


Introduction
Migraine is a major public health concern due to its prevalence and individual and societal burden. 1
Its management is challenging, as less than 20% of individuals with migraine seek professional help Reference Katsarava, Mania, Lampl, Herberhold and Steiner2 and typically self-manage with over-the-counter medication. Reference Katsarava, Mania, Lampl, Herberhold and Steiner2 Due to the complex and multidimensional nature of the disease, a biopsychosocial approach combining both pharmacological and non-pharmacological interventions is considered the best treatment. Reference Andrasik, Flor and Turk3 The results of cognitive-behavioral therapy (CBT) are modest yet have benefits in reducing pain. Reference Ng, Venkatanarayanan and Kumar4,Reference Bae, Sung and Kwon5 Clinical practice guidelines 6 state that CBT can be used alone or in conjunction with medication. CBT is a family of interventions that encompasses different techniques (e.g., psychoeducation, self-monitoring, relaxation) that target different factors. Reference Hofmann, Asnaani, Vonk, Sawyer and Fang7 Little attention has been paid to specific elements and whether they may impact CBT’s effects.
Conventional CBT includes face-to-face sessions with a therapist for 8–12+ sessions, but this approach has considerable practical and financial limitations. Reference Brown, Newman, Noad and Weatherby8 One promising solution is self-guided Internet-based CBT (iCBT).
The research on iCBT interventions for migraine is at a preliminary stage. There are few published studies. Most of them are pilots with small samples, and a minority showed effectiveness in reducing headaches. Reference Minen, Torous and Raynowska9,Reference Mosadeghi-Nik, Askari and Fatehi10 There is a need for larger, pragmatic randomized clinical trials (RCTs) to evaluate the effectiveness of iCBT interventions for migraine before recommending their use.
The primary purpose of this study was to compare the effectiveness of two iCBT interventions against a waitlist control. The interventions were SPHERE (Specialized Program for Headache Reduction), which uses a broad CBT approach including psychoeducation, self-monitoring and skills training, covering most factors that have been linked to migraine, and PRISM (Personalized Intervention for Self-Management of Migraine), a personalized intervention that identifies an individual’s triggers and provides CBT skills, building on frequently recommended advice to either cope with or avoid triggers. Reference Graf, Kim and Brewer11 We examined at least a 50% reduction in the number of headache days over 4 weeks (primary outcome) and a statistically significant reduction in peak headache severity over 4 weeks (secondary outcome), as well as a reduction in headache-related functional impairment and depressive symptomatology (exploratory outcomes) from baseline to 4 months post-randomization. We hypothesized that SPHERE or PRISM would reduce the number of headache days and peak headache pain intensity compared to waitlist control.
The secondary purpose of this study was to evaluate the uptake, adherence and satisfaction with the iCBT interventions.
Methods
Procedures and participants
A prospective parallel three-arm RCT was conducted. Participants were recruited globally using online social media, as well as partnerships with headache clinics and professional associations. Recruitment started in April 2018 and ended in August 2019 when the target sample size was obtained. Eligibility was determined based on self-report and involved a two-step process. Interested individuals accessed a 12-item online survey that assessed preliminary eligibility (step one). Inclusion criteria for preliminary eligibility were (1) aged 14–40 years. We selected this age range for two reasons: (a) to target migraine in the early stages to increase the likelihood of influencing behaviors and (b) to reach a wide age range to potentially benefit as many people as possible; (2) fluent in English; (3) living with migraine as indicated by a score of 2 and above on the ID Migraine; Reference Lipton, Dodick and Sadovsky12 (4) living with migraine for a minimum of 3 months (for 14–17 years old) or 1 year (for 18–40 years); and (5) owning a smartphone with Internet access that is used for more than texting and calling. Exclusion criteria for preliminary eligibility were (1) a known underlying reason for headaches; (2) pregnant, planning to get pregnant in the following 4–6 months or breastfeeding. Since hormonal changes greatly influence migraine in women, these groups are recommended to be excluded from trials of behavioral treatments Reference Penzien, Andrasik and Freidenberg13 because it would be challenging to ascertain if these interventions are the reason for improvements in the outcome measures; (3) inability to give informed consent; (4) diagnosed with psychosis and/or schizophrenia; and (5) having participated in the pilot RCT. If eligible in the preliminary stage, individuals were asked to provide electronic informed consent. Once consented, participants were asked to complete a T1 assessment to confirm eligibility for the second step for enrollment into the study and obtain baseline data. The T1 assessment involved completing an electronic headache diary (EHD) daily for 4 weeks and completing an online baseline questionnaire. To be eligible, they had to have a minimum of 4 headache days in a 4-week period at T1. Exclusion criteria included (1) having completed less than 14 daily EHD entries at T1 or (2) having more than 20 headache days in the 4-week period since the management of highly frequent migraine attacks or chronic daily migraine is especially difficult and complex and low-intensity interventions are more intended to prevent the escalation of mild or moderate conditions into more severe ones. Criteria were aligned with the American Headache Society and the International Headache Society guidelines. Reference Penzien, Andrasik and Freidenberg13
Participants eligible for study enrollment were then randomized 1:1:1 to the SPHERE, PRISM or waitlist group with stratification by age (14–21 years and 22–40 years). A permuted block randomization procedure 14 was generated by an external researcher who prepared sealed numbered envelopes. The research assistant allocated the eligible participants to their group, which participants were not blind to. Those allocated to SPHERE or PRISM received a link and were encouraged to use their program for 4 months via automated notifications. A final assessment, at 4 months post-randomization (T2), included a 4-week headache diary assessment and another online questionnaire. Participants received an honorarium following completion of the assessments at T1 and T2. After T2, those assigned to the waitlist were given access to either PRISM or SPHERE.
