Each year 2·3 million women are diagnosed with breast cancer along with 685 000 deaths from breast cancer globally(Reference Sung, Ferlay and Siegel1). In addition to oncology treatments, cancer survivors are eager to seek nutritional approaches to further improve their survival(Reference Guo, Kuo and Shih2,Reference Stull, Snyder and Demark-Wahnefried3) . The World Cancer Research Fund (WCRF) and the American Institute for Cancer Research (AICR) recommend cancer survivors to follow their cancer prevention guidelines, which encourage gradual reductions in animal foods and concurrent increases in plant foods to shift towards a plant-based diet(4,Reference Clinton, Giovannucci and Hursting5) . Such a diet is characterised by plentiful anti-inflammatory components and low-energy density(Reference Farmer6–Reference Recio, Andujar and Rios8) and may reduce inflammation(Reference Hermsdorff, Zulet and Puchau9,Reference Hosseini, Berthon and Saedisomeolia10) and adiposity(Reference Tran, Dale and Jensen11), resulting in better breast cancer prognosis(Reference Caan, Cespedes Feliciano and Prado12–Reference Pierce, Ballard-Barbash and Bernstein14).
However, not all plant foods are healthful. For example, certain plant foods (such as whole grains, fruits, and vegetables) are generally considered as healthful and associated with better breast cancer prognosis(Reference Ernest, Lemus and Hsu15,Reference Farvid, Holmes and Chen16) , whereas some plant foods (such as fruit juices, sugar-sweetened beverages, and refined grains) are less healthful and associated with worse survival after breast cancer diagnosis(Reference Farvid, Holmes and Chen16–Reference Farvid, Spence and Rosner18). Thus, it is important to differentiate plant foods by their health-related effects and explore biological mechanisms through which different plant-based dietary patterns may impact the prognosis of breast cancer survivors.
We derived three plant-based diet indices that emphasised different aspects of plant-based foods:(Reference Chen, Drouin-Chartier and Li19–Reference Kim, Caulfield and Garcia-Larsen22) an overall plant-based diet index (PDI) that emphasised consumption of all plant foods (regardless of healthful or unhealthful), healthful plant-based index (hPDI) that emphasised consumption of healthful plant foods and unhealthful plant-based index (uPDI) that emphasised consumption of unhealthful plant foods, and we previously reported that the associations of PDI, hPDI, and uPDI with breast cancer survival differed in directions and magnitudes(Reference Anyene, Ergas and Kwan23), likely through their differing impacts on inflammation and adiposity(Reference Eichelmann, Schwingshackl and Fedirko24,Reference Ratjen, Morze and Enderle25) . To provide insight into such potential biological mechanisms that may affect breast cancer prognosis, we selected several important inflammation biomarkers related to systemic inflammation (high-sensitivity C-reactive protein [hsCRP]), pro-inflammatory cytokines (IL-1β, IL-6, IL-8, and TNF-α) and anti-inflammatory cytokines (IL-4, IL-10, and IL-13). Regarding adiposity and other body composition measurements, we measured the areas of muscle, visceral adipose tissue (VAT) and subcutaneous adipose tissue (SAT) from clinical computed tomography (CT) scans. We thus conducted a cross-sectional study to examine the associations of plant-based diet indices with inflammation biomarkers and body composition among 3659 breast cancer survivors at approximately 2 months after diagnosis.
Methods
Study cohort
The Pathways Study is an ongoing prospective cohort study with active follow-up that enrolled 4504 women with breast cancer diagnosed between late 2005 and May 2013 in Kaiser Permanente Northern California (KPNC)(Reference Kwan, Ambrosone and Lee26). Women with newly diagnosed invasive breast cancer were identified through rapid case ascertainment and enrolled on average 2 months after diagnosis. The enrolment rate was 40·3 % of eligible participants during the study period, and enrolled participants were representative of the breast cancer population at KPNC. Participants were interviewed in person and their sociodemographic, anthropometric, dietary and lifestyle and other information were collected through questionnaires and measurements. Blood specimens were collected at baseline and then sent to Roswell Park Comprehensive Cancer Center (Buffalo, NY, USA) for blood component fractionation into plasma and serum samples for long-term storage at –150°C in liquid nitrogen freezers. Clinical CT scans within 6 months of diagnosis and before chemotherapy or radiation were extracted for body composition assessment. This study was approved by the institutional review boards at all participating institutions, and all participants provided written informed consent at the time of enrolment.
Dietary assessment
A modified version of Block 2005 Food Frequency Questionnaire (FFQ) was collected at a median of 2·0 (interquartile 1·6–2·6) months after cancer diagnosis(27). This questionnaire included 139 food items plus additional dietary questions to be representative of a wide range of dietary factors and accommodate more ethnically (such as Asian and Hispanic) diverse foods. Participants were asked how often (from never to every day), on average, they consumed a defined portion of these food items in the past 6 months. A total of 845 participants were excluded because of incomplete questionnaires (n 782) or implausible calorie intake (n 63; <400 or >4000 calories per day for women). Thus, the final study population was 3659 for this analysis.
Based on nutrient and culinary similarities (online Supplementary Table 1), food items were combined into eighteen food groups and then constructed into three large categories: healthful plant foods (such as whole grains, fruits, and vegetables), less healthful plant foods (such as fruit juices, refined grains, and sugar-sweetened beverages) and animal foods (such as egg, meat, and animal fat)(Reference Satija, Bhupathiraju and Rimm20,Reference Satija, Bhupathiraju and Spiegelman21) .
