


Introduction
Suicide remains a significant global public health concern, with over 727,000 deaths reported annually, according to the World Health Organization [1]. It is currently the 15th leading cause of death worldwide and the second leading cause among individuals aged 15–29 years [2]. In Spain, recent data from the National Institute of Statistics (INE) indicate a concerning upward trend in suicide mortality, highlighting the urgent need for evidence-based prevention strategies to reduce this burden [3].
Suicidal behaviour is a complex, multifactorial phenomenon influenced by biological, psychological, social, and environmental factors [Reference Knipe, Padmanathan, Newton-Howes, Chan and Kapur4]. Among the most critical predictors of suicide are previous attempts: it is estimated that for every completed suicide, there are approximately 25 attempts [5]. Previous attempts are among the strongest predictors of suicide: for every death by suicide, there are estimated 25 attempts [5], and approximately one in five individuals admitted to an emergency department following a suicide attempt will reattempt within a short period, emphasizing the need for targeted interventions aimed at preventing recurrence [Reference de la Torre-Luque, Pemau, Ayad-Ahmed, Borges, Fernandez-Sevillano and Garrido-Torres6].
Effective suicide prevention requires robust, population-based registries that can guide the design and implementation of tailored intervention programmes. Cohort studies play a crucial role in this context, enabling researchers to identify high-risk populations and track suicidal behaviour over time [Reference Kapur, Cooper, King-Hele, Webb, Lawlor and Rodway7]. Understanding the baseline characteristics of individuals who attempt suicide – and how these factors relate to the likelihood of reattempt – is essential for developing precise, evidence-informed prevention efforts [Reference Olfson, Wall, Wang, Crystal, Gerhard and Blanco8].
Over the past two decades, several international cohorts have investigated suicidal behaviour, differing in inclusion criteria, sample size, geographic scope, follow-up duration, and data collection methods [Reference Kapur, Cooper, King-Hele, Webb, Lawlor and Rodway7, Reference Park, Lee, Lee, Moon, Jeon and Shim9–Reference dos Santos Machado, Ballester, Cao, Mwangi, Caldieraro and Kapczinski13]. Despite methodological variability, consistent patterns have emerged: a predominance of female participants – particularly in younger samples – high psychiatric comorbidity (notably mood, anxiety, and personality disorders), frequent prior suicide attempts, and elevated rates of alcohol misuse [Reference Kapur, Cooper, King-Hele, Webb, Lawlor and Rodway7, Reference Park, Lee, Lee, Moon, Jeon and Shim9, Reference Irigoyen-Otiñano, Llorca-Bofí, Adrados-Pérez, Arenas-Pijoan, Nicolau-Subires and Albert-Porcar12, Reference Machado, Ballester, Cao, Mwangi, Caldieraro and Kapczinski14, Reference Wiktorsson, Marlow, Runeson, Skoog and Waern15]. Self-poisoning has been identified as the most frequent method of attempted suicide across various countries and healthcare settings [Reference Carroll, Metcalfe and Gunnell16]. Participants are often unemployed, single, or living alone, and report low educational attainment or socioeconomic status [Reference Kapur, Cooper, King-Hele, Webb, Lawlor and Rodway7, Reference Wiktorsson, Marlow, Runeson, Skoog and Waern15].
In Spain, no cohort has yet included participants across broad age ranges and multiple catchment areas nationwide using standardized clinical assessments. [Reference Kapur, Cooper, King-Hele, Webb, Lawlor and Rodway7, Reference Irigoyen-Otiñano, Llorca-Bofí, Adrados-Pérez, Arenas-Pijoan, Nicolau-Subires and Albert-Porcar12, Reference Machado, Ballester, Cao, Mwangi, Caldieraro and Kapczinski14]In response to this gap, the SURVIVE cohort study was established to examine the sociodemographic and mental health factors associated with suicide attempt recurrence in a nationally representative sample. Participants aged 12 years and older who present to one of eight participating emergency departments across Spain following a suicide attempt are recruited and followed annually. The primary aims of the SURVIVE cohort are to: (1) describe the sociodemographic and clinical characteristics of individuals presenting with suicide-related behaviours in Spain; (2) collect longitudinal data to identify factors associated with suicide attempt recurrence over time; and (3) evaluate the effectiveness of targeted psychosocial interventions in reducing suicidal behaviour within 12 months of the index attempt. This article presents the baseline sociodemographic and clinical characteristics of the SURVIVE cohort participants at the time of their index suicide attempt.