The trial protocol was approved by the ethics committee at the home institution of the principal investigator and at each participating headache clinic. The trial was registered at ClinicalTrials.gov. The CONSORT reporting guidelines Reference Schulz, Altman and Moher15 were followed. Unanticipated problems were recorded and reported to the ethics committee at the home institution, and adverse events were not monitored. Changes to the eligibility criteria were made after the initiation of the trial to facilitate recruitment and generalizability (see Figure 1).
Flowchart of the participants. After 4 months of recruitment, we removed the stable pattern exclusion criterion (i.e., stable pattern of headaches for 6 months) (step 1); we added that those in the 14–17 age range had to self-report headaches for at least 3 months instead of 1 year (step 1), and we only excluded participants that report more than 20 headache days during the 4-week period at T1 instead of 15 headache days (step 2).

iCBT interventions
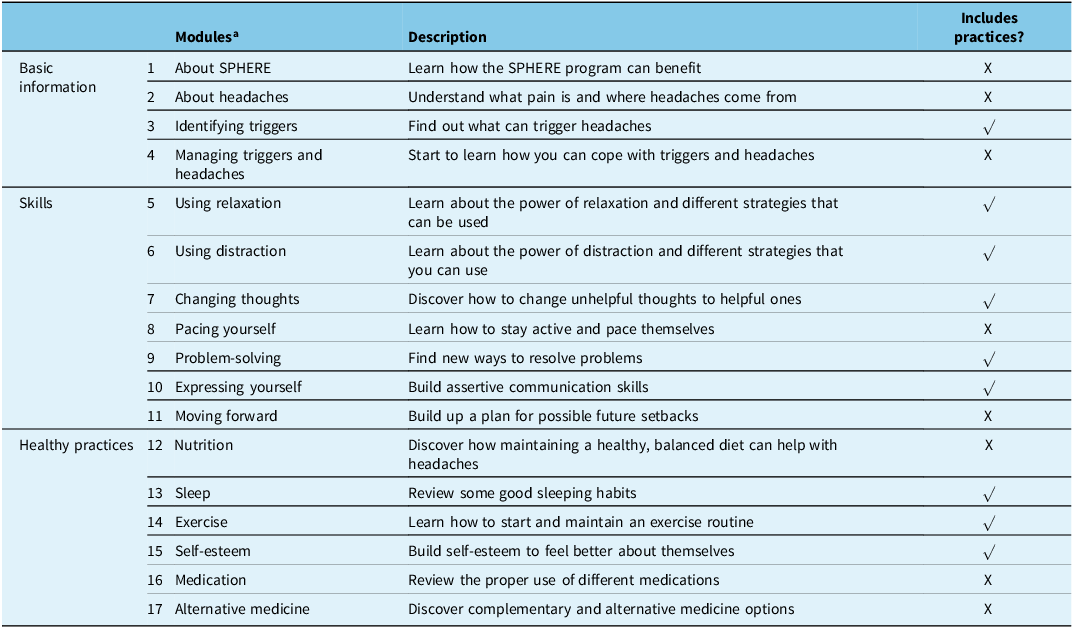
SPHERE consists of 17 20-minute interactive multimedia modules providing education about headaches, teaching CBT skills and encouraging healthy habits (see Table 1). Each module content is organized into sections including Goals, Getting Started, Let’s Talk/Let’s Practice and a Quiz. Nine out of the 20 modules include “practices” to allow users to practice and reinforce the skills or healthy practices learned in the modules in their everyday lives. Users are encouraged to complete at least two modules and accompanying practice activities each week. The use of SPHERE also includes the myWHI headache diary Reference Huguet, McGrath and Wheaton16 to track relevant information (e.g., potential triggers and headache frequency) and a discussion forum to connect SPHERE users. Reference Huguet, Stinson and Mackay17 The SPHERE forum was monitored by a moderator who was supervised by a licensed psychologist.
Content of SPHERE

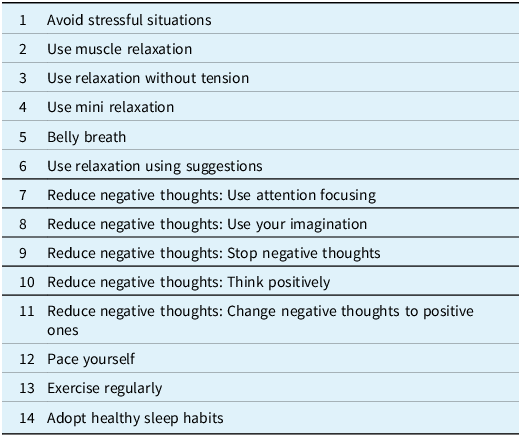
PRISM explains to users what a trigger is and the importance of identifying and coping with it. PRISM encourages users to consistently track a maximum of five potential triggers and record their headaches. PRISM lists 31 common triggers, but users can add their own. PRISM assesses the association between potential triggers and headaches and provides feedback on which suspected factors may be a trigger for the specific user (single or combinations of factors can be identified). A minimum amount of data is required for PRISM to analyze data (i.e., five headaches and seven exposures to the same possible trigger). Data are analyzed and updated every day. Once identified, users receive recommendations for either avoiding or coping with the triggers that cannot be avoided by using CBT skills that are taught through the application (see Table 2). Videos, animations or narrative examples are used to illustrate CBT skills. Users are encouraged to choose a recommendation and commit to it by setting a goal, which includes setting a start and end date for them to follow the selected recommendation. Users are then encouraged to continue tracking their headaches and exposures to the triggers, as well as completion of goals. Through the reports, users can see whether their headaches are improving and their level of adherence to the selected recommendation. Potential triggers and recommendations were developed based on a review of the scientific literature and a Delphi study with headache experts.
