


Intellectual disabilities are lifelong conditions accounting for significant limitations in intellectual functioning and adaptive behaviour across cognitive, social and practical domains, with onset during the developmental period, typically in preschool. 1,2 The estimated global prevalence of ‘idiopathic intellectual developmental disability’ is around 2% 3 and the incidence around 1.8%. Reference Maulik, Lakhan, Kishore, Sahu, Bertelli, Sagar, Bertelli, Deb, Munir, Hassiotis and Salvador-Carulla4 People with intellectual disabilities experience significant health inequalities related to barriers to specialised healthcare, diagnostic overshadowing, stigma and limited access to education and employment, 5 all of which complicate the recognition and management of mental disorders.
Primary studies of people with intellectual disabilities report significant rates of mental comorbidities, ranging from 30 to 50%. Reference Maulik, Lakhan, Kishore, Sahu, Bertelli, Sagar, Bertelli, Deb, Munir, Hassiotis and Salvador-Carulla4,Reference Cooper, Smiley, Morrison, Williamson and Allan6–Reference Emerson and Hatton9 These elevated figures vary according to diagnostic system, age and clinical setting (e.g. in-patients versus community services), Reference Maulik, Lakhan, Kishore, Sahu, Bertelli, Sagar, Bertelli, Deb, Munir, Hassiotis and Salvador-Carulla4,Reference Cooper, Smiley, Morrison, Williamson and Allan6–Reference Emerson and Hatton9 underscoring the substantial mental health burden and setting the context for examining disorder-specific prevalence patterns.
Determining the prevalence of specific mental disorders in people with intellectual disabilities with or without other neurodevelopmental disorders (e.g. autism spectrum disorder (ASD)) is challenging, due to historical variations in diagnostic systems, difficulties in finding representative samples, Reference Bertelli, Cooper and Salvador-Carulla10,Reference Cooper, Melville and Einfeld11 limited availability of tailored diagnostic criteria for people with intellectual disabilities, and the complex interface between behaviours and mental disorders. Reference Bowring, Painter and Hastings12 Although people with intellectual disabilities are known to experience the full spectrum of mental disorders, evidence remains fragmented: systematic reviews vary widely in scope, diagnostic frameworks, population definitions and reporting practices, and often omit key subgroups or characteristics, e.g. sex, age (including older people) or those with co-occurring neurodevelopmental conditions.
To our knowledge, although two umbrella reviews have explored mental Reference Hossain, Khan, Sultana, Ma, McKyer and Ahmed13 and physical Reference Rydzewska, Dunn and Cooper14 comorbidity in autistic people, none has synthesised the prevalence of specific mental disorders in people with intellectual disabilities despite a growing number of systematic reviews on this matter. However, the review-level evidence remains fragmented across diagnostic categories, settings, diagnostic frameworks and population subgroups. As a result, it is difficult to interpret prevalence estimates consistently across disorders, or to identify where evidence is strong, weak or entirely lacking. An updated umbrella review is therefore needed to integrate available evidence, appraise the methodological quality of existing research, identify consistencies and discrepancies across reviews and highlight critical gaps in the evidence-based literature.
There were three research questions:
-
(a) What is the prevalence of specific mental disorders in people with intellectual disabilities without comorbid neurodevelopmental disorders?
-
(b) What is the prevalence of specific mental disorders in people with intellectual disabilities with other neurodevelopmental disorders (e.g. ASD)?
-
(c) What are the gaps in the literature on the prevalence of comorbid mental disorders in people with intellectual disabilities with or without other neurodevelopmental disorders?
Where available, we compared prevalence rates in people with intellectual disabilities with those in the general population.
Method
We conducted this umbrella review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann and Mulrow15 (Supplementary Tables 9 and 10), and the protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO, reference no. CRD42021230023, later updated to CRD42024610611). Reference Santambrogio, Capellazzi, Papola, Ayub, Barbui and Bertelli16,Reference Santambrogio, Boido, Marchetti, Besana, Francia and Ayub17
Literature sources
Author J.S. developed a systematic search strategy, assisted by G.B. and the bibliographic services of the University of Milano-Bicocca. ‘Developmental Disabilities’, ‘Intellectual Disability’, ‘Persons with Mental Disabilities’, ‘Learning Disabilities’, ‘Specific Learning Disorder’ and ‘Comorbidity’ were used as medical subject headings terms and adapted through six databases: the Cochrane Library, PubMed, PsycINFO (via ProQuest interface), Embase, CINAHL and Epistemonikos. Filters for systematic reviews or meta-analysis were applied when appropriate and available. G.B. and M.M. searched the grey literature on the following web platforms: World Psychiatric Association, European Psychiatric Association, National Association for the Dually Diagnosed, European Association for Mental Health in Intellectual Disability, International Association for the Scientific Study of Intellectual and Developmental Disabilities and World Health Organization. In addition, we performed manual searches for all articles selected at full-text screening through backward-and-forward citation tracking, with searches conducted up to mid-December 2024 (see Supplementary Table 1 for further details on the search strategy).
Eligibility criteria
We included studies if the following criteria applied: (a) included a systematic review of observational studies (cross-sectional, cohort, ecological studies); (b) summarised the prevalence of different mental disorders; and (c) were conducted in children and/or adults, the latter including people above the age of 65 years, unless otherwise specified, with intellectual disabilities of any aetiology.
Reviews that primarily investigated other populations (e.g. autistic people) were included if they presented studies in which at least 50% of the sample participants had an intellectual disability, and if they reported prevalence data for this group. We included genetic syndromes most frequently associated with a high (or near-complete) penetrance of intellectual disabilities, namely Down syndrome, fragile-X syndrome, Williams syndrome, 22q11.2 deletion syndrome and Prader–Willi syndrome, while excluding reviews that focused predominantly on either genetic investigations or rarer syndromic types.
Book chapters and textbooks were excluded unless these explicitly referred to systematic reviews; theses and conference abstracts with systematic searches were excluded; however, we searched for corresponding peer-reviewed, full-text publications for potential inclusion. We did not report prevalence estimates of ASD or attention-deficit hyperactivity disorder (ADHD) in people with intellectual disabilities when these conditions were presented as mental disorders in people with intellectual disabilities without providing further specific information on the co-occurrence of other mental disorders in people with both intellectual disabilities and another neurodevelopmental condition, such as ASD or ADHD.
Study selection
We searched six databases (inception to 17 October 2024) and carried out a manual search up to 15 December 2024. Articles retrieved from the database search were exported into EndNote 21 (for Windows; Clarivate Analytics, Philadelphia, PA, USA; https://endnote.com/) and, following de-duplication, two groups of reviewers (J.S., E.F., F.B.; and G.B., M.M.) independently screened titles and abstracts for full-text inclusion and conducted the final study selection. G.B. conducted the manual search on all studies included at the full-text screening stage through backward-and-forward citation tracking using Scopus. No language restriction was applied.
G.B. and M.M. independently assessed the eligibility of all studies retrieved through the database and manual searches. Any conflicts during any of the above evaluations were resolved by discussion with a senior author (J.S. or A.H.).
Data synthesis
Following discussion with an expert statistician (L.M.), and in accordance with Chapter V of the Cochrane Handbook for Systematic Reviews of Interventions, Reference Pollock, Becker, Pieper and Hartling18 we decided that presenting outcomes as reported in the included systematic reviews, without re-analysis or modification of the original analyses, was an appropriate approach in carrying out the umbrella review. A quantitative approach, Reference Fusar-Poli and Radua19 given the limited number of meta-analyses identified and substantial differences in terms of the included populations and mental disorders examined, would not have provided additional value beyond what was already highlighted in the original reviews. Instead, we conducted an overview of reviews to synthesise the current body of the evidence presented, consistent with the approach used in other umbrella reviews. Reference Hossain, Khan, Sultana, Ma, McKyer and Ahmed13,Reference Rydzewska, Dunn and Cooper14,Reference Ferraro, Cashin, Wand, Smart, Berryman and Marston20 We summarised the relevant findings both descriptively and in tabular form. We extracted and reported prevalence data and presented either meta-analyses or subgroup analyses for specific mental disorders stratified by age, sex and ASD or ADHD comorbidity, when available. We reported the main findings from systematic reviews that provided a quantitative synthesis of prevalence estimates, using data from the random-effects model when consistent with results from other approaches (e.g. quality-effects model or leave-one-out analysis), when applied. Prevalence estimates were reported with the same decimal precision as in the original reviews. We compared prevalence estimates for mental disorders with those in the general population (DSM-5-TR diagnoses) and organised them by specific diagnoses.
