

Highlights
-
• In Cushing’s disease (CD), early postoperative QOL often fails to normalize; hypertension and physical health improved in our cohort.
-
• Clustering identified five QOL trajectories (three severity groups), revealing marked heterogeneity in recovery.
-
• The QOL-CD detected nuanced changes and strong links between emotional, mental and social domains, supporting individualized, psychosocially informed follow-up.
Introduction
Cushing’s disease (CD) is characterized by sustained elevations in cortisol arising from hypersecretion of adrenocorticotropin hormone (ACTH) from a pituitary neuroendocrine tumor. Reference Nishioka and Yamada1 Recent estimates suggest that CD affects roughly 2.2 people per 100,000 worldwide. Reference Giuffrida, Crisafulli and Ferraù2 Due to the widespread role of cortisol, CD can cause many debilitating symptoms that can impair one’s physical, emotional, social and functional quality of life (QOL). Reference Nishioka and Yamada1,Reference Cusimano, Huang, Marchie, Smyth and Kovacs3,Reference He, Findling and Auchus4
The primary treatment for CD is transsphenoidal surgery (TSS) for resection of the pituitary tumor. Through negative feedback, the prolonged high cortisol level prior to surgery leads to severe downregulation of the healthy ACTH-producing cells of the pituitary gland. This effect leads to abnormally low cortisol levels, or a “withdrawal state” following removal of the tumor. Reference He, Findling and Auchus4 Recovery of endogenous cortisol regulation via the hypothalamic–pituitary–adrenal (HPA) axis can range from several weeks to years. Reference Balasko, Zibar Tomsic, Kastelan and Dusek5
Until the HPA axis recovers, hormone replacement therapy is needed to treat glucocorticoid withdrawal syndrome (GWS; also known as cortisol or steroid withdrawal syndrome), as this syndrome leads to a different profile of symptoms that include muscle weakness, extreme fatigue and hypersomnolence. Reference He, Findling and Auchus4,Reference Balasko, Zibar Tomsic, Kastelan and Dusek5 Mood changes tend to develop more slowly over time, ranging from mood swings to depression. Reference He, Findling and Auchus4
These multifaceted and lasting symptoms of CD and its treatment have sparked interest in researching QOL in CD patients. A systematic review of QOL studies showed decreased QOL in all domains (based on the Short Form-36 survey or SF-36) for active CD patients compared with healthy controls and reference values. Reference Andela, Scharloo, Pereira, Kaptein and Biermasz6 Further studies have demonstrated significant reductions in all domains of QOL before treatment and improvements across these domains following treatment, although full normalization of QOL is not typically achieved. Reference Cusimano, Huang, Marchie, Smyth and Kovacs3,Reference Lindsay, Nansel, Baid, Gumowski and Nieman7–Reference Zarino, Verrua and Ferrante9 In some studies, QOL reductions lasted as long as 12 months postoperatively in some patients. Reference Theodorou, Tan and Bakkar8,Reference Zarino, Verrua and Ferrante9 A qualitative study characterized the GWS phase acutely following Cushing’s treatment as having more pain, severe fatigue, worries about physical appearance, disorders with family life and partner relationships, decreased work/school performance, helplessness often leading to depression and a negative perception of QOL. Reference Lindsay, Nansel, Baid, Gumowski and Nieman7,Reference Gotch10
Several disease-specific instruments have been developed to assess QOL in patients with Cushing’ s syndrome and CD, most notably the CushingQoL questionnaire and the Tübingen CD-25 Inventory. Reference Webb, Badia and Barahona11,Reference Milian, Honegger, Teufel, Wolf and Psaras12 Studies using these tools consistently demonstrate marked impairment in QOL at diagnosis and incomplete recovery following treatment, with deficits persisting for years despite biochemical remission. Reference Andela, Scharloo, Pereira, Kaptein and Biermasz6–Reference Zarino, Verrua and Ferrante9 Long-term follow-up studies have shown that although some domains may improve after surgery, full normalization of QOL is uncommon even 5–10 years after treatment. Reference Lindsay, Nansel, Baid, Gumowski and Nieman7,Reference Theodorou, Tan and Bakkar8 These findings underscore that biochemical cure does not equate to complete functional recovery.