Methods
Study design
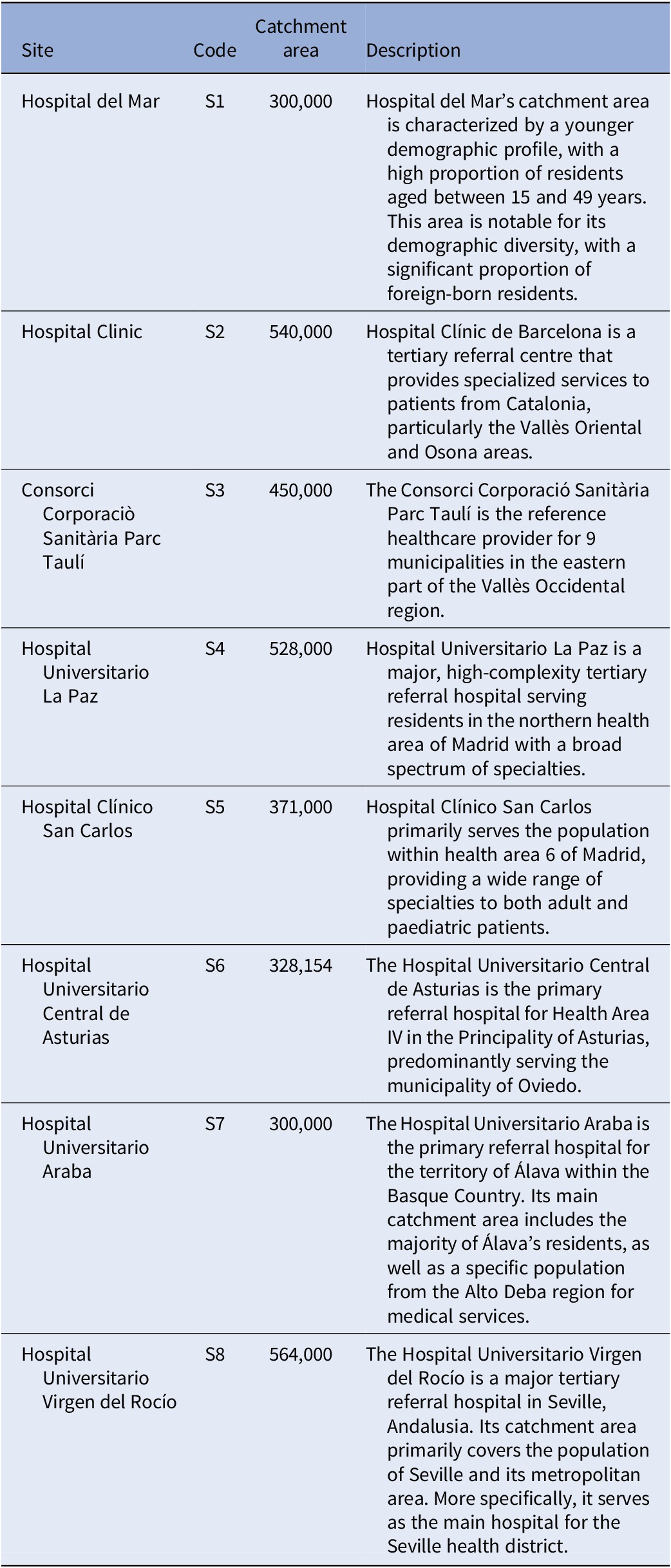
The Suicide Prevention and Intervention Study (SURVIVE) project is a collaboration between eight hospital services providing emergency care in the cities of Barcelona (Catalonia), Madrid (Autonomous Community of Madrid), Oviedo (Principado de Asturias), Seville (Andalusia), and Vitoria (Basque Country) in Spain. Recruitment locations included general hospitals with specialized psychiatric services and a dedicated psychiatric ward. A detailed account of service provision is given in Table 1. At each participating site, the ethics committee approved the study. Informed consent was obtained from all participants before any study-related procedures were conducted.
Site descriptions and catchment area coverage

Participants
Participants were recruited between November 2020 and March 2023. Those who agreed to participate were scheduled for the assessment within 15 days of the index suicide attempt, which was conducted at the outpatient clinics of the same facility. In some cases, participants were admitted for inpatient treatment after the emergency evaluation; these assessments were performed either during the inpatient stay or shortly after discharge, always within the 15-day window. Inclusion criteria for both samples (i.e., adolescents and adults) comprise a suicide attempt (understood as a self-injurious act committed with at least some intent to die [Reference Posner, Brent, Lucas, Gould, Stanley and Brown17]) within the last 15 days, the ability to complete questionnaires and interviews, and having given informed consent. A clinician evaluated the participants to determine eligibility based on the study’s inclusion criteria and obtained their consent to be approached by a SURVIVE research assistant.
Measures
A structured form was used to collect participants’ information, including age, sex, educational level, employment, and marital status, number of children, country of origin, religion, pharmacological treatment, family history of suicide, substances (drugs/alcohol) used before the attempt, and the method of the attempt.
When adolescent- and adult-specific versions of questionnaires were available (e.g., Mini-International Neuropsychiatric Interview (MINI), PHQ-9), the corresponding versions were administered. To reduce assessment burden, a subset of key self-report instruments was selected for each subsample.
The presence of psychiatric disorders was determined using the MINI for adults [Reference Sheehan, Janavs, Baker, Harnett-Sheehan, Knapp and Sheehan18] and MINI for children and adolescents (MINI-KID) [Reference Sheehan, Sheehan, Shytle, Janavs, Bannon and Rogers19]. Suicidality was assessed using the Columbia-Suicide Severity Rating Scale (C-SSRS) [Reference Posner, Brown, Stanley, Brent, Yershova and Oquendo20, Reference Al-Halabí, Sáiz, Burón, Garrido, Benabarre and Jiménez21]. Participants were assessed for suicidal ideation and behaviour throughout their lifetime and during the 15 days preceding the index attempt.
A battery of self-reported measures was also administered in both adolescents and adults, including the following: (i) The Patient Health Questionnaire (PHQ-9) [Reference Kroenke, Spitzer and Williams22, Reference Diez-Quevedo, Rangil, Sanchez-Planell, Kroenke and Spitzer23] was used to assess the severity of depressive symptoms experienced over the past 2 weeks; (ii) The Barratt Impulsiveness Scale (BIS-11) [Reference Patton, Stanford and Barratt24, Reference Martínez-Loredo, Fernández-Hermida, Fernández-Artamendi, Carballo and García-Rodríguez25] was used to assess impulsivity traits; (iii) The Childhood Trauma Questionnaire-Short Form (CTQ-SF) [Reference Bernstein, Stein, Newcomb, Walker, Pogge and Ahluvalia26, Reference García-Fernández, Martínez-Cao, Sánchez-Fernández-Quejo, Bobes-Bascarán, Andreo-Jover and Ayad-Ahmed27] was used to assess the exposure to childhood maltreatment, comprising five sub-scales (emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect), and (iv) The EuroQoL – 5 Dimensions – 5 Levels (EQ-5D-5L) [Reference Hernandez, Garin, Pardo, Vilagut, Pont and Suárez28] was used to assess quality of life, which includes five dimensions (mobility, self-care, daily activities, pain/discomfort, and anxiety/depression). A visual analogue scale (VAS) was also used to assess overall health perception, ranging from 0 (worst imaginable health) to 100 (best imaginable health).
