


Chronic obstructive pulmonary disease (COPD) is marked by breathing difficulties, cough and sputum production resulting from abnormalities in the airways or alveoli. It leads to a progressively worsening and irreversible airflow limitation, significantly affecting patients’ quality of life and imposing a burden on healthcare systems. According to the WHO, COPD is expected to rank as the third most common cause of death globally by 2030(1). Therefore, the management of COPD becomes a critical public health issue. The main environmental exposures for COPD include tobacco smoke and toxic particles and gases from indoor and outdoor air pollution. Tobacco smoke contains numerous harmful chemicals that can cause airway inflammation, oxidative stress (OS) and cellular damage, ultimately limiting airflow and declining lung function(Reference Higham, Bostock and Booth2). Despite efforts to prevent COPD, such as reducing smoke exposure, many smokers still face high odds of this disease. Host-immune factors are also among the contributors to the development of COPD(Reference Lareau, Fahy and Meek3).
Some studies have demonstrated that increased OS often leads to reduced antioxidants in COPD patients. OS refers to the disruption of the cellular redox balance in cells or organisms due to excessive production of oxidative substances or diminished ability to remove them. It can cause inflammation and cellular damage(Reference Luu, Wen and Li4). OS is mainly caused by an excess of free radicals. Previous studies have confirmed that dietary antioxidants can neutralise free radicals, reduce OS and enhance the body’s resistance to pathogens, thus alleviating pulmonary inflammation and preventing respiratory diseases such as COPD(Reference Schulze, Martínez-González and Fung5). Such nutrient antioxidants as vitamins A, C, E, Mg, Zn and Se are commonly assessed in the Dietary Antioxidant Quality Score (DAQS)(Reference Tur, Serra-Majem and Romaguera6). A study by Aghajani et al. (Reference Aghajani, Wong and Azimi7) suggested a negative correlation between DAQS and the severity of COVID-19 infection. A USA study also demonstrated a potential association between increased dietary niacin intake and reduced odds of COPD in aged, middle-aged and older adults(Reference Shi, Pu and Zhang8). Additionally, a study has indicated that diets rich in vitamins, fibre, fruits and vegetables are more effective in reducing the odds of COPD(Reference Blaner, Shmarakov and Traber9), as they contain a high level of antioxidant vitamins. Conversely, poor-quality diets lacking high-quality proteins, minerals and fibre-rich fruits and vegetables are related to a higher odds of chronic respiratory diseases(Reference Li, Tang and Guo10).
Considering the previous studies on the relationship between diet, environmental factors tobacco exposure and lung diseases, we hypothesised that a higher-quality DAQS may be associated with lower odds of COPD in adults with tobacco smoke exposure. By utilising data from the National Health and Nutrition Examination Survey, this study seeks to investigate the impact of DAQS on the association between smoking and COPD in adults.
Methods
Study population
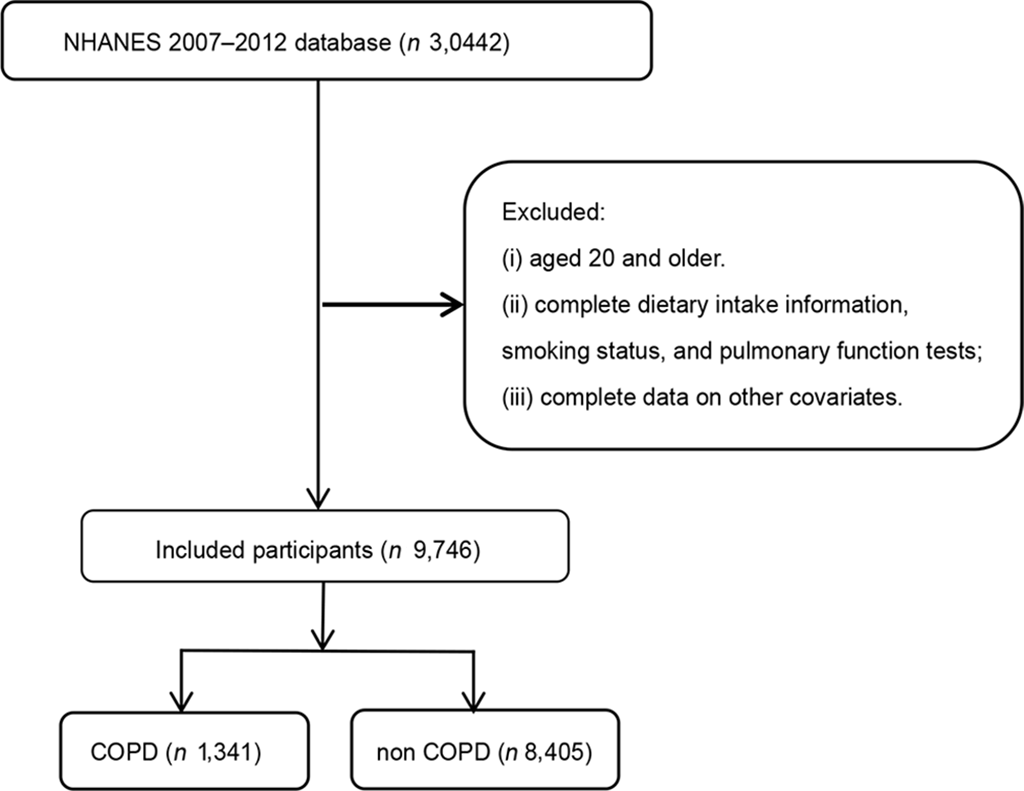
Data for this cross-sectional study were extracted from the 2007–2012 National Health and Nutrition Examination Survey. All research procedures were authorised by the National Center for Health Statistics Research Ethics Review Board, and participants had provided informed consent. According to the Ethics Review Board of Traditional Chinese Medicine in Zunyi Province, the cross-sectional study was exempted from ethical review. The inclusion criteria were as follows: (i) aged 20 years and older; (ii) complete dietary intake information, smoking status and pulmonary function tests and (iii) complete data on other covariates.
