



Medieval hospitals, poverty and charity
The medieval poor included both an entrenched underclass and individuals experiencing poverty at specific points in their lives, perhaps as they became unable to work or their support networks failed (Rawcliffe Reference Rawcliffe1999: 9; Dyer Reference Dyer2010). Hospitals were one of the most common sources of help for the needy and, with 500 hospitals scattered across England, almost every town had one, as did many rural areas (Prescott Reference Prescott1992; Orme & Webster Reference Orme and Webster1995). Most were small charitable institutions that provided food and shelter for 10–20 residents who lived communally, ate at a common table and attended religious services. Hospitals were usually run by small groups of brethren and lay servants. Financially, hospitals were supported by donations of money or property, which provided rental income. Such donations afforded benefactors an opportunity to exercise Christian charity and ensure that the inmates prayed for their souls, speeding one's journey through purgatory (Rawcliffe Reference Rawcliffe1995: 14). Medieval charity was often as much about the spiritual benefit for donors as it was about helping the poor (Dyer Reference Dyer2010; Casson et al. Reference Casson, Casson, Lee and Phillips2020). Unlike modern hospitals, however, these institutions rarely provided medical care, and hospitals’ functions varied immensely. Some sheltered people with specific diseases, notably leprosy, while others housed travellers or poor pilgrims. Most had more vaguely defined roles, providing relief for the sick, poor and old (Rawcliffe Reference Rawcliffe2013). The specific role of each hospital was influenced by its local setting and the wealth and attitudes of its benefactors, and these roles could change over time (Rubin Reference Rubin1987).
Understanding how hospitals operated can offer a unique glimpse of both medieval poverty and charity, but investigating how specific hospitals operated is complicated (Orme & Webster Reference Orme and Webster1995). Most surviving archival material relates to the management of hospitals and, paradoxically, we know much more about their donors than about their residents. Hospital statutes occasionally give some clues—for example St John's Hospital, Oxford, prohibited the admittance of ‘epileptics’ (Dyer Reference Dyer1998)—but it is unclear how systematically such rules were applied. Demographic studies of residents, using both textual and archaeological sources, can reveal whether hospital managers followed the institutional rules for the admission of individuals of specific ages and/or sexes, for example, admitting infants at St Mary Spital, London (Thomas et al. Reference Thomas, Sloane and Phillpotts1997) or children at St Bartholomew's Hospital, Bristol (Price & Ponsford Reference Price and Ponsford1998). Palaeopathological studies also can also reveal the medical conditions that the hospitals’ residents suffered from, for example, leprosy at St Margaret's, High Wycombe (Farley & Manchester Reference Farley and Manchester1989) or more general complaints, as at St Giles by Brompton Bridge, North Yorkshire (Cardwell et al. Reference Cardwell1995). Such studies complement documentary records, yet hospital patients “remain an often intangible presence” (Rawcliffe Reference Rawcliffe1999: 162).
In this article, we examine the biographies of individuals who lived and died in a medieval hospital in Cambridge, England. An osteobiographical approach involves treating the skeleton not as a source of fragmented data but as a layered record of a complex, coherent life narrative. We assemble multiple types of skeletal and molecular data for each individual and arrange these sequentially within their lifespans, integrating as much historical context as possible and seeking connections between all this information. Moreover, while osteobiography usually works with single skeletons, here we attempt a collective osteobiography, examining the extent of the similarities and differences between individual life courses within the community of a medieval hospital. This approach allows us to address major questions about medieval hospitals and charity in new ways. Here we ask: what life paths led individuals to the hospital? How did time in the hospital form part of an individual's overall life course? And what does this tell us about the operation of this important and widespread medieval institution?
The Hospital of St John the Evangelist, Cambridge
By AD 1200, Cambridge was a town of 2000–3000 residents (Figure 1). Linked by river to the North Sea and lying along the main route by land from London to Norwich, it was the economic centre of a prosperous agricultural landscape. The town reached its peak medieval population just before the Black Death (1348–49) at approximately 5000 townspeople, supplemented by 500–1000 university scholars and religious professionals living in monasteries, friaries and convents (Cam Reference Cam and Roach1959; Casson et al. Reference Casson, Casson, Lee and Phillips2020: 70).
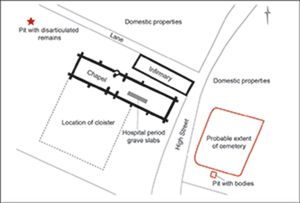
Location of The Hospital of St John the Evangelist and other sites studied (map by V. Herring).