To better understand how CD and its treatment impact patients’ QOL, we 1) investigated changes in domain-specific QOL before and after surgery with biochemical cure, 2) looked for correlations between changes in QOL domains and 3) clustered CD patients into subgroups based on patterns in the changes of QOL before and after biochemically curative surgery.
Understanding how QOL changes before and after surgery will provide insights into improving management of these patients by allowing patients, caregivers and healthcare providers to be made more aware of and better prepare for the difficult postoperative recovery from CD treatment.
Methods
This study was approved by the Unity Health Toronto Research Ethics Board (#06-077 and #24-247) and was conducted in accordance with the standards outlined by the Declaration of Helsinki.
Patients
Patients treated for CD at our hospital from 2008 to 2024 were included in the study. Patients with acute comorbidities (e.g., severe infection) severely affecting QOL were excluded from the study. Chronic comorbidities were not exclusionary to preserve sample size and generalizability of our findings. Patients were classified as having either hormonally active or cured CD according to Endocrine Society guidelines; criteria for biochemical cure necessitated either morning serum cortisol level <138 nmol/L or a 24-hour urinary free cortisol (UFC) of 10–20 µg/day within 7 days following tumor resection. Reference Nieman, Biller and Findling13 Further confirmation of successful treatment was based on 1-mg dexamethasone suppression tests and midnight salivary cortisol measurements at the discretion of the care providers. A subset of patients provided data at both phases of disease, comprising the study sample for our paired analysis. Individuals with recurrent or cyclical CD and those receiving ketoconazole therapy at the time of questionnaire completion were excluded from the paired analysis to mitigate confounding. Additionally, to account for HPA axis recovery and time-dependent effects, patients not receiving glucocorticoid replacement therapy and data collected more than 1 year postoperatively were excluded from the paired analysis. The study cohort represents all patients treated for CD at our institution during the study period who met inclusion criteria and completed QOL questionnaires as part of routine clinical care; exclusions from specific analyses were based on predefined clinical factors and availability of paired pre- and postoperative data.
Data collection
Data were collected prospectively at the time of routine neurosurgery and endocrinology clinic visits using patient-reported questionnaires and clinical assessments. QOL questionnaires were administered contemporaneously with clinical evaluations and did not rely on retrospective recall of prior QOL. Routine pituitary endocrinological testing, including salivary cortisol measurement, UFC, and dexamethasone suppression tests were conducted alongside each clinical visit as part of standard clinical practice. Symptom duration and dosing of hormone replacement medication were extracted retrospectively from clinical documentation.
In addition to the QOL questionnaires detailed below (see Quality of Life Assessment), the study questionnaire battery included age, sex, diagnosis, primary treatment, comorbidities, and binary self-reports of relevant signs and symptoms.
QOL assessment
Data on QOL were collected prospectively at the time of preoperative and postoperative patient visits following implementation of the validated QOL-CD questionnaire in clinical practice after its validation. Patients were not asked to retrospectively assess QOL at earlier disease stages. In accordance with standard clinical practice, patients were assessed 3 and 6 months postoperatively; however, the precise timing of follow-ups varied slightly due to scheduling constraints. The QOL-CD (version 3) was used to measure CD-specific QOL; this unique, validated questionnaire was developed specifically to assess the multidimensional nature of QOL in CD patients. Reference Cusimano, Huang, Marchie, Smyth and Kovacs3 The QOL-CD consists of six subscales: general health, emotional health, physical health, mental status, social well-being and (satisfaction with) medical treatment. Reference Cusimano, Huang, Marchie, Smyth and Kovacs3 The QOL-CD comprises a total of 34 items distributed across six subscales: general health (6 items), emotional health (6 items), physical health (7 items), mental status (6 items), social well-being (6 items), and satisfaction with medical treatment (3 items). Based on prior validation studies and routine clinical use, the questionnaire typically requires approximately 10–15 minutes to complete. An overall score can be calculated as the average of these six subscales, where higher scores indicate greater QOL. Accordingly, the present analysis was designed to characterize early postoperative QOL changes rather than long-term recovery or normalization.
