



Introduction
Food insecurity (FI) is defined as a lack of regular access to enough safe and nutritious food for normal growth and development and an active and healthy life(1). FI is not only traditionally prevalent in low-income countries, but more recently has become a health concern in higher-income countries including the UK, Australia, Canada, and the USA(Reference Loopstra2). FI goes beyond being without food or experiencing hunger; individuals or households can be classified as experiencing FI if they are worried about accessing or acquiring food that meets their nutritional requirements(Reference Pool and Dooris3). FI most commonly affects individuals with low socio-economic status (SES), especially those living on low incomes(Reference Loopstra, Reeves and Tarasuk4).
Paradoxically, in high-income countries, food insecurity has been associated with an increased risk of obesity, especially in women(Reference Aggarwal, Monsivais and Cook5–Reference Johnstone and Lonnie8). Potential explanations for the obesity–food insecurity paradox include the Resource Scarcity Hypothesis(Reference Dhurandhar9), where individuals perceive threat cues from their environment, indicating an upcoming shortage of food, triggering a behavioural response of increased caloric intake. Another potential explanation is the Insurance Hypothesis(Reference Nettle, Andrews and Bateson10), where individuals store fat in their bodies in anticipation of future food shortages. Other, more plausible, explanations for this paradox relate to the cost of foods, where foods higher in fat, salt, and sugar are typically less expensive (per calorie) than healthier alternatives, meaning less healthy options become a sensible economic choice for many, especially those living on a low income(Reference Drewnowski11,Reference Eskandari, Lake, Rose, Butler and O’Malley12) , which has recently exacerbated during the cost-of-living crisis(Reference Stone, Brown, Douglas, Green, Hunter and Lonnie13). Additionally, an individual’s environmental context and available resources may result in less healthy food purchases and consumption through limited access to healthy food and/or insufficient resources or facilities to store, prepare, and cook food(Reference Briazu, Masood, Hunt, Pettinger, Wagstaff and McCloy14–Reference Shinwell and Defeyter16). Furthermore, those living on a low income or experiencing FI may be reluctant to buy foods such as fruit and vegetables due to the potential for waste given their short shelf life, or the risk that their children or families will reject them due to taste preferences(Reference Daniel17,Reference Moran, Khandpur, Polacsek and Rimm18) .
Interlinked individual, societal, political, and economic factors within the environment influence an individual’s risk of developing obesity and may also decrease their responsiveness or their ability to engage with weight management interventions(Reference Adams, Mytton, White and Monsivais19–Reference Theis and White22). Prior strategies and interventions devised to address obesity have faced criticism for placing strong emphasis on behaviour change at the individual level. These interventions often draw heavily on individual agency and mistakenly assume all members of society have equitable access to personal resources (i.e., the time to source and prepare healthy food) or psychological resources (i.e., the well-being or motivation) required to engage with public health campaigns(Reference Adams, Mytton, White and Monsivais19,Reference Theis and White22) . Instead, mid-to-upstream-level population health interventions – for example, reformulation of food items by manufacturers(Reference Gressier, Swinburn, Frost, Segal and Sassi23,Reference Yeung, Gohil, Rangan, Flood, Arcot and Gill24) – or nudges – such as changes to the in-store supermarket environment that encourage the adoption of a healthier purchasing behaviour (i.e., removing less healthy food items from prominent placement and high footfall areas)(Reference Vecchio and Cavallo25,Reference Bucher, Collins, Rollo, McCaffrey, De Vlieger and Van der Bend26) – may be a more equitable course of action(Reference Adams, Mytton, White and Monsivais19). To understand and address public health challenges such as obesity, a more comprehensive approach that integrates multiple levels relating to the individual, their environment, and the policies that impact their lives is required(Reference Agurs-Collins, Persky, Paskett, Barkin, Meissner and Nansel27,Reference Stevens, Pratt, Boyington, Nelson, Truesdale and Ward28) .
UK survey data indicates that around 76–83% of food consumed in the home is purchased from the supermarket(Reference Bashir29,30) . Data from the USA indicates 41% of respondents shopped for groceries in the supermarket once a week, with a further 29% doing so two to three times a week.(Reference Ozbun31) Worldwide, household shoppers spend approximately $1.38 trillion annually in supermarkets and trends show continual upward growth(Reference Ozbun32). Supermarkets have been found to facilitate access to healthy food in resource-poor communities (facing socio-economic challenges) through the provision of low in-store food prices and increased availability, and through the marketing of healthy food products(Reference Madlala, Hill, Kunneke, Lopes and Faber33). Supermarkets utilise an array of marketing techniques aimed at influencing purchasing behaviour and increasing sales. For example, the traditional marketing mix is commonly employed and uses behaviour change levers related to the 4Ps – product, price, place, and promotion(Reference Cameron, Charlton, Ngan and Sacks34–Reference McCarthy, Shapiro and Perreault37) – as well as nudges(Reference Ferrari, Cavaliere, De Marchi and Banterle38,Reference Bauer, Aarestrup, Hansen and Reisch39) , and education(Reference Nikolaus, Muzaffar and Nickols-Richardson40). Studies exploring the impact of these levers as interventions in the supermarket context provide evidence to suggest they play a role in changing consumer behaviour, increasing consumer purchases of healthier foods(Reference Atanasova, Kusuma, Pineda, Frost, Sassi and Miraldo41–Reference Slapø, Schjøll, Strømgren, Sandaker and Lekhal45), and could have the potential to contribute to public health strategies aimed at improving population health(Reference Hartmann-Boyce, Bianchi, Piernas, Riches, Frie and Nourse36). However, authors reported limitations surrounding the findings, such as the inclusion of studies at high risk of bias(Reference Hartmann-Boyce, Bianchi, Piernas, Riches, Frie and Nourse36,Reference Shaw, Ntani, Baird and Vogel44) , low–moderate quality(Reference Adam and Jensen42,Reference Slapø, Schjøll, Strømgren, Sandaker and Lekhal45) , and studies that failed to examine how an increase in the purchase of a ‘healthier’ food item impacts sales of less healthy foods(Reference Karpyn, McCallops, Wolgast and Glanz43). Given that shoppers in high-income countries, including those living on low incomes, purchase most of the food they consume at home from supermarkets(Reference Bashir29,30,Reference Wu, Fuchs, Lian, Haldimann, Schneider and Mayer46) , the supermarket environment appears to offer the potential to influence health in these countries.
While obesity remains a key public health concern, another interwoven global issue is climate change(Reference An, Ji and Zhang47,Reference Trentinagli, Parolini, Donzelli and Olper48) . Evidence suggests that adherence to government recommendations around healthy eating, such as the Eatwell Guide in the UK(49), not only incurs benefits for health but can also reduce an individual’s environmental footprint through associated reductions in greenhouse gas (GHG) emissions(Reference Scheelbeek, Green, Papier, Knuppel, Alae-Carew and Balkwill50). Supermarkets may play a critical role, as one part of the wider food system, in helping to address climate change, since they have the capacity to influence purchasing behaviour and ultimately population diet(Reference Bauer, Aarestrup, Hansen and Reisch39).
Society tends to view environmental sustainability as a concern reserved for modestly wealthy individuals, typically of White ethnicity(Reference Pearson, Schuldt, Romero-Canyas, Ballew and Larson-Konar51). However, evidence suggests that the environmental concerns of those living on a low income and minority ethnic groups have been underestimated(Reference Pearson, Schuldt, Romero-Canyas, Ballew and Larson-Konar51,Reference Kemp and van Nunen52) . Qualitative research involving people experiencing food insecurity in the UK revealed this population held a good understanding of, and a desire to purchase, foods that were environmentally sustainable – for example, locally grown produce, food with less or recyclable packaging, and plant-based meat alternatives(Reference Hunter, Stone, Brown, Hardman, Johnstone and Greatwood53). Such findings suggest environmental sustainability is not a priority solely reserved for more affluent members of society. However, people experiencing FI reported the high price point of such food items presented a barrier to their purchase(Reference Hunter, Stone, Brown, Hardman, Johnstone and Greatwood53).
Systematic review evidence examining the effectiveness of interventions aimed at improving the dietary quality or environmental sustainability of diets within the supermarket context have historically focused on studies involving the general population(Reference Hartmann-Boyce, Bianchi, Piernas, Riches, Frie and Nourse36,Reference Adam and Jensen42,Reference Slapø, Schjøll, Strømgren, Sandaker and Lekhal45) , specific intervention types (e.g., nudges and choice architecture)(Reference Bauer, Aarestrup, Hansen and Reisch39,Reference Lindstrom, Tucker and McVay54) , or implications for policy(Reference Mah, Luongo, Hasdell, Taylor and Lo55,Reference Hodges, Lowery, Patel, McInnis and Zhang56) . However, to our knowledge, there is currently no in-depth exploration of the characteristics or the potential ‘active ingredients’(Reference Craig, Dieppe, Macintyre, Michie, Nazareth and Petticrew57) of supermarket-based interventions aimed at improving the healthiness and/or sustainability of diets within potentially vulnerable populations, i.e., those living with obesity or those on a low income(Reference Stone, Christiansen, Johnstone, Brown, Douglas and Hardman58). Therefore, this scoping review aimed to understand the characteristics of supermarket-based interventions, including what behaviour change levers and different combinations of levers have been implemented, to support healthier and/or more sustainable food purchasing for people living with obesity and overweight (PLWO/Ow) and/or FI in high-income countries.
