The definition of the metabolic syndrome (MetS) in children and adolescents, according to the International Diabetes Federation (IDF)(1), is based on a high waist circumference associated with two or more abnormal parameters: glycaemia, blood pressure, TAG and HDL-cholesterol.
The prevalence of the MetS(Reference Moraes, Fulaz and Netto-Oliveira2) in children over 4 years old and adolescents ranged from 2·2 to 52·1 % in a review including sixteen studies conducted in America, Europe and Asia(Reference Moraes, Fulaz and Netto-Oliveira2). In another review, including thirteen studies conducted in Iran, this prevalence varied from 1·0 to 22 %(Reference Kelishadi, Hovsepian and Djalalinia3). This great range of variation could be due to the differences in diagnostic and also because the MetS is a multi-causal disease that enrols genetic and environmental factors, such as a sedentary lifestyle, stress levels and food habits(Reference Kaur4). The MetS individuals usually present a pro-thrombotic/inflammatory status, where oxidative stress promotes a series of metabolic changes: central obesity leads to insulin resistance, hyperglycaemia, hypertriacylglycerolaemia, high LDL-cholesterol and low HDL-cholesterol concentration(Reference Grundy, Cleeman and Daniels5–Reference Zheng, Zhou and Huang12).
Se is an essential trace element that composes several selenoproteins(13,Reference Hariharan and Dharmaraj14) . The daily intake of Se is recommended for maintaining homoeostasis in the human body(Reference Hariharan and Dharmaraj14). Se deficiency could lead to inflammatory status(Reference Duntas and Benvenga15,Reference Spina, Guallar and Rayman16,Reference Bleys, Navas-Acien and Stranges17) , being associated with the MetS. It is an enzymatic cofactor in different metabolic processes, such as in activities related to cellular inflammation and lipid peroxides(13,Reference Hariharan and Dharmaraj14) – although it is not clear how Se affects our biological functions(Reference Benstoem, Goetzenich and Kraemer18). Studies on its association with chronic non-communicable diseases, CVD and the MetS had conflicting results(Reference Benstoem, Goetzenich and Kraemer18).
The increase in non-communicable diseases and the metabolic changes cited above have been associated with unhealthy life habits: less physical activity, more sedentary activities and replacement of fresh food by ultra-processed food products – dietary pattern related to nutrient-poor diet(19). Studies investigating Brazilian adolescents’ diet(Reference de Almeida Alves, Retondario and Bricarello20,Reference Souza, Barufaldi and Abreu21) found a high intake of traditional Brazilian food such as beans, rice and meat and, at the same time, a high intake of unhealthy food, sugar through sweetened beverages and processed foods(Reference de Almeida Alves, Retondario and Bricarello20,Reference Souza, Barufaldi and Abreu21) . Thus, the MetS treatment involves lifestyle changes to control body weight and to reduce chronic inflammation(Reference Huang22,23) .
Taking into account that the relationship between Se and non-communicable diseases, CVD and the MetS is not clear in the literature, the increasing prevalence of these outcomes in early life and adolescence, and the lack of studies conducted in middle-income/developing countries – where the Se intake can have a considerable variability – this article aimed to investigate the association between the dietary Se intake and the MetS or its parameters (high waist circumference, hyperglycaemia, high blood pressure, high TAG and low HDL-cholesterol) in the Study of Cardiovascular Risks in Adolescents (ERICA), a large probabilistic and representative sample of Brazilian adolescents.
Materials and methods
This research is part of the ERICA study. ERICA is a Brazilian national cross-sectional multicentre school-based study, conducted between 2013 and 2014 in all of the twenty-six Brazilian States and Federal District, in both rural and urban areas. The ERICA protocol, design, rationale, sample and data collection are described in other studies(Reference Bloch, Szklo and Kuschnir24,Reference Vasconcellos, Silva and Szklo25) . The sampling was developed using a multistage design, and considering an expected prevalence of the MetS in 4 % adolescents of, a maximum estimation error of 0·9 %, a 95 % confidence level and a design effect of 2·97 due to school clustering(Reference Vasconcellos, Silva and Szklo25). The total sample of the ERICA study reached more than 70 000 adolescents between 12 and 17 years of age, from both public and private schools, attending morning and afternoon school. Because of the need for 12 h of fasting, only morning students participated in the blood sample collection. In this way, the inclusion criteria of this paper were adolescents from the ERICA study with complete data on their dietary intake, anthropometry and biochemical analyses, reaching 39 956 adolescents. Adolescents with a total energy intake of < 1,673·6 kJ/d (400 kcal/d) or > 33,472·0 kJ/d (8000 kcal/d) (388 subjects) were excluded from the analyses(Reference Zhang, Wang and Wang26), with 39 568 adolescents in total. More details of response rate in the ERICA study can be found in Silva et al. (Reference Silva, Klein and Souza27). Data used in this research are briefly described below.