We distinguished between reviews primarily investigating autistic people with intellectual disabilities and those focusing on specific subgroups of people with intellectual disabilities (e.g. by setting, syndrome or level of intellectual disabilities) or specific diagnoses. For each systematic review with a narrative synthesis of results, we reported the range of prevalence estimates for each condition based on at least two relevant primary studies and described the characteristics of the original systematic review, considering only the primary studies relevant to our scope. For every primary study listed in these reviews, a mean IQ cut-off of ≤70 was applied to determine ascertainment of intellectual disabilities when the diagnosis was not otherwise specified.
Data extraction
Two reviewers (G.B. and M.M.) independently extracted data using a standardised form, with any disagreements resolved through discussion with a senior reviewer.
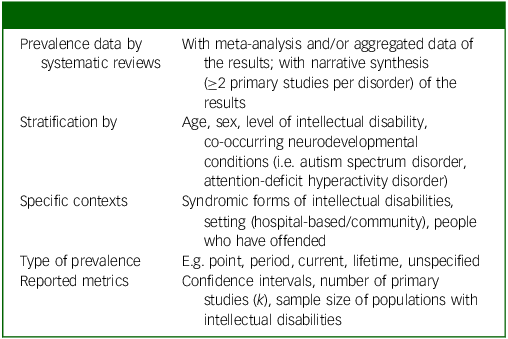
Data extraction included study design, year of publication, number of primary studies (k), corresponding author’s country, time frame, databases searched, total sample size and range of populations, population characteristics, assessment of mental comorbidity and key findings relevant to the review objectives, including the type of prevalence investigated. We reported information on N, age, level of intellectual disabilities and whether the considered population was predominantly male or female. Table 1 provides a concise overview of the extracted prevalence characteristics, summarising how prevalence data were reported across the included systematic reviews.
Overview of extracted prevalence characteristics

Quality appraisal
Two reviewers (G.B. and M.M.) independently assessed the overall reporting quality of all included reviews using ‘A Measurement Tool to Assess Systematic Reviews’ (AMSTAR-2), Reference Shea, Reeves, Wells, Thuku, Hamel and Moran21 resolving any discrepancies through consensus with a senior reviewer. AMSTAR-2 consists of 16 items, of which 7 (nos 2, 4, 7, 9, 11, 13 and 15) are identified as critical. Each of the items was given a rating of either ‘yes’, ‘partial yes’ or ‘no’, which contributes to confidence in the overall quality rating of each included systematic review. Reference Shea, Reeves, Wells, Thuku, Hamel and Moran21 We considered the critical weakness related to the absence of a preregistered protocol as not applicable to reviews published in or before 2011, i.e. prior to the introduction of PROSPERO.
Results
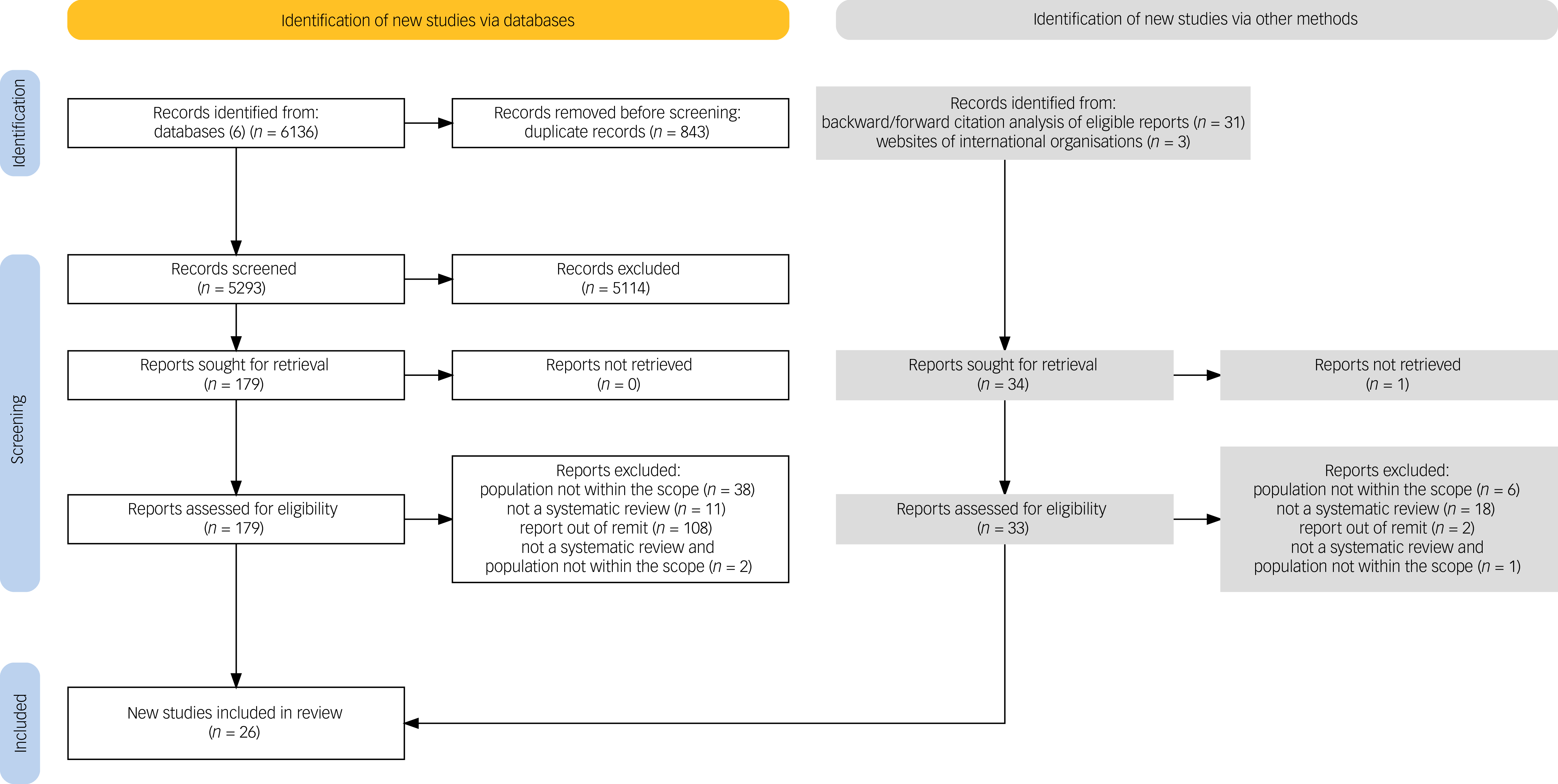
Figure 1 summarises the process of study identification. Following EndNote de-duplication, the database search yielded 5293 records for title and abstract screening of which 179 were included in full-text screening, and 20 reviews met eligibility criteria. The manual search resulted in 34 new reports, from which 1 full-text example was unavailable and 6 reviews were included. Supplementary Tables 5–8 present the lists of studies assessed at full-text screening, including those retained and those excluded, with corresponding reasons for the decision to include or exclude. Most of the excluded studies were either out of scope, not systematic reviews or involving non-relevant populations.
Study selection process.

Table S2 shows the main characteristics of the included systematic reviews, with Tables 2 and 3 reporting the main findings from systematic reviews including a meta-analysis or subgroup analysis, and from systematic reviews with a narrative synthesis of results, respectively.
Prevalence of mental disorders in people with intellectual disabilities: evidence from systematic reviews with meta-analyses or subgroup analyses

ID, intellectual disabilities; ASD, autism spectrum disorder; OCD, obsessive–compulsive disorder; AGO, agoraphobia; GAD, generalised anxiety disorder; SAD, separation anxiety disorder; SPHOBIA, specific phobia; SP, social phobia; PTSD, post-traumatic stress disorder.
a. Prevalence rate, 95% CI, N = population, k = number of primary studies relevant to intellectual disabilities in the included reviews.
b. According to the original review by Maïano et al, the combined prevalence estimates for anxiety disorders included estimates for OCD and PTSD.
c. For prevalence estimates calculated using the quality-effects model and leave-one-out analysis, please refer to the original systematic review by Edwards et al.
d. Prevalence estimates reported according to the random-effects model. For estimates based on the quality-effects model, please see the original review by Royston et al (supplementary materials). According to the original review by Royston et al, the combined prevalence estimates for anxiety disorders included those for OCD and PTSD.