We computed three previously established plant-based diet indices:(Reference Satija, Bhupathiraju and Rimm20,Reference Satija, Bhupathiraju and Spiegelman21) (1) PDI, which emphasises consumption of all plant foods (regardless of healthfulness) while reducing consumption of animal food; (2) hPDI, which emphasises intakes of healthful plant food groups; and (3) uPDI, which emphasises intakes of less healthful plant food groups(Reference Farvid, Barnett and Spence17,Reference Farvid, Spence and Rosner18) . For each food group, participants’ intake was ranked into quintiles (Q; from Q1 to Q5). If the food group was consistent with the emphasis of that index, positive points were assigned (Q1 → Q5:1 point → 5 points); otherwise, reverse points were assigned (Q5 → Q1:1 point → 5 points). Therefore, the final possible ranges for three indices were 18 to 90 points across the eighteen food groups.
Inflammation biomarkers
Out of 3659 participants with valid FFQ at baseline, 3350 (91·6 %) provided blood at a median of 2·8 (interquartile: 2·0–3·3) months after diagnosis, of whom 3329 (99·4 %) were tested for hsCRP using serum samples and 3350 (100 %) were tested for pro-inflammatory and anti-inflammatory cytokines using plasma samples.
Serum samples were assayed to quantitatively determine the concentrations of hsCRP in the Advanced Research and Diagnostic Laboratory at the University of Minnesota using a latex-particle enhanced immunoturbidimetric assay kit (Roche Diagnostics) and read on the Roche Cobas 8000 Chemistry analyser (Roche Diagnostics). Four samples had concentrations below the limitation of detection (LOD: 0·15 mg/L) and were assigned a value of LOD/
 $\sqrt 2 $
(Reference Lambert, Peterson and Terpenning28,Reference Lubin, Colt and Camann29) .
$\sqrt 2 $
(Reference Lambert, Peterson and Terpenning28,Reference Lubin, Colt and Camann29) .
Plasma samples were assayed for pro-inflammatory cytokines (IL-1β, IL-6, IL-8, and TNF-α) and anti-inflammatory cytokines (IL-4, IL-10, and IL-13) using commercially available multiplex bead array kits (MilliporeSigma Inc.) and read on the Luminex 200 analyser (Luminex Corporation Inc.). Following the manufacturer’s instructions, the experiment and instrument set-up were performed in the Flow and Immune Analysis Shared Resource at Roswell Park Comprehensive Cancer Center and completed using two batches in 2013 and 2018. To account for possible batch effects, plasma samples from seventy-two participants were repeatedly assayed in both 2013 and 2018. The concentrations of each cytokine were determined by extrapolating each experimental fluorescence intensity value against each cytokine’s standard curve using the BeadView software (Luminex Corporation Inc.). To account for plate-to-plate variability and normalise cytokine concentration data, a common sample consisting of pooled participant samples was processed across each plate. For each cytokine and plate, a reliable lower analytical limit of detection (RLAL; value of the lowest prepared standard curve concentration) and LOD (value of assay buffer alone) were defined. For all cytokines (except IL-6), <3 % of plasma samples had concentrations below the LOD, whereas 10 % of plasma samples had concentrations below the LOD for IL-6. Samples below the LOD were assigned a value of RLAL/
 $\sqrt 2 $
or LOD/
$\sqrt 2 $
or LOD/
 $\sqrt 2 $
, whichever was smaller(Reference Croghan and Egeghy30).
$\sqrt 2 $
, whichever was smaller(Reference Croghan and Egeghy30).
Body composition
Out of 3659 participants with valid FFQ, 741 (20·3 %) had available CT scans at a median of 1·5 (interquartile: 0·4–1·7) months after diagnosis. Two centrally trained research staff quantified the cross-sectional areas (cm2) of muscle and adipose tissue from CT scans at the third lumbar vertebra (L3) using SliceOmatic Software, version 5·0 (TomoVision Inc.)(31). The areas of muscle, VAT, and SAT were determined using anatomic knowledge and tissue-specific Hounsfield unit ranges(Reference Cheng, Caan and Chen32). Additionally, the coefficients of variation between two raters were 0·66 % for muscle, 6·72 % for VAT, and 0·79 % for SAT(Reference Caan, Cespedes Feliciano and Prado12,Reference Cespedes Feliciano, Chen and Lee13) . Prior studies suggested that single-slice areas on abdominal CT scans are highly correlated with whole-body volumes of muscle and adipose tissue from MRI(Reference Shen, Punyanitya and Wang33,Reference Mourtzakis, Prado and Lieffers34) .
Participant characteristics
Through the KPNC resources including the KPNC Virtual Data Warehouse, KPNC Research Database (containing electronic health record data) and KPNC Cancer Registry, we obtained information on age at diagnosis (years), stage (I, II, III, IV), oestrogen receptor (ER; positive, negative, unknown), progesterone receptor (PR; positive, negative, unknown), human epidermal growth factor receptor 2 (HER2; positive, negative, unknown) and Elixhauser comorbidity index (0, 1, 2, ≥3, unknown). Through baseline questionnaires augmented when appropriate with data from electronic health records, we obtained self-reported race and ethnicity (American Indian/Alaska Native, Asian/Pacific Islander, Black, Hispanic, non-Hispanic White), education (high school or less, some college, college graduate, postgraduate, unknown), income (<$50 000, $50 000–$89 999, ≥$90 000, unknown), marital status (married, single, unknown), menopausal status (premenopausal, postmenopausal), body mass index (BMI; kg/m2), physical activity (MET-h/week) and smoking status (never, former, current, unknown).
