


Depressive disorders are highly prevalent and a leading contributor to the global burden of disease(1). A large meta-analysis demonstrates a two-fold increase in all-cause mortality risk in people with depressive disorders compared with people without depression/general population controls. This includes markedly higher suicide risk (5·8-fold) and elevated mortality from natural causes (1·6-fold)(Reference Chan, Solmi and Lo2). Major depressive disorder has negative impacts on quality of life and is associated with increased risk of chronic disease, including cancer and heart disease(Reference Luppino, de Wit and Bouvy3–Reference Correll, Solmi and Veronese5). Antidepressant treatment is suboptimal for many individuals with depression; in the STAR*D trial, two-thirds of people with depression do not respond to first-line antidepressant therapy(Reference Rush, Trivedi and Wisniewski6). A large meta-analysis of psychological treatments for depression found similar remission rates with cognitive behavioural therapy(Reference Cuijpers, Miguel and Harrer7). There is an urgent need to identify adjunctive treatments to reduce the substantial burden of depression.
There is accumulating evidence that a healthy diet can improve symptoms of depression. A meta-analysis of sixteen randomised controlled trials suggest that diet interventions can improve depressive symptoms across a range of healthy individual and clinical cohorts(Reference Firth, Marx and Dash8). All but one of the studies in this meta-analysis examined samples with nonclinical depression. As such, an important research question is whether diet is effective in treating clinical depression. In a meta-analysis of a Mediterranean diet in adults with depressive disorder or subclinical depression symptoms, Mediterranean diet interventions significantly reduced depressive symptoms relative to controls (standardised mean difference = –0·53; 95 % CI: –0·90, –0·16)(Reference Bizzozero-Peroni, Martínez-Vizcaíno and Fernández-Rodríguez9). However, there was considerable between-study heterogeneity, which could be due to differences in intervention modality (i.e. group vs. individual), intervention features (i.e. diet alone, composite or combination), intervention duration, or in the control conditions applied. For example, the three randomised controlled trials investigating a Mediterranean diet alone (i.e. without additional nutrient supplementation or lifestyle intervention)(Reference Jacka, O’Neil and Opie10–Reference Francis, Stevenson and Chambers12) were 3–12 weeks’ duration and were delivered one on one through dietary counselling by a dietitian or nutritionist(Reference Jacka, O’Neil and Opie10,Reference Bayes, Schloss and Sibbritt11) or via an educational video(Reference Francis, Stevenson and Chambers12). Control conditions also varied across studies; one study used unblinded habitual diet as the control condition(Reference Francis, Stevenson and Chambers12) and two employed social befriending(Reference Jacka, O’Neil and Opie10,Reference Bayes, Schloss and Sibbritt11) .
The selection and design of control conditions are critically important for the precise estimation of treatment effects in dietary research. Some studies have adopted social befriending as a control. This may control for researcher interaction but does not constitute a comparable treatment with regard to type of intervention or contextual components. For example, diet counselling typically incorporates elements such as motivational interviewing and goal setting, which may independently influence mood and therefore represent active therapeutic components in their own right. Previous critique in this field also highlights concerns regarding unequal expectancy effects and potential selection bias if study advertising and recruitment do not sufficiently obscure the trial’s intent(Reference Molendijk, Fried and Van der Does13). Therefore, well-controlled trials are still needed to confirm whether a Mediterranean diet is efficacious beyond that accounted for by placebo, positive behaviour change or other nonspecific factors.
A feeding trial, in which all food is provided to participants, is ideal for providing proof-of-concept evidence that a specific diet has effectiveness because it maximises adherence and enables the incorporation of a placebo (sham) diet(Reference Tien, Hockey and So14). Feeding trials also enable better evaluation of the effect of known quantities of foods and nutrients on physiology. Considering the methodological weaknesses of prior research, the aims of this trial were to investigate the effectiveness of a traditional Mediterranean diet on depressive symptoms in people with major depressive disorder (MDD) through a double-blind sham-controlled randomised feeding trial design and to investigate potential mechanisms. We hypothesise that a 4-week traditional Mediterranean diet will lead to a greater reduction in depressive symptoms compared with a sham diet in people with MDD experiencing a major depressive episode.
