


Statement of Research Significance
Research Questions or Topics: Clinical neuropsychology historically prioritizes the assessment of “cold” cognitive functions, often overlooking affective and motivational domains (“hot” cognition). This article addresses the need to systematically integrate assessments of emotional reactivity, emotion regulation, emotion recognition, and social cognition into routine clinical neuropsychological practice. Main Findings: Drawing on affective neuroscience evidence, this paper identifies four core affective–motivational domains that critically shape cognitive functioning, functional outcomes, and rehabilitation engagement. It highlights validated self-report scales and performance-based tasks available for clinical use, while underscoring their current underutilization in routine assessment. Study Contributions: This paper provides a structured, clinically oriented framework for incorporating affective and motivational assessment into neuropsychological evaluation. By offering a curated overview of standardized tools and emphasizing their utility in capturing clinically relevant dimensions of everyday functioning, it bridges the gap between neuroscience research and clinical practice, with implications for diagnosis, rehabilitation planning, and quality of life.
Introduction
A patient may recall a word list without difficulty yet fail to recognize or regulate anger in social interactions, resulting in interpersonal misunderstandings and tension. Which of these abilities is more consequential for daily life? This paradox captures one of the most persistent limitations of current neuropsychological practice: the traditional focus on cognitive domains, while neglecting the systematic assessment of emotional and motivational processes. Since its origins, clinical neuropsychology has aimed to identify and quantify deficits in specific cognitive domains. Historically, neuropsychological assessments have emphasized “cold” cognition, including attention, memory, language, visuospatial abilities, and executive functions, while affective processes were often considered secondary or even epiphenomenal (Casaletto & Heaton, Reference Casaletto and Heaton2017). Already in the 1990s, researchers and clinicians highlighted the risks of this neglect, showing that emotional and motivational disturbances can strongly interact with neuropsychological performance and functional outcomes (Reitan & Wolfson, Reference Reitan and Wolfson1997; Sherman et al., Reference Sherman, Shaw and Glidden1994). Contemporary affective neuroscience established that cognition and emotion are deeply integrated within large scale brain circuits (Okon-Singer et al., Reference Okon-Singer, Hendler, Pessoa and Shackman2015; Pessoa, Reference Pessoa2008; Todd et al., Reference Todd, Miskovic, Chikazoe and Anderson2020). Neuroimaging evidence further demonstrates that emotional and cognitive processes are reciprocally integrated within large-scale brain circuits (Dolcos et al., Reference Dolcos, Iordan and Dolcos2011; Malezieux et al., Reference Malezieux, Klein and Gogolla2023). Emotions provide the motivational force that prioritizes stimuli, guides learning, and shapes behavior, yet emotional–motivational assessment remains infrequently applied in clinical neuropsychology. Surveys of professional practice show that most clinicians infrequently administer standardized performance-based tasks and clinical scales assessing affective processing, focusing almost exclusively on cognition (Priluck & Fedio, Reference Priluck and Fedio2022). In this context, it is crucial to recognize that while tasks provide performance-based metrics, self-report scales are essential to incorporate the patient’s subjective experience, offering a broader perspective on the patient’s perceived functional status. This allows the evaluation to move beyond task-based quantitative measures, integrating the patient’s perspective into a more comprehensive clinical profile. In everyday practice, this omission has several consequences: without systematic assessment of emotional reactivity, regulation, recognition, and social cognition, integrating both performance-based measures and subjective reports, clinicians may miss critical predictors of outcome such as affective dysregulation, impaired empathy, or reduced social cognition, deficits that can be as disabling as cognitive impairments in daily functioning (Henry et al., Reference Henry, von Hippel, Molenberghs, Lee and Sachdev2016; McDonald, Reference McDonald2017). Moreover, alterations in emotional or motivational functioning may represent early or distinctive markers of neurological and neurodegenerative conditions, including frontotemporal dementia, traumatic brain injury, and their systematic evaluation can therefore refine differential diagnosis and clinical characterization (e.g., Bertoux et al., Reference Bertoux, Delavest, de Souza, Funkiewiez, Lépine, Fossati, Dubois and Sarazin2012; Henry et al., Reference Henry, von Hippel, Molenberghs, Lee and Sachdev2016).