The Hospital of St John the Evangelist was founded c. 1195 (Rubin Reference Rubin1987). For most of its history, it consisted of a dormitory building in which the inmates lived, a chapel and service outbuildings (Rubin Reference Rubin1987; Orme & Webster Reference Orme and Webster1995). Run on quasi-monastic lines, it housed probably a dozen or so inmates, a staff of 4–6 clerics and some lay servants. The hospital was a moderately wealthy institution that owned property, collected rents and may have lent money (Orme & Webster Reference Orme and Webster1995; Dyer Reference Dyer1998: 70–71). During the fifteenth century, the hospital's fortunes declined and it was eventually dissolved to create St John's College in 1511 (Cessford Reference Cessford2015). Inmates, and occasionally townsfolk, were buried in the hospital's cemetery, while clerical staff and wealthy benefactors were buried in and around the hospital's chapel (Rubin Reference Rubin1987; Faber Reference Faber2006; Cessford Reference Cessford2015; Robb et al. Reference Robb, Inskip, Cessford, Dittmar, Kivisild, Mitchell, Mulder, O'Connell, Price, Rose and Scheib2019). Excavations in 2010–11 by the Cambridge Archaeological Unit recovered almost 400 complete and partial skeletons from the hospital cemetery (Cessford Reference Cessford2015). The burials largely comprise extended supine inhumations, orientated west–east, in simple earth-cut graves, shrouded and without grave goods (Figure 2).
Reconstructed plan of the Hospital of St John the Evangelist. Left: general layout. Right: detail of excavated area of cemetery (plans by V. Herring after Cessford et al. Reference Cessford2015: figs 1 & 7).

Like all medieval towns, Cambridge must have been a sea of need. Poverty was common in medieval towns (Dyer Reference Dyer1998); for example, approximately 20 per cent of the population of sixteenth-century Norwich lived below the poverty line (Rawcliffe Reference Rawcliffe1999: 9). There is no reason to suppose that poverty was less rife a few centuries earlier or that the population of Cambridge was any better off. There must have been scores of people in need of charity at any time. The Hospital of St John the Evangelist could accommodate perhaps 10–20 long-term inmates at a time, providing them with room, board and clothing for life (Rubin Reference Rubin1987). With such generous support, the hospital's residents must have formed a small ‘elite’ among the needy of Cambridge; but with limited capacity, how did the hospital's managers choose whom to take in?
The hospital's charter or mission statement established the main criteria. The hospital was initially established for the “poor and infirm” and for the “maintenance of poor scholars and other sick people”. Its charter explicitly excluded pregnant women, lepers, the wounded, the severely disabled and the insane (Rubin Reference Rubin1987: 171–3). The inmates also included some corrodians, that is, people who donated their property to the hospital in return for food, clothing and housing for the rest of their lives (Underwood Reference Underwood2008: xviii). A second criterion was piety. Most benefactors stated frankly that their donations were made to benefit their souls and those of their relatives (Underwood Reference Underwood2008). Thus, the residents admitted must have been expected to be of good reputation, humble, grateful and at least conventionally pious. These criteria leave much latitude, however, and policies can be applied in many ways. We therefore turn to the archaeological evidence to assess how individuals might have ended up living—and ultimately dying—in this institution. Did the Hospital of St John the Evangelist support the poor, decrepit or seriously ill? Did it prefer university scholars or townspeople? How were these individuals selected to receive this charity?
Bioarchaeology and biographical approaches: materials and methods
Collective biography, sometimes called prosopography, is the study of whether members of a group had similar or interacting life experiences. Though it has been pursued experimentally in historical research (e.g. life on a Victorian street in Oxford, Erben Reference Erben1996), collective biographical approaches based on the integration of multiple strands of archaeological data to reconstruct life histories are relatively recent (Novak Reference Novak2017; Robb Reference Robb2019; see also Fiorato et al. Reference Fiorato, Boylston and Knüsel2000; Stirland Reference Stirland2000; Novak Reference Novak2008; Geber Reference Geber2015). Here, we combine skeletal and molecular evidence to reconstruct individual life experiences and to consider these life stories in the context of groups within the wider community.
