


University students are at a developmentally vulnerable life stage characterised by intensified academic, social and psychological demand. Mental health issues frequently observed during this period – particularly depression, anxiety and stress – negatively impact students’ academic performance and overall life satisfaction(Reference Solmi, Radua and Olivola1,Reference Doğan, Keser and Şen2) . Meta-analytic data reveal that depression and anxiety are prevalent among university students at 24·4 % and 33 %, respectively, and these rates have increased further with the COVID-19 pandemic(Reference Sheldon, Simmonds-Buckley and Bone3,Reference Deng, Zhou and Hou4) . Studies conducted in Türkiye also show that these rates are high, with 61·5 % of students reporting moderate to severe stress and 52 % reporting generalised anxiety(Reference Başoğlu, Özgüven and Ataoğlu5), underscoring a public health priority. Building on this, we situate eating-related risk within today’s food environment, where ultra-processed foods (UPF) are widely available and heavily marketed, plausibly intensifying stress-related vulnerabilities in young adults(Reference Monteiro and Cannon6).
Food addiction is characterised by a compulsive behavioural pattern involving tolerance, cravings, loss of control and excessive food intake despite negative consequences(Reference Schulte and Gearhardt7). The reported prevalence rates among college students range from 6·4 % to 21·9 %, underscoring food addiction as a significant behavioural risk for young adults(Reference Romero-Blanco, Hernández-Martínez and Parra-Fernández8,Reference Granero, Jiménez-Murcia and Gearhardt9) . Consistent with current scholarship, we adopt the NOVA framework and treat ‘food addiction’ as disproportionately involving UPF, rather than ‘high-calorie foods’ broadly(Reference Monteiro, Cannon and Levy10). This UPF-specific lens is theoretically grounded: mechanistic work shows that UPF are created and delivered in ways that parallel addictive drugs (e.g. high ‘dose’ of rewarding ingredients and rapid absorption enhanced by additives), which helps explain craving and loss of control in susceptible individuals(Reference Monteiro and Cannon6,Reference Gearhardt and Schulte11) . Notably, combining refined carbohydrate with fat produces supra-additive reward responses, further clarifying why UPF – not minimally processed foods – are most implicated in addictive-like eating. Building on this UPF framing, this study interprets eating risks primarily through an environment-first lens: ultra-processed products’ formulation, price, availability and marketing systematically elevate approach motivation and cue reactivity, which can amplify stress-related vulnerabilities in students beyond individual restraint or preference.
The relationship between stress and eating behaviours has been examined using both psychological and neurobiological frameworks. Chronic stress increases cortisol levels via the hypothalamic–pituitary–adrenal axis, which in turn increases the appetite for high-energy, rewarding foods(Reference Tomiyama12–Reference van der Valk, Savas and van Rossum14). Similarly, psychological models (escape theory and restraint theory) argue stress can trigger overeating by narrowing self-focus or disrupting dietary control(Reference Heatherton and Baumeister15,Reference Herman and Polivy16) . Coping strategies are a critical mediating mechanism that may influence the relationship between stress and eating behaviours. Research has indicated that adaptive coping strategies (e.g. planning and using emotional social support) regulate eating behaviours, whereas maladaptive strategies (e.g. denial and mental disengagement) exacerbate problematic eating behaviours(Reference Carver17,Reference Yönder Ertem and Karakaş18) . Some findings suggest that avoidant coping partially mediates the relationship between stress and emotional eating, with self-regulatory capacity strengthening this effect(Reference Henderson, Obeid and Buchholz19,Reference Ling and Zahry20) . When students appraise stressors as threatening and coping resources as insufficient, they are more likely to choose maladaptive strategies, including emotional eating(Reference Gibson21). Previous research has demonstrated that eating self-regulation partially mediates the relationship between perceived stress and emotional eating, while the combination of emotional eating and self-regulation fully mediates the relationship between stress and sweet food consumption(Reference Ling and Zahry20). Integrating the UPF literature strengthens this pathway logic: environmental risk factors that escalate addictive drug use – low cost, high availability and frequent marketing – also promote excessive UPF intake, thereby increasing the odds that stress-driven, emotion-focused coping will manifest as UPF-seeking and loss of control. Accordingly, rather than attributing overeating under stress solely to individual escape or failed restraint, we situate behaviour within UPF exposure – that is, products engineered to be hard to resist – so that coping is evaluated alongside the food environment(Reference Stariolo, Lemos and Khandpur22).
This study addresses both the theoretical and methodological gaps identified in the existing literature. First, most studies on the relationships between stress, coping and eating behaviours are limited to Western samples; empirical findings examining these relationships in contexts with diverse sociocultural structures, such as Turkey, are lacking. This limits the cultural generalisability of the data and hinders the development of context-specific intervention strategies. Second, in most studies explaining the impact of stress on eating behaviours, coping strategies are either treated as direct influencing variables or their function as mediating mechanisms has not been sufficiently tested. Theoretical frameworks suggest that these variables indirectly influence eating behaviours through complex interactions between them. Third, stress, coping and eating behaviours are often treated as isolated variables, and models testing these constructs at the multivariate and structural levels are rare in the literature. In this context, comprehensive models examining how stress impacts food addiction via coping strategies are expected to provide significant theoretical and practical contributions to the literature.