Data collection and interpretation
Social and demographic data (sex, age, type of school and country region) were collected by a self-administered questionnaire using a personal digital assistant (PDA), LG GM750Q® model(Reference Bloch, Szklo and Kuschnir24). Age was classified into two groups: 12–13 years old and 14–17 years old due to Se intake recommendations(13); afterwards, adolescents were classified according to the type of school (public or private) and school location (urban or rural area).
Dietary intake data were collected by 24-h recall (24hR) applied for the entire sample. This tool was applied using the ERICA-REC 24 h – a software developed specifically for the present study. Interviewers were trained to use the software by applying the multiple-pass method(Reference Conway, Ingwersen and Vinyard28) to minimise memory bias. To convert food into nutrients, the ERICA-REC 24 h contains a list of foods commonly consumed in Brazil(29). Foods reported by the adolescents that were not found in the software list were added by the interviewers. In a random subsample of two students per class (about 7 % of total sample), a second 24hR was applied to allow within-person variability adjustment. This procedure was based on the guidelines of the National Cancer Institute pointing the use of a 24hR on the whole sample and a second one on a subsample as acceptable, since the subsample size is large enough(30). Se intake (exposure variable) obtained from the first 24hR was adjusted for within-person variability in the second 24hR(Reference Freedman, Guenther and Dodd31), according to the National Cancer Institute guidelines. The use of Se supplementation was not investigated.
Our trained staff (a field team, trained to collect data) measured anthropometric data with the adolescents not wearing shoes and dressed in light clothing, using standard procedures(Reference Lohman, Roche and Martorell32). Weight was measured once, using an electronic digital scale (Líder® P150 m), with 200 kg of capacity and 50 g of precision. Height was measured twice using a stadiometer (Alturexata®), and the result was the mean calculated through the PDA. Differences higher than 0·5 cm between the two measures were not considered. In this way, BMI was calculated (kg/m2) to be used in the statistical model (proxy of energy intake(Reference Willett and Willet33)).
The outcome variables were the MetS and its parameters: high waist circumference, high blood pressure, high glycaemia, high TAG and low HDL-cholesterol. Waist circumference was collected using an inelastic tape of fibreglass (Sanny®), 1·5 m long and a 1 mm line spacing. Two sequential measurements were taken in the halfway point between the iliac crest and the last rib. Adolescents were erect, with their abdomen relaxed, in expiratory apnoea. Results were registered directly on the PDA, which calculated the mean value considered for the analyses. Differences greater than 1·0 cm were not considered and, therefore, new measurements were required. Waist circumference was classified as adequate (lower than p90 for adolescents between 12 and 15 years old and/or lower than 90 cm for boys or lower than 80 cm for girls between 16 and 17 years old) or inadequate or high (equal to or higher than p90 for adolescents between 12 and 15 years old, and/or equal to or higher than 90 cm for boys or higher than 80 cm for girls between 16 and 17 years old(1)).
Blood pressure measurement was conducted in two stages. First, the right arm circumference of adolescents was measured with the Sanny®’s inelastic measuring tape on the halfway point between the acromion and olecranon to choose the correct cuff(Reference Bloch, Szklo and Kuschnir24,Reference Lohman, Roche and Martorell32) . Results were registered on the PDA. When accessing the device to register blood pressure, it showed the appropriated cuff size in the display. Next, blood pressure was measured using an Omron® 705-CPINT digital monitor, tested for the same age group(Reference Stergiou, Yiannes and Rarra34). Blood pressure was measured with the adolescents sitting down, leaning on the backrest, feet on the floor and right arm extended with the antecubital fossa at heart level. After a 5-min rest, three measurements were taken with the intervals of 3 min between them(Reference Bloch, Szklo and Kuschnir24). The results were registered directly on the PDA, ignoring the first values and calculating the mean between the last two values. Blood pressure was classified as adequate (systolic blood pressure lower than 130 mmHg and/or diastolic blood pressure lower than 85 mmHg) or inadequate/hypertensive (systolic blood pressure equal to or higher than 130 mmHg and/or diastolic blood pressure equal to or higher than 85 mmHg(1)).