Dietary Antioxidant Quality Score evaluation
In this study, vitamins and minerals with antioxidant effects were used to calculate DAQS. Interviews were conducted with participants to gather their 24-h dietary recall. The first interview was carried out in person at the Mobile Examination Center, and the second one was conducted by telephone after 3–10 d. The total food intake and nutrient supplements consumed by participants were recorded. The intake of vitamins A, C, E, Zn, Mg and Se over 2 days was averaged. Daily intake was then compared with the recommended daily intake (2015–2020 Dietary Guidelines, health.gov). If the intake was below two-thirds of the recommended daily intake, it was scored as 0; if intake exceeded two-thirds of the recommended daily intake, it was scored as 1. The total DAQS varied from 0 (low quality) to 6 (high quality). Based on their scores, participants were classified into three DAQS groups: ≤ 3 (low DAQS), 4 (median DAQS) and ≥ 5 (high DAQS).
Smoking exposure assessment
Smoking status was categorised into three groups based on a smoking questionnaire. Participants were defined as current smokers if their responses indicated either daily or occasional smoking to the question ‘Do you smoke now?’. Those who reported having quit smoking, regardless of the duration (days, months or years), were classified as former smokers. Participants who answered ‘no’ to the question ‘Have you ever smoked a minimum of 100 cigarettes in your lifetime?’ were classified as never smokers.
Chronic obstructive pulmonary disease assessment
This study focused on adults with COPD aged over 20 years. The diagnostic criteria for COPD were as follows: forced expiratory volume in 1 s/forced vital capacity ratio < 0·7 after the administration of a bronchodilator.
Covariates
Confounding variables were selected based on prior literature and clinical plausibility. A systematic review of studies investigating COPD in relation to smoking and dietary antioxidants was conducted to identify potential confounders. The covariates were as follows: demographic information, including gender, age, race, marital status, education level, family poverty:income ratio; body measurements, including BMI, waist circumference; lifestyle factors, including alcohol consumption and underlying health conditions, including CVD, diabetes and hypertension. Race was divided into four categories: Mexican American, non-Hispanic White, non-Hispanic Black and other races (including other Hispanic/ethnic groups). Marital status was divided into married/cohabitation, widowed/divorced/separated and unmarried. Education level was divided into < high school diploma (9th grade or below, 9th–11th grade or 12th grade without a diploma), high school diploma/GED or equivalent and > high school diploma (college or AA degree or higher education). Alcohol consumption was classified as yes/no, with drinkers defined as those consuming at least twelve alcoholic beverages annually and non-drinkers as those consuming fewer than twelve alcoholic beverages per year. Hypertension was confirmed if the doctor had informed the patients of their diagnosis. Diabetes was diagnosed if any of the following criteria were met: HbA1c ≥ 6·5 % or 2-h oral glucose tolerance test ≥ 200 mg/dl or fasting blood glucose ≥ 126 mg/dl. Alternatively, diabetes was also diagnosed if the participant responded ‘yes’ to any of the following questions: (1) ‘Has a doctor told you that you have diabetes?’ (2) ‘Are you currently taking insulin injections?’ and (3) ‘Are you taking medication to lower your blood sugar?’ CVD was defined based on responses to the following questions: (1) ‘Has a doctor ever diagnosed you with congestive heart failure?’ (2) ‘Has a doctor ever diagnosed you with coronary heart disease?’ (3) ‘Has a doctor ever diagnosed you with angina?’and (4) ‘Has a doctor ever informed you that you have had a stroke?’
Statistical analysis
Given the complex multistage sampling design of National Health and Nutrition Examination Survey, recommended sample weights were applied to each participant to ensure population representativeness (WTDR2D/3). All weighted analyses were conducted using the R survey package. Categorical variables in the baseline information table were demonstrated as counts and weighted percentages, with the χ 2 test used for comparisons. Since the sample size exceeded 5000, the Anderson–Darling test for normality was employed to assess whether continuous variables were normally distributed. As the results indicated that continuous variables were non-normally distributed, the Mann–Whitney test was applied, with results presented as median (interquartile range). A weighted multivariable logistic regression model was employed to first explore the link between DAQS and COPD, then to investigate the link between smoking and COPD in adults and finally to appraise the combined impact of DAQS and adult smoking on COPD, including OR and 95 % CI. The Crude Model was not adjusted for covariates, while model 1 adjusted for confounders, including gender, age, race, education, marital status and the poverty:income ratio. Besides, model 2 further adjusted for BMI, alcohol consumption, smoking, diabetes, blood pressure (BP) and CVD as additional confounding factors.
Subgroup analysis was performed based on such adjusted variables as gender, alcohol consumption, diabetes, BP and CVD to investigate the moderating effect of DAQS on the link between smoking and COPD in adults. Statistical analyses were performed using R (version 4.4.1, Foundation for Statistical Computing). A two-sided P value < 0·05 was deemed statistically significant.
Missing data
For key variables (e.g. smoking status, lung function measures and dietary data), complete-case analysis was applied when the proportion of missing data was < 5 %. When missingness was ≥ 5 %, multiple imputation by chained equations (five imputations) was performed. The imputation model included age, sex, race/ethnicity, educational level, BMI, smoking status and outcome variables.