Methods
The scoping review was undertaken following the Joanna Briggs Institute (JBI) Manual for Scoping Reviews(59) and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) extension for scoping reviews(Reference Tricco, Lillie, Zarin, O’Brien, Colquhoun and Levac60). The review software package Covidence(61) was used to manage data screening and extraction.
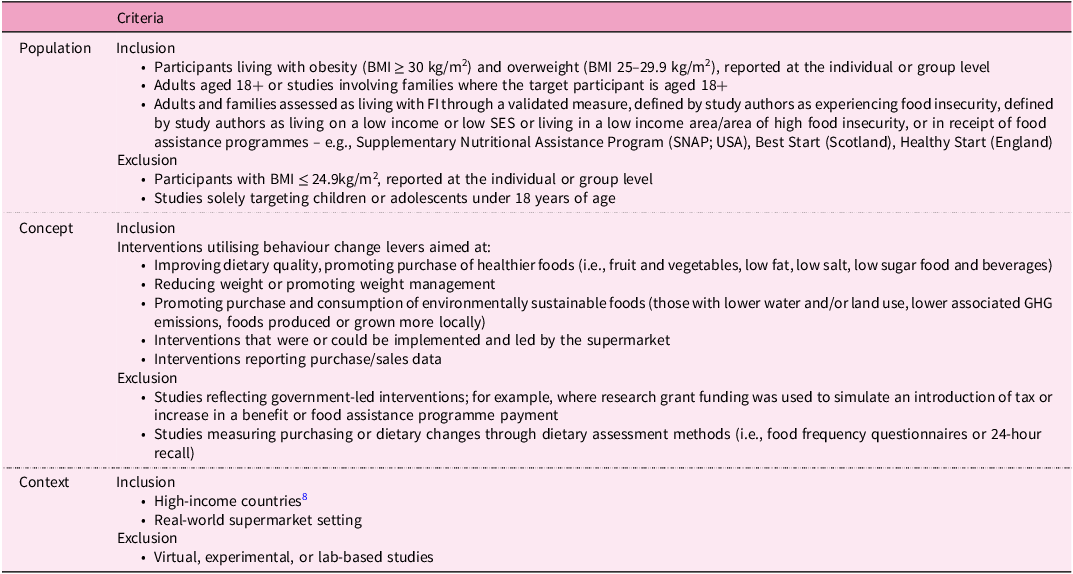
The population, concept, context (PCC) framework was used to identify the main components of the study research question, inclusion criteria, and to aid the development of the search strategy(59). As the study progressed, amendments were made to the research protocol and the PCC components; for example, the decision to include people living with overweight as well as obesity, the use of proxies for food insecurity, the exclusion of government-led or interventions unlikely to be implemented by supermarkets, i.e., cash incentives, and a requirement for studies to report objective purchasing or loyalty card data. The final PCC inclusion and exclusion criteria are outlined within Table 1.
PCC inclusion/exclusion criteria

The scoping review protocol was pre-registered on the Open Science Framework. (https://doi.org/10.17605/OSF.IO/3K8DN)
Search strategy, screening, and selection of evidence
The search strategy, focusing on supermarket, retail, or grocery store interventions within the context of food, was developed with assistance from an experienced librarian within Robert Gordon University.
The search strategy was adapted for each specific database and ran in Medline, Embase, CINAHL, Scopus, and Web of Science databases with relevant subject headings (i.e., ‘fruit’, ‘vegetables’, ‘obesity’, ‘consumer behaviour’, ‘diet’), selected to further refine the search results (see supplementary data 1). Databases were searched up to 16 October 2024. All resulting articles were uploaded to Covidence(61).
Published, peer-reviewed, primary research studies were included. Conference abstracts were excluded, along with study protocols and opinion papers. Studies published in any language were eligible for consideration where there was an abstract of the paper available in English. There were no restrictions regarding date range.
Eligible studies reported objectively measured purchasing, sales, or transaction data. Participants within the studies were required to be living with obesity or overweight (LWO/Ow; having a BMI ≥ 25 kg/m2, measured at the group, sub-group or individual level) and/or be experiencing FI. FI was required to be identified through a validated measure or defined by study authors using an established proxy measure (i.e., living on a low income, low SES, or in receipt of food assistance programmes such as the Supplementary Nutritional Assistance Program (SNAP) in the USA or Healthy Start in England)(Reference Loopstra, Reeves and Tarasuk62). Studies were required to include adults aged 18 and over or families where the target participant was aged 18 and above. Eligible studies involved supermarket-led interventions aimed at changing consumer purchasing behaviour using any behaviour change lever. Eligible studies often reported levers similar to those defined by Slapø et al(Reference Slapø, Schjøll, Strømgren, Sandaker and Lekhal45) (e.g., pricing, promotion, place) and therefore these definitions were adapted for use within the current review (supplementary data 2). Studies were required to be delivered in real-world physical supermarket settings and conducted in high-income countries.
Studies were excluded where (a) purchasing patterns were measured through self-report or food consumption; (b) a proportion of participants were described as food insecure or LWO/Ow, but failed to provide any accompanying sub-group analyses in relation to the intervention: (c) they were virtual or experimental; (d) they were conducted in mid-low income countries; or (e) they reflected government-led interventions – for example, where research grant funding was used to simulate an introduction of tax or increase in a benefit or food assistance programme payment.
All titles and abstracts were reviewed independently by two of three reviewers (E.H., H.C.G., R.A.S.) against the inclusion criteria. Abstracts selected for full text review were discussed by two reviewers and any disagreement settled through consensus with input from the third. Articles that met the approval of all three reviewers were subject to data extraction. E.H., H.C.G., and R.A.S. also conducted handsearching of the reference lists of studies identified for inclusion in the review.
Data extraction, analysis, and presentation of results
Data extraction was undertaken independently by two reviewers. Any disagreements were resolved through discussions with the third reviewer. Titles and abstracts of retrieved studies were reviewed and the full text of potentially relevant citations examined in greater detail. To aid the full text review, a data extraction form, developed by the research team and hosted in Covidence, captured details including author surname, year of publication, country, setting, study aim, participant characteristics (age, gender, ethnicity), food insecurity indicator, i.e., supermarket in an area of high deprivation, or indicator of obesity, i.e., area with high obesity prevalence, outcome measure, data collection methods, main findings, conclusions, and study funding. E.H., R.A.S., and H.C.G. transferred all extracted data collected via this form into an Excel spreadsheet, systematically organised according to the intervention behaviour change lever adapted from Slapø et al (supplementary data 2)(Reference Slapø, Schjøll, Strømgren, Sandaker and Lekhal45). Categorising the data in this manner helped synthesise the findings and enabled the identification and narrative description of similarities and differences across studies. Quality of evidence was not formally assessed; however, any limitations of the included studies, identified by reviewers during data extraction or highlighted by study authors, were considered and are reported in the Discussion. The extracted data were synthesised and the intervention characteristics (i.e., behaviour change levers and combinations of levers) are reported.
