


Introduction
Disorganized attachment has enduring consequences for children’s socioemotional health (Cooke et al., Reference Cooke, Kochendorfer, Stuart-Parrigon, Koehn and Kerns2019; Fearon et al., Reference Fearon, Bakermans-Kranenburg, Van Ijzendoorn, Lapsley and Roisman2010; Madigan et al., Reference Madigan, Brumariu, Villani, Atkinson and Lyons-Ruth2016), including externalizing problems (Fearon et al., Reference Fearon, Bakermans-Kranenburg, Van Ijzendoorn, Lapsley and Roisman2010; Madigan et al., Reference Madigan, Brumariu, Villani, Atkinson and Lyons-Ruth2016), borderline symptoms, dissociation, and suicidality into adulthood (Carlson, Reference Carlson1998; Lyons-Ruth et al., Reference Lyons-Ruth, Bureau, Holmes, Easterbrooks and Brooks2013; Obsuth et al., Reference Obsuth, Hennighausen, Brumariu and Lyons-Ruth2014). While numerous interventions address disorganized attachment once it has emerged (Bakermans-Kranenburg et al., Reference Bakermans-Kranenburg, Van Ijzendoorn and Juffer2005; Facompré et al., Reference Facompré, Bernard and Waters2018), the continued prevalence of disorganized attachment in one in four children in the general population (Madigan, Fearon, et al., Reference Madigan, Fearon, van Ijzendoorn, Duschinsky, Schuengel, Bakermans-Kranenburg, Ly, Cooke, Deneault, Oosterman and Verhage2023) necessitates identifying early antecedents to help prevent its onset. Disrupted caregiving (e.g., frightening or intrusive behaviors) is the strongest predictor of disorganized attachment, but only explains approximately 10% of its variance (Goldberg et al., Reference Goldberg, Benoit, Blokland and Madigan2003; Madigan et al., Reference Madigan, Bakermans-Kranenburg, Van Ijzendoorn, Moran, Pederson and Benoit2006). Thus, additional contributing risk factors must be considered.
A recent meta-analysis found disorganized attachment is more common in samples with low socioeconomic status (31%) and caregiver psychopathology (31%), compared to samples with higher socioeconomic status (21%) or without psychopathology (23%; Madigan et al., Reference Madigan, Fearon, van Ijzendoorn, Duschinsky, Schuengel, Bakermans-Kranenburg, Ly, Cooke, Deneault, Oosterman and Verhage2023). A systematic review of longitudinal determinants (McIntosh et al., Reference McIntosh, Schnabel, Youssef and Olsson2021) identified two studies linking sociodemographic factors to attachment disorganization (Fish, Reference Fish2001; Goodman et al., Reference Goodman, Hans and Cox1999). However, other risk factors that may amplify disrupted caregiving and tend to co-occur with sociodemographic risks (e.g., caregiver psychopathology) were rarely investigated (McIntosh et al., Reference McIntosh, Schnabel, Youssef and Olsson2021). Moreover, studies have seldom tested whether potential risk factors interact with one other to influence the development of attachment disorganization (McIntosh et al., Reference McIntosh, Schnabel, Youssef and Olsson2021). To advance the understanding of how attachment disorganization develops, the current study investigated the main and moderating longitudinal effects of maternal disrupted caregiving, depression, psychopathology (i.e., substance use, posttraumatic stress, and psychosis), maternal history of childhood maltreatment (HCM), and sociodemographic risk on infant attachment disorganization in a Canadian pregnancy cohort.
Attachment theory and disorganization
According to attachment theory (Bowlby, Reference Bowlby1982), infants adaptively acquire safety and comfort from their caregivers through proximity seeking and contact maintenance. In turn, caregivers act as secure bases and safe havens by signaling safety, offering protection, and providing comfort during distress (Ainsworth et al., Reference Ainsworth, Blehar, Waters and Wall1978). Predictable interactions with caregivers allow most infants to develop organized behavioral strategies that evoke coregulation from their caregivers. These strategies are elicited and observed using the Strange Situation Procedure (SSP), where secure, avoidant, and ambivalent attachment are reliably identified (Ainsworth et al., Reference Ainsworth, Blehar, Waters and Wall1978). However, some infants display “disorganized” attachment behaviors around their caregivers, including conflicted, fearful, or disoriented behaviors (e.g., freeze, approach, and then avoidance of caregiver). These behaviors reflect a lack of organized strategies available to secure safety and comfort from caregivers (Main & Solomon, Reference Main and Solomon1986, Reference Main and Solomon1990). Whether measured categorically (i.e., classification as disorganized versus organized) or continuously (i.e., scores ranging from low to high levels of disorganization), meta-analytic research has shown disorganized attachment is linked with internalizing problems (d = 0.47; Madigan et al., Reference Madigan, Brumariu, Villani, Atkinson and Lyons-Ruth2016), externalizing problems (d = 0.34 to 0.58; Fearon et al., Reference Fearon, Bakermans-Kranenburg, Van Ijzendoorn, Lapsley and Roisman2010; Madigan et al., Reference Madigan, Brumariu, Villani, Atkinson and Lyons-Ruth2016), greater negative affect (d = 0.61; Cooke et al., Reference Cooke, Kochendorfer, Stuart-Parrigon, Koehn and Kerns2019), and reduced positive affect (d = −0.28; Cooke et al., Reference Cooke, Kochendorfer, Stuart-Parrigon, Koehn and Kerns2019) in childhood.
The etiology of attachment disorganization
Many theories on the etiology of attachment disorganization stem from the hypothesis that attachment experiences are transmitted intergenerationally through caregiving behaviors (Verhage et al., Reference Verhage, Schuengel, Madigan, Fearon, Oosterman, Cassibba, Bakermans-Kranenburg and van2016). Main and Hesse (Reference Main and Hesse1990) suggested caregivers who re-experience attachment-related fear or dissociation might display frightening (e.g., verbal aggression) or frightened (e.g., hypervigilance, dissociation) behaviors in caregiving contexts. These behaviors may induce fear in infants, with frightening behaviors signaling threat, and frightened behaviors signaling caregiver unavailability to attend to infant needs (Hesse & Main, Reference Hesse and Main2000). Infants in these situations have been hypothesized to face “paradoxical situations” because their caregivers serve as sources of fear, but also as the primary sources of safety and coregulation (Main & Hesse, Reference Main and Hesse1990). Consequently, these infants may experience “fright without solution” and momentarily engage in the contradictory behaviors characteristic of disorganized attachment (Hesse & Main, Reference Hesse and Main2000; Main & Hesse, Reference Main and Hesse1990).
Lyons-Ruth et al. (Reference Lyons-Ruth, Bronfman and Parsons1999) proposed infants also encounter fear-eliciting stimuli outside of caregiving behaviors that warrant adequate and appropriate caregiving responses to modulate fear arousal. When caregiving responses are inadequate, infants may again lack means to coregulate their arousal, resulting in disorganized behaviors (Lyons-Ruth et al., Reference Lyons-Ruth, Bronfman and Parsons1999). From this perspective, these disrupted caregiving behaviors can encompass affective communication errors (e.g., failing to soothe or recognize distress), role boundary confusion (e.g., prioritizing caregiver needs over the child’s), and withdrawal (e.g., holding the child out with stiff arms), as well as fearful and disoriented behaviors (e.g., apprehension related to the child) and negative-intrusive behaviors (e.g., mocking the child) previously operationalized in Main and Hesse’s measure of frightened and frightening behavior (Lyons-Ruth et al., Reference Lyons-Ruth, Bronfman and Parsons1999). This broader conceptualization of disrupted caregiving was operationalized in the Atypical Maternal Behavior Instrument for Assessment and Classification (AMBIANCE; Bronfman et al., Reference Bronfman, Madigan and Lyons-Ruth2009-2014), which has now been implemented to investigate maternal disrupted caregiving across a myriad of studies.
Empirically, maternal disrupted caregiving has demonstrated consistent associations with attachment disorganization (Madigan et al., Reference Madigan, Bakermans-Kranenburg, Van Ijzendoorn, Moran, Pederson and Benoit2006) and child psychopathology (e.g., Lyons-Ruth et al., Reference Lyons-Ruth, Bureau, Holmes, Easterbrooks and Brooks2013). It also mediates the relation between maternal unresolved attachment (i.e., an adult attachment representation reflecting unresolved emotional difficulties when discussing past attachment-related traumas or losses) and infant attachment disorganization (Madigan et al., Reference Madigan, Bakermans-Kranenburg, Van Ijzendoorn, Moran, Pederson and Benoit2006). Moreover, decreases in disrupted caregiving have accounted for reductions in disorganized attachment in randomized controlled trials (Tereno et al., Reference Tereno, Madigan, Lyons-Ruth, Plamondon, Atkinson, Guedeney, Greacen, Dugravier, Saias and Guedeney2017; Yarger et al., Reference Yarger, Bronfman, Carlson and Dozier2020). Thus, disrupted caregiving is critical for understanding and addressing the complexities of parent–child attachment and intergenerational transmission processes.
Disrupted caregiving is a well-established antecedent of disorganized attachment, yet correlational studies find it only accounts for 10% of its variance (Madigan et al., Reference Madigan, Bakermans-Kranenburg, Van Ijzendoorn, Moran, Pederson and Benoit2006, Reference Madigan, Voci and Benoit2011). Other caregiving constructs, including maternal unresolved attachment representations (1%) and insensitivity (4%), explain even less of its variance in meta-analyses (Van Ijzendoorn et al., Reference Van Ijzendoorn, Schuengel and Bakermans–Kranenburg1999; Verhage et al., Reference Verhage, Schuengel, Madigan, Fearon, Oosterman, Cassibba, Bakermans-Kranenburg and van2016). To isolate caregiving processes uniquely implicated in attachment disorganization, it is therefore important to distinguish disrupted caregiving from maternal sensitivity. Although these constructs share conceptual overlap and are moderately correlated in meta-analyses (Van Ijzendoorn et al., Reference Van Ijzendoorn, Schuengel and Bakermans–Kranenburg1999; Verhage et al., Reference Verhage, Schuengel, Madigan, Fearon, Oosterman, Cassibba, Bakermans-Kranenburg and van2016), they are not interchangeable, as reflected in the comparatively weaker and more inconsistent associations between sensitivity and attachment disorganization (Madigan et al., Reference Madigan, Bakermans-Kranenburg, Van Ijzendoorn, Moran, Pederson and Benoit2006; Madigan et al., Reference Madigan, Fearon, van Ijzendoorn, Duschinsky, Schuengel, Bakermans-Kranenburg, Ly, Cooke, Deneault, Oosterman and Verhage2023; Van Ijzendoorn et al., Reference Van Ijzendoorn, Schuengel and Bakermans–Kranenburg1999).