For the collection of blood, adolescents were fasting from 12 to 14 h and asked about medicines, current health problems and how they slept the night before. Answers were typed directly on laptops. Four tubes were collected per adolescent. Blood samples were processed in local labs to separate serum from plasma and stored at 0–10°C until being flown to the reference lab in which the analyses were conducted(Reference Bloch, Szklo and Kuschnir24). Biochemical analyses were conducted to investigate fasting glucose (by the hexokinase method(35)), TAG (by the kinetic enzymatic method(Reference Xavier, Izar and Faria Neto36)) and HDL-cholesterol (by the enzymatic colorimetric method(Reference Xavier, Izar and Faria Neto36))(Reference Cureau, Bloch and Henz37). Glycaemia was considered adequate when it is lower than 100 mg/dl; TAG were considered adequate when lower than 150 mg/dl and HDL-cholesterol was classified as adequate when equal to or higher than 40 mg/dl for boys of any age and for girls between 12 and 15 years old, and equal to or higher than 50 mg/dl for girls between 16 and 17 years old(1).
The MetS was classified according to the most recent IDF definition for children and adolescents at the time of this study(1): high waist circumference associated with two or more abnormal parameters: glycaemia, blood pressure, TAG and/or HDL-cholesterol. The risk of developing CVD and type 2 diabetes mellitus increases according to the increase in the number of the MetS parameters(Reference Andreadis, Tsourous and Tzavara38). In this way, individuals were classified according to the number of the MetS parameters, from individuals with zero to individuals with the five parameters.
Theoretical model and statistical analyses
Confounders were defined based on a theoretical model proposed according to the causal graph theory(Reference Glymour, Greenland, Rothman, Greenland and Lash39), which are directed acyclic graphs drawn to show causal process hypothesis(Reference Cortes, Faerstein and Struchiner40). The theoretical model is presented in Fig. 1.
Theoretical model of analysis.

In Fig. 1, a dashed line links the association between Se intake (exposure variable) and the MetS (outcome variable). Dark grey variables (BMI, sleep duration, smoking, physical activity, alcohol consumption, screen time, waist circumference, age and sexual maturation) represent associated factors such as sex, family income and energy intake. Type of school (public or private) is being used as a proxy of family income, because income was a variable with a lot of missing data. BMI Z-score was used as a proxy of energy intake in adjustment(Reference Willett and Willet33,Reference Rouhani, Haghighatdoost and Surkan41,42) . Socio-economic factors, such as family income, have an important role in the environment in which people live, their lifestyle and, consequently, their health(Reference Beenackers, Kamphuis and Giskes43). In the theoretical model, type of school (public or private) is being used as a proxy of family income. Eating habits (such as energy intake), physical activity, sedentary lifestyle/screen time and sleep duration could be risk factors to obesity, hyperglycaemia and dyslipidaemia(44,Reference Abreu, Barufaldi and Bloch45,Reference Boucher, Adesanya and Owei46,Reference D’Aniello, Troisi and D’Amico47,Reference Nguyen, Pham and Lee48,Reference Kang, Wang and Cheon49,Reference Theorell-Haglow and Lindberg50) . Given the fact that there are no data related to energy intake for the entire sample in the 2 d, the BMI was used as a proxy of energy intake in the adjustment(Reference Willett and Willet33,Reference Rouhani, Haghighatdoost and Surkan41,42) . Obesity, smoking, alcohol consumption, bad eating habits, lack of physical activity, sedentary lifestyle and no enough sleep may also represent risk factors to hypertension development(44,Reference Chen, Smith and Harbord51,Reference Fava, Sjogren and Montagnana52,Reference Guo, Zheng and Wang53) . Those are behaviour variables that interact with each other. On the other hand, sex, age and sexual maturation are individual factors associated with the MetS(44,Reference Hajian-Tilaki54,Reference Reinehr55) .
There is confounding when exposure and outcome share one or more than one common causes(Reference Glymour, Greenland, Rothman, Greenland and Lash39,Reference Cortes, Faerstein and Struchiner40) . In this way, we can see in the theoretical model that white variables (family income and energy intake) are associated with both the MetS and Se intake and, therefore, are included in the minimal model of analyses as confounders. By controlling both family income and energy intake, it is possible to block all the back-door paths and, therefore, control the model(Reference Glymour, Greenland, Rothman, Greenland and Lash39,Reference Cortes, Faerstein and Struchiner40) . The light grey variable (soil Se content) is associated with the Se intake(Reference Ortuño, Ros and Periago56); it, however, could not be measured in this study.