Internationally, professional organizations have underscored the need to consider emotional, motivational, and behavioral factors within neuropsychological assessment. The American Academy of Clinical Neuropsychology (AACN) Practice Guidelines emphasize that emotional status, behavior, and motivation should be observed and reported as integral components of a comprehensive evaluation (Board of Directors, 2007). More recently, the Minnesota Conference Guidelines for education and training in clinical neuropsychology identify emotional, motivational, and social functioning as essential domains of professional competence (Stringer et al., Reference Stringer, Fuchs, Bordes Edgar, Bristow, Correia, Penna, Reyes, Whiteside, Block, Bodin, Butt, Calamia, Didehbani, Dodzik, Dotson, Fernandes, Freece, Fuller, Getz and Schmitter-Edgecombe2026). Similarly, the European Federation of Psychologists’ Associations (EFPA) competence framework includes the assessment of affective, motivational, and interpersonal functioning among the core skills required of professional psychologists (EFPA, 2015). Despite these recommendations, a significant gap remains between professional guidelines and routine clinical practice. Many widely used affective instruments still lack widespread clinical dissemination compared to cognitive batteries. This mismatch highlights both a current weakness and a strategic opportunity for the field. In this article, we propose that emotional–motivational domains should be considered as a core component of neuropsychological assessment. We delineate four central areas, namely emotional reactivity, emotion regulation, emotion recognition, and social cognition/theory of mind (ToM). These domains are defined as “central” insofar as they reflect core components of affective and social functioning, supported by distinct yet highly integrated neural systems (Adolphs, Reference Adolphs2009; Davidson, Reference Davidson2004; Gross, Reference Gross and Gross2014; Happé et al., Reference Happé, Cook and Bird2017). Beyond these discrete domains, we also address emotional–cognitive interference as a cross-cutting modulatory mechanism that may influence global neuropsychological performance. By outlining representative standardized tasks and scales for the evaluation of the above-mentioned domains, we aim to illustrate their clinical implications and highlight the need for their systematic inclusion in neuropsychological assessment protocols, moving beyond a purely “cold” cognitive approach. The tools and paradigms described were selected based on their clinical relevance, psychometric robustness, and widespread use in the international literature. This selection was not intended as a systematic review, but rather as a theoretically driven overview aimed at illustrating their potential integration into clinical assessment, consistent with established frameworks in affective and social neuroscience (Adolphs, Reference Adolphs2009; Davidson, Reference Davidson2004). Consistent with current professional guidelines (AACN, 2007; EFPA, 2015), we posit that while standardized neuropsychological tasks cannot achieve full ecological validity in the sense of reproducing, real-world conditions, their integration with multi-source clinical data, including subjective clinical reports, observations, and information from caregivers, allows for the characterization of clinically relevant dimensions of everyday functioning. Such integrated approach is essential to characterize the patient’s individual clinical profile and provide an informative sample of the real-world challenges faced by patients. By combining empirical evidence with qualitative clinical data, our aim is to advocate for a multidimensional approach to neuropsychology that better reflects the complexity of the individual’s functioning in daily life.
Emotional domains and assessment tools
Emotional reactivity
Emotional reactivity involves the intensity, speed, and duration of affective responses, or “affective chronometry” (Davidson, Reference Davidson1998, Reference Davidson2004). Alterations manifest as exaggerated responses, blunting, or contextually inappropriate reaction. Right-hemisphere damage often impairs facial emotion recognition and subjective responding, while emotional distress significantly reduces quality of life in stroke survivors (Fong et al., Reference Fong, Ho, Wan and Au-Yeung2022). In practical terms, this may translate into a patient who becomes disproportionately irritable at minor frustrations or, conversely, shows a flat affect that relatives interpret as apathy – both scenarios profoundly shaping rehabilitation outcomes.
Among the most established experimental paradigms for assessing emotional reactivity, the Affective Picture Viewing paradigm plays a central role (Bradley & Lang, Reference Bradley, Lang, Cacioppo, Tassinary and Berntson2007; Lang et al., Reference Lang, Bradley and Cuthbert2008). Participants are exposed to a standardized set of affective pictures varying in valence (pleasant, unpleasant, neutral) and arousal (high, medium, low), drawn from the International Affective Pictures System (IAPS; Lang et al., Reference Lang, Bradley and Cuthbert2008). Emotional responses are measured through physiological indices such as heart rate, skin conductance, facial electromyography, pupillary dilation, and event-related potentials. In addition, or when physiological recordings are not feasible, subjective affective responses can be assessed using Self-Assessment Manikin (SAM; Bradley & Lang, Reference Bradley and Lang1994), a non-verbal pictorial rating scale that allows participants to evaluate each stimulus along the dimensions of valence (pleasant-unpleasant), arousal (activation-calm), and dominance (controlled-in control). Together, these measures capture the multidimensional nature of emotional reactivity, its intensity, speed, and duration, providing both physiological and subjective indices of affective responding (Bradley & Lang, Reference Bradley, Lang, Cacioppo, Tassinary and Berntson2007).
Beyond performance-based tasks, standardized self-report questionnaires provide efficient tools for clinical practice. The Perth Emotional Reactivity Scale – Short Form (PERS-S) (Becerra et al., Reference Becerra, Preece, Campitelli and Scott-Pillow2019) is an 18-item self-report measure assessing three core components of emotional reactivity: ease of activation (how readily emotions are triggered), intensity (the strength of emotional responses), and duration (how long emotions last), measured separately for positive and negative emotions. The PERS-S has demonstrated sound internal consistency and robust factorial validity across both clinical and non-clinical samples. Combining emotional picture-viewing tasks with self-report tools like the PERS-S can enhance clinical sensitivity to subtle affective changes, providing a more comprehensive clinical profile that offers an informative sample of the patient’s functioning in real-world contexts.
Emotion regulation
Emotion involves modulating emotional states to achieve goals (Gross, Reference Gross and Gross2014). Dysregulation is a transdiagnostic risk factor, associated with mood disorders, personality changes after brain injury, and deficits in executive functioning. Inadequate regulation often undermines treatment adherence. For instance, a patient with preserved executive test scores may struggle to control sudden outbursts of anger in social settings, leading to job loss or family conflict – issues that traditional neuropsychological batteries would fail to capture. Among self-report instruments, the Emotion Regulation Questionnaire (ERQ; Gross & John, Reference Gross and John2003) is one of the most widely used tools to assess individual differences in habitual regulation strategies. It measures two key dimensions: cognitive reappraisal, i.e., reinterpreting situations to alter their emotional impact, and expressive suppression, i.e., inhibiting outward emotional expression. Higher use of reappraisal is generally associated with better psychological well-being, whereas reliance on suppression correlates with maladaptive outcomes (Gross & John, Reference Gross and John2003; Ioannidis & Siegling, Reference Ioannidis and Siegling2016). The instrument has shown high internal consistency and sound test–retest reliability across multiple international validations, supporting its use in both research and clinical settings. The Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, Reference Gratz and Roemer2004) and its short forms (DERS-16, DERS-SF; Bjureberg et al., Reference Bjureberg, Ljótsson, Tull, Hedman, Sahlin, Lundh, Bjärehed, DiLillo, Messman-Moore, Gumpert and Gratz2016; Sousa et al., Reference Sousa, Linharelhos, Silva and Rijo2023) offer a broader, multidimensional assessment of regulatory difficulties. The DERS captures six domains: nonacceptance of emotional responses, difficulties engaging in goal-directed behavior, impulse control difficulties, lack of emotional awareness, limited access to regulation strategies, and lack of emotional clarity. The scale demonstrates strong psychometric properties and provides a more comprehensive assessment of emotional dysregulation compared to ERQ, making it particularly suitable for clinical populations with complex affective or behavioral symptoms (Gratz & Roemer, Reference Gratz and Roemer2004; Ioannidis & Siegling, Reference Ioannidis and Siegling2016). Although these instruments primarily assess dispositional aspects of emotion regulation, they can also be employed to monitor long-term changes following rehabilitation or psychological interventions aimed at improving emotional control.