Materials and methods
Overview
This is a 4-week double-blind, sham-controlled, randomised feeding trial of a Mediterranean diet for the treatment of moderate to severe MDD. Participants will be randomised 1:1 to receive a Mediterranean diet or a sham control diet designed to reflect typical dietary intake of the general population and considered dietary intakes of individuals with depression. A sham diet was selected to facilitate a placebo control. The primary outcome is the between-group differential change in depression severity at week four measured by the Montgomery-Åsberg Depression Rating Scale (MADRS)(Reference Montgomery and Asberg15). Exploratory outcomes include between-group differential change in patient-rated depression severity, anxiety and quality-of-life. Blood and stool samples will be collected to assess potential mechanisms. Twenty-two healthy individuals without depression will also be recruited and will receive a Mediterranean diet for 4 weeks. Data from healthy individuals will be used to determine whether clinical and biological responses to the intervention are unique to depression and whether the diet treatment modulates depression-related neurobiology. All participants will complete assessments and have samples collected at baseline and 4 weeks.
The trial is being conducted in accordance with the National Health and Medical Research Council (NHMRC) National Statement on Ethical Conduct in Human Research(16) and aligns with Good Clinical Practice(17). The trial protocol was developed in accordance with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) 2025 statement, which provides a comprehensive checklist for complete and transparent clinical trial protocol reporting. Approval to conduct the trial was received from the Human Research Ethics Committees of Barwon Health (23/75), Monash University (44424) and Deakin University (2023-297). Electronic informed consent will be obtained from all participants before any assessments are administered.
Eligibility
Individuals aged 18–65 years with a diagnosis of MDD, according to the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5) will be recruited. A diagnosis of MDD will be determined using the Structured Clinical Interview for DSM-5 Disorders, Research Version (SCID-5-RV) by research dietitians, following standardised training and under psychiatrists’ (PH, DK) oversight. In addition, participants must be experiencing a major depressive episode with moderate to severe depressive symptoms defined as score≥ 20 on the MADRS, have poor diet quality via a modified Total Diet Score(Reference Russell, Flood and Sadeghpour18), be willing and able to undertake and adhere to the requirements of a 4-week feeding trial and attend all trial appointments, reside in meal delivery zones, have access to a smartphone/tablet/computer with internet access and kitchen facilities (e.g. microwave or oven, freezer) and have a nominated preferred general practitioner. Antidepressant therapy and other therapies are allowed provided their frequency or dose remains unchanged throughout the intervention period.
Exclusion criteria include active suicidal ideation as assessed by self-report and by the researcher checking participant eligibility; self-reported psychiatric comorbidities, including bipolar I or II disorder, psychotic disorder, personality disorder, substance use disorder (including excess alcohol use), eating disorder or score ≥ 3 on the Sick, Control, One, Fat, Food (SCOFF) eating disorder screening questionnaire(Reference Morgan, Reid and Lacey19); history of a significant comorbid medical disorder (e.g. cancer, diabetes and dementia); history of major gastrointestinal surgery, irritable bowel syndrome or inflammatory bowel disease. Participants will also be excluded if they are considered treatment resistant (i.e. have failed two or more trials of antidepressant therapy for the current major depressive episode); have significant diet restrictions or allergy/intolerance, sociocultural or religious reasons that would interfere with adherence; exceed 300 min/week of moderate or 150 min/week of vigorous activity; have body mass index < 18·5 kg/m2 or > 40 kg/m2 calculated using self-reported data or have reported unstable weight in the past 3 months (> 5 % bodyweight change); are pregnant or breast-feeding or have used probiotic, prebiotic and/or synbiotics or changed their pharmacological and/or psychological treatment for depression in the past 4 weeks.
Recruitment
Recruitment is being conducted at two research centres: Monash University, Alfred Campus, Melbourne, and a regional site at Deakin University, Waterfront Campus, Geelong. Participants will be recruited from the community through communication with outpatient mental health and GP services, flyers in community health services, university campuses and health services, community noticeboards, libraries and supermarkets, private clinical networks, traditional media and social media advertising. Recruitment commenced in October 2023 and is anticipated to occur over a 2–2·5-year period.