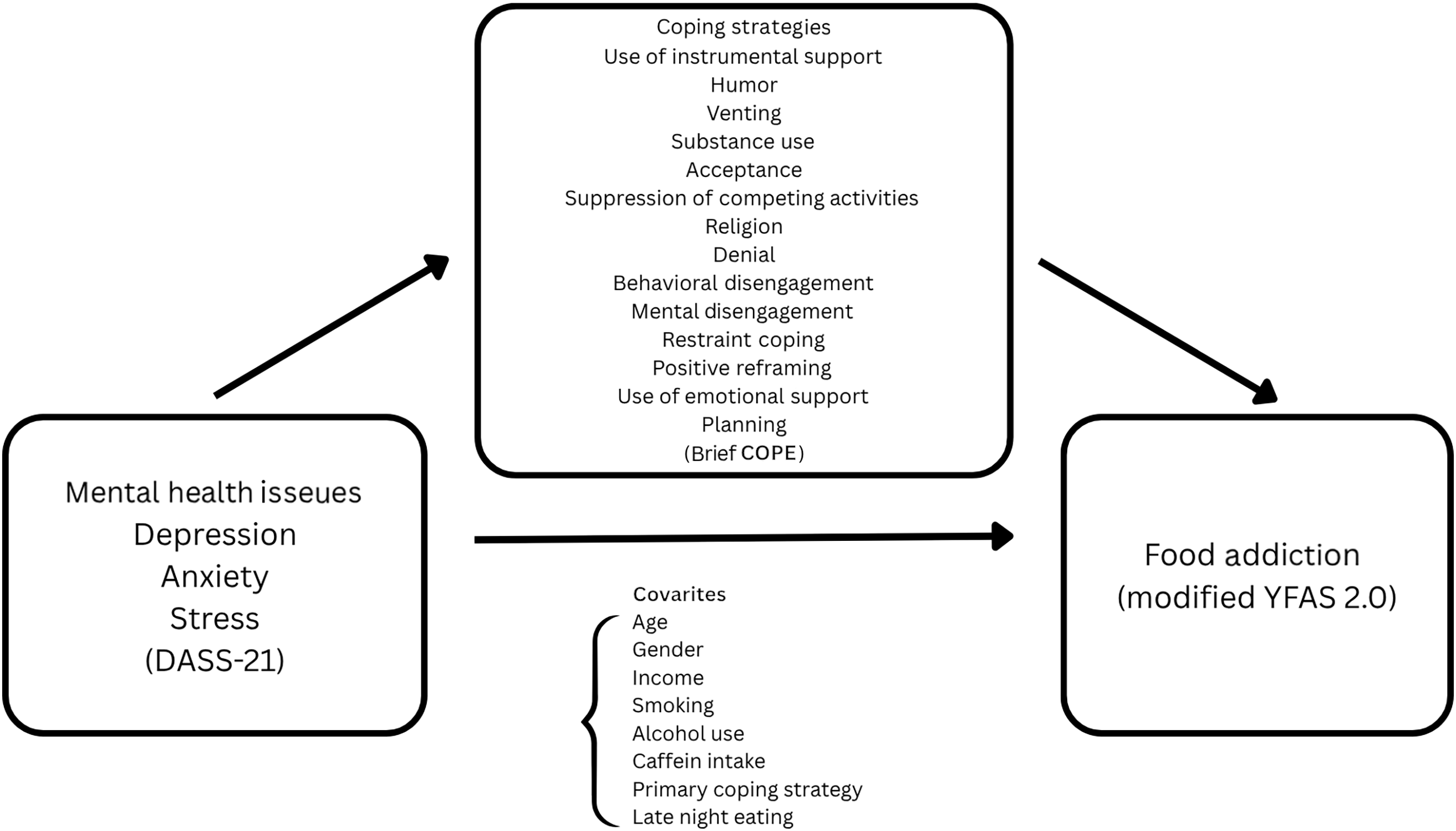
Guided by Lazarus and Folkman’s (1984) Transactional Stress Model, we explicitly map our constructs to the model’s components and test a theory-driven mediation pathway within today’s UPF-saturated food environment(Reference Lazarus and Folkman23). Primary appraisal is operationalised as current distress – depression, anxiety and stress; secondary appraisal (perceived coping resources) is acknowledged conceptually but not directly measured in this study; and enacted coping is captured with selected subscales representing adaptive (e.g. acceptance, emotional social support and humour) and maladaptive strategies (e.g. behavioural disengagement, restraint coping and suppression of competing activities). Within this framework, we model the pathway distress → enacted coping → food addiction, treating food addiction as a UPF-weighted phenotype (Figure 1). Therefore, this study aimed to examine the mediating role of adaptive and maladaptive coping strategies in the relationship between mental health issues (depression, anxiety and stress) and food addiction among university students using a multivariate approach. This study is, to our knowledge, among the first in Türkiye to evaluate whether coping strategies statistically transmit the associations between depression, anxiety and stress and food addiction in a large university sample, while interpreting these effects through an environment-first, UPF-focused lens. In doing so, we move beyond person-centric ‘escape/restraint’ explanations to a model that integrates stress appraisal, coping behaviour and an obesogenic, UPF-dense context.
Research model.

Research hypotheses
H1: Higher levels of depression, anxiety and stress will be positively associated with food addiction scores.
H2: Adaptive coping strategies will be negatively associated with food addiction scores, while maladaptive coping strategies will be positively associated with food addiction scores.
H3: Depression, anxiety and stress will be negatively associated with adaptive coping and positively associated with maladaptive coping.
H4: When controlling for demographics and health behaviours, depression, anxiety and stress will positively predict food addiction scores.
H5: Adaptive coping strategies (e.g. acceptance, humour and using emotional social support) will attenuate the relationship between depression/anxiety/stress and food addiction.
H6: Maladaptive coping strategies (e.g. restraint coping, mental disengagement and behavioural disengagement) will amplify the relationship between depression/anxiety/stress and food addiction.
Method
Research design
This study utilised a quantitative correlational research design. This study examined the relationships among university students’ mental health issues (depression, anxiety and stress), food addiction and coping strategies and evaluated the mediating role of coping strategies in this relationship. A cross-sectional design was used, and data were collected at a single time point.
Participants
The study population consisted of students enrolled at a university in Istanbul during the 2024–2025 academic year (n 13 342; Biruni University Periodic Student Statistics, 2024)(24). Based on the known population sampling formula (95 % power), a minimum sample size of 374 students was calculated. The study included individuals who were active students at a university during the 2024–2025 Spring semester, were 18 years of age or older, volunteered and had Turkish literacy skills. Participants with a history of clinically diagnosed eating disorders were excluded.
The study was completed with the participation of 1947 students. A post hoc power analysis based on the study results yielded a statistical power of over 95 % with parameters n 1947, f2 = 0·242, α = 0·05 and df = 3.