The data analysed include burial treatment, age at death, stature, sex, palaeopathological conditions, markings of muscle attachments and activity-related skeletal changes, an Index of Poor Childhood Environment (IPCE), humeral functional anatomy, diet-related isotopes (dentine and rib carbon and nitrogen), mobility-related isotopes (enamel strontium) and human and pathogen ancient DNA (aDNA). In total, 30–50 bioarchaeological and molecular observations were collected from each of 337 adults and 69 non-adults from the Hospital of St John the Evangelist, Cambridge (see online supplementary material (OSM) for methodology). Although this article focuses specifically on the hospital's community, the analysis is informed by a comparison with data for 121 contemporaneous townspeople from Cambridge (from the All Saints by the Castle parochial church cemetery, founded c. AD 940–100 and closed by 1365) and 18 religious professionals (friars from the Augustinian Friary founded in AD 1279/1280–89 and closed in 1538; Dittmar et al. in press). The result is one of the richest osteobiographical datasets for medieval England, in terms both of the quantity of data and of the detail of the individual lives documented.
In assembling the data, it quickly became clear that those buried in the hospital differed from both the townspeople and the friars in several respects. For example, the hospital community was more diverse than the other groups, suggesting that the hospital housed a particularly heterogeneous population. The investigation of this evidence therefore required a complex analytical strategy. While it was clear that the hospital sample contained groups of similar skeletons, much as with social groups in a modern population, they were likely to be fuzzily rather than clearly bounded and distinguished in each case by a different set of specific features whose significance depended on context. We therefore approached the data in a series of iterative stages, exploring variability in particular subgroups to isolate their distinctive characteristics. This process generated a series of recurrent clusters of similar individuals, forming groups with fuzzy rather than clear-cut boundaries, which we discuss in turn below (see OSM for more on methods and data).
The fortunate unfortunates: who ended up in the hospital?
Medieval Cambridge was a complex social landscape. Ancient DNA analysis demonstrates that, genetically, the hospital's population was indistinguishable from other people living in Cambridge at the time. However, unlike in the parish cemeteries, no kinship links have been found among the hospital inmates (Hui et al. Reference Hui, Scheib, D'Atanasio, Inskip, Cessford, Biagini, Robb and Kivisild2023), which suggests that they were admitted according to individual need, not place of residence or family ties. Moreover, unlike in parish cemeteries, young children under seven (‘infants’ in medieval terminology) are absent from the hospital cemetery and only 16 per cent of the burials are of individuals aged 7–16 years old at death; the vast majority are adults.
Ancient DNA techniques can be used to determine sex, including that of non-adults; its application here leads to a sex profile for the hospital population that differs from that presented in previous publications (see Dodwell Reference Dodwell2015). Of the 154 adults and 22 non-adults for whom sex could be determined, about 60 per cent are male and 40 per cent female (see also Inskip et al. Reference Inskip, Scheib, Wohns, Ge, Kivisild and Robb2019), with no sex difference in age-at-death profiles. As clerics and scholars were exclusively male, the presence of numerous women confirms that the hospital served the town's wider population.
Comparing the hospital residents with townspeople and friars shows that, on average, male and female hospital residents were approximately 20mm shorter than townsmen/women. Compared to the friars and townspeople, a greater proportion of the hospital's residents died as young adults (Table S3); related to this, the hospital's population also show lower rates of trauma and age-related conditions compared to the other two groups. The residents of the hospital do, however, demonstrate a higher average Index of Poor Childhood Environment (see OSM Table S2) and more of them suffered from skeletally visible tuberculosis than is the case for the other groups. Hence, the health inequalities of medieval Cambridge are not only reflected in the hospital's population, but these individuals also show greater variation in terms of many bioarchaeological variables compared to other groups, encompassing in one community the entire range of variability known in medieval Cambridge. This suggests that its population was heterogeneous, mixing different social groups in one institution. Below, we explore this heterogeneity by discussing the collective osteobiographies of some of these groups.
People like everybody else
We began our analysis simply by comparing individuals from the hospital with contemporary samples from other sites in medieval Cambridge to see whether any distinguishing features of health, nutrition or activity give clues to why they were buried at the hospital. About half the adults in the hospital sample are skeletally similar to the townsfolk and friars (the older male described in Robb et al. Reference Robb, Inskip, Cessford, Dittmar, Kivisild, Mitchell, Mulder, O'Connell, Price, Rose and Scheib2019 (PSN356/Burial958) is an example of one such hospital person). Skeletal data are coarse-grained proxies and some may have been poor, ill or needy, without displaying skeletal indicators of it. However, there are at least four other possibilities. A few may be corrodians. Some may not be hospital residents but townspeople who requested burial there (Robert Curteis is one historically documented example, Robb et al. Reference Robb, Inskip, Cessford, Dittmar, Kivisild, Mitchell, Mulder, O'Connell, Price, Rose and Scheib2019). Some may be hospital lay servants. However, most may have been ordinary townspeople for most of their lives before being driven to need. In this ‘life cycle poverty’ (Dyer Reference Dyer2010), they may have encountered illness or some other circumstance preventing them from working, combined with isolation or the death of a spouse, parents or working child which meant they lacked the family as a safety net. Their need may not necessarily have been severe or long lasting. Their backstories, and skeletons, would be essentially the same as other townspeople.