The RAND-36 (also known as SF-36 version 2) was used as a measure of general QOL. Reference Ware and Sherbourne14 The questionnaire consists of eight subscales: general health, mental health, vitality, bodily pain, social functioning, physical functioning, role limitations due to personal or emotional problems (role emotional) and role limitations due to physical health problems (role physical). Reference Ware and Sherbourne14 Rather than providing an overall score, two distinct scores, the physical component score (PCS) and mental component score (MCS) were reported. The study design reflects prospective collection of patient-reported outcomes at clinical encounters, rather than longitudinal recall of QOL prior to questionnaire implementation.
Statistical analysis
All data cleaning, preparation, statistical analysis and figure creation were performed using R (version 4.3.2; R Foundation for Statistical Computing, Vienna, Austria) within RStudio (version 2023.06.1+524). Primary packages used included dplyr (v1.1.4) for data manipulation, ggplot2 for visualization, mice for multiple imputation and base R statistical functions. 15–Reference van Buuren and Groothuis-Oudshoorn19 Descriptive statistics were calculated for continuous variables, and frequencies were generated for other variables. A familywise type I error rate of 5% was used, and multiple comparisons were accounted for with a Bonferroni correction. Data missing from the QOL-CD and RAND-36 were imputed via multiple imputations (2 × 5 iterations) using predictive mean matching. A Pearson correlation matrix was used to investigate associations between changes in QOL-CD subscales. Odds ratios were calculated for the signs and symptoms assessed by the study questionnaire. A sensitivity analysis was used to investigate if the timing of postoperative follow-up significantly impacted QOL-CD scores.
Paired analysis
A subset of patients completed questionnaires both before and after surgery, allowing for a paired analysis of QOL-CD and RAND-36 scores between the two time points. Given the limited sample size, nonparametric methods were used. Changes in QOL-CD scores (referred to as “change scores”) were calculated for each domain as the difference between early postoperative and pretreatment values.
Hierarchical Euclidean clustering was applied to change scores for each QOL-CD subscale as an exploratory, descriptive approach to visualize heterogeneity in early postoperative QOL trajectories. The optimal number of clusters was determined using a silhouette analysis. Each cluster was characterized based on size and domain-level QOL changes.
Results
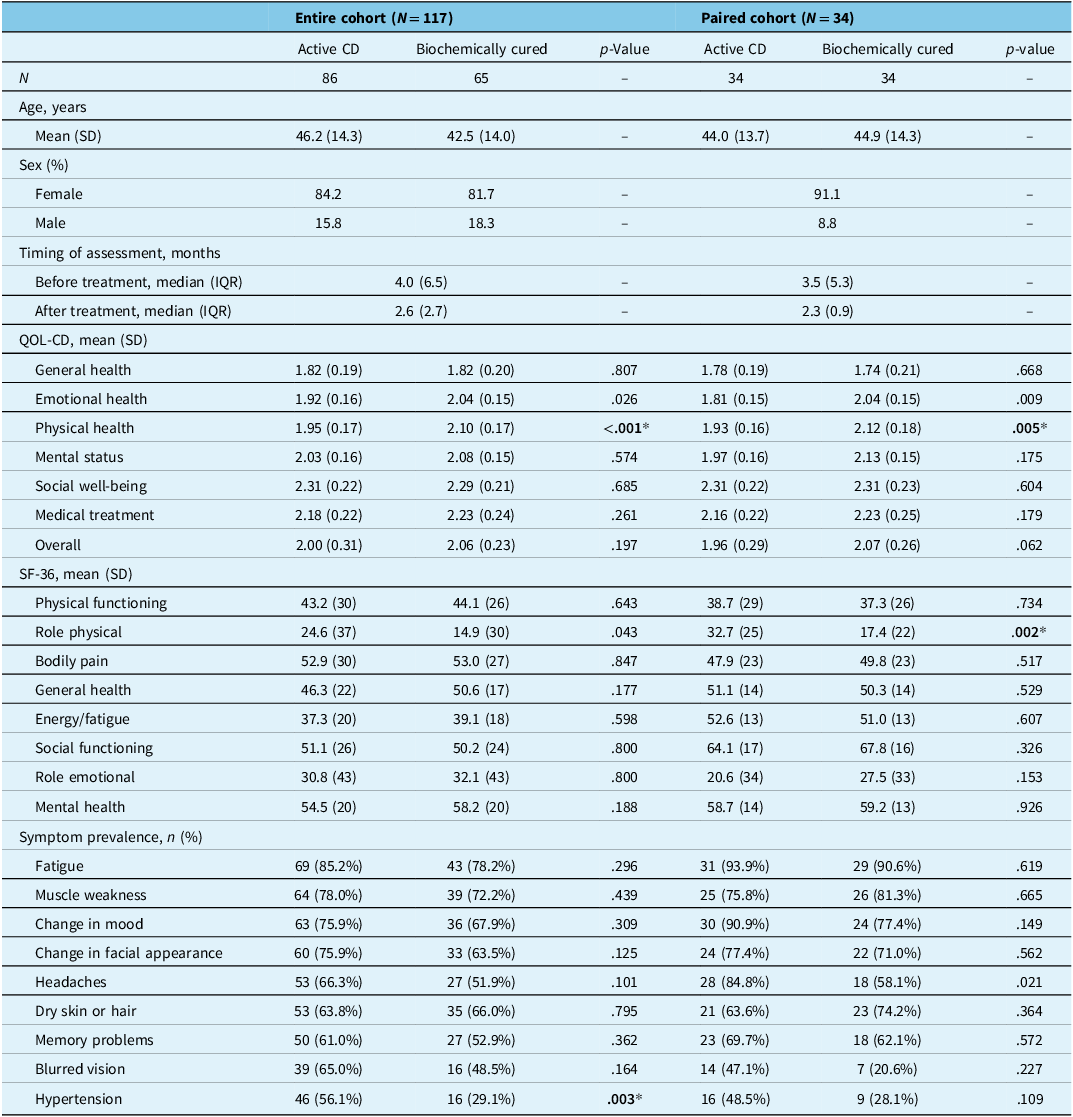