Results
Baseline characteristics of participants
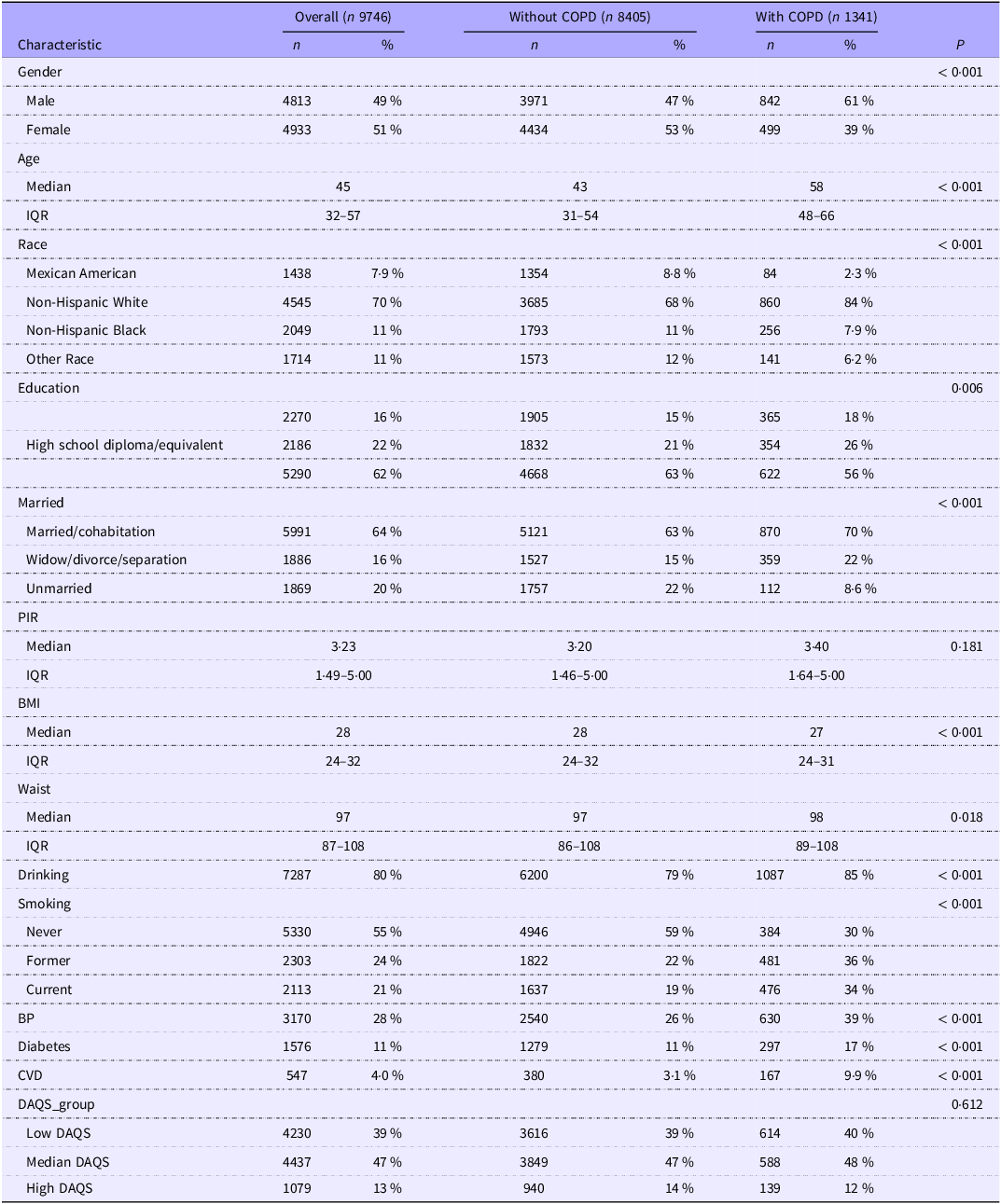
As illustrated in Table 1, 9746 participants were included in this study, of whom 1341 had COPD. The participant selection flow chart is presented in Figure 1. In the COPD group, the majority of the population was male (n 842), with a median age of 58. A higher proportion of the included participants tended to be non-Hispanic White (n 3685) individuals, those who had higher education (n 622) and those who were in a married or cohabiting status (n 870). Additionally, the COPD group had a higher percentage of alcohol consumers (n 1087) and smokers, with only 30 % being non-smokers. The number of individuals with hypertension, diabetes and CVD in the COPD group was 630 (39 %), 297 (17 %) and 167 (9·9 %), respectively. In contrast to the non-COPD group, the COPD group was significantly older and had a lower BMI, and these differences were statistically significant (P < 0·05). Statistically significant differences (P < 0·05) were also observed in waist circumference, drinking, smoking, BP, diabetes, CVD, education, marital status, race and gender between the COPD and non-COPD groups. No statistically significant difference was observed in the family poverty:income ratio between the two groups (P > 0·05).
The characteristics of the studied adults

COPD, chronic obstructive pulmonary disease; IQR, interquartile range; BP, blood pressure; PIR, poverty:income ratio; DAQS_group, Dietary antioxidant quality score group.
The flow chart of analytic sample selection.

Relationship between Dietary Antioxidant Quality Score, smoking exposure and chronic obstructive pulmonary disease
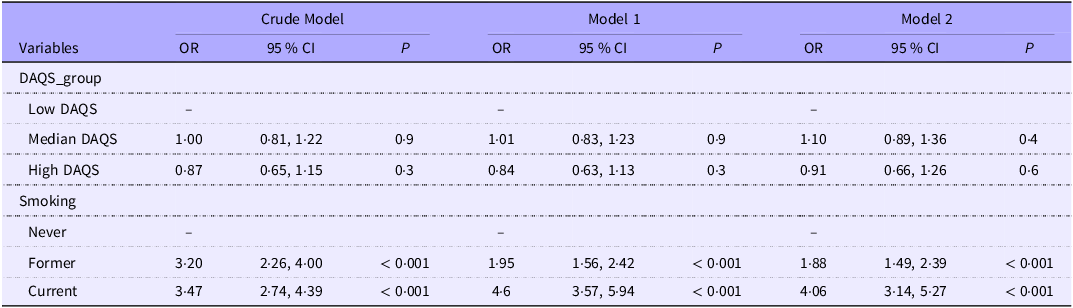
A weighted multivariable logistic regression model was utilised to investigate the impact of DAQS on COPD in adults and the impact of smoking on COPD in adults. First, the relationship between DAQS and COPD in adults was analysed. As illustrated in Table 2, in the unadjusted model, compared with low DAQS, both moderate and high DAQS showed no correlations (P > 0·05) with COPD. After controlling for gender, age, race, education, marital status and poverty:income ratio in model 1, and further adjusting for BMI, smoking, drinking, diabetes, BP and CVD in model 2, no significant correlation (P > 0·05) was found between DAQS and COPD.
Association between DAQS and smoking with COPD

COPD, chronic obstructive pulmonary disease; DAQS, Dietary Antioxidant Quality Score; PIR, poverty:income ratio; BP, blood pressure.
Model 1: adjustment for gender, age, race, education, marital status and PIR.
Model 2: adjustment for gender, age, race, education, marital status, PIR, BMI, drinking, diabetes, BP and CVD.