The ‘shame-faced’ poor
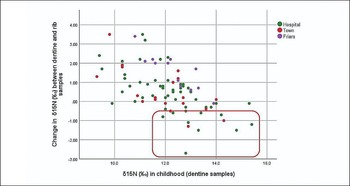
By and large, most people in the St John's Hospital's nutrition late in life (as reflected in their rib carbon and nitrogen isotope values) either resembled their childhood nutrition (as shown in their dentine isotope values) or suggest an improvement in nutrition over their lifetime (Rose Reference Rose2020). For example, the carbon and nitrogen values of St John's Hospital inmates frequently increase between childhood and the last decades of life, probably reflecting the effect of the institutional diet with regular provision of meat, fish and dairy compared with childhood foods. Despite this general trend, however, at least five and possibly up to eight individuals from the hospital show an unusual combination of factors (see Figure 3): their (childhood) dentine nitrogen isotope values are above the median for the hospital population, they lived to middle age or older, and by the last decade of life their nitrogen isotope values are at least 0.5‰ lower than their childhood value. As a group, these individuals are skeletally unremarkable; they are of mixed stature, with no indicators of particularly poor childhoods, and no signs of any unusual physical activity or health (Table S9). The unusual decrease in isotope values in later life suggests a shift in diet. For example, PSN92/Burial 363 is an older male (60+ years) of short stature and robust build who had survived the Black Death before dying in the later fourteenth century with an active metastatic tumour; nitrogen and carbon isotope values from late in the life of this individual (rib samples) are substantially lower than their childhood (dentine) values.
Dentine collagen δ15N (‰, horizontal axis) against ‰ change in δ15N between dentine collagen and rib collagen (vertical axis). Red box highlights individuals with a rib δ15N value substantially lower than their dentine value, indicating a decrease in dietary quality towards the end of their lives (figure by the authors).

These individuals may have had a poorer diet later in life compared with that eaten during their childhoods. Isotopic values reflect multiple factors, and we do not know exactly when during their lives these nutritional changes occurred. Intriguingly, these individuals may illustrate a particular aspect of late medieval doctrine about charity. The pauperes verecundi were “the shame-faced poor, people who had fallen from comfort to poverty” and who were therefore “seen as a case especially deserving, when many other poor folk were being chastised as wilful and undeserving” (Rubin Reference Rubin1987: 72–3). The existence of the ‘deserving poor’ threatened the moral order, suggesting that it was possible to live virtuously and prosperously but still fall victim to fortune. The sampled individuals, all middle aged or older, who show a reduction in their nitrogen and carbon isotope values towards the ends of their lives might reflect a concentration of such people at the hospital and this may suggest that, conforming to theological recommendations, the hospital particularly extended its charity to (older) individuals who had fallen from comfort to want. Presumably the ones we can identify in this way were not resident for long enough to benefit from the hospital's institutional diet.
Poor, young and ill
Compared to contemporary townspeople, the adults buried at the hospital demonstrate disproportionate numbers of individuals dying as young adults, individuals with high values on the Index of Poor Childhood Environment (Table S2), and individuals with skeletal tuberculosis dying between 18 and 25 years of age (Table S5). A group of 10–12 individuals with these characteristics frequently plot together on scatterplots and in cluster analyses (Table S6). Between two-thirds and three-quarters of this group are female. PSN90/Burial 360, for instance, was a 1.5m-tall woman with robust humeri, suggesting habitual hard work, who died before her mid-20s with active tuberculosis in her spine and pelvis.