Of the 117 patients with eligible data, 86 contributed data during the active CD phase, while 65 provided data after biochemical cure. A subset of 34 patients had data available from both disease phases, comprising the paired cohort. Unless otherwise specified, analyses of the full cohort represent cross-sectional comparisons between disease phases rather than longitudinal within-patient changes. The mean ages before and after treatment were 46.2 ± 14.3 and 42.5 ± 14.0 years in the entire cohort and 44.0 ± 13.7 and 44.9 ± 14.3 years in the paired cohort. The sample was predominantly female at both time points (entire cohort: active = 84.2%, biochemically cured = 81.7%; paired cohort = 91.1%). Preoperative questionnaires were completed a median of 4.0 months before surgery in the entire cohort and 3.5 months in the paired cohort, while postoperative questionnaires were completed at a median of 2.6 and 2.3 months after surgery, respectively. The length of the follow-up interval postoperatively did not significantly affect QOL-CD scores. Characteristics of both cohorts are provided in Table 1.
Descriptive statistics for a cohort of 117 patients with CD and a subset of 34 patients with paired data from the active and early postoperative phases of disease

In the latter phase of disease, all patients were biochemically cured of CD according to Endocrine Society criteria. p-Values are given for odds ratio calculations for each symptom and t-tests for other variables, representing tests for differences in each variable between the two time points. CD = Cushing’s disease; SD = standard deviation; IQR = interquartile range; TSS = transsphenoidal surgery; QOL = quality of life; SF-36 = Short Form-36 survey. Significant p-values after accounting for multiple corrections are indicated with an asterisk
Unpaired cohort (n = 117)
In the unpaired cohort, comparisons between patients assessed during active disease and those assessed during the early postoperative phase demonstrated differences in several clinical and QOL measures (Table 1). Hypertension was less prevalent among patients assessed in the biochemically cured phase compared with those assessed during active disease (OR = 0.31, 95% CI = 0.14–0.66, p = .003). Patients assessed in the postoperative phase also reported a lower number of antihypertensive medications, whereas no significant difference was observed for diabetes medications. Physical health scores on the QOL-CD were higher in the postoperative phase compared with the active disease phase (W = 3505, p < .001). Associations between changes in emotional health, mental status, and social well-being were examined in the paired cohort and are reported separately below.