Trial procedures
Eligibility will be assessed through a three-phase screening process. Prospective participants will complete an online screening questionnaire via REDCap to assess preliminary eligibility. Eligible participants will be invited to attend a first screening call via telephone or online videoconferencing and will receive the Participant Information and Consent Form. During the first screening call, the trial requirements will be described to the participant and they will be shown an example menu plan that presented a mix of intervention and control meals (online Supplementary information) by a research dietitian to facilitate a decision to participate. To be eligible, individuals must consume a habitual diet representative of average diet quality or worse, which is a score of no greater than 11 on a modified Total Diet Score(Reference Russell, Flood and Sadeghpour18) (online Supplementary information). This criterion was included to exclude individuals already on a high quality diet. If this phase of screening is passed, informed consent will be obtained, contact details of a nominated general practitioner will be collected, and the individual will proceed to a second screening call in which the researcher will administer the MADRS to assess severity of depressive symptoms. If the individual meets eligibility criteria for symptom severity, a SCID will be administered to assess whether the diagnostic threshold for current MDD is met.
Eligible individuals will attend two in-person trial visits. Trial visit 1 will occur approximately one week following completion of screening to allow time to assess baseline gastrointestinal symptoms and diet (see below). During trial visit 1 (baseline), participants will complete a series of assessments (Table 1) and will then be randomised to receive either a Mediterranean diet or sham control diet for 4 weeks. Participants will return for trial visit 2 (week 4) to complete repeat assessments and answer a blinding question to assess blinding integrity (i.e. ‘Which of these diets do you think you were allocated to?’: I don’t know, control diet, intervention diet). They will then receive an information sheet about healthy eating for mood, be provided contact information for relevant mental health and dietary support services should they wish to seek assistance, and be reimbursed for any reasonable travel expenses associated with participation. During the following 4-week intervention period, weekly calls to participants assess for adherence, adverse events, medication changes and allow for participants to ask questions.
Schedule of assessments

Randomisation and blinding
Participants with MDD will be allocated to the intervention arms using computer-generated block randomisation, with varying block sizes of 2 and 4, in a 1:1 ratio (intervention to control). The randomisation sequence is generated by a researcher not involved in data collection or participant recruitment. Randomisation will be stratified by sex and presence of current psychotherapy and/or antidepressant treatment at therapeutic dose. All participants recruited as healthy controls will receive the intervention diet and will not be randomised.
Although double-blinding is possible in a feeding trial, blinding in dietary trials is exceedingly challenging and therefore several processes and procedures will be implemented to safeguard blinding. The dietary patterns being investigated will be concealed from participants and instead participants will be told that they are taking part in a trial investigating dietary patterns and their effects on depressive symptoms. Participants and the researcher collecting clinical data will be blinded to group allocation until after analysis is completed. The success of participant and researcher blinding will be measured at trial visit 2 using the James Blinding Index and Bang Blinding Index(Reference Kolahi, Bang and Park20). Unblinded researchers will attend trial visits to verify diet records, coordinate meal orders and provide written instructions about the diet and conduct weekly calls. These unblinded researchers will not have any role in the collection of primary outcome data or analysis of the data.