Furthermore, the following self-report scales were utilized exclusively in the adult sub-sample: (i) The Generalized Anxiety Disorder scale (GAD-7) [Reference Spitzer, Kroenke, Williams and Löwe29] was used to assess anxiety symptoms; (ii) The Brief Symptom Inventory (BSI) [Reference Derogatis and Melisaratos30] was used to evaluate a global index of psychopathological symptoms; (iii) The Acquired Capability for Suicide Scale-Fearlessness About Death (ACSS-FAD) [Reference Ribeiro, Witte, Van Orden, Selby, Gordon and Bender31] was used to measure fearlessness about death and pain tolerance; and (iv) The Reflective Functioning Questionnaire (RFQ-8) [Reference Ruiz-Parra, Manzano-García, Mediavilla, Rodríguez-Vega, Lahera and Moreno-Pérez32] was used to measure capacities for hypo-mentalizing (uncertainty about mental states) and hyper-mentalizing (certainty about mental states).
In the adolescent sub-sample, the Strengths and Difficulties Questionnaire (SDQ) [Reference Goodman33, Reference Ortuño-Sierra, Sebastián-Enesco, Pérez-Albéniz, Lucas-Molina and Fonseca-Pedrero34] was used to evaluate behavioural and emotional difficulties using five subscales (emotional problems, conduct problems, and hyperactivity/inattention).
Data analyses
The sociodemographic and clinical characteristics of cohort participants were obtained using descriptive statistics. For continuous variables, the Mann–Whitney U test was applied when normality assumptions were not met. For categorical variables, Pearson’s chi-square (χ2) test was used. Post hoc analyses were carried out using corrected standardized residuals to identify which cells in the contingency tables significantly contributed to the overall chi-square statistic [Reference Beasley and Schumacher35].
Results
Cohort’s sociodemographic and clinical profile
Between November 2020 and March 2023, a total of 1,730 participants were included in the cohort.
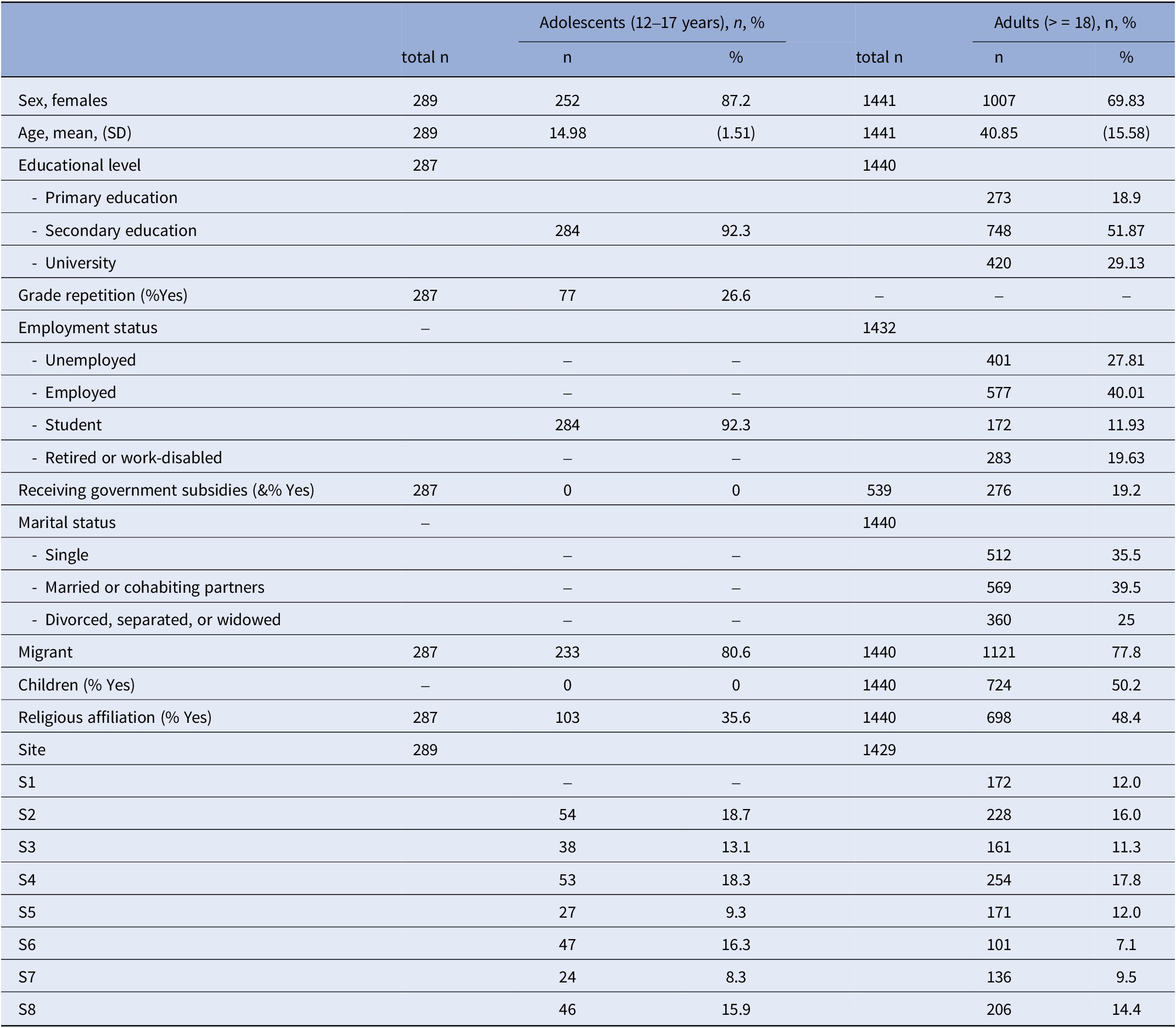
The adolescent sample comprised 289 participants recruited across seven sites (site S1 does not provide mental health care for adolescents, and therefore, did not participate in recruitment). Most sites each contributed between 13 and 19% of the adolescent sample, while two sites (S5 and S7) recruited fewer than 10% of participants. Adolescents included in the cohort were predominantly female (87.2%), with a mean age of 15 years (SD = 1.51). All participants were enrolled in secondary education, and 26.6% had repeated a grade. Migrant status was reported by 19.4, and 35.6% reported religious affiliation (see Supplemenatry Table 1).
