


Introduction
When countries face a health crisis, like the COVID-19 pandemic, a mitigation mechanism involves the public’s participation. However, distrust in the government and medical system because of discrimination can hinder the participation and eradication of the crisis. Existing studies demonstrate the critical effects that ethnic marginalization had during public health crises. The seminal work by Cohen (Reference Cohen1999) illustrates how the historical marginalization has endangered addressing the AIDS crisis within African American communities. Lieberman (Reference Lieberman2009) argues that the ethnic boundaries in South Africa and India have prevented effective policy responses against AIDS through attributions of blame and prejudice to certain ethnic groups. Throughout the history of pandemics across the globe, marginalization based on ethnicity and race has been shown to heighten during public health crises (Dionne and Turkmen, Reference Dionne and Turkmen.2020).
In this context, existing scholarship discusses the relationship between ethnicity and vaccination intention. The history of racial injustices and unpleasant experiences with the healthcare system have affected vaccine hesitancy among the ethnically and racially marginalized (Black and Hispanics) in the US (Hildreth and Alcendor, Reference Hildreth and Alcendor.2021; Khubchandani and Macias, Reference Khubchandani and Macias.2021; Woolf et al., Reference Woolf2021). The vaccine hesitancy among ethnically minoritized communities is also found elsewhere, such as Hong Kong (Singh et al., Reference Singh, Lai, Wang, Asim, Chan, Wang and Yeoh2021) and Venezuela (Andrade, Reference Andrade2021).
The aim of this study is to examine the relationship between ethnic marginalization, political trust, and vaccination intention in 14 African countries. This study builds on previous studies’ findings that ethnically marginalized groups of people are more hesitant to comply with public health policies or receive vaccines out of their distrust of the government and health system (Arriola and Grossman, Reference Arriola and Grossman.2021; Nguyen et al., Reference Nguyen2022). Arriola and Grossman (Reference Arriola and Grossman.2021) emphasize that “ethnicized trust” was significant in explaining different patterns of HIV/AIDS policy compliance among Guineans (809). Nguyen et al. (Reference Nguyen2022) argues that discrimination against racially minoritized groups engenders government distrust and influences COVID-19 vaccine hesitancy in the US and the UK. This study incorporates arguments from previous studies on ethnicity, health, and political trust and suggests that the decreased government trust based on ethnic marginalization can influence the level of vaccination intention during a health crisis. A case in consideration is COVID-19 vaccination.
This study offers an original contribution by using a “causal mediation analysis” method to examine the mediating role of political trust in the relationship between ethnic marginalization and vaccination intention. Another contribution is this study’s focus on African countries. The causal mediation analysis of nationally representative survey data, collected between 2019 and 2022 across 14 African countries, finds that the relationship between ethnic marginalization and vaccination intention is mediated by government trust. Individuals who perceive unfair treatment toward their ethnic group by the government are less likely to trust that the same government will ensure vaccine safety and, therefore, are less inclined to receive vaccines. We further our analysis by discussing cross-country heterogeneity in ethnic relations among these countries and narrowing our analysis to a single country case of Morocco. The findings indicate that the marginalized Amazighen and Sahrawi ethnic groups have lesser vaccination intentions due to their lower levels of trust in the government.
The findings have implications for global health policy. To prepare for a crisis is to address the injustice during non-crisis times. This study’s results suggest that the marginalization of ethnic minorities during non-crisis times erodes their political trust and negatively affects their vaccination intention during crisis times. Public health is a public good that necessitates all citizens’ collective action. If the government excludes certain groups of individuals from public goods during non-crisis times, whether it is political power or healthcare access, it cannot expect them to work for public goods only during crisis times. Public policies during non-crisis times are critical for the success of crisis mitigation policies. Therefore, ethnic marginalization as a root factor must be addressed to increase political trust and public health policy compliance during a crisis.
Background: approaching ethnic marginalization and political trust
The discussion of ethnic marginalization in African countries entails perspectives of constructivism and historical institutionalism by considering inherited institutions in laying out how ethnic marginalization and government distrust develop. Accordingly, this section starts by discussing the impact of colonization on ethnic dynamics in African countries. Then, the latter half of the section discusses how the extent to which ethnic identities become salient in the society and politics vary across countries depending on local contexts and institutional configuration in each country. Thus, this background section highlights the cross-country heterogeneity and non-deterministic views of constructed ethnic relations as well as the agency of each state in building power-sharing institutions, while recognizing the historical injustices of colonialism in discussing government distrust in African countries.
First, it is critical to recognize that colonial institutions were not set up to foster unity but to divide African societies to facilitate resource extraction and control by the colonial governments (Acemoglu et al., Reference Acemoglu, Johnson and Robinson.2001). Ethnic diversity itself is not inherently conflictual (Beissinger, Reference Beissinger2008). Rather, divisions and conflicts are a function of the colonial institutions (Rabinowitz, Reference Rabinowitz2020), and the perspective of historical institutionalism suggests that political institutions are path dependent. This includes extractive institutions that marginalizes segments of the population, eroding political legitimacy and political trust.
At the same time, whether and to what extent ethnic identity becomes salient and mobilized in the society and politics depend on more factors. For instance, evidence of ethnic favoritism by a co-ethnic political leader as reflected on such things as health and education outcomes depends on types of public goods and outcomes (Kramon and Posner, Reference Kramon and Posner.2013). It may also depend on regime types. Burgess et al. (Reference Burgess, Jedwab, Miguel, Morjaria and Padró i Miquel.2015) find a presence of ethnic favoritism in Kenya under authoritarian regimes, but not when Kenya is a democracy. To further challenge the deterministic effect of ethnic diversity in politics, Horowitz (Reference Horowitz2022) finds that political leaders do not necessarily mobilize voters across ethnic lines in multiparty democracy. In Kenya since 2002, presidential candidates have adopted policies that appeal to a broader audience in order to attract swing voters who do not share the same ethnic identities with presidential candidates (Horowitz, Reference Horowitz2022). Indeed, “between 30% and 52% of voters in sub-Saharan Africa tend not vote for their ethnic group’s party” (Harris, Reference Harris2022). In Malawi, Ferree et al. (Reference Ferree, Dulani, Harris, Kao, Lust, Jansson and Metheney2023) find limited evidence that the pandemic intensifies the ethnic identities.
Thus, this study is not about the effect of ethnic diversity during the pandemic and is not about a linkage between ethnic diversity and societal conflicts. Nor is it based on deterministic views about multi-ethnic societies. Rather, it is about specific circumstances where ethnic marginalization by the government is present and it erodes political trust. In such circumstances, historical exclusion influences deep-seated sentiments of dissatisfaction and distrust (Phillips, Reference Phillips2006).
Trust is a critical concept during times of the global health crises. Previous studies mainly focused on two separate but related types of trust that can influence individuals’ social and political decision-making processes in the global COVID-19 crisis: trust in the health system and trust in the government/political system. For instance, individuals in Malawi expressed a greater intention for COVID-19 testing when it is offered by the WHO rather than public clinics, reflecting a greater trust in the WHO over the national healthcare system (Ferree et al., Reference Ferree, Harris, Dulani, Kao, Lust and Metheney2021). Individuals with more trust in health authorities, especially pro-government health authorities, were less susceptible to COVID-19 conspiracy theories in Turkey (Wu et al., Reference Wu, Ozan Kuru, Çarkoglu, Cemalcilar and Yıldırım2024). On the other hand, the concern over COVID-19 reduced trust in the government to handle the pandemic, while it did not affect turnout and vote choice in the 2020 presidential election in Malawi (Dulani et al., Reference Dulani, Harris, Lust, Ferree, Kao, Jansson and Metheney2021).
This study focuses on political trust as individuals’ perception of the government’s ability to handle its tasks (Dulani et al., Reference Dulani, Harris, Lust, Ferree, Kao, Jansson and Metheney2021; Dal and Tokdemir, Reference Dal and Tokdemir.2022). Political trust inspires citizens’ actions because trust judgment shows the beliefs and trustworthiness of the political institutions and systems (Levi and Stoker, Reference Levi and Stoker.2000). Therefore, when individuals face social and political distortion, such as ethnic marginalization, political distrust can grow, and the political system’s untrustworthiness can lead to citizens’ uncooperative behaviors.