Paired cohort (n = 34)
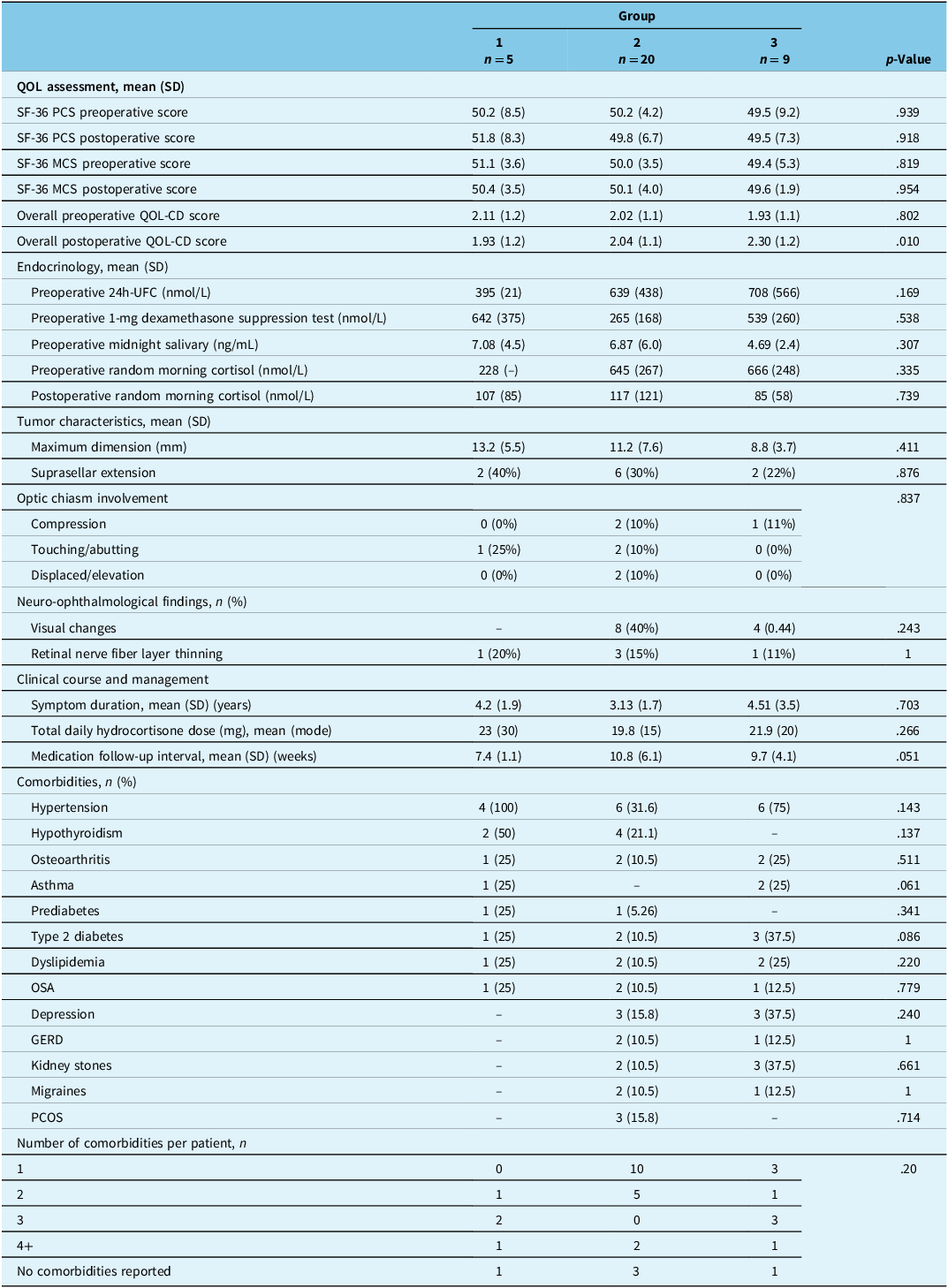
In the paired cohort, QOL-CD scores in the physical health (V = 406, p = .005) domains were significantly higher after biochemical cure. Exploratory clustering analysis identified five descriptive patterns of QOL changes (Figure 1). For descriptive purposes, these patterns were summarized into three broader response categories based on the direction and magnitude of QOL changes: Group 1 (n = 5) consisted of the Afflicted and Divergent-Mixed clusters, which showed decreases in all QOL domains. Group 2 (n = 20), the Marginal cluster, experienced declines in most QOL domains. Group 3 (n = 9), including the Flourishing and Elevating-OK clusters, showed significant improvements across all domains of QOL (Figure 2). Overall QOL-CD scores differed between the three groups in the early postoperative phase of disease (χ 2 = 9.3, df = 2, p = .10). Preoperative UFC tended to be higher in Groups 2 and 3 than in Group 1, although the difference was not statistically significant. Details of QOL, endocrinology, tumor characteristics, ophthalmology and comorbidities in the three groups are presented in Table 2.
Domain-level changes in quality of life (QOL) after 34 patients were successfully treated for Cushing’s disease (CD). Euclidean clusters of QOL change scores are shown on the x-axis. More red shading reflects worsening QOL scores, while bluer shading indicates improved QOL scores.

Polygon plots of the domains of quality of life (QOL) measured using the QOL-CD scale in 34 patients with CD measured during active disease and after surgical biochemical cure. Patients were grouped based on treatment response that was negative (Group 1), marginal (Group 2) or positive (Group 3). Values further from the center of the plot indicate greater QOL. QOL-CD = Quality of Life-Cushing’s Disease Questionnaire; CD = Cushing’s disease.

Comparison of three groups of CD patients based on treatment response

Group 1 patients showed worsening in all domains of QOL, Group 2 showed worsening in several domains of QOL and Group 3 demonstrated improvements across all QOL domains. QOL = quality of life; SF-36 = Short Form-36 survey; PCS = Physical Component Summary; MCS = Mental Component Summary; QOL-CD= Quality of Life-Cushing’s Disease Questionnaire; OSA = obstructive sleep apnea; GERD = gastroesophageal reflux disease; PCOS = polycystic ovary syndrome; UFC = urinary free cortisol. Significant p-values are indicated with an asterisk
Discussion