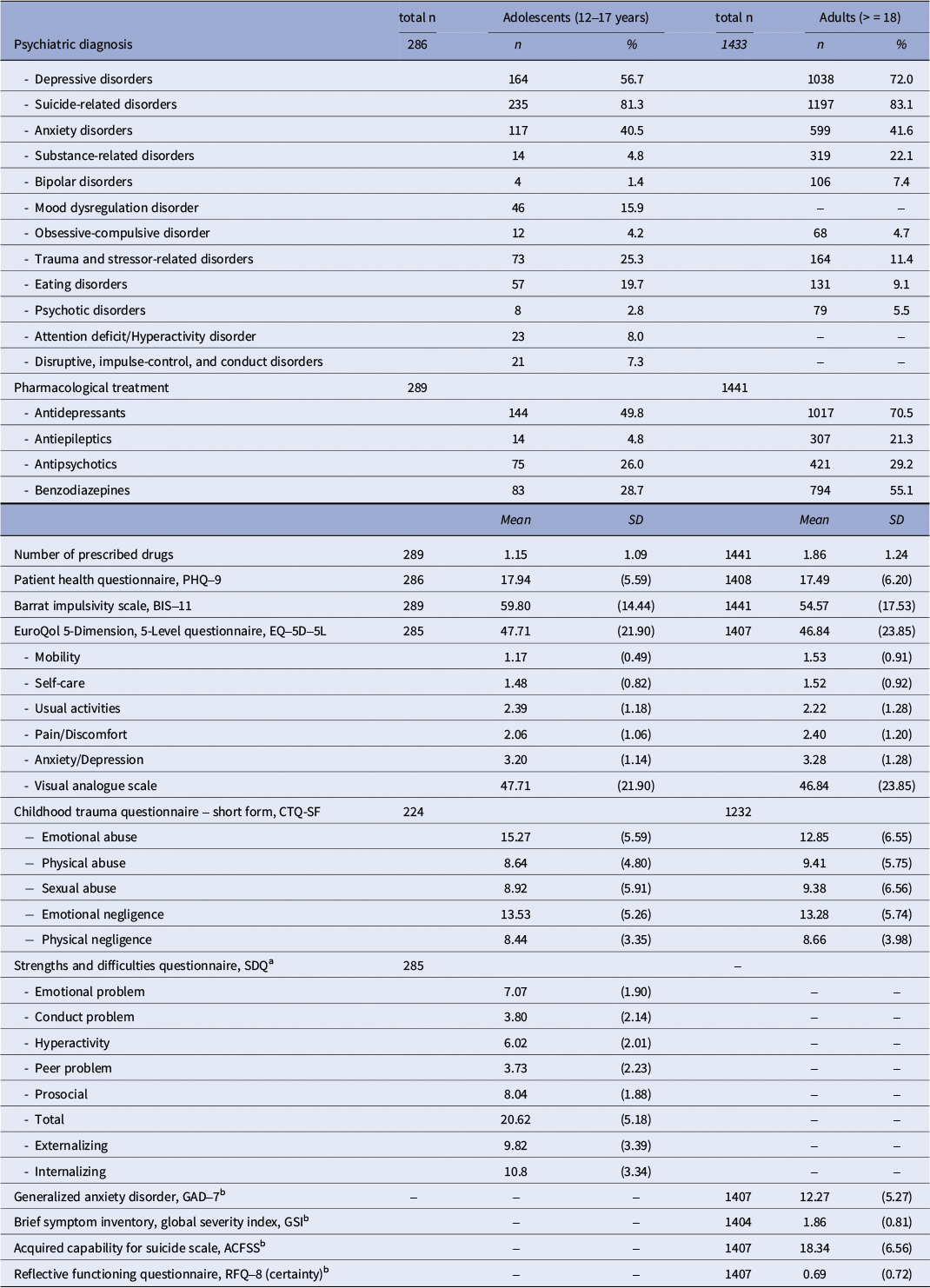
Among adolescents, suicide-related disorders were most prevalent (81.3%), followed by depressive (56.7%) and anxiety disorders (40.5%). Trauma- and stressor-related disorders (25.3%) and eating disorders (19.7%) were also frequent. Substance-related (4.8%) and bipolar disorders (1.4%) were infrequent. Antidepressants were prescribed to 49.8%, benzodiazepines to 28.7%, antipsychotics to 26.0%, and antiepileptics to 4.8%. Participants averaged 1.15 medications (SD = 1.09, range = 0–4).
Self-reported symptoms among adolescents included a mean PHQ-9 score of 17.94 (SD = 5.59) and a BIS-11 score of 59.80 (SD = 14.44). The SDQ revealed elevated scores in emotional symptoms, conduct problems, hyperactivity, and peer difficulties, with a total difficulties score of 20.62 (SD = 5.18). High scores in emotional abuse (mean = 15.27, SD = 5.59) and emotional neglect (mean = 13.53, SD = 5.26) were reported.
The adult group included 1441 participants. Recruitment took place across eight sites. Most sites contributed between 11% and 18% of the total sample, while two sites recruited fewer than 10% of participants.