Without accounting for maternal sensitivity, it is difficult to determine whether associations attributed to disrupted caregiving reflect its unique features (e.g., frightened or dissociative behaviors) or normative variations in caregiving sensitivity. Meta-analyses have shown attachment disorganization is substantially higher in child maltreatment samples (65%; Madigan et al., Reference Madigan, Fearon, van Ijzendoorn, Duschinsky, Schuengel, Bakermans-Kranenburg, Ly, Cooke, Deneault, Oosterman and Verhage2023), yet also emerges in the absence of maltreatment, potentially through less severe but still disrupted forms of caregiving (Cyr et al., Reference Cyr, Euser, Bakermans-Kranenburg and Van Ijzendoorn2010). Together, these findings highlight the need to distinguish disrupted caregiving from both sensitivity and other sources of sociodemographic or psychosocial risk when examining developmental pathways to attachment disorganization. Accordingly, maternal sensitivity was included as a covariate to isolate the unique contribution of disrupted caregiving to attachment disorganization.
A broader lens for understanding the development of attachment disorganization
To account for variance in disorganized attachment not explained by caregiving, Bernier and Meins (Reference Bernier and Meins2008) proposed a threshold model for understanding its development. This model suggests children’s vulnerability for disorganized attachment depends on the presence or absence of child characteristics (e.g., genetic alleles, temperamental characteristics), sociodemographic risks (e.g., low family income, caregiver education), and caregiving-related factors (e.g., psychopathology, HCM). Any of these factors may either lower children’s threshold for developing disorganized attachment or amplify caregiver risk of engaging in disrupted caregiving. From this theoretical perspective, caregiver HCM, psychopathology symptoms, or sociodemographic factors may directly contribute to disorganized attachment, potentially by altering children’s stress physiology or behavioral regulation, or indirectly increase the propensity for disrupted caregiving by increasing caregiver stress and arousal.
Although Bernier and Meins did not explicitly differentiate between prenatal and postnatal exposures, risk factors occurring during either period could influence the threshold for developing disorganized attachment by affecting children’s neurobiological development (e.g., brain regions involved in stress response) or by shaping their environment (e.g., caregiving behaviors through alterations in caregiver stress). In this study, sociodemographic risk and maternal psychopathology (i.e., substance use, posttraumatic stress, and psychosis), depression, and HCM were explored as antecedents of infant attachment disorganization, particularly in the context of maternal disrupted caregiving. Hereafter, caregivers are referred to as “mothers” because other caregivers were not included in the sample.
Maternal depression
Multiple mechanisms may link maternal depression to attachment disorganization (Barnes & Theule, Reference Barnes and Theule2019). Depression may increase the risk for attachment disorganization through its association with caregiver behavior. Observational studies have shown mothers with depression display less responsivity and reciprocity, more withdrawal and intrusiveness, and greater negative affect with their infants (Flowers et al., Reference Flowers, McGillivray, Galbally and Lewis2018; Wan & Green, Reference Wan and Green2009). Prenatal depression may also convey risk for attachment disorganization through the prenatal programming of stress, potentially through effects on fetal brain development or exposure to HPA axis dysregulation in pregnancy (Davis et al., Reference Davis, Hankin, Swales and Hoffman2018). Consequently, there may be a main effect of maternal depression on infant attachment disorganization.
However, reviews of maternal depression and attachment have yielded mixed results based on symptom severity and measurement timing. In a meta-analysis, Martins and Gaffan (Reference Martins and Gaffan2000) reported a greater proportion of infant disorganized attachment in clinical (28%) versus nonclinical samples (17%). In another meta-analysis, maternal depressive symptoms correlated with preschool attachment disorganization (r = 0.13), with stronger effects in clinical samples (Badovinac et al., Reference Badovinac, Martin, Guérin-Marion, O’Neill, Pillai Riddell, Bureau, Spiegel and Tachibana2018). A review of perinatal longitudinal risk factors found maternal depression was only a significant antecedent in clinical samples, with no differences for prenatal versus postnatal depression (McIntosh et al., Reference McIntosh, Schnabel, Youssef and Olsson2021). Notably, only four samples were available for inclusion in McIntosh et al.’s review, and three samples were high-risk (e.g., history of major depressive disorder, low income). Therefore, maternal depression’s effect on attachment disorganization may vary by timing or co-occurring contextual stressors (e.g., comorbidity, low income) common in clinical samples. Examining these associations in low-risk samples is important to clarify whether maternal depression alone contributes to attachment disorganization, or whether its impact is contingent on broader environmental adversities.
Although research on maternal depression and parenting is extensive (Bernard et al., Reference Bernard, Nissim, Vaccaro, Harris and Lindhiem2018; Borairi et al., Reference Borairi, Deneault, Madigan, Fearon, Devereux, Geer, Jeyanayagam, Martini and Jenkins2024; Letourneau et al., Reference Letourneau, Dennis, Cosic and Linder2017), its relation to disrupted caregiving requires further investigation. A study of 51 mother–infant dyads by Khoury et al. (Reference Khoury, Bosquet Enlow, Patwa and Lyons-Ruth2020) found postpartum, but not prenatal, depression interacted with mothers’ hair cortisol concentration to predict disrupted caregiving at four months postpartum. Mothers with higher postpartum depressive symptoms and higher cortisol levels in pregnancy exhibited more withdrawal at four months postpartum. In contrast, mothers with lower postpartum depressive symptoms and higher cortisol levels showed comparatively less withdrawal. Therefore, the relation between maternal depression and disrupted caregiving may be nuanced and extend to broader developmental outcomes for offspring (Borairi et al., 2024). The current study sought to examine both the main and interactive effects of prenatal and postnatal depression on infant attachment disorganization.
Maternal psychopathology
Maternal substance use, psychosis, and posttraumatic stress have been proposed to directly contribute to the development of attachment disorganization through unique and shared mechanisms. Regarding substance use, Hyysalo et al. (Reference Hyysalo, Gastelle and Flykt2022) hypothesized infants may be at greater risk for disorganized attachment due to the teratogenic effects of prenatal substance use on infant emotion regulation and soothability, caregiving difficulties (e.g., lower responsiveness to infant cues, greater hostility during caregiving), and cumulative adversities that often co-occur with substance use (e.g., lower income, low social support). Hyysalo et al. (Reference Hyysalo, Gastelle and Flykt2022) did not find support for the association between maternal substance use and attachment disorganization in a meta-analysis of seven studies, but noted significant, unexplained heterogeneity and that six of the included studies reported positive associations with disorganization. This heterogeneity may suggest the association between maternal substance use and attachment disorganization is moderated by other risk factors (e.g., socioeconomic inequities) that vary across studies.
Regarding maternal psychosis, Wan and Green (Reference Wan and Green2009) proposed infants may be more vulnerable to disorganized attachment given the consequences of psychosis on caregiving (e.g., interactional deficits, lack of insight about symptom impact on caregiving) and genetic vulnerability to abnormal neonatal behavior. Flowers et al. (Reference Flowers, McGillivray, Galbally and Lewis2018) hypothesized mothers with psychotic disorders may engage in more frightening or frightened behaviors, withdrawal, and affective communication errors (e.g., blunted affect), thereby increasing the likelihood of attachment disorganization. In both reviews, few studies examined the relation between maternal psychosis and attachment disorganization. The studies were also limited by small sample sizes and comorbid mental health problems (e.g., psychotic disorder and depressive disorder). Consequently, it is critical to explore both the main effect of maternal psychosis and potential moderating influences on attachment disorganization.
Finally, maternal posttraumatic stress may be associated with infant attachment disorganization both directly and in interaction with other risk factors. Prior research links maternal posttraumatic stress symptoms to offspring disorganized attachment (Bosquet Enlow et al., Reference Bosquet Enlow, Egeland, Carlson, Blood and Wright2014; Van Ee et al., Reference Van Ee, Kleber, Jongmans, Mooren and Out2016), suggesting a potential main effect. In addition, posttraumatic stress may exacerbate the impact of caregiving disruptions on attachment, particularly when mothers display dissociation, avoidance, or emotional reactivity to normative infant behaviors (Bosquet Enlow et al., Reference Bosquet Enlow, Egeland, Carlson, Blood and Wright2014; Van Ee et al., Reference Van Ee, Kleber, Jongmans, Mooren and Out2016). Although anomalous caregiving behaviors are often studied as mediators, evidence for mediation remains inconsistent (Van Ee et al., Reference Van Ee, Kleber, Jongmans, Mooren and Out2016), suggesting posttraumatic stress may instead interact with caregiving behavior to increase risk for attachment disorganization.
Maternal history of childhood maltreatment (HCM)
Although mechanisms linking maternal HCM to attachment disorganization are similar to those hypothesized for posttraumatic stress, the strength of these associations may vary by the type and timing of trauma. In a meta-analysis, the prevalence of disorganized attachment did not significantly vary with the presence of maternal HCM (38% with HCM, 21% without HCM; Madigan et al., Reference Madigan, Fearon, van Ijzendoorn, Duschinsky, Schuengel, Bakermans-Kranenburg, Ly, Cooke, Deneault, Oosterman and Verhage2023). However, the sizeable difference in prevalence between groups suggests there may be variability across studies. The authors noted subjective and objective measures of maltreatment may differ in their predictive abilities. Specifically, subjective self-report measures might demonstrate stronger associations with disorganized attachment because they reflect the emotional and psychological impacts of maltreatment on present thoughts, emotions, and behaviors.
Consistent with this hypothesis, studies using self-report measures of maternal HCM report a higher proportion of infant disorganized attachment (44%; Berthelot et al., Reference Berthelot, Ensink, Bernazzani, Normandin, Luyten and Fonagy2015). Ludmer et al. (Reference Ludmer, Gonzalez, Kennedy, Masellis, Meinz and Atkinson2018) also found self-reported HCM significantly predicted next generation attachment disorganization, with stronger associations among mothers with more plasticity alleles of the OXTR receptor gene (rs53576; linked to greater environmental sensitivity) and higher cortisol output during the SSP. These findings suggest genetic and physiological factors may moderate the association between maternal HCM and infant disorganization, highlighting complex nuances among these variables.