Beyond self-report questionnaires, performance-based tasks allow for the direct evaluation of emotion regulation processes in controlled settings. Instructed reappraisal tasks typically present participants with emotionally evocative pictures (e.g., drawn from the IAPS) and provide explicit instructions to either down-regulate (reduce) or up-regulate (intensify) their emotional response to negative or positive stimuli. Emotional responses during these tasks can be measured at multiple levels – behavioral (e.g., facial expressions), subjective (e.g., ratings of valence and arousal), and physiological (e.g., peripheral or central measures). Such multimodal assessment offers complementary insights into the implementation of regulatory strategies and their reliance on prefrontal control mechanisms (Hajcak & Nieuwenhuis, Reference Hajcak and Nieuwenhuis2006; Hajcak et al., Reference Hajcak, MacNamara and Olvet2010). In clinical settings, difficulties in emotion regulation may be reflected in incongruent or persistent facial expressions, limited shifts in reported valence or arousal, or reduced modulation of physiological responses, indicating impaired implementation of regulatory strategies.
Emotion recognition
The ability to recognize the emotional states of others through facial, vocal, and bodily cues is a cornerstone of adaptive social interaction. Impairments in emotion recognition are frequent after neurological damage, and are also prominent in frontotemporal dementia, schizophrenia, and stroke (Henry et al., Reference Henry, von Hippel, Molenberghs, Lee and Sachdev2016). Deficits in recognition are associated with reduced social functioning and increased risk of mood disturbances, reinforcing their clinical significance. A typical example is the patient with frontotemporal dementia who succeeds in memory and language tests but consistently misreads his/her partner’s emotional expressions, fueling interpersonal strain that far outweighs cognitive deficits in everyday impact.
Several standardized performance-based tasks and instruments have been developed to assess emotion recognition. The Florida Affect Battery (FAB, Bowers et al., Reference Bowers, Blonder and Heilman1991) provides a comprehensive assessment of emotion recognition across both facial and prosodic modalities, including subtests for affect discrimination and naming across visual and auditory channels. In contrast, the Facial Expressions of Emotion: Stimuli and Tests (FEEST; Young et al., Reference Young, Perrett, Calder, Sprengelmeyer and Ekman2002) focuses specifically on static facial expressions derived from the “Ekman 60 Faces” stimuli originally developed by Ekman and Friesen (Reference Ekman and Friesen1976), and yields separate scores for basic emotions such as happiness, anger, fear, sadness, surprise, and disgust. The short version of the FEEST has been recently developed and validated for clinical and research applications (Kuhlmann & Margraf, Reference Kuhlmann and Margraf2023). For rapid, computerized screening, the Penn Emotion Recognition Test (ER-40; Kohler et al., Reference Kohler, Turner, Bilker, Brensinger, Siegel, Kanes, Gur and Gur2003) provides a concise and psychometrically validated measure of facial emotion recognition. Participants are shown 40 photographs of faces depicting basic emotions (happiness, sadness, anger, fear, and neutral) at varying intensity levels and are asked to identify the emotion expressed. The task yields accuracy scores for individual emotions and an overall recognition index, and has demonstrated good reliability and sensitivity to clinical deficits (Pinkham et al., Reference Pinkham, Penn, Green, Harvey and Gur2014).
Notable efforts have aimed to integrate emotion recognition tasks directly into widely used neuropsychological batteries to facilitate routine assessment. A prominent example is the Advanced Clinical Solutions (ACS) designed to supplement the Wechsler Adult Intelligence Scale - Fourth Edition (WAIS-IV) and the Wechsler Memory Scale - Fourth Edition (WMS-IV) (Pearson, 2009). Despite framing these abilities within the broader construct of Social Perception, the ACS specifically assesses the perceptual component of social cognition through facial affect naming and prosody identification tasks. Being co-normed with the WAIS-IV, the ACS offers robust psychometric properties and allows clinicians to interpret social–emotional deficits directly in the context of general intellectual functioning. Its wide availability and standardization across multiple countries make it a valuable resource for clinical practice.
Furthermore, dynamic tools offer greater relevance to real-world functioning than static photographs. The Awareness of Social Inference Test (TASIT; McDonald et al., Reference McDonald, Flanagan, Rollins and Kinch2003), while broadly used for social cognition, provides a specific subtest for emotion recognition (Part 1: The Emotion Evaluation Test), which assesses the recognition of spontaneous emotional expressions in dynamic video scenarios. Multidomain tools such as EMOTICOM (Bland et al., Reference Bland, Roiser, Mehta, Schei, Boland, Campbell-Meiklejohn, Emsley, Munafo, Penton-Voak, Seara-Cardoso, Viding, Voon, Sahakian, Robbins and Elliott2016) also include modules for facial emotion recognition, allowing integration with tasks of motivation and impulsivity. Nonetheless, fully standardized multimodal clinical tools that integrate facial, vocal, and bodily cues, and that include comprehensive normative data across different cultures, are still needed. Other established instruments provide complementary perspectives on emotional processing. The Bell-Lysaker Emotion Recognition Test (BLERT; Bell et al., Reference Bell, Bryson and Lysaker1997) uses dynamic audiovisual stimuli to assess emotion recognition from both facial and vocal cues, offering a more nuanced and multimodal representation of social interactions than static tasks..