Data collection instruments
Data were collected online using Google Forms from March to May 2025. Participants were provided with informed consent at the beginning of the survey; consenting individuals completed the Personal Information Form, Depression-Anxiety-Stress-21 Scale (DASS-21), Coping Orientation to Problems Experienced Inventory (Brief COPE) and Modified Yale Food Addiction Scale 2.0 (mYFAS 2.0) scales.
Personal Information Form
This form, developed by the researchers, consisted of twenty-two questions that evaluated the participants’ sociodemographic characteristics (age, sex, faculty, grade, marital status, etc.), health status (physical illness, psychiatric disorder, medication use), lifestyle habits (exercise, smoking, alcohol, caffeine use) and nutritional behaviours (skipping meals, eating at night, number of main meals/snacks).
Depression-Anxiety-Stress-21 Scale
Developed by Lovibond and Lovibond (1995)(Reference Lovibond and Lovibond25) and adapted into Turkish by Sarıçam (2018)(Reference Sarıçam26), the DASS-21 is a twenty-one-item scale that assesses depression, anxiety and stress levels. The scale uses a four-point Likert-type scale (0 = never, 3 = often/almost always). Each subscale consists of seven items, and the subscale scores range from 0 to 21. The Cronbach’s α reliability coefficients for the Turkish version were reported as α = 0·87 for depression, α = 0·85 for anxiety and α = 0·81 for stress(Reference Sarıçam26). The reliability coefficients obtained in this study were α = 0·88 for depression, α = 0·83 for anxiety and α = 0·86 for stress.
Coping Orientation to Problems Experienced Inventory
Developed by Carver (1997)(Reference Carver17) and adapted into Turkish by Bacanlı, Sürücü and İlhan (2013), the Brief COPE is a twenty-eight-item instrument that assesses individuals’ coping strategies for stress. The scale consists of fourteen subscales, each containing two items. Participants responded using a four-point Likert-type scale (1 = never, 4 = often). The test–retest reliability of the Turkish version ranges from 0·44 to 0·90, and the internal consistency coefficients range from 0·39 to 0·92. The subscales use instrumental social support, humour, focusing and venting on emotions, substance use, acceptance, abandoning other activities, turning to religion, denial, behavioural disengagement, mental disengagement, self-limitation, positive reinterpretation, using emotional social support and planning. The coping strategies are grouped into two categories: adaptive strategies – acceptance, planning, active coping, use of instrumental support, positive reframing, use of emotional support, humour and religious coping – and maladaptive strategies – self-blame, denial, self-distraction, venting, disengagement and substance use(Reference Bacanlı, Sürücü and İlhan27,Reference Ünal and Uçar28) . In this study, the Cronbach’s α values of the sub-dimensions ranged from 0·47 to 0·90.
Modified Yale Food Addiction Scale 2.0
Developed by Schulte and Gearhardt (2017)(Reference Schulte and Gearhardt7) and adapted into Turkish by Tok, Ekerbiçer and Yazıcı (2023)(Reference Tok, Ekerbiçer and Yazıcı29), the mYFAS 2.0 is a thirteen-item scale that assesses food addiction symptoms. The scale was developed based on the substance use disorder criteria in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) and assesses eating habits over the past 12 months. The scale includes items with varying response options (2–8), and the total score ranges from 0 to 13. The Cronbach’s α reliability coefficient for the Turkish version was reported to be α = 0·80(Reference Tok, Ekerbiçer and Yazıcı29). The reliability coefficient obtained in this study was α = 0·91.
Statistical analysis
Data analysis was performed using IBM SPSS (v.29.0) and PROCESS Macro 4.2 plugin. The distributional characteristics of the data were assessed using the Kolmogorov–Smirnov test, as well as skewness and kurtosis values. Despite some deviations from normality, parametric tests were justified by the sufficiently large sample size (n 1947). Outliers were identified using z-scores, boxplots and the Mahalanobis distance method. Multicollinearity was assessed using the variance inflation factor, and all basic assumptions were met.
Pearson’s correlation analyses were performed to identify relationships among variables, and the internal consistency of the scales was assessed using Cronbach’s α coefficients. We controlled multiple comparisons within test families – Holm–Bonferroni for the three-test families (DASS-21 intercorrelations; DASS-21 ↔ mYFAS) and Benjamini–Hochberg FDR (q = 0·05) for the 42-test DASS-21 ↔ Brief COPE set – reporting raw and adjusted p-values; mediation models (pre-specified paths with bootstrapped CI) were not additionally adjusted.
Age, sex, socio-economic status, smoking, alcohol and caffeine use, problem experience and night eating behaviour were defined as control variables. Hierarchical multiple regression analyses were conducted to examine whether mental health issues (depression, anxiety and stress) predicted food addiction.
Hayes (2022) PROCESS Macro Model 4 (simple mediation) was used for the mediation analyses(Reference Hayes30). Each mental health issue (depression, anxiety and stress) was defined as an independent variable (X), food addiction as a dependent variable (Y) and each coping strategy as a mediator (M). The control variables (covariates) were included in each analysis.
To reduce multiple testing and enhance interpretability, we limited mediators to subscales that met all of the following a priori criteria: (i) conceptual relevance to emotion regulation/eating-to-cope pathways; (ii) acceptable internal consistency in this sample (α ≥ 0·60); and (iii) evidence of association with both the predictor (depression/anxiety/stress) and the outcome (mYFAS) at the bivariate level after multiplicity control within the mental health issues and Brief COPE family. Subscales meeting criteria were humour, acceptance, emotional social support (adaptive) and suppression of competing activities, behavioural disengagement and restraint coping (maladaptive). Other Brief COPE subscales are reported descriptively but were not modelled as mediators.
The statistical significance of the mediation effects was assessed using the bootstrap method with 5000 samples. Indirect effects were considered statistically significant if the 95 % CI did not include zero. Analyses were reported only for coping strategies that demonstrated significant mediation effects. Two-tailed analyses were performed for all statistical tests, and the significance level was set at 0·05.
Results
The participants had a mean age of 20·76 (sd 3·35) years, and the majority were female (82·6 %) and single (97·3 %). Nearly half of the participants (47·4 %) were enrolled in the Faculty of Health Sciences. Regarding class distribution, the majority (54·2 %) were first-year students.