Alto et al. (Reference Alto, Warmingham, Handley, Rogosch, Cicchetti and Toth2021) further supported the link between maternal HCM and infant attachment disorganization via maternal depression and maternal sensitivity. While maternal HCM may directly contribute to attachment disorganization, its impact may also be moderated by disrupted caregiving behaviors. Indeed, recent studies have suggested maternal HCM increases the risk of disrupted caregiving (Guyon-Harris et al., Reference Guyon-Harris, Madigan, Bronfman, Romero and Huth-Bocks2021; Khoury et al., Reference Khoury, Dimitrov, Enlow, Haltigan, Bronfman and Lyons-Ruth2021), suggesting mothers with HCM may be more vulnerable to caregiving difficulties implicated in the development of attachment disorganization.
Sociodemographic risk
Theoretical and empirical work have positioned cumulative sociodemographic risk (e.g., low income, low parent education, minoritized race/ethnicity) as a contextual risk factor for attachment disorganization (e.g., Cyr et al., Reference Cyr, Euser, Bakermans-Kranenburg and Van Ijzendoorn2010; Madigan et al., Reference Madigan, Fearon, van Ijzendoorn, Duschinsky, Schuengel, Bakermans-Kranenburg, Ly, Cooke, Deneault, Oosterman and Verhage2023). For example, low family income and maternal education may increase the risk of attachment disorganization through associations with elevated caregiver stress and potential caregiving impacts. These stressors may limit time, knowledge of, and access to resources that enhance the caregiving environment (e.g., parenting books, therapeutic supports) and co-occur with low social supports (Ayoub & Bachir, Reference Ayoub and Bachir2023). In turn, these conditions may increase the likelihood of engaging in disrupted caregiving (e.g., Lyons-Ruth et al., Reference Lyons-Ruth, Bronfman and Parsons1999; Roubinov & Boyce, Reference Roubinov and Boyce2017). In meta-analyses, low socioeconomic status and cumulative socioeconomic risks, typically inclusive of low income and low parent education, have been associated with higher rates of disorganization (Cyr et al., Reference Cyr, Euser, Bakermans-Kranenburg and Van Ijzendoorn2010; Madigan et al., Reference Madigan, Fearon, van Ijzendoorn, Duschinsky, Schuengel, Bakermans-Kranenburg, Ly, Cooke, Deneault, Oosterman and Verhage2023). Furthermore, Gedaly and Leerkes (Reference Gedaly and Leerkes2016) found maternal insensitivity was associated with attachment disorganization when sociodemographic risk was high, but not low, suggesting broader contextual adversity may heighten children’s vulnerability to caregiving disruptions.
Although low maternal education and family income have historically been examined in sociodemographic risk composites in relation to attachment disorganization (Madigan et al., Reference Madigan, Fearon, van Ijzendoorn, Duschinsky, Schuengel, Bakermans-Kranenburg, Ly, Cooke, Deneault, Oosterman and Verhage2023), minoritized race/ethnicity represents a critical dimension of structural disadvantage known to intersect with other sociodemographic disadvantages (Alegría et al., Reference Alegría, NeMoyer, Falgàs Bagué, Wang and Alvarez2018; Ayoub & Bachir, Reference Ayoub and Bachir2023; Berry et al., Reference Berry, Londoño Tobón and Njoroge2021) and explain disparities in child development (Alegría et al., Reference Alegría, NeMoyer, Falgàs Bagué, Wang and Alvarez2018; Ayoub & Bachir, Reference Ayoub and Bachir2023; Berry et al., Reference Berry, Londoño Tobón and Njoroge2021). Critically, minoritized race/ethnicity is not an inherent risk factor for attachment disorganization, nor disrupted caregiving. Rather, differences in caregiving found between minoritized and non-minoritized groups may be attributable to socioeconomic discrepancies (e.g., employment, income) resulting from discrimination (Madigan et al., Reference Madigan, Fearon, van Ijzendoorn, Duschinsky, Schuengel, Bakermans-Kranenburg, Ly, Cooke, Deneault, Oosterman and Verhage2023) or from the impacts of discrimination on stress processes within the mother–child relationship (Berry et al., Reference Berry, Londoño Tobón and Njoroge2021). For example, maternal experiences of racism may directly shape the development of attachment and socioemotional difficulties in offspring through the fetal programming of prenatal stress and allostatic load and inflammation in pregnancy (Berry et al., Reference Berry, Londoño Tobón and Njoroge2021).
In a previous meta-analysis, Cyr et al. (Reference Cyr, Euser, Bakermans-Kranenburg and Van Ijzendoorn2010) found the prevalence of disorganized attachment was higher among minoritized groups, compared to non-minoritized groups. The authors attributed these findings to the persistence of cooccurring sociodemographic risks (e.g., housing instability) that are more common in minoritized groups, as cooccurring risks in non-minoritized groups tend to be more transitory in nature. However, Gedaly and Leerkes (Reference Gedaly and Leerkes2016) did not identify a main effect of race, nor an interaction with parenting, on attachment disorganization when examined as a unique risk factor in a community sample from the United States. Thus, attachment disorganization may be better explained by the accumulation of sociodemographic risks rather than any single factor alone. Studies have shown maternal discrimination contributes to increased distress and harsh or intrusive caregiving (Berry et al., Reference Berry, Londoño Tobón and Njoroge2021), which may amplify the likelihood of engaging in disrupted caregiving. Consequently, cumulative sociodemographic risk and disrupted caregiving may interact to create a heightened risk environment for the development of attachment disorganization.
The current study
This study examined which longitudinal risk factors across prenatal and postnatal periods predicted infant attachment disorganization in the context of observed maternal disrupted caregiving. Given the low prevalence of disorganized attachment (n = 32, 14.1%) in the sample, and to enhance predictive power, attachment disorganization was investigated continuously, rather than categorically. It was hypothesized that: (1) disrupted caregiving would demonstrate the strongest association with attachment disorganization among the hypothesized antecedents; and (2) sociodemographic risk, maternal depression, psychopathology (i.e., substance use, psychosis, and posttraumatic stress), and HCM would demonstrate significant, albeit weaker, main effects on attachment disorganization while controlling for disrupted caregiving. Due to limited research on differences in the timing of maternal mental health’s impact on attachment disorganization, no hypotheses were made regarding the roles of prenatal versus postnatal depression and psychopathology.
Given that the hypothesized antecedents may moderate the impact of disrupted caregiving on attachment disorganization (Gedaly & Leerkes, Reference Gedaly and Leerkes2016; Guyon-Harris et al., Reference Guyon-Harris, Madigan, Bronfman, Romero and Huth-Bocks2021; Khoury et al., Reference Khoury, Bosquet Enlow, Patwa and Lyons-Ruth2020, Reference Khoury, Dimitrov, Enlow, Haltigan, Bronfman and Lyons-Ruth2021), theoretically guided interactions among candidate predictors of attachment disorganization that align with developmental models emphasizing cumulative and conditional risk processes (Rutter & Sroufe, Reference Rutter and Sroufe2000) were explored. Specifically, interactions were probed where sociodemographic or psychosocial risks would be expected to strengthen or attenuate the association between disrupted caregiving and attachment disorganization. This focus reflects theoretical accounts in which risk operates by exacerbating or buffering caregiving effects, rather than producing crossover or contrastive (X-shaped) interactions that involve reversals in effect direction, lack grounding in attachment theory, and are more likely to reflect sample-specific type I artifacts. The aim was therefore to examine theoretically meaningful conditional processes rather than all mathematically possible interaction forms. No a priori hypotheses were made regarding potential interactions between disrupted caregiving and the other hypothesized antecedents.
Method
Study design
The Alberta Pregnancy Outcomes and Nutrition (APrON) study is a prospective longitudinal pregnancy cohort of 2,189 mothers and their offspring enrolled during pregnancy from central and southern regions of Alberta, Canada (see Kaplan et al., Reference Kaplan, Giesbrecht, Leung, Field, Dewey, Bell, Manca, O’Beirne, Johnston, Pop, Singhal, Gagnon, Bernier, Eliasziw, McCargar, Kooistra, Farmer, Cantell and Goonewardene2014 for a review of the study rationale and methodology). The secondary analyses in this study involved a subsample of participants from the APrON study, called the Fetal Programming (FetalPro) study. The subsample was collected to investigate maternal perinatal stress biomarkers and their impact on the maternal-child relationship and child neurodevelopmental outcomes. Families who agreed to participate in additional data collection were included in the subsample. Study approval was obtained from the University of Calgary Conjoint Health Research Ethics Board (ID # REB14-1702 and 22720) and the University of Alberta Health Research Ethics Biomedical Panel (ID # Pro00002954).
Participants
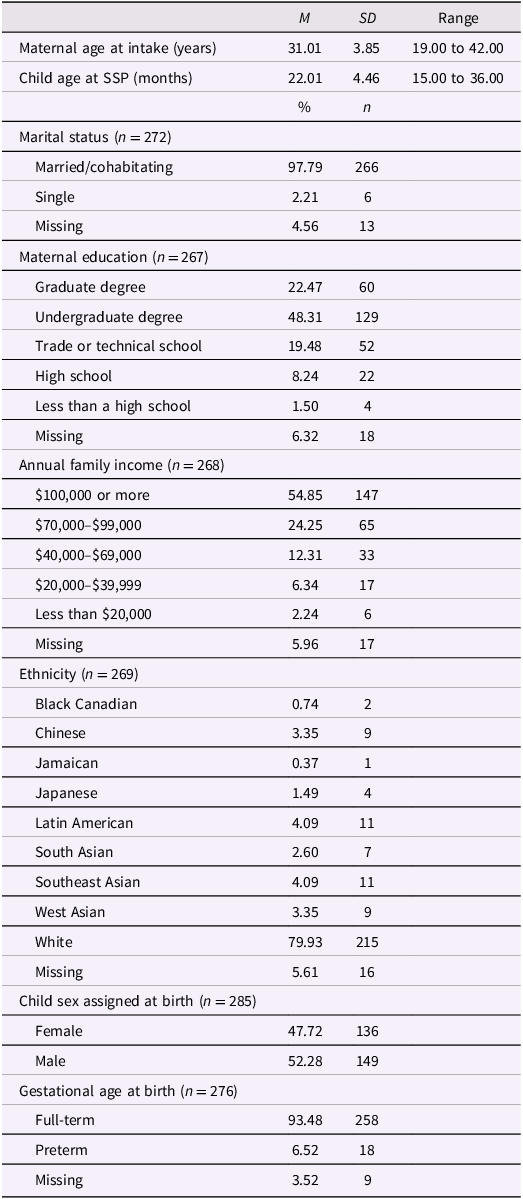
Pregnant mothers were recruited between 2010 and 2012 from maternity, ultrasound, family medicine, and obstetrics clinics in Calgary, Alberta. Mothers provided informed consent prior to participation. Participants were included if they: (a) had a singleton pregnancy, (b) were less than 22 weeks of gestation at the first study visit, and (c) were 18 years of age or older. Participants were excluded if they reported: (a) steroid medication use, (b) smoking, (c) substance use during pregnancy, or (d) known pregnancy or fetal complications (e.g., genetic abnormalities). Additional recruitment and retention details have been reported elsewhere (Kaplan et al., Reference Kaplan, Giesbrecht, Leung, Field, Dewey, Bell, Manca, O’Beirne, Johnston, Pop, Singhal, Gagnon, Bernier, Eliasziw, McCargar, Kooistra, Farmer, Cantell and Goonewardene2014; Letourneau et al., Reference Letourneau, Aghajafari, Bell, Deane, Dewey, Field, Giesbrecht, Kaplan, Leung and Ntanda2022). Participating mothers were older, reported higher family incomes and education levels, and were more frequently married compared with mothers in Alberta and across Canada, while their nationality was similar (Letourneau et al., Reference Letourneau, Aghajafari, Bell, Deane, Dewey, Field, Giesbrecht, Kaplan, Leung and Ntanda2022). Sample characteristics are provided in Table 1.