Social cognition and the theory of mind
Social cognition encompasses the set of cognitive and affective processes that enable individuals to perceive, interpret, and respond appropriately to social information. It involves multiple components, including the recognition of emotions, the understanding of social cues and norms, empathy, and the capacity to infer others’ beliefs, intentions, and emotions – collectively referred to as ToM. While closely related, ToM specifically denotes the ability to infer mental states and predict others’ behavior, whereas social cognition represents a broader construct that also includes affective and motivational aspects such as empathy and moral reasoning (Adolphs, Reference Adolphs2009; Happé et al., Reference Happé, Cook and Bird2017).
Deficits in this domain are formally recognized in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR; American Psychiatric Association, 2022) as a core neurocognitive feature (see also Henry et al., Reference Henry, von Hippel, Molenberghs, Lee and Sachdev2016). Converging evidence from neuroimaging and lesion studies highlights the role of prefrontal and temporo-parietal circuits in social cognition, with the right hemisphere damage often producing disproportionate impairments. Clinically, impaired social cognition is associated with poorer quality of life and reduced autonomy (Henry et al., Reference Henry, von Hippel, Molenberghs, Lee and Sachdev2016), and may also contribute to increased caregiver burden. This can be seen in patients who appear cognitively intact on standard testing yet fail to understand irony or hidden intentions in everyday conversation, leaving them socially isolated despite “normal” neuropsychological profiles.
Several standardized instruments and tasks are available. The Reading the Mind in the Eyes Test (RMET; Baron-Cohen et al., Reference Baron-Cohen, Wheelwright, Hill, Raste and Plumb2001) provides a rapid measure of primarily affective ToM, requiring participants to infer complex mental states by selecting the most appropriate descriptor for photographs of the eye region. Although widely used for its brevity, it has been criticized for its limited representativeness of complex social interactions, cultural bias, and partial coverage of ToM components, being more related to emotion perception and lexical knowledge than to inferential reasoning (Olderbak et al., Reference Olderbak, Wilhelm, Olaru, Geiger, Brenneman and Roberts2015). Dynamic, video-based tasks offer more contextually rich and multidimensional approaches. Regarding dynamic assessment, the TASIT (Parts 2 and 3; McDonald et al., Reference McDonald, Flanagan, Rollins and Kinch2003) presents short acted video vignettes depicting everyday interactions to assess the comprehension of sarcasm and deception. Participants are asked to interpret the communicative intentions of the actors, offering a more informative sample of pragmatic and social-inferential abilities. The Movie for the Assessment of Social Cognition (MASC; Dziobek et al., Reference Dziobek, Fleck, Kalbe, Rogers, Hassenstab, Brand, Kessler, Woike, Wolf and Convit2006) adopts a similar format, showing a film sequence in which participants answer multiple-choice questions about characters’ thoughts, feelings and intentions. The Edinburgh Social Cognition Test (ESCoT; Baksh et al., Reference Baksh, Abrahams, Auyeung and MacPherson2018) is a recent instrument combining ToM and social norm understanding within brief animated scenarios. It provides separate indices for cognitive and affective ToM as well as for knowledge of implicit social rules, offering an integrated evaluation of social cognition that better approximates aspects of everyday social functioning. Finally, the Mini-SEA battery (Bertoux et al., Reference Bertoux, Delavest, de Souza, Funkiewiez, Lépine, Fossati, Dubois and Sarazin2012) combines faux-pas detection with emotion recognition, capturing both affective and cognitive components of social cognition. It has been validated in several neurodegenerative conditions, including frontotemporal dementia. Collectively, these instruments provide complementary perspectives for the multidimensional assessment of social cognition and ToM, although further work is needed to enhance their capacity to capture clinically relevant dimensions of everyday functioning, and to improve their cross-cultural adaptation, and clinical integration.
Emotional-cognitive interference: A modulatory mechanism
Emotional and motivational processes continuously interact with cognitive processes, shaping attention, executive control, and memory. This interaction, often referred to as emotional–cognitive interference, describes how affective stimuli can bias or disrupt cognitive performance, particularly under conditions requiring selective attention or inhibitory control (Dolcos & McCarthy, Reference Dolcos and McCarthy2006; Okon-Singer et al., Reference Okon-Singer, Hendler, Pessoa and Shackman2015; Pessoa, Reference Pessoa2008). While “interference” implies a disruptive cost to “cold” cognitive efficiency, this interaction reflects an adaptive prioritization of biologically and socially salient information (Dolcos et al., Reference Dolcos, Iordan and Dolcos2011; Pessoa, Reference Pessoa2008). Clinically, performance costs in standardized tasks often correspond to the adaptive ability to reorient attention toward meaningful environmental cues (Okon-Singer et al., Reference Okon-Singer, Hendler, Pessoa and Shackman2015). Understanding this dynamic is essential: patients may perform adequately in neutral contexts yet show marked inefficiency under emotional salience (Phillips et al., Reference Phillips, Drevets, Rauch and Lane2003; Todd et al., Reference Todd, Miskovic, Chikazoe and Anderson2020).