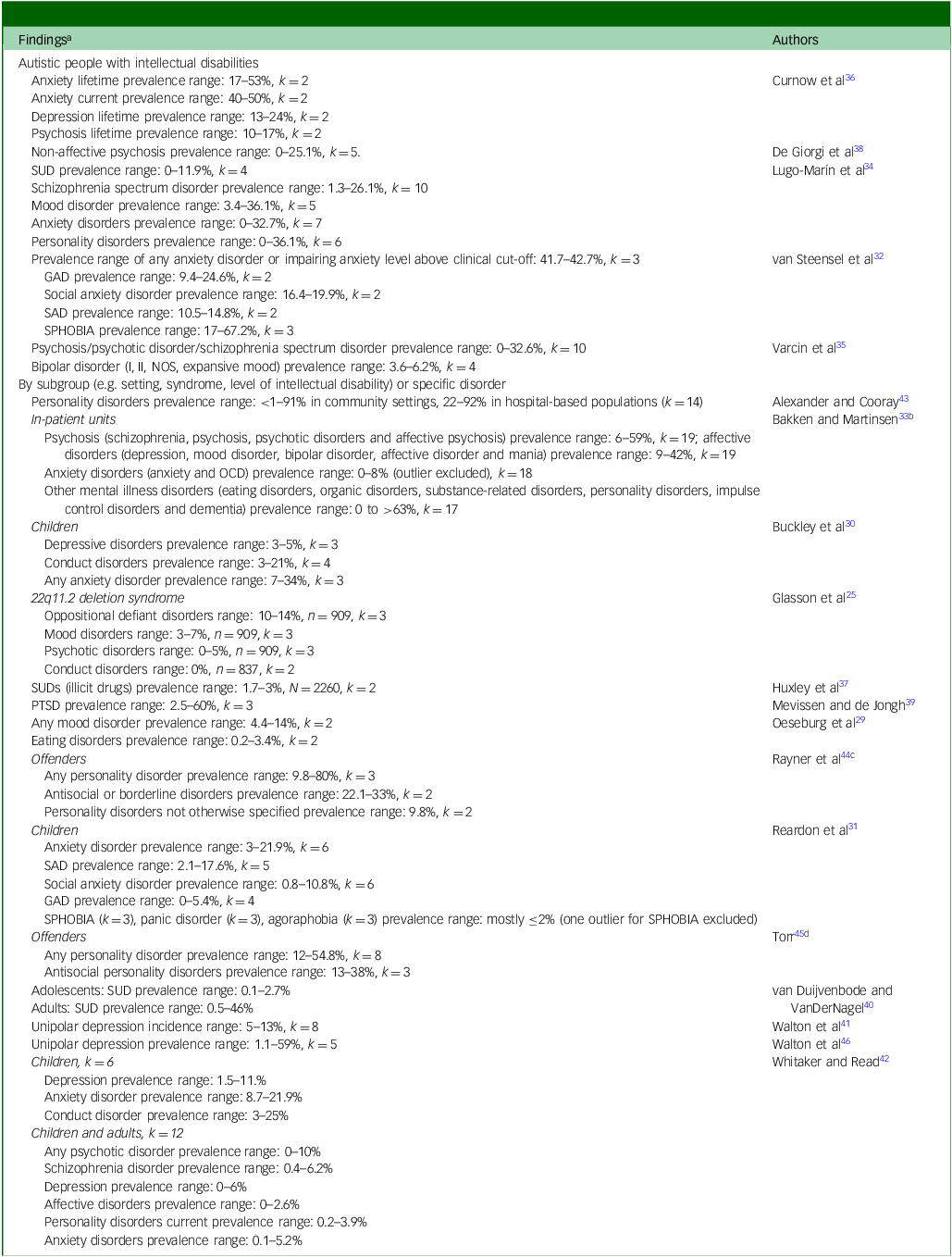
Prevalence of mental disorders in people with intellectual disabilities: evidence from narrative reviews

SUD, substance use disorder; GAD, generalised anxiety disorder; SAD, separation anxiety disorder; SPHOBIA, specific phobia; NOS, not otherwise specified; OCD, obsessive–compulsive disorder; PTSD, post-traumatic stress disorder.
a. k = number of primary studies relevant to intellectual disabilities included in the review.
b. Prevalence ranges were extracted from Table 1 of the original systematic review by Bakken et al.
c. The original review by Rayner et al included two studies that used overlapping data.
d. Prevalence ranges were extracted from Table 1 of the original systematic review by Torr et al.
Of the 26 reviews, 7 included a meta-analysis Reference Mazza, Rossetti, Crespi and Clerici7,Reference Aman, Naeem, Farooq and Ayub22–Reference Royston, Howlin, Waite and Oliver27 and 2 reported prevalence estimates based on either subgroup analyses or group comparisons. Reference Hollocks, Lerh, Magiati, Meiser-Stedman and Brugha28,Reference Oeseburg, Dijkstra, Groothoff, Reijneveld and Jansen29 These 9 reviews reported data on a total of 248 606 people with intellectual disabilities, Reference Mazza, Rossetti, Crespi and Clerici7,Reference Aman, Naeem, Farooq and Ayub22–Reference Oeseburg, Dijkstra, Groothoff, Reijneveld and Jansen29 including 15 221 with syndromic intellectual disabilities. Reference Edwards, Jones, Pearson, Royston, Oliver and Tarver24,Reference Glasson, Buckley, Chen, Leonard, Epstein and Skoss25,Reference Royston, Howlin, Waite and Oliver27 Systematic reviews with narrative results included a cumulative total of 238 636 people with intellectual disabilities. These figures represent the unadjusted sum of participants across included reviews, and may include overlapping primary studies.
Six systematic reviews focused on children/adolescents or youth up to age 22 years, Reference Glasson, Buckley, Chen, Leonard, Epstein and Skoss25,Reference Maïano, Coutu, Tracey, Bouchard, Lepage and Morin26,Reference Oeseburg, Dijkstra, Groothoff, Reijneveld and Jansen29–Reference van Steensel, Bögels and Perrin32 3 on adults, Reference Bakken and Martinsen33–Reference Varcin, Herniman, Lin, Chen, Perry and Pugh35 5 on adolescents/adults, Reference Mazza, Rossetti, Crespi and Clerici7,Reference Aman, Naeem, Farooq and Ayub22,Reference Hollocks, Lerh, Magiati, Meiser-Stedman and Brugha28,Reference Curnow, Rutherford, Maciver, Johnston, Prior and Boilson36,Reference Huxley, Martha, Y. and Hayhurst37 8 across all ages Reference Daveney, Angela, Cornelius, Faith and Sen23,Reference Edwards, Jones, Pearson, Royston, Oliver and Tarver24,Reference Royston, Howlin, Waite and Oliver27,Reference De Giorgi, De Crescenzo, D.Alò, Rizzo Pesci, Di Franco and Sandini38–Reference Whitaker and Read42 and 4 with limited or no age data. Reference Alexander and Cooray43–Reference Walton and Kerr46 Most of the studies included predominantly male participants, Reference Mazza, Rossetti, Crespi and Clerici7,Reference Aman, Naeem, Farooq and Ayub22,Reference Edwards, Jones, Pearson, Royston, Oliver and Tarver24–Reference Maïano, Coutu, Tracey, Bouchard, Lepage and Morin26,Reference Hollocks, Lerh, Magiati, Meiser-Stedman and Brugha28,Reference Buckley, Glasson, Chen, Epstein, Leonard and Skoss30,Reference Bakken and Martinsen33–Reference De Giorgi, De Crescenzo, D.Alò, Rizzo Pesci, Di Franco and Sandini38,Reference Torr45 with nine reporting limited or no sex-related information. Reference Oeseburg, Dijkstra, Groothoff, Reijneveld and Jansen29,Reference Reardon, Gray and Melvin31,Reference van Steensel, Bögels and Perrin32,Reference van Duijvenbode and VanDerNagel40–Reference Rayner, Wood, Beail and Nagra44,Reference Walton and Kerr46 Only three studies reported populations with an overall female predominance. Reference Daveney, Angela, Cornelius, Faith and Sen23,Reference Royston, Howlin, Waite and Oliver27,Reference Mevissen and de Jongh39
More detailed information on characteristics and diagnostic procedures was available in reviews that included meta-analyses. Most of the reviews reported multiple sites and the strategies of recruiting study participants, and included primary studies in which diagnoses of mental disorders were established through structured or semi-structured clinical interviews, based on international diagnostic criteria or other validated assessment tools. Reference Mazza, Rossetti, Crespi and Clerici7,Reference Aman, Naeem, Farooq and Ayub22–Reference van Steensel, Bögels and Perrin32,Reference Lugo-Marín, Magán-Maganto, Rivero-Santana, Cuellar-Pompa, Alviani and Jenaro-Rio34,Reference Varcin, Herniman, Lin, Chen, Perry and Pugh35,Reference Huxley, Martha, Y. and Hayhurst37,Reference Mevissen and de Jongh39,Reference Walton and Kerr41,Reference Whitaker and Read42,Reference Torr45,Reference Walton and Kerr46