Theory: linking ethnic marginalization, political trust, and vaccination intention
The sense of unfairness determines whether people think the government works in their interest. Ethnic marginalization breeds long-lasting historical and perennial sentiments that strengthen the bonds within the marginalized group (Jamal, Reference Jamal2005; Masuoka, Reference Masuoka2006) and consolidates a unified consciousness. According to the fairness heuristic theory, there is a relationship between fair treatment and the perception of safety and belonging in an organization (in this case, a state) that uses a fair procedure (Tyler and Lind, Reference Tyler and Lind.1992). Fair treatment influences a feeling of belonging and acceptance of the outcome of the procedure (Tyler and Lind, Reference Tyler and Lind.1992). Among marginalized groups, group identity shapes the heuristics by which they evaluate their government. Their feeling of fairness in political institutions will influence trust and compliance with public policy (Grimes, Reference Grimes2006).
Once political trust becomes an ethnically relevant matter, and citizens repeatedly experience governmental ethnic favoritism and discrimination, individuals start to mistrust the state, demonstrated by rejecting or resisting state policies (Arriola and Grossman, Reference Arriola and Grossman.2021). Governmental discrimination in health service provisions (Carpenter, Reference Carpenter2012) and varying policy preferences over different social groups (Lieberman, Reference Lieberman2009; Lieberman and McClendon, Reference Lieberman and McClendon.2013) can create conflicting reputations of the government among citizens (Carpenter, Reference Carpenter2014). A varying quality of the service provisions to different ethnic groups can exacerbate mistrust of the government. In this case, politically marginalized ethnic groups (that lack political power and co-ethnic elites in the government) are more likely to doubt governmental policies and less likely to comply with the policies, because they cannot trust that the policies are truly beneficial for their group (Arriola and Grossman, Reference Arriola and Grossman.2021).
As a result, basic public policy implementations, such as public health protocol, become difficult (Levi et al., Reference Levi, Sacks and Tyler.2009). Historical and structural oppression breeds distrust in the government during a public health crisis (e.g., the Ebola outbreak in 2014) (Benton and Dionne, Reference Benton and Dionne.2015). Previous research has shown that non-compliance with health protocol and underperformed health outcomes are associated with political mistrust (LaVeist et al., Reference LaVeist, Isaac and Williams.2009; Heymann et al., Reference Heymann2015; Mesch and Schwirian, Reference Mesch and Schwirian.2015; Alsan and Wanamaker, Reference Alsan and Wanamaker.2018). Arriola and Grossman (Reference Arriola and Grossman.2021) show that “ethnicized” government trust influenced citizens’ compliance with HIV/AIDS-related public health advisory in Guinea. During the West African Ebola crisis, citizens’ distrust of the government was related to non-compliance with the government-mandated health protocols, such as mandated quarantine or burial practices (Arthur et al., Reference Arthur, Horng, Tandanpolie, Gilstad, Tantum and Luby2023) as well as social distancing and sanitation against the virus (Blair et al., Reference Blair, Morse and Tsai.2017).
Marginalized ethnic groups become attuned to associating public policy and services not with their interest but with the interest of the political majority. In the eyes of the marginalized, the government does not serve their interest but the interest of the political majority. In situations where credible information to base upon decisions is not available, procedural fairness becomes a heuristic substitute in the process of judging an outcome one has received from the authority (Van den Bos et al., Reference Van den Bos, Lind, Wilke. and Cropanzano2001). Therefore, when citizens cannot acquire complete information because of a fast-changing emergency crisis, ethnically politicized and marginalized groups who also distrust the government, are more likely to resist government health protocols by perceiving that they are unfair or even malevolent and that compliance would bring further disadvantages (Cordasco et al., Reference Cordasco, Eisenman, Glik, Golden and Asch2007; Hewlett and Hewlett, Reference Hewlett and Hewlett.2008; Wilkinson and Fairhead, Reference Wilkinson and Fairhead.2017). Members of an ethnic group may judge whether the government works in their interest depending on whether public policy outcomes meet their needs. If they perceive unfair treatment, they will not trust the government (Schildkraut, Reference Schildkraut2005). Perceived procedural fairness determines government legitimacy and compliance (Grimes, Reference Grimes2006).
The lack of trust in the government can worsen during crisis times. Some crisis mitigation policies may be draconian and could exacerbate the existing distrust. For instance, during the COVID-19 pandemic, some governments adopted harsh measures that violated individual human rights by strongarming their populations (Altshuler, Reference Altshuler2020). Marginalized groups are more likely to be affected; they will likely be on the wrong end of the government’s strict policies during health emergencies (Sekalala et al., Reference Sekalala, Dagron, Forman and Mason Meier2020; Yu and Keralis, Reference Yu and Keralis.2020) due to baked-in institutional unfairness. For instance, a Sahrawi man in Morocco-occupied Western Sahara cited a fear of dying from vaccination. People from his ethnicity who took the vaccine were forced to do so by the police (Kushner, Reference Kushner2022).
A social-psychological mechanism explains the above relational patterns between ethnic marginalization, “ethnicized trust,” and health policy (non-)compliance. According to the motivated reasoning theory, individuals often make a decision based on information that aligns with their predispositions, existing values, and social identities rather than seeking evidence (Kunda, Reference Kunda1990; Taber and Lodge, Reference Taber and Lodge2013; Dal and Tokdemir, Reference Dal and Tokdemir.2022; Wu et al., Reference Wu, Ozan Kuru, Çarkoglu, Cemalcilar and Yıldırım2024). Particularly in times of heightened uncertainty and lack of expertise, such as the global health crisis, individuals tend to rely more on the informational shortcuts and heuristics they acquire from social experiences and surroundings (Popkin, Reference Popkin1991; Dal and Tokdemir, Reference Dal and Tokdemir.2022). The perceived procedural fairness (Van den Bos et al., Reference Van den Bos, Lind, Wilke. and Cropanzano2001) or social and political cleavages, such as partisanship and ethnic cleavages (Dal and Tokdemir, Reference Dal and Tokdemir.2022; Wu et al., Reference Wu, Ozan Kuru, Çarkoglu, Cemalcilar and Yıldırım2024), play a role as a heuristic and influence individuals’ judgment and decision-making in health policy (non-) compliance. In this respect, during the global COVID-19 health crisis when acquiring accurate information was difficult, it was inevitable for individuals to rely on their marginalized ethnic identity and “ethnicized trust.”
Accordingly, while the aforementioned studies focus on health policy compliance (LaVeist et al., Reference LaVeist, Isaac and Williams.2009; Heymann et al., Reference Heymann2015; Mesch and Schwirian, Reference Mesch and Schwirian.2015; Blair et al., Reference Blair, Morse and Tsai.2017; Alsan and Wanamaker, Reference Alsan and Wanamaker.2018; Arriola and Grossman, Reference Arriola and Grossman.2021; Arthur et al., Reference Arthur, Horng, Tandanpolie, Gilstad, Tantum and Luby2023), citizens’ attitudes toward COVID-19 vaccination promoted by the governments is also a critical issue. Part of the hesitancy stems from politicians being at the forefront of the vaccination campaign instead of doctors (Kushner, Reference Kushner2022). For the marginalized Sahrawi, unfairness in the political system influences the perception of the state. Those who view the state to be acting in their favor are more likely to trust that the government will ensure vaccine safety than those who think otherwise. Therefore, raising awareness about vaccination in times of a health crisis might not resonate with the politically marginalized (Razai et al., Reference Razai, Osama, McKechnie and Majeed2021). This applies to minoritized groups’ response to health crises in general.
In sum, people who feel that their ethnic group is marginalized will be less willing to be vaccinated. An ethnicity tends to become salient during health crises times (Dionne and Turkmen, Reference Dionne and Turkmen.2020). Dionne and Turkmen (Reference Dionne and Turkmen.2020) examine a history of pandemics and find that marginalized groups of people based on national origins, ethnicity, and race experience increased discrimination. This further marginalization of minority groups was also a prevalent issue during the COVID-19 pandemic (Dionne and Turkmen, Reference Dionne and Turkmen.2020). This may even further the distrust that the marginalized groups have toward the dominant authority.