This study offers exploratory insight into the variety of QOL recovery patterns in CD patients before and after biochemically successful treatment. Our findings highlight the complex nature of posttreatment recovery in biochemically cured CD. Our analysis using paired pre- and postoperative data revealed three provisional subgroups of treatment responses. Despite full endocrinological replacement with hydrocortisone, about three-quarters of our patients were not significantly better in their reports of QOL; group 2 had declines in most domains or modest changes (n = 20 or 59%) and group 1 had widespread worsened QOL (n = 5 or 15%). One-quarter of patients reported QOL widespread domain improvements (group 3, n = 9 or 26%). We could not relate these changes in QOL to any specific clinical, laboratory or radiological variable, although there we observed a nonsignificant tendency for patients in group 3 to have higher preoperative 24-hour UFC levels. Taken with prior findings, this pattern is consistent with UFC as a candidate prognostic marker, but our study was not designed or powered to evaluate prognostic performance. Reference Schernthaner-Reiter, Siess and Gessl20
Together, these findings highlight an array of responses to CD treatment within the first few postoperative months. Importantly, the limited improvement observed in many patients during this early postoperative period is consistent with prior literature demonstrating that recovery of QOL following successful treatment of CD is often delayed and may remain incomplete for years. Reference Andela, Scharloo, Pereira, Kaptein and Biermasz6,Reference Lindsay, Nansel, Baid, Gumowski and Nieman7 Studies using the CushingQoL and Tübingen CD-25 instruments have shown persistent impairments in physical, emotional and social domains long after biochemical remission. Reference Webb, Badia and Barahona11,Reference Milian, Honegger, Teufel, Wolf and Psaras12 Within this context, the worsening or marginal changes observed in the majority of our patients are not unexpected and likely reflect the acute glucocorticoid withdrawal phase, during which symptoms such as fatigue, weakness, mood disturbance and cognitive impairment are common. Reference He, Findling and Auchus4,Reference Balasko, Zibar Tomsic, Kastelan and Dusek5,Reference Gotch10 Despite achieving biochemical cure of CD, many patients did not experience QOL improvements within the time frame of the study, while a minority showed notable recovery posttreatment. One plausible explanation for this variation in recovery patterns relates to differences in the restoration of endogenous cortisol regulation, which is known to vary in timing; however, we did not test this directly. Reference Balasko, Zibar Tomsic, Kastelan and Dusek5 Larger longitudinal studies with extended follow-up will be required to confirm these early recovery patterns, to determine how early postoperative trajectories relate to long-term QOL outcomes, and to identify clinical or biological factors that may predict sustained recovery or persistent impairment.