All analyses were performed using the SAS® statistical software 9.4 (Statistical Analysis System). Sample characteristics are presented as prevalence with a 95 % CI. Se intake is presented as median intake (µg) and interquartile interval (p25–p75) for the entire sample, as well as by sex and country region. Sample outcome characteristics are presented as prevalence, and 95 % CI by sex, type of school and country region.
Logistic regression was applied to investigate the association between Se intake and outcomes. We used p10 and p90 values from Se intake distribution as default, and the presence or absence of the MetS, high TAG, high waist circumference, low HDL-cholesterol, high glycaemia and high blood pressure. We adjusted the model for nutritional status (Z-score) and type of school, according to the theoretical model (Fig. 1). All regression results are shown as OR and P-value, stratified by sex. Only variables with P < 0·05 were considered statistically significant. Sample weight and complexity of sample design were taken into account, applying the replication technique called Fay-modified Balanced Repeated Replication(Reference Barbosa, Sichieri and Junger57).
Ethical considerations
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Ethical Committee of the Federal University of Rio de Janeiro (Code #01/2009, Process #45/2008). The approval of the Ethical Committees of each State and Federal District was also obtained. The study includes only the students who signed the consent form, which was also signed by their parents.
Results
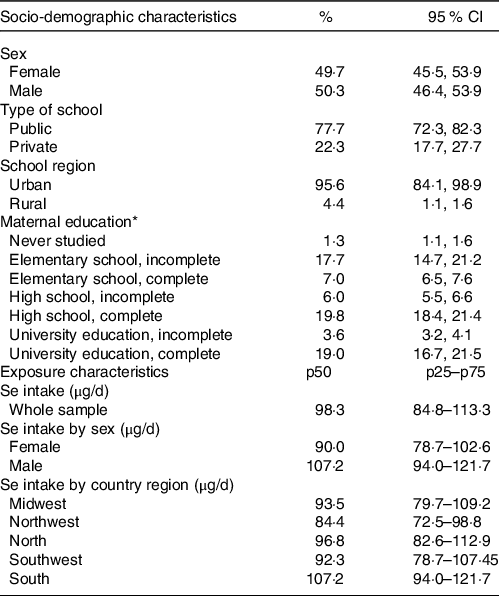
This study included 39 568 adolescents between 12 and 17 years old. Sample socio-demographic and exposure characteristics are shown in Table 1, while outcome-related information is presented in Tables 2, 3 and 4.
Sample socio-demographic and exposure characteristics
(Percentages and 95 % confidence intervals)

p25–p75, interquartile interval.
* 28 794 responses (22·23 % of missing data).
The outcomes by sex and type of school
(Mean values and 95 % confidence intervals)

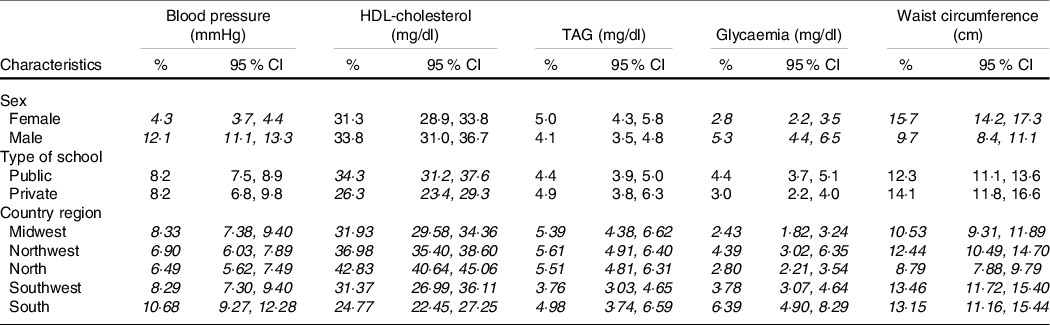
The prevalence of the abnormal levels of the metabolic syndrome parameters and 95 % confidence interval, by sex, type of school and country region*
(Percentages and 95 % confidence intervals)

* Italic variables indicate statistically significant difference between/among groups.