Example of recommendations and skills taught by PRISM to help cope with one of the major triggers of migraine attacks: stress

Both interventions are mobile-optimized web-based applications accessible by smartphone. In an attempt to satisfy diversity and inclusion for a diverse set of potential users, both interventions were tailored to employ characters with different characteristics in terms of age, gender and ethnicity. Participants received technical support and automated tailored reminders to stay engaged and reinforce their efforts. SPHERE and PRISM underwent in-lab usability testing with users Reference Huguet, Rozario, McGrath and Wozney18 and the feasibility of the two interventions and the full protocol was evaluated through a pilot RCT. 19
Waitlist control
They were not offered access to either SPHERE or PRISM but were put on a waiting list to receive their preferred program after 4 months post-randomization.
Measures
Screening measures for eligibility
ID -Migraine Reference Lipton, Dodick and Sadovsky12 was used to screen for migraine. ID-Migraine has shown good validity for the diagnosis of migraine. Reference Lipton, Dodick and Sadovsky12,Reference Zarifoğlu, Karli and Taşkapilioğlu20
A 12-item survey was used to see if potential participants met the criteria for preliminary eligibility (step 1) and to collect sociodemographic and headache characteristics.
A version of myWHI diary Reference Huguet, McGrath and Wheaton16 was used to track headaches.
Primary and secondary outcome measures (at T1 and T2)
The primary outcome (i.e., achieving at least a 50% reduction in the number of headache days per month) and secondary outcome (i.e., reduction in maximum headache severity) were evaluated using a simplified version of the myWHI diary. Reference Huguet, McGrath and Wheaton16 Participants recorded every day whether or not they had a headache and the highest pain intensity using an 11-point numerical rating scale (NRS-11) for 4 weeks.
Exploratory outcome measures (at T1 and T2)
The Migraine Disability Assessment Scale–Pediatric version (PedMIDAS)(21) and the Migraine Disability Assessment Scale (MIDAS) Reference Stewart, Lipton, Kolodner, Liberman and Sawyer22 were used for participants between 14 and 17 years old and for those between 18 and 40 years, respectively. PedMIDAS examines headache disability in school, at home and in extracurricular and social activities. MIDAS assesses the impact of headaches on work, school, household work and non-work time including family, social and leisure activities. Both measure scores range from 0 to 240, with a higher score indicating greater impact. Scores can also be categorized according to the degree of disability (“little or no disability: score 0–5; “mild”: score 6–10; “moderate”: score 11–20; “severe”: score 21–40; “very severe” ≥ 41). Both measures are valid and reliable. Reference Hershey, Powers, Vockell, LeCates, Kabbouche and Maynard21,Reference Stewart, Lipton, Kolodner, Liberman and Sawyer22
The Center for Epidemiological Studies–Depression Scale (CES-D) Reference Radloff23 evaluates depressive symptomatology. Using a 4-point Likert scale, individuals rate the occurrence of 20 depressive symptoms. Scores range from 0 to 60, with higher scores indicating more depressive symptoms. The CES-D also provides a cutoff point of 16 to screen for significant depressive symptomatology. The CES-D has sound psychometric properties. Reference Radloff23,Reference Hedborg and Muhr34
Acceptability measure (at T2)
The 8-item Client Satisfaction Questionnaire (CSQ-8) Reference Larsen, Attkisson, Hargreaves and Nguyen25,Reference Nguyen, Attkisson and Stegner26 evaluates consumer satisfaction with health and human services. Scores range between 8 and 32, with a higher score indicating higher satisfaction. It has been shown to be a reliable measure and to have good construct validity. Reference Attkisson and Zwick27 The following cut-off categories were used: low level of satisfaction (8–20), intermediate (21–26) or high (27–32). Reference Larsen, Attkisson, Hargreaves and Nguyen25
Sample size
Sample size estimates assumed that 20% of the control would clinically improve on the primary outcome (i.e., ≥ 50% reduction in monthly headache days) Reference Day, Thorn and Ward28 and a 15% difference for participants in the treatment groups, with both groups combined, would be regarded as the minimal clinically important difference. Assuming a power of 80% and a (two-sided) significance level of 5%, 101 participants per group were required. The sample size was calculated with G-Power Reference Erdfelder, Faul and Buchner29 on the contrast between the combined treatment groups (n = 202) and the waitlist group (n = 101). A 40% attrition rate was anticipated. Reference Meyerowitz-Katz, Ravi, Arnolda, Feng, Maberly and Astell-Burt30 Thus, a total of 424 were needed. The primary analysis was planned to include all randomized subjects (intent-to-treat) using multiple imputations. A completers-only secondary analysis was also preplanned.