Moreover, our findings support the use of the QOL-CD as a CD-specific QOL measure. As expected for a disease-specific instrument, the QOL-CD was more sensitive to differences in QOL than the generic SF-36 in this cohort, reflecting its ability to capture issues specific to CD rather than indicating a formal psychometric superiority. This highlights the value of the QOL-CD in capturing the nuanced recovery patterns that the SF-36 may miss.
Several studies have investigated the postoperative course for CD patients. One study reported improvements in QOL as measured by the RAND-36 just 1 week after surgery. Reference Cusimano, Huang, Marchie, Smyth and Kovacs3 However, when compared to population-based norms, CD patients continued to exhibit significant deficits in physical, emotional and social well-being postoperatively. Reference Cusimano, Huang, Marchie, Smyth and Kovacs3 These findings are consistent with the possibility that some patients may benefit from further care to restore full recovery, a question that requires prospective evaluation. Gotch et al. Reference Gotch10 similarly reported substantial disruptions in daily life in a qualitative study of Cushing’s patients. Fatigue and weakness were most commonly reported, closely matching the most prevalent pretreatment symptoms in our sample. Improvements in fatigue and weakness were not detected in our time frame, which may indicate that this aspect of recovery occurs beyond our follow-up window.
A systematic review by Andela et al. Reference Andela, Scharloo, Pereira, Kaptein and Biermasz6 confirmed that QOL impairments persist in remitted CD, particularly in fatigue, muscle weakness, pain and emotional distress, including depressive symptoms. While biochemical cure leads to some improvement, the review found that full QOL normalization is rare despite multi-year follow-up intervals. Our study complements these findings by identifying five clusters of QOL trajectories, aggregated into three broader response groups. This heterogeneity suggests that individualized follow-up may be warranted, to be tested in confirmatory studies. Most patients (74%) experienced persistent or worsening symptoms (Groups 1 and 2), while a subset (26%) showed significant QOL improvements (Group 3). This aligns with prior reports that remission does not guarantee full functional recovery and underscores the need for individualized follow-up.
Andela et al. Reference Andela, Scharloo, Pereira, Kaptein and Biermasz6 also reported long-term emotional distress in remitted CD, whereas our study found early postoperative improvements in emotional health. This discrepancy may be due to differences in follow-up duration – our median follow-up was 2.6 months, whereas Andela et al. Reference Andela, Scharloo, Pereira, Kaptein and Biermasz6 included longer-term studies. Given the delayed-onset mood disturbances seen in GWS, it is possible that early emotional improvements may not be sustained over time. Our findings reinforce the importance of monitoring emotional health beyond the immediate postoperative period. The identification of distinct recovery subgroups suggests that standardized follow-up schedules may not be sufficient and that some patients may require early psychosocial support to improve long-term outcomes. Future studies should investigate whether these early improvements predict sustained recovery or whether additional interventions are needed to mitigate the emotional effects of GWS. Furthermore, Gotch et al. Reference Gotch10 reported substantial emotional instability (61%) and depression (32%) in their qualitative study, emphasizing persistent mood disturbances, cognitive impairment and social withdrawal. In our cohort, QOL-CD emotional health scores correlated strongly with both mental status (r = 0.66, p < .001) and social well-being (r = 0.53, p = .001), reinforcing the interdependence of psychological and social recovery. Gotch et al. Reference Gotch10 similarly highlighted that emotional dysregulation often disrupts social functioning, further impairing daily life. Collectively, these results support the need for longitudinal, individualized psychosocial assessment and intervention after CD surgery, with ongoing attention to the evolving interplay between emotional aspects of GWS and social functioning.
