean squared residual (SRMR). Model fit was considered acceptable when TLI and CFI ≥ 0.90, and RMSEA and SRMR ≤ 0.08 (Hu & Bentler, Reference Hu and Bentler1999; McDonald & Ho, Reference McDonald and Ho2002).
Results
Descriptive statistics
Table 3 presents the descriptive statistics of the key study variables. In the sample, 7.4% (n = 35) of the children scored more than two standard deviations below the mean on the PPVT-4 (standard score < 70), BSID-3 expressive, or receptive subscales (scaled score < 4). 4.9% of the children (n = 23) were identified as having clinically significant internalizing symptoms at age 4 (T-score ≥ 70; Achenbach & Rescorla, Reference Achenbach and Rescorla2000), and 24.1% (n = 114) scored in the clinically elevated range for depressive symptoms at age 10 (T-score ≥ 65; Kovacs, Reference Kovacs2012). Child age at the time of assessment showed no significant associations with the focal variables examined, including early language ability (rs = 0.07 to 0.09), self-concept domains (rs = −0.002 to 0.13), depressive symptoms (r = 0.03), and internalizing problems (r = −0.01), all ps > .05. As such, it was not included as a covariate in the following analyses.
Descriptive statistics of key study variables
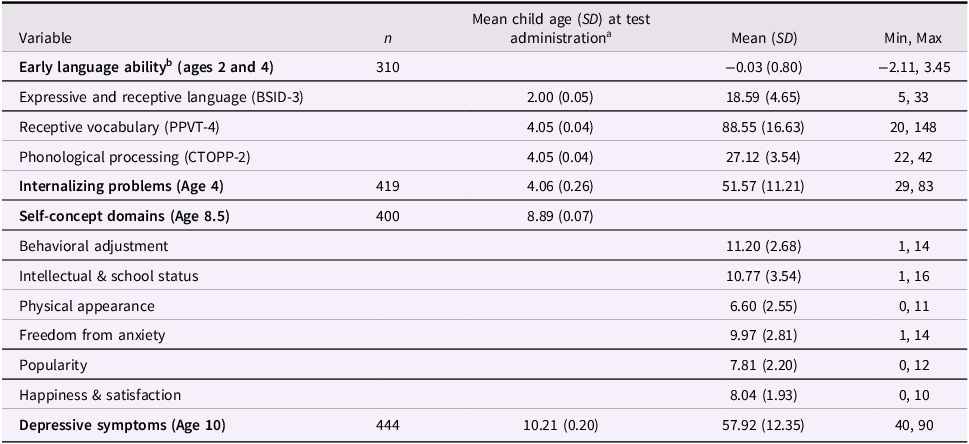
Table 3 Long description
The table presents descriptive statistics of key study variables. It has 10 rows and 5 columns. The columns are labeled Variable, n, Mean child age (SD) at test administration, Mean (SD), and Min, Max. The rows list different variables such as Early language ability, Expressive and receptive language (BSID-3), Receptive vocabulary (PPVT-4), Phonological processing (CTOPP-2), Internalizing problems (Age 4), Self-concept domains (Age 8.5), Behavioral adjustment, Intellectual & school status, Physical appearance, Freedom from anxiety, Popularity, Happiness & satisfaction, and Depressive symptoms (Age 10). Each row provides specific data for these variables, including the number of participants (n), mean child age at test administration, mean and standard deviation (SD), and minimum and maximum values.
Note. n = number of participants with available data. BSID-3 = Bayley Scales of Infant and Toddler Development (total scaled scores), PPVT-4 = Peabody Picture Vocabulary Test (standard scores), CTOPP-2 = Comprehensive Test of Phonological Processing (scaled scores). T-scores for internalizing problems and depressive symptoms, and raw scores for self-concept domains were utilized. aAge in decimal years is reported. bReferring to latent variable scores.
Preliminary analyses
Bivariate correlations of the key study variables are reported in Table 4. Early language ability was positively associated with self-concept in the following domains: behavioral adjustment, intellectual and school status, freedom from anxiety, and happiness and satisfaction. Two self-concept domains (i.e., physical appearance and popularity) were excluded from subsequent analyses, given that there were no significant associations with early language ability. Early language ability and all self-concept domains were negatively associated with depressive symptoms.
Correlation matrix of study variables
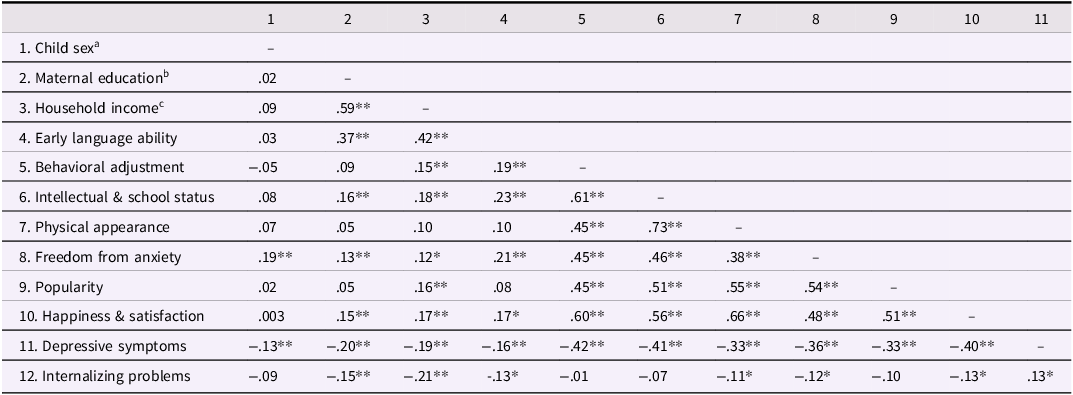
Table 4 Long description
A table titled 'Correlation matrix of study variables' with 12 rows and 11 columns. The table presents correlation coefficients between various study variables. Row labels include Child sex, Maternal education, Household income, Early language ability, Behavioral adjustment, Intellectual & school status, Physical appearance, Freedom from anxiety, Popularity, Happiness & satisfaction, Depressive symptoms, and Internalizing problems. Column headers are numbered from 1 to 11. Each cell contains a correlation coefficient value, with some values marked with asterisks indicating significance levels. Notable trends include high positive correlations between Early language ability and Intellectual & school status, and negative correlations between Depressive symptoms and several other variables.
Note. T-scores for internalizing problems and depressive symptoms, and raw scores for self-concept domains were utilized. aChild biological sex was coded as 0 = female; 1 = male. bMaternal education was coded ordinally (1 = Primary and below to 4 = University). cHousehold income was coded ordinally (1 = $0 - $1,999 to 4 = $6,000 and above). **p < .01, *p < .05.