Sample characteristics (N = 285)
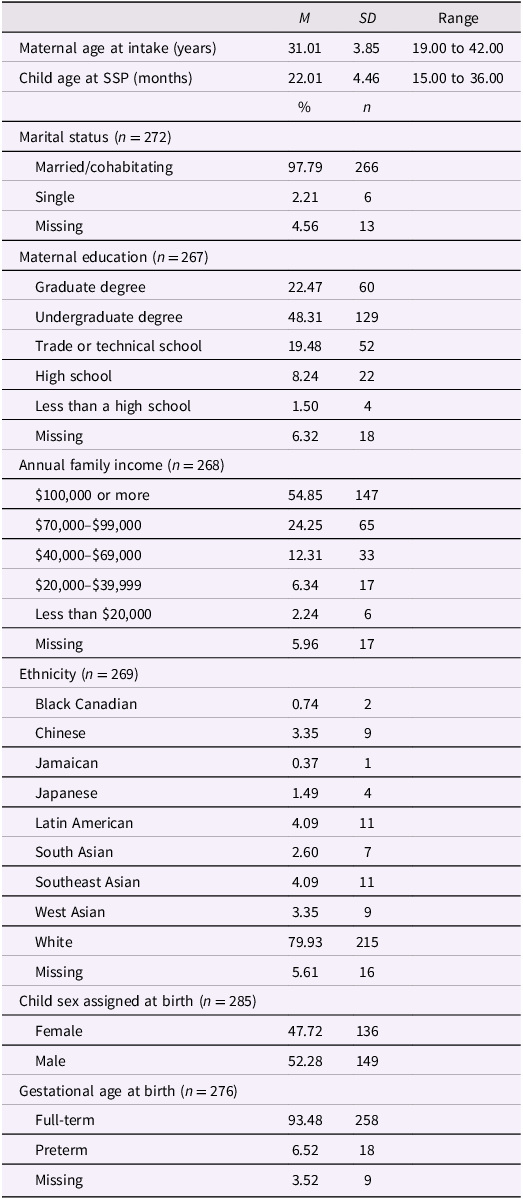
Table 1 Long description
The table presents sample characteristics of 285 participants. It includes 13 rows and 5 columns. The columns are labeled M, SD, Range, and % and n. The rows are labeled with various characteristics such as Maternal age at intake, Child age at SSP, Marital status, Maternal education, Annual family income, Ethnicity, Child sex assigned at birth, and Gestational age at birth. Each row provides specific data points for these characteristics. For example, Maternal age at intake has a mean of 31.01 years, a standard deviation of 3.85, and a range from 19.00 to 42.00 years. Child age at SSP has a mean of 22.01 months, a standard deviation of 4.46, and a range from 15.00 to 36.00 months. Marital status includes categories like Married/cohabitating, Single, and Missing, with respective percentages and counts. Maternal education levels range from Graduate degree to Less than a high school, with corresponding percentages and counts. Annual family income categories include $100,000 or more, $70,000-$99,000, and so on, with respective percentages and counts. Ethnicity includes categories like Black Canadian, Chinese, Jamaican, and others, with respective percentages and counts. Child sex assigned at birth includes Female and Male, with respective percentages and counts. Gestational age at birth includes Full-term and Preterm, with respective percentages and counts.
Note. Missing data resulted when the birth record could not be obtained, or birth outcomes were not reported.
Procedures
During pregnancy, mothers reported their age, education, family income, and obstetric history. Mothers rated their symptoms of depression on the Edinburgh Perinatal/Postnatal Depression Scale (EPDS) and substance use, psychosis, and posttraumatic stress on the Psychiatric Diagnostic Screening Questionnaire (PDSQ) in their third trimester (27–42 weeks of gestation) and at three months postpartum. Mother–infant dyads participated in a naturalistic free-play observation at six months postpartum, which was coded with the AMBIANCE for disrupted caregiving. At 22 months postpartum, dyads participated in the SSP, which was coded for infant attachment disorganization. Mothers retrospectively reported their HCM on the Adverse Childhood Experiences (ACEs) Questionnaire at 24 months postpartum.
Measures
Maternal childhood maltreatment
The ACEs Questionnaire (Felitti et al., Reference Felitti, Anda, Nordenberg, Williamson, Spitz, Edwards, Koss and Marks1998) is a 10-item self-report measure that assesses the presence (1 = yes) or absence (0 = no) of child maltreatment (i.e., physical abuse, verbal abuse, sexual abuse, physical neglect, and emotional neglect) and household dysfunction (i.e., domestic violence, parent divorce or separation, parent substance abuse, parent mental illness, and parent incarceration) prior to age 18. Responses are summed across items to create a total ACEs score, ranging from 0 (no ACEs) to 10 (all ACEs assessed). Composite scores are obtained for child maltreatment and household dysfunction by summing the responses across items relevant to each domain. To remain consistent with the literature examining maternal HCM and attachment disorganization, only the child maltreatment composite was included in analyses. The ACEs Questionnaire has demonstrated good reliability and internal consistency (Bruskas & Tessin, Reference Bruskas and Tessin2013) and acceptable test–retest reliability (Dube et al., Reference Dube, Williamson, Thompson, Felitti and Anda2004). Internal consistency was acceptable (Cronbach’s α = .71) for child maltreatment.
Maternal depression
The EPDS (Cox et al., Reference Cox, Holden and Sagovsky1987) is a 10-item self-report questionnaire, with total scores ranging from 0 to 30. Higher scores reflect greater depression severity, and a clinical cutoff of ≥13 suggests a probable diagnosis of clinical depression (Jomeen & Martin, Reference Jomeen and Martin2007). The EPDS has demonstrated excellent reliability and validity in perinatal samples (Cox et al., Reference Cox, Holden and Sagovsky1987; Jomeen & Martin, Reference Jomeen and Martin2007). Internal consistency was acceptable (Cronbach’s α > 0.80). Prenatal and postnatal depression scores were included independently and modeled separately in the analyses.
Maternal psychopathology
Mothers reported symptoms of prenatal and postnatal alcohol use, drug use, posttraumatic stress, and psychosis on corresponding scales of the PDSQ (Zimmerman & Mattia, Reference Zimmerman and Mattia2001). Respondents rate the presence (1) or absence (0) of each symptom, which are summed to create total scores for each scale. Higher scores reflect greater self-reported symptomology. The PDSQ has demonstrated good-to-excellent internal consistency, test–retest reliability, and validity (Zimmerman & Mattia, Reference Zimmerman and Mattia2001). The PDSQ uses established DSM-IV diagnostic criteria to determine whether responses meet the threshold for a “probable” diagnosis. The number of endorsed responses required to suggest a probable diagnosis of that disorder varies by scale.
Data reduction
To reduce the number of variables, composite psychopathology scores were created (see Lickenbrock and Braungart-Rieker (Reference Lickenbrock and Braungart-Rieker2015) for a similar data reduction approach). All prenatal scales were significantly correlated with at least one other prenatal scale (r’s ranged from .16 to .37). However, the postnatal scales were not significantly associated with one another, potentially due to missing data on these scales (49.1%). In addition, no mothers reported postnatal drug use. Thus, only a prenatal psychopathology composite was retained using the prenatal scales. Maternal depression was excluded from this composite due to the differences in questionnaires administered, inability to combine postnatal depression with other postnatal psychopathology scales, and to allow for comparison with the broader literature, as more research exists on maternal depression and attachment disorganization than other forms of psychopathology. The prenatal psychopathology composite was created by obtaining z-scores for the prenatal alcohol use, drug use, psychosis, and posttraumatic stress scales and summing them. Higher composite scores indicated greater symptomatology.
Maternal disrupted caregiving
Mothers and their infants participated in videotaped free-play interactions with a standard set of age-appropriate toys for approximately four minutes when infants were six months old. Previous studies have shown disrupted caregiving can be validly assessed in 3–12 minute interactions (Eirich et al., Reference Eirich, Pador, Watt, Racine, Lyons-Ruth and Madigan2024; Madigan et al., Reference Madigan, Bakermans-Kranenburg, Van Ijzendoorn, Moran, Pederson and Benoit2006) and with infants as young as four months (e.g., Khoury et al., Reference Khoury, Bosquet Enlow, Patwa and Lyons-Ruth2020). Maternal behavior was coded for disrupted caregiving using the AMBIANCE (Bronfman et al., Reference Bronfman, Madigan and Lyons-Ruth2009-2014; Bronfman et al., Reference Bronfman, Parsons and Lyons-Ruth1992-2008). Raters observe and write a narrative description of each interaction, then code the frequency of approximately 150 behavioral items using the written narrative and repeated observation. The behavioral items map onto five dimensions of disrupted caregiving that have evidence of construct validity: affective communication errors, role/boundary confusion, fearful/disorientation, intrusiveness/negativity, and withdrawal (Haltigan et al., Reference Haltigan, Madigan, Bronfman, Bailey, Borland-Kerr, Mills-Koonce and Lyons-Ruth2017). Frequency counts are totaled and compared with qualitative descriptions for each dimension, ranging on scales from 1 (no disrupted behavior) to 7 (disrupted behavior with little-to-no ameliorating behavior). An overall disrupted caregiving score is derived from the dimensional ratings by comparing the ratings to qualitative descriptions of disrupted caregiving, ranging on scales from 1 (no disrupted behavior) to 7 (disrupted behavior with little-to-no ameliorating behavior) with a cutoff score of > 4 for categorical classification as “disrupted.”