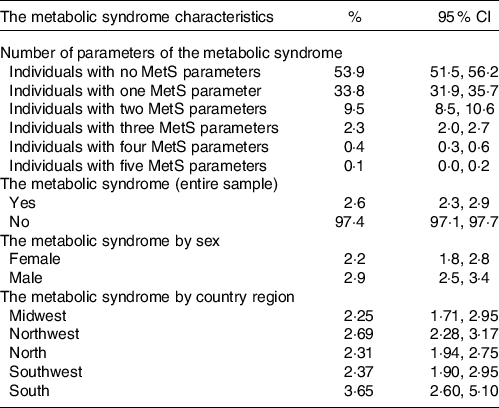
Distribution of the number of the metabolic syndrome parameters and the metabolic syndrome prevalence, according to the number of parameters and by sex and country region
(Percentages and 95 % confidence intervals)

Most of the participants were from public schools (77·7 %) and urban areas (95·6 %). The median Se intake was 98·3 µg/d for the entire sample, with no statistical differences between sexes and among country regions.
On average, mean values were normal according to the MetS classification for all the parameters. Hypertension and hyperglycaemia were statistically more prevalent among boys, while high waist circumference was higher among girls. All prevalence of the MetS parameters presented statistical differences among country regions. Regarding the entire sample, 46·1 % of adolescents have one or more MetS parameters. Concerning the MetS as main outcome, its prevalence was 2·6 % and was higher among boys. No statistical differences were found between sexes or among country regions.
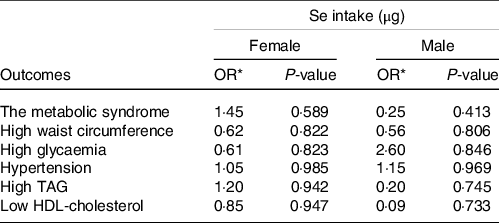
We found no association between the MetS or its parameters and Se intake for both female and male groups (Table 5), as well as in the country regions (data not shown).
Logistic regression for the metabolic syndrome or its parameters and Se intake by sex
(Odds ratios)

Se intake, selenium intake.
* Adjusted for BMI Z-score by sex (as energy intake proxy) and type of school (as family income proxy), according to the theoretical model.
Discussion
This study aimed to investigate the association between the dietary Se intake and the MetS or its parameters in a large probabilistic and representative sample of Brazilian adolescents. Main results show that Se intake was not statistically associated with the MetS and its parameters. Results demonstrate statistical differences between sexes for the prevalence of hypertension, hyperglycaemia and high waist circumference.
Daily median Se intake was higher than dietary recommendations(13). A study developed with the ERICA database found an adequate Se intake among adolescents by applying the estimated average requirement) cut-off method, although differences between sexes and age groups were found(Reference Retondario, Souza and Fernandes58). In this way, for Brazilian adolescents, the Se intake values found in this study seem to be sufficient to meet their nutritional needs. Other studies conducted with Brazilian adolescents found diverse results. A population-based study conducted with adolescents between 14 and 18 years old found Se intake values higher than the ones found in this study (p50 was 106·0 µg for girls and 129·0 µg for boys), concluding that Se intake among adolescents in Brazil is adequate(Reference Verly Junior, Cesar and Fisberg59). On the other hand, a study conducted with adolescents from public schools in a Northeastern city in Brazil found much lower values(Reference Falcão, Lyra and Morais60). Falcão et al. found median values ranging from 25·2 to 28·4 µg for boys and from 24·1 and 24·5 µg for girls, concluding that there is a high prevalence of inadequate Se intake in this region(Reference Falcão, Lyra and Morais60). Known natural sources of dietary Se are mushrooms, Brazil nuts, broccoli, cereals, breads, millets, wheat, nuts and meats(Reference Banuelos, Zhi-Qing and Xuebin61), but Se levels depend on soil composition(Reference Silva Junior, Wadt and Silva62). An investigation involving more than 70 000 Brazilian adolescents found that the main dietary sources of Se for this age group were meat, pasta, poultry and fish(Reference Retondario, Souza and Fernandes58), probably because of their dietary habits.
A higher prevalence of hypertension in boys (12·1 %) in relation to girls (4·3 %) was found. Although hypertension is a disease which could be developed by both males and females, a systematic review and a meta-analysis on Brazilian studies observed a higher prevalence in boys (9·3 %), with a lower prevalence in girls (6·5 %)(Reference Gonçalves, Galvão and Andrade63).
