Highlights
-
Access to carotid artery stenting was greater than endarterectomy during the COVID-19 pandemic.
-
The rates of stroke and death following carotid artery stenting during the pandemic were similar to pre-pandemic conditions.
-
Carotid artery stenting is a reasonable alternative to endarterectomy if access to surgical suites and recovery units become limited.
Introduction
Extracranial internal carotid artery (ICA) stenosis is responsible for 10–20% of all ischemic strokes and transient ischemic attacks. Reference Flaherty, Kissela, Khoury, Alwell, Moomaw and Woo1,Reference Cheng, Brown, Simister and Richards2 The risk of stroke recurrence is higher for patients with large artery atherosclerosis than with other etiologic subtypes, and this risk is greatest early after a symptomatic event. Reference Flach, Muruet, Wolfe, Bhalla and Douiri3,Reference Lovett, Coull and Rothwell4 Clinical practice guidelines suggest early carotid endarterectomy (CEA) or carotid artery stenting (CAS), ideally within the first two weeks of the last clinical event. Reference Kleindorfer, Towfighi, Chaturvedi, Cockroft, Gutierrez and Lombardi-Hill5,Reference Gladstone, Lindsay, Douketis, Smith, Dowlatshahi and Wein6 CEA is generally preferred over CAS, except in situations such as high carotid bifurcation, surgically inaccessible stenosis, contralateral carotid artery occlusion or history of neck irradiation.
The global COVID-19 pandemic that started in March 2020 led to drastic changes in healthcare delivery and resource management. Overall, there were fewer carotid revascularization procedures (both CEA and CAS) and fewer diagnostic cerebral angiograms performed internationally during the early waves of the COVID-19 pandemic. Reference Qureshi, Agunbiade, Huang, Akhtar, Abraham and Akhtar7–Reference Crespy, Benzenine, Mariet, Baudry, Bernard and Bejot10 In order to preserve critical resources such as anesthesia and capacity of intensive care units and operating rooms, some centers in Europe explicitly advocated shifting from CEA toward CAS, with one Italian study subsequently demonstrating a higher proportion of patients received CAS. Reference Sterpetti, Gabriele, Borrelli, Campagnol, Iannone and Costi8,Reference Rinaldi, Brioschi, Marazzi, Pallini and Marone11,Reference Hellegering, Van Der Laan, Heide, Uyttenboogaart, Zeebregts and Bokkers12 Within the Canadian landscape, we also faced similar pressures to steward appropriate hospital resources. At our center, access to operating rooms was relatively challenging compared to access to the angiosuite because of staffing challenges and bed pressure in surgical and anesthetic units. For example, following CAS, patients would be admitted directly under neurology in the neurological acute care unit versus being admitted under vascular surgery for post-CEA care in the post-anesthetic care unit managed by anesthesia. A same-day discharge protocol following CAS was developed in London, Ontario, which was associated with a minimal rate of immediate postprocedural stroke, though long-term outcomes were not studied. Reference Kiwan, Jukes, Mayich, Boulton, Sharma and Pelz13
As the single academic health center that performs CEA and CAS in an administrative region that serves 1.2 million people, our comprehensive stroke center in Ottawa, Ontario, Canada, provides all carotid revascularization care. During the early pandemic, we observed a reduction in referrals to our stroke prevention clinic and code stroke activation, Reference Dowlatshahi, Stotts, Bourgoin, Gocan, Dunn and Powell14 while it appeared that more cases of CAS were performed. We therefore conducted a focused review of our clinical practice to study the impact of the COVID-19 pandemic on indications and outcomes of CAS.
Our hypothesis is that the pandemic conditions were associated with higher rates of CAS and potentially worse outcomes than we had experienced previously. With more cases of CAS being performed during the pandemic, we speculate that some patients may not have met the same inclusion criteria for CAS as in pre-pandemic conditions, therefore increasing the risk of complications of CAS. The primary objective of our study was to determine the frequency of non-serious and serious complications following CAS over a two-year period from June 2019 to May 2021. The secondary objective was to assess complications by patient characteristics and organ systems.