Intervention and control diets
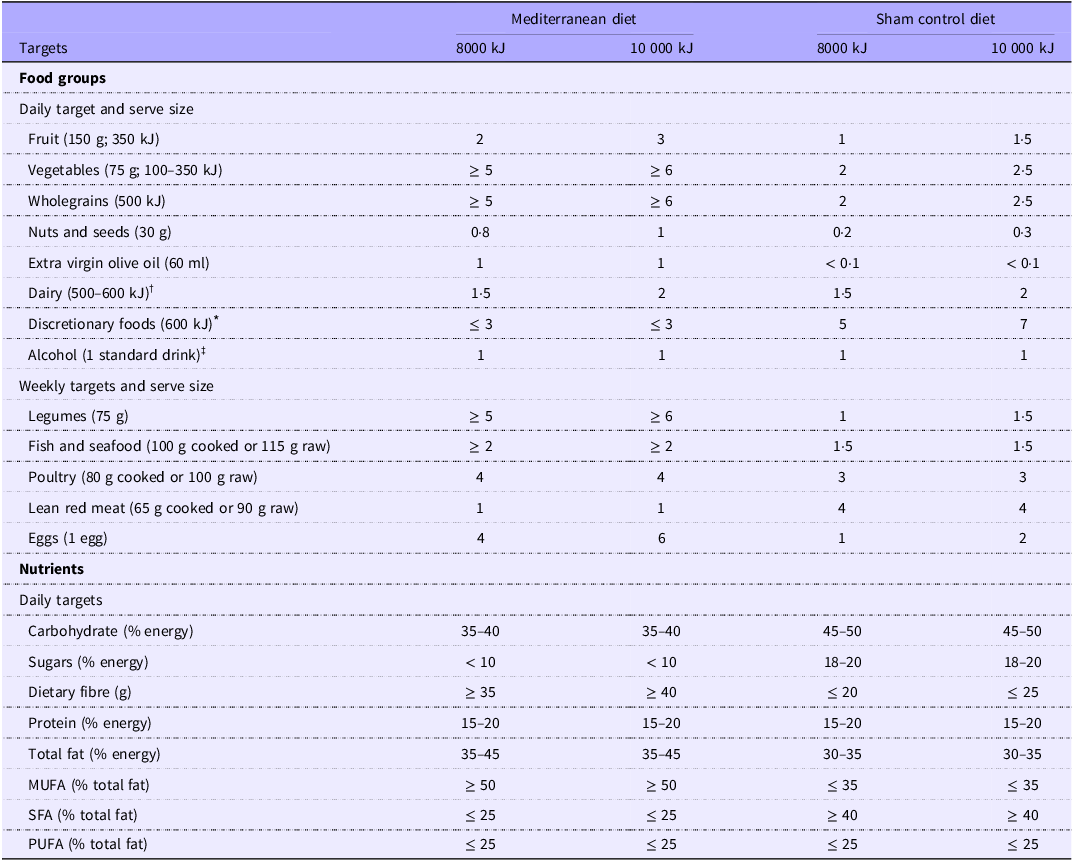
The design and development of intervention and control diets was undertaken by dietetic members of the research team (DT, TR, MH and HMS). Four individuals with lived experience of MDD contributed to the design of trial materials, intervention delivery and recruitment and retention strategy via a focus group in July 2023. Once the diets had been designed, they were validated by comparing with the pre-determined food group targets (Table 2) using nutrition analysis software (Foodworks Professional Version 10; Xyris Software, Australia Pty Ltd). An a priori variance of ±10 % was deemed acceptable. Where variance exceeded 10 %, adjustments were made to the menu until targets had been reached.
Food group targets for the Mediterranean diet and sham control diet at two energy levels

Serve sizes for all food groups, other than extra virgin olive oil, are taken from the Australian Guide to Healthy Eating(41).
* Examples of discretionary foods: Chocolates, chips, muffins, sweet or savoury pastries, processed meats, butter and jam.
† Cheese or yoghurt preferable to milk.
‡ This was an allowance rather than a target. Applicable only for participants already consuming alcohol. Mediterranean diet-100 ml red wine; Sham diet-1 standard drink (any type).
Participants will be provided all food and snacks for the duration of the 4-week trial and will be instructed to eat according to appetite while refraining from non-trial provided food. Provided diets are based on a 7-d rotating menu cycle, comprising a total of three meals and three snacks daily. Food will be delivered weekly with all meals provided in identical trays. Approximately half of the meals are provided ready-made from a commercial meal delivery company and the remaining provided as ingredients from a supermarket delivery for simple meal preparation. Where supermarket items are unavailable, the researcher selects alternative products that facilitate the overall diet to meet the targets for the assigned dietary pattern.
The Mediterranean diet was designed on the basis of an extensive literature search to reflect a traditional Mediterranean diet that is rich in vegetables, fruits, legumes, whole grains and nuts, has extra virgin olive oil as the principal source of dietary fat; moderate intake of fish; and low in red meat and processed foods(Reference Estruch, Ros and Salas-Salvadó21,Reference Serra-Majem, Tomaino and Dernini22) . Specific targets for each food group is provided in Table 2.