Data also showed differences in low HDL-cholesterol prevalence according to the type of school. Studies conducted with adolescents did not discuss this issue. However, studies conducted with adults worldwide have found divergent results on the association between HDL-cholesterol and deprivation(Reference Rouvre, Vol and Gusto64), whereas an inverse association has been described for men from China, Poland and Russia(Reference Perova, Davis and Tao65), and women from Sweden(Reference Wamala, Merlo and Bostrom66); in the USA, however, it seems to be directly associated with white men(Reference Perova, Davis and Tao65).
Glycaemia prevalence was statistically higher for boys, while waist circumference was higher for girls. These findings concerning glycaemia agree with some studies. Bang(Reference Bang67) investigated the prevalence and related factor of the MetS in 404 Korean adolescents between 12 and 18 years old and found elevated fasting glucose in 7·8 % of the sample, which is higher among boys. In the same way, Agredo-Zúñiga et al. (Reference Agredo-Zuniga, Aguilar-de Plata and Suarez-Ortegon68) assessed the association between waist:height ratio and cardio-metabolic risk in 1672 children and adolescents between 10 and 17 years old in Colombia, in which boys had a higher prevalence of hyperglycaemia than girls. Benmohammed et al. (Reference Benmohammed, Valensi and Balkau69) investigated the MetS and its parameters in 1100 adolescents between 12 and 18 years old and observed the same difference between sexes.
However, some other researchers found no difference between sexes. Rodrigues et al. (Reference Rodrigues, Perez and Pires70) assessed the occurrence of the MetS and associated risk factors in 380 Brazilian adolescents between 10 and 14 years old attending public schools and found no differences between sexes for fasting glucose. The same happened with Beck et al. (Reference Beck, Lopes and Giuliano71) while investigating risk factors for CVD in 660 adolescents between 14 and 19 years old in a municipality in Southern Brazil. In the same way, Quadros et al. (Reference Quadros, Gordia and Silva72) investigated the prevalence of dyslipidaemia, high blood glucose and high blood pressure in 1139 schoolchildren between 6 and 18 years old in a municipality in Northwest Brazil and found no differences between sexes.
Findings on waist circumference corroborate with studies in which excess abdominal fat was more prevalent in girls, such as the abovementioned study by Beck et al. (Reference Beck, Lopes and Giuliano71) and Hu et al. (Reference Hu, Huang and You73), which aimed to assess the prevalence of abdominal obesity in a cross-sectional study conducted in China with 15 364 fifteen-year-old adolescents. However, our results differ from other studies. Bang(Reference Bang67), when investigating Korean adolescents between 12 and 18 years old, found a higher waist circumference for boys. Similarly, Fernandes et al. (Reference Fernandes, Rosa and Silva74) found a higher waist circumference for boys when investigating abdominal obesity and excess of body fat in 807 adolescents between 11 and 17 years old in Brazil. Other studies, on the other hand, found no differences between sexes, such as the aforementioned studies by Benmohammed et al. (Reference Benmohammed, Valensi and Balkau69) and MacPherson et al. (Reference MacPherson, de Groh and Loukine75), which investigated the prevalence of the MetS and its risk factors in 1228 Canadian children and adolescents between 10 and 18 years old.
The global risk associated with the MetS depends on the number of parameters affecting people(Reference Andreadis, Tsourous and Tzavara38). It was found that 46·1 % of the entire sample have mild MetS (one or more parameters), and that 0·5 % have severe MetS (four or more associated parameters)(Reference El Brini, Akhouayri and Gamal76). In our sample, 77·7 % of the subjects were from public schools. A study conducted with data from the ERICA study found that adolescents from public schools have higher chances of having less healthy eating habits than those from private ones(Reference Barufaldi, Abreu Gde and Oliveira77), which could lead to central obesity – the main parameter of the MetS. Considering adolescence as a window of opportunity to prevent non-communicable diseases related to nutrition in adulthood(78), these findings highlight the need to pay attention to preventive and corrective measures to prevent and/or reduce risk factors.
The MetS prevalence was low (2·6 %) and could be explained by the MetS definition proposed by the IDF, which requires the presence of high waist circumference to classify the individuals as the MetS patients(Reference Kuschnir, Bloch and Szklo79). In a small study performed with adolescents (n 241) from public and private schools in a Brazilian city(Reference Guilherme, Nascimento and Molena-Fernandes80), the MetS prevalence ranged from 1·7 % (95 % CI 0·0, 3·3), using the IDF definition, to 17·4 % (95 % CI 12·6, 22·3), using a definition based on the National Cholesterol Education Program-Adult Treatment Panel III criteria, modified for children and adolescents(Reference de Ferranti, Gauvreau and Ludwig81). Another study(Reference Vanlancker, Schaubroeck and Vyncke82), enrolling adolescents (n 1004) from the Healthy Lifestyle in Europe by Nutrition in Adolescence study, compared the prevalence of the MetS using different definitions for this population. The prevalence of the MetS in this study varied from 1·6 to 3·8 % depending on the used definitions, and it was 2·7 % when they used the IDF definition(Reference Vanlancker, Schaubroeck and Vyncke82). Although we have no consensus to support the choice of definition to be used, using a more specific one has been reported as more appropriate(Reference Kuschnir, Bloch and Szklo79).