Indeed, existing studies also report common instances of vaccine hesitancy among racially and ethnically marginalized communities in other parts of the world (Andrade, Reference Andrade2021; Hildreth and Alcendor, Reference Hildreth and Alcendor.2021; Khubchandani and Macias, Reference Khubchandani and Macias.2021; Singh et al., Reference Singh, Lai, Wang, Asim, Chan, Wang and Yeoh2021; Woolf et al., Reference Woolf2021; Nguyen et al., Reference Nguyen2022). For instance, in the UK, vaccine hesitancy was high among Black (71.8%) and Pakistani/Bangladeshi (42.3%) ethnic groups because they did not trust the vaccine (Robertson et al., Reference Robertson, Reeve, Niedzwiedz, Moore, Blake, Green, Katikireddi and Benzeval2021; Hussain et al., Reference Hussain, Latif, Timmons, Nkhoma and Nellums2022). These concerns about vaccines emanate from previous interactions with the government and the heightened ethnic marginalization during pandemics. Marginalized ethnic groups will likely view government interventions as the means to advance agendas that will lead to their detriment. Hence, the following hypothesis:
Ethnic marginalization hypothesis (H1): Perceiving unfair treatment toward one’s ethnic group by the government influences vaccination intention.
This study goes further to disentangle the relationship between ethnic marginalization and vaccination intention. As discussed above, ethnic marginalization influences distrust in government policy implementation. Therefore, government trust mediates the relationship between sentiments of ethnic marginalization and vaccine hesitancy. Political trust is key in determining the relationship between perceived ethnic marginalization and vaccine hesitancy – it is a mediating factor. People who feel that the government unfairly treats their ethnic group will likely distrust the government. Among these people, willingness to be vaccinated is dependent upon their trust in the government’s ability to ensure vaccine safety for them. Hence, the following hypothesis:
Government Trust Mediation Hypothesis (H2): Political trust mediates the relationship between ethnic marginalization and vaccination intention.
Data, variables, and methods
Data
This study uses Afrobarometer Round 8 data. The Afrobarometer survey is nationally representative, with a minimum of 1,200 responses within each country. The Round 8 survey was conducted between 2019 and 2022 in 34 countries. Survey questions about the COVID-19 pandemic were included for 15 countries, and 14 countries include all relevant questions used in this study.Footnote 1
Dependent variable
The dependent variable is Vaccination Intention, measuring individuals’ vaccination intentions of the COVID-19 vaccines. It is measured by a survey question: “If a vaccine for COVID-19 becomes available and the government says it is safe, how likely are you to try to get vaccinated?” The answers are coded from one to four: 1 = very unlikely; 2 = somewhat unlikely; 3 = somewhat likely; and 4 = very likely. The higher values denote greater vaccination intentions. Among respondents, 47% have intentions to vaccinate. See variables’ distribution in the online Supplementary Materials (Figure A8 and Table A14).
Mediating variable
The mediating variable, Government Vaccine Trust, estimates the levels of trust in the government to ensure vaccine safety. The survey question asks: “How much do you trust the government to ensure that any vaccine for COVID-19 that is developed or offered to citizens is safe before it is used in this country?” The variable ranges from one to four: 1 = not at all; 2 = just a little; 3 = somewhat; and 4 = a lot. The higher values denote greater trust, and 16% of respondents have a high level of trust that the government will ensure the safety of the COVID-19 vaccine, and 20.5% trust the government “a little.” See viable distribution in the Supplementary Materials (Figure A10 and Table A14).
This study also conducts a robustness check to ensure that a different measurement of the mediating variable produces similar results. In a robustness check, a mediating variable is Government Legitimacy. This is an index combining four variables on political trust: Trust Ruling Party, Trust Legislature, Trust Executive, and Trust Local Government. Each variable ranges from zero to three: 0 = not at all; 1 = just a little; 2 = somewhat; and 3 = a lot. The higher the value, the greater the trust in each political institution. We created an index using a factor analysis (see Table A5 in the Supplementary Materials).
We also conduct another robustness check with a perception of corruption as a mediating variable. A high level of corruption not only erodes political trust but also exacerbates ethnic marginalization through an unequal allocation of resources. Perceived corruption is a perceived change in the level of corruption in one’s country in the past year, ranging from a decrease to an increase: 1 = decreased a lot; 2 = decreased somewhat; 3 = stayed the same; 4 = increased somewhat; 5 = increased a lot.
Independent variable
The independent variable is Unfair Treatment (Ethnicity). It measures how often an individual respondent’s ethnic group is unfairly treated by the government, with a survey question: “How often, if ever, are [respondent’s ethnic group] treated unfairly by the government?” It varies from zero to three: 0 = never; 1 = sometimes; 2 = often; and 3 = always. The higher values denote a greater perception of unfair treatment based on ethnicity, and only 10% percent of respondents say that their government treats them unfairly. See viable distribution in the Supplementary Materials (Figure A9 and Table A14).
A robustness check adopts a different measurement of the independent variable, that is a perception of unfair treatment based on ethnicity by other individuals. This variable addresses individual-level (rather than political) unfair treatment based on ethnicity. Unfair Treatment (Individual) estimates the frequency of encountering unfair treatment by other citizens based on ethnicity and ranges from zero to three: 0 = never; 1 = once or twice; 2 = several times; and 3 = many times.
Another robustness check uses ethnicity as an independent variable. We use the Ethnic Power Relations (EPR) data 2021 to determine the status of each ethnicity in each country. The EPR data codes levels of access to state power for each politically relevant ethnic group in every countryFootnote 2 . Each ethnic group is categorized based on a level of political power (please see the codebook for the definitions): monopoly, dominance, senior partner, junior partner, powerless, and discrimination. The Afrobarometer survey includes a variable indicating each respondent’s ethnicity. Using the information from EPR and Afrobarometer, we created an individual-level dichotomous variable: 1 = minority (discrimination, powerless, and junior partner) and 0 = majority (monopoly, dominance, and senior partner). See variable distribution in the Supplementary Materials (Figure A11 and Table A14).
Control variables
Control variables include various socio-economic status factors. Age is a continuous variable with a minimum of 18 years old. Education measures the levels of highest educational attainment and ranges from no formal education (0) to postgraduate education (9). Gender is a dichotomous variable: 0=female and 1=male. Residency is also a dichotomous variable: 0 = urban and 1 = rural. Employment status ranges from one to four: 0 = unemployed and not job searching; 1 = unemployed and job searching; 2 = employed part-time; and 3=employed full time. Individual Living Conditions range from very bad (1) to very good (5). Lastly, Social Media Exposure estimates a frequency of social media consumption as a news source and ranges from never (0) to every day (4).
Analytical methods
This study conducts a series of statistical analyses to assess the relationship between Vaccination intention, Unfair Treatment (Ethnicity), and Government Vaccine Trust. First, since the ethnic marginalization hypothesis (H1) expects a negative relationship between Vaccination intention and Unfair Treatment (Ethnicity), we first conduct ordered logistic regression analysis with the former as a dependent and the latter as an independent variable along with country-fixed effects. Before proceeding to causal mediation analyses, we also examine two additional ordered logistic regression models: (1) Government Vaccine Trust as a dependent variable and Unfair Treatment (Ethnicity) as an independent variable and (2) Vaccination intention as a dependent variable and both Unfair Treatment (Ethnicity) and Government Vaccine Trust as independent variables with country-fixed effects to determine the validity of H2. We also examine H1 and H2 using a structural equation modeling (SEM).
Then, we conduct causal mediation analyses (CMA) with Vaccination intention as a dependent variable, Government Vaccine Trust as a mediator variable, and Unfair Treatment (Ethnicity) as an independent variable. We use the STATA functions medeff and medsens to conduct CMA.Footnote 3 We also conduct a post-estimation analysis to test a violation of the sequential ignorability assumption using medsens. Please see Note 2 in the Supplementary Materials for more detailed explanations about the CMA model specification.
Lastly, we discuss the cross-country heterogeneity in degrees of ethnic marginalization that exists across African countries and zooms in on a country case of Morocco where a dominant ethnicity and marginalized ethnicity clearly exist. Please see the discussion section for a further discussion of cross-country heterogeneity and a case selection process. Using the Afrobarometer Round 8 with a subset of Morocco data, we conduct CMA with ethnicity as an independent variable, vaccination intention as a dependent variable, and government vaccine trust as a mediating variable. This analysis examines political trust and vaccination intention based on ethnicity rather than perceived ethnic marginalization.