In dietary research, an ‘inert’ placebo diet is not possible. Therefore, a sham control diet was designed to represent mean dietary intakes of Australians from the 2011–2012 National Nutrition and Physical Activity Survey which was the most recent survey at the time of menu design(23), whilst also considering the habitual dietary intake of individuals living with moderate to severe major depressive disorder(Reference Opie, O’Neil and Jacka24) (Table 2), and to mimic the corresponding Mediterranean diet meals in appearance where possible. Extra virgin olive oil will be provided to participants separately as total oil targets for the Mediterranean diet group could not be met with bespoke frozen meals alone. Oil will be provided in opaque bottles so participants are not aware of the amount supplied. Measuring spoons will be provided to standardise quantities; 15–20 ml/d will be added in the Mediterranean diet group meals once per day and 5 ml/week in the sham control diet (to one meal/week).
Both diets were developed for two energy levels (8 mJ/d or 10 mJ/d), as per previous recommendations(Reference Tien, Hockey and So14), to enable the intervention to meet the nutritional needs of a range of participants, but were not designed to achieve weight loss. Diets may be adjusted based on participant hunger, activity level and bodyweight changes. Detailed written instructions for complying with the diet, coded by colour only, will be provided to each participant that include recipes for breakfast and some lunch meals, and an additional ‘free food’ list with examples of self-sourced foods and portion sizes that can be consumed in a given day that are in alignment with the diet targets. Instructions will be coded by colour only, and not mention the diet pattern. Beverages and seasonings will not be provided, however, a list of suitable options will be supplied. No more than four cups of tea or coffee are allowed to be consumed, and there are set limits for alcohol for each diet (Table 2). An example of a 1-d menu for each diet is presented in online Supplementary information.
Data collection and outcome measures
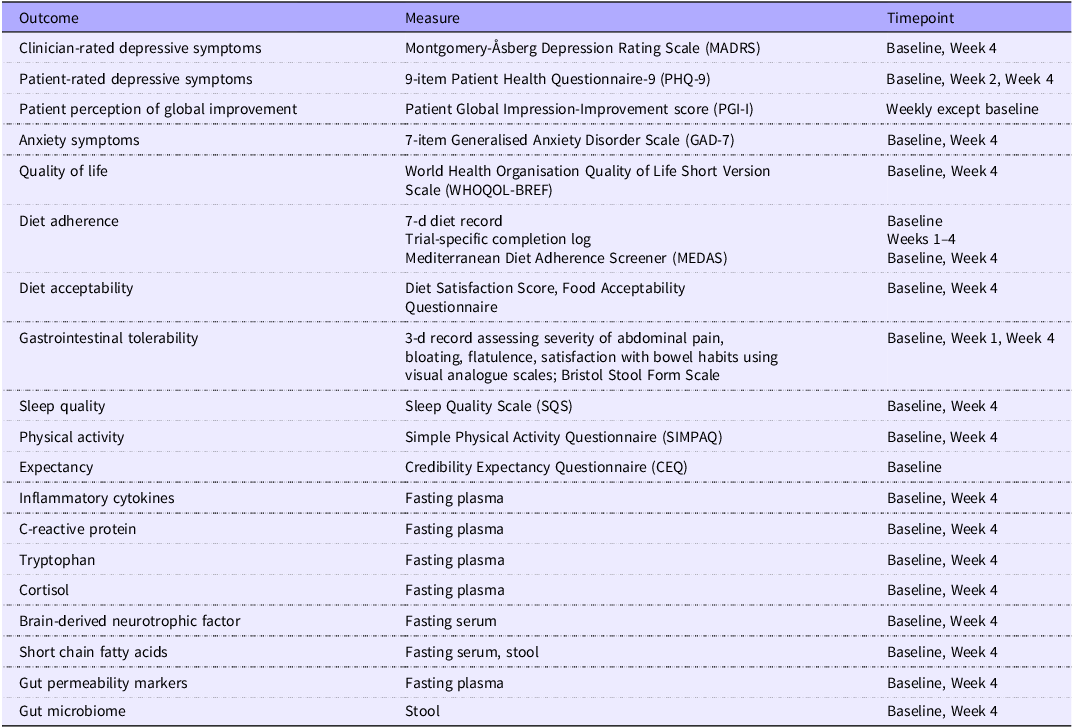
Table 1 presents outcome measures and corresponding timepoints of measurement. Demographic data including gender, age, ethnicity and education will be collected at baseline together with current medication and supplement use, medical history, bodyweight and height.