Prior to this study, the first author (JC) and reliability coder (Dr. Elisa Bronfman) achieved reliability certification (ICC’s ≥ .70, N = 20) on a standard set of AMBIANCE training videos. Approximately 20% of the dyads (n = 55) from the current sample were randomly selected for double coding to assess interrater reliability. The coders were blinded to all other measures while coding. Agreement was good for overall disrupted caregiving, ICC = .85, p < .001.
Infant attachment disorganization
The SSP (Ainsworth et al., Reference Ainsworth, Blehar, Waters and Wall1978) involves a series of eight structured episodes that include two separations and two reunions between the primary caregiver, infant, and a stranger (i.e., a research confederate), designed to evoke mild levels of infant stress and amplify attachment behaviors. It is a valid assessment of infant attachment between 11 and 24 months of age (Madigan et al., Reference Madigan, Fearon, van Ijzendoorn, Duschinsky, Schuengel, Bakermans-Kranenburg, Ly, Cooke, Deneault, Oosterman and Verhage2023). In this study, infants were observed through a one-way mirror and videotaped for coding. Attachment behaviors were scored on a 9-point scale of disorganized behaviors, with scores ≥ 5.5 typically qualifying as disorganized (Main & Solomon, Reference Main and Solomon1990). Disorganized infants demonstrate a lack organized strategies for coping with the stress of separation-reunions and display inconsistent and incoherent behaviors. The sixth author (MH), deemed reliable by A. Sroufe (Institute of Child Development, University of Minnesota) and M. van IJzendoorn (Cambridge University) and blind to parenting measures, independently scored the videos. An expert coder at the Institute for Child Development coded a randomly selected subset (15%) of the videos for reliability, Cohen’s κ = 0.73.
Sociodemographic risk
Consistent with previous research (e.g., Nagy et al., Reference Nagy, Kenyhercz and Szele2022; Thomas-Argyriou et al., Reference Thomas-Argyriou, Letourneau, Dewey, Campbell and Giesbrecht2021), a sociodemographic risk composite was created by summing and reflecting z-scores for ethnicity (0 = minoritized, 1 = white), family income (1 = < $20,000/year, 2 = $20,000–$39,999, 3 = $40,000–$69,000, 4 = $70,000–$99,999, 5 = $100,000 or more), and maternal education (1 = completed less than a high school degree, 2 = completed high school, 3 = completed a trade or technical school, 4 = completed an undergraduate degree, 5 = completed a graduate degree). Higher composite scores indicated greater sociodemographic risk (i.e., minoritized race/ethnicity, lower family income, and lower maternal education).
Covariates
To isolate the unique effect of disrupted caregiving on attachment disorganization, maternal sensitivity was included as a covariate (e.g., Van Ijzendoorn et al., Reference Van Ijzendoorn, Schuengel and Bakermans–Kranenburg1999). To avoid shared measurement variance, maternal sensitivity was assessed with the Nursing Child Assessment Satellite Training (NCAST) when children were six months old (Sumner & Spietz, Reference Sumner and Spietz1994). Mother–child interactions during a teaching task ranging from 1-5 minutes were coded by a blinded and reliable coder, who achieved interrater reliability > 90% and intrarater reliability > 98%. To control for factors related to one or more key variables, maternal age, child age, child sex (0 = male, 1 = female), and gestational status (0 = full-term, 1 = preterm) were included as covariates (Madigan et al., Reference Madigan, Fearon, van Ijzendoorn, Duschinsky, Schuengel, Bakermans-Kranenburg, Ly, Cooke, Deneault, Oosterman and Verhage2023; McIntosh et al., Reference McIntosh, Schnabel, Youssef and Olsson2021; Van Ijzendoorn et al., Reference Van Ijzendoorn, Schuengel and Bakermans–Kranenburg1999).
Missing data
Three hundred and ten expecting mothers were enrolled in the study. Three mothers did not continue due to miscarriage. Two dyads were excluded due to suspected developmental disabilities (e.g., autism). Twenty mothers dropped out after completing the prenatal EPDS, which resulted in missing data across most variables. Reasons for dropout have been previously reported (Letourneau et al., Reference Letourneau, Aghajafari, Bell, Deane, Dewey, Field, Giesbrecht, Kaplan, Leung and Ntanda2022). Mothers who dropped out did not significantly differ from all other mothers on measures of prenatal depression (p = .333), income (p = .422), marital status (p = .172), ethnicity (p = .068), or education (p = .159), and were removed from further analyses. In total, N = 285 mother–child dyads were eligible for inclusion and 190 dyads had complete data across all variables. Data were missing for disrupted caregiving (6.0%), attachment disorganization (22.1%), maternal HCM (16.1%), prenatal depression (3.9%), postnatal depression (5.3%), prenatal psychopathology (9.5%), and sociodemographic risk (6.7%). The data appeared to be missing completely at random (MCAR) according to Little MCAR’s test, χ2 (131) = 151.96, p = .102.
Data screening
Variables were screened for outliers and statistical assumption violations using z-score transformations for all continuous variables, and visual inspection of histograms, Q-Q plots, skewness and kurtosis values, matrix scatter plots, Mahalanobis distance values, Levene’s test for equality of variances and Box’s test of homogeneity of variance-covariance matrices using child sex and ethnicity as grouping variables. Eight outliers exceeded z-scores of ±3.00 on maternal prenatal depression (n = 4) and postnatal depression (n = 4; Mowbray et al., Reference Mowbray, Fox-Wasylyshyn and El-Masri2019). These values fell within the plausible upper tails of risk distributions, and winsorizing would have artificially truncated meaningful variability; therefore, outliers were retained in analyses. Sensitivity analyses excluding outliers produced substantively identical results. Positive skewness was observed for prenatal depression, postnatal depression, prenatal psychopathology, HCM, and sociodemographic risk. A maximum likelihood robust estimator was employed to account for deviations from normality (Yuan & Bentler, Reference Yuan and Bentler2000). Pairwise linearity was satisfactory. Assumptions of homoscedasticity and homogeneity of the variance-covariance matrices were met across levels of child sex and ethnicity.
Statistical analyses
Descriptive statistics were performed in IBM SPSS (Version 29.0.2.0). Remaining analyses were conducted in MPlus 8.8 (Muthén & Muthén, Reference Muthén and Muthén1998–2017). Full information maximum likelihood (FIML) was used to estimate the missing data. FIML utilizes all observed data, including the model structure and interdependencies between variables, without imputing missing values. When the data are MCAR, FIML yields unbiased parameter estimates by maximizing the likelihood function based on the observed data and model parameters (Enders, Reference Enders2001). Maternal HCM, prenatal depression, postnatal depression, prenatal psychopathology, disrupted caregiving, and sociodemographic and psychosocial risk were examined as predictors of attachment disorganization, with maternal sensitivity, maternal age, child sex, child age, and gestational status included as covariates.
All predictors and covariates were centered to reduce multicollinearity. In line with developmental theories emphasizing cumulative and conditional risk, interactions between maternal disrupted caregiving and candidate risk factors were tested to evaluate whether sociodemographic or psychosocial risk amplified or attenuated associations with attachment disorganization. Interaction terms showing significant or clearly marginal effects (p < .10) in these prescreening models were then carried forward into the final multivariate models.
Interaction terms for significant predictors were computed using the centered variables prior to analyses. Simple slope analyses examined the strength of the associations in the moderation analyses. A power analysis performed in G*Power (Faul et al., Reference Faul, Erdfelder, Buchner and Lang2009) indicated there was sufficient power to reliably detect small effect sizes (Cohen’s f 2 = 0.016, corresponding to β ≈ .125), given the number of model of variables (13), available sample size (N = 285), alpha of < .05, and acceptable power ≥ .80.
Results
Descriptive statistics
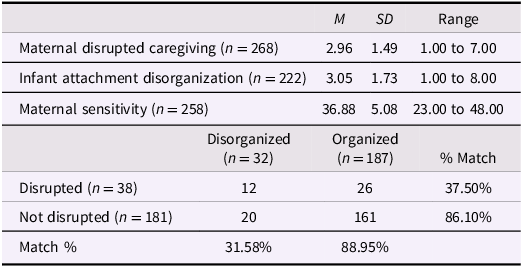
Descriptive statistics for maternal HCM, depression, and psychopathology are presented in Supplementary Table 1. As shown in Table 2, most mothers (67.5%) were classified as “not disrupted” and demonstrated low levels of disrupted caregiving. Most infants (84.2%) were classified with organized attachments and demonstrated low levels of attachment disorganization.
Descriptive statistics and cross-tabulations for caregiving and attachment measures
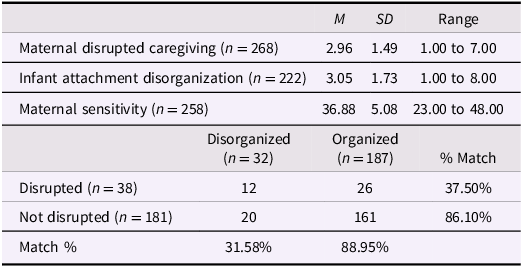
Table 2 Long description
The table presents descriptive statistics and cross-tabulations for caregiving and attachment measures. It has two main sections. The first section includes three rows and four columns. The columns are labeled M, SD, and Range. The rows are labeled Maternal disrupted caregiving (n = 268), Infant attachment disorganization (n = 222), and Maternal sensitivity (n = 258). The values in the rows are as follows: Row 1: M, 2.96; SD, 1.49; Range, 1.00 to 7.00. Row 2: M, 3.05; SD, 1.73; Range, 1.00 to 8.00. Row 3: M, 36.88; SD, 5.08; Range, 23.00 to 48.00. The second section includes a cross-tabulation of Disorganized and Organized attachment types with Disrupted and Not disrupted caregiving types. The columns are labeled Disorganized (n = 32), Organized (n = 187), and % Match. The rows are labeled Disrupted (n = 38) and Not disrupted (n = 181). The values in the rows are as follows: Row 1: Disorganized, 12; Organized, 26; % Match, 37.50%. Row 2: Disorganized, 20; Organized, 161; % Match, 86.10%. The Match % row shows 31.58% for Disorganized and 88.95% for Organized.