As shown in Table 5, results from independent samples t-tests indicated that girls reported significantly poorer self-concept in the domain of freedom from anxiety at age 8.5, t(398) = −3.85, p < .001, and more severe depressive symptoms than boys at age 10, t(442) = 2.70, p = .007. There were no significant sex differences across the other variables.
Comparison of key variables between boys and girls
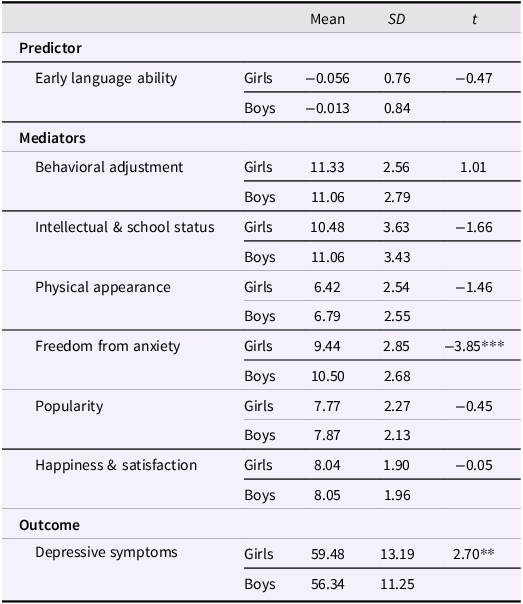
Table 5 Long description
A table comparing key variables between boys and girls. The table has 11 rows and 6 columns. The columns are labeled Predictor, Mediators, Outcome, Mean, SD, and t. The rows are labeled with different variables and their corresponding values for girls and boys. The variables include Early language ability, Behavioral adjustment, Intellectual & school status, Physical appearance, Freedom from anxiety, Popularity, Happiness & satisfaction, and Depressive symptoms. Each variable has mean, standard deviation (SD), and t-values for both girls and boys. Notable trends include significant differences in freedom from anxiety and depressive symptoms between boys and girls.
Note. ***p < .001, **p < .01.
Preliminary analyses also revealed significant associations between child ethnicity and early language ability (F (2, 307) = 5.58, p = .004), self-concept in the domains of behavioral adjustment (F (2, 397) = 4.98, p = .007), intellectual and school status (F (2, 397) = 10.76, p < .001), freedom from anxiety (F (2, 397) = 3.80, p = .02), and depressive symptoms (F (2, 441) = 6.29, p = .002). Therefore, ethnicity was retained as a covariate in the path analyses. Descriptive statistics for the key study variables by child ethnicity, as well as detailed post hoc comparison results, are presented in Supplementary Table S1.
Baseline mediation model
We first examined the mediation model in the full sample, adjusting for sociodemographic factors (child sex, ethnicity, maternal education, household income), language-group classification (monolingual vs. bilingual/multilingual), and child internalizing problems at age 4. The model demonstrated a good fit to the data, CFI = 0.95, TLI = 0.91, RMSEA = 0.05, SRMR = 0.04, χ2 = 63.34, p < .001. Children’s early language ability was positively associated with their self-concept in the domains of behavioral adjustment, intellectual and school status, freedom from anxiety, and happiness and satisfaction at age 8.5. However, out of the four included domains of self-concept, only behavioral adjustment significantly predicted depressive symptoms at age 10 (see Figure 1). There was a significant indirect effect of children’s early language ability on their depressive symptoms through the behavioral adjustment domain (β = −0.05, 95% CI [−0.08, −0.02]), but not the other three self-concept domains (see Table 6). The direct path between early language ability and depressive symptoms was non-significant, with 38.5% of the total effect being mediated by behavioral adjustment. In terms of covariate effects, higher maternal education (β = 0.17, p = .04) and household income (β = 0.31, p < .001) were associated with better early language ability. Bi/multilingual status at age 4 was linked to poorer early language ability (β = −0.15, p = .02). Only child sex was significantly related to depressive symptoms (β = −0.11, p = .01), with boys reporting less severe depressive symptoms than girls.
Standardized coefficients are reported. c represents the total effect, while c’ represents the direct effect. Dotted lines denote non-significant paths. Maternal education, household income, child sex, ethnicity, language-group classification (monolingual vs. bilingual/multilingual), and child internalizing problems at age 4 were included as covariates in the model. ***p < .001, **p < .01, *p < .05.

Figure 1 Long description
A diagram illustrating the relationship between early language ability and depressive symptoms through various self-concept domains. The diagram includes early language ability as the starting point, connected to four self-concept domains: behavioral adjustment, intellectual and school status, freedom from anxiety, and happiness and satisfaction. Each of these domains is linked to depressive symptoms. Arrows indicate the direction of influence, with standardized coefficients provided for significant paths. Dotted lines denote non-significant paths. The diagram shows that early language ability positively influences behavioral adjustment, intellectual and school status, and freedom from anxiety, which in turn negatively influence depressive symptoms. Maternal education, household income, child sex, ethnicity, language-group classification, and child internalizing problems at age 4 are included as covariates in the model.
Summary of total, direct, and indirect effects from early language ability to depressive symptoms
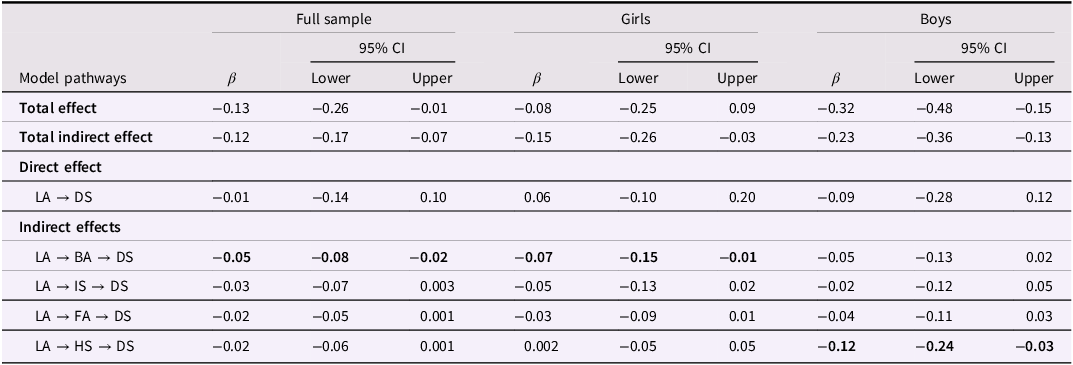
Table 6 Long description
A table comparing the effects of early language ability on depressive symptoms across a full sample, girls, and boys. The table has 10 rows and 12 columns. Column headers are Model pathways, β, 95% CI Lower, 95% CI Upper for Full sample, β, 95% CI Lower, 95% CI Upper for Girls, β, 95% CI Lower, 95% CI Upper for Boys. Row labels are Total effect, Total indirect effect, Direct effect, LA -> DS, Indirect effects, LA -> BA -> DS, LA -> IS -> DS, LA -> FA -> DS, LA -> HS -> DS. Row 1: Total effect, -0.13, -0.26, -0.01, -0.08, -0.25, 0.09, -0.32, -0.48, -0.15. Row 2: Total indirect effect, -0.12, -0.17, -0.07, -0.15, -0.26, -0.03, -0.23, -0.36, -0.13. Row 3: Direct effect, LA -> DS, -0.01, -0.14, 0.10, 0.06, -0.10, 0.20, -0.09, -0.28, 0.12. Row 4: Indirect effects, LA -> BA -> DS, -0.05, -0.08, -0.02, -0.07, -0.15, -0.01, -0.05, -0.13, 0.02. Row 5: LA -> IS -> DS, -0.03, -0.07, 0.003, -0.05, -0.13, 0.02, -0.02, -0.12, 0.05. Row 6: LA -> FA -> DS, -0.02, -0.05, 0.001, -0.03, -0.09, 0.01, -0.04, -0.11, 0.03. Row 7: LA -> HS -> DS, -0.02, -0.06, 0.001, 0.002, -0.05, 0.05, -0.12, -0.24, -0.03.