Results
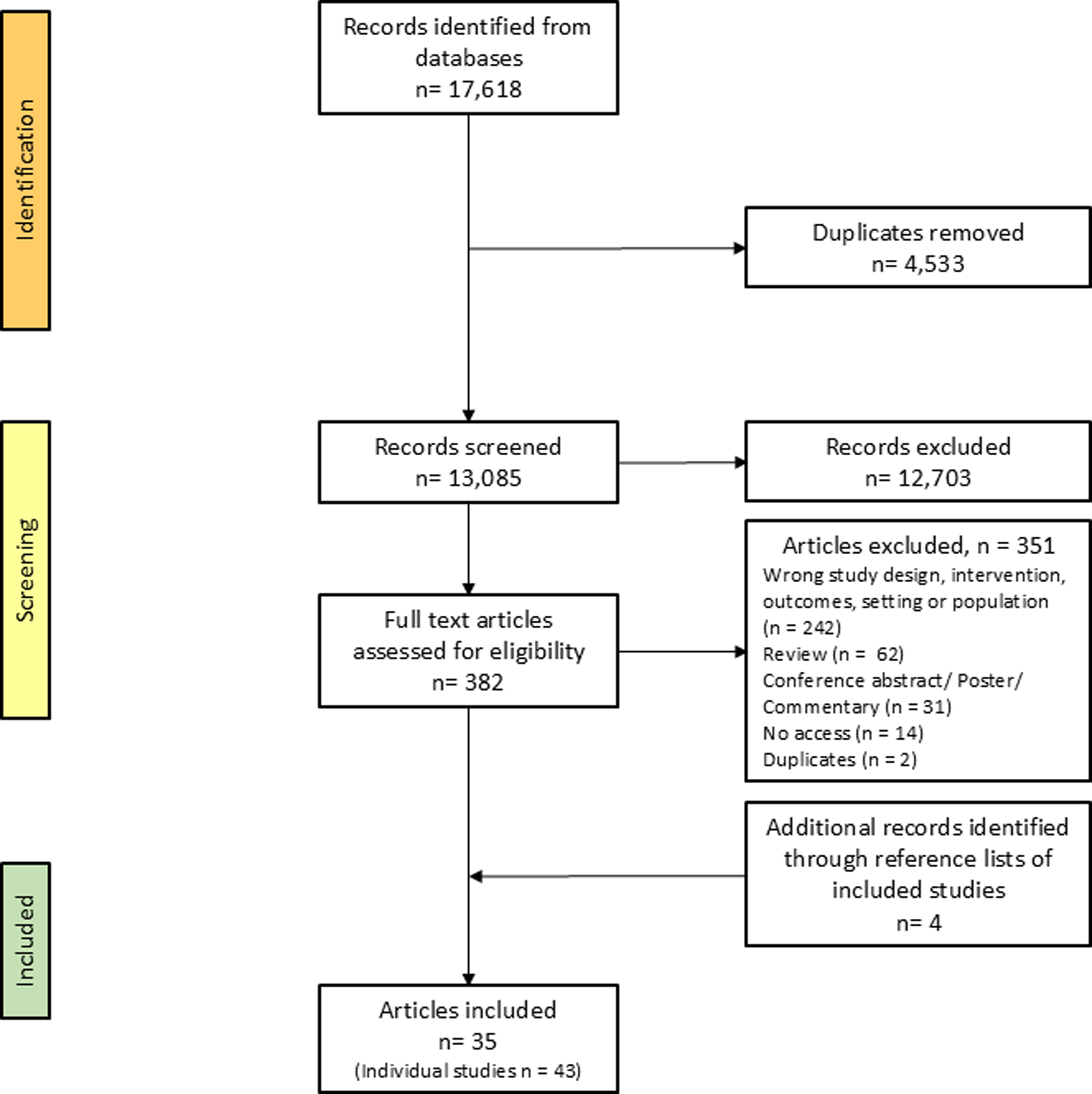
The initial search retrieved 17,618 articles. After removing duplicates, 13,085 titles and abstracts were screened by E.H., H.C.G., and R.A.S. A total of 382 full texts were assessed for eligibility, with 35 articles identified as suitable for inclusion (Figure 1). Three articles included multiple studies(Reference Huitink, Poelman, Seidell, Kuijper, Hoekstsra and Dijkstra63–Reference Piernas, Harmer and Jebb65), resulting in a total of 43 studies being included within the review. Included studies are summarised in supplementary Table 2.
Flow diagram of scoping review.

Characteristics of supermarket interventions
Studies were conducted in the USA (n = 19)(Reference Bernales-Korins, Ang, Khan and Geliebter66–Reference Phipps, Braitman, Stites, Wallace, Singletary and Hunt68,Reference Banerjee and Nayak70,Reference Polacsek, Moran, Thorndike, Boulos, Franckle and Greene72,Reference Moran, Khandpur, Polacsek, Thorndike, Franckle and Boulos74,Reference Melo, Zhen and Colson79,Reference Gustafson, Kent and Prate81,Reference Milliron, Woolf and Appelhans84–Reference Franckle, Levy, Macias-Navarro, Rimm and Thorndike88,Reference Payne and Niculescu90,Reference Phipps, Braitman, Stites, Singletary, Wallace and Hunt91,Reference Surkan, Tabrizi, Lee, Palmer and Frick93,Reference Adjoian, Dannefer and Willingham95–Reference Moran, Thorndike, Franckle, Boulos, Doran and Fulay97) , UK (n = 15)(Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Studies 1–3),Reference Piernas, Harmer and Jebb65 (Studies 1–6),Reference Thomas, Moore, Onuselogu, Dalton, Rains and Lowry69,Reference Nakamura, Suhrcke, Jebb, Pechey, Almiron-Roig and Marteau71,Reference Piernas, Harmer and Jebb75,Reference Vogel, Crozier, Penn-Newman, Ball, Moon and Lord76,Reference Stead, MacKintosh, Findlay, Sparks, Anderson and Barton92,Reference Trewern, Chenoweth, Christie and Halevy94) , the Netherlands (n = 7)(Reference Huitink, Poelman, Seidell, Kuijper, Hoekstsra and Dijkstra63 (Studies 1, 2), Reference Waterlander, de Boer, Schuit, Seidell and Steenhuis73,Reference Huitink, Poelman, Seidell, Pleus, Hofkamp and Kuin77,Reference Papies, Potjes, Keesman and van Koningsbruggen80,Reference Stuber, Lakerveld, Kievitsbosch, Mackenbach and Beulens82,Reference Huitink, Poelman, van Den Eynde, Seidell and Dijkstra83) , France (n = 1)(Reference Gamburzew, Darcel, Gazan, Dubois, Maillot and Tomé89), and Australia (n = 1)(Reference Ball, McNaughton, Le, Abbott, Stephens and Crawford78). While 39 studies explored interventions aimed at improving the healthiness of supermarket purchases made by PLWO/Ow and/or FI (i.e., increasing the purchase of fruit and vegetables, decreasing purchase of unhealthy snacks), three examined the impact of interventions aimed at increasing plant-based food items(Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Studies 1, 2),Reference Trewern, Chenoweth, Christie and Halevy94), and one study(Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Study 3)) aimed to increase purchases within both a healthy and environmentally sustainable food category (seasonal fruit and vegetables).
Study design
The majority (n = 21) were non-randomised experimental studies(Reference Huitink, Poelman, Seidell, Kuijper, Hoekstsra and Dijkstra63 (Studies 1, 2),Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Study 3),Reference Piernas, Harmer and Jebb65 (Studies 1–3, 5, 6),Reference Phipps, Braitman, Stites, Wallace, Singletary and Hunt68,Reference Thomas, Moore, Onuselogu, Dalton, Rains and Lowry69,Reference Moran, Khandpur, Polacsek, Thorndike, Franckle and Boulos74–Reference Huitink, Poelman, Seidell, Pleus, Hofkamp and Kuin77,Reference Papies, Potjes, Keesman and van Koningsbruggen80,Reference Huitink, Poelman, van Den Eynde, Seidell and Dijkstra83,Reference Gamburzew, Darcel, Gazan, Dubois, Maillot and Tomé89,Reference Payne and Niculescu90,Reference Surkan, Tabrizi, Lee, Palmer and Frick93,Reference Adjoian, Dannefer and Willingham95,Reference Gustafson, Ng and Jilcott Pitts96) . There were 15 randomised controlled trials(Reference Bernales-Korins, Ang, Khan and Geliebter66,Reference Geliebter, Ang, Bernales-Korins, Hernandez, Ochner and Ungredda67,Reference Banerjee and Nayak70,Reference Polacsek, Moran, Thorndike, Boulos, Franckle and Greene72,Reference Waterlander, de Boer, Schuit, Seidell and Steenhuis73,Reference Ball, McNaughton, Le, Abbott, Stephens and Crawford78,Reference Stuber, Lakerveld, Kievitsbosch, Mackenbach and Beulens82,Reference Milliron, Woolf and Appelhans84–Reference Franckle, Levy, Macias-Navarro, Rimm and Thorndike88,Reference Phipps, Braitman, Stites, Singletary, Wallace and Hunt91,Reference Stead, MacKintosh, Findlay, Sparks, Anderson and Barton92,Reference Moran, Thorndike, Franckle, Boulos, Doran and Fulay97) and seven observational studies(Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Studies 1, 2),Reference Piernas, Harmer and Jebb65 (Study 4),Reference Nakamura, Suhrcke, Jebb, Pechey, Almiron-Roig and Marteau71,Reference Melo, Zhen and Colson79,Reference Gustafson, Kent and Prate81,Reference Trewern, Chenoweth, Christie and Halevy94) . Only three studies evaluated interventions lasting longer than six months(Reference Piernas, Harmer and Jebb65 (Study 1),Reference Thomas, Moore, Onuselogu, Dalton, Rains and Lowry69,Reference Vadiveloo, Guan, Parker, Perraud, Buchanan and Atlas85) , while Nakamura and colleagues(Reference Nakamura, Suhrcke, Jebb, Pechey, Almiron-Roig and Marteau71) evaluated the impact of price-based interventions in supermarkets in the UK for one-year (individual intervention lengths not specified). Eighteen studies evaluated interventions lasting between three and six months(Reference Piernas, Harmer and Jebb65 (Studies 2,3,5,6),Reference Polacsek, Moran, Thorndike, Boulos, Franckle and Greene72–Reference Moran, Khandpur, Polacsek, Thorndike, Franckle and Boulos74,Reference Vogel, Crozier, Penn-Newman, Ball, Moon and Lord76,Reference Ball, McNaughton, Le, Abbott, Stephens and Crawford78,Reference Melo, Zhen and Colson79,Reference Milliron, Woolf and Appelhans84,Reference Foster, Karpyn, Wojtanowski, Davis, Weiss and Brensinger87–Reference Gamburzew, Darcel, Gazan, Dubois, Maillot and Tomé89,Reference Phipps, Braitman, Stites, Singletary, Wallace and Hunt91,Reference Surkan, Tabrizi, Lee, Palmer and Frick93,Reference Gustafson, Ng and Jilcott Pitts96,Reference Moran, Thorndike, Franckle, Boulos, Doran and Fulay97) , while the remaining 21 studies evaluated interventions that ran for fewer than three months. Eleven studies reported follow-up data(Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Studies 1–3),Reference Bernales-Korins, Ang, Khan and Geliebter66–Reference Phipps, Braitman, Stites, Wallace, Singletary and Hunt68,Reference Waterlander, de Boer, Schuit, Seidell and Steenhuis73,Reference Ball, McNaughton, Le, Abbott, Stephens and Crawford78,Reference Phipps, Braitman, Stites, Singletary, Wallace and Hunt91,Reference Stead, MacKintosh, Findlay, Sparks, Anderson and Barton92,Reference Trewern, Chenoweth, Christie and Halevy94) , ranging from four weeks(Reference Bernales-Korins, Ang, Khan and Geliebter66–Reference Phipps, Braitman, Stites, Wallace, Singletary and Hunt68) to six months(Reference Ball, McNaughton, Le, Abbott, Stephens and Crawford78).