Methods
Study design and setting
This is a retrospective cohort study that took place at the Ottawa Hospital in Ontario, Canada. This study was approved by the Ottawa Hospital’s Research Ethics Board. The Ottawa Hospital’s Research Ethics Board has also waived the participants’ consent given the study’s retrospective nature. This study was reported according to the STROBE statement.
The Ottawa Hospital is a comprehensive stroke center that provides hyperacute stroke treatment in the form of thrombolysis and endovascular thrombectomy, as well as carotid revascularization that includes CEA by vascular surgery and CAS by neurointerventionalists trained in radiology, neurology or neurosurgery. Typically, conscious sedation was used in the pre-pandemic and pandemic periods. General anesthesia would be used if the patient became agitated or hemodynamically unstable, and the decision to change to general anesthesia would involve a thorough discussion between the anesthesiologist and the neurointerventionalist. Patients who undergo CAS are admitted under neurology in the neurological acute care unit and are monitored there postprocedurally. The Ottawa Hospital is the only comprehensive stroke center that provides hyperacute stroke treatment and carotid revascularization for east-central Ontario, western Quebec and the territory of Nunavut.
Participant selection
We identified consecutive patients coded as receiving CAS through the hospital’s Picture Archiving and Communication System (PACS) from June 1, 2019, to May 31, 2021. The pre-pandemic period was defined as June 2019 to March 15, 2020, and the pandemic period was defined as March 16, 2020, to May 31, 2021. We began our analysis on June 1, 2019, because that was when our hospital system began using the EPIC electronic medical record and data prior to EPIC is not accessible. We chose mid-March 2020 as the start of the COVID-19 pandemic in Ottawa because the first local COVID-19 case was confirmed on March 11, 2020, a provincial state of emergency was declared on March 17, 2020, alongside directives to postpone non-urgent surgeries and procedures. The City of Ottawa declared a state of emergency with shutdowns on March 25, 2020. 15 We ended our analysis on May 31, 2021, reflecting exactly two years since the start of the study.
We excluded patients whose CAS were performed acutely during endovascular thrombectomy, who received stenting of an artery other than the extracranial ICA or procedures for in-stent thrombosis, as well as patients without baseline imaging (i.e., patients transferred from peripheral hospitals whose neuroimaging was performed there instead).
Data collection
Two investigators (HS, KS) independently reviewed the charts of included patients. Any discrepancies were resolved after consultation with the senior investigator (MS). Baseline demographics, past medical history, pre-CAS imaging details (imaging modality, degree of stenosis by NASCET criteria), 16 degree of stenosis on digital subtraction angiography, complications from stenting, timing of stenting in relation to index event, complications in the first 24 hours after CAS, serious complications beyond 24 hours after CAS and consultation by vascular surgery were captured. If the degree of stenosis was not available in the imaging report, the images were reviewed by the first and last author (HS, MS) on PACS. A subset of these images was further reviewed by two blinded neuroradiologists (SC, EP) to ensure accuracy.