Among the hospital's population, therefore, was a group of young adults who were poor, had experienced difficult childhoods, and who were often chronically ill (Table S8). The hospital may have cared for such individuals as children, supporting them into early adulthood. The cemetery contained a number of children over six years of age, which suggests that they were accepted into the hospital (younger children may have been considered too disruptive, as at St Giles Hospital in Norwich; Rawcliffe Reference Rawcliffe1999). About two-thirds of non-adults buried at the hospital are male; these may also include some young, ill scholars as well as townspeople. The females were most probably townspeople, especially as institutions such as the hospital were unlikely to employ young, unmarried women as lay servants (Rawcliffe Reference Rawcliffe2013). Nearly all of these individals display cribra orbitalia (pathological new bone formation in the orbits) and new periosteal bone (reflecting trauma, infectious disease or other illness) somewhere on the skeleton; about one-third have rib lesions suggesting chronic respiratory diseases and many have other skeletal indicators of tuberculosis. As sick children would normally be cared for by their parents, many of the sub-adults at the hospital may have been orphans who were unable to work (cf. Thomas et al. Reference Thomas, Sloane and Phillpotts1997). The ‘young, poor, and ill’ adults were probably those same children who survived to the threshold of adulthood or who were taken in at a slightly older age.
This group of young individuals of poor health illustrates the sharpest edge of poverty. Many, perhaps most, people in medieval English towns belonged to the working poor, doing strenuous and sometimes dangerous work and living at the margin of economic viability. They may have subsisted entirely on the cheapest foods, and any illness, injury, loss of work or price increase could lead to hunger (Dyer Reference Dyer1998). But below the working poor, there seems to have been another stratum: the ‘structurally poor’ (Dyer Reference Dyer2010), who, working or not, suffered want as a normal daily condition. Some of the hospital residents may have been selected from among this stratum, prioritising young people who could not work and who had no family safety net. Many died young. But at least some appear to have survived long enough in the hospital for the carbon and nitrogen isotope values of their ribs to register the improved diet they enjoyed there (Rose Reference Rose2020)—evidence of charity making a difference.
The lifelong poor
For all age groups, the cemetery of the Hospital of St John contained a greater number of individuals with indicators of a poor childhood than other sites (Table S7). In addition to the inheritance of their early years—low dentine carbon and nitrogen isotope values, reduced adult stature, enamel hypoplasia and cribra orbitalia—these individuals often show signs of intense physical labour. For example, PSN331/Burial 900, a short (1.51±0.37m) 46- to 59-year-old woman, displays the strongest humeral diaphyseal rigidity of any individual in the sample. This individual may have laboured, lifting and carrying until something, possibly a painful foot infection, prevented her from working. The presence of this individual in the cemetery hints at the hospital's admissions policy. Among the hospital residents who have indicators of poor childhoods and who died at advanced ages, there are at least twice as many women as men. The population of medieval Cambridge comprised slightly more older women than older men; given that those who died young in the hospital are disproportionately female, this may reflect a belief that women were weaker, more in need of charitable aid, or (perhaps accurately) more vulnerable to poverty. More generally, this group of the ‘lifelong poor’ from the hospital includes many of the shortest individuals buried in the various Cambridge cemeteries. Indeed, for the period when the hospital was in operation, the hospital cemetery contains 15 of the 25 shortest females in our skeletal samples, and 16 of the 20 shortest males.
University scholars
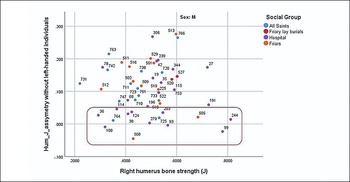
Across the wider population sample of medieval Cambridge, women typically have symmetrical humeri, while men have right-dominant asymmetry (with an index of asymmetry over 5%), probably reflecting their work regimes (Mulder Reference Mulder2020; Figure 4). At the Hospital of St John, by contrast, 11 of the 27 males from whom laser scans of the humeri have been taken (see OSM) show highly symmetrical humeri, often also quite gracile humeri (Figure 5). (A)symmetry of bone architecture forms predominantly in late adolescence/early adulthood in response to activity regimes (Pearson & Lieberman Reference Pearson and Lieberman2004). Thus, the hospital contained a relatively discrete group of males who did not conform to a typical male work pattern at this point in their lives. These individuals date predominantly to the later fourteenth and fifteenth centuries. Similar patterns of upper-arm symmetry during this period are observed in two Augustinian friars and two individuals from All Saints by the Castle (Table S10). For the friars at least, it may perhaps be for similar occupational reasons.
Humeral strength (J) asymmetry (excluding left-dominant people, presumably left-handed); vertical axis is index of asymmetry. Note male-female difference among townspeople (All Saints) and low median for hospital males compared with male townspeople and friars (figure by the authors).

Right humerus bone strength (J) (horizontal axis) against humerus J asymmetry (vertical axis) in adult males. Box highlights individuals with symmetrical humeri (figure by the authors).