The Emotional Stroop Task (Williams et al., Reference Williams, Mathews and MacLeod1996) measures the degree of interference exerted by emotionally salient information on selective attention processes. Participants are asked to name the color of emotionally charged or neutral words as quickly and accurately as possible. Longer reaction times or higher error rates for emotional words reflect a difficulty in disengaging attention from affective content, indicating biased information processing. Variants of this paradigm have been applied to the study of anxiety, depression, post-traumatic stress disorder, and brain injury (Dresler et al., Reference Dresler, Mériau, Heekeren and van der Meer2009).
The Affective Go/No-Go Task (Murphy et al., Reference Murphy, Sahakian, Rubinsztein, Michael, Rogers, Robbins and Paykel1999; Schulz et al., Reference Schulz, Fan, Magidina, Marks, Hahn and Halperin2007) evaluates inhibitory control under emotional load. Participants are instructed to respond to stimuli from a target emotional category (Go) and to withhold responses to stimuli from a non-target category (No-Go), with a higher proportion of go trials inducing a prepotent response tendency. Emotional stimuli (e.g., happy or sad faces, positive or negative words, pleasant or unpleasant pictures) are used to elicit affective interference, making inhibition more demanding. Commission errors and reaction times in emotional versus neutral conditions provide an index of how affective context influences inhibitory mechanisms. Reduced inhibition for emotionally salient cues occurs in healthy individuals and tends to be amplified in individuals with mood disorders, frontotemporal lesions, and traumatic brain injury (Elliott et al., Reference Elliott, Rubinsztein, Sahakian and Dolan2000; Hsieh et al., Reference Hsieh, Leyton, Caga, Flanagan, Kaizik, O’Connor, Kiernan, Hodges, Piguet and Mioshi2016).
The Dot-Probe Task (Bradley et al., Reference Bradley, Mogg, White, Groom and de Bono1999; MacLeod et al., Reference MacLeod, Mathews and Tata1986; Mogg & Bradley, Reference Mogg and Bradley2018) examines attentional orienting toward and disengagement from emotional stimuli. Two stimuli, typically one emotional and one neutral, are briefly presented side by side, followed by a probe (e.g., a dot) replacing one of them. Faster responses to probes appearing in the location of emotional stimuli indicate an attentional bias toward affective information. The task has been widely used in anxiety research and, more recently, in studies of acquired brain injury, highlighting alterations in emotional salience processing and difficulties in attentional shifting.
Although originally developed for experimental research, these tasks provide valuable insights into how emotional processing modulates cognitive control, attention, and response inhibition, crucial functions for adaptive behavior in everyday life – resulting in interference with performance. The targeted inclusion of emotional modulation measures in neuropsychological assessment protocols may enhance diagnostic precision and improve the clinical utility and predictive power of cognitive evaluation, particularly in patients with emotional dysregulation or inconsistent cognitive performance across neutral and emotional contexts (Dolcos & McCarthy, Reference Dolcos and McCarthy2006; Okon-Singer et al., Reference Okon-Singer, Hendler, Pessoa and Shackman2015; Pessoa, Reference Pessoa2008).
Discussion
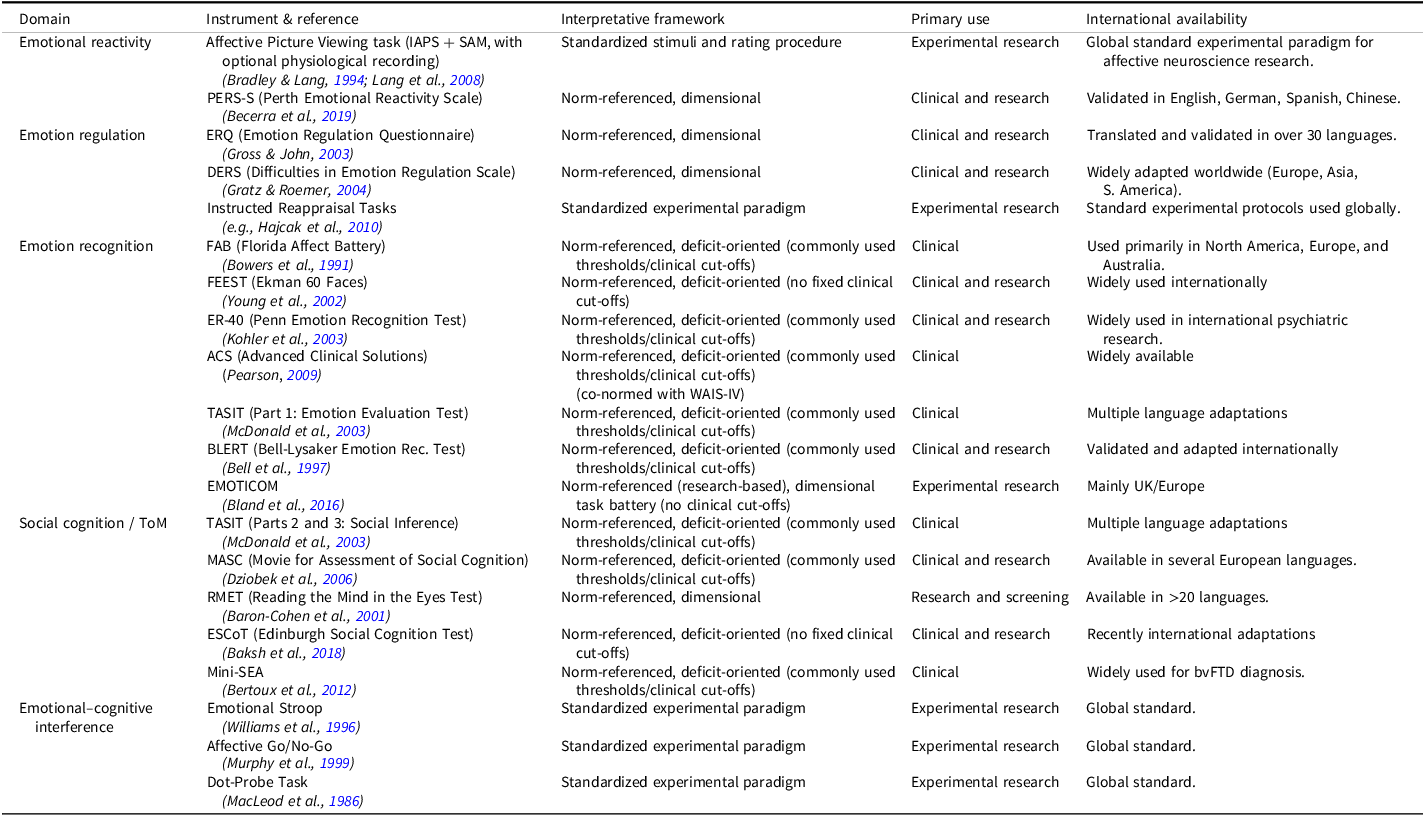
The evidence highlights a discrepancy in current neuropsychological practice: validated tools for affective processes are available (see Table 1; Quesque et al., Reference Quesque, Nivet, Etchepare, Wauquiez, Prouteau, Desgranges and Bertoux2022; Rabin et al., Reference Rabin, Barr and Burton2005, Reference Rabin, Paolillo and Barr2016), their systematic use remains rare (Henry et al., Reference Henry, von Hippel, Molenberghs, Lee and Sachdev2016; McDonald, Reference McDonald2017; Priluck & Fedio, Reference Priluck and Fedio2022).