Moreover, the relationship between smoking and COPD was explored. In the unadjusted model, smoking was associated with the development of COPD. Compared with non-smokers, the odds of developing COPD were 3·2 times higher in the former smokers group (OR = 3·2, 95 % CI: 2·26, 4·00, P < 0·001) and 3·47 times higher in the current smokers group (OR = 3·47, 95 % CI: 2·74, 4·39, P < 0·001). In contrast to former smokers, current smokers had a higher likelihood of developing COPD. In the adjusted model 1, in comparison with non-smokers, the odds of developing COPD were 1·95 times higher in former smokers and 4·6 times higher in current smokers (OR = 4·6, 95 % CI: 3·57, 5·94, P < 0·001). In the adjusted model 2, smoking remained strongly associated with COPD as the odds of developing COPD in former smokers were 1·88 times higher than those in non-smokers, and the odds of developing COPD in current smokers were 4·06 times higher than those in non-smokers (OR = 4·06, 95 % CI: 3·14, 5·27, P < 0·001).
Impact of Dietary Antioxidant Quality Score on the relationship between smoking exposure and chronic obstructive pulmonary disease
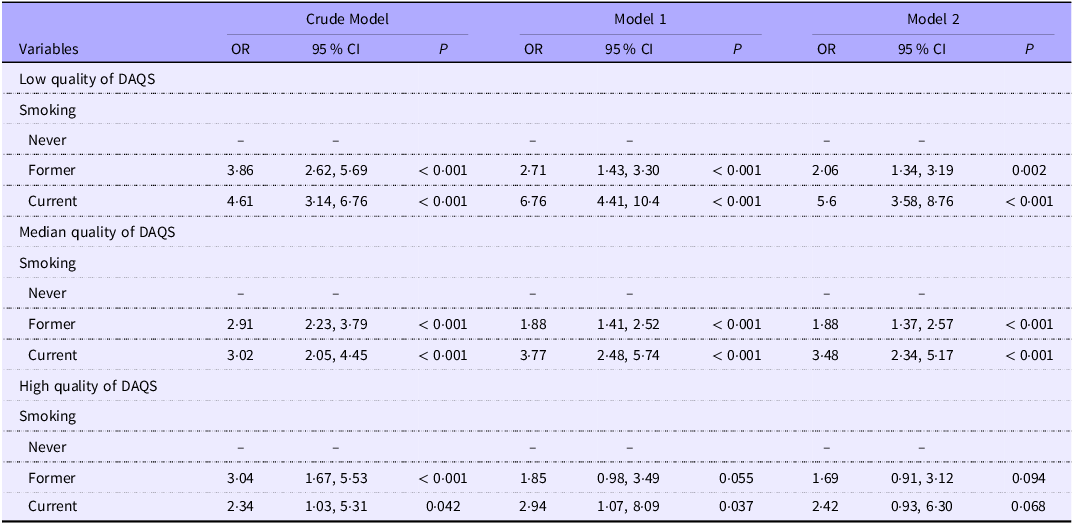
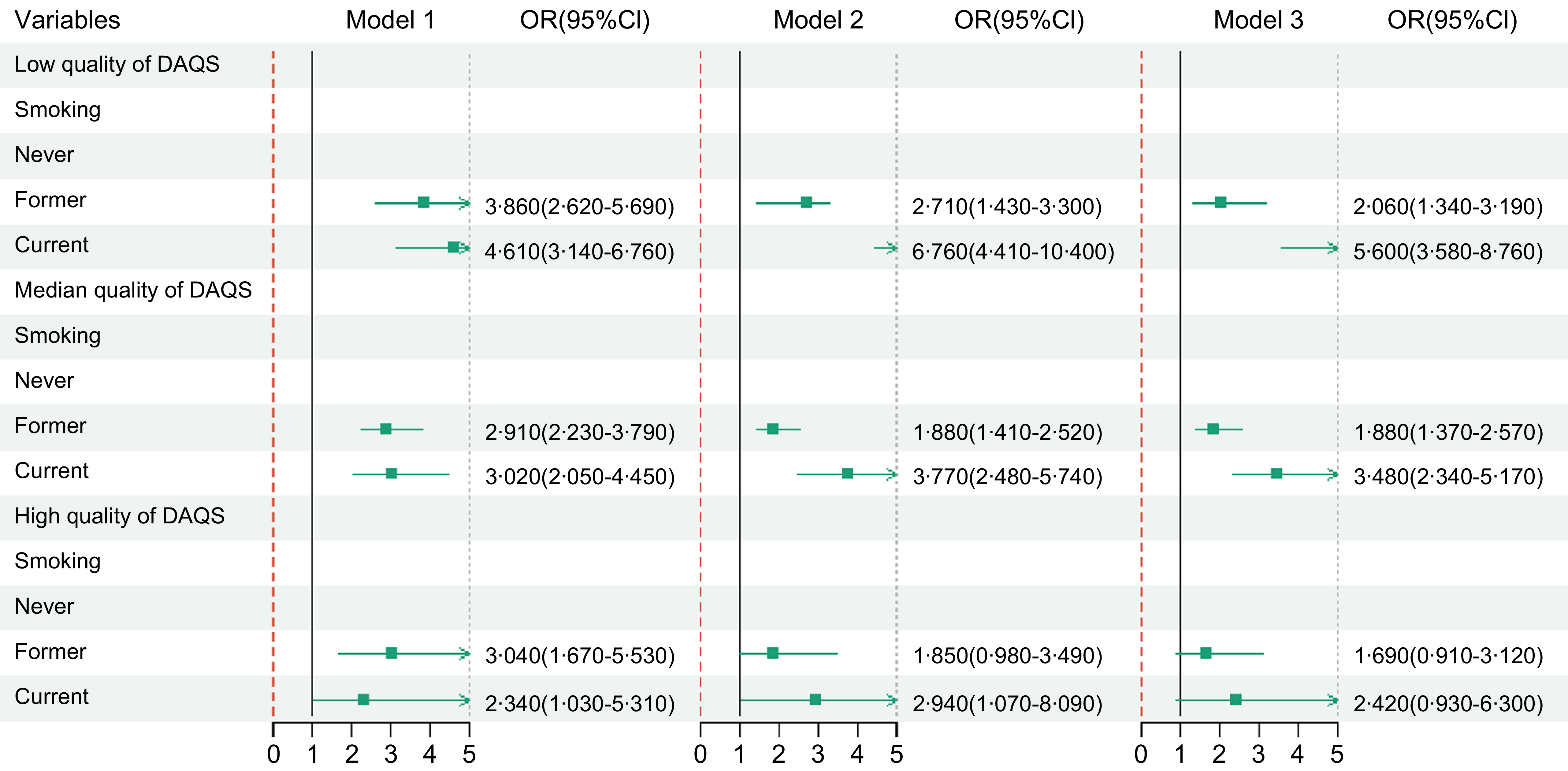
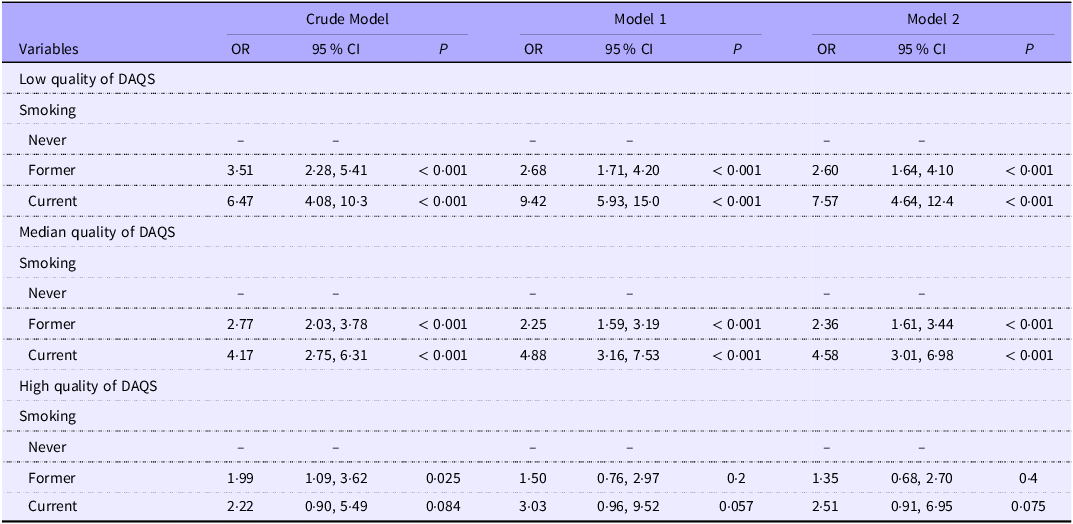
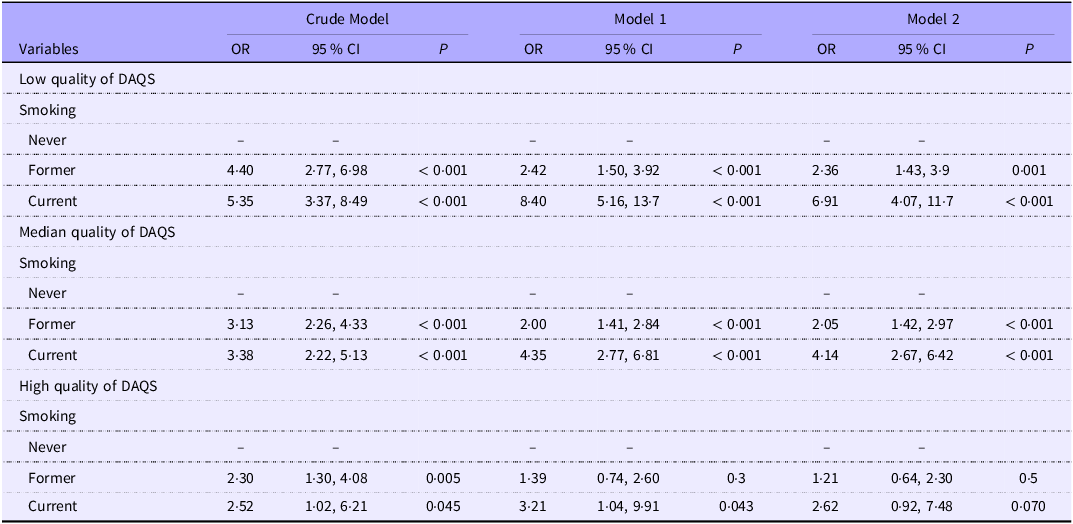
The impact of DAQS on the relationship between adult smoking and COPD is illustrated in Table 3 and Figure 2. As observed, in the crude model of the low DAQS group, the number of former smokers with COPD was 3·86 times higher than non-smokers with COPD (OR = 3·86, 95 % CI: 2·62, 5·69, P < 0·001), and the number of current smokers with COPD was 4·61 times higher than non-smokers with