Analysis and results
Ordered logistic regression and structural equation analysis
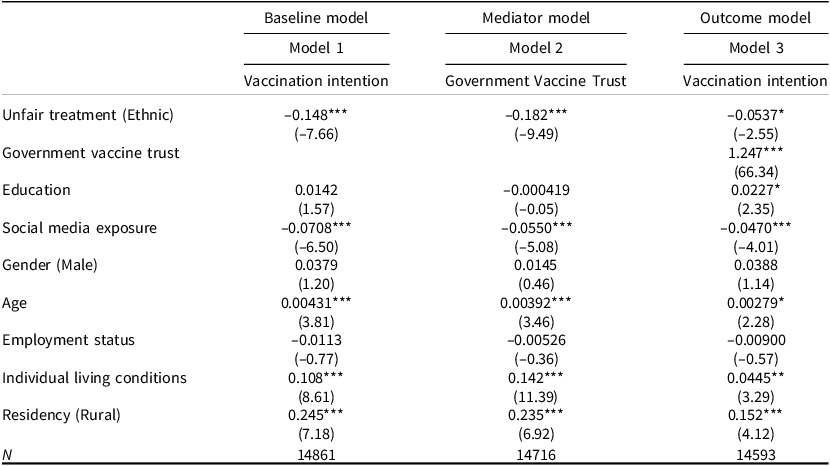
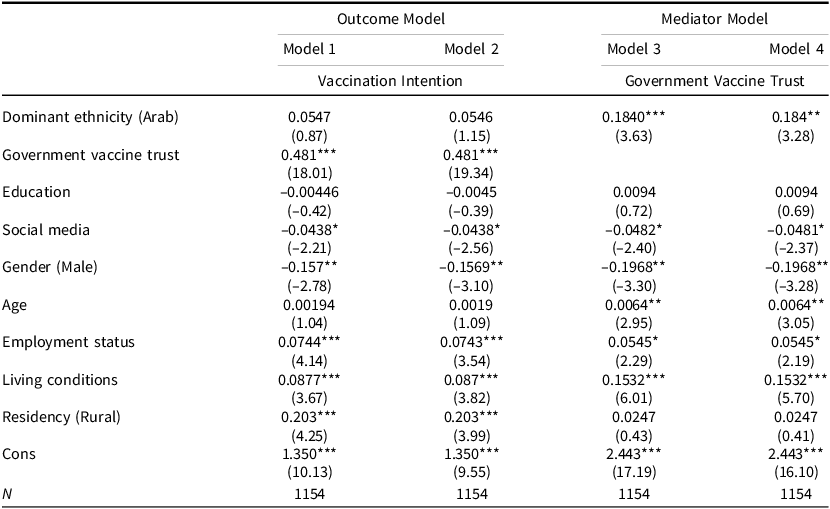
Before proceeding to CMA, we first conduct ordered logistic regression analysesFootnote 4 and structural equation analyses. Table 1 reports the ordered logistic estimation for two outcomes: Government Vaccine Trust and Vaccination Intention. Vaccination Intention is the main outcome variable, while Government Vaccine Trust is the mediator variable. The baseline model (Model 1), excluding the mediator variable (Government Vaccine Trust), tests the direct effect of the independent variable (Ethnic Unfair Treatment) on the outcome variable (Vaccine hesitancy) with individual-level control variables and country fixed-effects. The results indicate that Unfair Treatment (Ethnicity) has a negative and statistically significant influence on vaccination intention. This means that those who perceive that they are treated unfairly by their government based on their ethnic identity are less likely to get vaccinated, supporting H1.
Ethnic marginalization and vaccination intention (Ordered logistic Analysis)

Note: Coefficient with t statistics in Parentheses, *p < 0.05 **p < 0.01 ***p < 0.001, All models include country fixed effect.
The mediator model (Table 1 Model 2) tests the relationship between the independent and mediator variables; thus Government Vaccine Trust is the dependent variable. The findings show that Unfair Treatment has a negative and statistically significant influence on Government Vaccine Trust. Perceived unfair treatment by the government based on ethnicity reduces trust in the government to ensure the safety of COVID-19 vaccines. This suggests that Unfair Treatment (Ethnicity) affects both Government Vaccine Trust and vaccination intention. The outcome model (Model 3) tests the relationship between the independent and outcome variables, accounting for the mediator and control variables. Once Unfair Treatment (Ethnicity) and Government Vaccine Trust are introduced in the same model, Unfair Treatment (Ethnicity) loses its statistical significance. Hence, when the indirect effect is considered, the direct effect diminishes. The disappearance of the direct effect indicates the existence of a stronger magnitude and significance of the mediator variable and satisfies the general condition of a mediation effect, as Baron and Kenny (Reference Baron and Kenny1986) argue. Thus, the mediator variable (Government Vaccine Trust) exhibits a mediation effect and requires a CMA.
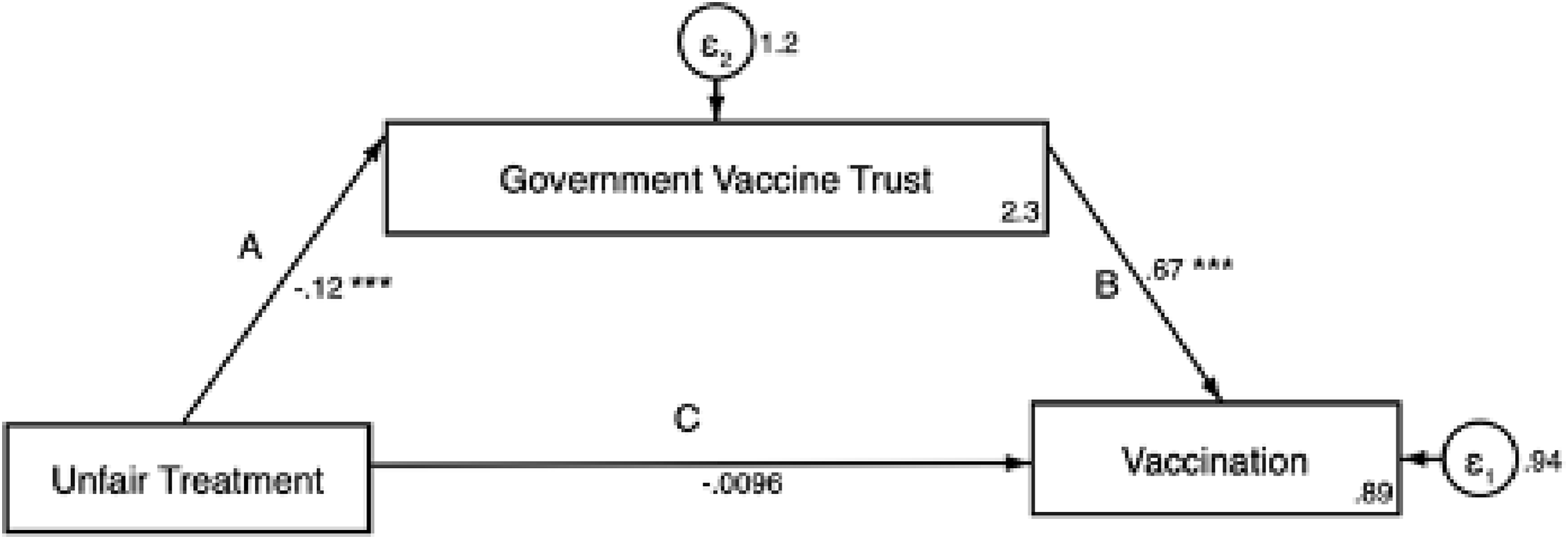
Figure 1 presents the relationship among the three key variables, using a structural equation modeling (SEM). The coefficients and levels of statistical significance (*) are indicated on the direction arrows. SEM also shows that the mediation is statistically significant. Both A and B are statistically significant. Path A shows that Unfair Treatment is negatively associated with Government Vaccine Trust, and Path B shows a positive relationship between Government Vaccine Trust and Vaccination intent. On the other hand, Path C shows that there is no direct relationship between Unfair Treatment and Vaccination intention when Government Vaccine Trust is accounted for. Therefore, the relationship between ethnic marginalization and vaccine hesitancy are fully mediated by trust in the government’s assurance of vaccine safety. Ethnic marginalization indirectly leads to vaccine hesitancy through the diminished trust.
Unfair treatment effect on vaccine hesitancy is mediated by Government Vaccine Trust (SEM Modeling).