Our study has several strengths and limitations that should be considered when interpreting the findings. One strength of this study is the incorporation of biochemical status into our inclusion criteria and cohort stratification. We classified patients based on the phase of disease (i.e., active or cured CD) rather than as strictly pre- or postoperative (which has been routine in the literature). Our patients were all managed by experienced neuroendocrinologists and were all on hydrocortisone replacement postoperatively. This design makes it more likely that observed patterns reflect underlying disease state rather than failed surgery, although residual confounding cannot be excluded. Additionally, the inclusion of clustering analysis offers descriptive insight into patient experiences, but cluster assignments are provisional and may be sensitive to analytic choices; stability should be evaluated in independent datasets. Given the modest size of the paired cohort, the clustering analysis should be interpreted as hypothesis-generating rather than as evidence of stable or generalizable subgroups. Our cohort is reflective of the broader CD population (81% female), which is consistent with the well-documented female predominance in CD, with reported female-to-male ratios ranging from 3:1 to 8:1. Reference Pecori Giraldi, Moro and Cavagnini21 The under-representation of males in our cohort and others will need to be addressed in future studies to determine if males experience the same issues as females. Furthermore, given the rarity of CD, our sample size is necessarily modest; accordingly, we frame this as a preliminary, hypothesis-generating analysis whose estimates should be confirmed in larger, multi-institutional cohorts rather than interpreted as definitive.
In conclusion, this study descriptively outlines the varied patterns of posttreatment QOL recovery in CD and suggests limitations of assessing treatment success based solely on biochemical remission. Our results can be used to better educate patients on the spectrum of wellness after surgery, particularly in respect to mental, emotional and physical health. Future research should test whether targeted interventions improve outcomes in the subgroups we provisionally identified. Expanding patients’ support systems in CD care may help address persistent impairments and improve overall functional recovery. Ultimately, a holistic approach that includes QOL assessments is essential for optimizing patient outcomes in CD care.
Conclusion
In this single-center cohort, QOL after biochemically curative surgery for CD was heterogeneous: hypertension and physical health improved overall, yet early postoperative QOL often did not normalize. Exploratory clustering of paired data illustrated distinct patterns in early postoperative QOL trajectories, which were summarized into three descriptive response categories, with only a minority showing broad domain improvements. Emotional health changes correlated with mental status and social well-being, supporting routine use of the disease-specific QOL-CD to detect at-risk patients and guide individualized, psychosocially informed follow-up. Limitations include modest paired sample size, early follow-up and exploratory clustering. Larger longitudinal multi-institutional studies should validate trajectories, assess prognostic markers and test targeted interventions.
Acknowledgments
None.
Author contributions
AZL and JS prepared, analyzed and tabulated the study data. AZL, MDC and JG conceived of the study design and interpreted findings. All authors contributed to the drafting, preparation and review of the study manuscript and provided approval of the final version to be submitted for publication. AA wrote some sections of the manuscript and helped respond to reviewer feedback, along with AZL.
Funding statement
This research was conducted without any funding to report.
Competing interests
The authors have no competing interests to disclose.



 Open access
Open access
Target article
Quality-of-Life Recovery in Cushing’s Disease: A Cluster Analysis
Related commentaries (1)
Reviewer Comment on Levitan et al. “Quality of Life Recovery in Cushing’s Disease: A Cluster Analysis”