The primary outcome is between-group differential change from baseline at week four in depression severity measured using the MADRS, a clinician-administered and well validated instrument to measure depression severity(Reference Montgomery and Asberg15). Exploratory outcomes include patient-rated depression severity measured using the 9-item Patient Health Questionnaire-9 (PHQ-9)(Reference Kroenke, Spitzer and Williams25), participants’ overall perception of improvement of depressive symptoms using the Patient Global Impression-Improvement score (PGI-I)(Reference Mohebbi, Dodd and Dean26), anxiety symptoms measured using the Generalized Anxiety Disorder Scale (GAD-7)(Reference Spitzer, Kroenke and Williams27), and quality of life using the World Health Organization Quality of Life Short Version Scale (WHOQOL-BREF)(28). Potential mediators and effect modifiers will be measured, including sleep quality, physical activity and treatment expectation bias. These are measured using the Sleep Quality Scale (SQS)(Reference Snyder, Cai and DeMuro29) and Simple Physical Activity Questionnaire (SIMPAQ)(Reference Rosenbaum, Morell and Abdel-Baki30), and Credibility Expectancy Questionnaire (CEQ)(Reference Borkovec and Nau31), respectively. Bodyweight will be measured using calibrated scales (Seca 813; Seca GmbH & Co. KG) at trial visits and weekly bodyweight will be self-measured at home by participants. Diet acceptability will be measured using the Diet Satisfaction Score(Reference Jospe, Haszard and Taylor32) and additional trial-specific food acceptability questions. Gastrointestinal tolerability will be measured using 3-d visual analogue scales for severity of abdominal pain, bloating, nausea, flatulence and satisfaction with bowel habits based on previously validated measures for pain(Reference Safikhani, Gries and Trudeau33), and stool consistency will be measured using the Bristol Stool Form Scale(Reference Heaton, Radvan and Cripps34).
Fasted blood samples (18·5 ml) will be collected using K2EDTA tubes and serum separator tubes at each trial visit by either an external pathology centre or a co-located health service pathology centre. Samples will be centrifuged at 1500 g at 4°C for 10 min. Plasma and serum aliquots (250 ul each) will be stored at –80℃ for subsequent analysis of circulating inflammatory cytokines, C-reactive protein, tryptophan, brain-derived neurotrophic factor, short chain fatty acids, cortisol and gut permeability markers. Participants will be advised to collect a stool sample on the morning of each trial visit and keep the sample refrigerated at 4°C until attending the research centre. Participants will be provided with instructions and a stool collection kit, including a collection container, gloves, anaerobic generator (Oxoid AnaeroGen Compact, Thermofisher Scientific) sachet and two resealable plastic bags to contain the box. A cool pack will be provided to maintain temperature when transporting the sample. If a sample is not collected prior to or at the visit, it will be collected on a subsequent day. For trial visit 1, the diet intervention will commence only after stool collection. For trial visit 2, if a sample is not able to be collected before or at the visit, the diet intervention will continue until the point of stool collection. Stool samples will be transported to the laboratory within 4 h and processed in an anaerobic hood. Whole stool samples (2 g per vial) will be stored in sterile 2 mL O-ring screw-cap cryovials at –80℃ for subsequent analysis of gut microbiome and metabolite composition.
Adherence
Participants will record their dietary intake using a 7-d food record at baseline and a trial-specific completion log to record consumption of the trial meals across the 4-week trial. Consumption of each meal and snack will be recorded as ‘all’, ‘3/4’,‘1/2’, ‘¼’, ‘none’ and participants are encouraged to provide notes detailing additional foods and drinks consumed, and details for why meals or snacks were not fully consumed. Participants will be classified as being adherent if ≥ 80 % of food was consumed over the entire intervention, poorly adherent if 50–79 % of food was consumed, and non-adherent if < 50 % of food was consumed. The Mediterranean Diet Adherence Screener(Reference Schröder, Fitó and Estruch35) will also be used as a supplementary measure of adherence.