With respect to academic achievement, 47·4 % of participants rated their performance as ‘average’. Most participants (60·1 %) reported their income as equal to their expenses. Most participants were unemployed (79·4 %) (Table 1).
Participants’ sociodemographic characteristics (n 1947)

Most participants reported no physical illnesses (85·4 %), psychiatric disorders (83·9 %) or regular medication use (86·1 %). A high proportion of participants (44·2 %) did not engage in regular exercise. Most participants did not smoke (77·2 %), 16·3 % consumed alcohol and 90·0 % consumed caffeinated beverages. Meal skipping was common among participants (90·9 %). Nighttime eating was reported by 47·6 % of the participants, whereas 52·4 % did not report this behaviour. The most frequently reported eating patterns were consumption of two main meals per d (64·7 %) and one snack per d (36·3 %). Most participants (68·4 %) reported sleeping for 6–8 h daily. When encountering problems, the coping method most frequently preferred by participants was talking to friends or family (41·1 %) (Table 2).
Participants’ general health characteristics (n 1947)

The descriptive analysis revealed that the mean depression subscale score of the DASS-21 was 6·14 (sd 4·70) (range: 0–21), with a Cronbach’s α reliability coefficient of 0·88. The mean score for the anxiety sub-dimension was 5·65 (sd 4·34) (min: 0, max: 21), and Cronbach’s α was 0·83. The mean score for the stress sub-dimension was 6·80 (sd 4·55) (min: 0, max: 21), and Cronbach’s α was 0·86. The total mean score for the mYFAS 2.0 Scale was 1·01 (sd 2·37) (range: 0–13), with high internal consistency (Cronbach’s α = 0·91), indicating strong reliability. Examination of the subscales of the Brief COPE showed higher mean scores for planning (5·22 (sd 1·74)), turning to religion (5·77 (sd 1·98)), positive reinterpretation (4·96 (sd 1·72)), acceptance (4·93 (sd 1·64)), instrumental social support (4·90 (sd 1·72)) and humour (4·72 (sd 2·02)). Cronbach’s α coefficients for the subscales ranged from 0·47 to 0·90, with the highest internal consistency found for the humour subscale (0·90) and the lowest for emotional social support (0·47) (Table 3).
Scales’ descriptive statistics

Correlation analyses revealed strong, positive and statistically significant correlations among depression, anxiety and stress scores (depression-anxiety: r = 0·724; depression-stress: r = 0·772; anxiety-stress: r = 0·796) remained significant after Holm adjustment (α = 0·05; all P_adj < 0·001). Moderate, positive and statistically significant correlations were found between the mYFAS scores and depression (r = 0·398), anxiety (r = 0·399) and stress (r = 0·417); likewise they remained significant after Holm adjustment α = 0·05; all P_adj < 0·001).
For DASS-21 – Brief COPE associations (3 × 14 = 42 tests), applying Benjamini–Hochberg FDR (q = 0·05) showed that 37/42 correlations remained significant after adjustment. The five that did not survive were depression–turning to religion, depression–positive reinterpretation, depression–planning, anxiety–positive reinterpretation and anxiety–planning; all others – including stress–positive reinterpretation – met the FDR threshold. Effects were generally small to moderate, with the largest magnitudes for behavioural disengagement (e.g. depression r = 0·440; anxiety r = 0·396; stress r = 0·379), as well as suppression of competing activities, denial and mental disengagement. Full raw and adjusted p-values are provided in Table 4. Among coping styles, instrumental social support and planning showed significant correlations with multiple other coping sub-dimensions. Overall, these findings suggest that as participants’ depression, anxiety and stress levels increase, their use of coping strategies also increases (Table 4).
Correlation analysis

DASS-21, Depression-Anxiety-Stress-21 Scale; mYFAS 2.0, Modified Yale Food Addiction Scale 2.0; Brief COPE, Coping Orientation to Problems Experienced Inventory; R, Pearson’s correlation coefficient.
P < 0·05.
Multiple comparisons controlled within families: †DASS↔mYFAS (3 tests) and ‡DASS intercorrelations (3 tests) via Holm–Bonferroni (α = 0·05); §DASS↔Brief COPE (3 × 14 = 42 tests) via Benjamini–Hochberg FDR (q = 0·05). Bold values indicate significance after adjustment.
Multiple linear regression analysis was performed to examine whether depression, anxiety and stress levels significantly predicted food addiction among university students. In the first model, only the DASS-21 subscales were entered; this model was statistically significant, F (3, 1943) = 156·62, P < 0·001. The model explained 19·5 % of the variance (R2 = 0·195). Depression (β = 0·151, P < 0·001), anxiety (β = 0·137, P < 0·001) and stress (β = 0·191, P < 0·001) were significant positive predictors of food addiction.
The second model included the control variables (sex, age, faculty, income, smoking, alcohol consumption, caffeine consumption, nighttime eating behaviour and experiencing problems). This expanded model was also statistically significant, F (12, 1934) = 42·42, P < 0·001, and accounted for 20·8 % of the variance in food addiction scores (R2 = 0·208). After controlling for these variables, depression (β = 0·145, P < 0·001), anxiety (β = 0·131, P < 0·001) and stress (β = 0·186, P < 0·001) significantly and positively predicted food addiction. Additionally, among the control variables, smoking (β = 0·052, P = 0·020) and nighttime eating behaviour (β = –0·090, P < 0·001) had significant effects on food addiction. All VIF values were below 5, indicating no multicollinearity issues within the model. The Durbin–Watson coefficient was 2·11, indicating no autocorrelation (Table 5).