Statistical analysis
Participant characteristics were summarised and compared by quintiles of plant-based diet indices using ANOVA for continuous variables and χ 2 tests for categorical variables. The concentrations of inflammation biomarkers were log-transformed to reduce the skewness in the distribution, and their results were exponentially transformed back for interpretation.
For adjusted analyses, we applied multivariable linear regression to estimate the associations of each plant-based index (per 10-point increase) with relative differences (%) in inflammation biomarkers and absolute differences (cm2) in body composition. The relative difference was defined as the absolute difference of cytokine concentrations divided by the previous cytokine concentration, when each plant-based index increased by 10 points. The absolute difference was defined as the difference in body composition measurements, when each plant-based index increased by 10 points. The relative difference, rather than absolute difference, was calculated for inflammation biomarkers since their data were log-transformed, and further details on analytic methods are included in the Supplementary Methods.
Considering biological plausibility and change-in-estimate criterion (10 % cut-off)(Reference Maldonado and Greenland35,Reference Mickey and Greenland36) , the following were included as potential covariates for multivariable linear regression:
-
(1) demographic and clinicopathological factors: age, race and ethnicity, education, income, marital status, menopausal status, stage, ER, PR, HER2, and Elixhauser comorbidity index.
-
(2) lifestyle factors: total energy intake, BMI, physical activity, and smoking status.
-
(3) blood collection and processing-related factors: season of blood draw, time of blood draw in relation to breast cancer treatment received, time of storage before assaying, and batch year.
For each inflammation biomarker, its statistical model was adjusted for (1) demographic and clinicopathological factors; (2) lifestyle factors; and (3) blood collection and processing-related factors. For each body composition measurement, its statistical model was adjusted for (1) demographic and clinicopathological factors and (2) lifestyle factors. Inflammation biomarkers and body composition measurements were not mutually adjusted in their statistical models. For covariates in multivariable analysis, we substituted missing data with median values for continuous covariates and ‘unknown’ for categorical covariates(Reference Little and Rubin37). For different inflammation biomarkers, their sample sizes may be different because (1) available blood samples differed when assaying hsCRP and other inflammatory cytokines, and (2) inflammation biomarkers had different missing values when performing laboratory assays.
For sensitivity analysis, we additionally adjusted for alcohol intake due to its controversial role in inflammation(Reference Imhof, Froehlich and Brenner38), body composition(Reference Steiner, Gordon and Lang39,Reference Beulens, van Beers and Stolk40) and breast cancer prognosis(Reference Kwan, Valice and Ergas41). For subgroup analysis, we analysed whether the associations of plant-based diet with inflammation biomarkers and body composition measurements differ by tumour stage (I v. II–IV), ER status (ER + v. ER–) and smoking status (current/former v. never).
We conducted statistical analyses using SAS statistical software, version 9·4 (SAS Institute Inc.) and R, version 4·4·0 (The R Foundation for Statistical Computing). All P-values were two-sided, and point estimates were presented with 95 % CI. We considered P-value < 0·05 as statistically significant and did not adjust for multiple comparisons.
Results
Descriptive statistics
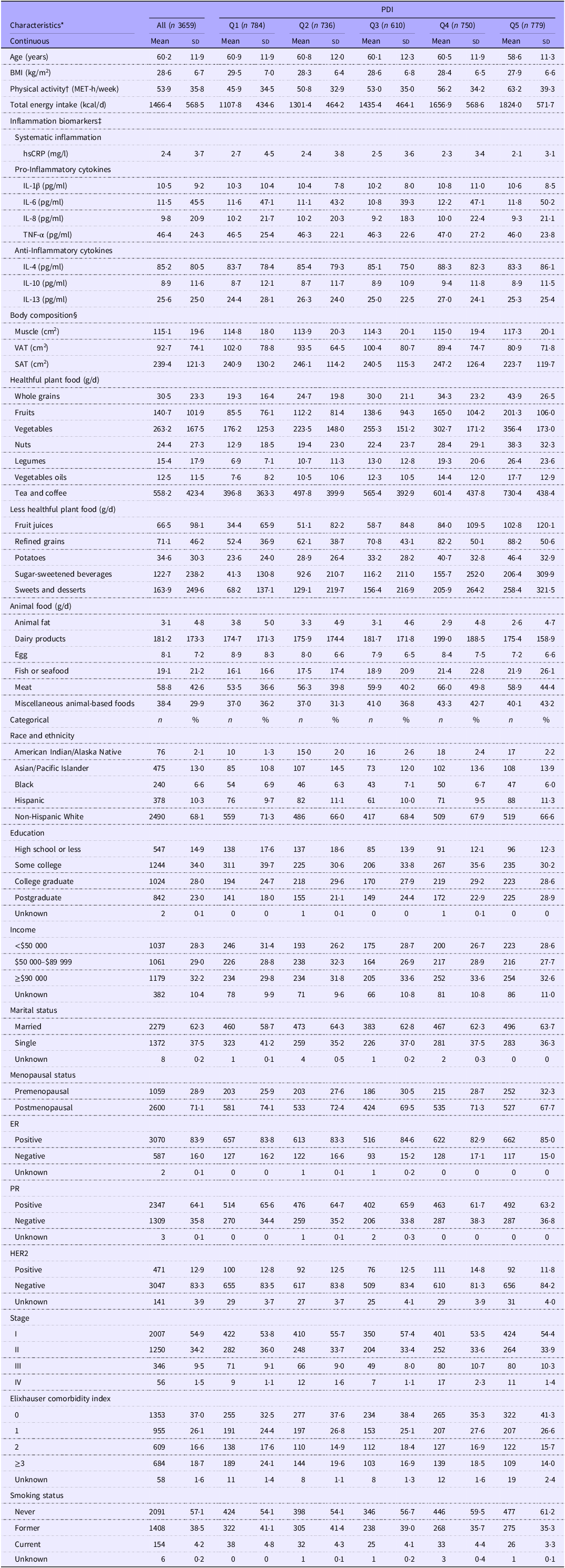
Of 3659 study participants included in the final analysis (Table 1), the mean (sd) of age was 60·2 (11·9) years and 2490 (68·1 %) self-identified as non-Hispanic White. The mean (sd) points of plant-based diet indices were 54·0 (6·8) for PDI, 54·2 (8·3) for hPDI and 54·0 (8·2) for uPDI. The correlations (r s) were 0·16 (P-value < 0·001) between PDI and hPDI, –0·17 (P-value < 0·001) between PDI and uPDI and –0·34 (P-value < 0·001) between hDPI and uPDI. For the intake of food groups, the correlations (r s) were 0·07 (P-value < 0·001) between healthful plant foods and unhealthful plant foods, 0·23 (P-value < 0·001) between healthful plant foods and animal foods and 0·28 (P-value < 0·001) between unhealthful plant foods and animal foods.