Fourteen studies evaluated interventions delivered in a single store(Reference Huitink, Poelman, Seidell, Kuijper, Hoekstsra and Dijkstra63 (Study 1),Reference Phipps, Braitman, Stites, Wallace, Singletary and Hunt68,Reference Polacsek, Moran, Thorndike, Boulos, Franckle and Greene72,Reference Moran, Khandpur, Polacsek, Thorndike, Franckle and Boulos74,Reference Melo, Zhen and Colson79–Reference Gustafson, Kent and Prate81,Reference Huitink, Poelman, van Den Eynde, Seidell and Dijkstra83,Reference Milliron, Woolf and Appelhans84,Reference Vadiveloo, Guan, Parker, Perraud, Buchanan and Atlas85,Reference Franckle, Levy, Macias-Navarro, Rimm and Thorndike88,Reference Phipps, Braitman, Stites, Singletary, Wallace and Hunt91,Reference Stead, MacKintosh, Findlay, Sparks, Anderson and Barton92,Reference Moran, Thorndike, Franckle, Boulos, Doran and Fulay97) . Twelve studies involved between two and eight stores,(Reference Huitink, Poelman, Seidell, Kuijper, Hoekstsra and Dijkstra63 (Study 2),Reference Bernales-Korins, Ang, Khan and Geliebter66,Reference Geliebter, Ang, Bernales-Korins, Hernandez, Ochner and Ungredda67,Reference Banerjee and Nayak70,Reference Waterlander, de Boer, Schuit, Seidell and Steenhuis73,Reference Vogel, Crozier, Penn-Newman, Ball, Moon and Lord76,Reference Chapman, Burstein, Sadeghzadeh, Shepherd and De Marco86,Reference Foster, Karpyn, Wojtanowski, Davis, Weiss and Brensinger87,Reference Gamburzew, Darcel, Gazan, Dubois, Maillot and Tomé89,Reference Payne and Niculescu90,Reference Surkan, Tabrizi, Lee, Palmer and Frick93,Reference Adjoian, Dannefer and Willingham95) five included 10–49 stores(Reference Piernas, Harmer and Jebb65 (Studies 2–4),Reference Huitink, Poelman, Seidell, Pleus, Hofkamp and Kuin77,Reference Gustafson, Ng and Jilcott Pitts96) , three utilised 50–99 stores (Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Study 2),Reference Piernas, Harmer and Jebb65 (Study 6),Reference Trewern, Chenoweth, Christie and Halevy94), and five involved over 100 stores(Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Studies 1, 3),Reference Piernas, Harmer and Jebb65 (Studies 1, 5),Reference Piernas, Harmer and Jebb75). Three studies described the intervention being conducted in multiple supermarkets (number not specified)(Reference Thomas, Moore, Onuselogu, Dalton, Rains and Lowry69,Reference Nakamura, Suhrcke, Jebb, Pechey, Almiron-Roig and Marteau71,Reference Ball, McNaughton, Le, Abbott, Stephens and Crawford78) , while one study was conducted online and involved a single supermarket retail chain(Reference Stuber, Lakerveld, Kievitsbosch, Mackenbach and Beulens82). Of those conducted in multiple stores, 25 studies evaluated interventions involving a single supermarket chain(Reference Huitink, Poelman, Seidell, Kuijper, Hoekstsra and Dijkstra63 (Study 2),Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Studies 1–3),Reference Piernas, Harmer and Jebb65 (Studies 1–6),Reference Bernales-Korins, Ang, Khan and Geliebter66,Reference Geliebter, Ang, Bernales-Korins, Hernandez, Ochner and Ungredda67,Reference Thomas, Moore, Onuselogu, Dalton, Rains and Lowry69,Reference Banerjee and Nayak70,Reference Piernas, Harmer and Jebb75–Reference Ball, McNaughton, Le, Abbott, Stephens and Crawford78,Reference Stuber, Lakerveld, Kievitsbosch, Mackenbach and Beulens82,Reference Chapman, Burstein, Sadeghzadeh, Shepherd and De Marco86,Reference Gamburzew, Darcel, Gazan, Dubois, Maillot and Tomé89,Reference Payne and Niculescu90,Reference Surkan, Tabrizi, Lee, Palmer and Frick93,Reference Trewern, Chenoweth, Christie and Halevy94,Reference Gustafson, Ng and Jilcott Pitts96) , while four studies involved multiple supermarket retailers(Reference Nakamura, Suhrcke, Jebb, Pechey, Almiron-Roig and Marteau71,Reference Waterlander, de Boer, Schuit, Seidell and Steenhuis73,Reference Foster, Karpyn, Wojtanowski, Davis, Weiss and Brensinger87,Reference Adjoian, Dannefer and Willingham95) .
Population
Twenty-six studies involved people experiencing FI identified through established proxy measures (see Search strategy, screening, and selection of evidence)(Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Studies 1–3),Reference Piernas, Harmer and Jebb65 (Studies 1–6),Reference Phipps, Braitman, Stites, Wallace, Singletary and Hunt68,Reference Thomas, Moore, Onuselogu, Dalton, Rains and Lowry69,Reference Piernas, Harmer and Jebb75,Reference Vogel, Crozier, Penn-Newman, Ball, Moon and Lord76,Reference Ball, McNaughton, Le, Abbott, Stephens and Crawford78,Reference Melo, Zhen and Colson79,Reference Gustafson, Kent and Prate81,Reference Stuber, Lakerveld, Kievitsbosch, Mackenbach and Beulens82,Reference Chapman, Burstein, Sadeghzadeh, Shepherd and De Marco86–Reference Trewern, Chenoweth, Christie and Halevy94) , five studies focused on PLWO/Ow(Reference Bernales-Korins, Ang, Khan and Geliebter66,Reference Geliebter, Ang, Bernales-Korins, Hernandez, Ochner and Ungredda67,Reference Papies, Potjes, Keesman and van Koningsbruggen80,Reference Milliron, Woolf and Appelhans84,Reference Vadiveloo, Guan, Parker, Perraud, Buchanan and Atlas85) , and 12 studies included PLWO/Ow and FI(Reference Huitink, Poelman, Seidell, Kuijper, Hoekstsra and Dijkstra63 (Studies 1, 2),Reference Banerjee and Nayak70–Reference Moran, Khandpur, Polacsek, Thorndike, Franckle and Boulos74,Reference Huitink, Poelman, Seidell, Pleus, Hofkamp and Kuin77,Reference Huitink, Poelman, van Den Eynde, Seidell and Dijkstra83,Reference Adjoian, Dannefer and Willingham95–Reference Moran, Thorndike, Franckle, Boulos, Doran and Fulay97) . Where reported, participant characteristics revealed predominantly female participants aged 18 years and over.
Measures of FI and BMI
None of the included studies reported utilising a validated measure of FI; therefore, in 36 out of the 38 studies reporting on FI, FI was inferred from area-level characteristics (i.e., deprivation decile related to the geographical location of the study supermarket(s)(Reference Huitink, Poelman, Seidell, Kuijper, Hoekstsra and Dijkstra63 (Studies 1, 2),Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Studies 1–3),Reference Piernas, Harmer and Jebb65, (Studies 1–6),Reference Polacsek, Moran, Thorndike, Boulos, Franckle and Greene72,Reference Piernas, Harmer and Jebb75–Reference Huitink, Poelman, Seidell, Pleus, Hofkamp and Kuin77,Reference Gustafson, Kent and Prate81–Reference Huitink, Poelman, van Den Eynde, Seidell and Dijkstra83,Reference Chapman, Burstein, Sadeghzadeh, Shepherd and De Marco86–Reference Payne and Niculescu90,Reference Stead, MacKintosh, Findlay, Sparks, Anderson and Barton92,Reference Surkan, Tabrizi, Lee, Palmer and Frick93,Reference Adjoian, Dannefer and Willingham95,Reference Moran, Thorndike, Franckle, Boulos, Doran and Fulay97) , receiving government assistance, such as SNAP or the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) in the US(Reference Phipps, Braitman, Stites, Wallace, Singletary and Hunt68,Reference Moran, Khandpur, Polacsek, Thorndike, Franckle and Boulos74,Reference Gustafson, Ng and Jilcott Pitts96) or Healthy Start in the UK(Reference Thomas, Moore, Onuselogu, Dalton, Rains and Lowry69), low income(Reference Banerjee and Nayak70,Reference Melo, Zhen and Colson79,Reference Phipps, Braitman, Stites, Singletary, Wallace and Hunt91,Reference Trewern, Chenoweth, Christie and Halevy94) , or low socio-economic status(Reference Nakamura, Suhrcke, Jebb, Pechey, Almiron-Roig and Marteau71). Two studies directly recruited people with lower SES/low income using questionnaires(Reference Waterlander, de Boer, Schuit, Seidell and Steenhuis73,Reference Ball, McNaughton, Le, Abbott, Stephens and Crawford78) .