70% of the adult sample were females, with ages ranging from 18 to 93 years (mean = 41, SD = 15.58). Over half (51.9%) had completed secondary education. Employment status: 40.1% employed, 27% unemployed, and 19.6% unable to work due to disability, receiving benefits, or retirement. Approximately one-third of adults reported being single (35%), while 39.5% were married or living with a partner. The remaining participants were divorced, separated, or widowed. Additionally, 50.2% of adults reported having children. Religious affiliation and migrant status were reported by 48.4 and 22.2% respectively.
In the adult sample, suicide-related (83.1%) and depressive disorders (72.0%) were the most common. Anxiety disorders were reported by 41.6% of adults, substance-related disorders by 22.1%, and bipolar disorders by 7.4%. Antidepressants were prescribed to 70.5%, benzodiazepines to 55.1%, antipsychotics to 29.2%, and antiepileptics to 21.3%. The mean number of medications was 1.86 (SD = 1.24, range = 0–5).
Adults reported a PHQ-9 mean score of 17.49 (SD = 6.20) and a BIS-11 score of 54.57 (SD = 17.53). The EQ-5D scores reflected poor quality of life, with anxiety/depression (M = 3.28, SD = 1.28) and pain/discomfort most affected (mean = 2.40, SD = 1.20). Emotional abuse and neglect emerged with the highest scores in the childhood trauma reports.
In summary, females were more prevalent in both adolescents and adults. Adults showed higher frequencies of depressive and substance-related disorders and greater use of psychotropic medication, whereas adolescents presented higher rates of eating and trauma- and stressor-related disorders. Across self-report measures, both groups displayed comparable levels of depressive symptoms, impulsivity, and functional impairment. Tables 2 and 3 present the sociodemographic and clinical characteristics of adolescents and adults in the SURVIVE cohort.
Baseline demographic characteristics by age and distribution across recruitment sites

Note: SD,Standard Deviation. S1 = Hospital del Mar; S2 = Hospital Clinic; S3 = Consorci Corporaciò Sanitària Parc Taulí; S4 = Hospital Universitario La Paz; S5 = Hospital Clínico San Carlos; S6 = Hospital Universitario Central de Asturias; S7 = Hospital Universitario Araba; S8 = Hospital Universitario Virgen del Rocío.
Baseline clinical characteristics by age groups

Note: aThis questionnaire was administered only to the adolescent group (12–17 years). bThese questionnaires were administered only to the adult group (≥18 years).
Characteristics of the index suicide attempt
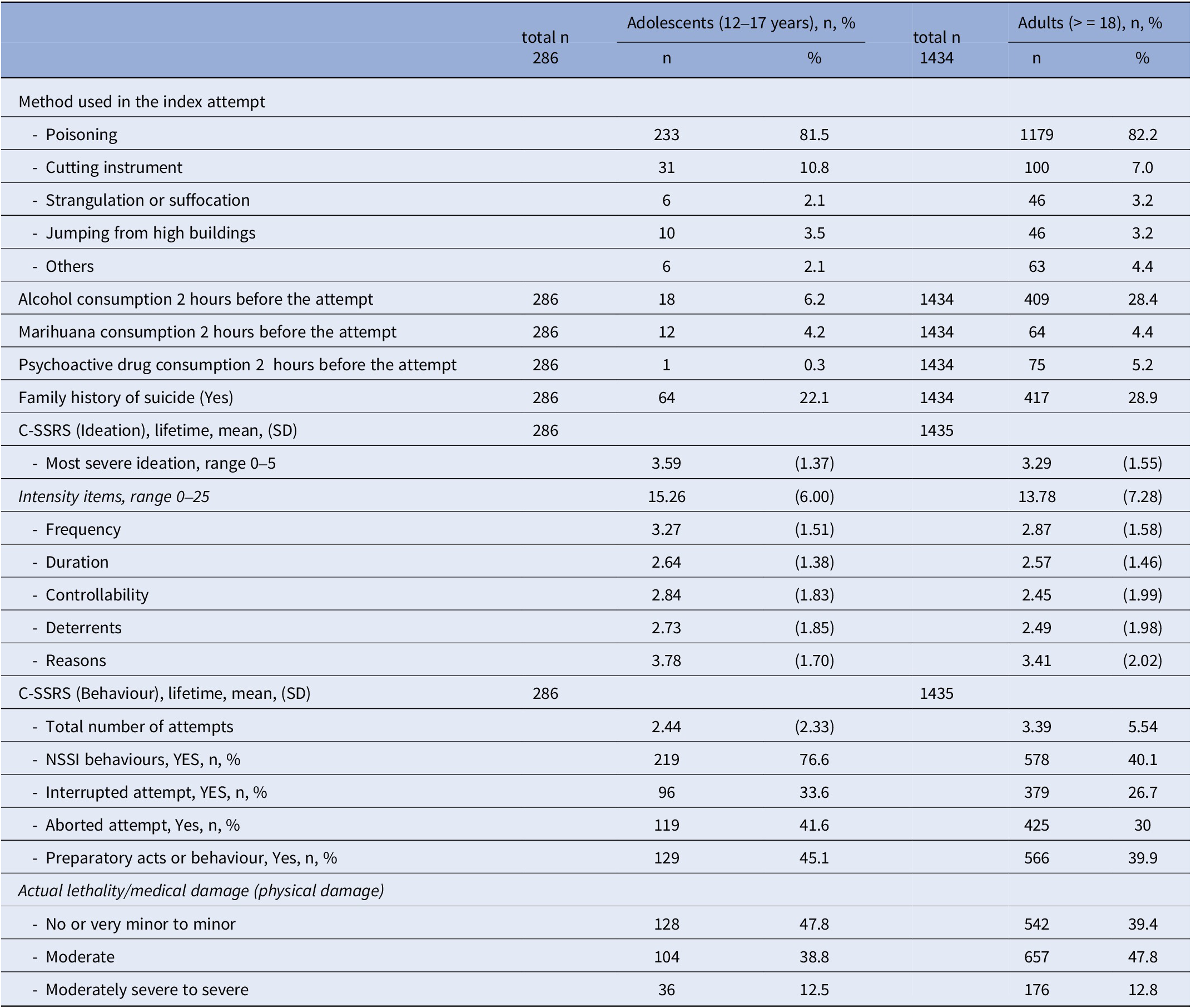
Poisoning was the most common method in adolescents (81.5%), followed by cutting (10.8%), jumping (3.5%), and strangulation or suffocation (2.1%). Only 6.2% reported alcohol use before the attempt, with low rates of marijuana (4.2%) and psychoactive drug use (0.3%). A family history of suicide was reported by 22.1% of adolescent participants.
