


Around a quarter of English psychiatric in-patient admissions are thought to be parents of dependents. Reference Maybery and Reupert1,Reference Wyatt, Aldridge, Callaghan, Dyke, Moulin and Spilsbury2 Such hospitalisations involve parent–child separation, disrupting the parent–child relationship Reference Dunn, Christiansen, Elsby-Pearson, Kramer, Swinburn and Platt3,Reference Reupert, Tchernegovski, Chen and Huddle4 and placing children at risk of impaired psychosocial outcomes. Reference Bell, Bayliss, Glauert, Harrison and Ohan5–Reference Konishi and Yoshimura7 The need to support relationships during parental hospitalisation is enshrined in numerous guidelines, including the European Convention on Human Rights and the Mental Health Act (1983), which states:
‘…every effort should be made to support parents [who have been hospitalised] to support their children.’ 8,9
To meet these requirements, services must first identify parents, yet this is done inconsistently, Reference Dunn, Startup and Cartwright-Hatton10 despite the need to do so being highlighted as far back as 2011 in reports by The Social Care Institute for Excellence and the Royal College of Psychiatrists. Reference Diggins11,12 A 2018 review found only one UK-based study that reported these data. Reference Wyatt, Aldridge, Callaghan, Dyke, Moulin and Spilsbury2 There is a similar lack of research evaluating service provision for such patients.
Given this lack of research, the current study sought to use a cost-effective Freedom of Information (FOI) approach to generate evidence on the extent to which English mental health trusts identify and support in-patients who are parents, by quantifying their prevalence and examining key indicators of family-focused practice.
Method
Aims
This study had two key aims:
-
(a) to quantify the prevalence of parents in in-patient settings;
-
(b) to begin to explore whether in-patient parents’ needs are being met. This was achieved by scrutinising a broad range of key metrics that are likely to be strong preliminary indicators of the quality of a trust’s family-focused practice:
-
(i) What (if any) information is collected on in-patients who are parents?
-
(ii) Do trusts maintain policies/procedures relating to in-patients who are parents?
-
(iii) Do trusts provide specific materials for in-patients who are parents, their children, their carers or their children’s carers?
-
(iv) The frequency of children’s visits to hospitalised parents.
-
Ongoing research examines these issues in greater depth – for example, assessing the quality and usefulness of policies and resources for parents/children/carers – but those findings are not reported here. The purpose of the present study was to provide a broad overview, giving a high-level picture of the general level of attention given by trusts to family-focused practice.
Design
A cross-sectional evaluation of all English NHS trusts that provide in-patient psychiatric care. Responses were sought under the Freedom of Information Act (2000), which allows access to certain information held by public bodies.
Procedures
FOI requests were sent to all English NHS trusts that provide any in-patient psychiatric care. In order to access information uncomplicated by the effects of the COVID-19 pandemic, trusts were asked to provide data relating to a 2-year period running from 1 January 2018 to 31 December 2019 inclusive. In summary, the request asked:
-
(a) overall number of admissions;
-
(b) number of admissions of parents (of a child <18 years);
-
(c) what data are routinely collected on parental status when an in-patient is admitted;
-
(d) trust or ward policies/procedures/handbooks/leaflets relating to the needs of in-patients who are parents, and/or their children;
-
(e) the number of visits by children to their in-patient parents.
The exact request is reproduced in Fig. 1.
Details of Freedom of Information request.

In cases where trusts failed to respond, or were unable to provide data because of resource limitations (organisations can legally reject requests that will take >18 h to fulfil), a shortened request was sent, and they were then asked to work through this in order, providing whatever data possible.
Analysis
This paper reports all data from questions 1, 2 and 4 (see Fig. 1), and summary data from question 3 (policies/procedures and materials – detailed data will be reported elsewhere).
To ensure accurate data extraction from the diverse and complex responses, a randomly selected 10% of trusts were double-extracted (by S.C.-H. and A.D.) and responses compared. This yielded a reliability rate of 96%, and therefore data extracted by the first coder were accepted as accurate.