Note: This figure is based on structural equation modeling (SEM) without covariates. Coefficients and levels of statistical significance on the direction arrows (*p < 0.05 **p < 0.01 ***p < 0.001). Constant and standard errors are also displayed.

Causal mediation analysis
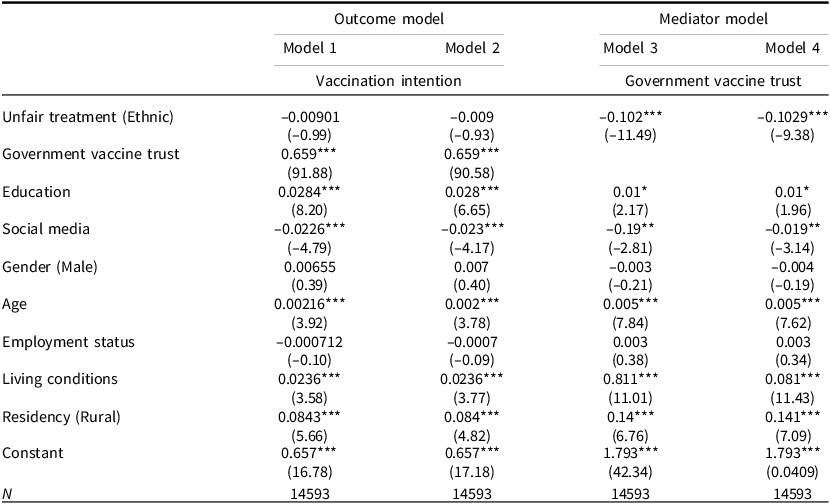
Based on the above-suggested role of the mediator, we expand our analysis to a causal mediation analysis (CMA) to confirm the mediation effect. Table 2 presents the result of CMA and supports H2. In Models 3 and 4 (mediator models), it shows that Unfair Treatment has a negative influence on Vaccination intention. In Models 1 and 2 (outcome models), Government Vaccine Trust has a positive influence on Vaccination intention, however the statistical significance of Unfair Treatment diminishes. The CMA results corroborate the results of the ordered logistic regression and SEM analyses. Government Vaccine Trust mediates the relationship between Unfair Treatment (Ethnicity) and Vaccination Intention. This suggests that ethnic marginalization affects a loss of trust in the government to ensure vaccine safety, and this loss of trust engenders vaccine hesitancy.
Ethnic marginalization and vaccination intention (CMA: medeff and medsens)

Note: Coefficient with t statistics in Parentheses, *p < 0.05 **p < 0.01 ***p < 0.001, All models include country fixed effects. Models 1 and 3 employ the medeff function to conduct a causal mediation analysis and Models 2 and 4 utilize the medsens function to conduct sensitivity analysis.
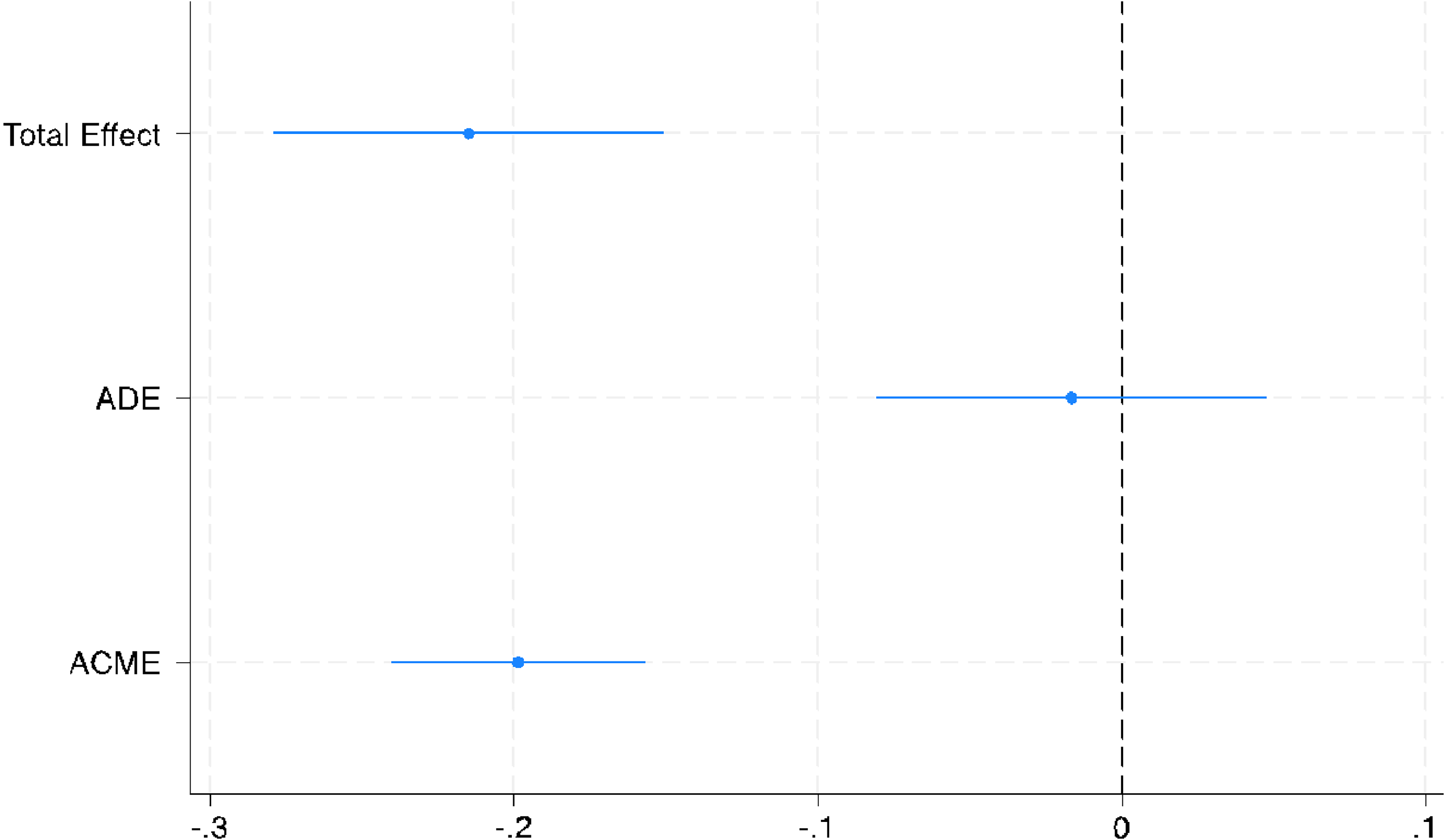
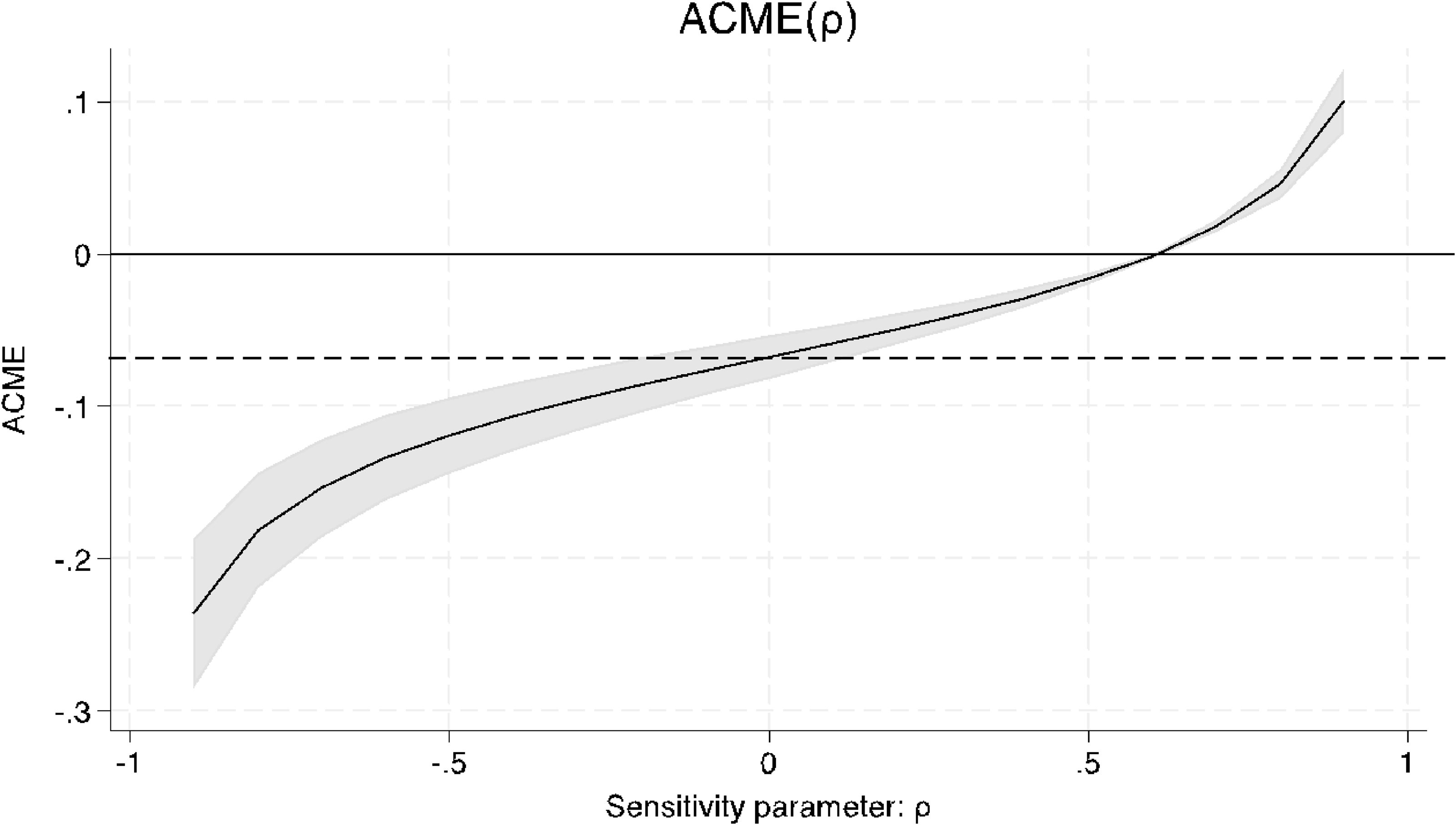
To check whether the estimated mediation effect is biased because of unobserved pre-test confounding factors between the mediator and the outcome variables, we estimate the average causal mediation effect (ACME). Table 3 and Figure 2 present the average causal mediation effect (ACME), average direct effect (ADE), and average total effect (ATE). Table 3 presents the total effect derived from the formula discussed in Note 2 in the Supplementary Materials. Namely, indirect effect (A * B) = −0.1984; direct effect (C) = −0.0164; and total effect (T) = A * B + C = −0.1984 + −0.0165 = −0.2149. The reduced (direct) model decomposition compares the estimated coefficient of Unfair Treatment and Vaccination Intention without including the Government Vaccine Trust, and the full (total) model includes Government Vaccine Trust. Therefore, the difference between the estimated coefficients of the main variables in the models is the indirect effect, which is part of the total effect running through Government Vaccine Trust (mediation effect). In Table 3 and Figure 2, the mediator, Government Vaccine Trust, has a statistically significant mediation effect. The causal mediation accounts for more than 51% of the total effect.
Effect decomposition plot for the mediator model.
Note: Average causal mediation effect (ACME), average direct effect (ADE), and average total effect (ATE). The point estimates are signified by the solid dot and line indicating 95% confidence limits of the influence of unfair treatment on vaccine hesitancy. The total effect is the average effect. The mediator is the Government Vaccine Trust.

Results of decomposition of causal mediation analysis

Note: The result shows the average causal mediation effect (ACME), average direct effect (ADE), and average total effect (ATE).
CMA assumes a sequential ignorability – no unmeasured confounders are related to the mediator and the outcome. This means that the likelihood of residual correlation between the mediator and the outcome variable is low. This is a sensitivity parameter
 $\rho$
(rho), the correlation between the residual of the mediator (Government Vaccine Trust) and the outcome variable (Vaccination Intention). A large value of
$\rho$
(rho), the correlation between the residual of the mediator (Government Vaccine Trust) and the outcome variable (Vaccination Intention). A large value of
 $\rho$
means that the model is less sensitive to unmeasured confounders. Figure 3 identifies that a
$\rho$
means that the model is less sensitive to unmeasured confounders. Figure 3 identifies that a
 $\rho$
value of 0.6 is required to determine that the mediation effect is zero (zero means a high sensitivity to unmeasured confounders). If the value is high when ACME equals zero, it indicates a less sensitivity to unmeasured pre-test confounders. That means the magnitude of unmeasured confounders needed to diminish the mediation effect of Government Vaccine Trust has to be high (Imai et al., Reference Imai, Keele, Tingley and Yamamoto2011). Thus, the