Eleven reviews were conducted in the UK, Reference Daveney, Angela, Cornelius, Faith and Sen23,Reference Edwards, Jones, Pearson, Royston, Oliver and Tarver24,Reference Royston, Howlin, Waite and Oliver27,Reference Hollocks, Lerh, Magiati, Meiser-Stedman and Brugha28,Reference Curnow, Rutherford, Maciver, Johnston, Prior and Boilson36,Reference Huxley, Martha, Y. and Hayhurst37,Reference Walton and Kerr41–Reference Rayner, Wood, Beail and Nagra44,Reference Walton and Kerr46 five in Australia, Reference Glasson, Buckley, Chen, Leonard, Epstein and Skoss25,Reference Buckley, Glasson, Chen, Epstein, Leonard and Skoss30,Reference Reardon, Gray and Melvin31,Reference Varcin, Herniman, Lin, Chen, Perry and Pugh35,Reference Torr45 four in the Netherlands, Reference Oeseburg, Dijkstra, Groothoff, Reijneveld and Jansen29,Reference van Steensel, Bögels and Perrin32,Reference Mevissen and de Jongh39,Reference van Duijvenbode and VanDerNagel40 two in Canada, Reference Aman, Naeem, Farooq and Ayub22,Reference Maïano, Coutu, Tracey, Bouchard, Lepage and Morin26 two in Italy Reference Mazza, Rossetti, Crespi and Clerici7,Reference De Giorgi, De Crescenzo, D.Alò, Rizzo Pesci, Di Franco and Sandini38 and one each in Norway Reference Bakken and Martinsen33 and Spain. Reference Lugo-Marín, Magán-Maganto, Rivero-Santana, Cuellar-Pompa, Alviani and Jenaro-Rio34 Two reviews are included in Tables 2 and 3, because they reported meta-analyses or subgroup analyses alongside a narrative synthesis of prevalence data from individual studies on different mental disorders. Reference Glasson, Buckley, Chen, Leonard, Epstein and Skoss25,Reference Oeseburg, Dijkstra, Groothoff, Reijneveld and Jansen29
AMSTAR-2 ratings were critically low for 16 reviews, Reference Aman, Naeem, Farooq and Ayub22,Reference Daveney, Angela, Cornelius, Faith and Sen23,Reference Glasson, Buckley, Chen, Leonard, Epstein and Skoss25,Reference Hollocks, Lerh, Magiati, Meiser-Stedman and Brugha28,Reference Oeseburg, Dijkstra, Groothoff, Reijneveld and Jansen29,Reference Reardon, Gray and Melvin31,Reference Bakken and Martinsen33,Reference Huxley, Martha, Y. and Hayhurst37,Reference Mevissen and de Jongh39–Reference Walton and Kerr46 low for 9 Reference Mazza, Rossetti, Crespi and Clerici7,Reference Edwards, Jones, Pearson, Royston, Oliver and Tarver24,Reference Maïano, Coutu, Tracey, Bouchard, Lepage and Morin26,Reference Royston, Howlin, Waite and Oliver27,Reference Buckley, Glasson, Chen, Epstein, Leonard and Skoss30,Reference van Steensel, Bögels and Perrin32,Reference Lugo-Marín, Magán-Maganto, Rivero-Santana, Cuellar-Pompa, Alviani and Jenaro-Rio34,Reference Varcin, Herniman, Lin, Chen, Perry and Pugh35,Reference De Giorgi, De Crescenzo, D.Alò, Rizzo Pesci, Di Franco and Sandini38 and moderate for 1. Reference Curnow, Rutherford, Maciver, Johnston, Prior and Boilson36 Eighteen reviews used a quality assessment tool for the included primary studies. Reference Mazza, Rossetti, Crespi and Clerici7,Reference Aman, Naeem, Farooq and Ayub22–Reference Buckley, Glasson, Chen, Epstein, Leonard and Skoss30,Reference van Steensel, Bögels and Perrin32,Reference Lugo-Marín, Magán-Maganto, Rivero-Santana, Cuellar-Pompa, Alviani and Jenaro-Rio34–Reference De Giorgi, De Crescenzo, D.Alò, Rizzo Pesci, Di Franco and Sandini38,Reference Walton and Kerr41,Reference Walton and Kerr46 The most frequent critical weaknesses found were the absence of a pre-established review protocol and the lack of a list of excluded studies. Supplementary Tables 2–4 provide scoring details and a description of the AMSTAR-2 tool.
Mental disorders in people with intellectual disabilities
Schizophrenia spectrum and other psychotic disorders
In adolescents and adults with intellectual disabilities, Aman et al Reference Aman, Naeem, Farooq and Ayub22 reported a prevalence of 3.46% (95% CI: 2.51–4.42%) for all psychotic disorders in 140 189 participants (≥14 years, k = 25), slightly lower than Mazza et al, who reported 3.9% (95% CI: 0.8–16.8%, k = 8) for unspecified psychotic disorder in 20 885 participants (>12 years). Reference Mazza, Rossetti, Crespi and Clerici7
Aman et al found a 2.91% (95% CI: 1.38–4.44%) point prevalence, including 5 high-quality studies, for all psychotic disorders; 3.75% (95% CI: 2.63–4.78%, N = 2664, k = 11) point prevalence for psychosis; and 3.30% (95% CI: 2.02–4.59%, N = 136 538, k = 11) point prevalence in studies without a clear prevalence type. Reference Aman, Naeem, Farooq and Ayub22 Although these authors estimated a prevalence of 3.55% (95% CI: 2.66–4.44%, k = 17) for schizophrenia, Mazza et al highlighted a prevalence of schizophrenia of 4.8% (95% CI: 2.4–9.1%, k = 9) in 21 125 adolescents and adults with intellectual disabilities. Reference Mazza, Rossetti, Crespi and Clerici7,Reference Aman, Naeem, Farooq and Ayub22 With reference to sex, sensitivity analyses by Aman et al Reference Aman, Naeem, Farooq and Ayub22 showed the prevalence of psychosis as 3.78% (95% CI: 2.56–5%, N = 28 830) in males and 4.10% (95% CI: 2.86–5.35%, N = 22 907) in females (k = 9); and, by level of intellectual disabilities, a prevalence of psychosis of 5.55% (95% CI: 3.86–7.25%) in mild, 4.21% (95% CI: 2.56–5.86%) in moderate and 0.89% (95% CI: 0.15–1.62%) in severe intellectual disabilities (k = 7).
Systematic reviews with narrative results also addressed psychotic disorders in people with intellectual disabilities; Whitaker and Read reported a prevalence range of 0–10% for any psychotic disorder, and 0.4–6.2% for schizophrenia across the lifespan. Reference Whitaker and Read42
According to DSM-5-TR, 1 the lifetime prevalence of schizophrenia spectrum disorders in the general population is estimated at 0.3–0.7%.