Outcome measures
The primary outcome of our study was the frequency of serious and non-serious complications following CAS. Serious complications were ischemic stroke (defined as new and persistent focal neurological deficits (at least a two-point increase from baseline score of National Institutes of Health Stroke Scale lasting longer than 24 hours or new ischemic infarct visible on repeat neuroimaging after 24 hours of CAS with or without clinical deficits), intracranial hemorrhage (ICH), myocardial infarction (MI) or death from any cause. Non-serious complications were defined as relevant medical events that required physician assessment, led to a change in medical therapy or further investigations outside the expected course of recovery and/or prolonged hospitalization. The non-serious complications were categorized by organ involvement. While non-serious complications could be clinically significant and relevant, we have chosen to label stroke, ICH, MI and death as serious complications in our study to be consistent with previous literature, where the primary outcomes for CAS and CEA were stroke, MI and death. Reference Brott, Hobson, Howard, Roubin, Clark and Brooks17,Reference Müller, Lyrer, Brown and Bonati18
Patients may have had more than one complication (i.e., hypotension from acute blood loss was counted as both hypotension and bleeding; death caused by stroke was counted as both a stroke and a death). The intraprocedural period was defined as the period between groin puncture and departure from the angiography suite. The postprocedural period was defined as the first 24 hours following the procedure. For patients who experienced a neurological deterioration in the first 24 hours, we assessed whether stroke or death occurred subsequently. There was also subsequent independent adjudication by the first and last author (HS, MS) to determine if their neurological deterioration was related to their index event or was a serious complication or led to a serious complication.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation (SD), and categorical variables were expressed as counts and percentages. Comparison of continuous variables was determined using the independent T-test, whereas the Mann–Whitney U test was used to evaluate ordinal variables, and the Pearson Chi-square test and the Fisher’s exact test were used to evaluate nominal variables. Unadjusted and adjusted odds ratios (OR) were reported with 95% confidence intervals (CI). Logistic regression was used to evaluate the difference in odds of complications before and during the COVID-19 pandemic, after adjusting for age, sex, degree of stenosis and timing of index event to procedure. These covariates were chosen based on clinical judgment as well as established research metrics for carotid revascularization. P < 0.05 was considered statistically significant. All statistical analyses were performed with SPSS version 29.0.1.0. (IBM Corp. in Armonk, NY, USA).
Results
Participants’ characteristics