Analysis
Analyses were performed with SPSS Statistics (version 29; IBM Corp) and JASP (version 16; JASP Team). Participant characteristics were summarized descriptively as mean and standard deviations (SD) or frequency counts and percentage.
Dropout rates were calculated as the number of participants who completed less than 14 days in the EHD at T2 divided by the total number of participants who were randomized. The balance between intervention versus control groups and completers versus non-completers was assessed by the Fisher’s exact test and a 2 (combined treatment group vs. control) × 2 (completers vs. non-completers) between groups Analysis-of-Variance (ANOVA). Q–Q plots, histogram and density plots were used to assess assumptions of normality of continuous variables.
To evaluate treatment outcomes, two preplanned orthogonal contrasts were conducted. We contrasted the combined treatment groups (i.e., PRISM and SPHERE) with the waitlist (primary analysis), and we compared the two treatment groups to one another (secondary analysis).
When evaluating treatment effects on the primary and secondary outcomes, Fisher’s exact tests and independent samples t-tests were conducted. T-tests showed that missing data were not missing at random but were found to be related to group assignment, percentage of headache days and maximum headache intensity at pretreatment. However, it was assumed that the specific values of the missing data were randomly distributed. For this reason, multiple imputation was performed using the EM (expectation maximization) algorithm based on participants’ age, number of headache days at baseline and percentage of headache days and maximum headache intensity at baseline and 4 months. Ten separate datasets were generated where missing values on the percentage of headache days from the diary had been replaced for all participants who did not complete at least 14 days of the post-assessment. The imputed data were used to calculate the percentage reduction and then converted to a binary variable indicating if a 50% reduction had occurred (coded 1) or not (coded 0). Treatment effect analyses were performed on the 10 datasets, and the consistency in the direction and size of the estimated effects when performing control-combined treatment comparison and PRISM-SPHERE comparison was evaluated. The results were also combined into one single estimated effect. Odds ratio’s and Cohen’s d effect sizes were calculated to indicate the effect size at 4 months for the primary (50% reduction in number of headache days) and secondary outcomes (reduction in maximum intensity).
To provide a comprehensive overview and show the possible influence of missing values on our analyses, as planned, we included completers analyses.
Mixed effects linear modeling was used to evaluate change in exploratory outcomes (i.e., functional impairment and depression). Each exploratory outcome was regressed into groups (two levels: combined treatment vs. control and PRISM vs. SPHERE) and time (two levels) and the interaction of the group by time. These analyses were conducted using an intention to treat (ITT) approach, and full information maximum likelihood was used to estimate model parameters.
Significance tests were 2-tailed at a significance level of 0.05 and were not adjusted for multiple testing.
To describe uptake, frequency counts and percentage of participants who logged in at least once into the programs were calculated. To describe adherence to SPHERE, we calculated as the primary indicator the frequency counts and percentage of users who completed at least 50% of the modules (i.e., any 9 out of the 17 modules) since it was established that a reasonable use of SPHERE to have some benefit was to have completed at least 50% of the modules. We also calculated the frequency counts and percentage of users who completed all 17 modules and each module, the mean and SD of modules completed per user (defined as a participant having visited the last page of the module) and the average percentage of users performing practices per completed module that includes practices. For PRISM, we calculated as the primary indicator the frequency counts and percentage of users who set a goal for a recommendation since it was established that a reasonable use of PRISM to have some benefit was to have used it at the extent that the system has identified a potential trigger and provided recommendations and the user has selected a recommendation and set at least one goal. We also calculated the mean and SD of diary entries per user, frequency counts and percentage of users for whom PRISM was able to identify a potential trigger and mean, SD and median days that a user who set a goal tracked goal completion.
To describe satisfaction with the interventions, we calculated means and SD for the total CSQ-8 score when treated as continuous and frequency counts and percentage for the CSQ-8 score when treated as a categorical.
Results
Participant characteristics
Figure 1 shows the flow of participants through the study. 2,613 were screened to reach our desired sample size.