Participant BMI was reported in 17 studies(Reference Huitink, Poelman, Seidell, Kuijper, Hoekstsra and Dijkstra63 (Studies 1, 2),Reference Bernales-Korins, Ang, Khan and Geliebter66,Reference Geliebter, Ang, Bernales-Korins, Hernandez, Ochner and Ungredda67,Reference Banerjee and Nayak70–Reference Moran, Khandpur, Polacsek, Thorndike, Franckle and Boulos74,Reference Huitink, Poelman, Seidell, Pleus, Hofkamp and Kuin77,Reference Papies, Potjes, Keesman and van Koningsbruggen80,Reference Huitink, Poelman, van Den Eynde, Seidell and Dijkstra83–Reference Vadiveloo, Guan, Parker, Perraud, Buchanan and Atlas85,Reference Adjoian, Dannefer and Willingham95–Reference Moran, Thorndike, Franckle, Boulos, Doran and Fulay97) . In seven studies, BMI was not listed within the eligibility criteria but was collected through baseline questionnaires(Reference Banerjee and Nayak70,Reference Polacsek, Moran, Thorndike, Boulos, Franckle and Greene72–Reference Moran, Khandpur, Polacsek, Thorndike, Franckle and Boulos74,Reference Milliron, Woolf and Appelhans84,Reference Vadiveloo, Guan, Parker, Perraud, Buchanan and Atlas85,Reference Moran, Thorndike, Franckle, Boulos, Doran and Fulay97) . Six studies cited high obesity prevalence rates in the study geographical area(Reference Huitink, Poelman, Seidell, Kuijper, Hoekstsra and Dijkstra63 (Studies 1, 2),Reference Huitink, Poelman, Seidell, Pleus, Hofkamp and Kuin77,Reference Huitink, Poelman, van Den Eynde, Seidell and Dijkstra83,Reference Adjoian, Dannefer and Willingham95,Reference Gustafson, Ng and Jilcott Pitts96) . Three studies specifically recruited shoppers with a BMI > 25 kg/m2, self-reported in questionnaires(Reference Papies, Potjes, Keesman and van Koningsbruggen80) or initially calculated through self-reported height and weight during a screening phone call and later verified during a consultation in the participant’s supermarket(Reference Bernales-Korins, Ang, Khan and Geliebter66,Reference Geliebter, Ang, Bernales-Korins, Hernandez, Ochner and Ungredda67) . The remaining study reported data related to participant BMI; however, it is not clear how this information was collected(Reference Nakamura, Suhrcke, Jebb, Pechey, Almiron-Roig and Marteau71).
Behaviour change levers
Intervention details, including behaviour change levers and combinations of levers utilised in multi-lever interventions, are summarised in supplementary Table 3, alongside the main findings of the studies.
Price Eight studies considered the effect of price-based interventions on food purchasing habits: two studies for PLWO/Ow(Reference Bernales-Korins, Ang, Khan and Geliebter66,Reference Geliebter, Ang, Bernales-Korins, Hernandez, Ochner and Ungredda67) , two studies for people experiencing FI(Reference Phipps, Braitman, Stites, Wallace, Singletary and Hunt68,Reference Thomas, Moore, Onuselogu, Dalton, Rains and Lowry69) , and four studies for PLWO/Ow and FI(Reference Banerjee and Nayak70–Reference Waterlander, de Boer, Schuit, Seidell and Steenhuis73). Price-based interventions included percentage discount on selected products (commonly fresh fruit and vegetables), discount coupons, set price discount (i.e., $1 off a specific food item), and buy-one-get-one-free offers. Discounts applied automatically at the checkout were found to increase the purchase of fruit and vegetables(Reference Bernales-Korins, Ang, Khan and Geliebter66,Reference Geliebter, Ang, Bernales-Korins, Hernandez, Ochner and Ungredda67,Reference Polacsek, Moran, Thorndike, Boulos, Franckle and Greene72) ; however, coupons provided to be redeemed at a later date showed mixed results(Reference Phipps, Braitman, Stites, Wallace, Singletary and Hunt68–Reference Banerjee and Nayak70,Reference Waterlander, de Boer, Schuit, Seidell and Steenhuis73) .
Promotion Two studies considered the effect of promotions on food purchasing behaviour in FI(Reference Piernas, Harmer and Jebb65 (Study 6)) and in PLWO/Ow and FI(Reference Moran, Khandpur, Polacsek, Thorndike, Franckle and Boulos74). Promotions on bundles of ingredients to make healthy meals and on low sugar and sugar-free beverages involving shelf labels, free-standing displays, and point-of-purchase messages had no impact on sales in areas of high deprivation(Reference Piernas, Harmer and Jebb65,Reference Moran, Khandpur, Polacsek, Thorndike, Franckle and Boulos74) .
Placement Seven studies considered the effect of product placement on food purchasing behaviour: five studies for people experiencing FI(Reference Piernas, Harmer and Jebb65 (Studies 1–3),Reference Piernas, Harmer and Jebb75,Reference Vogel, Crozier, Penn-Newman, Ball, Moon and Lord76) and two studies in PLWO/Ow and FI(Reference Huitink, Poelman, Seidell, Kuijper, Hoekstsra and Dijkstra63 (Study 1),Reference Huitink, Poelman, Seidell, Pleus, Hofkamp and Kuin77). Removing or replacing unhealthy food items in specific store areas (i.e., checkout or high footfall areas) reduced the purchase of these items in the majority of studies(Reference Huitink, Poelman, Seidell, Kuijper, Hoekstsra and Dijkstra63 (Study 1),Reference Piernas, Harmer and Jebb65 (Studies 1, 2),Reference Piernas, Harmer and Jebb75,Reference Vogel, Crozier, Penn-Newman, Ball, Moon and Lord76) , but showed no effect on purchase patterns in two studies(Reference Piernas, Harmer and Jebb65 (Study 3),Reference Huitink, Poelman, Seidell, Pleus, Hofkamp and Kuin77).
Education Two studies considered the effect of education-based interventions (i.e., skill building newsletters, simplified labelling systems) on food purchasing behaviour in people experiencing FI and found no(Reference Ball, McNaughton, Le, Abbott, Stephens and Crawford78) or little effect(Reference Melo, Zhen and Colson79) on purchasing patterns.
Nudging Four studies reported findings from nudging strategies (i.e., point of decision prompts(Reference Gustafson, Kent and Prate81), an inlay indicating a place for vegetables in the shopping trolley(Reference Huitink, Poelman, van Den Eynde, Seidell and Dijkstra83)) on increasing healthier food purchasing behaviours: one in PLWO/Ow(Reference Papies, Potjes, Keesman and van Koningsbruggen80), two studies in people experiencing FI(Reference Gustafson, Kent and Prate81,Reference Stuber, Lakerveld, Kievitsbosch, Mackenbach and Beulens82) , and one study for PLWO/Ow and FI(Reference Huitink, Poelman, van Den Eynde, Seidell and Dijkstra83).
Results suggest, targeted(Reference Papies, Potjes, Keesman and van Koningsbruggen80), narrowly defined(Reference Gustafson, Kent and Prate81), informational nudges(Reference Stuber, Lakerveld, Kievitsbosch, Mackenbach and Beulens82) and a shopping trolley inlay(Reference Huitink, Poelman, van Den Eynde, Seidell and Dijkstra83) may play useful roles in encouraging healthier food purchases, but all studies were of short duration.
Multiple lever interventions Twenty studies explored the effect of multi-lever interventions: two studies involving PLWO(Reference Milliron, Woolf and Appelhans84,Reference Vadiveloo, Guan, Parker, Perraud, Buchanan and Atlas85) , 14 studies focusing on people experiencing FI(Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Studies 1–3),Reference Piernas, Harmer and Jebb65 (Studies 4, 5),Reference Chapman, Burstein, Sadeghzadeh, Shepherd and De Marco86–Reference Trewern, Chenoweth, Christie and Halevy94), and four studies involving PLWO/Ow and FI(Reference Huitink, Poelman, Seidell, Kuijper, Hoekstsra and Dijkstra63 (Study 2),Reference Adjoian, Dannefer and Willingham95–Reference Moran, Thorndike, Franckle, Boulos, Doran and Fulay97). Twelve studies investigated the impact of two intervention levers: education and price(Reference Vadiveloo, Guan, Parker, Perraud, Buchanan and Atlas85,Reference Phipps, Braitman, Stites, Singletary, Wallace and Hunt91,Reference Stead, MacKintosh, Findlay, Sparks, Anderson and Barton92,Reference Moran, Thorndike, Franckle, Boulos, Doran and Fulay97) , education and promotion(Reference Piernas, Harmer and Jebb65 (Study 4),Reference Milliron, Woolf and Appelhans84), price and promotion(Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Study 1)), placement and promotion(Reference Foster, Karpyn, Wojtanowski, Davis, Weiss and Brensinger87,Reference Adjoian, Dannefer and Willingham95) , placement and nudge(Reference Payne and Niculescu90), placement and price(Reference Huitink, Poelman, Seidell, Kuijper, Hoekstsra and Dijkstra63 (Study 2), Reference Piernas, Harmer and Jebb65 (Study5)). Seven studies investigated the impact of three intervention levers: education, placement, and promotion(Reference Gamburzew, Darcel, Gazan, Dubois, Maillot and Tomé89,Reference Surkan, Tabrizi, Lee, Palmer and Frick93) , education, promotion, and price(Reference Franckle, Levy, Macias-Navarro, Rimm and Thorndike88), placement, promotion, and price(Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Studies 2, 3),Reference Trewern, Chenoweth, Christie and Halevy94), placement, price, and nudges(Reference Chapman, Burstein, Sadeghzadeh, Shepherd and De Marco86). One study investigated the impact of four intervention levers: education, placement, promotion, and price(Reference Gustafson, Ng and Jilcott Pitts96).