Descriptive characteristics of 3659 women with breast cancer by quintiles of PDI

ER, oestrogen receptor; HER2, human epidermal growth factor receptor 2; MET, metabolic equivalents; PDI, overall plant-based diet index; PR, progesterone receptor; SAT, subcutaneous adipose tissue; VAT, visceral adipose tissue.
* Continuous variables were presented as mean (sd) and categorical variables were presented as number (%). For inflammation biomarkers, the geometric mean (geometric sd) was presented instead. Percentages may not add up to 100 % because of rounding. P-value was calculated using ANOVA for continuous variables and χ 2 tests for categorical variables. If the assumptions of χ 2 tests were violated, likelihood ratio χ 2 tests were used instead.
† Number of missing for physical activity: 4.
‡ Number of observations available for inflammatory biomarkers: 3329 for hsCRP; 3348 for IL-8; 3349 for IL-4; 3350 for IL-1β, IL-6, TNF-α, IL-10 and IL-13.
§ Number of observations available for body composition (muscle, VAT and SAT): 741.
Compared with those in the lowest quintile of PDI (Table 1), participants in the highest quintile of PDI were more likely to be younger; have higher physical activity, total energy intake, and education; and have lower BMI, systemic inflammation, and comorbidities. Compared with those in the lowest quintile of hPDI (online Supplementary Table 2), participants in the highest quintile of