$\rho$
value of 0.6 is required to determine that the mediation effect is zero (zero means a high sensitivity to unmeasured confounders). If the value is high when ACME equals zero, it indicates a less sensitivity to unmeasured pre-test confounders. That means the magnitude of unmeasured confounders needed to diminish the mediation effect of Government Vaccine Trust has to be high (Imai et al., Reference Imai, Keele, Tingley and Yamamoto2011). Thus, the
 $\rho$
value of 0.6 means that the correlation between error terms must be 0.6 for the mediation effect to be absent. Although there is no standard value of
$\rho$
value of 0.6 means that the correlation between error terms must be 0.6 for the mediation effect to be absent. Although there is no standard value of
 $\rho$
that acts as a threshold, Imai et al. (2011) suggest that one strategy to interpret it is through cross-study comparisons. Existing studies find a mediation effect with a
$\rho$
that acts as a threshold, Imai et al. (2011) suggest that one strategy to interpret it is through cross-study comparisons. Existing studies find a mediation effect with a
 $\rho$
value equal to or below 0.6 (Flores et al., Reference Flores, Haider-Markel, Lewis, Miller, Tadlock and Taylor2018; Zeng and Li, Reference Zeng and Li.2019; Christensen et al., Reference Christensen, Leino, Setälä and Strandberg2022). Additionally, Keele et al. (Reference Keele, Tingley and Yamamoto.2015) argue that a
$\rho$
value equal to or below 0.6 (Flores et al., Reference Flores, Haider-Markel, Lewis, Miller, Tadlock and Taylor2018; Zeng and Li, Reference Zeng and Li.2019; Christensen et al., Reference Christensen, Leino, Setälä and Strandberg2022). Additionally, Keele et al. (Reference Keele, Tingley and Yamamoto.2015) argue that a
 $\rho$
value of 0.3 is a “modest” violation (953). Taken together, we interpret the current result in that the average causal mediation effect (ACME) is significantly different from zero, indicating a presence of a mediation effect.
$\rho$
value of 0.3 is a “modest” violation (953). Taken together, we interpret the current result in that the average causal mediation effect (ACME) is significantly different from zero, indicating a presence of a mediation effect.
Average causal mediation effect as a function of degree of violation of sequential ignorability assumption (Government Vaccine Trust as a Mediator).
Note: The sensitivity parameter is 0.6.

Robustness checks
Government legitimacy as a mediator
The Supplementary Materials report the results of robustness checks. Table A1 shows the results of CMA with Government Legitimacy as a mediating variable. As previously discussed, this measurement estimates a general level of trust in the government unrelated to the issue of vaccines. The result is consistent and supports H2 that the relationship between ethnic marginalization and vaccination intention is mediated by levels of trust in the government. The results of the mediator models (Models 3 and 4) are consistent with Table 2. In the outcome models (Models 1 and 2), Government Legitimacy is positive and statistically significant, corroborating the results from Table 2. The only difference is that Unfair Treatment has a statistical significance, indicating a partial mediation rather than a complete mediation.
Nonetheless, the mediation effect is statistically significant. Table A2 and Figure A1 show that the average causal mediation effect (ACME) is statistically significant. Since the direct effect of ethnic marginalization persists when a mediation is accounted for, this is a case of partial mediation. The result of the sensitivity analysis in Figure A2 also shows that the mediation effect exists, although the sensitivity parameter indicates that there are likely unmeasured confounders.
Corruption as a mediator
The next robustness check uses another measurement of the mediating variable: perceived government corruption. Table A3 shows the result of CMA with Corruption as a mediating variable and suggests that the relationship between ethnic marginalization and vaccination intention is partially mediated by perceived government corruption. Models 3 and 4 show that the unfair treatment by the government based on ethnicity is positively associated with a perception that the government is corrupt. Models 1 and 2 show that the perceived government corruption reduces the vaccination intention. Since Unfair Treatment remains statistically significant, the mediation is partial. Figures A3 and A4 corroborate the presence of the mediation effect.