Multiple linear regression results: relationship between mental health issues and control variables and food addiction

Mediation analyses (PROCESS Model 4, Bootstrap = 5000) revealed that several coping strategies significantly mediated the relationships between depression, anxiety and stress levels and food addiction. Across all models, the direct effects (c′) of depression, anxiety and stress on food addiction remained positive and significant (for the runs shown in Table 6: Depression c′ = 0·169–0·150, Anxiety c′ = 0·182–0·163, Stress c′ = 0·183–0·172; all P < 0·001), indicating partial mediation. For depression to food addiction, adaptive mediators showed positive indirect effects: Humour (a = +0·084, P < 0·001; b = +0·059, P = 0·030; a × b = +0·005, 95 % CI (0·001, 0·010)), Acceptance (a = +0·070, P < 0·001; b = +0·130, P < 0·001; a × b = +0·009, (0·004, 0·015)) and Emotional social support (a = +0·061, P < 0·001; b = +0·128, P < 0·001; a × b = +0·008, (0·002, 0·015)). Maladaptive mediators were also positive: Suppression of competing activities (a = +0·091, P < 0·001; b = +0·118, P = 0·001; a × b = +0·008, (0·001, 0·016)), Behavioral disengagement (a = +0·135, P < 0·001; b = +0·172, P < 0·001; a × b = +0·023, (0·010, 0·035)) and Restraint coping (a = +0·083, P < 0·001; b = +0·085, P = 0·026; a × b = +0·006, (0·000, 0·013)).
Mediation analyses of coping strategies on the relationship between mental health issues and food addiction (PROCESS Model 4, Bootstrap = 5000)

DASS-21, Depression Anxiety Stress Scale-21; YFAS, Yale Food Addiction Scale 2.0; β, standard regression coefficient.
For anxiety to food addiction, adaptive mediators were again positive: Humour (a = +0·091, P < 0·001; b = +0·118, P = 0·001; a × b = +0·006, (0·001, 0·012)), Acceptance (a = +0·135, P < 0·001; b = +0·173, P < 0·001; a × b = +0·011, (0·005, 0·017)) and Emotional social support (a = +0·083, P < 0·001; b = +0·085, P = 0·026; a × b = +0·009, (0·003, 0·017)). Maladaptive mediators were likewise positive: Suppression of competing activities (a = +0·096, P < 0·001; b = +0·109, P = 0·003; a × b = +0·009, (0·002, 0·017)), Behavioral disengagement (a = +0·128, P < 0·001; b = +0·193, P < 0·001; a × b = +0·025, (0·013, 0·038)) and Restraint coping (a = +0·078, P < 0·001; b = +0·096, P = 0·012; a × b = +0·007, (0·001, 0·013)).
For stress to food addiction, adaptive mediators were positive: Acceptance (a = +0·083, P < 0·001; b = +0·143, P < 0·001; a × b = +0·012, (0·006, 0·019)) and Emotional social support (a = +0·087, P < 0·001; b = +0·108, P = 0·0017; a × b = +0·010, (0·002, 0·019)). Humour did not mediate (a = +0·112, P < 0·001; b = +0·047, P = 0·074; a × b = +0·005, 95 % CI (–0·000, 0·011)). Among maladaptive mediators, Behavioral disengagement (a = +0·117, P < 0·001; b = +0·214, P < 0·001; a × b = +0·024, (0·013, 0·035)) and Restraint coping (a = +0·088, P < 0·001; b = +0·115, P = 0·001; a × b = +0·007, (0·000, 0·014)) showed positive indirects. Suppression of competing activities did not mediate (a = +0·113, P < 0·001; b = +0·075, P = 0·041; a × b = +0·008, 95 % CI (–0·009, 0·018)).
Across models, the proportion mediated ranged from about 11–12 % for adaptive coping to about 19–22 % for maladaptive coping (e.g. Depression→FA: adaptive 11·5 %, maladaptive 22·0 %; Anxiety→FA: adaptive 12·1 %, maladaptive 21·7 %; Stress→FA: adaptive 12·0 %, maladaptive 19·2 %), consistent with partial mediation. In every model, path a (IV→Mediator) and path b (Mediator→YFAS) were positive and statistically significant, accounting for the positive indirect effects reported in Table 6.
Discussion
This study examined participants’ mental health issues and food addiction tendencies, along with their coping strategies, using data obtained from 1947 university students in İstanbul, Türkiye. The findings indicate that higher depression, anxiety and stress scores are associated with higher food addiction scores, and coping style systematically tracks this relationship. Adaptive strategies were associated with lower rates of food addiction, whereas maladaptive strategies were associated with higher rates of mental health issues and food addiction. Taken together, these results indicate that food addiction is not simply a physiological issue but rather a complex phenomenon closely linked to mood states and stress-coping strategies. Consistent with recent scholarship, we conceptualise ‘food addiction’ as disproportionately involving UPF – industrial formulations rich in refined ingredients and additives – rather than high-energy foods in general, aligning clinical and policy discourse with the product class most implicated in addictive-like eating(Reference Monteiro and Cannon6,Reference Monteiro, Cannon and Levy10,Reference Monteiro, Cannon and Levy31) . Against this backdrop, studies have shown that the prevalence of food addiction among university students is substantial. Romero-Blanco et al. (2021) reported a prevalence of 6·4 % among students(Reference Romero-Blanco, Hernández-Martínez and Parra-Fernández8). In Spain, Escrivá-Martínez et al. (2023) reported mild food addiction in 12·5 % of students, moderate addiction in 11·3 % and severe addiction in 20·6 %(Reference Escrivá-Martínez, Galiana and Herrero32). A study among medical students in India reported a high food addiction prevalence rate of 27·4 %(Reference Soman33). Similarly, a recent Turkish study found that 40 % of students met the criteria for food addiction, underscoring variability across settings but a consistently non-trivial burden(Reference Kayaoğlu, Göküstün and Ay34). These varying prevalence rates indicate that food addiction differs across cultures and samples but consistently emerges as a significant issue among young adults in all studies. Aligned with this literature, the reliable measurement tools and large sample size employed in our study strengthen the observed association between mental health and food addiction among university students, which is consistent with the existing literature.