No association between the dietary Se intake and the MetS or its parameters was found. To the best of our knowledge, this is the first study conducted with adolescents to investigate this association. Therefore, we will discuss these findings, comparing them with studies carried out with different samples and populations. Our results corroborate an interventional study conducted in France, as well as two other Chinese studies – all of them were carried out with adults(Reference Czernichow, Vergnaud and Galan83,Reference Bian, Gao and Zhang84,Reference Li, Guo and Wu85) . However, an Iranian study investigated this association for both men and women between 35 and 65 years old and found that a higher Se intake was associated with a lower prevalence of the MetS(Reference Motamed, Ebrahimi and Safarian86). This study applied IDF definition to classify the MetS subjects, which is a similar definition as the one applied in this study (but for adults). Nonetheless, unlike the method applied in our study, the Iranian researchers used a single 24-h dietary recall, whereas Se intake means were directly compared between groups with and without the MetS. The adjustment made with the second 24hR brings a less biased result regarding nutrient intake to our study, which should result in findings that are closer to the actual intake(30).
In the same way, a Chinese study conducted with both men and women between 18 and 84 years old found that higher Se intake was associated with a lower prevalence of the MetS, as well as a lower prevalence of high waist circumference, a lower prevalence of high diastolic blood pressure and a lower prevalence of hyperglycaemia(Reference Wei, Zeng and Gong87). This study applied the American Heart Association Guidelines to define the MetS and used a semi-quantitative FFQ to assess the dietary intake. Costa et al. compared different diagnostic criteria employed to identify the MetS in adolescents and found significant differences among the criteria(Reference Costa, Santos and Goldraich88), making it difficult to compare the prevalence levels found in the studies. Still, in the Chinese study, Se medians were directly compared among quartiles, while we used the National Cancer Institute approach(30).
On the other hand, another Iranian study found that higher intake of a dietary pattern including Se was associated with a higher prevalence of the MetS(Reference Khayyatzadeh, Moohebati and Mazidi89). In this study, the IDF definitions of the MetS were used, which is similar to our study (but for adults), and Se intake was assessed by a single 24-h dietary recall (a more biased choice, as discussed above). The association between the MetS and nutrients was assessed using dietary patterns, in one of which Se was found. Dietary pattern methods are important approaches to investigate how diet composition is related to the outcome of interest(Reference Cutler, Flood and Hannan90). However, since they use an association of dietary components, it is difficult to compare their findings with other studies that investigate isolated nutrients.
Two systematic reviews published in 2015(Reference Tajaddini, Keikha and Razzazzadeh91) and 2018(Reference Retondario, Fernandes and Rockenbach92) found that there are controversies around the association between Se and the MetS parameters (central obesity(Reference Hosseini, Saedisomeolia and Allman-Farinelli93), high blood pressure(Reference Kuruppu, Hendrie and Yang94), high glycaemia(Reference Wang, Yang and Wei95,Reference Vinceti, Filippini and Rothman96) , high TAG and low HDL-cholesterol)(Reference Zhang, Liu and Guo97). Studies investigating the association between the MetS and Se suggest these controversial results may be explained by the U-shaped performance curve of Se intake when considering cardio-metabolic outcomes, when both Se-replete and Se-depleted subjects may be exposed to health damages(Reference Rayman98).