hPDI were more likely to be older, non-Hispanic White, postmenopausal, early stage, and never smokers; have higher physical activity and education; and have lower BMI, total energy intake, systemic inflammation, muscle, VAT, SAT, and comorbidities. Compared with those in the lowest quintile of uPDI (online Supplementary Table 3), participants in the highest quintile of uPDI were more likely to be younger, racial and ethnic minorities, single, premenopausal, and current smokers; have higher BMI, systemic inflammation, and comorbidities; and have lower physical activity, total energy intake, education, income, and SAT.
Plant-based diet, inflammation biomarkers and body composition
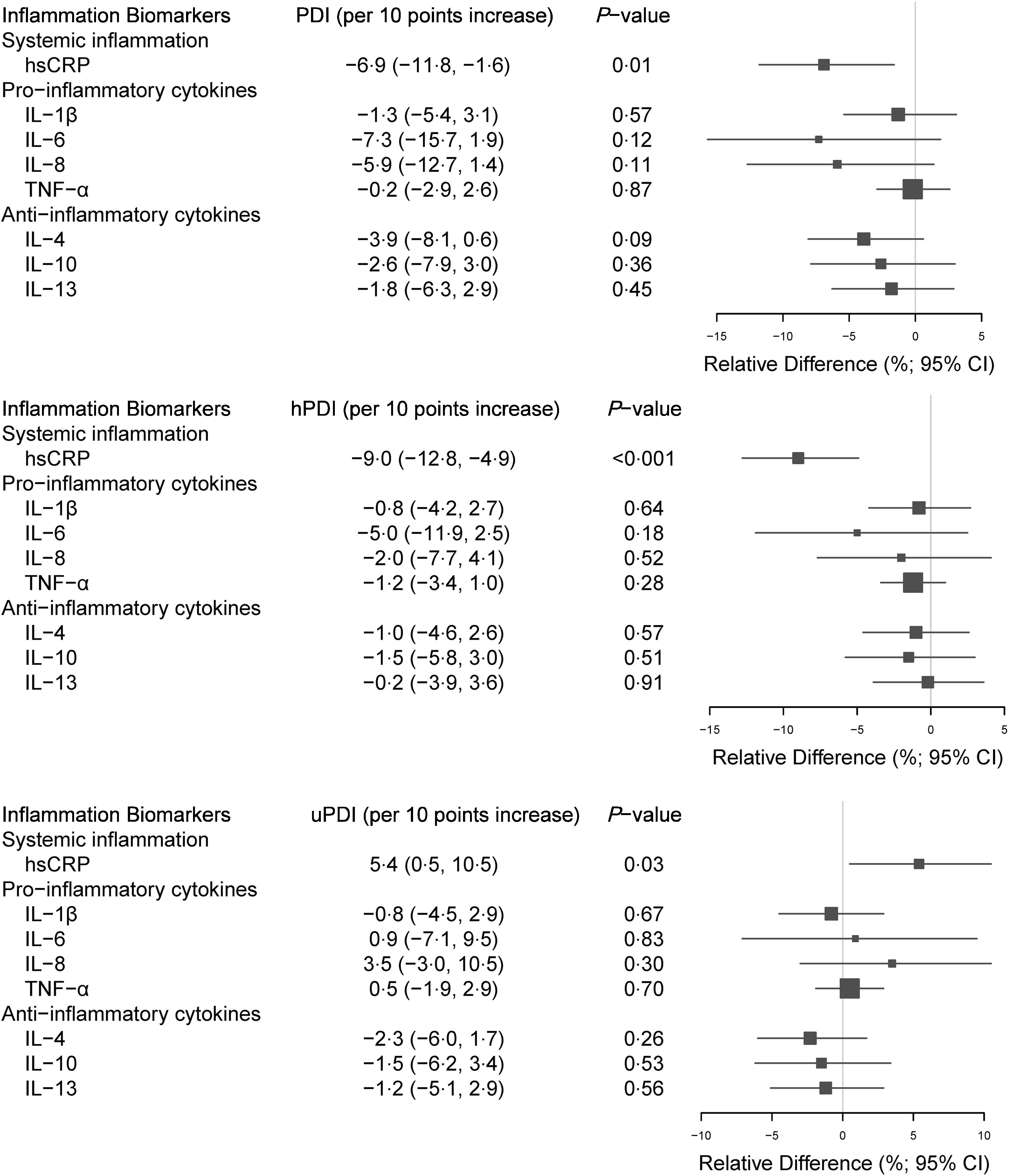
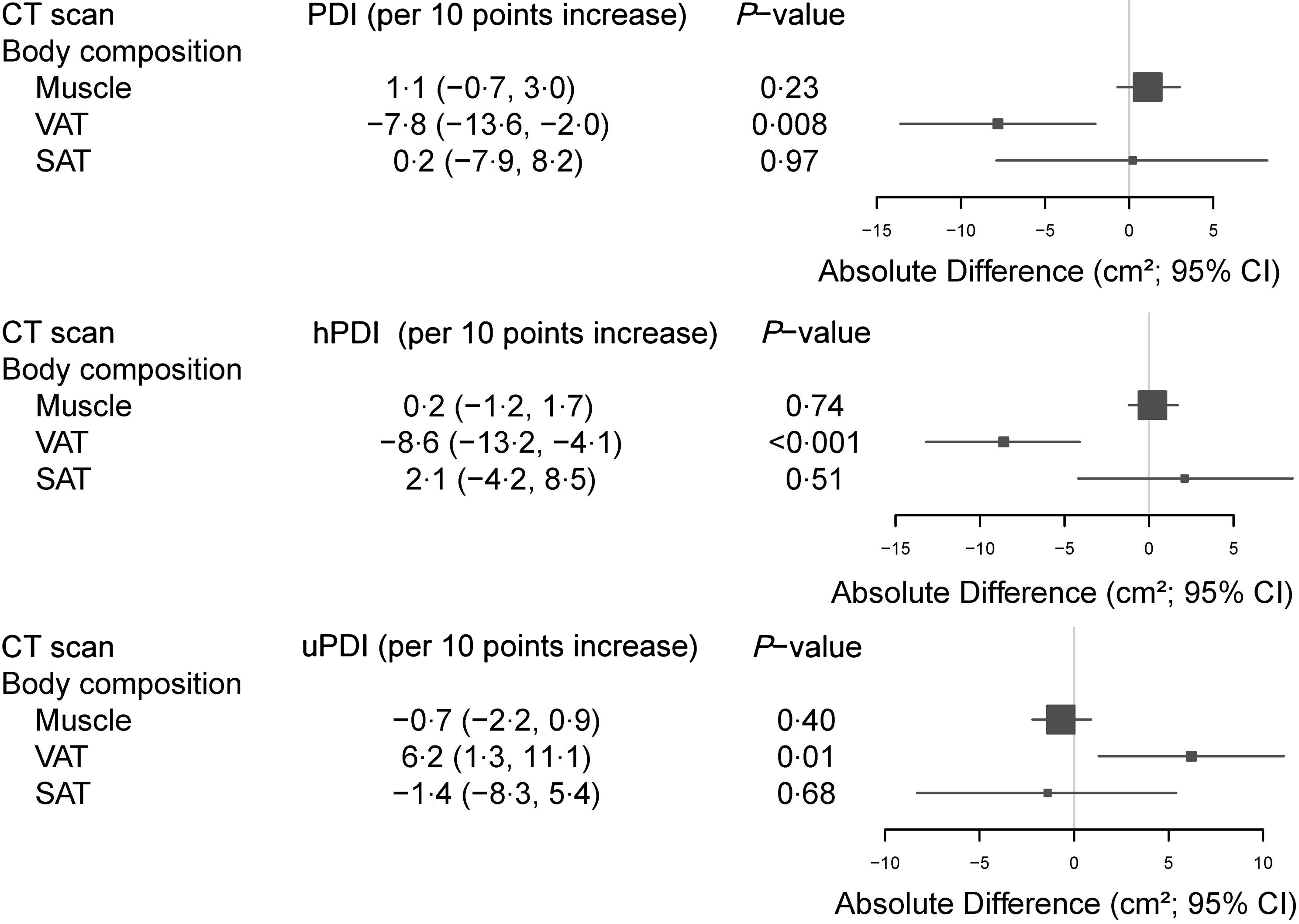
In multivariable adjustment analyses for three plant-based diet indices with inflammation biomarkers (Fig. 1) and body composition (Fig. 2), significant associations were only found for hsCRP and VAT, but not for other inflammation biomarkers or body composition measurements. Per 10-point increase for each index, the relative difference in hsCRP was –6·9 % (95 % CI –11·8%, –1·6%) for PDI, –9·0 % (95 % CI –12·8%, –4·9%) for hPDI and 5·4 % (95 % CI 0·5%, 10·5%) for uPDI; and the absolute difference in VAT was –7·8 cm2 (95 % CI –13·6 cm2, –2·0 cm2) for PDI, –8·6 cm2 (95 % CI –13·2 cm2, –4·1 cm2) for hPDI and 6·2 cm2 (95 % CI 1·3 cm2, 11·1 cm2) for uPDI.