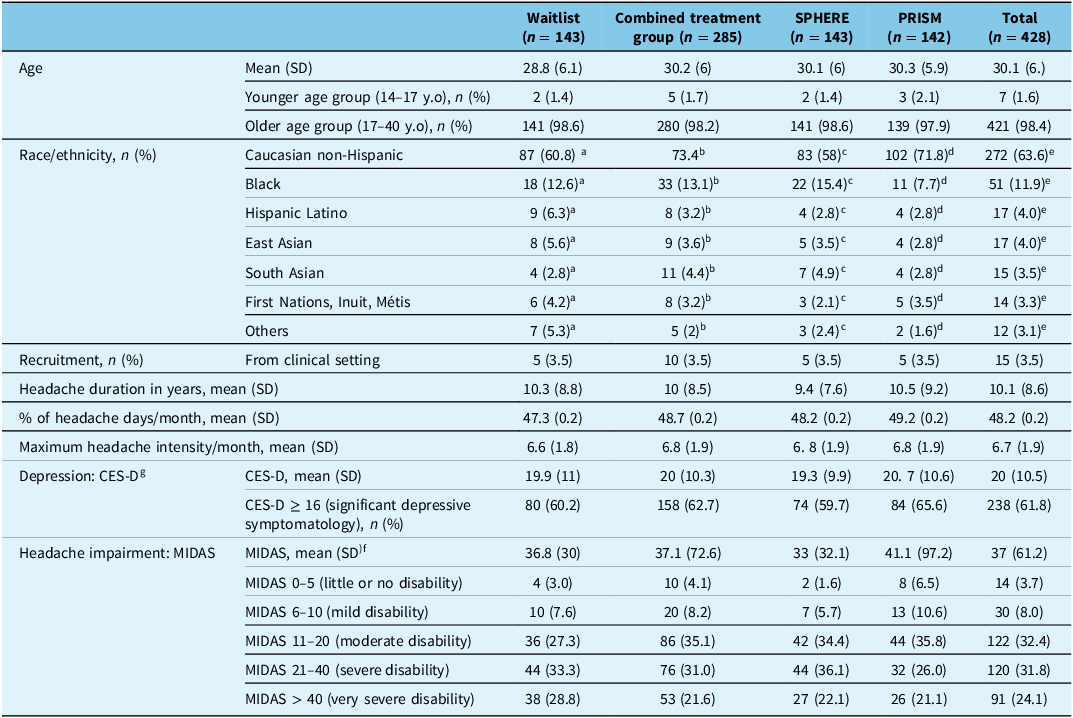
Participants were predominantly Caucasian non-Hispanic, females, over age 18 and recruited from the online community. At baseline, participants reported on average that they had lived with headaches for 10.3 years, that their headaches occurred on almost 50% of the days and had moderate intensity and that they experienced severe disability due to headaches (see Table 3).
Baseline characteristics of the participants

a 10 participants with missing data.
b 33 participants with missing data.
c19 participants with missing data.
d 14 participants with missing data.
e 43 participants with missing data.
f Only participants who were aged between 18 and 40 (n = 421, 98.4% of the total sample) were asked to complete Migraine Disability Assessment Scale (MIDAS). Only 377 participants completed the MIDAS.
g Only 385 participants complete the Center for Epidemiological Studies–Depression Scale (CES-D).
Missing treatment outcome data
Of the 428 people randomized, 207 participants did not complete at least 14 days of the 4 months post-randomization headache days measure and headache intensity measure (a 48% dropout rate) (see Figure 1). The dropout rate was not evenly distributed across the treatment and control: 113 of the 143 (79.0%) randomized control participants completed post-test measures, whereas only 108 of the 285 (37.9%) randomized treatment participants completed (Fisher’s exact p < 0.001).
There was no overall difference between the control and treatment groups on the percentage of headache days at baseline (50% control vs. 48% treatment, F = 0.81, p = 0.368). However, there was a difference on the baseline percentage of headache days between participants who completed post-test measures versus those who did not (44% completers vs. 53% non-completers, F = 14.46, p < 0.001). There was no interaction between group assignment and whether participants completed post-test measures on percentage headache days (F = 0.4, p = 0.526). A similar pattern was found when a 2 × 2 between groups ANOVA on baseline maximum headache intensity was performed. There was no overall difference between the control and treatment groups on baseline maximum headache intensity (6.9 control vs. 6.7 treatment, F = 0.91, p = 0.341). However, there was a difference on baseline headache intensity between participants who completed post-test measures versus those who did not (6.3 completers vs. 7.4 non-completers, F = 20.90 p < 0.001). There was no interaction between group assignment and whether participants completed post-test measures on headache intensity (F = 0.62, p = 0.432).
Primary and secondary treatment outcomes
Comparison between Internet-based treatment (combined treatment groups) and control
Intention-to-treat analyses
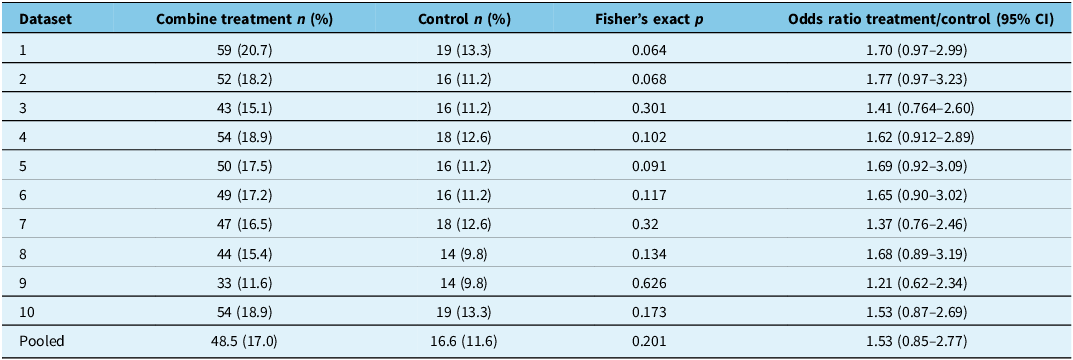
Table 4 displays the pooled odds ratio when comparing treatment against control on the primary outcome derived from the 10 imputed datasets. A nonsignificant effect of the intervention on a >50% reduction in headache days was found (17% vs. 11.6%, p = 0.20).