Safety and adverse events
Safety protocols were developed for trial visits and weekly calls in conjunction with the team psychiatrists (PH, DK), to monitor the safety of participants throughout the trial. All participants will be advised to continue usual care from their treating clinician while participating in the trial. At weekly assessments, if a participant expresses suicidal ideation, selects mood as ‘much worse’ or ‘very much worse’ on the patient global impression-improvement score or scores 1, 2 or 3 on the Patient Health Questionnaire-9 item 9, the principal investigator will be notified, and a suicide risk screening assessment will be administered. If the participant is assessed as high suicide risk, the rostered team mental health clinician, and emergency services where indicated, will be notified. Such participants will subsequently be withdrawn from the trial to ensure their safety.
Adverse events
All adverse events (AE) will be documented in the participant electronic trial record and will include: the onset date, duration, date of resolution (if resolved), severity (mild, moderate, or severe), seriousness, actions taken, outcome and likelihood of the relationship of the AE to the trial intervention (definitely related, probably related, possibly related, unlikely to be related and definitely unrelated). In the circumstance of a severe adverse event, participants will be encouraged to attend medical services, and the participant will be followed up until the AE resolves, stabilises, or a participant is lost to follow-up. Any treatment related to an AE will be documented. One blinded and one independent unblinded psychiatrist will review AEs every six months for the purposes of evaluating ongoing trial safety.
Data analysis and dissemination
A sample size of 22 participants per group was selected to achieve at least 18 completers per group to meet the trial’s aims regarding quantifying a treatment signal and feasibility. This sample size is in line with previously conducted feeding studies in populations with cardiometabolic diseases(Reference Krishnan, Adams and Allen36), diabetes(Reference Gardner, Landry and Perelman37) and weight management(Reference Liu, Zhang and Ye38). A sample size of 18 per trial arm achieves 80 % power to detect a standardised mean difference of one for between-group change in MADRS at the significance level of 0·05. The biostatistician and researcher conducting the analysis will be blinded to group allocation until the primary endpoint has been analysed. The primary analysis of the primary endpoint will be an intention-to-treat analysis including all randomised participants who received the intervention diet for at least 1 day. Additionally, a per-protocol analysis will include data from all participants who completed the trial, who were assessed for the primary outcome within ± 3 d of the 28-d timepoint, and were considered adherent to the diet.
The primary outcome (mean difference in change between MADRS scores between intervention and control groups) will be analysed using generalised estimation equation models. The generalised estimation equation for the primary outcomes includes nominal independent variables for follow-up timepoint, intervention allocation, and the two–way interaction between time and group allocation. The two-way interaction measures between-group differential change from baseline at week 4 and estimates the intervention effect. All continuous exploratory outcomes will be analysed similarly. A ≥ 50 % reduction in MADRS score will be used to classify participants into responder and non-responder categories consistent with criteria used in antidepressant drug trials(Reference Papakostas, Trivedi and Shelton39,Reference Raison, Sanacora and Woolley40) . Dietary intake will be analysed to determine adherence and to assess the integrity of the sham diet. Diet acceptability and gastrointestinal tolerability will be compared between and within groups. Missing data will be imputed using appropriate multiple imputation techniques. Exploratory analysis may be conducted comparing participants receiving treatment (anti-depressant medication and/or psychotherapy) and not receiving treatment. Exploratory analyses may also be conducted to assess baseline differences between responders and non-responders. Responses from the blinding assessment will be assessed and reported using a contingency table (2 × 3 format). If required, subgroup analyses will be conducted to assess change in MADRS score among participants with incorrect/’I don’t know’ allocation guesses and among those with correct allocation guesses.
Biological measures will be compared between MDD and healthy individuals at baseline. The differential impact of the Mediterranean diet on biological measures will be examined in the MDD and healthy individuals. The impact of diet on microbiome-gut-brain axis signalling pathways will be evaluated including compositional and functional alterations in the gut microbiome, immune function, gastrointestinal permeability, host and microbial tryptophan metabolism and biomarkers of stress physiology including cortisol.