Individual-level ethnic marginalization as an independent variable
We also conduct a robustness check with a different estimate of the independent variable. Table A4 and Figure A5 shows the CMA results with Treated Unfair (Individual) as an independent variable, measuring a perception of unfair treatment based on ethnicity by other individuals. The results are consistent that the relationship between interpersonal ethnic marginalization and vaccination intention is completely mediated by the Government Vaccine Trust. This suggests that an experience of discrimination based on ethnicity by other citizens also leads to distrust in the government, and this distrust results in a lower vaccination intention.
Models with sample weighting
We conduct a further robustness check by accounting for sample weightings. After conducting causal mediation analysis using ordered logistic and medeff analysis, we find that the results are consistent with the overall results. The negative influence of perceived marginalization on vaccination intent and the mediation effect of trust in government remain consistent (see Tables A8 and A9).
Models with a dichotomous dependent variable
We also dichotomize vaccination intent to test the strength of our findings. We code respondents who are very unlikely and those who are somewhat unlikely to take the vaccine as 0 and those who are somewhat likely and very likely to take the vaccine as one 1. The results remain consistent (see Table A10).
Ethnicity as an independent variable
We also introduce an objective measure of ethnic marginalization. Based on each respondent’s ethnicity, we created a dichotomous variable: minority ethnic groups (1) and majority ethnic group (0) (more explanation is provided in the independent variable section).Footnote 5 The results show that belonging to minoritized ethnic groups lead to a reduced willingness to get vaccinated and the mediating effect of trust in government remains consistent (See Tables A11 and A12 and Figures A6 and A7). Members of minoritized groups are less likely to trust the government, hence are less likely to get vaccinated, especially when they feel marginalized.
Switching the independent and mediator variables
Lastly, we reverse the independent and mediation variables to test for an endogeneity. We use trust in the government as the independent variable and unfair treatment as a mediating variable. Switching the independent and mediator variables shows that perceived ethnic marginalization does not have a mediating effect on trust in government because it does not diminish the positive statistically significant relationship between trust in government and vaccination intent. Instead, its relationship with vaccination intent is diminished by trust in government (see Table A13).
Discussion
The findings from the survey data in 14 African countries indicate that the relationship between ethnic marginalization and vaccine hesitancy is mediated by government trust. The finding is notable, especially given that the survey was conducted before the rollout of COVID-19 vaccines in 8 of the 14 countries surveyed. Please see Table A7 for the timing of the survey and vaccine rollout. This suggests that the relationship between ethnic marginalization, political trust, and vaccination intention existed prior to arrivals of particular vaccines.
As discussed previously, it is also important to note that there is a great cross-country heterogeneity in terms of ethnic relations across the 14 African countries examined. According to the EPR data, 10 of the 14 countries have some sort of power-sharing arrangement between senior and junior partners. Among the sample countries, only Morocco has a dominant ethnic group and at least one ethnic group explicitly discriminated against.Footnote 6 This heterogeneity in ethnic relations suggests that there are likely differences across countries in terms of the association between ethnic marginalization and vaccination intention, and so a further investigation is needed by disaggregating countries.
Accordingly, we further our investigation by narrowing our analyses to a single country, Morocco. Morocco provides a suitable case because the Amazighen are coded as powerless and Sahrawi are coded as discriminatedFootnote 7 , while Arabs are coded as dominant by the EPR data. In Morocco, the Arabs are the dominant ethnic group, and the Amazighen have had limited political influence since independence (Maddy-Weitzman, Reference Maddy-Weitzman2011). The Sahrawis have been marginalized under the Moroccan occupation (Dann, Reference Dann2014). Based on the theory, an expectation is that vaccination intention is lower among the Amazighen and the Sahrawis compared to the Arabs, because their marginalization has engendered distrust toward the government.
Table A6 in the Supplementary Materials provides support for H1 that marginalized ethnic communities are more vaccine hesitant. Model 1 examines the relationship between ethnicity and vaccination intention. The results show that the politically dominant Arabs tend to have a higher vaccination intention. This means that the marginalized Sahrawi and Amazighen are less likely to accept vaccination. However, Model 2 does not clarify whether the Sahrawi and the Amazighen are vaccine hesitant due to the marginalization they face from the government or due to some other reasons.
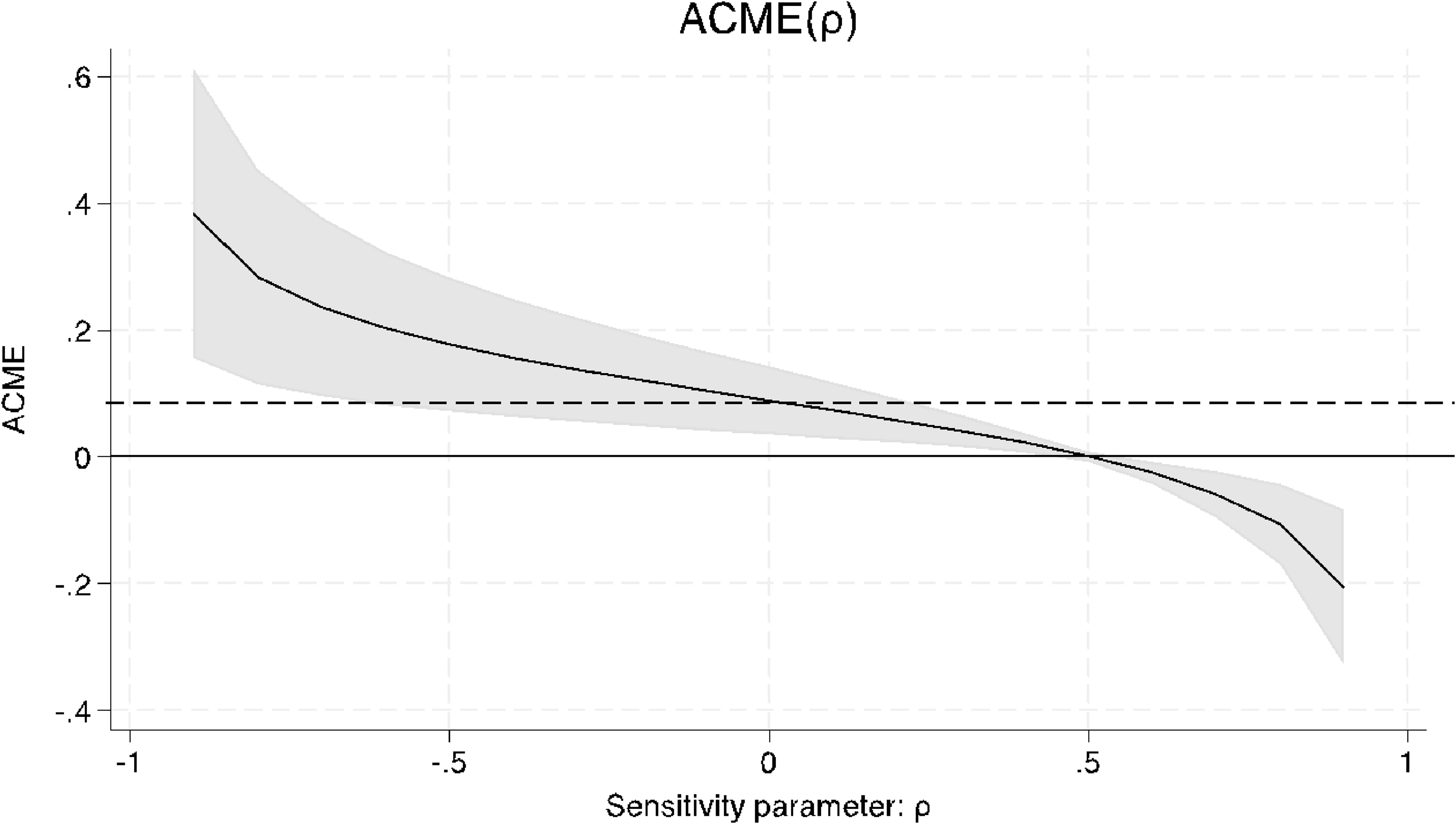
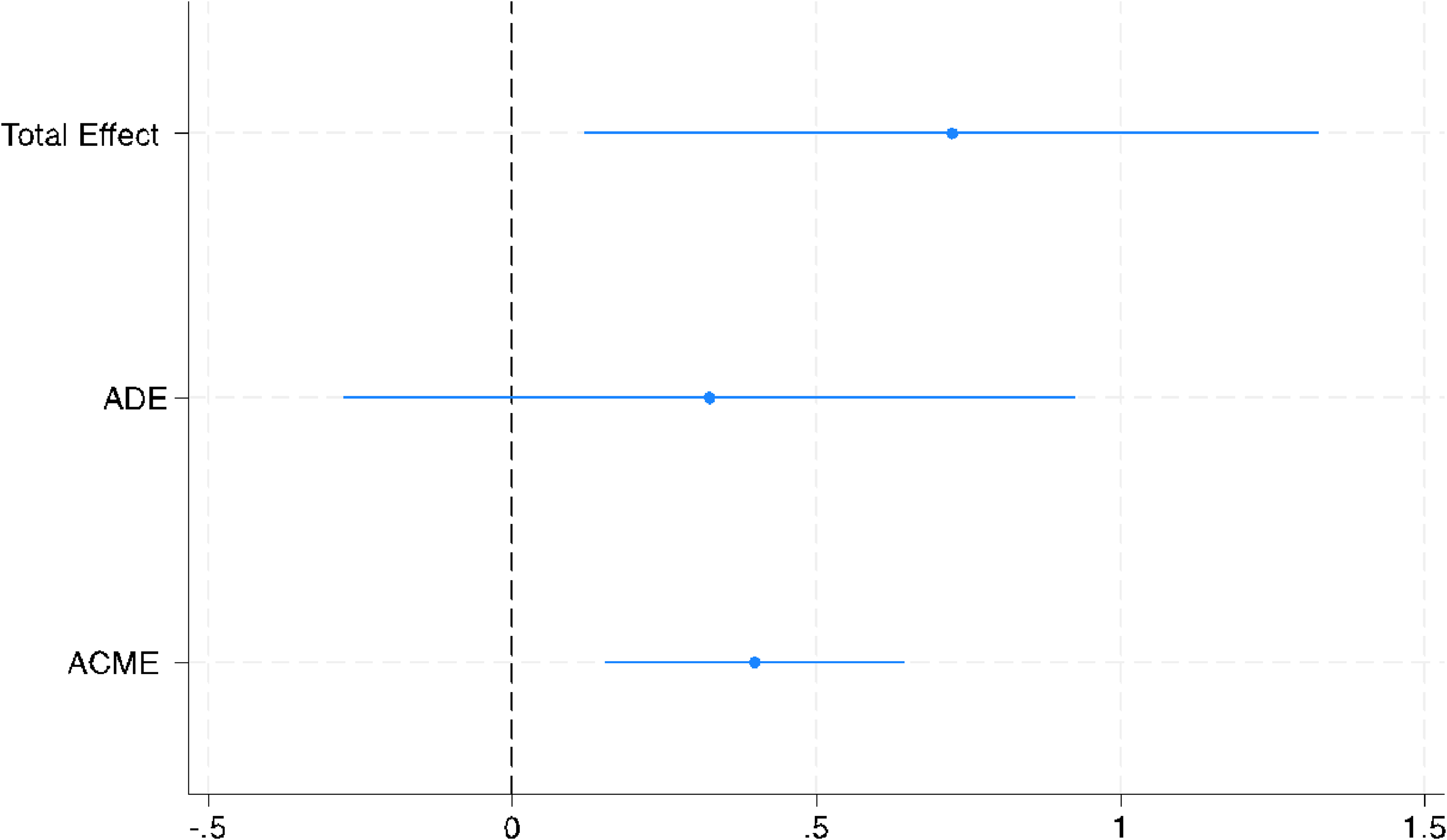