Mood disorders
Mazza et al reported a prevalence of what they generally termed ‘mood disorders’ of 6.7% (95% CI: 5–8.8%, k = 12) in 9118 people with intellectual disabilities, Reference Mazza, Rossetti, Crespi and Clerici7 whereas Oeseburg et al reported a prevalence range of 4.4–14% (k = 2) for any mood disorder. Reference Oeseburg, Dijkstra, Groothoff, Reijneveld and Jansen29
In the general population, the 12-month prevalence of all mood disorders among adults was found to be 9.7%. 47
Depressive disorder
Maïano et al reported a prevalence of combined subtypes of depressive disorder of 2.8% in youth (<21 years) with intellectual disabilities (95% CI: 1.1–6.7%, N = 55 090, k = 10), 3.4% (95% CI: 1.5–7.4%, k = 3) for dysthymic disorder and 2.5% (95% CI: 1.2–5.4%, k = 4) for major depressive disorder. Reference Maïano, Coutu, Tracey, Bouchard, Lepage and Morin26
The same study reported a prevalence of depressive disorder in adolescents (12–22 years) with intellectual disabilities of 1.4% (95% CI: 0.4–5.1%, k = 3). Reference Maïano, Coutu, Tracey, Bouchard, Lepage and Morin26 By level of intellectual disability, the prevalence of depressive disorder was found to be 17.1% (95% CI: 8.4-31.8%, k = 2) in borderline intellectual functioning (BIF) and 9.4% (95% CI: 3.8–21.6%, k = 5) in mild, 3.5% (95% CI: 1.4–8.5%, k = 3) in moderate, 2.6% (95% CI: 0.6–10.3%, k = 3) in severe, 4% (95% CI: 0.6–25.6%, k = 2) in profound and 3.4% (95% CI: 0.7–15.2%, k = 2) in those with unspecified intellectual disabilities. Reference Maïano, Coutu, Tracey, Bouchard, Lepage and Morin26
Systematic reviews with narrative results reported variable prevalence rates of depression in children and adolescents with intellectual disabilities. Buckley et al found a prevalence range of 3–5% (k = 3). Reference Buckley, Glasson, Chen, Epstein, Leonard and Skoss30 Whitaker et al reported a range of 1.5–11% (N = 218 277, k = 6) Reference Whitaker and Read42 and, in a broader sample including both children and adults (k = 12), they reported a prevalence range of 0–6% for depression and 0–2.6% for affective disorders. Regarding cognitive level, Walton and Kerr found a unipolar depression prevalence range of 1.1–59% (k = 5, N = 542) in people with severe or profound intellectual disabilities. Reference Walton and Kerr46
Globally, according to WHO, depression affects 3.8% of the population, including 5.7% of adults >60 years; in the USA, the 12-month prevalence of major depressive disorder is about 7% (DSM-5-TR). 1,48
Bipolar disorder
We found no meta-analytic prevalence estimates of bipolar I and II disorder (BDI and BDII, respectively) in people with intellectual disabilities. Annual prevalence of BDI in the population without intellectual disabilities has been estimated at 0–0.6%, with the lifetime prevalence of BD II at around 0.3%. 1
Obsessive–compulsive disorder
Maïano et al reported the prevalence of obsessive–compulsive disorder (OCD) as 2.4% (95% CI: 0.8–7.2%, N = 1664, k = 6) in children/adolescents with intellectual disabilities, and as 12% (95% CI: 7.2–19.2%, k = 2) in adolescents with intellectual disabilities. Reference Maïano, Coutu, Tracey, Bouchard, Lepage and Morin26
By level of intellectual disabilities, Maïano et al reported the prevalence of OCD as 3.3% (95% CI: 0.5–20.3%, k = 2) in BIF, 2.5% (95% CI: 0.8–7.6%, k = 2) in mild and 1.6% (95% CI: 0.3–8.4%, k = 2) in moderate intellectual disabilities, but no data were available for other levels of intellectual disabilities. Reference Maïano, Coutu, Tracey, Bouchard, Lepage and Morin26
DSM-5-TR estimates a 12-month OCD prevalence of 1.1–1.8%, 1 consistent with a meta-analysis by Fawcett et al who reported the global prevalence of OCD as 1.1% (current), 0.8% (period) and 1.3% (lifetime). Reference Fawcett, Power and Fawcett49 Regarding the prevalence of OCD in children and adolescents, the review of Krebs and Heyman reported an estimated prevalence of between 0.25 and 4% (k = 3). Reference Krebs and Heyman50
Anxiety disorders
We found the combined prevalence of anxiety disorders to be 5.4% (95% CI: 2.5–11.5%, k = 18) among 57 774 children, adolescents and young adults with intellectual disabilities, and 5.5% (95% CI: 3.3–9%) among 4494 adolescents and adults (aged >12 years) with intellectual disabilities (k = 9). Reference Mazza, Rossetti, Crespi and Clerici7,Reference Maïano, Coutu, Tracey, Bouchard, Lepage and Morin26
In adults, Maïano et al reported prevalence estimates for specific anxiety disorders: agoraphobia 0.6% (95% CI: 0.1–3.6%, k = 2); panic disorder 0.3% (95% CI: 0.1–1.2%, k = 2); generalised anxiety disorder (GAD) 2.2% (95% CI: 0.5–9.1%, k = 5); separation anxiety disorder (SAD) 5% (95% CI: 1.8–13.3%, k = 4); social phobia 2.7% (95% CI: 1.2–5.8%, k = 5); and specific phobias (SPHOBIA) 11.5% (95% CI: 4–28.9%, k = 4). Reference Maïano, Coutu, Tracey, Bouchard, Lepage and Morin26
Among children aged 4–11 years, the overall prevalence of anxiety disorders was 1.2% (95% CI: 0.02–49.10%, N = 43 894, k = 3). For adolescents aged 12–21 years, the overall prevalence was 7.9% (95% CI: 0.6–54.6%, N = 44 079, k = 5), with GAD at 8.7% (95% CI: 2.4–27.1%, k = 2), social phobia at 5.4% (95% CI: 1.9–14.6%, k = 2) and SPHOBIA at 19.8% (95% CI: 11.8–31.3%, k = 2). Reference Maïano, Coutu, Tracey, Bouchard, Lepage and Morin26 Subgroup analyses by level of intellectual disabilities showed prevalence estimates of combined anxiety disorder of 3.3% (95% CI: 0.5–20.3%, k = 2) in youth aged 0–22 years with BIF, and 8.1% (95% CI: 5.2–12.3%, k = 4) in mild, 1.7% (95% CI: 0.4–6.7%, k = 2) in moderate and 3.5% (95% CI: 1.3–8.9%, k = 2) in severe intellectual disabilities. Reference Maïano, Coutu, Tracey, Bouchard, Lepage and Morin26
Oeseburg et al, in their sample of 1202 children and adolescents aged 0–21 years with intellectual disabilities, reported an overall prevalence of any anxiety disorder of 17.1% (95% CI: 15.1–19.4%, k = 3). Reference Oeseburg, Dijkstra, Groothoff, Reijneveld and Jansen29
Systematic reviews with narrative results reported wide variability in prevalence estimates of anxiety disorders in children and adolescents with intellectual disabilities. Buckley et al found a range of 7–34% (k = 3), Reference Buckley, Glasson, Chen, Epstein, Leonard and Skoss30 with Reardon et al reporting a prevalence of 3–21.9% for any anxiety disorder (N = 1801, k = 6), 2.1–17.6% (k = 5) for SAD, 0.8–10.8% (k = 6) for social anxiety disorder and 0–5.4% (k = 4) for GAD. Reference Reardon, Gray and Melvin31 Social phobia, panic disorder and agoraphobia were mostly <2% (each k = 3). Reference Reardon, Gray and Melvin31 Whitaker et al reported a prevalence of 8.7–21.9% (k = 6) in children and adolescents, and of 0.1–5.2% (k = 12) in mixed samples of children and adults. Reference Whitaker and Read42
Globally, anxiety disorders affect 4.05% of the population, Reference Javaid, Hashim, Hashim, Stip, Samad and Ahbabi51 with 31.1% of US adults experiencing any anxiety disorder during their lifetime, 52 whereas the cumulative incidence by 18 years is 7.85% in girls and 4.58% in boys. Reference Dalsgaard, Thorsteinsson, Trabjerg, Schullehner, Plana-Ripoll and Brikell53
Post-traumatic stress disorder
Mevissen and de Jongh reported post-traumatic stress disorder (PTSD) prevalence rates of 2.5–60% (k = 3) in 359 people with intellectual disabilities across the lifespan. Reference Mevissen and de Jongh39 These findings were later updated by Daveney et al, who reported a prevalence of 10% (95% CI: 0.4–19.5%, k = 4) in 1453 people with intellectual disabilities across the lifespan, with subgroup analyses by age showing PTSD prevalence at 8% (95% CI: –8 to 24%, N = 1333, k = 2) in adults and 12.95% (95% CI: –8.2 to 33%, N = 120, k = 2) in children and adolescents. Reference Daveney, Angela, Cornelius, Faith and Sen23 Maïano et al reported a PTSD prevalence of 1.1% (95% CI: 0.3–3.7%, k = 4) in children and adolescents with intellectual disabilities. Reference Maïano, Coutu, Tracey, Bouchard, Lepage and Morin26
Schincariol et al reported an overall PTSD prevalence of 23.95% (95% CI: 20.74–27.15%) in the general population. Reference Schincariol, Orrù, Otgaar, Sartori and Scarpazza54 National lifetime estimates of PTSD vary considerably across country-income groups and WHO regions, but averaged 3.9% overall. Reference Koenen, Ratanatharathorn, Ng, McLaughlin, Bromet and Stein55
Personality disorders, disruptive, impulse-control and conduct disorder
One review estimated the prevalence of personality disorders of 2.8% (95% CI: 1.2–6.8%, N = 3949, k = 5) in adolescents and adults with intellectual disabilities. Reference Mazza, Rossetti, Crespi and Clerici7 Regarding specific disorders in children and adolescents (<19 years), Oeseburg et al reported the prevalence of conduct disorder at 5.1% (95% CI: 4.1–6.4%, N = 1535, k = 5), and at 12.4% (95% CI: 10.7–14.4%, N = 1202, k = 3) for oppositional defiant disorder. Reference Oeseburg, Dijkstra, Groothoff, Reijneveld and Jansen29