Data will be disseminated to participants through a plain language summary and to clinicians and researchers through conventional scientific dissemination routes (e.g. conferences and scientific publication).
Discussion
There is an urgent need to identify definitive new approaches to reduce the global burden of depressive disorders. There is accumulating evidence that diet intervention, and specifically the Mediterranean diet, has strong potential for improving symptoms of depression. However, uncertainty remains regarding whether improvements reflect change in specific dietary components, expectancy effects or other nonspecific factors. A hypothetical example of a nonspecific factor is participation in a new diet encouraging participants to address other lifestyle issues (e.g. trying to sleep better and exercise more) that may affect their mood. Alternatively, commitment to a new diet, including planning meals, cooking and tracking food, could improve mood through increased activity and routine. Previous trials have been limited by lack of blinding, inadequate controls and minimal investigation of underlying biological mechanisms, leaving critical questions unanswered. The Optimising Nutritional Psychiatry Treatment: Investigating the Mediterranean Diet to Improve Symptoms of Major Depressive Disorder trial will address these key gaps through investigating the effectiveness of a Mediterranean diet in clinical depression through a rigorously designed double-blind sham-controlled randomised feeding trial. By integrating comprehensive biological sampling and mechanistic analyses, this trial will also provide new insights into how diet may influence mood. In both ways, the study will advance the developing evidence that supports diet as an adjunctive approach to treat depressive symptoms in people with MDD.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114526107272
Acknowledgements
We acknowledge our focus group of people with lived experience of MDD who provided input into the design of trial materials, intervention delivery and recruitment and retention strategy. We also acknowledge Tayla John, Research Fellow and mental health nurse (Deakin University), who assisted in the development of our safety escalation protocol and provided occasional mental health support to participants and staff.
This work was supported by the National Health and Medical Research Council under Grant APP2018118.
H. M. S. conceptualised the study. D. T. and H. M. S. wrote the draft. All authors reviewed and approved the final manuscript.
D. T. and L. P. are supported by a Department of Medicine, Monash University PhD scholarship. C. K. Y.’s department, the Department of Gastroenterology, Monash University receives royalties from the sales of digital apps, online education course on the FODMAP diet. No author receives personal renumeration. F. N. J. has received competitive grant/research support from the Brain and Behavior Research Institute, the National Health and Medical Research Council, Australian Rotary Health, the Geelong Medical Research Foundation, the Ian Potter Foundation and the University of Melbourne; industry support for research from Meat and Livestock Australia, Woolworths Limited, the a2 Milk Company and Be Fit Food; philanthropic support from the Fernwood Foundation, Wilson Foundation, the JTM Foundation, the Serp Hills Foundation, the Roberts Family Foundation and the Waterloo Foundation and travel support and speakers’ honoraria from Sanofi-Synthe´labo, Janssen Cilag, Servier, Pfizer, Network Nutrition, Angelini Farmace´utica, Eli Lilly and Metagenics. F. N. J. has written two books for commercial publication. She is on the scientific advisory board of the Dauten Family Center for Bipolar Treatment Innovation and Zoe Limited. She is currently supported by an National Health and Medical Research Council Investigator grant L1 (#1194982). The Food & Mood Center has received grant/research support from the a2 Milk Company, Be Fit Food, Meat and Livestock Australia and Woolworths Limited and philanthropic support from the Fernwood Foundation, Wilson Foundation, the JTM Foundation, the Serp Hills Foundation, the Roberts Family Foundation and the Waterloo Foundation. G. C. has received honoraria from Janssen, Probi, Apsen and Ingelheim Boehringer as an invited speaker; is in receipt of research funding from Pharmavite, Fonterra, Reckitt, Nestle and Tate and Lyle and has been paid for consultancy work by Yakult, Zentiva, Bayer Healthcare and Heel Pharmaceuticals. This support neither influenced nor constrained the contents of this manuscript. H. M. S. has received research funding from the Rome Foundation, honoraria from Dietitian Connection, Rome Foundation, Falk Pharmaceuticals and Dietitians Australia and has received travel funding for an International Scientific Association for Prebiotic and Probiotic Consensus meeting. The other authors have no competing interests to declare.



 Open access
Open access