Thus, Table 4 conducts CMA and suggests that the relationship between ethnicity and vaccination intention is mediated by government vaccine trust. Models 1 and 2 show models with a vaccination intention as an outcome variable and find that the ethnicity loses its statistical significance when government vaccine trust is introduced as a mediator. This means that the Amazighen and Sahrawi have lower vaccination intentions, and their main reason is being mistreated by the government. Figures 4 and 5 corroborate the presence of the mediation effect.
Ethnic marginalization and vaccine hesitancy in Morocco (CMA: Medeff and Medsens)

Note: Coefficient with t statistics in Parentheses, *p < 0.05 **p < 0.01 ***p < 0.001. Models 1 and 3 employs the medeff function to conduct a causal mediation analysis and Models 2 and 4 utilize the medsen function to conduct sensitivity analysis.
Average causal mediation effect as a function of degree of violation of sequential ignorability assumption (Morocco).
Note: The mediator is Government Vaccine Trust and the independent variable is Ethnicity (Arab). The sensitivity parameter is 0.4963.

Effect decomposition plot for the mediator model (Morocco).
Note: Average causal mediation effect (ACME), average direct effect (ADE), and average total effect (ATE). The point estimates are signified by the solid dot and line indicating 95% confidence limits of the influence of ethnicity on vaccine hesitancy. The total effect is the average effect. The mediator is Government Vaccine Trust and the independent variable is Ethnicity (Arab) in Morocco.

The case analysis of Morocco also corroborates the earlier finding. This result suggests that it is not the ethnic identity per se that is driving the vaccine hesitancy, but rather, the vaccine hesitancy is attributed to the marginalization they experience as an ethnic group. Due to the government marginalization of their ethnic minority communities, they cannot trust the same government that treats them unfairly. This is consistent with our argument because we suggest that vaccine hesitancy among ethnic minority communities stems from their marginalization.
Conclusion
The results of the causal mediation analysis suggest that ethnically marginalized groups of people have lower vaccination intentions because the discrimination by the government erodes their political trust, so they also cannot trust the vaccines distributed by the same government. This study builds on previous studies’ findings regarding the link between ethnic minorities and health policy noncompliance, as well as the link between political trust and health policy non-compliance. The current contribution is to connect these dots and examine the relationship between ethnicity, political trust, and vaccination intention.
A caveat remains that the study does not control for all potential variables. It is especially important to note that levels of healthcare access were not accounted for in the current study. Those who experience barriers to healthcare access due to issues of costs, locations, and bureaucratic hurdles may be less likely to get vaccinated. At the same time, those who lack adequate healthcare access may distrust the government for its failure to ensure public service provisions. As such, future studies need to account for various aspects of healthcare access.
Another caveat exists in interpreting the outcome of our findings. Since our study utilized 14 African countries’ survey data, we cannot argue that the findings directly reflect a continent-wide pattern of the mediating relationship between ethnic marginalization and vaccination intention. However, the findings are relevant to broader contexts and offer a theoretical implication. Vaccine hesitancy among ethnic minority communities is reported in other regional contexts, such as North America and Europe (Nguyen et al., Reference Nguyen2022) to Asia (Singh et al., Reference Singh, Lai, Wang, Asim, Chan, Wang and Yeoh2021) and Latin America (Andrade, Reference Andrade2021). Recognizing the cross-country heterogeneity in ethnic relations and power sharing agreements, future studies can examine the same hypotheses in different country contexts with a history of ethnic marginalization but different institutional settings. Following the seminal work by Cohen (Reference Cohen1999), future studies can also examine an intersectionality of multiple layers of marginalization.
Additionally, while this study examines COVID-19 vaccines, it has broader implications for health crisis management policies in general. If the government wants citizens’ cooperation during crisis times, it needs to invest in policies during non-crisis times. These are policies that address the historical marginalization of certain communities. The institutions that maintain structural injustice need to be reformed. This requires sustained policy efforts far in advance of any potential crises. Public health is public goods, and public goods provision demands collective action. The state cannot expect collective action in crisis times if it does not guarantee impartial public goods provisions in non-crisis times. The greatest irony is that viruses do not discriminate, but humans do.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1755773926100344.
Data availability statement
Data is publicly available on the Afrobarometer’s website at https://www.afrobarometer.org/
Acknowledgment
The authors thank the valuable feedback we received at the invited talk at the Department of Statistics Speaker Series at Oklahoma State University. The authors are responsible for all errors.
Financial support
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests
The authors declare no conflicts of interest.
Ethical statement
This article does not contain any studies with human participants or animals performed by any of the authors.




 Open access
Open access