Systematic reviews with narrative results also reported on conduct disorder in children and adolescents with intellectual disabilities: Buckley et al found a prevalence range of 3–21% (k = 4), Reference Buckley, Glasson, Chen, Epstein, Leonard and Skoss30 and Whitaker et al of 3–25% (k = 6), Reference Whitaker and Read42 whereas for personality disorder in people with intellectual disabilities, Whitaker et al reported a prevalence range of 0.2–3.9% (k = 12) in mixed samples of children and adults. Reference Whitaker and Read42
In Western countries, the prevalence of any personality disorder in the general population is about 12%, Reference Volkert, Gablonski and Rabung56 whereas the 1-year prevalence estimates for conduct disorder in high-income countries range from 2% to over 10%, with a median of 4%. 1
Other mental disorders (eating and substance-use disorders)
No reviews reported meta-analyses for these mental disorders in people with intellectual disabilities; however, systematic reviews with narrative results have highlighted the following findings. Huxley et al reported a prevalence range of substance-use disorder (SUD) for illicit drugs at 1.7–3% in 2260 people with intellectual disabilities (k = 2), Reference Huxley, Martha, Y. and Hayhurst37 and van Duijvenbode and VanDerNagel found a prevalence of SUD at 0.1–2.7% in adolescents, and 0.5–46% in adults, with mild intellectual disabilities, and in BIF. Reference van Duijvenbode and VanDerNagel40 Oeseburg et al reported the prevalence range for eating disorders at 0.2–3.4% (k = 2). Reference Oeseburg, Dijkstra, Groothoff, Reijneveld and Jansen29
Compared with the general population, the lifetime and 12-month prevalence of eating disorders have been estimated at 0.91 and 0.43%, respectively. Reference Qian, Wu, Liu, Zhu, Jin and Zhang57 Global epidemiological estimates indicate that substance-use disorders affect approximately 2.2% of the world’s population, with alcohol-use disorders accounting for the largest proportion. Reference Castaldelli-Maia and Bhugra58
Mental disorders in syndromic intellectual disabilities
Down syndrome
Edwards et al included 11 studies involving 2152 people with Down syndrome. They reported a prevalence of 8% (95% CI: 4–13%, k = 11) for any anxiety disorder, and 4% (95% CI: 0–9%, k = 4) for SPHOBIA/phobic anxiety, in 933 participants. The same sample showed a 2% (95% CI: 0–4%, k = 4) prevalence for OCD and 6% (95% CI: 2–10%, k = 2) prevalence for selective mutism in 155 people with Down syndrome. Reference Edwards, Jones, Pearson, Royston, Oliver and Tarver24 Walton and Kerr reported a prevalence of unipolar depression ranging 5–13% (k = 8) in 1928 people with Down syndrome across the lifespan (aged 6–78 years). Reference Walton and Kerr41
Fragile-X syndrome
Edwards et al reported a prevalence of any anxiety disorder (including PTSD) of 49% (95% CI: 39–60%, k = 19) in 3882 people with fragile-X syndrome across the lifespan, and of 43% (95% CI: 23–62%, k = 7) in 1214 male participants. Reference Edwards, Jones, Pearson, Royston, Oliver and Tarver24 Consistent with these findings, Glasson et al reported a prevalence of any anxiety disorder of 42% (95% CI: 35–48%, k = 2) in 107 children. Reference Glasson, Buckley, Chen, Leonard, Epstein and Skoss25
Regarding specific anxiety disorder in fragile-X syndrome, Edwards et al reported the following prevalence estimates: SPHOBIA, 52% (95% CI: 38–67%, k = 2); social anxiety, 28% (95% CI: 16–41%, k = 7); GAD, 14% (95% CI: 5–22%, k = 5); SAD, 13% (95% CI: 7–19%, k = 5); panic disorder with agoraphobia, 27% (95% CI: 12–65%, k = 2); and OCD, 16% (95% CI: 2–30%, k = 4). Reference Edwards, Jones, Pearson, Royston, Oliver and Tarver24
Williams syndrome
Glasson et al reported a prevalence of any anxiety disorder of 46% (95% CI: 35–58%, k = 2) in 75 children and adolescents. Reference Glasson, Buckley, Chen, Leonard, Epstein and Skoss25 Royston et al reported a prevalence of any anxiety disorder of 48% (95% CI: 30–67%, k = 7) in 391 people with Williams syndrome and mild intellectual disabilities; SPHOBIA of 40% (95% CI: 27–54%, k = 9); GAD of 11% (95% CI: 5–19%; k = 7); SAD of 7% (95 CI: 2–15%, k = 6); social anxiety disorder of 1% (95% CI: 0–3%, k = 6); panic disorder of 2% (95% CI: 1–4%, k = 6); PTSD of 2% (95% CI: 0–4%, k = 4); agoraphobia of 2% (95% CI: 0–5%, k = 3); and OCD of 4% (95% CI: 2–6%, k = 7). Reference Royston, Howlin, Waite and Oliver27 Prevalence estimates using the random-effects analytic model were similar to those derived from the quality-effects model, Reference Royston, Howlin, Waite and Oliver27 and PTSD and OCD were included in the overall estimate of anxiety disorders.
22q11.2 deletion syndrome
For any anxiety disorder in 22q11.2 deletion syndrome, Edwards et al estimated a prevalence of 38% (95% CI: 32–45%, N = 2272, k = 34) across the lifespan, equal to that of any anxiety disorder reported by Glasson et al (38%, 95% CI: 27–50%, k = 3) in 909 children/adolescents (6–17 years). Reference Edwards, Jones, Pearson, Royston, Oliver and Tarver24,Reference Glasson, Buckley, Chen, Leonard, Epstein and Skoss25
For specific anxiety disorder, Edwards et al reported a prevalence estimate of 28% (95% CI: 21–35%, k = 18) for SPHOBIA; 9% (95% CI: 7–11%, k = 15) for social anxiety/social phobia; 13% (95% CI: 10–16%, k = 17) for GAD; 6% (95% CI: 4–8%, k = 14) for SAD; 9% (95% CI: 7–12%, k = 21) for OCD; 1% (95% CI: 0–2%, k = 4) for panic disorder; 2% (95% CI: 0–3%, k = 3) for agoraphobia; and 2% (95% CI: 1–3%, k = 6) for PTSD. Reference Edwards, Jones, Pearson, Royston, Oliver and Tarver24
Glasson et al reported, in a sample of 909 people with 22q11.2 deletion syndrome, a prevalence range of oppositional defiant disorder of 10–14%, mood disorder 3–7% and psychotic disorder 0–5% (k = 3). No conduct disorder was detected in a sample of 837 people with 22q11.2 deletion syndrome (k = 2). Reference Glasson, Buckley, Chen, Leonard, Epstein and Skoss25
Prader–Willi syndrome
No reviews of prevalence estimation of specific mental disorders in people with Prader–Willi syndrome were identified.
Mental disorders in autistic people with intellectual disabilities
Although no meta-analyses specifically addressed the co-occurrence of intellectual disabilities and ASD, 8791 autistic people with intellectual disabilities were included in 6 reviews primarily investigating people with ASD. Reference Hollocks, Lerh, Magiati, Meiser-Stedman and Brugha28,Reference van Steensel, Bögels and Perrin32,Reference Lugo-Marín, Magán-Maganto, Rivero-Santana, Cuellar-Pompa, Alviani and Jenaro-Rio34–Reference Curnow, Rutherford, Maciver, Johnston, Prior and Boilson36,Reference De Giorgi, De Crescenzo, D.Alò, Rizzo Pesci, Di Franco and Sandini38
Hollocks et al conducted a subgroup analysis, reporting a lower prevalence of current depression in autistic people with intellectual disabilities compared with those without intellectual disabilities (14% [95% CI: 5–28%, N = 512, k = 6] versus 26% [95% CI: 20–32%, N = 1413, k = 16]). Reference Hollocks, Lerh, Magiati, Meiser-Stedman and Brugha28 In the same study, the prevalence of any anxiety disorder was 20% (95% CI: 7–39%, N = 394, k = 6) in autistic people with intellectual disabilities versus 24% (95% CI: 19–43%, N = 1050, k = 7) in those without intellectual disabilities, whereas the prevalence of OCD was 24% (95% CI: 14–36%, N = 177, k = 3) and 20% (95% CI: 10–34%, N = 970, k = 7), respectively. The authors tested subgroup differences using meta-regression analyses, finding a significant difference for depression but not for anxiety or OCD (meta-regression coefficient for depression, β = 0.12, p = 0.03; not reported for anxiety and OCD). Reference Hollocks, Lerh, Magiati, Meiser-Stedman and Brugha28
Regarding psychosis, Varcin et al identified a prevalence of any psychotic disorder at 0–32.6% (k = 10) in 1107 autistic adults with intellectual disabilities, Reference Varcin, Herniman, Lin, Chen, Perry and Pugh35 and De Giorgi et al reported non-affective psychosis prevalence range at 0–25.1% (k = 5) in 359 autistic people with intellectual disabilities across the lifespan. Reference De Giorgi, De Crescenzo, D.Alò, Rizzo Pesci, Di Franco and Sandini38 Curnow et al reported a lifetime prevalence of psychosis of 10–17% (k = 2) in 4208 autistic adolescents and adults with intellectual disabilities. Reference Curnow, Rutherford, Maciver, Johnston, Prior and Boilson36 Lugo-Marín et al Reference Lugo-Marín, Magán-Maganto, Rivero-Santana, Cuellar-Pompa, Alviani and Jenaro-Rio34 reported prevalence estimates for schizophrenia spectrum disorders of 1.3–26.1% (k = 10) in autistic adults with intellectual disabilities.