We screened 187 patient files,140 of whom met the inclusion criteria. The most common reasons for exclusion were stenting of another artery or of the intracranial ICA (N = 16) and CAS performed during endovascular thrombectomy (N = 10). Figure 1 shows the process of inclusion and exclusion of patients in the study.
Flow diagram detailing the inclusion criteria, exclusion criteria and the number of patients included in the study. CAS = carotid artery stenosis; PACS = Picture Archiving and Communication System.

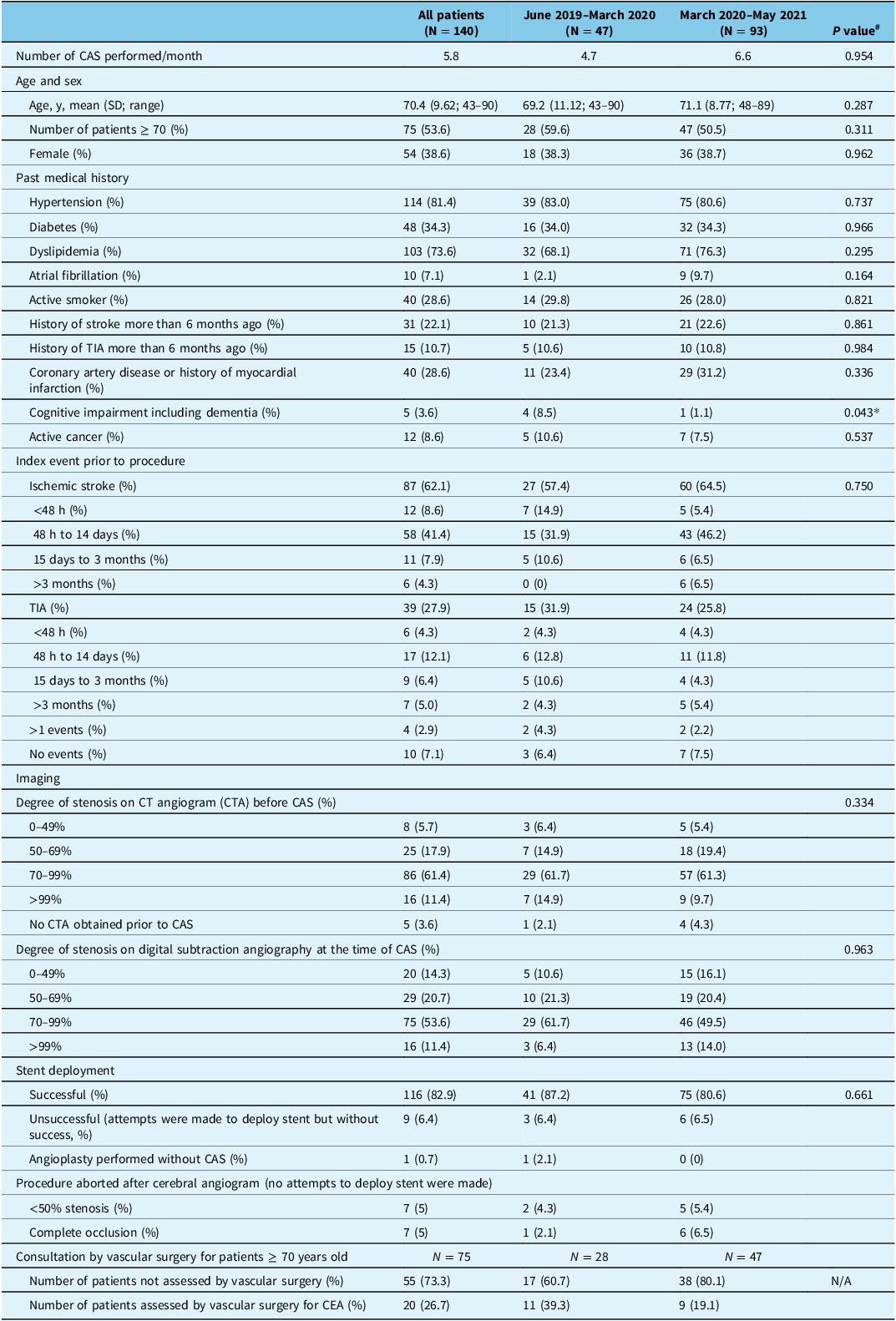
We identified 47 patients in the pre-pandemic period and 93 patients in the pandemic period. On average, 4.7 cases of CAS per month were performed in the pre-pandemic period versus 6.6 cases per month in the pandemic period (p = 0.954). The mean age of patients was 70.4 ± 9.62 years (range, 43–90 years), and 54% were female. These two groups did not differ in their age, sex distribution and comorbidities, except fewer patients with cognitive impairment presented during the pandemic period (p = 0.043). Additionally, there were no statistical differences between the two groups in the timing of their index event prior to undergoing CAS nor the degree of stenosis measured on CT angiogram and digital subtraction angiography. The vast majority of patients (82.9%) had successful stent placement with no significant difference before and during the pandemic. About 10% of all patients had their procedure aborted after the cerebral angiogram due to either < 50% stenosis or complete occlusion of the ICA. Table 1 outlines the comparison of demographics, index event, imaging and status of stent deployment.
Comparison of demographics, index event, imaging, status of stent deployment and consultation by vascular surgery before and during the COVID-19 pandemic

Table 1 Long description
The table compares patient demographics, index events, imaging, and stent deployment before and during the COVID-19 pandemic. It has 27 rows and 5 columns. The columns are labeled as follows: All patients (N = 140), June 2019–March 2020 (N = 47), March 2020–May 2021 (N = 93), and P value. The rows include various metrics such as the number of CAS performed per month, age and sex, past medical history, index event prior to procedure, imaging details, degree of stenosis on CT angiogram before CAS, degree of stenosis on digital subtraction angiography at the time of CAS, stent deployment status, and consultation by vascular surgery for patients aged 70 years or older. Each row provides specific data points for each column, detailing the comparison between the pre-pandemic and pandemic periods. Notable trends include the mean age of patients, the percentage of females, and the successful stent placement rates, with no significant differences observed in most categories except for cognitive impairment.
CAS = carotid artery stenting; TIA = transient ischemic attack; CEA = carotid endarterectomy.
* Statistically significant, p < 0.05.