COPD (OR = 4·61, 95 % CI: 3·14, 6·76, P < 0·001). Both results indicated significant correlations. After adjusting for confounding factors in model 1 and model 2, similar results were observed (P < 0·001). In the crude model of the moderate DAQS group, the number of former smokers with COPD was 2·91 times higher than the non-smoker group with COPD (OR = 2·91, 95 % CI: 2·23, 3·79, P < 0·001), and the number of current smokers with COPD was 3·02 times higher than non-smokers with COPD (OR = 3·02, 95 % CI: 2·05, 4·45, P < 0·001). Both results indicated significant correlations. In model 1 and model 2, similar findings were also observed (P < 0·001). In the crude model of the high DAQS group, the number of former smokers with COPD was 3·04 times higher than non-smokers with COPD (OR = 3·04, 95 % CI: 1·67, 5·53, P < 0·001), and the number of current smokers with COPD was 2·34 times higher than non-smokers with COPD (OR = 2·34, 95 % CI: 1·03, 5·31, P = 0·042). In model 1, the number of current smokers with COPD was 2·94 times higher than that of non-smokers with COPD (OR = 2·94, 95 % CI: 1·07, 8·09, P = 0·037). These results suggested a strong correlation. However, the results for former smokers v. non-smokers in model 1 and model 2, as well as current smokers v. non-smokers in model 2, did not show significant correlations (P < 0·05). These results suggested that, in comparison to low and moderate DAQS, high DAQS can moderate the association between smoking and COPD in adults.
Effect of DAQS on the association between smoking and COPD

COPD, chronic obstructive pulmonary disease; DAQS, Dietary Antioxidant Quality Score; PIR, poverty:income ratio; BP, blood pressure.