Intention-to-treat sample: Effectiveness of self-guided Internet-based treatment versus waitlist control on a >50% reduction in headache days. Imputed percentage and counts of participants achieving a 50% reduction of headache days and corresponding Fisher’s exact test and odds ratios for each imputation

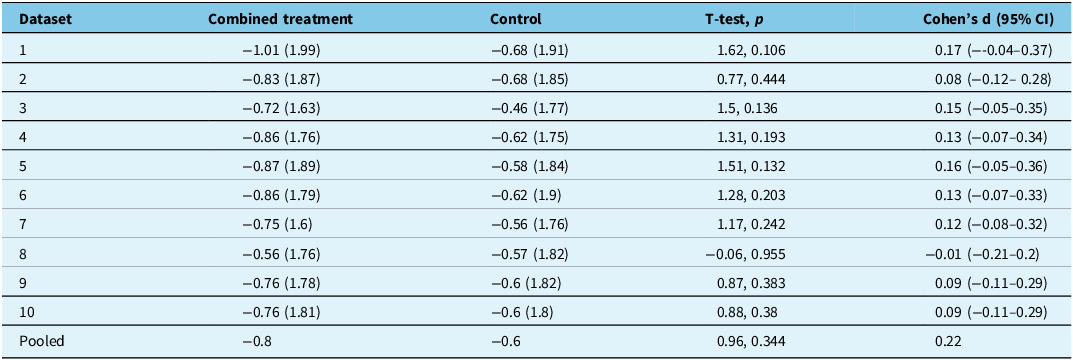
Table 5 shows the mean change scores between baseline and post-treatment on maximum headache intensity for combined treatment and control group in each imputation dataset. Almost all these differences as well as the pooled difference were not statistically significant (−0.8 points vs. −0.6 points, p = 0.34).
Intention-to-treat sample: Effectiveness of self-guided Internet-based treatment versus waitlist control. Mean change scores (SD) from baseline to treatment on maximum headache intensity and corresponding t-tests and Cohen’s d for each imputation

Completers analysis
Of those who completed the EHD (n = 221), a greater percentage of participants in the combined treatment group versus the control group met the primary outcome (24/108, 22.2% vs. 13/113, 11.5%, p = 0.047). There was no difference in mean change in maximum headache intensity in the combined treatment group versus the control group (−0.5 points vs. −0.7 points, p = 0.381).
Comparison between the two iCBT groups
Intention-to-treat analyses
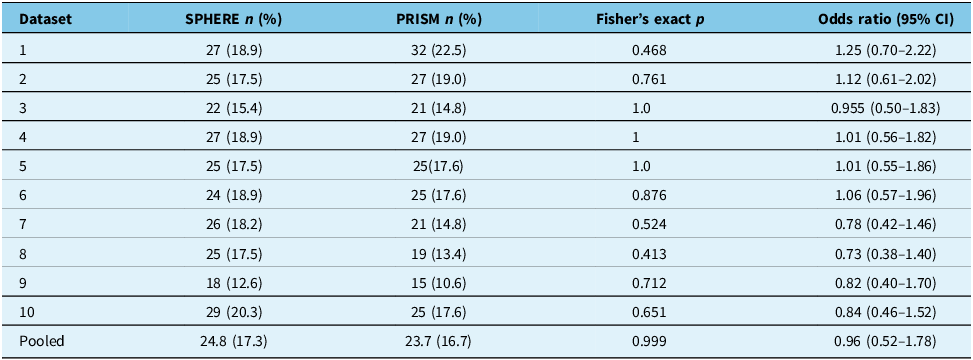
Table 6 shows the percentage of participants allocated to PRISM and SPHERE who achieved at least a 50% reduction in headache days across 10 imputations. Fisher’s exact tests show a consistent pattern indicating no difference between the treatment groups (SPHERE: 17.3% vs. PRISM: 16.7%, p = 0.99).
Intention-to-treat sample: Effectiveness of PRISM versus SPHERE. Imputed percentage and counts of participants achieving a 50% reduction of headache days and corresponding Fisher’s exact test and odds ratios for each imputation

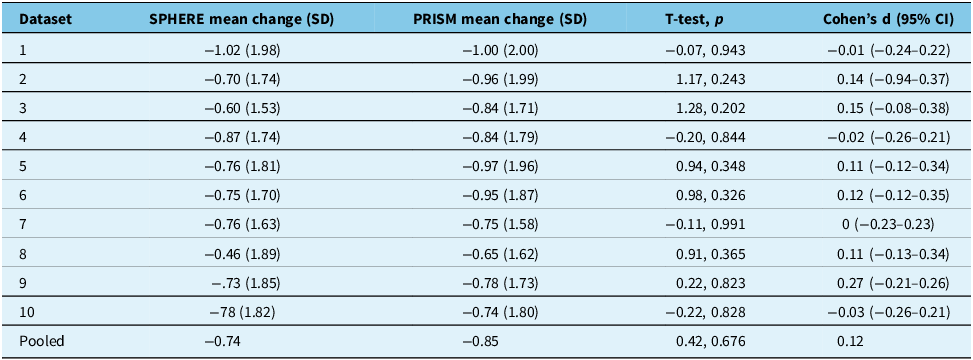
None of the differences in estimated change scores from baseline to post-treatment on maximum headache intensity either for each imputation or the pooled difference was found to be statistically significant. See Table 7.
Intention-to-treat sample: PRISM versus SPHERE. Mean change scores (SD) from baseline to treatment on maximum headache intensity and corresponding t-tests and Cohen’s d for each imputation

Exploratory outcomes (intention-to-treat analyses)
Comparison between Internet-based treatment (combined treatment groups) and control
There was a significant decrease in MIDAS scores from baseline to post-treatment (F = 28.05, p < 0.001) among all participants, but no significant difference between combined treatment and control (F = 0.7, p = 0.402).