Results
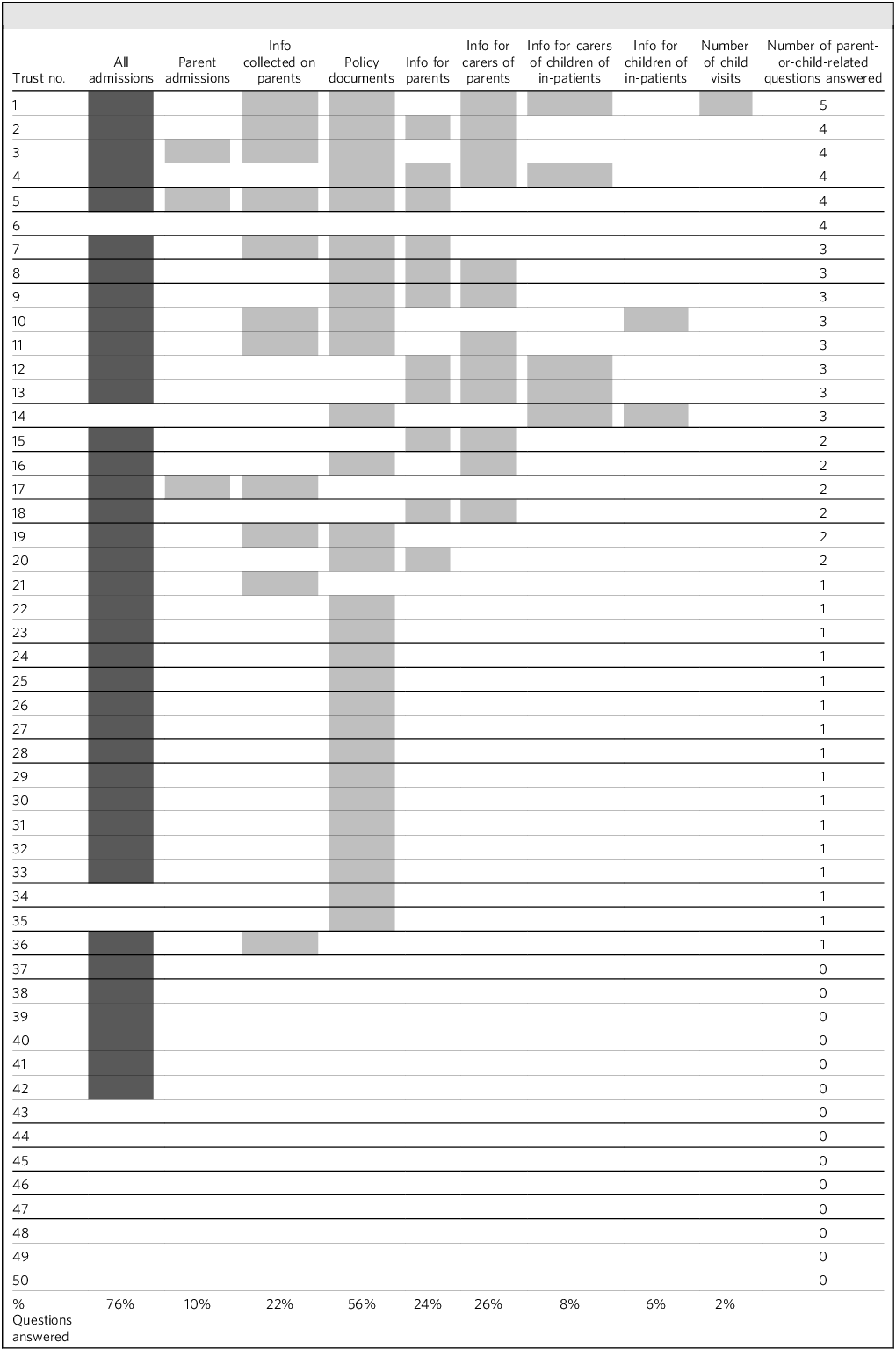
Three trusts (6%) that (according to their websites) provide in-patient psychiatric care failed to respond entirely; the remaining 47 provided at least partial information (see Table 1). Responses to the questions are listed below.
Trust-level responses to Freedom of Information (FOI) request items

Shaded cells indicate at least a partial response to the question. Dark grey shading denotes an answer to our first question about all total number of admissions (not just parents); light grey shading denotes answers to questions specifically about in-patients who are parents or their children.