# Independent t-test, Pearson Chi-square test, Fisher’s exact test or Mann–Whitney U test, where appropriate.
Complications
A) Intra-procedure
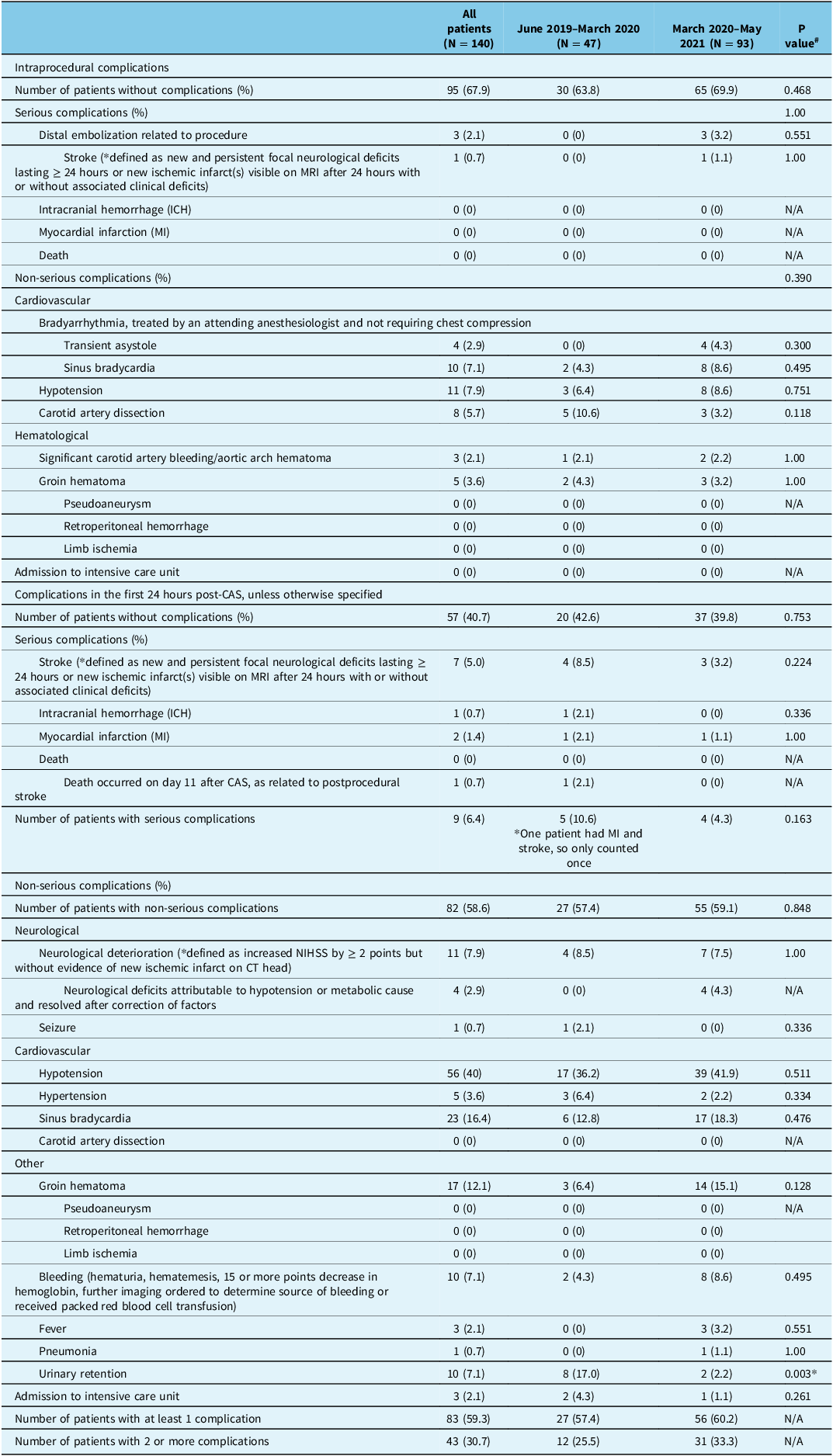
One patient had a serious complication in the pandemic period, which was an intraprocedural stroke. There were no intraprocedural strokes in the pre-pandemic period. Intraprocedural ICH, MI or deaths did not occur in the pre-pandemic and pandemic periods.