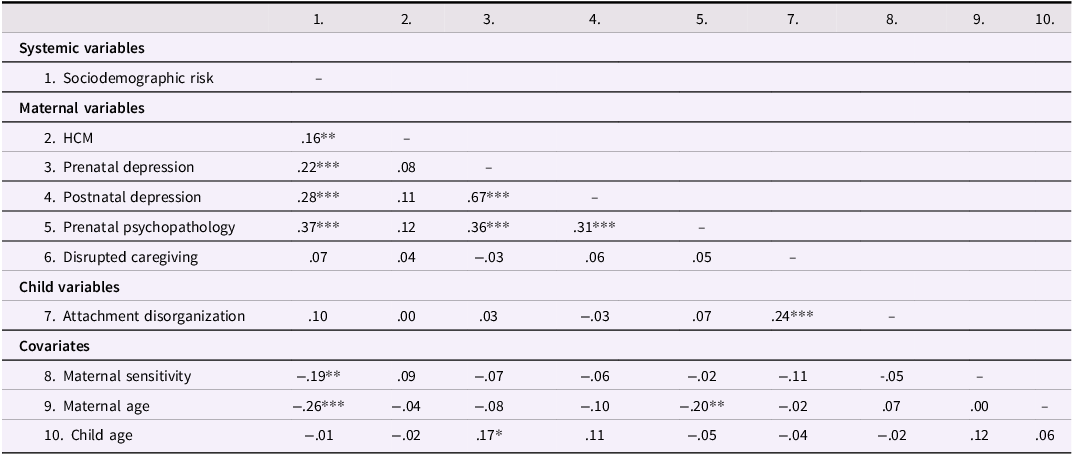
Bivariate correlations are presented in Table 3 (see Supplementary Table 2 for correlations after FIML). Sociodemographic risk was positively associated with maternal HCM, prenatal and postnatal depression, and prenatal psychopathology, and negatively associated with maternal sensitivity and age. Maternal HCM was not associated with any variables. Prenatal depression was positively correlated with postnatal depression, prenatal psychopathology, and child age. Postnatal depression was positively associated with prenatal psychopathology. Prenatal psychopathology was negatively correlated with maternal age. Disrupted caregiving and attachment disorganization were positively associated with one another, but not with any other variables.
Pairwise bivariate correlations among continuous study variables before FIML (N = 211 to 274)
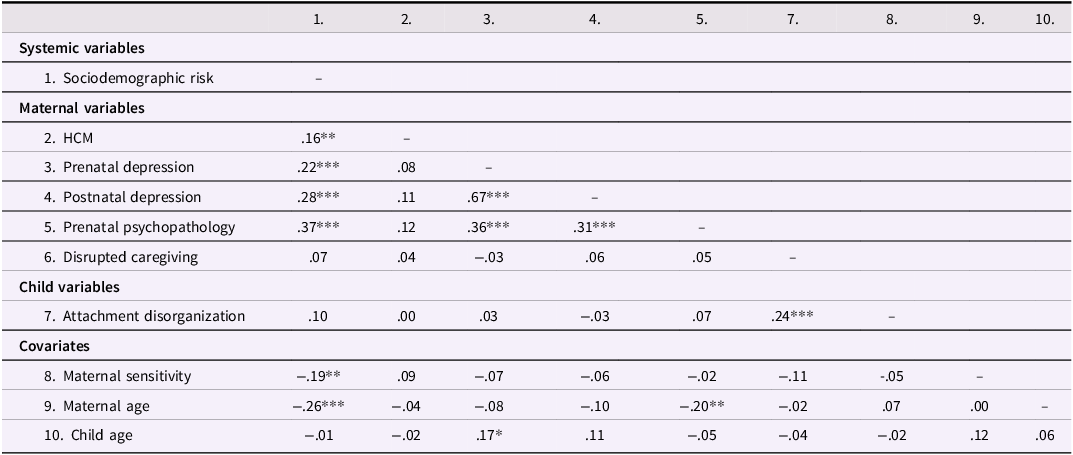
Table 3 Long description
The table presents bivariate correlations among continuous study variables before FIML, with data ranging from N = 211 to 274. It includes systemic variables, maternal variables, child variables, and covariates. The table has 10 columns and 8 rows, including headers. Column headers are numbered from 1 to 10. Row labels include Sociodemographic risk, HCM, Prenatal depression, Postnatal depression, Prenatal psychopathology, Disrupted caregiving, Attachment disorganization, Maternal sensitivity, Maternal age, and Child age. Row 1: Sociodemographic risk, empty values. Row 2: HCM, 0.16. Row 3: Prenatal depression, 0.22, 0.08. Row 4: Postnatal depression, 0.28, 0.11, 0.67. Row 5: Prenatal psychopathology, 0.37, 0.12, 0.36, 0.31. Row 6: Disrupted caregiving, 0.07, 0.04, -0.03, 0.06, 0.05. Row 7: Attachment disorganization, 0.10, 0.00, 0.03, -0.03, 0.07, 0.24. Row 8: Maternal sensitivity, -0.19, 0.09, -0.07, -0.06, -0.02, -0.11, -0.05. Row 9: Maternal age, -0.26, -0.04, -0.08, -0.10, -0.20, -0.02, 0.07, 0.00. Row 10: Child age, -0.01, -0.02, 0.17, 0.11, -0.05, -0.04, -0.02, 0.12, 0.06.
Note. ∗p < .05, ∗∗p < .01, ***p < .001. HCM = maternal history of childhood maltreatment.
Prediction of infant attachment disorganization
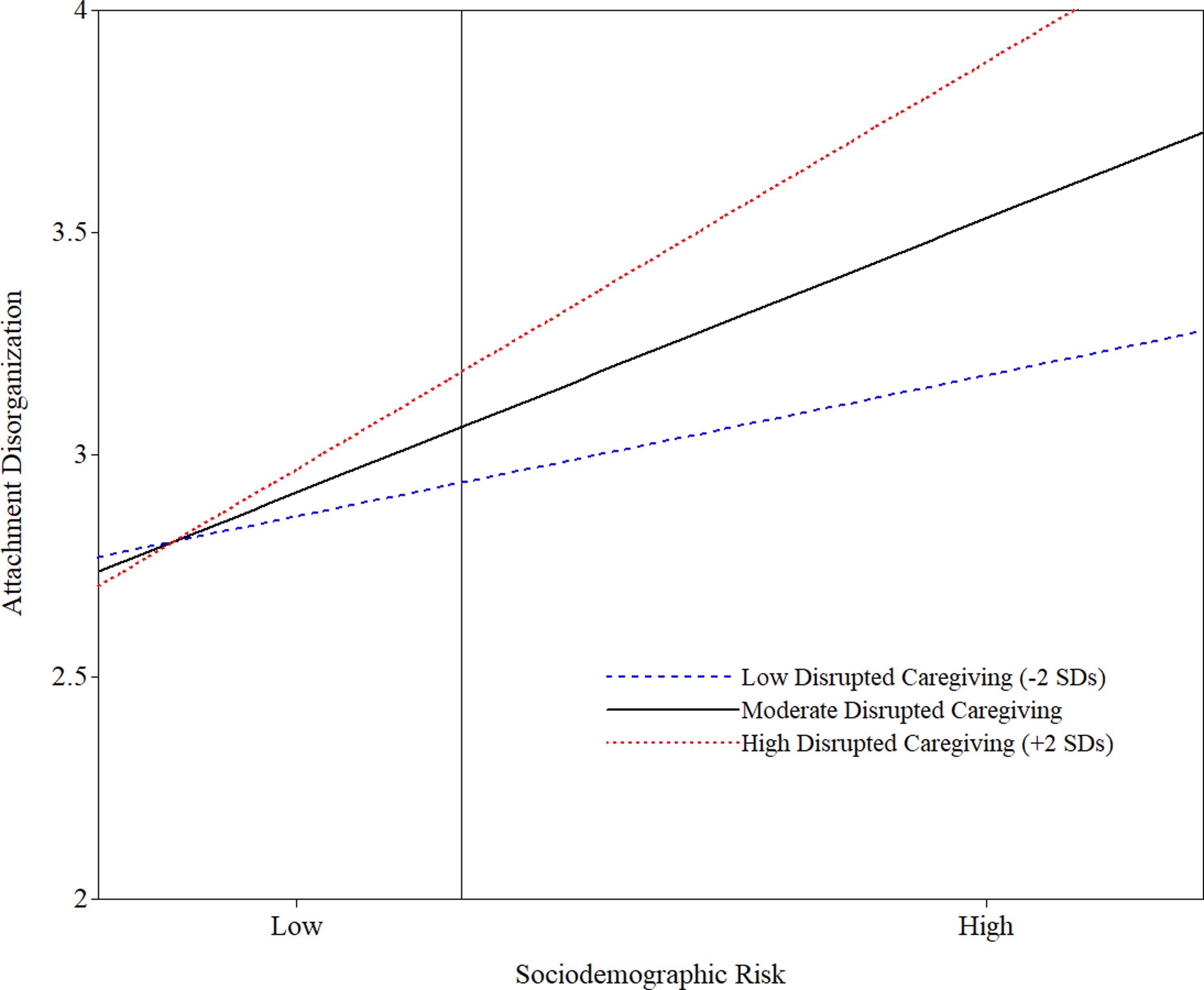
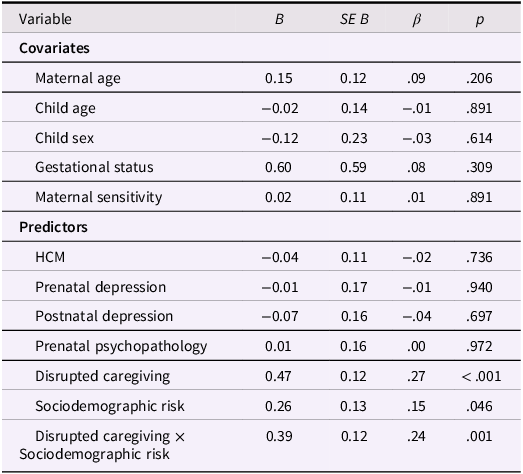
Only sociodemographic risk (β = .15, p = .046) and disrupted caregiving (β = .27, p < .001) were uniquely associated with greater attachment disorganization, independent of covariates and all other predictors (see Table 4). In line with theoretically guided hypotheses, the interaction of sociodemographic risk and disrupted caregiving (β = .24, p = .001) was associated with greater attachment disorganization. The model accounted for 16.6% of the variance in attachment disorganization (p = .010). These results suggested sociodemographic risk and disrupted caregiving were independently and jointly associated with higher levels of attachment disorganization. No other theoretically guided interactions tested in the candidate set were significant (see Table 4).