Model 1: adjustment for gender, age, race, education, marital status and PIR.
Model 2: adjustment for gender, age, race, education, marital status, PIR, BMI, drinking, diabetes, BP and CVD.
Visual chart.

The interaction between smoking and chronic obstructive pulmonary disease on Dietary Antioxidant Quality Score
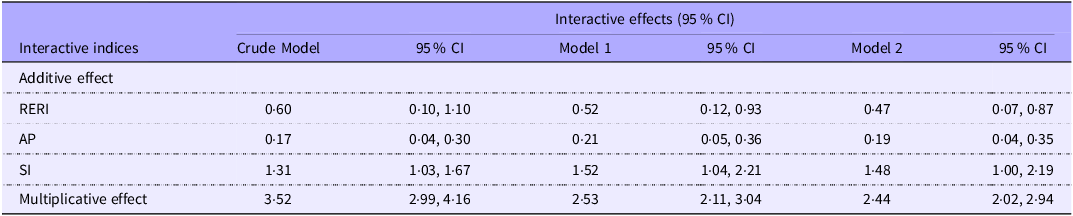
After comprehensive adjustment for potential confounders, the 95 % CI for RERI and AP were greater than 0, while those for SI and the multiplicative interaction term were greater than 1 (Table 4), indicating the presence of both additive and multiplicative interactions between smoking and DAQS in relation to the odds of COPD.
The interaction between smoking and COPD on DAQS

COPD, chronic obstructive pulmonary disease; DAQS, Dietary Antioxidant Quality Score; PIR, poverty:income ratio; BP, blood pressure.
Model 1: adjustment for gender, age, race, education, marital status and PIR.
Model 2: adjustment for gender, age, race, education, marital status, PIR, BMI, drinking, diabetes, BP and CVD.
Subgroup analysis
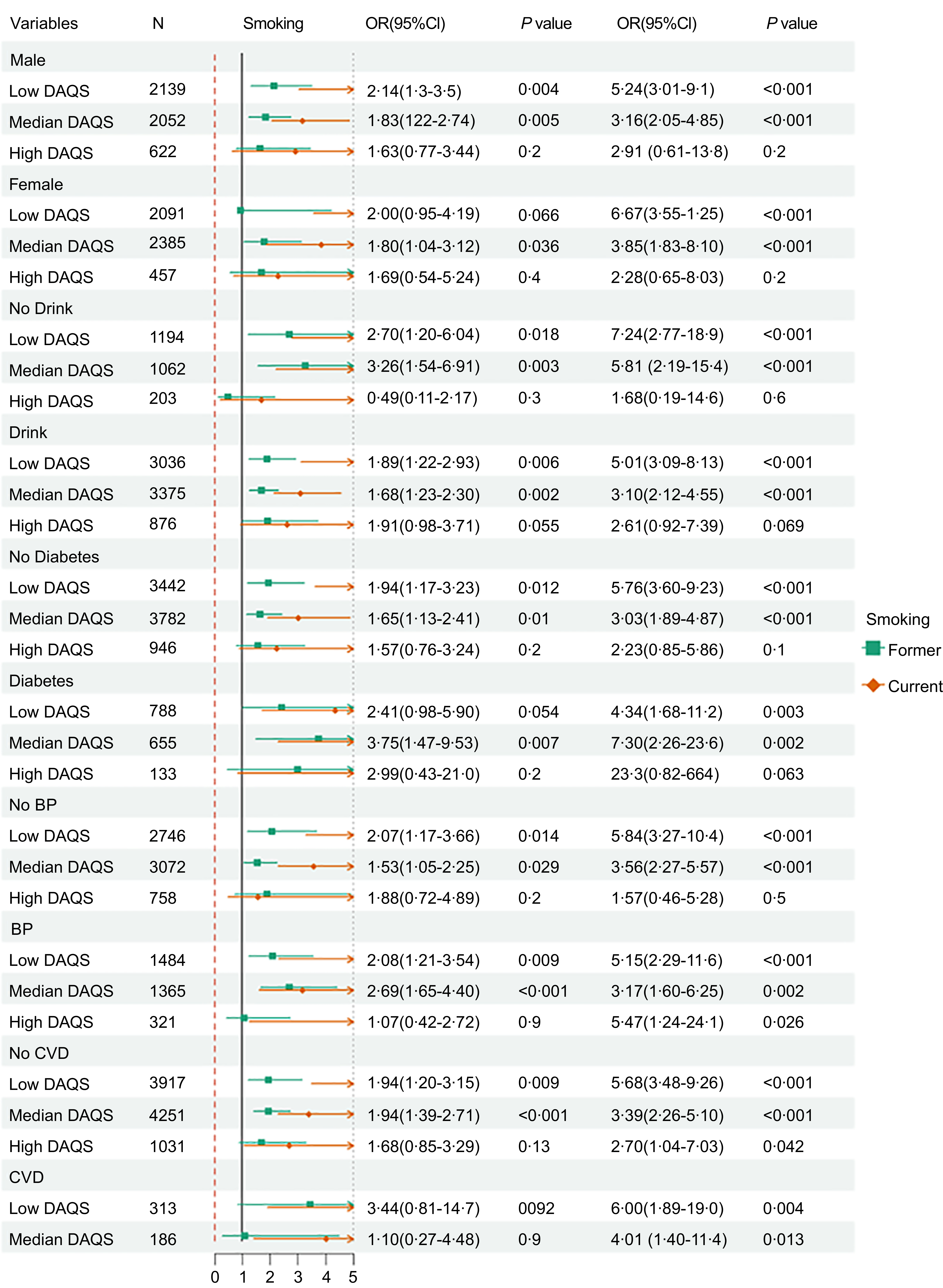
To explore the moderating effect of DAQS on the relationship between smoking and COPD in adults, a subgroup analysis based on gender, alcohol consumption, diabetes, BP and CVD was conducted (Figure 3). First, in the gender-based subgroup analysis, we found that smoking and COPD were correlated in both the low and moderate DAQS groups for both men and women (P < 0·05). No significant impact of DAQS on the relationship between current smoking and COPD was observed in the high DAQS group (P > 0·05). However, it suggested that high DAQS can moderate the association between adult smoking and COPD. Moreover, similar results were observed in subgroup analysis based on patients with and without alcohol consumption, with and without diabetes and without high BP. In the high DAQS group, the subgroup analysis based on individuals with high BP or with or without CVD demonstrated that the relationship between current smoking and COPD remained significant (P < 0·05), but DAQS could not moderate the relationship between them.