Seventeen patients experienced non-serious complications in the pre-pandemic period versus 27 patients in the pandemic period, which was not a statistically significant difference (OR 0.722, 95% CI 0.343–1.520). Comparing non-serious complications by organ systems did not reveal further differences. The most common non-serious complications were hypotension (7.9%) and sinus bradycardia (7.1%), all treated pharmacologically without admission to the ICU. Five patients developed groin hematoma; none of them developed pseudoaneurysm, retroperitoneal bleed or limb ischemia or required surgical management of bleeding.
B) Post-procedure
Within the first 24 hours after the procedure, seven patients experienced stroke: four in the pre-pandemic period versus three patients in the pandemic period. One patient experienced an ICH, and this was in the pre-pandemic period. Two patients experienced postoperative MIs, one in each of the pre-pandemic and pandemic periods. No patients died in the first 24 hours. One patient with a stroke died on postoperative day 11. There were no statistical differences in the frequency of serious complications between the two groups (OR 0.378, 95% CI 0.096–1.478).
Non-serious complications occurred in 83 patients, 27 in the pre-pandemic period versus 56 patients in the pandemic period. No statistical differences were observed overall (OR 1.07, 95% CI 0.527–2.183), though less urinary retention occurred in the pandemic period (p = 0.003). The most common non-serious complications in the first 24 hours were hypotension (40%), bradycardia (23%) and groin hematoma (12.1%). Seventeen patients developed groin hematoma, but none developed pseudoaneurysm, retroperitoneal hemorrhage or limb ischemia or required surgical management of bleeding.
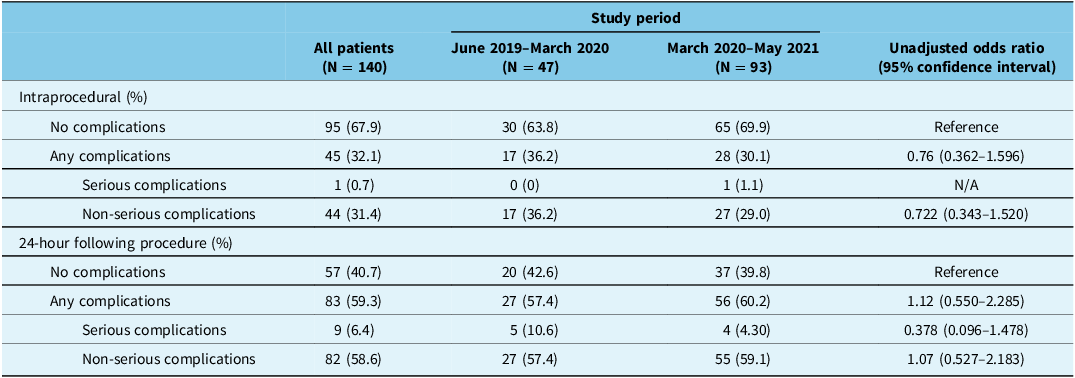
Tables 2 and 3 demonstrate the comparison of the frequency of serious and non-serious complications in the intraprocedural and postprocedural periods in the pre-pandemic and pandemic periods.
Comparison of frequency of complications (serious and non-serious complications) in the intraprocedural and postprocedural study period before and during the COVID-19 pandemic

Table 2 Long description
A table comparing complication frequencies during intraprocedural and postprocedural periods before and during COVID-19. The table has 10 rows and 5 columns. Column headers are: All patients (N = 140), June 2019–March 2020 (N = 47), March 2020–May 2021 (N = 93), and Unadjusted odds ratio (95 percent confidence interval). Row labels are: Intraprocedural (percent) with sub-labels No complications, Any complications, Serious complications, Non-serious complications, and 24-hour following procedure (percent) with sub-labels No complications, Any complications, Serious complications, Non-serious complications. Row 1: Intraprocedural (percent), No complications, 95 (67.9), 30 (63.8), 65 (69.9), Reference. Row 2: Intraprocedural (percent), Any complications, 45 (32.1), 17 (36.2), 28 (30.1), 0.76 (0.362–1.596). Row 3: Intraprocedural (percent), Serious complications, 1 (0.7), 0 (0), 1 (1.1), N/A. Row 4: Intraprocedural (percent), Non-serious complications, 44 (31.4), 17 (36.2), 27 (29.0), 0.722 (0.343–1.520). Row 5: 24-hour following procedure (percent), No complications, 57 (40.7), 20 (42.6), 37 (39.8), Reference. Row 6: 24-hour following procedure (percent), Any complications, 83 (59.3), 27 (57.4), 56 (60.2), 1.12 (0.550–2.285). Row 7: 24-hour following procedure (percent), Serious complications, 9 (6.4), 5 (10.6), 4 (4.30), 0.378 (0.096–1.478). Row 8: 24-hour following procedure (percent), Non-serious complications, 82 (58.6), 27 (57.4), 55 (59.1), 1.07 (0.527–2.183).