There was no change in CES-D scores between baseline and post-test and no significant group by time interaction (F = 1.88, p = 0.171 and F = 0.002, p = 0.964, respectively).
Comparison of the two Internet-based treatments
All participants showed an overall decrease in the transformed MIDAS scores from baseline to post-treatment (F= 13.10, p < 0.001). Also, participants allocated to SPHERE showed a statistically significant decrease compared with participants allocated to PRISM (F = 4.48, p = 0.036).
There was no evidence of statistically significant change in CES-D scores between baseline and post-treatment (F = 1.11, p = 0.294) nor a group by time interaction (F = 0.03, p = 0.868).
Interventions usage
Among SPHERE participants (n = 143), 33 (23.1%) never logged in, and those who logged in at least once (n = 110, 76.9%) completed an average of 4.05 modules (SD = 5.67). When a module that includes “practices” was completed, on average, 20.13% of users completed the “practices.” The percentage of participants who completed at least 50% of modules was 19.01% (21/110), and the percentage of participants who completed all the 17 modules out of those who logged in at least once was 10.91% (12/110). Figure 2 shows the percentage of participants who completed each module.
Percentage of participants completing each module out of those who logged in to SPHERE at least once.

Among PRISM participants (n = 142), 26 (18.31%) never logged in, and those who logged in at least once (n = 116, 81.69%) made an average of 26.94 diary entries (SD = 31.94) over the 4-month period. Among the 116 participants users who logged in at least once, they entered an average of 8.27 headache episodes (SD = 9.08) and an average of 22.63 exposures to potential triggers that they were interested in exploring (SD = 40.06). Sixty participants (51.72% out of the 116) entered at least 5 headaches, which was the minimum required number of episodes that needed to be tracked for PRISM to start to analyze data and look for relationships between users’ headaches and possible triggers. Among the 116 participants users who logged in at least once, PRISM identified a potential trigger (either single or a combination) for 17 of them (14.65%). Nine out of the 17 users (52.94%) who were informed about their potential triggers and received recommendations selected a recommendation and committed to it by setting at least one goal. After this, each of these 9 users tracked for an average of 22.11 days (SD = 19.73) or a median of 16 days whether they have achieved or not that goal, and during an average of 37 days (SD = 15.67) and median of 16 days, they reported that they had reached their goal.
Satisfaction with the interventions
The mean CSQ-8 score for participants assigned to SPHERE was 23.84 (SD = 4.37, n = 59). Twelve participants (20.3%) reported low satisfaction, 35 (59.3%) reported intermediate satisfaction and 12 (20.3%) reported high satisfaction.
The mean CSQ-8 score for participants assigned to PRISM was 23.44 (SD = 4.87, n = 63). Eighteen participants (28.6%) reported low satisfaction, 28 (44.4%) reported intermediate satisfaction and 17 (27%) reported high satisfaction.
Discussion
The purpose of this study was to compare the effectiveness of two iCBT interventions against a waitlist control and to describe uptake, adherence and satisfaction with the interventions. Results did not show clinically significant reductions in headache days, which was our primary measure of outcome when performing ITT analyses, although analysis with completers showed that both iCBT programs were superior to the control condition. Despite the two CBT interventions being quite different, we found the differences in outcomes were not different statistically.
Four published RCTs have investigated the effect of iCBTs in adults with migraine against waitlist/treatment as usual; Reference Sorbi, Kleiboer, van Silfhout, Vink and Passchier31–Reference Hedborg and Muhr34 only one of them evaluated the effect on clinically meaningful reductions in headache days and showed that the intervention was effective after following participants for 11 months. Reference Hedborg and Muhr34 Due to the lack of data and lack of consistent results, it is still premature to draw firm conclusions about the efficacy of the self-guided Internet interventions. Further studies with longer follow-ups are needed.
The results on all prespecified secondary outcomes and exploratory outcomes were consistent with the primary result. The interventions did not have a significant effect on reducing maximum headache intensity, disability or depression. Our findings are consistent with research examining the effect of interventions on headache intensity Reference Sorbi, Kleiboer, van Silfhout, Vink and Passchier31,Reference Kleiboer, Sorbi, van Silfhout, Kooistra and Passchier33 and disability. Reference Sorbi, Kleiboer, van Silfhout, Vink and Passchier31–Reference Kleiboer, Sorbi, van Silfhout, Kooistra and Passchier33 There have been inconsistencies in the effect on depression. Reference Bromberg, Wood, Black, Surette, Zacharoff and Chiauzzi32
The uptake rates of both interventions were high, but levels of adherence to the interventions were low, and the non-completion rate of the primary outcome in our trial was higher than the anticipated 40% in the trial design. Varied levels of uptake and low adherence to the interventions and study protocols are characteristic of trials of Internet interventions, Reference Crutzen, de Nooijer, Brouwer, Oenema, Brug and de Vries35,Reference Ryan, Bergin and Wells36 especially self-guided ones. Reference Richards and Richardson37 Plausibly, the low adherence to the interventions could be the primary reason for not achieving statistically significant improvements in the primary outcome. Reference Glenn, Golinelli and Rose38 Participants may have found a novel treatment modality appealing at first but may have dropped out due to factors that prevented them from sustaining engagement with intervention or successfully responding to treatment (e.g., baseline symptom severity and overall impairment, Reference Devineni and Blanchard39,Reference Ström, Pettersson and Andersson40 lack of immediate consequences and rewards, suboptimal cues to action within the intervention, lack of human guidance within the intervention Reference Musiat, Johnson, Atkinson, Wilksch and Wade41 and amount of data entry required, especially for PRISM). Reference Michie, Johnston and Abraham42 Others may have decided they no longer needed the interventions after experiencing improvement in symptoms. Reference Szafranski, Smith, Gros and Resick43
Moreover, consistent with other health behavior change trials, we found baseline symptom severity to be related with levels of attrition. Reference Devineni and Blanchard39,Reference Ström, Pettersson and Andersson40 We also found differential attrition where participants in the treatment group (i.e., combined iCBT) were much more likely to drop out than the inactive control group. Reference Crutzen, Viechtbauer, Spigt and Kotz44 Differential attrition could be because of the greater effort required to participate in the treatment arms. An additional contributing factor may have been the additional incentive of participants assigned to the control group after the completion of the post-randomization assessment, which was absent in the treatment groups, as the control group could gain access to the treatment of their choice after completing the assessment.