The limitations of this study are related to the measure of food Se content, the 24hR in adolescents and the omitted-variable bias. Food Se content is affected by the Se amount in the soil. Even though a national food composition table(29) was used, Brazil is a continental country and soil Se content varies(Reference Silva Junior, Wadt and Silva62,Reference Moraes, Welch and Nutti99) . Besides, a study on Brazilian nutrient intake databases reported that almost 90 % of the information in the food composition table comes from international food databases(Reference Giuntini, Coelho and Grande100) (Nutrition Data System for Research, from the University of Minnesota, and the Food Composition Table from the Dr Ricardo Jorge National Health Institute, from Lisbon)(29). The use of the 24hR in adolescents has some points to highlight: the adolescents could have had some difficulties in reporting portion sizes; the reports can be under- or overestimated because of unstructured eating habits, concerns with self-image and rebellion against authority; moreover, as observed in adults, obese adolescents underreported to a greater extent than normal-weight subjects(Reference Livingstone, Robson and Wallace101,Reference Livingstone and Black102) . Trying to reduce this reporting bias, we repeated a second 24hR over non-consecutive days(Reference Kerr, Wright and Dhaliwal103), using the multiple-pass method(Reference Raper, Perloff and Ingwersen104) as an interview technique, which organises the application of the 24hR into five steps, aiming to obtain more reliable reports. Furthermore, the ERICA study presents a complex and representative sample, which aims to obtain not individual but population estimates of the food intake of Brazilian adolescents. The 24hR was chosen because it is considered the most appropriate method to assess the association between diet and health outcomes(Reference Barufaldi, Abreu and Veiga105). Another study limitation could be the omitted-variable bias. Trying to reduce this, we used a theoretical model to support our choices(Reference Glymour, Greenland, Rothman, Greenland and Lash39,Reference Cortes, Faerstein and Struchiner40) . Additionally, the use of Se supplements was not investigated. Nonetheless, Se supplementation is not usual in Brazil(Reference Moraes, Welch and Nutti99,Reference dos Reis, El-Ramady, Santos, Pilon-Smits, Winkel and Lin106) .
This study’s strengths are the large probabilistic sample which reached a regional and national representativeness of 12–17-year-old Brazilian adolescents. Moreover, our statistical analyses were previously based on a theoretical model to identify a minimal group of confounder variables to justify causal process(Reference Glymour, Greenland, Rothman, Greenland and Lash39,Reference Cortes, Faerstein and Struchiner40) . Lastly, it is important to highlight the choice of the 24hR to assess dietary intake applied twice in a subsample to allow within-person variability adjustment as to the correct Se intake distribution.
Conclusions
Se intake was not associated with the MetS or its parameters in Brazilian adolescents between 12 and 17 years old. The lack of association could be due to the adequate Se intake in the study population (100 % of the sample). Another possible explanation is the Se U-shaped performance curve of Se intake related to cardio-metabolic outcomes. More studies conducted with adolescents are necessary to produce consistent literature findings and clarify this issue. We suggest that future studies explore dietary patterns associated with the MetS and its parameters in Brazilian adolescents.
Acknowledgements
The authors would like to thank the Post Graduate Program in Nutrition of the Federal University of Santa Catarina, Brazil, and the Coordenação do Aperfeiçoamento do Pessoal do Ensino Superior (CAPES, Coordination for higher Education Staff Development)/Social Demand Program for the scholarship granted to the authors A. R., R. F. and L. P. B. The authors would also like to thank the Fundação de Amparo à Pesquisa e Inovação de Santa Catarina (FAPESC, Santa Catarina State Foundation for Research and Innovation Support) for the scholarship granted to M. A. A. The authors thank Fernando Pizzatto de Moraes for collaborating on the final artwork of the graphical abstract.
This study was funded by the Post Graduate Program in Nutrition, Universidade Federal de Santa Catarina (UFSC, Federal University of Santa Catarina) – Social Demand Program/CAPES (Scholarship grant to Ms. Retondario, Mr. Fernandes, and Ms. Bricarello); the FAPESC (Scholarship to Ms. Alves); the Financiadora de Estudos e Projetos (FINEP, Financer of Studies and Projects) (grant number 01090421) and the Conselho Nacional de Pesquisa (CNPq, National Research Council) (grant numbers 565037/2010-2, 405009/2012-7 and 457050/2013-6). The founding sponsors had no role in the design, data collection, analysis or interpretation of the study, or in the writing of the manuscript or decision to publish the results.
A. R. worked in the project design, analysis and interpretation of data, and writing the manuscript; A. M. S. worked in the data analysis and interpretation, writing and reviewing the manuscript; L. P. B., M. A. A., R. F., E. B. S. M. T, L. A. Z. R. Z., R. S., and J. L. F. A. contributed significantly to writing and reviewing the manuscript. F. A. G. V. guided all steps of the research, such as project design, collection, analysis and interpretation of data, manuscript idealisation and revision of the final text. All authors read and approved the final version of the manuscript.
The authors declare no conflict of interest.