It is unlikely that these individuals were chronically ill and unable to work as young adults; they have few indicators of a poor childhood environment, their adult health is unremarkable, and most lived to at least 35 years of age. Their skeletally attested illnesses tend to be ailments of age (such as osteoarthritis), and most trauma is confined to fractures of the ribs or vertebrae. Unlike the friars, the hospital residents with high humeral symmetry have few or no Schmorl's nodes (affecting the discs of the vertebrae) and they lack signs of specialised labour such as idiosyncratically developed entheses, unusual eburnation (a symptom of osteoarthritic change), or activity-related non-metric traits. Their rib carbon and nitrogen isotopic values are almost all above the population median.
These men probably did not undertake heavy labour or a specialised manual work during early adulthood; they lived in reasonable health with above-average nutrition, normally surviving to middle age or older. Since these individuals are found at the hospital in some numbers, whereas very few have been recorded at other sites, it seems likely that they were university scholars. Supporting ‘poor scholars’ was one of the hospital's statutory charitable missions (Rubin Reference Rubin1987; Underwood Reference Underwood2008). University-based clerics did not have the same novice-to-grave institutional support as clergy in religious orders. Scholars would have supported themselves, through teaching, family support and charitable patronage, particularly if they lived and worked in hostels and halls (which were financed by their members’ contributions) rather than colleges (which had endowed financial support). Much like others outliving their capacity to work, when they encountered old age or infirmity, poor scholars would have risked indigence; even college-based scholars could lose their places due to ill-health (Cobban Reference Cobban1999: 77–8). As the University grew rapidly in the fourteenth and fifteenth centuries, the admission of poor scholars into the hospital is likely to have increased.
Identifying this burial cohort as scholars not only fills in a missing but textually attested group, it also adds new information—particularly on their backgrounds. Geographically, most students of the University would have come from eastern England, with many from the north (the dioceses of Lincoln and York). Most students from southern or western Britain attended Oxford, and few from Scotland, Ireland or continental Europe came to Cambridge (Aston et al. Reference Aston, Duncan and Evans1980). In our sample, three of the four probable scholars sampled display strontium isotope ratios consistent with growing up in East Anglia. The exception (PSN99/Burial 372, aged 26–35 years at death) has a strontium isotope ratio consistent with areas in south-western and northern England, Wales, Scotland or overseas. Given the University's known catchment for students, it is likely that this individual was from northern England; the closest relevant area would be between Nottingham and Doncaster. Regardless of the scholars’ origins, their childhood environments are typically not among the poorest attested in the hospital cemetery; for example, their IPCE scores are more similar to the wider Cambridge population than the ‘poor’ individuals from the hospital discussed above. Even if being a career student may have ultimately streamed them into a charitable institution, academia was not a pursuit for the poor.
Waifs and strays: people dying out of place
Strontium isotope sampling of 123 individuals from medieval Cambridge encompassing the three population groups of the Hospital of St John the Evangelist, the townspeople and the friars reveals at least three individuals who must have come from outside East Anglia (Rose Reference Rose2020). All three were buried at the hospital. One is the probable scholar discussed above. The other two are PSN332/Burial 901, a young female (18–25 years) with strontium isotope values suggestive of a childhood in south-western or north-western England, Wales, Scotland, Norway, Brittany, central France or further afield, and genetic affinities with Dutch and Scandinavian populations (Hui et al. Reference Hui, Scheib, D'Atanasio, Inskip, Cessford, Biagini, Robb and Kivisild2023); and PSN66/Burial 276, a young male (18–25 years) whose strontium isotope values indicate that he either came from overseas or from western Wales, Cumbria and the Scottish highlands where such values are found in small, thinly populated areas.
It is probable that these two individuals were short-term visitors; in the late medieval period, most historically documented long-term migrants to East Anglia came from regions such as Flanders, where the underlying geology is similar to Cambridge and therefore not distinguishable through strontium isotopes. Given the difficulty of east-west land travel within Britain during the medieval period, the individuals with non-local strontium isotope ratios probably came from around the North Sea or from northern France via maritime routes. North Sea trade routes linked the Baltic, Norway, Scotland and East Anglia. Indeed, via the rivers Ouse and Cam, Cambridge was the furthest inland node on this North Sea network, and it hosted the Stourbridge Fair, one of the largest annual trade fairs in England (Miller & Hatcher Reference Miller and Hatcher1995). Our two individuals may have come to Cambridge to trade or for other purposes but died there. Thus, they may never have lived in the hospital, but were simply buried there. Travellers often worried about how they would receive proper Christian burial if they died far from home, as they belonged neither to a parish nor to another institution providing burial for its members (M. Rubin, pers. comm.). Hospital cemeteries were consecrated ground and, given the Hospital of St John's charitable mission, providing Christian burial for such outsiders would have been an important, final act of charity.