Suicidal ideation was severe, with a mean score of 3.59 (SD = 1.37) on the C-SSRS and a mean intensity score of 15.26 (SD = 6.00). The average number of lifetime suicide attempts was 2.44 (SD = 2.33). Non-suicidal self-injury (NSSI) was highly prevalent (76.6%), and preparatory behaviours were also common: 33.6% had experienced interrupted attempts, 41.6% aborted attempts, and 45.1% engaged in preparatory actions. Regarding medical consequences, 12.5% of adolescents experienced moderately severe to severe medical damage.
Among adults, self-poisoning was also the predominant method (82.2%), followed by cutting (7.0%), jumping (3.2%), and strangulation or suffocation (3.2%). Pre-attempt substance use was more common in this group: 28.4% reported alcohol use, 4.4% marijuana, and 5.2% psychoactive drugs. A family history of suicide was reported by 28.9% of adult participants. C-SSRS scores showed a slightly lower severity of suicidal ideation in adults (mean = 3.29, SD = 1.55; intensity = 13.78, SD = 7.28). Adults reported a higher mean number of previous suicide attempts (mean = 3.3, SD = 5.54). NSSI was reported by 40.1% of adults. Interrupted, aborted, and preparatory behaviours were reported by 26.7, 30.0, and 39.9% respectively. Regarding lethality, 12.8% of adults experienced moderate to severe physical harm during the index attempt Table 4.
Characteristics of the index suicide attempt by age groups

Abbreviations: SD, standard deviation; C-SSRS, columbia suicide severity rating scale.
Discussion
This study provides a comprehensive overview of the baseline characteristics of individuals presenting with a suicide attempt to emergency departments across eight hospitals in five Spanish regions. To our knowledge, it represents the largest multicentre, naturalistic cohort study on suicidal behaviour in Spain to date, and one of the few international studies that includes both adolescents and adults starting from the age of 12.
This finding is consistent with previous research [Reference Kapur, Cooper, King-Hele, Webb, Lawlor and Rodway7, Reference Mehanović, Rosso, Cuomo, Diecidue, Maina and Costa10, Reference Irigoyen-Otiñano, Llorca-Bofí, Adrados-Pérez, Arenas-Pijoan, Nicolau-Subires and Albert-Porcar12] and meta-analytic data [Reference Miranda-Mendizabal, Castellví, Parés-Badell, Alayo, Almenara and Alonso36]showing that females, particularly adolescents and young adults, have nearly twice the risk of suicide attempts compared to males. Several hypotheses have been proposed to explain this difference, including gender-specific risk factors and differences in suicide stigma and help-seeking behaviours [Reference Miranda-Mendizabal, Castellví, Parés-Badell, Alayo, Almenara and Alonso36, Reference Calear, Batterham and Christensen37]. The mean age among adults is consistent with similar findings in Spanish and international cohorts [Reference Irigoyen-Otiñano, Llorca-Bofí, Adrados-Pérez, Arenas-Pijoan, Nicolau-Subires and Albert-Porcar12, Reference Wei, Liu, Zhang, Wang, Chu and Jia38]. Educational attainment was modest, with nearly half of the adult sample having completed secondary education, and employment rates were relatively high compared to other cohorts [Reference Kapur, Cooper, King-Hele, Webb, Lawlor and Rodway7, Reference Irigoyen-Otiñano, Llorca-Bofí, Adrados-Pérez, Arenas-Pijoan, Nicolau-Subires and Albert-Porcar12]. Approximately 20% of adults were receiving state benefits, a proportion similar to Kapur’s study [Reference Kapur, Cooper, King-Hele, Webb, Lawlor and Rodway7].
Religious affiliation, a variable rarely reported in previous studies, was identified in over a third of adolescents and nearly half of adults. This finding invites further exploration, as prior research (e.g., MONSUE cohort [Reference Carli, Mandelli, Zaninotto, Iosue, Hadlaczky and Wasserman39]) has suggested that religious affiliation may exert a protective influence against more lethal suicidal behaviours.
Migration status emerged as a key factor, with about one in five participants across both age groups identified as migrants. This is comparable to data from the prior cohort studies [Reference Mehanović, Rosso, Cuomo, Diecidue, Maina and Costa10, Reference Carli, Mandelli, Zaninotto, Iosue, Hadlaczky and Wasserman39] and reinforces concerns raised in the literature about increased suicide risk and reduced access to psychiatric care in migrant populations [Reference Lipsicas, Mäkinen, Wasserman, Apter, Bobes and Kerkhof40]. Given its potential relevance, a systematic assessment of migration status in suicide research and clinical care is warranted.
Psychiatric disorders were prevalent in both age groups, predominantly depressive and anxiety disorders, confirming trends reported in other cohorts [Reference Barakat, Brunelin, Abrial, Neige, Chalancon and Scholl11, Reference Irigoyen-Otiñano, Llorca-Bofí, Adrados-Pérez, Arenas-Pijoan, Nicolau-Subires and Albert-Porcar12, Reference Machado, Ballester, Cao, Mwangi, Caldieraro and Kapczinski14]. Trauma- and stressor-related disorders and eating disorders were more frequent in adolescents, while substance use disorders were more common in adults. Unfortunately, we did not collect data on personality disorders – particularly borderline personality disorder – which are known to be strongly associated with suicidal behaviour in youth and adults [Reference Machado, Ballester, Cao, Mwangi, Caldieraro and Kapczinski14].