Mood disorders ranged from 3.4 to 36.1% (k = 5) in autistic adults with intellectual disabilities, Reference Lugo-Marín, Magán-Maganto, Rivero-Santana, Cuellar-Pompa, Alviani and Jenaro-Rio34 with Varcin et al finding rates of bipolar disorder or manic episodes of 3.6–6.2% (k = 4) in 437 autistic adults with intellectual disabilities. Reference Varcin, Herniman, Lin, Chen, Perry and Pugh35
Curnow et al reported a lifetime prevalence of depression of 13–24% (k = 2) in autistic adolescents and adults with intellectual disabilities. Reference Curnow, Rutherford, Maciver, Johnston, Prior and Boilson36
Regarding anxiety disorders, Curnow et al described a lifetime prevalence range of 17–53% and a current prevalence range of 40–50% in autistic adolescents and adults with intellectual disabilities (k = 2). Reference Curnow, Rutherford, Maciver, Johnston, Prior and Boilson36 Higher estimates, at 41.7–42.7% (k = 3), for any anxiety or impairing anxiety level were shown by van Steensel et al in autistic children and adolescents with intellectual disabilities, Reference van Steensel, Bögels and Perrin32 and Lugo-Marín et al identified an anxiety disorder prevalence range of 0–32.7% (k = 7) in autistic adults with intellectual disabilities. Reference Lugo-Marín, Magán-Maganto, Rivero-Santana, Cuellar-Pompa, Alviani and Jenaro-Rio34
Regarding specific anxiety disorders, van Steensel et al reported a prevalence range of GAD at 9.4–24.6% (k = 2), social anxiety disorder at 16.4–19.9% (k = 2), SAD at 10.5–14.8% (k = 2) and SPHOBIA at 17–67.2% (k = 3) in a population of 369 autistic children and adolescents with intellectual disabilities. Reference van Steensel, Bögels and Perrin32
Lugo-Marín et al reported a prevalence range for personality disorder at 0–36.1% (k = 6), and for SUD at 0–11.9% (k = 4), among autistic adults with intellectual disabilities. Reference Lugo-Marín, Magán-Maganto, Rivero-Santana, Cuellar-Pompa, Alviani and Jenaro-Rio34
Mental disorders in offenders
Regarding offenders with intellectual disabilities, Rayner et al described a prevalence range of 9.8–80% (k = 3) for any personality disorder, 22.1–33% (k = 2) for antisocial or borderline personality disorder and 9.8% (k = 2) for personality disorder not otherwise specified, in a population of 372 offenders with intellectual disabilities. Reference Rayner, Wood, Beail and Nagra44 Torr found a prevalence range for any personality disorder of 12–54.8% (k = 8), and 13–38% (k = 3) for antisocial personality disorder, Reference Torr45 in 769 offenders with intellectual disabilities.
Mental disorders by setting
Regarding specific settings, Bakken and Martinsen examined the characteristics and mental disorder diagnoses of 3996 adults with intellectual disabilities admitted to in-patient units. Reference Bakken and Martinsen33 The prevalence range reported for psychotic disorders ranged 6–59% (k = 19); for affective disorders (including depression, mood disorder, bipolar disorder, affective disorder and mania) 9–42% (k = 19); for anxiety disorders (including anxiety and OCD) 0–8%, excluding one outlier (k = 18); and for other mental disorders (e.g. eating disorders, organic disorders, substance-related disorders, personality disorders, impulse-control disorders and dementias) 0–63% (k = 17). Reference Bakken and Martinsen33
Alexander and Cooray examined the published literature on the diagnosis of personality disorders in intellectual disabilities, reporting a prevalence range of <1–91% in community settings and 22–92% in hospital-based populations (k = 14). Reference Alexander and Cooray43
Discussion
Prevalence of mental disorders in people with intellectual disabilities
Compared with the general population, people with intellectual disabilities appeared to have higher prevalence estimates for both schizophrenia spectrum disorders (with estimates over six times higher) and OCD (nearly double, especially in children and adolescents). Anxiety disorders also appeared more frequent, although estimates varied by age. Compared with the general population, mood disorders appeared to be less prevalent, as were PTSD and personality disorders, possibly reflecting underdiagnosis. Reference Scheirs, Muller, Manders and van der Zanden59,Reference Arnold, Huang, Srasuebkul, Cvejic, Michalski and Trollor60
In syndromic intellectual disabilities, meta- or subgroup analyses were available only for anxiety disorders, including subtypes including social phobia, GAD, panic disorder, PTSD and OCD. Anxiety disorders were mostly associated with the phenotypes of fragile-X syndrome, Williams syndrome and 22q11.2 deletion syndrome, but not of Down syndrome.
Our umbrella review indicated that ASD, ADHD and intellectual disabilities are often studied as separate conditions, with only one review conducting subgroup analysis comparing autistic adults with and without intellectual disabilities. Reference Hollocks, Lerh, Magiati, Meiser-Stedman and Brugha28
The small number of meta-analyses that stratified data by intellectual disability severity or sex suggested higher rates of psychosis, OCD, anxiety and depression in mild intellectual disabilities, and a slightly higher prevalence of psychosis in females than males.
Findings in context
Several structural and methodological challenges hinder the accurate identification of mental disorders in people with intellectual disabilities. These include the limited availability of screening and diagnostic tools specifically designed or adapted for this population, Reference Bertelli, Bianco, Prasher, Davidson and Santos61,Reference Flynn, Vereenooghe, Hastings, Adams, Cooper and Gore62 coupled with diagnostic overshadowing, Reference DellArmo and Tassé63 whereby a mental disorder/symptom is attributed to intellectual disabilities. Variability in the quality and accessibility of mental health services across countries Reference Maulik, Lakhan, Kishore, Sahu, Bertelli, Sagar, Bertelli, Deb, Munir, Hassiotis and Salvador-Carulla4,Reference Hassiotis64 also plays a role. For example, people with BIF often lack access to intellectual disabilities services because eligibility criteria vary by region, hindering appropriate identification and care. These factors are likely to bias prevalence estimates, particularly in studies relying on clinical diagnoses rather than epidemiological investigations. Reference Bradford, Meyer, Khan, Giardina and Singh65,Reference Dattani66
Additional challenges arise from the debate as to whether mental disorders may manifest as ‘behavioural equivalents’, or whether such behavioural changes should never, or only rarely, be considered as expressions of psychopathology, Reference Eaton, Tarver, Shirazi, Pearson, Walker and Bird67,Reference Painter, Hastings, Ingham, Trevithick and Roy68 especially in people with severe/profound intellectual disabilities and communication difficulties. Reference Bakken69 This may help explain the higher reported rates of mental disorders in people with mild intellectual disabilities compared with those with more severe intellectual disabilities, in which diagnosis may not be possible to establish.
Underdiagnosis remains largely unaddressed, because most studies and reviews did not consider bias from the inconsistent application of diagnostic criteria. Although some reviews included primary studies using adapted criteria alongside DSM and/or ICD diagnoses, none reported prevalence data separately by diagnostic system versus adapted criteria, limiting the evaluation of their impact. Peña-Salazar et al identified previously undiagnosed mental disorders in 29.6% of participants with intellectual disabilities, with major depressive and anxiety disorders being the most prevalent. Reference Peña-Salazar, Arrufat, Santos, Fontanet, González-Castro and Más70 Deb et al, using routinely collected data, similarly reported an increase in diagnosed mental disorders, from 15.7 to 17.3%, over 12 years in adults in the Czech Republic with intellectual disabilities. Reference Deb, Jarkovský, Melicharová, Holub, Limbu and Třešňák71
Mood and depressive disorders illustrate how these challenges contribute to under-recognition or misdiagnosis in people with intellectual disabilities. Symptoms such as labile mood or irritability may be misinterpreted as behaviours that challenge, or as psychosis. They may also go unrecognised due to a lack of adapted diagnostic criteria, or because people with intellectual disabilities may be unable to self-report core depressive features, including depressed mood or loss of interest and pleasure lasting at least 2 weeks. Reference Maulik, Lakhan, Kishore, Sahu, Bertelli, Sagar, Bertelli, Deb, Munir, Hassiotis and Salvador-Carulla4,Reference Bertelli, Bianco, Prasher, Davidson and Santos61–Reference Hassiotis64,Reference Eaton, Tarver, Shirazi, Pearson, Walker and Bird67–Reference Bakken69 Our umbrella review reported a 2.8% prevalence estimate for depressive disorders in youth with intellectual disabilities, Reference Maïano, Coutu, Tracey, Bouchard, Lepage and Morin26 and 6.7% for any mood disorder, Reference Mazza, Rossetti, Crespi and Clerici7 contrasting with recent primary studies Reference Scheirs, Muller, Manders and van der Zanden59,Reference Arnold, Huang, Srasuebkul, Cvejic, Michalski and Trollor60,Reference Peña-Salazar, Arrufat, Santos, Fontanet, González-Castro and Más70 that suggest higher rates of depression. When adapted criteria are used, 13.7% may represent the lower limit of actual prevalence. Reference Scheirs, Muller, Manders and van der Zanden59
In this umbrella review we included only studies reporting diagnoses of mental disorders, excluding those addressing mental health symptoms alone, because diagnoses offer greater specificity and comparability. Although symptoms are observable indicators, they do not in themselves confirm a mental disorder. Reference Stein, Phillips, Bolton, Fulford, Sadler and Kendler72 However, this is not the only approach to understanding mental health presentations in this population. For example, most of the literature on SUD examined patterns of use and misuse alongside formal diagnoses, Reference Huxley, Martha, Y. and Hayhurst37,Reference van Duijvenbode and VanDerNagel40 illustrating the broad spectrum of substance-related behaviours seen in people with intellectual disabilities, which, although it captures clinically relevant phenomena, does not provide information about the number of people requiring some form of intervention.