Where reported, the rationale for the use of multi-lever interventions varied with selection based on encouraging findings from previous studies(Reference Chapman, Burstein, Sadeghzadeh, Shepherd and De Marco86,Reference Trewern, Chenoweth, Christie and Halevy94,Reference Gustafson, Ng and Jilcott Pitts96) , gaps in research(Reference Foster, Karpyn, Wojtanowski, Davis, Weiss and Brensinger87–Reference Gamburzew, Darcel, Gazan, Dubois, Maillot and Tomé89), testing a novel delivery mode(Reference Milliron, Woolf and Appelhans84), or specific framework(Reference Vadiveloo, Guan, Parker, Perraud, Buchanan and Atlas85,Reference Surkan, Tabrizi, Lee, Palmer and Frick93) (for more detailed information see supplementary data 3).
There was high heterogeneity in the operationalisation of the behaviour change levers themselves, the different combinations of levers utilised within the multi-lever studies, and the impact of these interventions in supporting healthy food purchasing patterns. Of the interventions designed to encourage the purchase of sustainable food items, two explored the impact of placement, promotion, and price levers(Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Study 1),Reference Trewern, Chenoweth, Christie and Halevy94) and another utilised price and promotion(Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Study 2)). These interventions had a greater influence on sales in stores located in less affluent areas; however, overall sales of the sustainable food items remained lower compared to sales in more affluent stores/areas (supplementary Table 3).
Figure 2 provides an overview of the number of studies using each of the different behaviour change levers and the number of interventions that targeted PLWO/Ow, those experiencing FI, or both, intervention length, number of stores, and follow-up.
Donut plot summarising study characteristics.
PLWO/Ow: People living with obesity or overweight; FI: food insecurity; N.I: no information

Discussion
This scoping review aimed to report on the characteristics of supermarket-based interventions that encouraged the purchase of healthier and more environmentally sustainable food in PLWO/Ow and/or FI using previously described proxy measures (see Search strategy, screening, and selection of evidence). A total of 35 articles (43 studies) reporting interventions from high-income countries were included. These described interventions utilising behaviour change levers including price, promotion, placement, nudges, and education, or a combination of these. The included studies illuminate challenges in understanding the optimal characteristics of studies aimed at supporting the purchase of healthy and environmentally sustainable food in this population.
Our search and screening processes revealed no eligible studies that involved people experiencing FI defined using a validated measure (e.g., the Food Insecurity Experience Scale(98) or the US Household Food Security Survey Module)(99). Nevertheless, broadening the inclusion criteria and using area-level demographic data related to characteristics associated with FI(Reference Loopstra, Reeves and Tarasuk62) helped mitigate this. As previously described, most studies used area-level data related to supermarket store location to identify their sample; however, some studies used specific strategies to recruit participants in receipt of government food assistance, such as in-store recruitment on days that aligned with monthly SNAP benefit payments(Reference Polacsek, Moran, Thorndike, Boulos, Franckle and Greene72) and offering top-up vouchers for £2 off fruit and vegetables to customers who presented a Healthy Start Voucher at the supermarket checkout(Reference Thomas, Moore, Onuselogu, Dalton, Rains and Lowry69). Supermarkets do not typically collect information relating to sensitive issues such as the receipt of government food assistance, and the difficulties in collecting such data through surveys are acknowledged(Reference Moore, Stinson and Welniak100,Reference Yan101) . This presents a challenge for supermarkets in determining and delivering the most effective interventions to support these populations.
Where retailers are unable to identify those in most need of support, they might use their limited budget on broad strategies such as offering a nationwide discount on specific healthy food items. While this approach may reach many consumers, the budget is spread very thin and the campaign or health promotion may only be beneficial for those consumers already motivated to make healthy choices. However, were supermarkets able to identify certain groups of consumers – i.e., those living on a low income – the same funds could be used to create targeted campaigns, deals, or offers tailored to this group, which could lead to a greater health impact for the target population. Similar sensitivities present when capturing height and weight data within the supermarket context to allow for the calculation of BMI(Reference Gorber, Tremblay, Moher and Gorber102,Reference Spencer, Appleby, Davey and Key103) . Potentially reflecting such challenges, only five studies included within this review had eligibility criteria that required participants to self-identify as a PLWO/Ow(Reference Bernales-Korins, Ang, Khan and Geliebter66,Reference Geliebter, Ang, Bernales-Korins, Hernandez, Ochner and Ungredda67,Reference Papies, Potjes, Keesman and van Koningsbruggen80) and/or FI(Reference Waterlander, de Boer, Schuit, Seidell and Steenhuis73,Reference Ball, McNaughton, Le, Abbott, Stephens and Crawford78) . However, it may not be pertinent to target supermarket-based interventions aimed at supporting the purchase of healthy, sustainable foods specifically towards PLWO. Data from the UK National Diet and Nutrition Survey revealed that only 33% of adults in the UK consumed the recommended five portions of fruit and vegetables a day(104). Data from the US Centers for Disease Control and Prevention (CDC) suggest that only 12.3% of adults in the USA meet fruit recommendations while 10% meet vegetable recommendations(Reference Lee, Moore, Park, Harris and Blanck105). Diet-related health concerns extend beyond overweight and obesity to other considerations – for example, cardiovascular disease and micronutrient deficiencies(Reference Mozaffarian106). Therefore, supermarket-based interventions to encourage the purchasing of healthier, more environmentally sustainable food may provide health benefits for all citizens, regardless of their BMI.
This scoping review highlighted a scarcity of literature focusing on interventions aimed at improving the environmental sustainability of supermarket purchases of PLWO/Ow and/or FI. Previous studies have primarily focused on promoting the purchase of healthier foods for their health benefits(Reference Luick, Bandy, Piernas, Jebb and Pechey64), without considering the associated environmental-related benefits(Reference Scheelbeek, Green, Papier, Knuppel, Alae-Carew and Balkwill50,Reference Clark, Springmann, Hill and Tilman107) . This may be driven by complexities surrounding measurement, classification, and also level of importance to the target population.
Measuring the environmental sustainability of different food and drink is challenging(Reference Clune, Crossin and Verghese108). Sustainability encompasses many facets, such as biodiversity, GHG emissions, and land and water use(Reference Brown, Harris, Potter and Knai109). Studies attempting to capture data on the environmental sustainability of food often utilise different methodologies, lack consideration of temporal or regional differences, focus only on specific food products, and do not cover all available food items(Reference Clune, Crossin and Verghese108). Another potential reason for a lack of studies exploring the purchase of environmentally sustainable foods may relate to the lack of any legal universal definition around what constitutes such a product(Reference Stone, Brown, Douglas, Greatwood, Griffiths and Hunter110). There is a paucity of data to allow the identification (and promotion) of a ‘more sustainable choice’ within specific food categories, and strict constraints have been set by the Competition and Markets Authority (CMA) to improve the accuracy of environmental reporting and prevent ‘greenwashing’ (i.e., making false statements about the environmental sustainability of a product)(111). Retailers rely on proxy measures, provided by manufacturers, such as certification schemes (e.g., Fair Trade or B Corp) to indicate different elements of sustainability for a food product that they could use for marketing purposes(Reference Stone, Brown, Douglas, Greatwood, Griffiths and Hunter110,112) . However, products labelled as ‘environmentally sustainable’ based on proxy measures tend to cost more compared to non-accredited alternatives(Reference Griffiths113). Therefore, despite expressing a desire to engage in environmentally sustainable shopping practices, such purchasing patterns may be impossible for those living on a low income(Reference Hunter, Stone, Brown, Hardman, Johnstone and Greatwood53).
In studies involving consumers living on a low income or shopping within a low income area, or minority ethic groups, researchers may have deemed environmental sustainability to be of less importance to these populations, mirroring societal views of environmental sustainability as a concern reserved for more affluent members of society(Reference Pearson, Schuldt, Romero-Canyas, Ballew and Larson-Konar51). Notably, the three studies included in the current review that focused on improving the environmental sustainability of diets through the promotion of plant-based meat and milk alternatives reported the greatest intervention effects in supermarkets situated in below-average affluence areas; however, increases in purchases were not enough to bring sales in line with stores located in more affluent areas(Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Studies 1, 2),Reference Trewern, Chenoweth, Christie and Halevy94). While population-level interventions to improve the environmental sustainability of diets using price, promotion, and placement levers might not worsen existing health inequalities, they may be unlikely to reduce them(Reference Luick, Bandy, Piernas, Jebb and Pechey64). Systematic review evidence, including sub-group analysis on low SES consumers, suggested price, either on its own or in combination with other levers, was the most effective strategy at increasing sales of healthy foods(Reference Brooker, Howlett, Brindal and Hendrie114).