Results of multiple linear regression predicting attachment disorganization (N = 285)
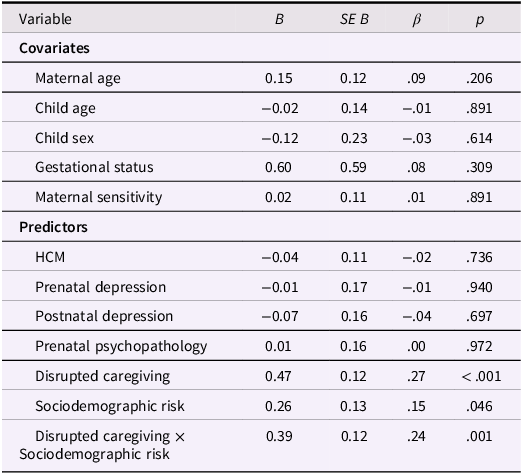
Table 4 Long description
A table with 15 rows and 5 columns. The columns are labeled Variable, B, SE B, β, and p. The table is divided into two sections: Covariates and Predictors. The Covariates section includes rows for Maternal age, Child age, Child sex, Gestational status, and Maternal sensitivity. The Predictors section includes rows for HCM, Prenatal depression, Postnatal depression, Prenatal psychopathology, Disrupted caregiving, Sociodemographic risk, and Disrupted caregiving × Sociodemographic risk. Each row lists values for B, SE B, β, and p. Notable values include p < .001 for Disrupted caregiving and Disrupted caregiving × Sociodemographic risk, and p = .046 for Sociodemographic risk.
Note. HCM = maternal history of childhood maltreatment. The same pattern of results emerged when prenatal and postnatal depression were combined into a composite depression score, and when scales from the prenatal psychopathology composite were entered as individual predictors in the model. When the regression was performed without the interaction term, disrupted caregiving significantly predicted infant attachment disorganization (β = .25, p < .001), but the association between sociodemographic risk and attachment disorganization did not reach statistical significance (β = .14, p = .077). All other predictors were nonsignificant. No other interactions were identified.
Simple slope analysis
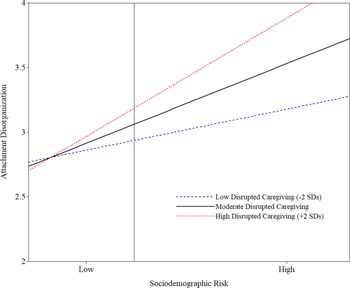
A simple slope analysis was conducted to examine the strength of the association between sociodemographic risk and attachment disorganization for mothers with high (2 SDs above the mean) and low (2 SDs below the mean) levels of disrupted caregiving. The association between sociodemographic risk and attachment disorganization was significant at high levels of disrupted caregiving (β = .33, p = .005), but not at low levels (β = .12, p = .215; see Figure 1).
The moderating role of maternal disrupted caregiving on the association between sociodemographic risk and infant attachment disorganization.
Note. Covariates included maternal sensitivity, maternal age, child age, child sex, and gestational status.
Discussion
This study examined longitudinal predictors of infant attachment disorganization in a low-risk Canadian pregnancy cohort. In partial support of hypotheses, observed maternal disrupted caregiving assessed at six months showed the strongest association with infant attachment disorganization at 22 months of age. After accounting for disrupted caregiving, sociodemographic risk was identified as the only other significant longitudinal correlate of attachment disorganization. In line with theoretically guided expectations and consistent with the threshold model proposed by Bernier and Meins (Reference Bernier and Meins2008), a significant interaction between disrupted caregiving and sociodemographic risk was found. Specifically, the association between sociodemographic risk and disorganization was only significant at high, but not low levels, of disrupted caregiving. These findings underscore the importance of considering both the unique and interdependent roles of caregiving and sociodemographic risk factors in the development of attachment disorganization.
The current findings align with previous research (e.g., Madigan et al., Reference Madigan, Bakermans-Kranenburg, Van Ijzendoorn, Moran, Pederson and Benoit2006), indicating disrupted caregiving as the most robust antecedent of infant attachment disorganization. The effect size was medium-to-large, based on adjusted benchmarks for attachment research (Schuengel et al., Reference Schuengel, Verhage and Duschinsky2021). These benchmarks, based on 75 meta-analyses of parent–child attachment, account for the complexities of attachment constructs and multifaceted determinants of child developmental (Schuengel et al., Reference Schuengel, Verhage and Duschinsky2021). Disrupted caregiving also remained the strongest predictor of attachment disorganization when other hypothesized risk factors were accounted for statistically. To support mothers at risk of engaging in disrupted caregiving, it is essential to identify the root causes of these challenges (e.g., maternal unresolved adult attachment representations, parenting stress, and maladaptive coping skills) that may serve as targets for preventive measures.
It is important to address disrupted caregiving behaviors in interventions aimed at reducing attachment disorganization, even in low-risk samples. The long-term stability of disrupted caregiving (Madigan et al., Reference Madigan, Voci and Benoit2011) and attachment disorganization (Opie et al., Reference Opie, McIntosh, Esler, Duschinsky, George, Schore, Kothe, Tan, Greenwood and Olsson2021) has been documented throughout early childhood. Furthermore, children with attachment disorganization are less likely to naturally transition to attachment security without adequate intervention (Opie et al., Reference Opie, McIntosh, Esler, Duschinsky, George, Schore, Kothe, Tan, Greenwood and Olsson2021). Results from two randomized controlled trials suggested interventions that reduce disrupted caregiving lower rates of disorganized attachment (Tereno et al., Reference Tereno, Madigan, Lyons-Ruth, Plamondon, Atkinson, Guedeney, Greacen, Dugravier, Saias and Guedeney2017; Yarger et al., Reference Yarger, Bronfman, Carlson and Dozier2020). Tereno, Madigan et al., (2017) reported that decreases in disrupted caregiving accounted for 25% of the intervention effect on disorganized attachment. Thus, evidence underscores the value of addressing disrupted caregiving early in children’s development, even when children are not classified as disorganized.
Sociodemographic risk was a significant predictor of infant attachment disorganization, demonstrating a small-to-medium effect size (Schuengel et al., Reference Schuengel, Verhage and Duschinsky2021). This finding extends previous meta-analytic evidence linking elevated sociodemographic risk to higher rates of disorganization (Cyr et al., Reference Cyr, Euser, Bakermans-Kranenburg and Van Ijzendoorn2010; Madigan et al., Reference Madigan, Fearon, van Ijzendoorn, Duschinsky, Schuengel, Bakermans-Kranenburg, Ly, Cooke, Deneault, Oosterman and Verhage2023). Notably, this result diverged from findings of Gedaly and Leerkes (Reference Gedaly and Leerkes2016), who did not find an effect of sociodemographic risk (i.e., maternal education, age, and an income-to-needs ratio) on infant attachment disorganization in a diverse community sample from the United States, when accounting for insensitive and anomalous caregiving behaviors. Differences in sample composition or measurement approaches may help explain these discrepancies. For instance, adversities experienced by minoritized groups (e.g., racism, historical trauma) may interact with other sociodemographic factors in shaping developmental risk. In this sample, minoritized families were more likely to have lower incomes than non-minoritized families. Future research is warranted to determine whether overt measures of racism and discrimination predict attachment disorganization, especially in conjunction with other sociodemographic risks.
An interaction between disrupted caregiving and sociodemographic risk in predicting attachment disorganization was identified. Sociodemographic risk was only linked to disorganization when disrupted caregiving was high, consistent with the threshold model proposed by Bernier and Meins (Reference Bernier and Meins2008), and findings from Gedaly and Leerkes (Reference Gedaly and Leerkes2016) who found maternal insensitivity predicted disorganization only at high levels of sociodemographic risk. Social-environmental risks may lower the threshold for disorganized attachment by weakening protective caregiving factors such as emotional availability and responsiveness. For children, this can lead to increased feelings of fear, confusion, or emotional insecurity in the caregiving relationship – especially when caregivers are overwhelmed by external pressures like unsafe neighborhoods, financial strain, or time scarcity (Lyons-Ruth et al., Reference Lyons-Ruth, Bronfman and Parsons1999; Roubinov & Boyce, Reference Roubinov and Boyce2017). These experiences may disrupt expectations of safety and support, heightening vulnerability to the effects of inconsistent or frightening caregiving. Moreover, chronic stressors during the perinatal period may influence offspring even before birth through fetal programming of maternal stress, shaping biological stress responses that increase later susceptibility to attachment disorganization (Berry et al., Reference Berry, Londoño Tobón and Njoroge2021). Longitudinal research is needed to clarify how sociodemographic and caregiving risks unfold over time and jointly or sequentially contribute to attachment disorganization.
Although Bernier and Meins (Reference Bernier and Meins2008) did not frame their threshold model of attachment disorganization within the context of ecological systems theory (Bronfenbrenner, Reference Bronfenbrenner2005), findings from the current study suggested these perspectives are complementary. From an ecological systems perspective, risk factors located within the caregiver-child microsystem may be more proximally related to the development of attachment disorganization (e.g., parenting behavior), while other risk factors located in broader social and environmental exosystems (e.g., sociodemographic risks) may be distally related influences, affecting the child through their interaction with proximal caregiving difficulties in the home environment. In the current study, the distal role of sociodemographic risk interacted with the proximal role of disrupted caregiving in the prediction of attachment disorganization, highlighting the need to investigate risk factors within multiple systems of influence, as well as interactions between systems, to better understand the complex development of attachment disorganization. Integrating ecological systems perspectives into attachment research could yield further insights into the systems shaping infant attachment disorganization (e.g., Lickenbrock & Braungart-Rieker, Reference Lickenbrock and Braungart-Rieker2015).