1a. How many individual admissions were made to each psychiatric in-patient ward in the trust?
This was asked as background data to question 1b. Data are not described here, but are reported under question 1b, as appropriate. Thirty-eight trusts returned basic information (most not disaggregated by ward, as requested). The reasons for failure to provide this information are outlined in Table 2.
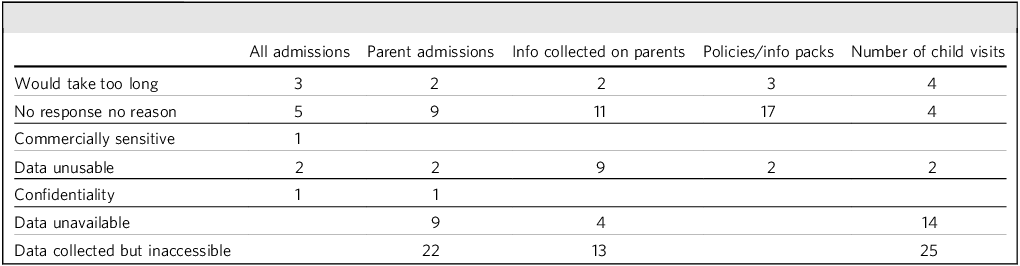
Reasons given by trusts for inability to provide data

Note: Numbers refer to number of trusts giving each explanation.
1b. How many of the patients reported under question 1a were parents?
Five trusts (10% of all trusts) provided meaningful responses to this question. Of these, in-patients were identified as parents in 4.3–21.0% of cases (mean 13.9%). The reasons for failure to provide these data are outlined in Table 2.
2a. What data are routinely collected on parental status when in-patients are admitted, or during their care?
Only 11 trusts could provide an answer to this question. The reasons for failure to provide these data are outlined in Table 2.
The following items were collected by one or more trusts; no trust captured all items.
-
(a) names of children <18;
-
(b) ages/dates of birth of children;
-
(c) does the patient have legal responsibility for child/ren? If not, who does?
-
(d) children’s current care arrangements;
-
(e) any other agencies involved with children;
-
(f) other adults living in household;
-
(g) do any children live with the patient (one trust specified this should be one night per week or more)? If not, their address;
-
(h) details of midwife/health visitor/school nurse/lead professional/GP/school;
-
(i) consent to notify health visitor/school practitioner? If not, reasons;
-
(j) has health visitor/school nurse notification been sent?
-
(k) any additional support required to parent children?
-
(l) has ‘early help’ been offered to parent?
-
(m) is patient a risk to their children/other children?
-
(n) is patient/partner pregnant?
Notably, completion of these fields was often not mandatory. In some trusts, completion of many fields was ‘triggered’ only when safeguarding risk was identified.
3. Trust/ward policies/procedures and information packs for parents, carers, children’s carers and children
-
(1) 28 trusts returned policies/procedures relating to in-patients who are parents.
-
(2) 11 sent in-patient welcome packs, of which 8 included reference to the needs of parents.
-
(3) 13 trusts sent information sheets for carers of in-patients.
-
(4) Only 8 sent carer materials that included reference to the needs of in-patient parents or their children and, in almost all cases, this was superficial and gave only (basic) information about children’s visits, often discouraging these.
-
(5) 3 provided information sheets for carers of in-patients’ children.
-
(6) 3 provided resources for the children of in-patients.
The reasons for failure to provide this information are outlined in Table 2.
4. Child visits
Only one trust was able to provide information on child visits to ‘secure services’, but they explained that data from ‘the Mental Health Service’ was available only in case-notes and could not be reasonably collated. For their secure services, over the course of the 2-year period in question, the number of child visits to ‘high secure’ was 206, to ‘medium secure’ was 142 and to ‘low secure’ was 13. Unfortunately, from the data available, we are unable to determine how many admissions were made overall to these wards, and therefore it has not been possible to calculate a ‘rate’ of child visits per patient.
The reasons given by trusts for failure to provide these data are outlined in Table 2.