Self-reported symptom scores, including measures of depression, impulsivity, and quality of life, were in line with prior studies [Reference Park, Lee, Lee, Moon, Jeon and Shim9, Reference Barakat, Brunelin, Abrial, Neige, Chalancon and Scholl11] and confirmed clinically significant psychological distress in both age groups. Like other studies [Reference Barakat, Brunelin, Abrial, Neige, Chalancon and Scholl11, Reference Andreo-Jover, Curto Ramos, Bobes, Bravo-Ortiz, Cebria and Crespo-Facorro41], we found a high prevalence of childhood trauma, with higher rates of moderate- severe emotional abuse in the adult sample than in the adolescent sample (68% vs. 47% respectively). Childhood trauma has been linked to suicide risk both directly and indirectly [Reference Pompili, Erbuto, Innamorati, Luciano, Sampogna and Abbate-Daga42]. Further analyses will help clarify the specific contribution of childhood trauma to the risk of suicide reattempt in this population.
Psychotropic medication use was high, with both groups receiving, on average, between 1.5 and 1.7 drugs. Antidepressants were the most frequently prescribed class, as in the study by [Reference Mehanović, Rosso, Cuomo, Diecidue, Maina and Costa10], followed by benzodiazepines and antipsychotics. Of note, very few previous cohort studies provide clear and detailed data on prescribed psychotropics, preventing comparisons across samples.
The most common method of suicide attempt was poisoning in both adolescents and adults, consistent with global patterns [Reference Carroll, Metcalfe and Gunnell16]. Alcohol and psychoactive substance use before the attempt was more common among adults. Adolescents reported higher levels of suicidal ideation severity and intensity, as assessed by the C-SSRS.
The level of medical damage associated with the index attempt showed that 12–13% of participants in both age groups experienced moderately severe to severe physical consequences, indicating a substantial subgroup at high lethality risk. This aligns with findings from [Reference Irigoyen-Otiñano, Llorca-Bofí, Adrados-Pérez, Arenas-Pijoan, Nicolau-Subires and Albert-Porcar12] and underlines the importance of considering physical injury severity when assessing suicide risk and planning aftercare.
Participants also reported multiple prior suicide attempts and a high frequency of behavioural indicators of suicide risk, such as aborted, interrupted, and preparatory acts. These behaviours – more commonly reported among adolescents – highlight the chronicity and seriousness of suicidal behaviour in this population and are aligned with risk models such as the C-SSRS framework.
Nearly one in four adolescents and almost a third of adults reported a family history of suicide. This adds to existing evidence that familial and genetic vulnerabilities may contribute to suicidal behaviour and suggests the importance of routine assessment of family history during suicide risk evaluations [Reference Runeson and Åsberg43].
NSSI was strikingly prevalent in adolescents (76.6%) and moderately present in adults (40.1%). NSSI is a known predictor of future suicide attempts and adverse clinical outcomes, including psychiatric hospitalization and substance use [Reference Horwitz, Czyz and King44, Reference Bjureberg, Kuja-Halkola, Ohlis, Lichtenstein, D’Onofrio and Hellner45]. Consistent with previous studies [Reference Hawton, Bergen, Casey, Simkin, Palmer and Cooper46, Reference Hjelmeland and Grøholt47], NSSI was more prevalent among adolescents than adults. Although adolescent self-injury may remit spontaneously in some cases [Reference Moran, Coffey, Romaniuk, Olsson, Borschmann and Carlin48], it often signals enduring emotion-regulation difficulties and increases the risk of adverse psychosocial outcomes later in life [Reference Borschmann, Becker, Coffey, Spry, Moreno-Betancur and Moran49]. Given these implications, ongoing monitoring of NSSI trajectories across follow-up waves of the cohort will be critical to identify persistence, remission, and associated clinical predictors. Its high prevalence in youth underscores the need for targeted early interventions that address both suicidal and non-suicidal self-harming behaviours.
The study has limitations. It does not include biological or genetic data or account for prior health service use, which could inform our understanding of help-seeking behaviour. The inclusion criteria excluded those who presented to non-hospital emergency services, and assessments occurred up to 15 days after the index attempt, possibly limiting state-sensitive variables. This timeframe was selected to ensure recruitment of individuals in close temporal proximity to the suicidal event, while allowing sufficient time for clinical stabilization and ethical feasibility of assessment. Although this window may limit the sensitivity of some state-dependent variables, it reflects the typical course of emergency care and referral pathways in Spain, where immediate follow-up evaluations are often scheduled within the first 2 weeks post-attempt. The lack of data on personality disorders and other variables, such as mental pain [Reference Pompili, Innamorati, Erbuto, Luciano, Sampogna and Abbate-Daga50], is also a limitation, given their relevance to suicide risk. Although the SURVIVE study is based on the follow-up of a large cohort of suicide attempters, the present report is focused on the baseline characteristics of the cohort, and thus, cross-sectional by nature [Reference Vieta and De Prisco51]. Nonetheless, the study’s strengths include a large, diverse sample, comprehensive assessments via structured interviews and validated self-report tools, and broad geographical coverage.
In conclusion, the SURVIVE cohort provides a robust baseline profile of individuals at high risk of suicide, revealing distinct patterns across adolescents and adults. From a clinical perspective, these findings underscore the need for comprehensive, age-sensitive assessments that address depression, trauma, and suicide-related behaviour following a suicide attempt. Incorporating contextual factors such as migration and social support could further enhance the effectiveness of suicide prevention strategies. Notably, NSSI was highly prevalent among adolescents, highlighting the need for focused prevention strategies in this subgroup. Lethality of the attempt, past suicidal behaviours, and family history further characterize a clinically severe population. These findings lay a foundation for subsequent analyses on predictors of suicidal behaviour recurrence and inform the design of tailored, age-specific interventions.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1192/j.eurpsy.2025.10143.