However, the operationalisation of all levers included in the current review were not identical. For example, price, the most commonly utilised lever, was operationalised through the use of coupons to the value of a set amount(Reference Phipps, Braitman, Stites, Wallace, Singletary and Hunt68–Reference Banerjee and Nayak70,Reference Vadiveloo, Guan, Parker, Perraud, Buchanan and Atlas85,Reference Franckle, Levy, Macias-Navarro, Rimm and Thorndike88,Reference Stead, MacKintosh, Findlay, Sparks, Anderson and Barton92,Reference Gustafson, Ng and Jilcott Pitts96) , percentage reductions(Reference Huitink, Poelman, Seidell, Kuijper, Hoekstsra and Dijkstra63 (Study 2),Reference Bernales-Korins, Ang, Khan and Geliebter66,Reference Geliebter, Ang, Bernales-Korins, Hernandez, Ochner and Ungredda67,Reference Waterlander, de Boer, Schuit, Seidell and Steenhuis73,Reference Chapman, Burstein, Sadeghzadeh, Shepherd and De Marco86,Reference Phipps, Braitman, Stites, Singletary, Wallace and Hunt91,Reference Moran, Thorndike, Franckle, Boulos, Doran and Fulay97) , set price reductions(Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Studies 1, 2),Reference Piernas, Harmer and Jebb65 (Study 5)), multibuy offers(Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Study 3),Reference Polacsek, Moran, Thorndike, Boulos, Franckle and Greene72), and price parity thresholds(Reference Trewern, Chenoweth, Christie and Halevy94); therefore, we recommend that these should not be interpreted interchangeably. Heterogeneity of the studies was also present in relation to the different combinations of levers included in multi-lever interventions. Therefore, despite study findings suggesting the potential effectiveness of price, placement, nudge, and various different combinations of levers (supplementary Table 3), taken together, the high heterogeneity presents challenges in ascertaining exactly what intervention characteristics may be best placed to support PLWO/Ow and/or FI. Another challenge in identifying what behaviour change levers may be most effective is the supermarket environment itself(Reference Gustafson, Kent and Prate81,Reference Huitink, Poelman, van Den Eynde, Seidell and Dijkstra83,Reference Vadiveloo, Guan, Parker, Perraud, Buchanan and Atlas85,Reference Chapman, Burstein, Sadeghzadeh, Shepherd and De Marco86,Reference Franckle, Levy, Macias-Navarro, Rimm and Thorndike88,Reference Payne and Niculescu90) . Real-world supermarket environments are busy, filled with promotions, deals, and offers(Reference Franckle, Levy, Macias-Navarro, Rimm and Thorndike88). In the USA, supermarkets typically stock over 37,000 products(115). When we consider the various price-based strategies that retailers (often simultaneously) use (i.e., everyday low prices, loyalty card discounts/rewards, and price matches), it becomes apparent that price-based interventions could be overlooked by the customer(Reference Franckle, Levy, Macias-Navarro, Rimm and Thorndike88). Within the busy supermarket environment, trying to determine the best prices whilst also attempting to read and interpret nutritional information could lead to cognitive overload, and impair consumer decision-making(Reference Ammerman, Hartman and DeMarco116). Even when armed with shopping lists, meal plans, or expressing a conscious desire to make healthier choices, cognitive overload may lead consumers to make less healthy purchasing decisions(Reference Dhuria, Lawrence and Crozier117). Cognitive overload may be greater for those living on lower incomes, whose financial concerns may consume finite mental resources(Reference Mani, Mullainathan, Shafir and Zhao118), and could further reduce engagement with health-promoting behaviours(Reference Kraft and Kraft119,Reference Sheehy-Skeffington, Jetten and Peters120) . Interventions targeting unconscious, automatic processes rather than deliberate conscious decision-making may therefore be more beneficial, especially for those experiencing FI. Supermarket interventions that tap into unconscious decision-making processes – for example, through placement or nudging – may play an important role in a multifaceted public health approach to reduce diet-related disease and lower the environmental impact of the food we purchase and consume(Reference Bauer, Aarestrup, Hansen and Reisch39). While studies included within the current review explore the influence of such levers, the majority are short in duration (supplementary Table 2) and longer-term trials are required. Vandenbroele et al.(Reference Vandenbroele, Vermeir, Geuens, Slabbinck and Van Kerckhove121) also highlighted the potential of using a nudge behaviour change lever to foster more environmentally friendly purchases, although acknowledged that individual attitudes towards sustainability are also an important driver of food choice(Reference Vandenbroele, Vermeir, Geuens, Slabbinck and Van Kerckhove121). Similarly, Ferrari and colleagues(Reference Ferrari, Cavaliere, De Marchi and Banterle38) suggested that nudging, as part of a multitiered intervention approach, could be an encouraging tool to supplement food policies geared toward sustainable food systems. To explore and understand the use of specific behaviour change levers and the ‘active ingredients’ of the intervention(Reference Hunter, Stone, Brown, Hardman, Johnstone and Greatwood53), the rationale for the use of multiple levers, based on well-conducted research or theory, should be clearly stated.
Within the included studies, there was often no consideration of any unintended consequences of reducing the price of healthier food on shoppers’ overall purchases. While a price reduction intervention may lead to an increase in the purchase of healthier foods, there is some evidence to suggest that this may also be accompanied by either no change or an increase in the purchase of less healthy food items for those of low SES(Reference Brooker, Howlett, Brindal and Hendrie114). Encouragingly, one study in the current review reported that money saved from discounts was not spent on food items from other categories(Reference Waterlander, de Boer, Schuit, Seidell and Steenhuis73), while another, removing confectionary from prominent in-store locations, found no indication that shoppers purchased similar items elsewhere in the store to compensate(Reference Piernas, Harmer and Jebb75). However, Piernas and colleagues acknowledge this study explored behaviours across one supermarket chain and so consumers may have purchased confectionary elsewhere(Reference Piernas, Harmer and Jebb75). Additionally, while empirical evidence is lacking, price promotions could potentially increase the purchase and overconsumption of foods, irrespective of their healthfulness, which is something that researchers, policymakers, and retailers may need to be mindful of when developing and evaluating interventions. Interventions delivered in the supermarket that target specific food categories or items may impact wider shopping behaviours, and wider changes in purchasing patterns should be considered and reported on by researchers wherever possible.