Reasons for refusal
As can be seen in Table 2, there were a range of reasons given for inability to return information. However, in the large majority of cases, these reasons related to inaccessibility of the information: either it was simply reported to be unavailable or, if it was collected, this was not in a form that would allow rapid collation and analysis – for example, it was held only in individual case-notes. In many situations no reason for failing to provide information was provided and, given the fact that (for the majority of trusts) other information was provided, it must be assumed that non-delivery again reflects a lack of existing processes to allow this.
Discussion
This study had two key aims: (a) to quantify the prevalence of parents in in-patient settings and (b) to begin to explore whether their needs were being met, by scrutinising key metrics that are likely to be strong preliminary indicators of the quality of a trust’s family-focused practice.
The results highlight the limited attention paid by trusts to the needs of in-patients who are parents.
We asked all English NHS trusts that provide in-patient psychiatric care to tell us how many of their in-patients were parents of children aged under 18 years. This basic information was available from just 10% of trusts: the remaining trusts (90% of the total) were unable to tell us how many of their in-patients were parents. This is noteworthy, given that mental health trusts are officially required to provide the Mental Health Services Data Set with information on whether each patient has any dependents aged under 18 years. Having explored these limited data, it appears that the proportion of in-patients who were parents of minors ranged from 4.3 to 21% (mean 13.9%). It is difficult to ascertain the reliability of these statistics: they appear lower than those reported in a review in which international prevalence rates ranged from 12.3 to 38.5%. Reference Wyatt, Aldridge, Callaghan, Dyke, Moulin and Spilsbury2 A more recent evaluation in the Czech Republic identified a prevalence rate of 34.6%. Reference Havelková, Havelka and Koros Bartošová13
We asked all trusts to tell us what information they collected when a parent was admitted. Only 11 trusts (22%) had access to this information, indicating wide variation in practice. Of the list of information types recorded by trusts, no single item was reported by all 11. Critically, in some settings, administration of these questions was triggered only in the event that a safeguarding risk was identified. It is clear that there is no standard practice and, in many settings, there may be no standard practice at all.
The Mental Health Act Code of Practice (2015) enshrines a number of rights for psychiatric in-patients: (a) the right to be supported to maintain a family role during hospitalisation, including for parents to be supported in parenting; (b) the right to be visited by anyone they wish; (c) that hospitals should have written policies regarding child visits to hospital; and (d) that information about visiting should be explained to children in a way they understand. Despite this, <60% of trusts were able to send us any kind of policy, procedure or information pack relating to patients with parental responsibilities or their children. Eleven trusts (22%) sent us ward welcome packs but, of these, only eight contained text (mostly brief) relating to the needs of parents and there was minimal information for carers of children or children themselves. Where policies referred to child visits, this generally indicated simply that decisions about visits should be documented and risk-assessed.
Moreover, no trust was able to provide information on how many parents had received visits, with only one trust being able to report the total number of visits – and this was just for some of their (secure) wards. Unfortunately, this latter information could not be connected to data on the total number of in-patients admitted to those wards, and so we were unable to calculate a ‘rate’ of child visits. It is, therefore, unclear whether trusts are supporting parents in having contact with their children and, until better data are gathered, it will remain so. Despite this, we suspect that most trusts do allow (if not facilitate) child visits. In a separate paper, we will describe the data provided on facilities for families visiting in-patient parents but, briefly, this indicates that although visits from children are expected, they are poorly supported.
To our eyes, these findings raise two major issues. The first relates to the poor state of information collected about psychiatric in-patients who are parents; the second relates to what this tells us about provision for such parents. The two are, of course, not unconnected. We will discuss them in turn.
First, the inability of the majority of trusts to answer our fairly basic questions is concerning. None of the 50 trusts we approached were able to answer all our questions: even the best could partially answer only just over half. The reasons given for this failure were manifold. In one or two cases the data were considered ‘commercially sensitive’ or the numbers involved were so small that they might breach confidentiality. However, in the majority of cases we were told (or it was implied) that the data were held only in individual case-notes and had not been collated in a centralised form. In other cases, we were told that the data were either not held (unclear whether this meant not held at all, or not held in centralised form) or we were given no reason at all.