Comprehensive overview of standardized tools and experimental paradigms for the assessment of affective and motivational domains

Table 1. Long description
The table presents a comprehensive overview of standardized tools and experimental paradigms for assessing affective and motivational domains. It includes columns for domain, instrument and task, interpretation, primary use, international use, and references. The table lists various instruments and tasks such as the International Affective Picture System, Emotional Stroop Task, Emotion Recognition from Dynamic Faces, and others. Each row provides details on the interpretation, primary use, and international use of these instruments. The table highlights the discrepancy in current neuropsychological practice, where validated tools are available but their systematic use remains rare.
Note: The column Interpretative framework specifies how scores are interpreted for each instrument. Norm-referenced, deficit-oriented instruments provide population-based normative data to identify statistically significant deviations from expected performance based on established thresholds, such as clinical cut-offs, percentiles, or deviations from the mean (e.g., Mini-SEA, FAB, ESCoT). These thresholds allow identification of potential impairments in a categorical manner (“impaired” vs “unimpaired”). Dimensional instruments are interpreted along continuous trait or ability dimensions using psychometric norms, such as means, standard deviations, or percentiles, to situate an individual’s performance relative to the population, without implying categorical clinical impairment (e.g., ERQ, PERS-S, DERS, RMET, EMOTICOM). Standardized experimental paradigms involve tasks with fixed stimuli and procedures to assess performance patterns, but typically lack normative reference values for individual clinical classification. Importantly, clinical or research use encompasses both deficit identification and dimensional assessment, and does not always imply the application of binary clinical cutoffs.
Figure 1 provides a conceptual overview of these domains and their interrelations, illustrating how emotional and motivational processes contribute to functional adaptation in daily life and how emotional modulation of cognitive control may influence cognitive performance. Surveys and review papers consistently show that most neuropsychologists seldom incorporate affective measures, focusing instead on traditional “cold” cognitive domains (Henry et al., Reference Henry, von Hippel, Molenberghs, Lee and Sachdev2016; McDonald, Reference McDonald2017; Priluck & Fedio, Reference Priluck and Fedio2022; Quesque et al., Reference Quesque, Nivet, Etchepare, Wauquiez, Prouteau, Desgranges and Bertoux2022; Rabin et al., Reference Rabin, Paolillo and Barr2016). This omission may have several important implications.
The model illustrates four core domains of emotional and motivational functioning: emotional reactivity, emotion regulation, emotion recognition, and social cognition/Theory of mind, each associated with representative assessment tools and clinical correlates. These domains collectively contribute to functional relevance of evaluation, supporting the identification of clinically relevant dimensions of functioning and informing rehabilitation planning. Additionally, emotional–cognitive interference is depicted as a cross-cutting modulatory mechanism reflecting the interplay between affect and cognition. This highlights how affective salience may influence standardized performance levels by prioritizing biologically and socially meaningful information. Abbreviations: PERS-S = Perth Emotional Reactivity Scale – Short Form; DERS = Difficulties in Emotion Regulation Scale; ACS = Advanced Clinical Solutions; TASIT = The Awareness of Social Inference Test; MASC = Movie for the Assessment of Social Cognition; Mini-SEA = Mini Social Cognition and Emotion Assessment; ER-40 = Emotion Recognition – 40 Items; FEEST = Facial Expressions of Emotion: Stimuli and Test; TBI = Traumatic Brain Injury; FTD = Frontotemporal Dementia; bvFTD = Behavioral Variant Frontotemporal Dementia. Created with BioRender.com.