H1: Relationship between mental health issues and food addiction
One of the primary findings of this study was the significant positive relationship between mental health issues and food addiction, confirming H1. This pattern indicates a clear dose–response link between current distress and addictive-like eating. This finding aligns with theoretical perspectives suggesting that food consumption serves not only to satisfy physical hunger but also to regulate emotions in the face of distress. Indeed, emotional eating behaviour is defined as turning to food to suppress or relieve negative mood and is observed more frequently in individuals with depressed mood, anxiety and chronic stress(Reference van Strien, Gibson and Baños35,Reference Silva, Meireles and Chagas36) . Mechanistically, the association is consistent with emotion regulation accounts and the UPF lens: under distress, individuals use eating to down-regulate negative affect, and UPF – engineered for hyperpalatability, rapid absorption and cue-driven reward – elevate approach motivation and loss of control compared with minimally processed foods(Reference Monteiro and Cannon6,Reference Gearhardt and Schulte11) . This helps explain why distress maps onto UPF-specific intake rather than ‘food’ in general. Notably, convergent self-report, behavioural and neuroimaging evidence indicates that ultra-processed (not minimally processed) foods are the ones most consistently linked to craving, loss of control and binge-type intake, reinforcing the UPF-specific lens adopted here(Reference Gearhardt and Schulte11). One other prominent hypothesis suggests that eating behaviours provide a short-term soothing effect and act as a coping mechanism. Research has shown that stressed individuals tend to gravitate towards ‘comfort foods’, particularly those rich in carbohydrates and fats(Reference van Strien, Gibson and Baños35,Reference Özkan, Danışmaz Sevin and Avcı37) . While the immediate pleasure and emotional relief from food intake can temporarily suppress negative emotions, in the long term this behaviour may evolve into a vicious cycle resembling addiction(Reference Monteiro, Cannon and Levy31,Reference Gearhardt, Bueno and DiFeliceantonio38) . Previous studies have indicated that impulse control is particularly challenging under anxiety and chronic stress, making it difficult for individuals to resist high-energy foods(Reference Piątkowska-Chmiel, Krawiec and Ziętara39). The biological psychiatry literature has also demonstrated that stress hormones and negative moods increase food cravings by activating the brain reward pathways(Reference Stariolo, Lemos and Khandpur22,Reference Wallace and Fordahl40) . This relationship is widely supported by the literature. A cross-sectional study in Turkey found that university students with food addiction had significantly higher depression, anxiety and stress scale scores than those without food addiction(Reference Kayaoğlu, Göküstün and Ay34). A national study conducted in Brazil during the COVID-19 pandemic among 5368 students found that students diagnosed with clinical anxiety disorders had over three times the risk of food addiction compared with students without anxiety. Similarly, students with depression had approximately 1·6 times the risk of food addiction(Reference da Silva Júnior, de Lima Macena and de Oliveira41). Converging evidence from Argentina also emphasises that negative affective states, such as depressive symptoms and stress, contribute significantly to food addiction, highlighting the critical role of stress-driven eating motivation in this relationship(Reference Fernández, Pilatti and Pautassi42). Collectively, these studies and our findings support the concept of ‘emotional eating’, indicating that emotional distress manifests through food consumption behaviours.
H2 and H3: relationships between coping strategies, food addiction and mental health issues
Another important finding of this study is that coping strategies show complex, bidirectional relationships with both mental health issues and food addiction, confirming with H2 and H3. The coping methods individuals employ to manage stress, and emotional difficulties influence both psychological well-being and eating behaviours in interconnected ways. In our study, adaptive coping strategies, particularly humour, acceptance (adapting to circumstances) and seeking emotional social support, were negatively correlated with food addiction scores. This suggests that students who cope constructively with stress, receive emotional support or utilise humour in difficult situations are likely to report lower levels of food addiction symptoms and, potentially, lower levels of depression and anxiety. Indeed, previous research indicates that university students commonly employ social support as a coping strategy, which effectively reduces anxiety and promotes overall psychological well-being(Reference Salam, Harith and Abdullah43,Reference Acoba44) . Adaptive coping strategies may help reduce emotion-driven overeating by providing healthier mechanisms for relieving emotional tension.
On the other hand, research has identified several maladaptive coping strategies positively correlated with mental health issues and food addiction. Maladaptive strategies such as self-limitation (suppressing emotions), behavioural disengagement (giving up or ceasing to seek solutions) and abandoning enjoyable activities (social isolation) are particularly linked to higher levels of depression and anxiety. Individuals who frequently use maladaptive coping strategies may be more inclined towards avoidance and denial instead of actively addressing their problems. Although avoidance-focused strategies may temporarily alleviate stress, they fail to address underlying problems and may cumulatively result in increased psychological distress over time(Reference Chaaya, Sfeir and Khoury45). Moreover, coping strategies involving avoidance and denial facilitate engagement in unhealthy behaviours such as emotional eating. The literature consistently reports that emotion-focused coping strategies, such as substance use or overeating to avoid confronting problems, are positively correlated with depression and anxiety symptoms(Reference Jaud and Lunardo46). Students experiencing mental health issues who use maladaptive coping strategies may further deteriorate their mental health and become vulnerable to unhealthy eating behaviours. In other words, individuals’ coping strategies play a critical role in either increasing or decreasing their risk of food addiction.
Beyond individual coping, an environment-first account clarifies why stress maps onto intake in UPF-saturated settings. We therefore situate stress-related overeating within UPF exposure rather than ‘escape/restraint’ tendencies alone. Experimental work shows that UPF are engineered and marketed to heighten approach motivation and intention to consume v. unprocessed/minimally processed foods – even when visual/aesthetic features are controlled – implicating product design (hyperpalatability, additives) as a proximal driver of cue-triggered intake rather than purely individual restraint failure(Reference Lemos, Coutinho and Silva47). In parallel, population data from COVID-19 indicate that symptoms of UPF addiction statistically mediate the link between psychological stress and emotional eating (about 60 % of the total effect), underscoring that distress operates through an addiction-like pathway tied specifically to UPF availability, not ‘food’ in general(Reference Stariolo, Lemos and Khandpur22). Taken together, our results align with a policy-relevant model: under stress, students are more susceptible to UPF-cue approach and addiction-like symptoms, which amplifies intake; thus, intervention levers should extend beyond individual coping to include healthier food environments (e.g. constraints on UPF access/marketing, default swaps towards minimally processed options) alongside coping-skills training(Reference Stariolo, Lemos and Khandpur22,Reference Lemos, Coutinho and Silva47) . Importantly, the broader ‘risk architecture’ also matters low cost, ubiquity and aggressive marketing of UPF increase exposure and exacerbate stress-eating loops, especially when maladaptive coping is present(Reference Monteiro and Cannon6,Reference Gearhardt and Schulte11) . Together, our results and the broader evidence support a dual-target strategy: strengthen adaptive coping (acceptance and social support) and de-risk the food environment (limit UPF access/marketing; default towards minimally processed options). This framing explains the observed pattern under H2 and H3 – distress shifts coping profiles towards maladaptive strategies, which, in a UPF-dense environment, increases the probability of addictive-like eating – while identifying clear levers for practice and policy.