Classification and comparison of specific serious and non-serious complications in the intraprocedural and postprocedural study period before and during the COVID-19 pandemic

Table 3 Long description
The table compares the frequency of serious and non-serious complications during intraprocedural and postprocedural periods before and during the COVID-19 pandemic. It has 140 rows and 7 columns. The columns are labeled as All patients (N = 140), June 2019–March 2020 (N = 47), March 2020–May 2021 (N = 93), and P value. The rows are grouped into Intraprocedural complications, Serious complications, Cardiovascular, Non-serious complications, and Postprocedural complications. Each row lists specific complications and their frequencies in the different periods. Notable trends include the number of patients without complications, various types of complications, and their occurrences in the specified periods.
MI = myocardial infarction; ICH = intracranial hemorrhage; CAS = carotid artery stenting; NIHSS = National Institutes of Health Stroke Scale.
* Statistically significant, p < 0.05.
# Pearson Chi-square test or Fisher’s exact test, where appropriate.
C) Overall complications
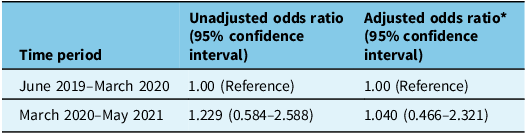
After adjusting for age, sex, degree of stenosis and timing of index event prior to CAS, there were no differences in the frequency of combined intraprocedural and postprocedural complications between the pre-pandemic and pandemic periods (OR 1.040, 95% CI 0.466–2.321; Table 4).
Unadjusted and adjusted association between the impact of the COVID-19 pandemic and combined intraprocedural and postprocedural complications

Table 4 Long description
A table with two rows and three columns comparing unadjusted and adjusted odds ratios of complications during different time periods. The columns are labeled Time period, Unadjusted odds ratio (95% confidence interval), and Adjusted odds ratio* (95% confidence interval). The first row represents the time period from June 2019 to March 2020 with unadjusted odds ratio of 1.00 (Reference) and adjusted odds ratio of 1.00 (Reference). The second row represents the time period from March 2020 to May 2021 with unadjusted odds ratio of 1.229 (0.584–2.588) and adjusted odds ratio of 1.040 (0.466–2.321).
* Adjusted for age, sex, degree of stenosis and timing of index event prior to procedure.
Consultation by vascular surgery
Consultations to vascular surgery for CEA for patients 70 years old and older occurred infrequently (26.7%). We observed a 50% decrease in the frequency of consultation by vascular surgery for endarterectomy in the pandemic period compared to the pre-pandemic period (19% vs. 39%). Of the 55 patients who were over age 70 but were not referred to vascular surgery for CEA, most did not have a documented rationale for stenting (36/55, 65%). However, this does not mean there were no indications for either procedure. We postulate this may be related to unintentional omission (where indications and contraindications for either endarterectomy or stenting were discussed in rounds but not ultimately documented) or copy-pasting in medical records or variation in local practice.