Note. Standardized coefficients and CI of standardized effects are reported. LA = early language ability; DS = depressive symptoms; BA = behavioral adjustment; IS = intellectual and school status; FA = freedom from anxiety; HS = happiness and satisfaction.
To further examine whether children’s early language ability was associated with their self-concept domains and depressive symptoms after accounting for cognitive ability, we conducted a supplementary analysis in which both early language ability and non-linguistic cognitive ability (assessed at age 4.5) were included as predictors in the baseline mediation model (see Supplement B for details). The magnitude and significance of the mediation pathways remained consistent with the previous results, supporting the robustness of the indirect effects of early language ability on subsequent depressive symptoms via self-concept.
Multi-group analysis on sex differences
Next, we tested a series of multi-group models to investigate whether there were differences in the mediating pathways based on child sex. The fit of the constrained model was only marginally acceptable, CFI = 0.92, TLI = 0.89, RMSEA = 0.06, SRMR = 0.06, χ2 (77) = 141.33, p < .001. The unconstrained model, which allowed the structural paths to vary across sex groups, demonstrated a good fit, CFI = 0.96, TLI = 0.92, RMSEA = 0.05, SRMR = 0.05, χ2 (52) = 83.22, p = .004. A comparison of the two models indicated that the constrained model provided a significantly poorer fit as compared to the unconstrained model, Δχ2 = 58.11, Δdf = 25, p < .001, suggesting that the mediating pathways were non-equivalent across sex. Thus, we examined the structural model separately for boys and girls.
As shown in Figure 2, better early language ability was associated with better self-concept across all four domains, regardless of child sex. Higher household income was associated with better early language ability among girls (β = 0.27, p = .03) and boys (β = 0.33, p < .001). Bi/multilingual status at age 4 was associated with poorer early language ability, but only among boys (β = −0.22, p = .004). No other covariate effects were significant. With regard to the mediation pathways, sex-specific associations were observed from the self-concept domains to subsequent depressive symptoms. For girls, self-concept in the domain of behavioral adjustment significantly mediated the association between early language ability and subsequent depressive symptoms, β = −0.07, 95% CI [−0.15, −0.01]. This mediating effect through behavioral adjustment was non-significant for boys, β = −0.05, 95% CI [−0.13, 0.02]. In contrast, the domain of happiness and satisfaction was a significant mediator in the association between early language ability and subsequent depressive symptoms only among boys, β = −0.12, 95% CI [−0.24, −0.03], but not among girls, β = 0.002, 95% CI [−0.05, 0.05]. Table 6 summarizes the total, direct, and indirect effects for both groups. Results from the Wald test of parameter constraints indicated a statistically significant difference in the indirect effect through happiness and satisfaction between boys and girls, χ2 (1) = 5.66, p = .02. However, there was no significant difference in the indirect effect through the domain of behavioral adjustment, χ2 (1) = 0.76, p = .38.
Standardized coefficients are reported for girls/boys. c represents the total effect, while c’ represents the direct effect. Bolded paths indicate a significant difference in the indirect pathway between the two groups, and dotted lines denote non-significant paths. Maternal education, household income, child ethnicity, language-group classification (monolingual vs. bilingual/multilingual), and child internalizing problems at age 4 were included as covariates in the model. ***p < .001, **p < .01, *p < .05.