Maternal depression and psychopathology did not predict attachment disorganization, despite prior meta-analytic associations (e.g., Badovinac et al., Reference Badovinac, Martin, Guérin-Marion, O’Neill, Pillai Riddell, Bureau, Spiegel and Tachibana2018; Madigan et al., Reference Madigan, Fearon, van Ijzendoorn, Duschinsky, Schuengel, Bakermans-Kranenburg, Ly, Cooke, Deneault, Oosterman and Verhage2023). These findings align with research suggesting associations may exist in high-risk or clinical samples, but perhaps not in lower-risk community samples (McIntosh et al., Reference McIntosh, Schnabel, Youssef and Olsson2021). The timing, chronicity, and severity of maternal depression may also play a crucial role in understanding this association. For example, a study using the NICHD SECCYD sample found maternal depression symptoms predicted disorganized attachment at 36 months, while depression within the first 15 months did not (Campbell et al., Reference Campbell, Brownell, Hungerford, Spieker, Mohan and Blessing2004). Physiological indicators of maternal perinatal stress, such as cortisol levels, may be stronger predictors of disrupted caregiving (e.g., Khoury et al., Reference Khoury, Bosquet Enlow, Patwa and Lyons-Ruth2020) and attachment disorganization (e.g., Kurbatfinski et al., Reference Kurbatfinski, Woo, Ntanda, Giesbrecht and Letourneau2024), compared with questionnaire measures. Alternatively, low base rates of depression and psychopathology reported in both the prenatal and postnatal periods in the current study may have led to reduced variance in the data, which in turn limits the statistical power to detect significant and potentially meaningful associations between variables. Finally, most mothers were married in this study. Partner social support, which could not be examined, may have buffered against cascading effects on attachment disorganization, providing a potential avenue for future research.
Lastly, maternal HCM did not predict attachment disorganization, possibly reflecting underlying complexities between distal experiences of maternal trauma and infant attachment disorganization in low-risk samples. Ludmer et al. (Reference Ludmer, Gonzalez, Kennedy, Masellis, Meinz and Atkinson2018) suggested higher maternal levels of cortisol secretion and more plasticity alleles of the OXTR receptor gene (rs53576) could increase infants’ cortisol levels or mothers’ likelihood to engage in disrupted caregiving behaviors, thereby lowering the threshold for attachment disorganization in samples with few social risks. Madigan et al. (Reference Madigan, Fearon, van Ijzendoorn, Duschinsky, Schuengel, Bakermans-Kranenburg, Ly, Cooke, Deneault, Oosterman and Verhage2023) also proposed social support may help mothers recover from HCM, protecting against subsequent difficulties. In samples with low rates of HCM, measuring the outcomes of trauma (e.g., unresolved attachment representations) or more proximal experiences (e.g., perinatal intimate partner violence) may help to elucidate nuances in the relation between maternal trauma histories and attachment disorganization.
Strengths and limitations
The comprehensive longitudinal and multi-method approach to understanding attachment disorganization is a strength of this study. However, several limitations should be noted. Due to feasibility constraints, reliance on questionnaire measures of maternal psychopathology and HCM may have introduced reporting biases and contributed to null findings. The psychopathology composite, while necessary for data reduction, may have obscured distinctions between specific symptoms, particularly regarding psychosis which is an area with limited research. Sociodemographic risk was assessed at a single time point. Although relatively stable over time, temporal changes in sociodemographic risk may influence disrupted caregiving and attachment disorganization, warranting future study. Categorical classifications of disrupted caregiving and disorganized attachment were not investigated due to low base rates in this sample. Secondary data use also limited the range of variables available for investigation. Future research should explore other sociodemographic risks (e.g., housing instability) and caregivers’ unresolved attachment representations when testing comprehensive etiological models of attachment disorganization.
The low-risk nature of the sample and exclusion of mothers with prenatal substance use may have contributed to low rates of maternal psychopathology, disrupted caregiving, and attachment disorganization. These measures were included because, even at low base rates, subtle variations in maternal psychopathology can have nuanced and clinically meaningful impacts on child outcomes. Moreover, while the participants and their reported symptoms were representative of families in a large urban region of Canada (Leung et al., Reference Leung, McDonald, Kaplan, Giesbrecht and Tough2013), generalizability may be limited to low-risk samples. Furthermore, minoritized groups were combined and contrasted with white dyads due to limited diversity in the sample, potentially overshadowing differences across ethnic backgrounds. Future studies should recruit more diverse samples and provide comparisons between various ethnic groups (not only with white groups) to better understand how marginalization relates to disrupted caregiving and attachment disorganization. Finally, although subsample recruitment was not driven by the present research questions and any selection bias is unlikely to be systematically tied to the focal variables, it may still have produced a lower-risk sample, further limiting generalizability.
Clinical implications
Clinical approaches should address both disrupted caregiving and broader sociodemographic risks to reduce the occurrence of attachment disorganization. Prenatal home visiting programs for socially disadvantaged families may improve parenting outcomes by bolstering social support and education about childhood development, positive parenting skills, and healthy parent–child interactions (Kirkbride et al., Reference Kirkbride, Anglin, Colman, Dykxhoorn, Jones, Patalay, Pitman, Soneson, Steare, Wright and Griffiths2024). Parenting interventions are considered a universal prevention strategy against offspring behavioral concerns for families with sociodemographic risks (Kirkbride et al., Reference Kirkbride, Anglin, Colman, Dykxhoorn, Jones, Patalay, Pitman, Soneson, Steare, Wright and Griffiths2024). Thus, interventions evidenced to reduce disrupted caregiving (e.g., Tereno et al., Reference Tereno, Madigan, Lyons-Ruth, Plamondon, Atkinson, Guedeney, Greacen, Dugravier, Saias and Guedeney2017; Yarger et al., Reference Yarger, Bronfman, Carlson and Dozier2020) or other parenting correlates of attachment disorganization (e.g., low reflective functioning; Anis et al., Reference Anis, Ross, Ntanda, Hart and Letourneau2022), could be beneficial for families across income levels. However, it is crucial to address barriers to engagement for low-income families (e.g., work-schedule conflicts) and develop culturally sensitive interventions to ensure the effectiveness of such interventions is maintained for families with sociodemographic disadvantages.
Combining cash transfer programs with interventions evidenced to reduce disrupted caregiving may be a promising area for future research (e.g., Fuller et al., Reference Fuller, Zaffar, Cohen, Pentland, Siddiqi, Vandermorris, Van Den Heuvel, Birken, Guttmann and de Oliveira2022). Importantly, the effectiveness of these programs varies by economic context, child gender, program implementation, mandatory conditions of income supplements, and local culture (Kirkbride et al., Reference Kirkbride, Anglin, Colman, Dykxhoorn, Jones, Patalay, Pitman, Soneson, Steare, Wright and Griffiths2024), suggesting these programs may only benefit certain at-risk dyads. Finally, coordination between mental health and social services is essential (Alegría et al., Reference Alegría, NeMoyer, Falgàs Bagué, Wang and Alvarez2018), as referrals from clinicians to social services may be insufficient for families facing social barriers. Community health workers and social workers can help families access housing, food security programs, and job placement resources, which have all been shown to alleviate social disparities for disadvantaged families (Alegría et al., Reference Alegría, NeMoyer, Falgàs Bagué, Wang and Alvarez2018; Kirkbride et al., Reference Kirkbride, Anglin, Colman, Dykxhoorn, Jones, Patalay, Pitman, Soneson, Steare, Wright and Griffiths2024).
Conclusions
This study found infants were more vulnerable to developing attachment disorganization in the context of greater sociodemographic risk and observed maternal disrupted caregiving. The association between sociodemographic risk and attachment disorganization was significant only at high levels of disrupted caregiving, suggesting the quality and stability of caregiving plays a crucial role in determining the impact of sociodemographic factors on infant attachment outcomes. Approaches to mitigate both disrupted caregiving and sociodemographic disadvantages may help create supportive environments for caregivers and children that foster improved attachment outcomes. Longitudinal research is needed to better understand how different sociodemographic risks (e.g., racism, low family income) interact with disrupted caregiving over time to influence attachment outcomes. The role of child characteristics should be incorporated into future investigations of Bernier and Meins’ (Reference Bernier and Meins2008) threshold model to help broaden understanding of how these characteristics interact with sociodemographic risks and disrupted caregiving to influence the development of attachment disorganization over time.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579426101205.
Data availability statement
Reporting for this study was prepared in accordance with Transparency and Openness Promotion (TOP) Level 2 Guidelines, and the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement.
Acknowledgments
The authors acknowledge the contributions of all the families who took part in the Alberta Pregnancy Outcomes and Nutrition (APrON) study, and the investigators, managers, research assistants, graduate and undergraduate students, volunteers and clerical staff of the APrON study team. The authors also thank Dr. Elisa Bronfman for coding a portion of the AMBIANCE videos.
Funding statement
This research was supported by a Social Sciences and Humanities Research Council of Canada Innovation Grant (SM, NR, AP, GG, NL, MH, TC), the Alberta Children’s Hospital Foundation Chair (NL), Alberta Innovates (JC, doctoral award), the Canadian Institutes of Health Research (TC, NL, GFG, grant number 219205), the Networks of Centres of Excellence (NCE): Allergy, Genes, and Environment Network (Allergen; NL, grant number 12GXE3), Vanier Canada (JC, doctoral award), a Children’s Hospital of Eastern Ontario Research Chair in Child and Youth Mental Health (NR), and the Canada Research Chairs Program (SM). Funding sources had no role in publication-related decisions.
Competing interests
The authors declare no competing interests.
Preregistration statement
This study was a secondary data analysis of the APrON Study and was not preregistered.
Availability of data
Per our data use agreement, we did not have approval to share the secondary dataset publicly. Researchers interested in accessing the data may submit a request to Dr. Nicole Letourneau (nicole.letourneau@ucalgary.ca), in accordance with the data governance procedures.
Availability of code
Our analytic code is available at https://osf.io/aymds/ under “Files”.
Availability of methods and materials
We have documented our study protocol and all necessary information to reproduce our analyses in the Method section of the manuscript. We are unable to share the AMBIANCE coding materials (e.g., written transcripts, coding manual) due to confidentiality restrictions and copyright protections. Researchers interested in using the AMBIANCE may contact AMBIANCE trainer, Dr. Sheri Madigan (sheri.madigan@ucalgary.ca).
AI statement
Parts of this manuscript were included in the first author’s dissertation, Cooke, J. E. (Reference Cooke2025). Caregiver-child attachment in early childhood: A multi-method investigation of caregiving antecedents and socioemotional outcomes (Doctoral thesis, University of Calgary, Calgary, Canada). Retrieved from https://prism.ucalgary.ca/items/d24605a2-4d5b-42a2-8fce-20d5d7673d1a. The authors used generative AI tools to assist with language editing and clarity. All intellectual content, analyses, and interpretations are the authors’ own, and the authors take full responsibility for the manuscript.



 Open access
Open access