This lack of usable, accessible data is concerning on several levels. If a trust does not know how many of its in-patients are parents, it cannot hope to provide services that meet their needs. And, if a trust cannot identify patients who are parents, it cannot ensure that those services are offered to them. At a most basic level we cannot be sure, based on these data, that trusts are fulfilling their safeguarding obligations. These difficulties replicate at the national level – if the Department of Health and Social Care does not know how many in-patients are parents, it cannot plan services for them and cannot commission appropriate research for them. We would urge the NHS, and individual trusts, to ensure that enquiry about parental responsibility is made at all in-patient admissions, and that this information should be recorded and collated centrally by trusts and also at the national level. At the moment there is no consensus on what information should be collected. We suggest that a set of basic questions be devised: every patient admitted should be asked about their parental status; for those who are parents of dependents, a list of further questions (relating not just to safeguarding, but also to the parent’s concerns about their children and their parenting) should be administered.
Second, it seems likely from the results of this study that provision for psychiatric in-patients who are parents (and their children) is poor. Despite being required by the Mental Health Act Code of Practice, only 28 of 50 trusts were able to direct us to a policy relating to in-patients who are parents. A small minority of trusts were able to show us adequate sources of information to be provided to in-patient parents, their carers or their children, but no trust managed all of this. This is disappointing but is a relatively easy fix: template policies and leaflets (for parents, for children and for children’s carers) should be made available, ready for minor local adaptations and rapid publication to those who need them. The quality and appropriateness of these policies and handouts is explored in more detail in ongoing research, and it is expected that recommendations for templates will emerge from this.
This study has a number of strengths, including the involvement of 94% of all English trusts that provide in-patient psychiatric care. We are unaware of any study that has achieved such widespread coverage. However, a number of limitations should be noted. As an unfunded study, resources were not available to pursue all data that were not readily produced. However, in trusts that were re-contacted for further information, this was generally unforthcoming. We believe it unlikely that a more assertive approach would have yielded substantially clearer results. In retrospect, we would have focused on asking a smaller number of questions in greater detail and would advise colleagues attempting FOI studies to do likewise. Many detailed questions remain, which the data from our broad-brush overview are unable to answer.
In addition, this study focuses on English trusts only, with the devolved nations each having distinct health systems with their own structures, policies and regulatory frameworks. For example, in Northern Ireland, health and social care have long been fully integrated into a single system and, for over a decade, they have had a national programme of family-focused practice. Given our study’s resources and remit, we judged it more feasible and meaningful to focus in depth on the largest system, NHS England, while recognising that future work could explore parallels and differences across the UK as a whole.
We recognise that a lack of response from a trust does not, per se, prove that the trust is failing to collect data or meet its responsibilities. However, if data cannot be accessed or provided, it strongly suggests that it is not being used to guide service delivery. For instance, if a trust cannot access its own child visitation policy, it cannot be confident that it is adhering to it.
English NHS trusts collect and collate data very poorly on psychiatric in-patients who are parents. The limited available data tell us that provision for such patients and their families is likely to be inadequate. We would urge leadership at both trust and national levels to improve both provision and the data collection around it, and to consider delegating the evaluation of this to the Care Quality Commission. The evidence is clear – both parents and their children suffer when they are separated by parental hospitalisation – but, with high-quality provision, this harm can be minimised. Based on the results of this study, it seems very unlikely that this provision is being made.
About the authors
Abby Dunn is an associate professor (psychology) in the School of Psychology, University of Sussex, Brighton, UK and an NIHR Advanced Fellow researching the intersection of parenting mental health and how to limit the intergenerational transmission of mental illness. Sam Cartwright-Hatton is a professor of clinical child and adolescent psychology at the University of Sussex, Brighton, UK, specialising in the prevention and treatment of childhood anxiety disorders with a current focus on interventions designed to limit the intergenerational transmission of anxiety.
Data availability
The data that support the findings of this study are available from the corresponding author, A.D., upon reasonable request.
Author contributions
A.D. formulated the research questions, designed the study, carried out data collection, analysed the data and wrote the article. S.C.-H. formulated the research questions, designed the study, carried out data collection, analysed the data and wrote the article.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.
Ethical standards
This study included only secondary data.


 Open access
Open access
eLetters
No eLetters have been published for this article.