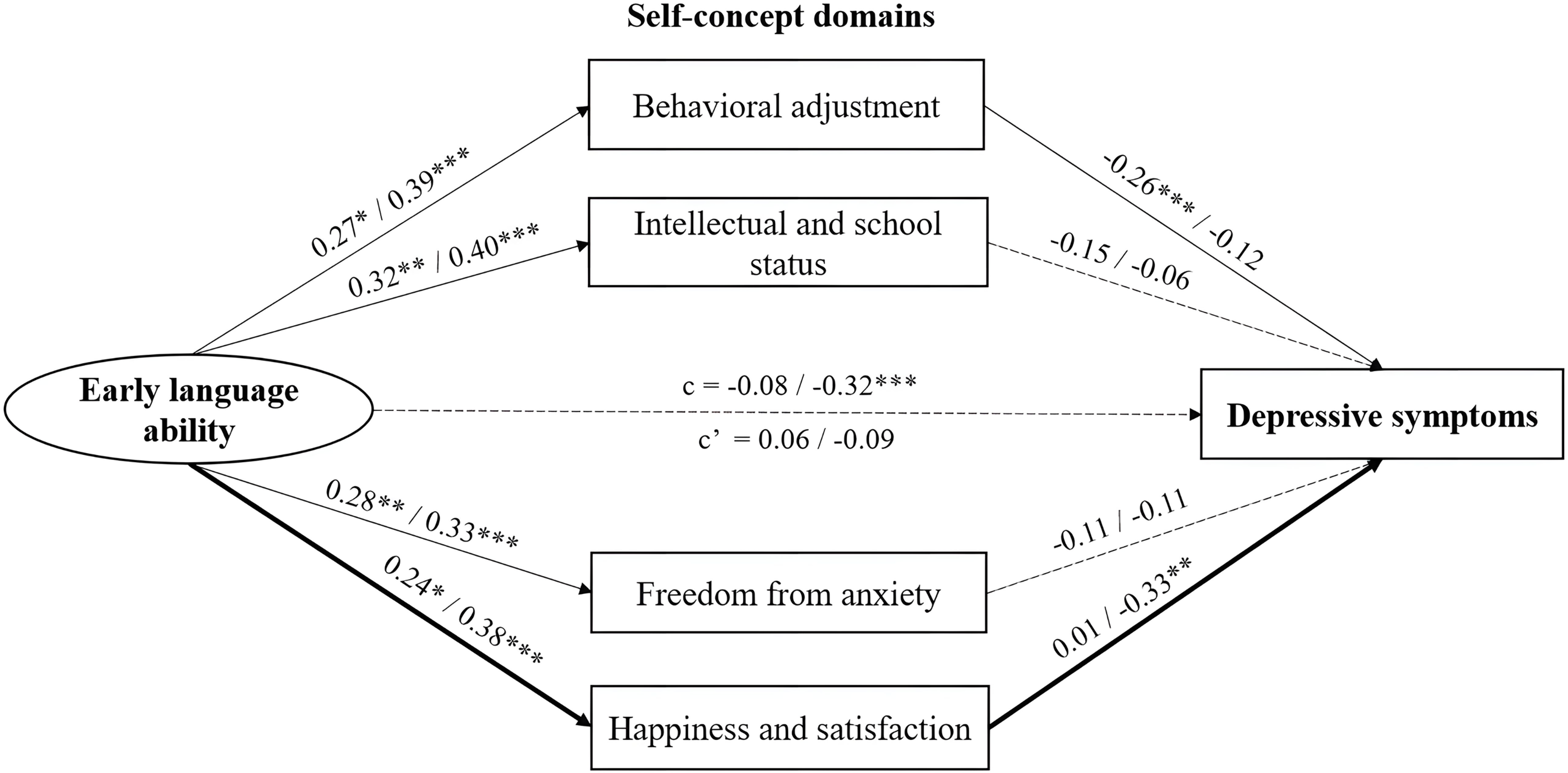
Figure 2 Long description
A diagram representing the relationship between early language ability and depressive symptoms through various self-concept domains. The diagram includes early language ability, behavioral adjustment, intellectual and school status, freedom from anxiety, happiness and satisfaction, and depressive symptoms. Arrows indicate the directional relationships between these components. Early language ability influences behavioral adjustment, intellectual and school status, freedom from anxiety, and happiness and satisfaction. These self-concept domains, in turn, affect depressive symptoms. The diagram also shows standardized coefficients for girls and boys, with bolded paths indicating significant differences in the indirect pathway between the two groups. Dotted lines denote non-significant paths. Maternal education, household income, child ethnicity, language-group classification, and child internalizing problems at age 4 are included as covariates in the model.
Discussion
The present study investigated the mediating role of children’s self-concept domains in the prospective association between their early language ability and depressive symptoms. In addition, we were interested in the moderating role of child sex in the mediation pathways. Within the full sample, poorer early language ability was indirectly associated with more severe depressive symptoms through the self-concept domain of behavioral adjustment. Multi-group analysis further showed that, for girls, only the domain of behavioral adjustment significantly mediated the association between early language ability and subsequent depressive symptoms. Conversely, this association was only mediated by the domain of happiness and satisfaction in boys. Overall, these findings suggest that there may be sex-specific mediating effects of self-concept domains in the association between early language ability and subsequent depressive symptoms.
Past research has only examined concurrent associations between language ability and self-concept (e.g., Lindsay et al., Reference Lindsay, Dockrell, Letchford and Mackie2002; Marton et al., Reference Marton, Abramoff and Rosenzweig2005). Utilizing longitudinal data, our study found that children’s language ability during the preschool years predicted their self-concept during middle childhood. Specifically, children with better early language ability demonstrated more positive self-concept across several domains, including behavioral adjustment, intellectual and school status, freedom from anxiety, and happiness and satisfaction. These findings indicate that early language difficulties may have implications for distinct aspects of self-concept development, particularly those that are relevant to academic, behavioral, and emotional problems (Jerome et al., Reference Jerome, Fujiki, Brinton and James2002). Next, results from the mediation analysis within the full sample indicated a significant indirect effect of language ability on depressive symptoms only via the behavioral adjustment domain, even after accounting for internalizing problems at baseline. Furthermore, there was no direct effect of early language ability on subsequent depressive symptoms. A number of studies to date have documented inconsistencies in the direct association between language abilities and emotional problems (e.g., Lindsay & Dockrell, Reference Lindsay and Dockrell2012; Redmond & Rice, Reference Redmond and Rice2002), underscoring the importance of examining the mediating mechanisms that underlie this relationship. Here, our findings point to children’s negative perception of their behavioral adjustment as a potential link between poorer language ability and more severe depressive symptoms.
As children acquire a greater understanding of social norms and expectations during middle childhood, behavioral adjustment becomes a central aspect of their developing self-concept and may be particularly salient relative to other domains of self-concept (Davis-Kean et al., Reference Davis-Kean, Jager and Andrew Collins2009; Markus & Nurius, Reference Markus and Nurius1986). For children with poorer language abilities, increased difficulties in communication and self-regulation may contribute to more behavioral problems over time (Petersen et al., Reference Petersen, Bates, D’Onofrio, Coyne, Lansford, Dodge, Pettit and van Hulle2013). Consequently, this can elicit increased negative feedback from teachers and parents regarding their behavioral conduct. In line with Cole (Reference Cole1990)’s competency-based model of depression, children’s heightened awareness of lapses in complying with standards of conduct set by teachers and parents may then lead to prolonged negative feelings about their own behavioral adjustment, and eventually manifest as more severe depressive symptoms during preadolescence.
Our findings not only lend support to the proposition that individuals with poorer self-concepts are at risk of increased depressive symptoms (Orth & Robins, Reference Orth and Robins2013; Sowislo & Orth, Reference Sowislo and Orth2013), but also indicate that language ability is an early-emerging vulnerability factor contributing to this risk pathway in Singaporean children. The associations between children’s early language ability and their self-concept domains remained robust even after accounting for the potential influence of non-linguistic cognitive ability and various sociodemographic factors. This highlights the unique contribution of children’s early language ability to their self-concept during middle childhood, over and above general cognitive ability. Considering the well-documented association between poor self-concept and increased depressive symptoms (e.g., Sowislo & Orth, Reference Sowislo and Orth2013), children’s language development during the early years clearly warrants careful attention. Building on this, future research should examine the extent to which supporting early language skills may have positive cascading effects on the development of self-concept.