Figure 1. Long description
The flowchart illustrates the framework for assessing emotional and motivational domains in neuropsychology. At the top, it highlights functional adaptation in daily life, emphasizing functional relevance, rehabilitation, and quality of life. This leads to four core domains: emotion reactivity, emotion regulation, emotion recognition, and social cognition/Theory of mind. Each domain is associated with specific assessment tools and clinical correlates. Emotion reactivity involves picture viewing tasks and sensitivity to affective stimuli, relevant to conditions like stroke, TBI, and mood disorders. Emotion regulation includes tasks and cognitive control, important for psychiatric disorders and brain injury. Emotion recognition assesses deficits in stroke, FTD, schizophrenia, Parkinson’s disease, and Alzheimer’s disease. Social cognition/Theory of mind focuses on empathy, social inference, and conditions like bvFTD, schizophrenia, and multiple sclerosis. At the bottom, emotional-cognitive interference is depicted, showing biases in attention and executive control under emotional load, relevant to TBI, FTD, and anxiety disorders.
First, it reduces the assessment’s coverage of clinically relevant dimensions of everyday functioning: cognitive in controlled conditions may fail to sample real-world challenges where affective and social demands are ubiquitous (McDonald, Reference McDonald2017). For example, might succeed on cognitive tasks but fail to interpret social cues or discontinue rehabilitation due to frustration, highlighting where “hot” measures could inform tailored treatment. Second, omitting these factors leads to incomplete diagnoses; social impairments may be missed despite “normal” executive scores (Henry et al., Reference Henry, von Hippel, Molenberghs, Lee and Sachdev2016). Third, it compromises rehabilitation planning, as dysregulation or impaired empathy hinders therapeutic engagement. Without systematic assessment, the mechanisms driving divergent clinical trajectories, such as successful reintegration versus treatment discontinuation, remain invisible to clinicians.
Moreover, emotional and motivational disturbances have a profound impact on patients’ families and primary caregivers. Beyond cognitive decline, “hot” changes like irritability or reduced empathy are often the most distressing for families (de Vugt & Verhey, Reference de Vugt and Verhey2013; Henry et al., Reference Henry, von Hippel, Molenberghs, Lee and Sachdev2016). Affective dysfunctions predict caregiver burden and family stress more strongly than cognitive deficits (García-Alberca et al., Reference García-Alberca, Lara, Garrido, Gris, González-Herero and Lara2014; Hsieh et al., Reference Hsieh, Leyton, Caga, Flanagan, Kaizik, O’Connor, Kiernan, Hodges, Piguet and Mioshi2016; Massimo et al., Reference Massimo, Powers, Evans, McMillan, Rascovsky, Eslinger, Ersek, Irwin and Grossman2015). Systematic assessment can therefore inform psychoeducational interventions aimed at improving family well-being. Encouragingly, recent advances in psychometric test development are beginning to address these shortcomings. An important distinction must be made here between performance-based tasks and clinical scales. Brief validated scales, such as the PERS-S for emotional reactivity (Becerra et al., Reference Becerra, Preece, Campitelli and Scott-Pillow2019) and the DERS-16 for emotion regulation (Bjureberg et al., Reference Bjureberg, Ljótsson, Tull, Hedman, Sahlin, Lundh, Bjärehed, DiLillo, Messman-Moore, Gumpert and Gratz2016; Sousa et al., Reference Sousa, Linharelhos, Silva and Rijo2023), allow for the integration of the patient’s subjective reports into the diagnostic process. Rather than merely classifying performance, these scales capture the patient’s perceived functional status, helping to bridge the gap between purely performance-based deficits and the specific functional challenges encountered in daily life. Furthermore, efforts have been made to integrate social cognition into standard batteries, such as the ACS for WAIS-IV, which allows for the assessment of social perception alongside intellectual functioning. Among these, dynamic measures like the TASIT (McDonald et al., Reference McDonald, Flanagan, Rollins and Kinch2003) and MASC (Dziobek et al., Reference Dziobek, Fleck, Kalbe, Rogers, Hassenstab, Brand, Kessler, Woike, Wolf and Convit2006) offer informative insights into complex social interactions. Beyond these clinical tools, experimental frameworks are emerging that aim to integrate affective, motivational, and cognitive processes within a unified approach. A prominent example is the EMOTICOM battery (Bland et al., Reference Bland, Roiser, Mehta, Schei, Boland, Campbell-Meiklejohn, Emsley, Munafo, Penton-Voak, Seara-Cardoso, Viding, Voon, Sahakian, Robbins and Elliott2016), which combines tasks of reinforcement learning, affective decision-making, and emotion recognition. Although primarily designed for research, such integrative paradigms may pave the way toward clinical tools that, when integrated into multi-source assessment protocols, may provide a more informative sample of the patient’s real-world functional outcomes. Importantly, the selective use of these instruments involves a trade-off between different interpretative frameworks: while norm-referenced instruments (e.g., Mini-SEA, ACS) provide population-based thresholds to identify categorical impairments, dimensional scales (e.g., ERQ, DERS) offer a more nuanced characterization of the patient’s experience without implying binary conceptualizations of clinical deficits.
Before implementing such targeted evaluations, it would be valuable to develop a brief screening tool for emotional–motivational functions, conceptually similar to the Mini-Mental State Examination (MMSE; Folstein et al., Reference Folstein, Folstein and McHugh1975) or the Montreal Cognitive Assessment (MoCA; Nasreddine et al., Reference Nasreddine, Phillips, Bédirian, Charbonneau, Whitehead, Collin and Chertkow2005) used in cognitive assessment. Such a measure should provide a rapid and standardized overview of the key affective–motivational domains discussed above, while also capturing the extent to which emotional or motivational factors modulate individual cognitive performance. This aspect is crucial, as it reflects the dynamic interplay and adaptive integration between “hot” and “cold” cognition. Within an integrated assessment framework, this modulation provides an informative sample of the patient’s real-world functional challenges, ultimately enhancing the clinical utility and predictive power of the neuropsychological evaluation.