Choosing residents and the institutional logic of a medieval charity
Need is not monolithic. Medieval poverty involved both the structurally poor, who suffered from lifelong severe deprivation, and those who experienced poverty as a result of specific adverse circumstances and events (Dyer Reference Dyer2010). The biographical analysis of individuals buried at the Hospital of St John the Evangelist in Cambridge suggests the presence of both the lifelong poor and people driven to need by particular life events. The hospital also looked after university scholars and those defined as deserving of charity for other reasons, in life or in death.
Charity is part of a moral economy, and poverty and need are framed within particular discourses. A major finding of this study is that the Hospital of St John's cemetery did not simply accumulate individuals as they died, like a municipal cemetery. It is a constructed population: everybody buried there is included by an act of institutional categorisation and selection. This burial population sheds light on the hospital's decision-making processes about who to admit, particularly as the formal rules of its charter left considerable freedom in these choices. One possible criterion was simply material need, providing for the homeless and hungry. But while a modern utilitarian view might prioritise using hospital resources to help the very poorest in society, another medieval criterion was spiritual merit, which was defined theologically. Besides perennial anxiety about separating genuine poor people from the undeserving or ‘lazy’ poor, hospitals may have become more selective after the Black Death, prioritising theological categories or specific groups (Rawcliffe Reference Rawcliffe1995; Dyer Reference Dyer2010). A third possible criterion was micro-politics. St Giles (Norwich) accepted property from a donor in return for agreeing to exclude people with certain illnesses, a clear example of policy being shaped by a donor's demands (Rawcliffe Reference Rawcliffe1995: 104). The Hospital of St John may have existed in a similar system of local relationships and favours, making it possible for clients and friends to obtain access to charity.
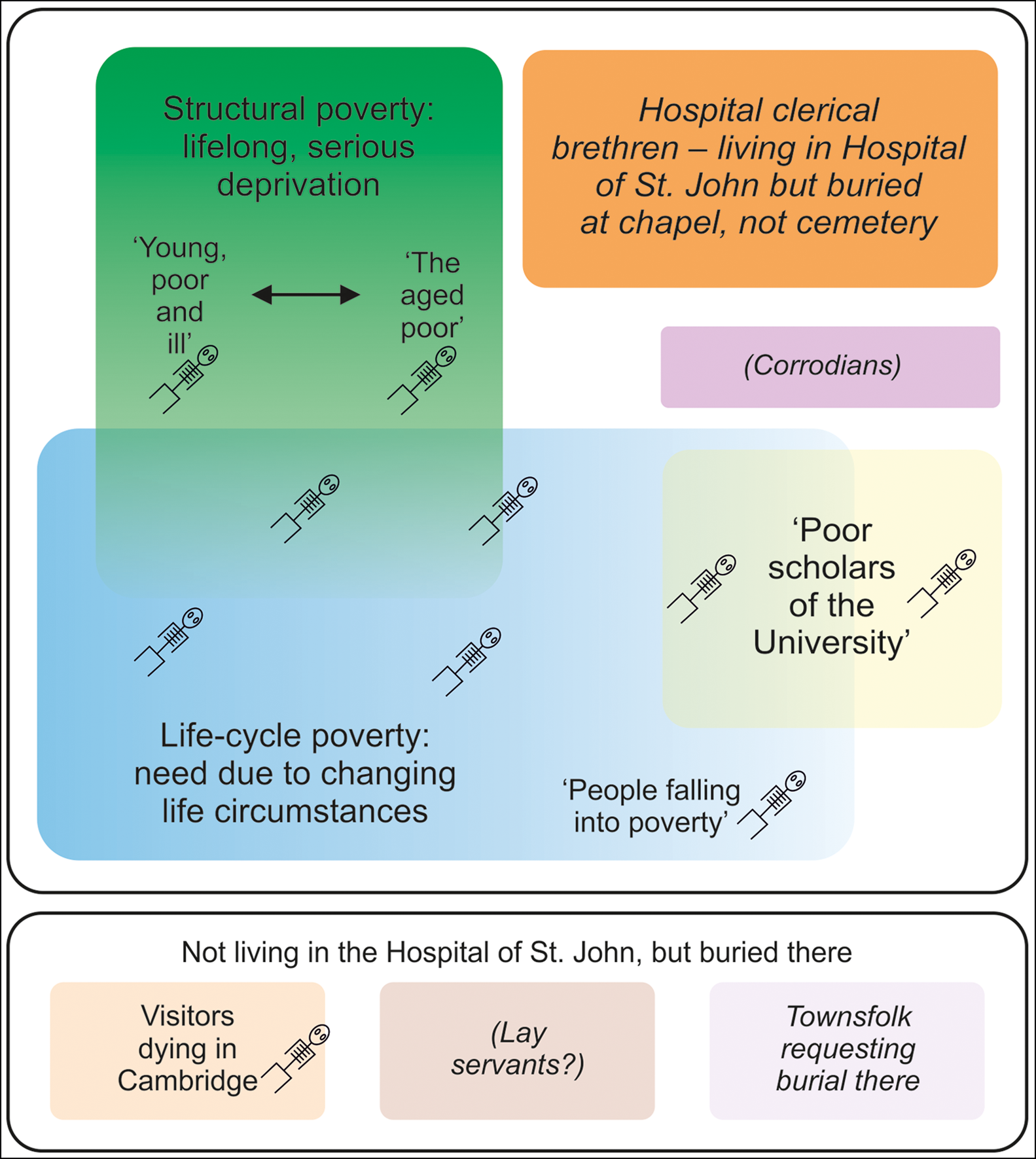
The osteobiographies of the residents of the Hospital of St John's show that the hospital managers conceived their charitable mission broadly, and people entered the hospital by many paths (Figure 6). Skeletal data cannot document all aspects of the life courses, and the ‘types’ identified here form fuzzy groupings rather than rigid, clearly bounded social categories. Nevertheless, they still give us a sense of how these people's lives varied. At any time, the dozen or so people living together in the hospital's dormitory might include weak, chronically ill poor children and young adults, older individuals who had toiled in poverty until they could work no longer, people who had lived comfortably until they encountered some misfortune, ill or retired university scholars, and townspeople who had purchased a place as a retirement plan. A few others joined them in the cemetery, including possible visitors who died while in Cambridge.