By demonstrating that early language ability also has significant implications for self-concept development (and subsequently, depressive symptoms) in Southeast Asian children growing up in a linguistically diverse context, findings from this study also extend the generalizability of previous work conducted with clinical samples in Western settings (e.g., Jerome et al., Reference Jerome, Fujiki, Brinton and James2002; Lindsay et al., Reference Lindsay, Dockrell, Letchford and Mackie2002; Lindsay & Dockrell, Reference Lindsay and Dockrell2012). As the present investigation is primarily centered on child-related factors, future work should aim to clarify the associations between language ability, self-concept, and subsequent depressive symptoms within a broader ecological framework. For example, investigating whether factors such as parent–child relationships and peer interactions buffer the impact of poorer language abilities on children’s self-concept development (see Paulus et al., Reference Paulus, Licata, Gniewosz and Sodian2018; Verschueren et al., Reference Verschueren, Doumen and Buyse2012), can provide a more comprehensive understanding of the risk and protective factors associated with increased depressive symptoms.
There were notable sex-specific mediation effects of self-concept on the relationship between early language ability and subsequent depressive symptoms. Specifically, the domain of behavioral adjustment mediated this association only among girls. These patterns may reflect both socialization processes and broader sociocultural influences within Singapore’s context. For girls, negative evaluations of behavioral adjustment may be particularly consequential due to their early socialization experiences. In line with gender socialization theories, girls often face higher expectations to self-regulate their behavioral problems (Keenan & Shaw, Reference Keenan and Shaw1997) and are typically encouraged to be more empathic than boys (Van der Graaff et al., Reference Van der Graaff, Branje, De Wied, Hawk, Van Lier and Meeus2014). Researchers have also proposed that girls’ enhanced capacity to recognize the impact of their behavioral problems on others may lead to more internalizing problems (Zahn-Waxler et al., Reference Zahn-Waxler, Cole and Barrett1991; Zahn-Waxler, Reference Zahn-Waxler and Davidson2001). Moreover, caregivers and teachers may socialize girls to become more attuned to their behavioral problems, given that externalizing behaviors such as aggression and defiance are generally viewed as less acceptable in girls than in boys (Huesmann et al., Reference Huesmann, Guerra, Miller, Zelli, Fraşczek and Zumkley1992; Simpson & Stevenson-Hinde, Reference Simpson and Stevenson-Hinde1985).
In addition to these socialization pressures, self-regulation and behavioral inhibition during social interactions are valued in Asian collectivistic societies due to cultural norms (Chen et al., Reference Chen, Hastings, Rubin, Chen, Cen and Stewart1998; Ho, Reference Ho and Bond1986). This may create heightened expectations for children, particularly girls, to adhere to standards of appropriate behavioral conduct. In this regard, stronger language abilities play a crucial role in supporting self-regulation (Vallotton & Ayoub, Reference Vallotton and Ayoub2011) by enabling children to employ a wider range of strategies for managing their emotions and behavior (Salmon et al., Reference Salmon, O’Kearney, Reese and Fortune2016). Together, these factors may explain why girls with poorer language abilities were more likely to report more negative self-evaluations of their behavioral adjustment. This may have reflected their increased awareness about falling short of expected behavioral standards, which thereby increased the risk for more severe depressive symptoms.
For boys, however, their self-perception in the domain of happiness and life satisfaction may play a more central role in the relationship between their early language ability and subsequent depressive symptoms. Higher language competence could potentially foster a more positive overall self-perception through factors such as better social functioning and more effective emotion regulation (see Fujiki et al., Reference Fujiki, Brinton and Clarke2002; Gallagher, Reference Gallagher1993). Although no studies have directly examined the relationship between the self-concept domain of happiness and satisfaction and depressive symptoms in children, relevant insights may be gleaned from research on the relationship between life satisfaction and depression in adult samples (Becchetti & Conzo, Reference Becchetti and Conzo2021; Gigantesco et al., Reference Gigantesco, Fagnani, Toccaceli, Stazi, Lucidi, Violani and Picardi2019). These studies have documented a much more robust association between life satisfaction and depression among males than females, suggesting that perceptions of general life satisfaction may have a more pronounced impact on emotional well-being for males. Results in the present study are aligned with this finding, in showing no significant association between girls’ self-concept in the domain of happiness and satisfaction and subsequent depressive symptoms. Instead, general self-acceptance and life satisfaction may serve as a distinctive pathway through which early language ability is associated with depressive symptoms in boys.
Of note, it is somewhat surprising that the self-concept domain of intellectual and school status did not emerge as a significant mediator in the association between early language ability and subsequent depressive symptoms for either boys or girls, considering the strong emphasis on academic excellence within Singapore’s sociocultural context (Lowe & Ang, Reference Lowe and Ang2012; Tan & Yates, Reference Tan and Yates2011). However, we take these findings to mean that the influence of early language ability on emotional well-being may operate more strongly through children’s overall self-acceptance and perceptions of their behavioral adjustment, rather than academic competence, during this specific period of primary school education (i.e., age 8.5). As academic pressures intensify in later stages of schooling, particularly when children in Singapore prepare for high-stakes examinations at the end of their primary school education (see Soo et al., Reference Soo, Karthikeyan, Lim, Bartholomaeus and Yelland2022), it may be important for future research to examine whether academic self-concept becomes a more salient mediator in the association between early language ability and depressive symptoms.
Limitations and future directions
Several limitations of this study should be noted. First, our analyses only focused on children’s self-concept during middle childhood. However, research suggests that children’s self-evaluations across self-concept domains become increasingly differentiated from childhood through late adolescence (Marsh & Ayotte, Reference Marsh and Ayotte2003). Studies have also shown that while some self-concept domains may fluctuate over time, others remain relatively stable (Bolognini et al., Reference Bolognini, Plancherel, Bettschart and Halfon1996; Young & Mroczek, Reference Young and Mroczek2003). Thus, future studies should investigate whether the mediating effects of the self-concept domains observed during middle childhood extend into adolescence. Relatedly, although the Piers-Harris 2 is a widely used measure of self-concept (see Butler & Gasson, Reference Butler and Gasson2005), it has yet to be validated within Singapore’s context. Previous research has shown that the Piers-Harris 2 demonstrates good reliability and validity in other Asian contexts (e.g., Flahive et al., Reference Flahive, Chuang and Li2011; Su et al., Reference Su, Lou, Zhang, Xie and Lui2002), which may suggest the measure’s applicability to children in Singapore. Nevertheless, our findings should still be interpreted in light of this methodological limitation, and future work examining Singaporean children’s self-concept should aim to evaluate the psychometric validity of the Piers-Harris 2 within this sociocultural context.