Adjusted† associations of plant-based Indices (per 10-point increase) with relative changes (%) of inflammatory biomarkers ‡ §. hPDI, healthful plant-based diet index; PDI, overall plant-based diet index; uPDI, unhealthful plant-based diet index. †Multiple linear regression were adjusted in separate models for (1) demographic and clinicopathological factors: age (years), race and ethnicity (American Indian/Alaska Native, Asian/Pacific Islander, Black, Hispanic, non-Hispanic White), education (high school or less, some college, college graduate, postgraduate, unknown), income (<$50 000, $50 000–$89 999, ≥$90 000, unknown), marital status (married, single, unknown), menopausal status (premenopausal, postmenopausal), stage (I, II, III, IV), ER (positive, negative, unknown), PR (positive, negative, unknown), HER2 (positive, negative, unknown) and Elixhauser comorbidity index (0, 1, 2, ≥3, unknown); (2) lifestyle factors: total energy intake (kcal/d), BMI (kg/m2), physical activity (MET-h/week) and smoking status (never, former, current, unknown); and (3) blood collection and processing-related factors: season of blood draw (Jan–Mar, Apr–Jun, Jul–Sep, Oct–Dec), time of blood draw in relation to breast cancer treatment received (prior to any treatment, after neoadjuvant chemotherapy before surgery, after surgery before adjuvant chemotherapy, after surgery and chemotherapy (with or without radiation or hormonal therapy), after radiation (with or without surgery or hormonal therapy), after hormonal therapy (with or without surgery), after other treatments), time of storage before assaying (years) and batch year (2013, 2018). ‡Number of observations used for calculations: 3329 for hsCRP; 3348 for IL-8; 3349 for IL-4; 3350 for IL-1β, IL-6, TNF-α, IL-10 and IL-13. §Concentrations of Inflammatory biomarkers were calculated on the log scale and exponentially transformed back for interpretation.

Adjusted† associations of plant-based Indices (per 10-point increase) with absolute changes (cm2) of body composition ‡. hPDI, healthful plant-based diet index; PDI, overall plant-based diet index; SAT, subcutaneous adipose tissue; uPDI, unhealthful plant-based diet index; VAT, visceral adipose tissue. † Multiple linear regression were adjusted in separate models for (1) demographic and clinicopathological factors: age (years), race and ethnicity (American Indian/Alaska Native, Asian/Pacific Islander, Black, Hispanic, non-Hispanic White), education (high school or less, some college, college graduate, postgraduate, unknown), income (<$50 000, $50 000–$89 999, ≥$90 000, unknown), marital status (married, single, unknown), menopausal status (premenopausal, postmenopausal), stage (I, II, III, IV), ER (positive, negative, unknown), PR (positive, negative, unknown), HER2 (positive, negative, unknown) and Elixhauser comorbidity index (0, 1, 2, ≥3, unknown); and (2) lifestyle factors: total energy intake (kcal/d), BMI (kg/m2), physical activity (MET-h/week) and smoking status (never, former, current, unknown). ‡ Number of observations used for calculations (muscle, VAT and SAT): 741.

Sensitivity analysis and subgroup analysis
After additional adjustment for alcohol intake, the associations of plant-based diet indices with inflammation biomarkers (online Supplementary Fig. 1) and body composition (online Supplementary Fig. 2) remained similar and the findings did not change: significant associations were only observed for hsCRP and VAT, but not for other inflammation biomarkers or body composition measurements.
Overall, the associations of plant-based diet indices with inflammation biomarkers and body composition did not differ by tumour stage, ER status and smoking status (online Supplementary Table 4). Although we observed a few significant interactions (P interaction < 0·05), there were no consistent patterns for these findings, and false-positive results in subgroup analyses may likely happen due to testing multiple hypotheses. Thus, these results should be interpreted cautiously, given that multiple comparisons were not adjusted.
Discussion
In this study of women with breast cancer, we found that greater concordance with an overall or healthful plant-based diet was significantly associated with lower hsCRP and VAT, whereas greater concordance with an unhealthful plant-based diet was significantly associated with higher hsCRP and VAT. These findings support recommending a plant-based diet, especially a healthful plant-based diet, for women with breast cancer.