To ensure a comprehensive reflection of the individual’s functioning, such a screening should not rely exclusively on self-report questionnaires, which mainly capture conscious and verbally mediated aspects of emotion. Instead, it should combine brief structured tasks with subjective rating and clinical observation, allowing for a multidimensional assessment of both explicit and implicit affective processes. Importantly, clinical observation should not be limited to unsystematic subjective impressions or isolated items often found in broader scales (e.g., generic ratings of apathy or disinhibition); rather, it should be integrated as a structured component of the clinical formulation. This structured screening would serve as an initial step to identify possible emotional or motivational alterations and their impact on daily functioning, thereby guiding further in-depth evaluation. Within this modular approach, not all patients will require an extended evaluation: instruments should be selected according to the specific clinical question and the patient’s observed symptoms. For example, in cases of interpersonal or social difficulties, an emotion recognition or Theory of Mind task may be added. Importantly, many of the affective measures described above, including both scales and structured tasks, are brief and can be administered within minutes, keeping the overall assessment time feasible while maintaining diagnostic depth.
Another crucial point concerns training. Many neuropsychologists report low confidence in selecting or interpreting affective measures, reflecting gaps in formal training and the limited systematic coverage of these domains in professional education (McDonald, Reference McDonald2017; Priluck & Fedio, Reference Priluck and Fedio2022). Expanding training programs to include standardized affective assessment tools is therefore essential to bridge the gap between the availability of validated instruments and their implementation in clinical practice.
Furthermore, efforts in cross-cultural adaptation are necessary to ensure that scientific knowledge translates into daily practice globally. Rather than a limitation, this represents a strategic opportunity: investing in validation and training could position the field toward a more integrative and comprehensive approach to neuropsychology. Taken together, these considerations highlight both the current limitations of practice and the opportunities for innovation. The next section outlines key directions for future development.
Future directions
The integration of affective and motivational domains into neuropsychological assessment requires not only theoretical advances but also practical solutions. Several priorities should guide future developments.
Training and expertise
Many neuropsychologists report limited confidence in selecting and interpreting affective measures, reflecting insufficient attention to these domains within academic and professional curricula. Expanding graduate programs, continuing education, and supervised clinical practice is essential to bridge the gap between available tools and their actual use in clinical settings.
Feasibility and sustainability
Some affective instruments, particularly dynamic video-based tasks are time-consuming and challenging to integrate into standard neuropsychological batteries. The development of shorter and computerized versions of these instruments could further reduce administration time.
Accessibility and cost
Several multidimensional instruments require expensive licenses, which limit their dissemination in public healthcare settings and small clinics. Investing in affordable or open-access adaptations, particularly digital formats, would promote wider implementation and equity of access.
Cross-cultural adaptation
In many countries, validated translations of affective assessment tools are still limited. Systematic efforts in cultural adaptation and validation are necessary to ensure scientific rigor and clinical applicability across diverse contexts.
Technological innovation
Advances in computerized testing, mobile applications, and virtual reality offer promising opportunities to embed emotional and social stimuli within more naturalistic and immersive digital environments. These tools may also facilitate the longitudinal monitoring of patients’ functioning in their everyday life contexts.
Development of emotional–motivational screening tools
Most available affective instruments were designed for research rather than routine practice. There is a pressing need for brief, psychometrically sound and culturally adaptable screening measures for early identification of alterations. Furthermore, integrative batteries combining affective and cognitive components should be developed to complement existing assessments without excessively prolonging evaluation time.
By addressing these priorities, neuropsychology can move beyond a purely cognitive focus toward a more comprehensive and patient-centered model of assessment that is both standardized and clinically feasible.
Conclusion
Emotions and cognition are deeply interconnected processes that jointly shape human behavior (Pessoa, Reference Pessoa2008; Todd et al., Reference Todd, Miskovic, Chikazoe and Anderson2020). By privileging only “cold” cognition, neuropsychology risks overlooking impactful consequences of brain disorders, such as impairments in emotion regulation and social interaction (Henry et al., Reference Henry, von Hippel, Molenberghs, Lee and Sachdev2016; McDonald, Reference McDonald2017). Validated tools now exist for assessing emotional reactivity, regulation, recognition, and social cognition. Growing evidence indicates that these domains are crucial not only for diagnostic accuracy, but also for capturing clinically relevant dimensions of functioning and predicting rehabilitation outcomes. To bridge the gap between research and practice, we advocate the systematic integration of emotional and motivational assessment within neuropsychological evaluation. A feasible next step may involve the development of a brief screening tool for emotional and motivational functions, conceptually analogous to the Mini-Mental State Examination (MMSE; Folstein et al., Reference Folstein, Folstein and McHugh1975) or the Montreal Cognitive Assessment (MoCA; Nasreddine et al., Reference Nasreddine, Phillips, Bédirian, Charbonneau, Whitehead, Collin and Chertkow2005) used in neurocognitive screening, followed by a modular approach tailored to the clinical question and patient profile. Such an approach would balance diagnostic depth with clinical efficiency, enhancing the predictive value of neuropsychological assessment. Ultimately, successful rehabilitation is not defined solely by whether a patient can sustain attention, remember information, or solve problems, but by whether they can return to work, maintain relationships, and navigate the emotional complexity of daily life. Neuropsychology must rise to this challenge. By integrating performance-based affective measures with subjective clinical reports and qualitative observations, we can move closer to the true goal of our field: characterizing the individual functional profile and supporting patients in achieving improved psychosocial outcomes, social reintegration, and autonomy.
Competing interests
The authors declare no competing interests.
Sources of support
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Use of artificial intelligence
ChatGPT (OpenAI, GPT-4) was used to support English language editing. All content was reviewed and approved by the authors, who take full responsibility for the manuscript.


 Open access
Open access