Next, our study only utilized children’s self-reports of their self-concept and depressive symptoms. We were primarily interested in examining children’s perceptions of their depressive symptoms, especially in considering how internalizing problems tend to be under-reported by parents in community samples (Rescorla et al., Reference Rescorla, Ginzburg, Achenbach, Ivanova, Almqvist, Begovac, Bilenberg, Bird, Chahed, Dobrean, Döpfner, Erol, Hannesdottir, Kanbayashi, Lambert, Leung, Minaei, Novik, Oh and Verhulst2013; Wang et al., Reference Wang, Liu, Wu, Yang, Wang and Wang2014). Additionally, research has shown that children and adolescents are capable of providing valid and reliable reports of their depressive symptoms (Angold et al., Reference Angold, Weissman, John, Merikangas, Prusoff, Wickramaratne, Gammon and Warner1987; Moretti et al., Reference Moretti, Fine, Haley and Marriage1985). One potential avenue for future research is to adopt a multi-informant approach in investigating the relationship between children’s language ability, self-concept, and depressive symptoms.
Third, our study was unable to fully account for other potential confounding factors that may have influenced the relationship between language ability, self-concept, and depressive symptoms. These include adverse childhood experiences, which have been linked to poorer language development, low self-concept, and an increased risk of depressive symptoms during adolescence (Allen & Oliver, Reference Allen and Oliver1982; Melamed et al., Reference Melamed, Botting, Lofthouse, Pass and Meiser-Stedman2024; Zhong et al., Reference Zhong, Hu, Chen, Li, Chen, Li and Xu2024). Children’s pubertal status is another potential confound, as both early and late pubertal maturation relative to same-aged, same-sex peers have been identified as risk factors for the onset and severity of depressive symptoms (Angold et al., Reference Angold, Costello and Worthman1998; Joinson et al., Reference Joinson, Heron, Araya, Paus, Croudace, Rubin, Marcus and Lewis2012). Complementing these findings, a recent systematic review has identified several risk factors for increased depressive symptoms among adolescents in Singapore. This includes childhood maltreatment, chronic medical conditions (i.e., asthma), and unhealthy lifestyle factors such as sleep deprivation, pathological gaming, and excessive internet use (Goh et al., Reference Goh, Tan, Luo, Ng, Sulaiman, Wong and Loh2025). These additional confounds were not considered within the scope of our study, which leaves open the possibility that they may have influenced the strength of the observed associations among early language ability, self-concept, and depressive symptoms. To better delineate the impact of children’s early language ability on their subsequent depressive symptoms, it would be important for future studies to account for the effects of these extraneous factors. Finally, it should be noted that our analytic sample consisted primarily of ethnic Chinese participants. Although this is unlikely to compromise generalizability as it closely reflects the overall ethnic composition in Singapore (Department of Statistics, Ministry of Trade & Industry, 2024), caution is warranted when extending these findings to Southeast Asian populations beyond Singapore. Replication in diverse cultural contexts would be necessary to establish cross-cultural generalizability.
To our best knowledge, this study is the first to examine children’s self-concept domains as a mediator in the prospective association between early language ability and depressive symptoms. Although the temporal ordering of the variables represents a relative strength of our study, an important caveat is that our findings do not provide definitive evidence of self-concept as a causal explanatory mechanism. Specifically, our mediation analysis only included children’s early language ability during the preschool period (ages 2 and 4), self-concept at age 8.5, and depressive symptoms at age 10. Each variable was only assessed once across these three measurement time points, with a relatively short interval between the assessments of children’s self-concept and depressive symptoms. Moreover, other proximal factors at the family, peer, and school levels that may have influenced the development of self-concept and depressive symptoms between these time points could not be accounted for. These limitations preclude firm conclusions regarding the developmental pathways among early language ability, self-concept domains, and depressive symptoms. Rather, our findings should be interpreted as preliminary evidence that self-concept domains may serve as an indirect pathway linking early language ability to subsequent depressive symptoms. Future studies should employ repeated measurements of language ability, self-concept, and depressive symptoms from childhood to preadolescence, and include a broader range of relevant covariates, to ascertain the directionality and causal nature of the hypothesized mediation pathways (see Maxwell & Cole, Reference Maxwell and Cole2007; O’Laughlin et al., Reference O’Laughlin, Martin and Ferrer2018).
Despite these limitations, a key strength of this study lies in its adjustment for children’s internalizing problems at age 4. This enabled us to examine whether early language ability and self-concept domains predicted additional variance in subsequent depressive symptoms beyond baseline levels of internalizing problems. Additionally, children’s early language ability was directly measured using standardized language assessments. This approach reduces shared method bias to some extent; however, it does not entirely eliminate it since both self-concept domains and depressive symptoms were self-reported by children. As discussed earlier, future work should consider multi-method assessments for a more comprehensive evaluation of children’s self-concept domains and subsequent emotional outcomes.
The present study provides novel insights into self-concept domains as a potential sex-specific pathway linking early language ability to depressive symptoms. However, specific recommendations for interventions to reduce the risk and severity of depressive symptoms in children with poorer language abilities cannot be made until these findings are replicated in longitudinal studies employing causal mediation analysis. Given the remarkably stable trajectories of language ability from the ages of school entry (Bornstein et al., Reference Bornstein, Hahn, Putnick and Suwalsky2014; Norbury et al., Reference Norbury, Vamvakas, Gooch, Baird, Charman, Simonoff and Pickles2017), identifying the intermediary mechanisms through which language difficulties are associated with poorer emotional outcomes is crucial for timely intervention. If our findings regarding the mediating role of self-concept are corroborated by future research, it would suggest that clinicians working with children with poorer language abilities could potentially place a greater emphasis on fostering positive self-concept during middle childhood. In line with the body of evidence demonstrating the effectiveness of targeted self-concept interventions (see O’Mara et al., Reference O’Mara, Marsh, Craven and Debus2006 for a meta-analysis), enhancing self-concept in the relevant domains may be one promising avenue for improving the emotional adjustment of children with poorer language abilities.
Conclusion
Drawing from a comprehensive pre-birth cohort in Singapore, the present study found that poorer early language ability may contribute to more severe depressive symptoms in preadolescence via the pathway of low self-concept. Our results also suggest that the mediating effects of self-concept domains in this association may be sex specific. For children with poorer language abilities, enhancing self-perception in the domain of behavioral adjustment may be especially important for reducing depressive symptoms in girls, whereas the domain of happiness and satisfaction may be more relevant for boys. Importantly, future research should expand on these preliminary findings by investigating the sex-specific developmental pathways among language ability, self-concept domains, and depressive symptoms using longitudinal designs with repeated assessments. This would allow for stronger inferences regarding the developmental timing and directionality of these associations, thereby providing a foundation for evaluating whether self-concept interventions aimed at mitigating depressive symptoms in children with language difficulties could benefit from a tailored approach that considers these sex differences.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579426101308.