H4: Predictive effect of mental health issues on food addiction
This study extended beyond correlational analysis by examining the extent to which mental health issues predict food addiction. Multiple regression analyses revealed that students’ depression, anxiety and stress levels significantly predicted food addiction scores, even when controlling for demographic factors and health behaviours, supporting H4. This finding suggests that mental health issues are not only concurrently associated with food addiction but also with daily behaviours (e.g. smoking, night eating). Previous studies have indicated that individuals experiencing high stress may resort to eating behaviours for emotional relief, potentially resulting in chronic patterns and eventually addiction(Reference Monteiro, Cannon and Levy31,Reference Gearhardt, Bueno and DiFeliceantonio38) . Chao et al. (2018) reported that, even after adjusting for depression, stress, BMI and demographics, current smokers – relative to never-smokers – experienced more frequent cravings for high-fat foods (including fast-food fats) and consumed these items more often. Moreover, nicotine dependence showed a positive association with overall food-craving frequency as well as cravings specifically for high fats, sweets and carbohydrate/starch foods(Reference Chao, White and Grilo48). Consistent with the previous literature on stress and emotional eating, students who reported higher stress levels in this study showed significantly increased food addiction scores.
Other findings support the predictive effects of mental health issues. A study conducted by Bartschi and Greenwood (2023) with 628 adults revealed that the increased severity of depressive symptoms explained the elevated BMI entirely through symptoms of food addiction(Reference Bartschi and Greenwood49). This finding suggests that depression increases the risk of weight gain and obesity through food addiction, highlighting the influential role of depressive symptoms in shaping eating habits. Similarly, Zheng et al. reported that depression directly predicted eating disorder symptoms in university female students(Reference Zheng, Han and Li50). Individuals experiencing anxiety or depression may resort to overeating and unhealthy food choices through various biological and psychological mechanisms. Individuals with anxiety disorders may display altered sensitivity to reward and punishment, prompting them to seek foods that offer immediate pleasure as a means of suppressing anxiety(Reference da Silva Júnior, de Lima Macena and de Oliveira41). Increased levels of stress-related hormones, such as cortisol, stimulate appetite and cravings for high-energy foods(Reference Özdemir Petek51). In a comprehensive review, Sinha (2018) emphasised that chronic stress disrupts the brain’s reward and motivation systems, thereby promoting overeating and weight gain(Reference Sinha13). LaFata notes several key advances: global UPF addiction prevalence estimates of about 14 % in adults and about 15 % in youth; documented inequities affecting people of colour and individuals facing food insecurity; evidence of dysregulation along the brain–gut–microbiome axis; early signals of withdrawal phenomena with UPF; and poorer weight management outcomes among those meeting UPF addiction criteria(Reference LaFata, Allison and Audrain-McGovern52). Another study reported that scores on the screening highly processed food consumption were positively associated with food addiction scores and with DASS-21 (P < 0·05)(Reference Mengi Çelik, Güler and Ekici53). In interpreting these results, we also treat food addiction as a substance-based phenotype operationalised with YFAS 2.0, which adapts the DSM’s 11 behavioural indicators to the specific features of UPF – clarifying why not all foods, or eating itself, are addictive (11). Collectively, these findings clearly illustrate that mental health issues profoundly and multidimensionally impact not only mood but also eating behaviours and weight management.
H5 and H6: the mediating role of coping strategies
Mediation analyses indicated that specific coping strategies significantly modified the impact of depression, anxiety and stress on food addiction. Adaptive coping strategies – including acceptance, humour and using emotional social support – significantly mediated the relationship between these psychological factors and food addiction; H5 was not supported. Although humour, acceptance and emotional social support are typically classed as adaptive, their positive indirect effects suggest co-activation under high distress: students mobilise adaptive strategies, yet – within a UPF environment – these may be insufficient to offset UPF-seeking, yielding net amplification of distress to food addiction. Conversely, maladaptive coping strategies, such as suppression of competing activities, behavioural disengagement and restraint coping, significantly mediated and strengthened this relationship; H6 was supported. These findings suggest that students’ coping strategies indirectly influence not only their mental health but also their eating behaviours.
The existing literature supports the mediating effect of coping strategies. In a study with Chinese female students, Zheng et al. (2020) demonstrated that depression influences eating disorder symptoms partly through the coping styles individuals adopt(Reference Zheng, Han and Li50). When individuals experiencing high levels of depression utilise negative coping styles, the adverse effects of depression on eating behaviours intensify. Consistent with our findings, negative coping strategies increase the likelihood that depression leads to problematic eating behaviours. Similarly, research on young adults in Argentina revealed that the relationship between stress, depression and food addiction is largely mediated by ‘eating to cope’ motivation and uncontrolled eating behaviours(Reference Fernández, Pilatti and Pautassi42). This finding highlights that mental health issues do not directly cause food addiction; instead, using food as a coping mechanism serves as a critical determinant. Therefore, the mediating mechanism revealed in our study is consistent with the evidence in the literature. The risk of food addiction is determined not merely by mental health issues alone but significantly by how individuals cope with such distress. Maladaptive coping strategies pose a dual risk by failing to effectively manage negative emotions and promoting unhealthy eating behaviours.