The Hospital of St John the Evangelist, Cambridge: a conceptual map. Skeletons indicate the kinds of individuals identified in this study; italics indicate groups attested in documentary records but not identified skeletally; parentheses indicate groups which may have been present but which are not attested textually (figure by the authors).
Conclusion
This article pioneers a new use of collective osteobiography, using skeletal evidence to draw out the various life paths of individuals and infer subgroupings based on clusters of bioarchaeological characteristics. It demonstrates how an apparently undifferentiated mass of individuals contained subgroups who followed different life paths. Such a strategy underscores how osteobiography can provide new information, rather than simply elaborating on what is already known from documentary or archaeological sources; this strategy highlights what can be achieved by using bioarchaeological evidence as the basis for collective osteobiography. In our case, it reveals that people entered the Hospital of St John the Evangelist via several routes: lifelong poverty, situational poverty, changes in worldly circumstances, university membership and dying far from home.
Beyond emphasising the variety of life paths that led people to the Hospital of St John, this approach sheds new light on the hospital's institutional logic. Hospital managers approached admissions decisions pragmatically and flexibly. Rather than privileging a narrow band of recipients which might maximise one factor—such as material benefit for the lifelong poor, spiritual value or political influence—instead, they chose to help a range of people. This not only fulfilled their statutory mission but also provided cases to appeal to a range of donors and their emotions: pity aroused by poor and sick orphans, the spiritual benefit to benefactors of supporting pious scholars, reassurance that there was restorative help when prosperous, upstanding individuals, similar to the donor, suffered misfortune. As a long-term strategy, this served the communities of both Cambridge and the Hospital of St John the Evangelist well, maintaining the institution through several centuries of change in a way that a tightly focused, single-cause mission might not.
Acknowledgements
We are particularly grateful to Trish Biers, Natasha Dodwell, Ben Neil and Miri Rubin for help in this research. We thank the editor and reviewers for comments, which have greatly improved this work.
Funding statement
Research was funded by the Wellcome Trust (Collaborative Grant 2000368/Z/15/Z), the McDonald Institute for Archaeological Research and St John's College, Cambridge.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.15184/aqy.2023.167.







 Open access
Open access