Data availability statement
Data from the Growing Up in Singapore Towards healthy Outcomes (GUSTO) study are not publicly available due to confidentiality requirements set by the local ethics review board. Requests for data access are subject to review and approval by the GUSTO executive committee.
Acknowledgements
We would like to thank the members of the GUSTO study team: Airu Chia, Andrea Cremaschi, Anna Magdalena Fogel, Anne Eng Neo Goh, Anne Rifkin-Graboi, Anqi Qiu, Arijit Biswas, Bee Wah Lee, Birit Froukje Philipp Broekman, Candida Vaz, Chai Kiat Chng, Chan Shi Yu, Choon Looi Bong, Daniel Yam Thiam Goh, Dawn Xin Ping Koh, Dennis Wang, Desiree Y. Phua, E Shyong Tai, Elaine Kwang Hsia Tham, Elaine Phaik Ling Quah, Elizabeth Huiwen Tham, Evelyn Chung Ning Law, Evelyn Keet Wai Lau, Evelyn Xiu Ling Loo, Fabian Kok Peng Yap, Falk Müller-Riemenschneider, Franzolini Beatrice, George Seow Heong Yeo, Gerard Chung Siew Keong, Hannah Ee Juen Yong, Helen Yu Chen, Hong Pan, Huang Jian, Huang Pei, Hugo P S van Bever, Hui Min Tan, Iliana Magiati, Inez Bik Yun Wong, Ives Lim Yubin, Ivy Yee-Man Lau, Jacqueline Chin Siew Roong, Jadegoud Yaligar, Jerry Kok Yen Chan, Jia Xu, Johan Gunnar Eriksson, Jonathan Tze Liang Choo, Jonathan Y. Bernard, Jonathan Yinhao Huang, Joshua J. Gooley, Jun Shi Lai, Karen Mei Ling Tan, Keith M. Godfrey, Keri McCrickerd, Kok Hian Tan, Kothandaraman Narasimhan, Krishnamoorthy Naiduvaje, Kuan Jin Lee, Li Chen, Lieng Hsi Ling, Lin Lin Su, Ling-Wei Chen, Lourdes Mary Daniel, Lynette Pei-Chi Shek, Maria De Iorio, Marielle V. Fortier, Mary Foong-Fong Chong, Mary Wlodek, Mei Chien Chua, Melvin Khee-Shing Leow, Michael J. Meaney, Michelle Zhi Ling Kee, Min Gong, Mya Thway Tint, Navin Michael, Neerja Karnani, Ngee Lek, Noor Hidayatul Aini Bte Suaini, Ong Yi Ying, Oon Hoe Teoh, Peter David Gluckman, Priti Mishra, Queenie Ling Jun Li, Sambasivam Sendhil Velan, Seang Mei Saw, See Ling Loy, Seng Bin Ang, Shang Chee Chong, Shiao-Yng Chan, Shirong Cai, Shu-E Soh, Stephen Chin-Ying Hsu, Suresh Anand Sadananthan, Swee Chye Quek, Tan Ai Peng, Varsha Gupta, Victor Samuel Rajadurai, Wee Meng Han, Wei Wei Pang, Yap Seng Chong, Yin Bun Cheung, Yiong Huak Chan, Yung Seng Lee, Zhang Han.
Funding statement
The GUSTO study is supported by the National Research Foundation (NRF) under the Open Fund-Large Collaborative Grant (OF-LCG; MOH-000504) administered by the Singapore Ministry of Health’s National Medical Research Council (NMRC) and the Agency for Science, Technology and Research (A*STAR). In RIE2025, GUSTO is supported by funding from the NRF’s Human Health and Potential (HHP) Domain, under the Human Potential Programme. This research was also supported by grants from the Singapore Ministry of Education Academic Research Fund Tier 1 (RG39/22; RG126/23), National University of Singapore Yong Loo Lin School of Medicine (NUHSRO/2021/093/NUSMed/13/LOA; NUHSRO/2025/001/NUSMed/001/GUSTO (bridging)/LOA), and Singapore Ministry of Education Science Social Science and Humanities Research Fellowship (MOE2019-SSHR-005) awarded to P.S.
Competing interests
The authors declare none.
Pre-registration statement
This manuscript reports a secondary analysis of data collected from the GUSTO study. The research design and analyses were not pre-registered.
AI statement
No generative AI tools were used in the preparation of this manuscript.