To date, three prospective cohort studies conducted in France(Reference Shah, Mahamat-Saleh and Ait-Hadad42), Spain,(Reference Romanos-Nanclares, Toledo and Sanchez-Bayona43) and the USA(Reference Romanos-Nanclares, Willett and Rosner44) and three case–control studies conducted in Iran(Reference Payandeh, Shahinfar and Amini45–Reference Sasanfar, Toorang and Booyani47) investigated the associations of plant-based diet indices with breast cancer risk. Their findings generally suggested that following an overall plant-based diet, especially a healthful plant-based diet, is associated with a lower risk of breast cancer, whereas following an unhealthful plant-based diet is associated with a higher risk of breast cancer(Reference Shah, Mahamat-Saleh and Ait-Hadad42–Reference Sasanfar, Toorang and Booyani47). Only one study (also conducted in the Pathways Study) investigated the associations of plant-based diet indices with breast cancer prognosis(Reference Anyene, Ergas and Kwan23). PDI, hPDI, and uPDI were not associated with overall, recurrence-free, and breast-cancer-specific survival(Reference Anyene, Ergas and Kwan23). However, higher hPDI was associated with better non-breast-cancer-specific survival (hazard ratio [HR] 0·83; 95 % CI 0·71, 0·98), whereas higher uPDI was associated with worse non-breast-cancer-specific survival (HR 1·20; 95 % CI 1·02, 1·41)(Reference Anyene, Ergas and Kwan23). Given that there are limited studies examining a plant-based diet and breast cancer prognosis and the WCRF and AICR recommend a plant-based diet (especially a healthful plant-based diet) to cancer survivors(4,Reference Clinton, Giovannucci and Hursting5) , a pressing need exists to explore potential biological pathways through which a plant-based diet may impact breast cancer survival. Our findings may add greater confidence that the WCRF/AICR recommendations are appropriate and provide additional evidence in refining these recommendations to maximise the beneficial effects of dietary guidelines on these pathways, which will ultimately contribute to improving breast cancer prognosis.
Our findings provide some of the first evidence regarding associations of plant-based diet indices with inflammation biomarkers in women with breast cancer. While studies in cancer populations are few, five cross-sectional studies assessed such associations in healthy populations regarding hsCRP(Reference Baden, Satija and Hu48–Reference Wang, Page and Gill52), IL-1β(Reference Kharaty, Harrington and Millar49,Reference Pourreza, Khademi and Mirzababaei50) , IL-6,(Reference Baden, Satija and Hu48) and TNF-α(Reference Kharaty, Harrington and Millar49). Three relatively large studies were conducted in the USA (the National Health and Nutrition Examination Survey (n 27 915)(Reference Wang, Page and Gill52) and Nurses’ Health Study II (n 831)(Reference Baden, Satija and Hu48)) and Ireland (Ireland Mitchelstown Cohort (n 1986))(Reference Kharaty, Harrington and Millar49), whereas two smaller studies were conducted in Iran (n < 400)(Reference Pourreza, Khademi and Mirzababaei50,Reference Shahinfar, Amini and Payandeh51) . The three large studies reported that higher PDI (especially higher hPDI) was significantly associated with lower hsCRP, but the two smaller studies reported null associations(Reference Pourreza, Khademi and Mirzababaei50,Reference Shahinfar, Amini and Payandeh51) . For uPDI, findings were inconsistent across the five studies(Reference Baden, Satija and Hu48–Reference Wang, Page and Gill52). Regarding IL-1β(Reference Kharaty, Harrington and Millar49,Reference Pourreza, Khademi and Mirzababaei50) and IL-6(Reference Baden, Satija and Hu48), null associations were reported for three plant-based indices. Regarding TNF-α(Reference Kharaty, Harrington and Millar49), higher hPDI was significantly associated with lower TNF-α, whereas null associations were observed for PDI and uPDI. In line with these previous studies in non-cancer populations, we found that (1) higher PDI and hPDI were significantly associated with lower hsCRP and the magnitude was stronger for hPDI (–9·0 %) than PDI (–6·9 %); (2) higher uPDI was significantly associated with higher hsCRP; and (3) PDI, hPDI, and uPDI were not associated with other inflammation biomarkers. The differing impact of a plant–based diet on hsCRP and other inflammation biomarkers suggested the complexity of inflammation and its regulation(Reference Grivennikov, Greten and Karin53). One possible explanation may be that hsCRP is an acute-phase protein synthesised by hepatocytes and acts as a marker of systemic inflammation(Reference Cheng, Shi and Shields54), whereas other biomarkers are primarily inflammatory cytokines produced by immune cells and more indicative of inflammation associated with the tumours and tumour microenvironment(Reference Mantovani, Allavena and Sica55). Thus, following a plant-based diet may first reduce systemic inflammation and then gradually impact the inflammatory microenvironment by regulating cancer-related immune responses(Reference Eichelmann, Schwingshackl and Fedirko24). In all, our findings suggest that following a plant-based diet, especially a healthful plant-based diet, is associated with lower inflammation, whereas following an unhealthful plant-based diet is associated with higher inflammation. In addition, our study adds important data and findings of IL-4, IL-8, IL-10, and IL-13 that were not available before.
We also conducted one of the first investigations into the associations of plant-based diet indices with body composition in cancer patients. Only one study in Iran assessed these associations among 390 adult overweight/obese women using bioelectrical impedance analysis to approximate fat mass and fat-free mass and non-elastic tapes to assess waist circumference as a surrogate of visceral adiposity:(Reference Pourreza, Khademi and Mirzababaei50) null associations were reported between three plant-based diet indices and these body composition measurements. Utilising clinical CT scans to directly assess muscle and adipose tissue, we found that (1) higher PDI and hPDI were significantly associated with lower VAT and the magnitude was stronger for hPDI (–8·6 cm2) than PDI (–7·8 cm2); (2) higher uPDI was significantly associated with higher VAT; and (3) PDI, hPDI, and uPDI were not associated with muscle or SAT. Our findings suggest that following a plant-based diet, especially a healthful plant-based diet, is associated with lower visceral adiposity, whereas following an unhealthful plant-based diet is associated with higher visceral adiposity. In addition, our study adds important data and findings of muscle and SAT that were not available before.