Discussion
In this retrospective cohort study of 140 consecutive patients undergoing CAS for extracranial ICA stenosis before and during the early COVID-19 pandemic, the combined rate of intraprocedural and postprocedural serious complications (ischemic stroke, ICH, MI, death) was 7.1%. Non-serious complications were common (31.4% during the intraprocedural period and 58.6% during the 24 hours following CAS), with no significant difference observed other than a lower frequency of urinary retention during the COVID-19 pandemic (p = 0.003). After accounting for age, sex, degree of stenosis and timing of index event leading to CAS, the combined rates of intraprocedural and postprocedural complications were similar before and during the COVID-19 pandemic (aOR 1.040, 95% CI 0.466–2.321). During the pandemic period, there was a 50% reduction in the proportion of patients over age 70 who were referred to vascular surgery for consideration of endarterectomy prior to undergoing stenting.
The COVID-19 pandemic presented a unique challenge in terms of timely access to carotid revascularization. Our data suggest that, at our center, two more cases of CAS were performed every month than had been during the pre-pandemic period. This may explain the decreased referral to vascular surgery that we observed. We did not observe an increased rate of intraprocedural or immediate postprocedural serious complications, which is similar to the experience of other Canadian comprehensive stroke centers. Reference Kiwan, Jukes, Mayich, Boulton, Sharma and Pelz13 Comparing our results to administrative registries studying 30-day stroke/death rate before the onset of the COVID-19 pandemic, our results (5.7%) were similar to theirs (3.7–12.09%). Reference Paraskevas, Kalmykov and Naylor19 We speculate this may be due to improved operator skills and/or design in endovascular instrumentation in the recent decade. We did not find an association between increasing age and complications of stenting or a difference in outcomes based on the patient’s sex. These findings are important given that current guidelines generally suggest that patients over the age of 70 would be better candidates for endarterectomy and that women may benefit less from carotid intervention than do men. Reference Kleindorfer, Towfighi, Chaturvedi, Cockroft, Gutierrez and Lombardi-Hill5,Reference Gladstone, Lindsay, Douketis, Smith, Dowlatshahi and Wein6,Reference Müller, Lyrer, Brown and Bonati18,Reference Bonati, Kakkos, Berkefeld, de Borst, Bulbulia and Halliday20 The heterogeneous reporting of sex-specific outcomes should be acknowledged, and our data add to the available evidence that women fare no differently than men after carotid artery revascularization. Reference Yogendrakumar, Shamy, Dewar, Fergusson, Dowlatshahi and Hamel21–Reference Howard, Algra, Howard, Bonati, de Borst and Bulbulia23
Our study findings have clinical implications and may support consideration of stenting over endarterectomy under specific circumstances, such as in situations where access to surgical suites and post-anesthesia care units is limited. Our experience suggests that this may be a reasonable approach that balances resource stewardship with commitment to deliver appropriate, time-sensitive stroke care. Future studies could explore longer term outcomes after stenting among patients generally considered candidates for endarterectomy, as available data are derived from studies conducted more than 15 years ago. Reference Müller, Lyrer, Brown and Bonati18
A strength of our study is that it represents real-world practice of stenting in a comprehensive stroke center with experienced operators during the COVID-19 pandemic. Our study specifically adds knowledge to a paucity of literature examining the impact of the pandemic on outcomes of carotid revascularization. We acknowledge some limitations of our study. First, we did not capture outcomes of a comparative cohort undergoing endarterectomy though we hope to explore this subsequently. Second, we did not assess outcomes at 30 days or beyond. However, to address this limitation, we selectively reviewed patients who had experienced early neurological events to assess if a serious complication such as death or stroke had occurred.
Conclusion
In this cohort of consecutive patients undergoing CAS at a comprehensive stroke center before and during the COVID-19 pandemic in Canada, the rates of stroke and death were similar to pre-pandemic conditions and were generally consistent with the published literature.
Acknowledgments
The authors have no acknowledgments to declare.
Author contributions
HS and MS conceived the study. HS, BD and MS designed the methodology. HS, KS and MS collected and reviewed the data. HS, RF, SC, EP and MS reviewed imaging. HS and MS performed analyses. DD and MS provided supervision. All authors contributed to the writing.
Funding statement
This research project received no specific financial support from any funding agency.
Competing interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.