Any impact of the intervention may be limited to the intervention period only. Eleven studies provided follow-up data post-intervention, with only one reporting a sustained effect (defined as evidence of the intervention’s continued impact on purchases at a specified follow-up period) of the intervention on the purchase of environmentally sustainable food items(Reference Trewern, Chenoweth, Christie and Halevy94). Two studies reported partially sustained effects(Reference Geliebter, Ang, Bernales-Korins, Hernandez, Ochner and Ungredda67,Reference Phipps, Braitman, Stites, Wallace, Singletary and Hunt68) , while seven studies found no sustained effect(Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Studies 1–3),Reference Bernales-Korins, Ang, Khan and Geliebter66,Reference Waterlander, de Boer, Schuit, Seidell and Steenhuis73,Reference Phipps, Braitman, Stites, Singletary, Wallace and Hunt91,Reference Stead, MacKintosh, Findlay, Sparks, Anderson and Barton92) . One further study reported no effect during, post-intervention, or at follow-up(Reference Ball, McNaughton, Le, Abbott, Stephens and Crawford78). Interventions may be required to continue in the longer term, raising questions about funding and economic viability(Reference Brooker, Howlett, Brindal and Hendrie114). Studies in the current review called for a consideration of the economic costs associated with interventions for both researchers and retailers(Reference Huitink, Poelman, Seidell, Kuijper, Hoekstsra and Dijkstra63,Reference Waterlander, de Boer, Schuit, Seidell and Steenhuis73,Reference Moran, Khandpur, Polacsek, Thorndike, Franckle and Boulos74,Reference Vogel, Crozier, Penn-Newman, Ball, Moon and Lord76,Reference Melo, Zhen and Colson79,Reference Foster, Karpyn, Wojtanowski, Davis, Weiss and Brensinger87,Reference Franckle, Levy, Macias-Navarro, Rimm and Thorndike88,Reference Payne and Niculescu90,Reference Phipps, Braitman, Stites, Singletary, Wallace and Hunt91,Reference Gustafson, Ng and Jilcott Pitts96) and the safeguarding of government funds for healthy-eating incentives to assist those living on a low income(Reference Thomas, Moore, Onuselogu, Dalton, Rains and Lowry69). Three studies, using a nudge lever to effectively increase healthy(Reference Gustafson, Kent and Prate81,Reference Chapman, Burstein, Sadeghzadeh, Shepherd and De Marco86) or reduce less healthy food purchases(Reference Papies, Potjes, Keesman and van Koningsbruggen80), were described as being ‘low cost’ to retailers in terms of delivery and implementation; however, details related to the specific costs associated with delivering an intervention were scarce and only reported in two other studies(Reference Geliebter, Ang, Bernales-Korins, Hernandez, Ochner and Ungredda67,Reference Ball, McNaughton, Le, Abbott, Stephens and Crawford78) . Information on the cost-effectiveness of these interventions was not available(Reference Geliebter, Ang, Bernales-Korins, Hernandez, Ochner and Ungredda67,Reference Ball, McNaughton, Le, Abbott, Stephens and Crawford78) . Adjoian et al.(Reference Adjoian, Dannefer and Willingham95) found that a decrease in purchases of less healthy food items at a healthy checkout counter (where all unhealthy snacks were substituted with healthy alternatives), compared to controls, was accompanied by a decrease in spending at the checkout(Reference Adjoian, Dannefer and Willingham95). The operational costs of introducing even a single trial, coupled with concerns around potential decreases in sales, may present a financial risk that supermarkets are unwilling to accept(Reference Huitink, Poelman, Seidell, Kuijper, Hoekstsra and Dijkstra63,Reference Luick, Bandy, Piernas, Jebb and Pechey64) . For example, Brooker and colleagues found discounts on healthy food and drinks of between 20% and 50% were required to ensure intervention effectiveness; however, they argued it is unclear whether such large discounts are sustainable for retailers in the long term(Reference Brooker, Howlett, Brindal and Hendrie114). Researchers need to be mindful of the commercial requirements faced by retailers(Reference Stone, Brown, Douglas, Greatwood, Griffiths and Hunter110,Reference Gravlee, Boston, Mitchell, Schultz and Betterley122) . Interventions aimed at maximising benefits for public health whilst simultaneously working to de-risk or mitigate potential losses and maintain supermarket profit margins – i.e., those which level the playing field between retailers, such as the high-fat salt or sugar (HFSS) legislation introduced across England from 2024(123,124) – are likely to be more acceptable to retailers and may help facilitate good working relationships with academia, something that has been acknowledged as being challenging(Reference Luick, Bandy, Piernas, Jebb and Pechey64,Reference Chapman, Burstein, Sadeghzadeh, Shepherd and De Marco86) . Supermarkets may also be reluctant to participate in research or collaborate with academia due to working to different timescales, with industry often requiring quick results(Reference Barnes, Pashby and Gibbons125), or concerns around the commercial sensitivity of data sharing and customer privacy(Reference Luick, Bandy, Piernas, Jebb and Pechey64). Additionally, the investment required by the retailer in terms of the staff, time, and resources to work on trials and share data can be substantial, can take them away from other commercial and legislative priorities, and is often underestimated by academics. Within the studies included in the current review, researchers reported challenges related to intervention implementation, including staff misunderstanding, difficulties gathering and analysing data, and different practices and priorities between academics and retailers(Reference Chapman, Burstein, Sadeghzadeh, Shepherd and De Marco86,Reference Phipps, Braitman, Stites, Singletary, Wallace and Hunt91,Reference Stead, MacKintosh, Findlay, Sparks, Anderson and Barton92) . Recommendations for researchers planning to conduct studies involving supermarkets centre on fostering and maintaining good relationships, having detailed data sharing agreements in place(Reference Chapman, Burstein, Sadeghzadeh, Shepherd and De Marco86), providing reassurance to retailers around researcher impartiality, and regularly sharing results with retailers(Reference Stead, MacKintosh, Findlay, Sparks, Anderson and Barton92). Despite the reported difficulties, studies in the current review provide proof of concept that collaborations between researchers and food retailers can be successfully established(Reference Piernas, Harmer and Jebb65,Reference Thomas, Moore, Onuselogu, Dalton, Rains and Lowry69,Reference Piernas, Harmer and Jebb75) .
Limitations
The lack of studies using validated measures of FI or BMI of participants and the use of area-level data as a proxy for such outcomes are potentially problematic. Not everyone residing in, or shopping at a supermarket within, an area of high deprivation or high obesity prevalence are living on a low income or living with obesity(126). Therefore, the use of area-level data may not provide the required granularity(Reference Luick, Bandy, Piernas, Jebb and Pechey64). To develop feasible and acceptable interventions, we need to ensure people with the relevant lived experience are recruited into the research. Ways to collect sensitive information, such as FI experience, to facilitate the involvement of the target population should be considered by those undertaking supermarket-based research to ensure the findings are applicable to support these populations to purchase healthier and more environmentally sustainable food.
Studies often had small sample sizes, with 14 studies involving a single supermarket (see supplementary Table 2), which presents difficulties in generalising study findings more widely or evaluating the ease of scaling up the intervention. Additionally, studies tended to have a relatively short duration, with 33 studies lasting less than six months (see supplementary Table 2). Indeed, exposure to an intervention may determine customer engagement. One study found frequent shoppers reported higher awareness of the intervention compared to those who shopped less often during the intervention period(Reference Gamburzew, Darcel, Gazan, Dubois, Maillot and Tomé89), suggesting repeated exposure to an in-store campaign may be necessary. Intervention length must be given careful consideration and intervention developers must be mindful that some consumers may only shop in a supermarket on a monthly basis(Reference Gamburzew, Darcel, Gazan, Dubois, Maillot and Tomé89,Reference Surkan, Tabrizi, Lee, Palmer and Frick93) .
Another limitation of the included studies is a lack of data surrounding fidelity. Fidelity is an important consideration required to allow a thorough evaluation of any intervention. This can be an issue when collaborating with supermarkets to evaluate and analyse retrospectively collected data on interventions previously conducted in store designed and delivered by supermarkets(Reference Luick, Bandy, Piernas, Jebb and Pechey64,Reference Piernas, Harmer and Jebb65) . The review was limited to studies reported and published in academic journals, and therefore does not capture data on supermarket-led interventions delivered and evaluated internally by the retailer. Finally, it should be highlighted that some studies were undertaken during 2020 and 2021 and were likely to be impacted by the Covid-19 pandemic(Reference Luick, Bandy, Piernas, Jebb and Pechey64 (Studies 1–3),Reference Thomas, Moore, Onuselogu, Dalton, Rains and Lowry69,Reference Trewern, Chenoweth, Christie and Halevy94) . Luick and colleagues(Reference Luick, Bandy, Piernas, Jebb and Pechey64) reported that a visual inspection of the data relating to the studies they analysed suggested that, during Covid-19, purchasing patterns in supermarkets changed, possibly due to an increase in the number of people buying products from local grocery stores(127) and the closure of hospitality. The two remaining studies detailed altering their data analysis plans to mitigate the impact of Covid-19 on study outcomes(Reference Thomas, Moore, Onuselogu, Dalton, Rains and Lowry69,Reference Trewern, Chenoweth, Christie and Halevy94) .
Conclusion
Supermarket-based interventions aimed at supporting the purchase of healthy and/or sustainable food for PLWO/Ow and/or FI in high-income countries often rely on proxy measures to identify these population groups. This broad approach probably means those without the relevant lived experience are included and may make it challenging for researchers to ensure study findings accurately reflect the purchasing behaviour of the target population. Specifically, there is a research gap in supporting those living with FI, where valid measures of assessing FI are applied. The interventions included in the review have been delivered in busy supermarket environments within which customers with financial concerns may be under greater cognitive burden and, therefore, are potentially less likely to engage. Furthermore, studies have employed a variety of behaviour change levers, including price, promotion, placement, nudges, and education, operationalised in numerous ways and in different combinations, making it difficult to establish the most effective lever or combination of levers that should be utilised. All of this presents substantial challenges for researchers and retailers in gathering data to inform public health policy and develop commercially focused guidance for the implementation of equitable interventions that best support the purchase of healthy and sustainable food for PLWO/Ow and/or FI.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954422426100377
Acknowledgements
The authors would like to acknowledge the late Colin MacLean, Liaison Librarian from Robert Gordon University, who provided guidance on the search strategy for the scoping review.
Authorship
E.H. developed the scoping review research question, performed database searches, compiled literature to be screened, screened literature for study inclusion or exclusion, and contributed to writing the manuscript. H.C.G and R.A.S. screened literature for study inclusion or exclusion, extracted data from included articles, and contributed to writing the manuscript. F.D. provided guidance on the development of the scoping review questions and contributed to writing the manuscript. A.M.J., C.A.H., C.G., M.L., M.G., N.S., and M.T. contributed to the writing of the manuscript. All authors reviewed and approved the final manuscript.
Financial support
This research was funded through the Transforming the UK Food System for Healthy People and a Healthy Environment SPF Programme, delivered by UKRI, in partnership with the Global Food Security Programme, BBSRC, ESRC, MRC, NERC, Defra, DHSC, OHID, Innovate UK, and FSA. FIO Food is grant award BB/W018021/1. E.H. was supported by Robert Gordon University. The funder had no role in the design, analysis, or writing of this article.
Competing interests
E.H., R.A.S., H.C.G., F.D., C.G., M.L., M.G, N.S., and M.T. report no conflicts of interest. A.M.J. holds a voluntary Advisory Committee role with the British Nutrition Foundation. C.A.H. declares research funding from the American Beverage Association (paid to institution), primary supervision on a PhD studentship funded by Coca-Cola, and personal honoraria from the International Sweeteners Association and International Food Information Council for work unrelated to the submitted abstract.
A preprint of an earlier version of this paper is available at https://doi.org/10.31219/osf.io/szbgc_v1.




 Open access
Open access