Our mediation results translate into concrete levers for practice and policy. Because maladaptive coping – particularly behavioural disengagement, restraint coping and suppression of competing activities – showed consistently positive a- and b-paths with positive indirect effects, brief skills-based programmes that reduce avoidance and passivity (behavioural activation to re-engage valued activities, structured problem-solving to replace rumination with plans and simple ‘if–then’ implementation intentions to interrupt withdrawal during peak affect) are warranted. At the same time, the adaptive strategies we examined (acceptance, emotional social support – and humour) also yielded positive indirect effects under high distress. We interpret this as co-activation rather than pure protection: when distress spikes, students mobilise adaptive skills, but within a UPF-dense environment these may be insufficient to counter reward-driven eating, leaving the net pathway to food addiction positive. Accordingly, interventions should be two-pronged: skill the person up (acceptance-based coping, affect labelling and structured help-seeking) while shaping the food context (default minimally processed options on campus, point-of-purchase prompts and lower UPF salience in vending/cafeterias). A stepped ‘screen-and-support’ pathway (e.g. screening → self-help modules → guided digital CBT/behavioural activation → clinician-led care as needed) fits the partial mediation pattern we observed.
Strengths and limitations
The strengths of this study include its large sample size (n 1947), representation of diverse subgroups and enhanced generalisability of the findings. Additionally, the Turkish versions of internationally recognised measurement tools (DASS-21, COPE-Brief and mYFAS 2.0) demonstrated adequate psychometric properties regarding validity and reliability. This is one of the first studies to examine the relationships between mental health issues, coping strategies and food addiction among a sample of university students in Turkey. In this regard, this study addresses a notable gap in the literature and provides an original contribution. Our findings not only deepen the understanding of individual psychopathology but also provide concrete insights for developing future interventions.
However, our study had some limitations that should be considered. First, because of the cross-sectional design of the study, the observed relationships do not imply causality. The use of self-reported measures may introduce potential biases, including social desirability bias and response awareness. Coping strategies were assessed exclusively at the individual level without considering relevant environmental factors. The fact that the sample consisted solely of university students limits the generalisability of these findings. Moreover, the scales used were for symptom assessment rather than clinical diagnosis; thus, the absence of clinical evaluations warrants a cautious interpretation. We did not include a direct measure of secondary appraisal; therefore, appraisal was inferred rather than observed, and coping was modelled as enacted behaviours downstream of appraisal. These limitations highlight the need for methodological and theoretical improvements in future research.
Conclusion
The findings of this study indicate that mental health issues, including depression, anxiety and stress, are significantly associated with food addiction among university students. Furthermore, coping strategies significantly mediated this relationship, indicating that individuals’ methods of coping with stress substantially influenced their risk of food addiction. Food addiction is not solely the outcome of mental health issues; it also reflects individuals’ coping responses to these symptoms. These results suggest that models explaining eating behaviours should include both emotional and behavioural components. As elaborated in the Discussion, we specifically highlight brief, skills-based interventions that reduce maladaptive coping (e.g. behavioural activation to counter disengagement; problem-solving to replace restraint coping) and strengthen adaptive coping (acceptance-based strategies and structured emotional-support training). In parallel, we recommend routine screening and a stepped-care pathway, alongside campus choice-architecture changes that make minimally processed options the default to support coping gains in a UPF-dense environment.
For practitioners, the development of adaptive coping skills should be considered a protective factor against food addiction. Early identification and management of mental health issues are critical for supporting psychological well-being and promoting healthy eating behaviours. These findings suggest the need for the holistic integration of coping-focused interventions into mental health services. Consistent with our mediation results, coping accounted for a meaningful portion of the total association (adaptive mediators approximately 11–12 %; maladaptive mediators approximately 19–22 %), reinforcing the clinical value of targeting coping patterns in prevention and treatment.
Future research should primarily adopt longitudinal designs to better establish causal relationships. Intervention-based experimental studies focusing on adaptive coping strategies could contribute to the development of more effective programmes aimed at preventing food addiction. Furthermore, future models should incorporate social support and cultural factors, and studies should involve larger and more diverse samples in terms of age, culture and socio-economic backgrounds. Finally, the use of multivariate models would be beneficial for comprehensively examining additional variables such as body image, self-esteem, obsessive-compulsive symptoms and social media use. Building on the current findings, future multivariate models should also include empirically signalled health-behaviour covariates (e.g. late-night eating and smoking) and test sequential/parallel mediation structures to clarify how these factors interact with coping to influence food addiction over time.
In conclusion, this study significantly contributes to the literature by demonstrating the dynamic interplay between mental health issues, coping strategies and food addiction in university students. Enhancing coping skills through psychological interventions should be the core of effective prevention and intervention strategies targeting food addiction. Future longitudinal and multidimensional studies will further extend these findings and contribute to the advancement of knowledge in this area.
Clinical implications
The findings of this study offer several important contributions to clinical practice by highlighting that coping strategies significantly influence the risk of food addiction. In particular, the protective role of adaptive coping strategies underscores the need for psychoeducational programmes to enhance stress management skills. Conversely, maladaptive coping strategies indicate specific dysfunctional behaviours that should be targeted in therapeutic interventions. The incorporation of eating behaviours into mental health assessments emphasises the importance of adopting an interdisciplinary clinical approach. These findings provide practical guidance for the development of holistic intervention programmes through interdisciplinary collaboration among professionals in nutrition and dietetics, psychiatrist, psychiatric nursing and clinical psychology.
Acknowledgements
The authors thank the participating students for their time and openness. The authors acknowledge the Biruni University Scientific Research Ethics Committee for approving the study and the institution for administrative support during data collection.
This research received no specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Conceptualisation: F. Ç., E. M., M. M. M. A. and S. N. O. A. Methodology: E. M. and M. M. M. A. Formal analysis: M. M. M. A. Investigation/Data curation: E. M. and S. N. O. A. Writing – original draft: E. M., M. M. M. A. and S. N. O. A. Writing – review and editing: F. Ç. and E. M. Supervision: F. Ç. Project administration: F. Ç. and E. M.
The authors declare no conflicts of interest related to this work.
The study was approved by the Biruni University Scientific Research Ethics Committee (Decision No: 2024-BİAEK/07-47; Date: 24 February 2025). Necessary institutional permission was obtained from Biruni University. Participants were informed about the purpose, method, risks and potential benefits of the study, which was conducted in accordance with the principles of the Declaration of Helsinki.







 Open access
Open access