The forest plot of smoking and COPD in adults stratified by gender, drinking, diabetes, BP, and CVD. COPD, COPD, chronic obstructive pulmonary disease; BP, blood pressure.

Sensitivity analysis
To assess the robustness of the findings, two sensitivity analyses were conducted. First, the analysis was restricted to participants aged ≥ 40 years to further evaluate the associations of DAQS with smoking and COPD (Table 5). In the high-quality DAQS group, model 2, adjusted for relevant covariates, showed no significant association (P > 0·05). In contrast, in the low-and medium-quality DAQS groups, the crude model and covariate-adjusted models 1 and 2 produced consistent significant associations (P < 0·05). Second, participants with possible asthma were excluded, and weighted logistic regression models were re-estimated (Table 6). In the high-quality DAQS group, model 2 again showed no significant association (P > 0·05). Conversely, significant associations persisted across models 1 and 2 in the low-and medium-quality DAQS groups (P < 0·001), further supporting the stability of the results.
Sensitivity analysis

DAQS, Dietary Antioxidant Quality Score; PIR, poverty:income ratio; BP, blood pressure.
Model 1: adjustment for gender, age, race, education, marital status and PIR.
Model 2: adjustment for gender, age, race, education, marital status, PIR, BMI, drinking, diabetes, BP and CVD.
Sensitivity analysis-excluding participants with asthma

DAQS, Dietary Antioxidant Quality Score; PIR, poverty:income ratio; BP, blood pressure.
Model 1: adjustment for gender, age, race, education, marital status and PIR.
Model 2: adjustment for gender, age, race, education, marital status, PIR, BMI, drinking, diabetes, BP and CVD.
Additionally, in model 3, the E-values suggested that the observed associations were unlikely to be fully explained by unmeasured confounding. For low-quality DAQS, the E-values were 2·23 for former smoking (HR = 1·44) and 4·16 for current smoking (HR = 2·37) in relation to COPD. For medium-quality DAQS, the corresponding E-values were 2·08 (HR = 1·37) and 3·14 (HR = 1·87). For high-quality DAQS, the E-values were 1·92 (HR = 1·30) and 3·14 (HR = 1·87). These results indicate that the observed associations are robust and unlikely to be attributable to residual confounding.
Discussion
Our study included 9746 adults, of whom 1341 (13·76 %) had COPD. Among the adult COPD patients, 34 % were current smokers, and 36 % had previously smoked. It indicated that smokers made up the majority of COPD patients, particularly in men, and the odds of COPD increased with age. The analysis indicated that DAQS modified the association between smoking and COPD, with attenuated OR observed in the high-DAQS group compared with the low-and medium-DAQS groups, particularly in males. The subgroup analysis further emphasised the reliability of this association. It is important to distinguish effect modification from a simple inverse association. These findings should not be interpreted as evidence of a direct inverse association between DAQS and COPD, as the main effect of DAQS was not statistically significant in the adjusted models (Table 2). Instead, DAQS appears to function as an effect modifier of the smoking–COPD relationship, potentially mitigating smoking-related oxidative stress.
Similarly, other studies have indicated that factors such as being male, smoking, older age and high-income countries are significant factors associated with COPD(Reference Rodríguez García, Ruano-Ravina and Pérez Ríos11). Previous studies have reported that even individuals with normal lung function may experience inflammation and structural damage due to smoking(Reference Polosa and Thomson12). Furthermore, smoke exposure has been confirmed to lead to more severe acute exacerbations of COPD(Reference Qi, Yan and Tang13), and current and former smokers have a higher prevalence of COPD(Reference Huang, Li and Ye14). By investigating the effects of smoking status on the quality of survival and emphysema in patients with acute exacerbations of COPD, Dingqi et al. (Reference Ding, Li and Xu15) found that current smokers had the poorest lung function, suggesting that smoking worsened lung tissue damage and was a contributing factor to AECOPD. Fekete et al. (Reference Fekete, Horvath and Santa16) also pointed out that COPD patients who never smoked had better quality of life, nutritional status and lung function in comparison to smokers. More studies unravelled that long-term smoking and continuous exposure to smoke could cause progressive airway inflammation and irreversible airway damage(Reference Wang, Qiu and Ji17). This is due to prolonged exposure to cigarette smoke, which increases OS markers in COPD patients, activates pattern recognition receptors and enlarges the alveolar septum(Reference Vij, Chandramani-Shivalingappa and Van Westphal18). The development of emphysema is marked by increased numbers of neutrophils and macrophages in the lungs, activation of airway epithelial cells, increased mucus secretion and excessive release of reactive oxygen species (ROS) by neutrophils and macrophages, which can damage anti-protease mechanisms and accelerate lung tissue degradation(Reference Schauer, Wheaton and Malarcher19,Reference McGuinness and Sapey20) . These factors contribute to fibrosis around the bronchioles and the destruction of alveolar walls in emphysema, ultimately leading to accelerated cellular senescence and apoptosis driven by immune responses(Reference Park21).