Due to the paucity of adherence and attrition research of Internet-delivered treatment, there are substantial gaps in the knowledge needed to inform modifications in future interventions to optimize uptake and adherence and ultimately realize improved outcomes. Strategies that influence patient-, intervention- and system-level factors related to patient engagement Reference Sorbi, Kleiboer, van Silfhout, Vink and Passchier31 (e.g., offering clinical guidance or coaching for motivational support, using more persuasive design features, using higher financial incentives and embedding interventions in existing service structures such as clinics) are being actively investigated in eHealth research Reference Crutzen, de Nooijer, Brouwer, Oenema, Brug and de Vries35,Reference Borghouts, Eikey and Mark46,Reference Gan, McGillivray, Larsen, Christensen and Torok47 and should be applied to iCBT interventions for headaches. With those additional supports in place, PRISM and SPHERE should be tested again to determine the effectiveness of these strategies. Advancement in iCBT in the context of headaches is still uncertain since limited research has been done on this population. Reference Andersson, Lundström and Ström48 However, high levels of initial uptake from young adult participants in this study and growing scientific interest in digital therapeutics Reference Chen and Luo49 generally suggest that self-managed iCBT for migraine remains an important question for future research.
Strengths, limitations and gaps
The strengths of this study included the randomized design, the large sample size, well-specified preplanned analyses and the use of rigorous outcomes in accordance with the recommendations by the American Headache Society and the International Headache Society guidelines. Reference Penzien, Andrasik and Freidenberg13
This study had several limitations. First, there was substantial attrition and differential attrition between intervention and control groups. We sought to balance groups post hoc through multiple imputation methods, but these methods may have introduced bias. Moreover, since the attrition was larger than expected, our study did not have adequate power when conducting completers-only analysis. Second, we did not conduct follow-ups longer than 4 months post-randomization. Future studies should examine longer-term outcomes. Third, most participants were recruited from the online community, and the results may not be generalizable to healthcare settings. Fourth, it was not possible to blind participants, which could have produced biased findings. Reference Pitre, Kirsh and Jassal50 Fifth, a wide age range was selected for this study, including adolescents and adults up to 40 years. However, the low number of adolescents made it not possible to determine the extent to which the results were applicable to the younger age groups. Sixth, following guidelines for controlled trials of behavioral treatments, Reference Penzien, Andrasik and Freidenberg13 we established achieving a 50% reduction in headache days as the primary treatment outcome. However, it may be difficult to reach this target with non-pharmacological interventions alone. Reference Luedtke, Basener and Bedei51 Future studies may need to look at a more modest reduction in headache days (e.g., 30%) or assess a different outcome as the primary outcome (e.g., disability). Reference Luedtke, Basener and Bedei51 Finally, participants assigned to the control group could have sought some form of treatment during the course of this study since it would have been unethical to deny those participants access. Consequently, the control group could have not been a true control.
We used a three-arm trial because CBT is not a uniform treatment. The differential effectiveness of iCBT using different techniques and strategies remains uncertain. It is important to compare and contrast iCBT programs to better understand whether a simplified or more complex (e.g., tailored or personalized) iCBT program works better and what needs to be done to optimize treatment.
Conclusions
It is unclear whether self-guided iCBT could help reduce the number of headache days in individuals with migraine. Further improvements and new trials will help us address treatment adherence, reduce dropouts, assess longer-term impacts and better tailor interventions to the needs of the patients.
Author contributions
AH conceived and designed the study, obtained necessary approvals, supervised data collection, had co-supervision of the overall coordination of the study and drafted and revised the manuscript for intellectual content. SR was involved in obtaining necessary approvals, data collection and edited the manuscript. BC and MM provided expert opinions regarding data analysis, conducted analyses and revised the manuscript for intellectual content. PJM contributed to the study conception and design of the study, had co-supervision of the overall coordination of the study and revised the article for intellectual content. All the rest of the authors revised the manuscript for intellectual content.
Funding statement
This work was supported by the Nova Scotia Health Research Foundation (Establishment Grant) and Canadian Institute of Health Research (Operating Grant, competition: 201309).
Competing interests
None.



 Open access
Open access