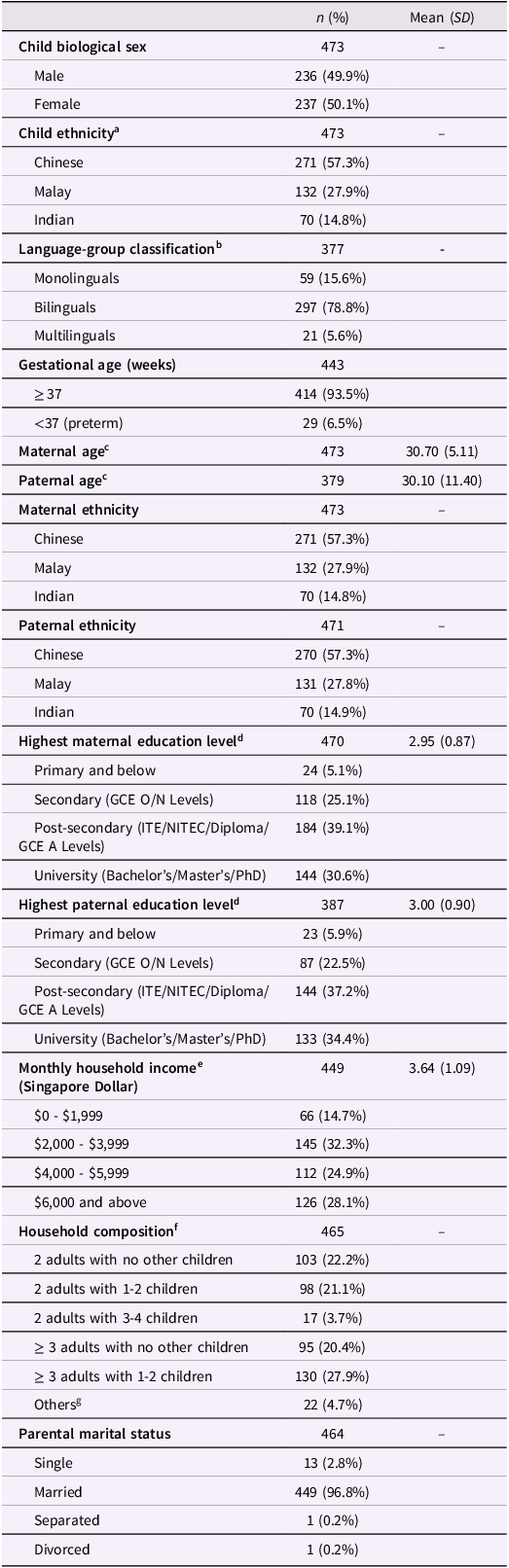
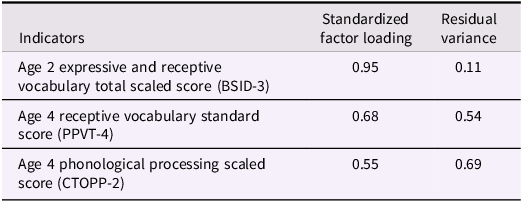
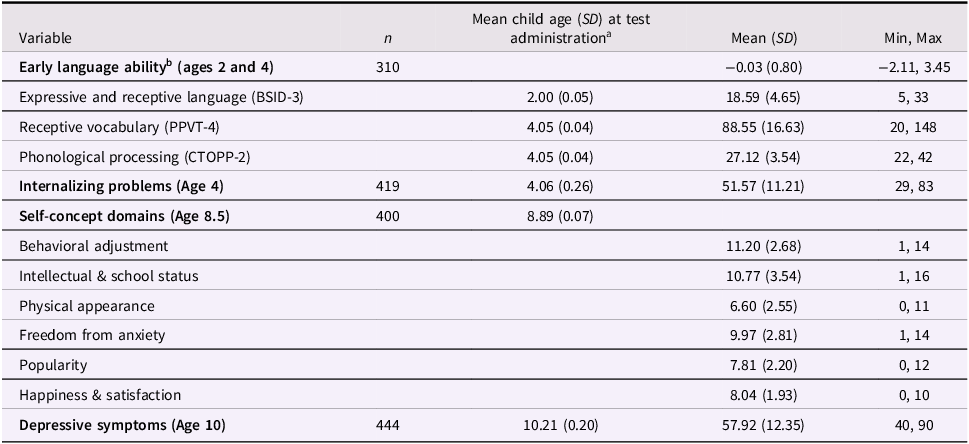
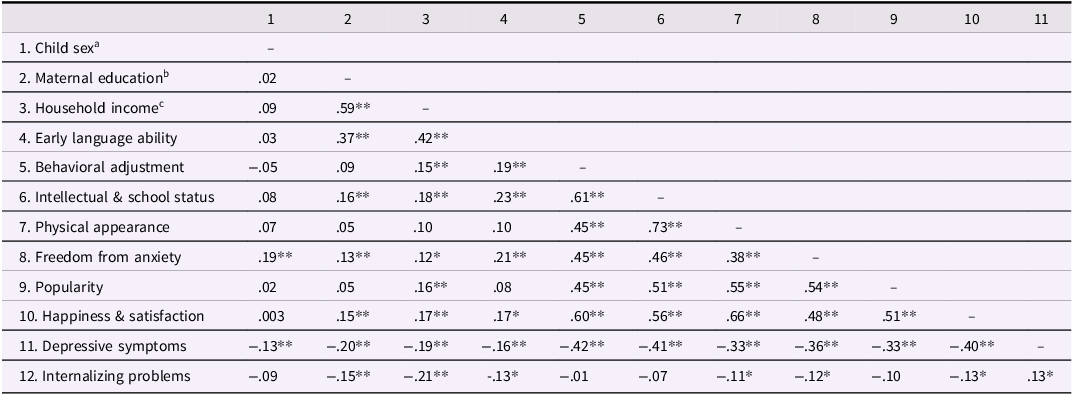
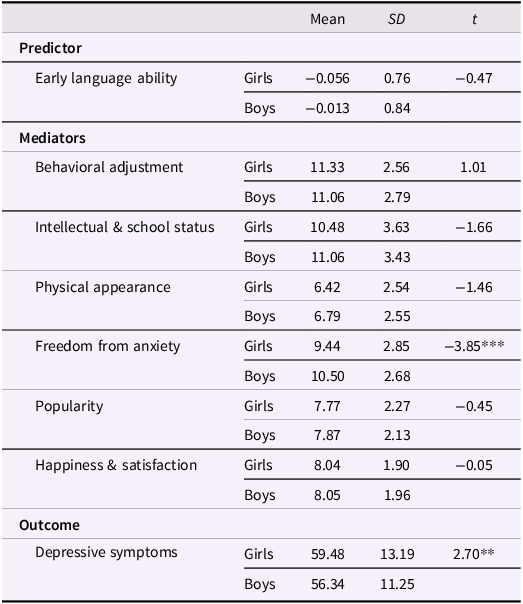

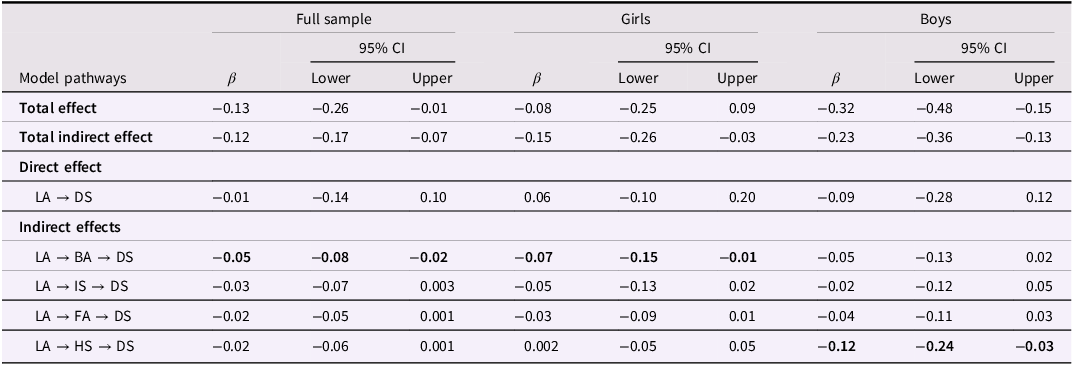
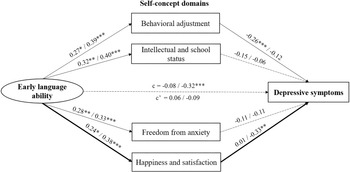



 Open access
Open access