Modern studies have increasingly proven the impact of diet on COPD(Reference Scoditti, Massaro and Garbarino22). Dietary antioxidants are believed to moderate the odds of COPD and protect lung function(Reference Joshi, Kim and Lee23). Dietary antioxidants can prevent or delay oxidative damage in the body. For instance, vitamins A, C and E are considered to help safeguard the respiratory system against oxidants, thereby alleviating symptoms in COPD patients. Additionally, minerals such as Se, Zn and Mg can reduce the generation and accumulation of free radicals in the body, neutralise generated free radicals, reduce OS and protect cells from oxidative damage. These anti-inflammatory and antioxidant activities help to maintain normal cell function and reduce the incidence of COPD(Reference Zheng, Shu and Si24). Lazzara et al. have concluded from their study that antioxidants may reduce the odds of COPD. Multiple studies have confirmed that a better-adjusted dietary index contributes to alleviating COPD symptoms and reducing the odds of COPD, particularly during hospitalisation for acute exacerbations(Reference Lazzara, Pinto and Di Vincenzo25). Some dietary antioxidants also support the repair and regeneration of lung tissue. For example, β-carotene can be converted into vitamin A, which is essential for maintaining the good condition of the respiratory mucosa and promoting the repair of lung tissue(Reference Zhu, Che and Xu26). A study reported a negative association between vitamin A and emphysema by analysing National Health and Nutrition Examination Survey 2007–2016 data, suggesting that adequate vitamin A supplementation may lead to anti-inflammatory responses, which help to modulate airway function in the lungs(Reference Shen, Bimali and Faramawi27). Vitamin C can remove superoxide-free radicals and prevent oxidative damage. In a study by Korean scholars, it was found that Vitamin C was effective in preventing the odds of COPD in non-smoking populations(Reference Park, Byun and Kim28). Furthermore, among smokers, those with higher vitamin C intake had the best lung function(Reference Shin, Shim and Lee29). Many studies have reported that the intake of antioxidant vitamin C reduces the odds of COPD and can modulate lung function(Reference Xiang and Wang30). Vitamin E breaks lipid peroxidation and acts as a major defense against oxidative damage(Reference Schünemann, Grant and Freudenheim31). Moreover, researchers have observed significant associations between dietary intake of vitamins C and E and the forced expiratory volume in 1 s/forced vital capacity ratio(Reference Tsiligianni and van der Molen32). Fu et al. (Reference Fu, Shi and Hu33) concluded that dietary intake of Se in USA adults was negatively correlated with COPD, suggesting that higher Se intake may be linked to a lower odds of COPD. Xu et al. also reported similar findings to ours(Reference Xu, Han and Lin34): higher intake of niacin was related to improved lung function indicators, suggesting that a diet rich in niacin may help improve lung health. However, studies on the effect of dietary antioxidant intake on modulating smoking and COPD in adults remain limited.
High DAQS can enhance the immune system and reduce OS, thereby reducing the odds of smoking-induced COPD. Dietary antioxidants can boost the immune system and neutralise or remove free radicals and other ROS, consequently reducing cellular damage(Reference Janciauskiene35). Harmful substances generated during smoking can produce a large number of free radicals and other ROS in the lungs, leading to airway inflammation and OS(Reference Li, Ren and Yu36), and ultimately causing the development of COPD. OS refers to an imbalance between pro-oxidants and antioxidants. Under physiological conditions, ROS can neutralise pathogens that may attack the body. One of their functions is to activate the signalling pathways of inflammatory cells, thereby triggering the immune system. However, when ROS are produced in excess and accumulate within cells, they exhibit a high oxidation state, causing severe and irreversible damage to tissues, either directly or by altering signalling pathways(Reference Magallón, Navarro-García and Dasí37,Reference Liu, Li and Chen38) . For example, chemicals, including nicotine in tobacco, can greatly increase ROS levels in the body, and the accumulated ROS intensifies the OS response. The heightened OS response can harm cellular and subcellular targets, including proteins, nucleic acids and lipids, leading to airway hyperreactivity, irreversible airway obstruction and airway remodelling, ultimately causing COPD and then making it worse(Reference Otake, Chubachi and Miyamoto39). The increased oxidative burden in COPD patients also originates from leukocytes and macrophages involved in pulmonary inflammation(Reference Lin and Thomas40). Antioxidants can inhibit key signalling pathways involved in the inflammatory response, reducing pulmonary stress, limiting the release of pulmonary inflammatory mediators and preventing the infiltration of inflammatory cells, thereby protecting lung tissue from damage. Dietary antioxidants can also improve pulmonary ventilation and gas exchange efficiency(Reference Ioniuc, Lupu and Dragan41). Our study, aimed at clarifying the moderating effect of dietary antioxidants, found that after adjusting for all confounding factors, adults with higher DAQS scores demonstrated a lower odds of COPD from smoking. These findings further support that higher DAQS levels are associated with reduced odds of COPD among adult smokers. The results of the above studies are consistent with ours, confirming the stability and reliability of our findings.
This study fills the gap in studies on the impact of dietary antioxidants on the relationship between adult smoking and COPD in the USA and may provide insights into management strategies for COPD patients who continue to smoke in the future. However, the mechanisms underlying these effects still require further investigation. Additionally, this study has some limitations. First, it cannot establish causality as the data come from a cross-sectional study. Second, unmeasured or insufficiently measured factors, such as occupational exposures, air pollution, genetic susceptibility and other sources of residual confounding, may have influenced the results. In addition, several covariates were self-reported, introducing potential recall bias. DAQS may not fully reflect long-term dietary intake, and selection bias cannot be entirely excluded. Third, this cross-sectional analysis was conducted without a preregistered protocol or a directed acyclic graph. Therefore, the findings should not be interpreted as causal effects of smoking or DAQS on COPD. The prevalence of COPD in the study sample was approximately 13·8 %, exceeding the conventional 10 % threshold for rare outcomes. In cross-sectional studies with non-rare outcomes, OR may overestimate prevalence ratios. Accordingly, the reported OR should be interpreted as measures of association rather than direct estimates of relative odds. For example, an OR of 4·06 for current smoking indicates a strong positive association with COPD prevalence, rather than implying a precisely fourfold increase in the odds. Prospective studies are warranted to more accurately quantify the odds of its incidence. Future studies could address these limitations by expanding the sample size, using more accurate measurement tools and clinical laboratory data and adopting longitudinal designs.
Conclusion
This study investigated the impact of different levels of DAQS on the relationship between smoking and COPD in adults. The results revealed that, in comparison to low and moderate DAQS, high DAQS helps to moderate the odds of COPD in adult smokers, particularly among men and drinkers. It is recommended that adult male smokers maintain a healthier diet and reduce alcohol consumption to lower their odds of COPD.
Acknowledgements
Not applicable.
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
All authors contributed to the study conception and design. Writing – original draft preparation: X. T., X. Z.; Writing – review and editing: X. T., X. Z., X. L., X. F., R. D.; Conceptualisation: R. D.; Methodology: R. D.; Formal analysis and investigation: X. T., X. Z., X. L., X. F., R. D.; Resources: R. D.; Supervision: R. D., and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
The authors declare no conflicts of interest.
The data that support the findings of this study are available from the corresponding author upon reasonable request.

 Open access
Open access