Strengths and limitations
The umbrella review approach has enabled the identification of cross-cutting methodological limitations that recur across disorder categories (e.g. heterogeneity in diagnostic criteria over time, limited availability of intellectual disabilities-adapted assessment tools and barriers to diagnostic recognition), and highlights systematic evidence gaps such as the scarcity of primary studies and reviews for certain disorders, and the limited reporting of stratified prevalence estimates. The high-level synthesis of evidence is essential to inform clinical awareness, guide research priorities and support tailored interventions for this underserved population, which are not achievable within single-study/disorder systematic reviews, ultimately leading to improved diagnosis and service planning. Therefore, our umbrella review provides an overarching evidence map and clearer interpretative boundaries for what can and cannot be concluded about psychiatric prevalence in people with intellectual disabilities.
This is the first umbrella review, to our knowledge, to synthesise evidence across a wide range of mental disorders in diverse populations of people with intellectual disabilities (with or without co-occurring ASD), and to facilitate comparison with prevalence data from the general population, where available. It also offers a comprehensive overview of the literature, including stratification by age, sex, level of intellectual disabilities, syndromic forms and specific subgroups such as offenders or in-patients, thereby enabling a broader understanding of comorbidity patterns in this population. By integration of findings across multiple systematic reviews, this umbrella review also highlights consistent evidence gaps, such as the limited availability of stratified prevalence data or the scarcity of primary studies for several disorders, that are not always evident at the level of individual reviews. However, umbrella reviews also have limitations. These include reliance on the methodological quality of the included reviews; the potential omission of new or pre-existing primary studies not included in reviews; methodological difficulties in handling heterogeneity; and overlapping data. Reference Choi and Kang73 Because we did not extract or analyse primary-level data in the included reviews, we were unable to investigate or address such overlap, and we therefore report these only as a potential limitation of the underlying evidence base rather than a feature that we could formally evaluate.
According to AMSTAR-2 ratings, only one included review was rated as being of ‘moderate’ quality, Reference Curnow, Rutherford, Maciver, Johnston, Prior and Boilson36 with the remainder rated either ‘low’ or critically ‘low’. To support the correct interpretation of the results, we report each original review’s AMSTAR-2 score (Table S2), provide confidence intervals when available and include general population prevalence estimates for comparison. The predominance of low or critically low methodological quality among the included reviews reduces the level of certainty that can be placed in their prevalence estimates, and must be taken into account when interpreting our results. Consequently, any patterns or comparisons identified in our synthesis should be understood as broad indications rather than precise epidemiological estimates, within the methodological boundaries inherent in an umbrella-review design.
Other well-known limitations inherent in the primary studies are likely to include definitions of intellectual disabilities and whether diagnostic criteria or clinical opinion were used. For example, Mazza et al used the category ‘mood disorder’, including both bipolar and depressive disorders, Reference Mazza, Rossetti, Crespi and Clerici7 whereas diagnostic reclassifications (e.g. PTSD and OCD are not included in anxiety disorders in DSM-5) affected how some reviews grouped these conditions.
Variations in the time frames of prevalence reporting time (e.g. point, period or lifetime) may limit the comparability of prevalence rates between the general population and people with intellectual disabilities. Most reviews included a higher proportion of males, which partly reflects the demographic distribution of people with intellectual disabilities. However, the potential for sex-specific differences has rarely been considered, limiting the generalisability and nuance of prevalence estimates.
Finally, our findings may also inform the debate on the relative risk contribution of intellectual disabilities to the onset of specific mental disorders; for example, our findings suggest that rates of depression in people with intellectual disabilities are lower than expected. Reference Scheirs, Muller, Manders and van der Zanden59 However, investigating these associations is beyond the scope of our review, and caution is warranted when interpreting the findings because the estimates were often based on few reviews or small samples, which restricts their generalisability.
Clinical and policy implications
On the whole, people with intellectual disabilities are at increased risk of developing comorbidities with mental disorders. Reliable, stratified prevalence estimates (e.g. by age, sex or level of intellectual disabilities) can support accurate diagnosis and personalised care, guide service planning, inform the development of targeted interventions (e.g. for people with psychosis) and address currently unmet needs at individual, family and systems levels.
Future research and gaps in the literature
High-quality systematic reviews and meta-analyses are lacking for several mental disorders in intellectual disabilities, including bipolar disorder (and rapid cycling), eating disorders, SUD and dementia, whether of syndromic or non-syndromic origin.
Evidence also remains limited for other disorders, including PTSD, specific anxiety disorders and personality disorders beyond antisocial/borderline types. Stratified prevalence data by sex, age, level of intellectual disabilities and co-occurring neurodevelopmental conditions (e.g. ASD, ADHD, tic disorders) are still scarce. However, reviews by Lugo-Marín et al and Varcin et al identified multiple primary studies on various mental disorders in autistic people with intellectual disabilities, indicating that future meta-analyses may be achievable. Ecological studies are also needed to capture the cultural and contextual variation of mental ill health, Reference Leibenluft, Allen, Althoff, Brotman, Burke and Carlson74 as is clinical research into improving diagnostic sensitivity to reduce underdiagnosis, together with validated tools adapted for people with intellectual disabilities. Reference Moss, Bertelli, Bertelli, Deb, Munir, Hassiotis and Salvador-Carulla75 New measures are emerging, such as SPAID-G, Reference Bertelli, Scuticchio, Ferrandi, Lassi, Mango and Ciavatta76 which, combined with clinical evaluation, show promise in diagnosing mental disorders in people with intellectual disabilities.
Addressing these gaps is crucial to advancing our understanding of mental disorders in people with intellectual disabilities, and to improving their mental healthcare. Future research should prioritise high-quality systematic reviews and meta-analyses, alongside studies that explore underrepresented conditions and sociodemographic factors. By doing so, we can work towards more accurate prevalence estimates, culturally sensitive diagnostic frameworks and tailored interventions that better meet the diverse needs of this population.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjo.2026.11036
Data availability
Data availability is not applicable to this article because no new data were created or analysed in this study.
Acknowledgements
The authors thank Drs Chiara Ossola, Maria Sole Zanetti and Sofia Bosco for generously providing translation support on a voluntary basis. The authors also thank Drs Laura Colombo and Annalisa Bardelli, from the Bibliographic Services of the University of Milano-Bicocca, for their valuable support in developing and refining the search strategy. The authors thank Professor Muhammad Ayub for his inspiring insights, which helped shape the early ideas of this work. The authors made use of DeepL, ChatGPT and Google Translate to assist with the inclusion and assessment of non-English primary studies. Fluent French- and Spanish-speakers checked two full-text screenings and the data retrieved in these languages.
Author contributions
A.H., C.B., G.B., J.S., M.B. and M.C. conceptualised the study. D.P., E.F., F.B., G.B., M.M. and J.S. curated the data. A.H., G.B., J.S., L.M. and M.M. performed the formal analysis. A.H., D.P., G.B., J.S., L.M. and M.M. contributed to the methodology. A.H. and J.S. supervised the project. G.B. and M.M. contributed to writing – original draft. A.H., G.B., J.S., L.M., M.M. and S.R. contributed to writing – review and editing. All authors contributed to data interpretation, critically revised the manuscript for important intellectual content and approved the final version. G.B and J.S. contributed equally to this work and are joint first authors.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
A.H. is a member of the International Editorial Board of British Journal of Psychiatry Open. She was not involved in the peer review or editorial decision-making process for this manuscript. All other authors have no interests to declare.




 Open access
Open access
eLetters
No eLetters have been published for this article.