Although vegetarian/vegan diet and Mediterranean diet are also considered ‘pro-plant’ diets, several differences should be noted. For example, a vegetarian/vegan diet typically emphasises abstaining from animal foods, which may be more challenging for patients to adopt(Reference Kwok, Umar and Myint56). The Mediterranean diet has been studied primarily for cardiovascular disease management and encourages moderate intake of alcohol(Reference Demarin, Lisak and Morović57), which has controversial roles in cancer prognosis and is discouraged by most nutrition guidelines for cancer survivors (including the WCRF/AICR guidelines)(4,Reference Kwan, Valice and Ergas41) . To our knowledge, no studies have looked into the associations of vegetarian/vegan diet with inflammation biomarkers and body composition among breast cancer survivors, and only one study assessed the Mediterranean diet and inflammation biomarkers (but no body composition measurements) using ceruloplasmin, haptoglobin and paraoxonase(Reference Negrati, Razza and Biasini58). These biomarkers may not be comparable to more classic inflammation biomarkers such as hsCRP, and this study reported null associations of Mediterranean diet with inflammation biomarkers(Reference Negrati, Razza and Biasini58).
Plant foods, especially healthful plant foods, are rich in chemical compounds with anti-inflammatory properties (such as carotenoids, vitamin C, vitamin E, flavonoids, and soluble fibre) and low in energy density(Reference Slavin and Lloyd59–Reference Cheng, Ou and Gatten61). By contrast, less healthful plant foods and animal foods typically have oxidative and pro-inflammatory constituents with high-energy density (such as saturated fatty acids, trans fatty acids, refined carbohydrates, and added sugar)(60,Reference Ley, Sun and Willett62–Reference Shah and Iyengar64) . A plant-based diet, especially a healthful plant-based diet, also has a lower glycaemic index and promotes favourable gut microbiome diversity that may reduce visceral lipogenesis and fat accumulation, whereas an unhealthful plant-based diet may exert the opposite impact(Reference Ratjen, Morze and Enderle25,Reference Le Roy, Bowyer and Castillo-Fernandez65–Reference Medawar, Huhn and Villringer67) . In line with the above biological pathways, we found that following an overall or healthful plant-based dietary pattern may reduce inflammation and visceral adiposity, whereas following an unhealthful plant-based dietary pattern may increase inflammation and visceral adiposity.
Limitations
This study has several limitations. First, although participants’ dietary intake was repeatedly collected after baseline in the Pathways Study, repeated measurements of inflammation and adiposity were not available. Thus, this cross-sectional study focused on the analysis of plant-based diet, inflammation, and adiposity proximal to breast cancer diagnosis. Future studies with repeated measurements are needed to confirm causal inferences regarding the longitudinal effects of plant-based dietary patterns on inflammation and body composition during the survivorship period. However, our study is the first to assess such associations among breast cancer survivors and can inform the potential mechanisms through which plant-based dietary patterns may impact breast cancer prognosis. Second, clinical CT scans are not the standard of care for stage I breast cancer and thus were only available for a subset of patients with breast cancer. However, our prior study suggested no differences in demographic or diagnostic characteristics between patients with v. without CT by each cancer stage(Reference Caan, Cespedes Feliciano and Prado12), which supported the generalizability of our findings.
Conclusions
Among breast cancer survivors, our findings suggest that following an overall plant-based diet, especially a healthful plant-based diet, may reduce inflammation and visceral adiposity, whereas following an unhealthful plant-based diet may increase inflammation and visceral adiposity. Future prospective studies with repeated measures in dietary patterns, inflammatory cytokines, and body composition among patients followed for breast cancer outcomes will inform the prognostic significance of these mechanistic findings.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114525000856.
Acknowledgements
This study was supported in part by a grant from the American Institute for Cancer Research and grants from the National Institutes of Health (R01CA251589, R01CA166701, R01CA105274, R50CA211108, P30CA016056, U01CA195565 and R01CA241409), a Community Health grant from The Permanente Medical Group Central Research Committee and start-up funding from Montefiore Einstein Comprehensive Cancer Center and Albert Einstein College of Medicine. The funders had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript; and decision to submit the manuscript for publication.
Author contributions are listed as the following: E. C. (Conceptualisation; Data curation; Formal analysis; Investigation; Methodology; Project administration; Resources; Software; Supervision; Validation; Visualisation; Writing – original draft; Writing – review and editing; Funding acquisition), C.-C. H. (Data curation; Formal analysis; Methodology; Writing – review and editing; Funding acquisition), I. J. E. (Data curation; Formal analysis; Methodology; Writing – review and editing), B. J. C. (Data curation; Methodology; Resources; Writing – review and editing; Funding acquisition), M. L. K. (Data curation; Resources; Writing – review and editing; Funding acquisition), J. M. R. (Data curation; Project administration; Resources; Writing – review and editing), T.-Y. D. C. (Writing – review and editing), N. J. S. (Data curation; Methodology; Writing – review and editing), J. R. H. (Data curation; Methodology; Writing – review and editing), H. M. (Data curation; Methodology; Writing – review and editing), H. S. (Writing – review and editing), S. Y. (Resources; Writing – review and editing; Funding acquisition), N. M. I. (Resources; Writing – review and editing; Funding acquisition), C. B. A. (Data curation; Resources; Writing – review and editing; Funding acquisition), L. H. K. (Conceptualisation; Data curation; Investigation; Methodology; Project administration; Resources; Supervision; Validation; Writing – review and editing; Funding acquisition), E. M. C. F. (Conceptualisation; Data curation; Investigation; Methodology; Project administration; Resources; Supervision; Validation; Writing – review and editing; Funding acquisition).
The authors have no conflicts of interest to disclose.