Data availability statement
Data are available from the authors upon reasonable request.
Acknowledgements
The following are members of the SURVIVE consortium: Iñigo Alberdi-Paramo, Natalia Angarita, José Luis Ayuso-Mateos, Maria Fe Bravo-Ortiz, Guillermo Cano-Escalera, Álvaro Carrasco-Diaz, Laura Comendador, Manuel Couce-Sánchez, Fernando Corbalán, Sandra Gómez-Vallejo, Eduardo Jiménez, Elvira Lara, Itziar Leal-Leturia, Luisa Lázaro, María Purificación Lopez-Peña, Pablo Mola-Cardenes, Marta Navas, Anna Pedrola-Pons, Juan Manuel Pastor Haro, Pablo Reguera, Carlamarina Rodríguez-Pereira, Julia Rodríguez-Revuelta, Miguel Ruiz-Veguilla, Maria Dolores Saiz-Gonzalez, Elisa Seijo-Zazo, Elizabeth Suarez-Soto, Lara Suárez-López, Alba Toll, Emma Vidal Bermejo, Mireia Vázquez, Miguel Velasco, Eduard Vieta, Iñaki Zorrilla.
Author contribution
All authors contributed to this paper and approved the final version. Conceptualization: V.P., M.E., P.A.S., and C.S. Methodology: V.P., A.T.-L., and P.A.S. Data analyses: A.T.-L., A.P., C.S., M.E., P.A.S., L.J., A.G.F., J.F.F., and T.B. Writing original draft: V.P., M.E., C.S., and P.A.S. Writing, review, and editing: J.A.J., W.A.A., M.T.B., M.A.B., A.I.C.M., M.C.R., I.C., B.C.F., M.D.M., J.F.F., A.G.F., I.G., L.J.T., A.G.P., D.J.P.V., A.P.T., A.P., I.V.P.D., B.P., and N.R.
Financial support
This study was supported by the Instituto de Salud Carlos III-FIS research grants (PI19/00236, PI19/00569, PI19/00685, PI19/00941, PI19/00954, PI19/01027, PI19/01256, PI19/01484, PI20/00229 and PI23/00147, PI23/01483, PI23/00822, PI23/00614, PI23/00085, PI23/00707, PI23/01469, PI23/01277, PI23/01367, PI23/01066), co-funded by the European Regional Development Fund (ERDF) “A Way to Build Europe.” Additional founding was received from: the Secretaria d’Universitats i Recerca del Departament d’Economia i Coneixement (2021 SGR 01358; 01431), CERCA Programme/Generalitat de Catalunya, the Fundació Clínic per la Recerca Biomèdica (Pons Bartran 2022-FRCB_PB1_2022), Institut d’Investigació i Innovació Parc Taulí, the Instituto de Salud Carlos III (ISCIII; S2022/BMD-7216 AGES 3-CM, S2017/BMD-3740 AGES-CM2-CM); and co-funded by the European Union (grant numbers: COV20/00988, PI17/00768, PI20/01113), Horizon 2020 research and innovation programme Societal Challenges (101016127), the Basque Government 2022111054, and the University of the Basque Country IT1631-22, Government of the Principality of Asturias (Ref. IDE/2024/774), “la Caixa” Foundation (Ref. HR23-00421 CaixaResearch Health 2023), CIBERSAM – Consorcio Centro de Investigación Biomédica en Red Salud Mental- (CB/07/09/0020 Group) and Fundació La Marató de TV3 (202226-30). NR contract is co-funded by the Instituto de Salud Carlos III, with file code CD23/00088, by virtue of Resolution of the Direction of the Instituto de Salud Carlos III, O.A., M.P. of December 13, 2023, awarding the Sara Borell and “Co-funded by the European Union” Contracts.
Competing interests
VP has been a consultant to or has received honoraria or grants from AB-Biotics, AstraZeneca, Bristol-Myers-Squibb, CIBERSAM, FIS- ISCiii, Janssen Cilag, Lundbeck, Otsuka, Servier, and Medtronic. IG has received grants and has served as a consultant, advisor, or CME speaker for the following entities: ADAMED, Angelini, Casen Recordati, Esteve, Ferrer, Gedeon Richter, Janssen Cilag, Lundbeck, Lundbeck-Otsuka, Luye, SEI Healthcare, Viatris, outside the submitted work. She also receives royalties from Oxford University Press, Elsevier, and Editorial Médica Panamericana. AGP has received grants and served as a consultant, advisor, or CME speaker for the following entities: Janssen-Cilag, Lundbeck, Otsuka, Pfizer, Sanofi-Aventis, Alter, Angelini, Exeltis, Novartis, Rovi, Takeda, the Spanish Ministry of Science and Innovation (CIBERSAM), the Ministry of Science (Carlos III Institute), the Basque Government, and the European Framework Programme of Research. DJPV reported receiving grants from and serving as a consultant or advisor for Rovi, Johnson and Johnson, and Lundbeck, with no financial or other relationship relevant to the subject of this article. PAS has been a consultant to and/or has received honoraria or grants from Adamed, Alter Medica, Angelini Pharma, “laCaixa Foundation,” CIBERSAM, Ethypharm Digital Therapy, European Commission, Government of the Principality of Asturias, Instituto de Salud Carlos III, Johnson & Johnson, Lundbeck, Otsuka, Pfizer, Plan Nacional Sobre Drogas, Rovi, Servier, and Viatris España outside the submitted work. The rest of the authors declare no conflict of interest.



 Open access
Open access
Comments
No Comments have been published for this article.