


Introduction
Globally around 19% of older people (aged ≥ 60 years) suffer malnutrition,(Reference Salari, Darvishi and Bartina1) defined as ‘a state resulting from lack of uptake or intake of nutrition leading to altered body composition (decreased fat free mass) and body cell mass leading to diminished physical and mental function and impaired clinical outcome from disease’.(Reference Sobotka2) Prevalence of malnutrition differs across healthcare settings, with higher prevalence in residential care (17.5%), hospital (22–28%), and rehabilitation (29.4%) settings compared to older people living in the community (3.1–8%).(Reference Cereda, Pedrolli and Klersy3,Reference Leij-Halfwerk, Verwijs and van Houdt4) Malnutrition increases hospital length of stay, escalates healthcare costs, is a key contributing factor in the aetiology of sarcopenia and frailty, and increases risk of morbidity and mortality.(Reference Elia, Stratton, Elia and Russel5–Reference Rus, Porter and Brunton7) Considering the adverse clinical outcomes associated with malnutrition, the identification and management of malnutrition is a vital patient-centred outcome to enhance older adult’s health and quality of life and to enable cost-effective treatment and care.
Oral nutritional supplements (ONS) are essential adjuncts in managing malnutrition in hospitalised older people. ONS are energy- and nutrient-dense products designed to increase dietary intake when diet alone is insufficient to meet daily nutritional requirements.(Reference Volkert, Beck and Cederholm8) According to expert consensus, ONS should contain both micro and macronutrients and provide at least 400 kcal and a minimum of 30 g of protein per day to improve nutritional status and decrease risk of functional decline.(Reference Volkert, Beck and Cederholm9) Overall, research suggests favourable impacts of ONS on nutritional status and healthcare costs, while the impacts on functional outcomes and mortality are more controversial.(Reference Milne, Potter, Vivanti and Avenell10,Reference Stratton, Hebuterne and Elia11) Nevertheless, to effectively produce clinical benefits, patients need good adherence and acceptability to the products on offer in hospital.(Reference Hubbard, Elia, Holdoway and Stratton12–Reference Gosney14)
There are numerous factors that may influence ONS adherence including type, variety, volume, temperature, energy density, duration and timing of supplementation, presentation, and whether any instruction or assistance has been given.(Reference Volkert, Beck and Cederholm9) The European Society for Clinical Nutrition and Metabolism (ESPEN) recommend that adherence should be assessed regularly when ONS are offered to older people with malnutrition and the form of ONS should be adapted to suit patient’s taste and eating capacity.(Reference Volkert, Beck and Cederholm8) Higher energy density ONS appear to have better adherence rates than lower energy density ONS, possibly related to their smaller volume.(Reference Hubbard, Elia, Holdoway and Stratton12,Reference Hébuterne, Frin and Lefevere15) Typically, research has investigated the adherence of ready-made multi-nutrient liquids in older patient groups and has found a mean adherence with ONS of 67% in hospital, 81% in the community and an overall adherence of 78.8% across healthcare settings.(Reference Hubbard, Elia, Holdoway and Stratton12) In other research, older hospitalised patient’s adherence with drink-based supplements was low (37%) and incurred a wasted cost of £18,294 per year across 4 geriatric wards in 1 hospital.(Reference Gosney14)
Supplemental preference may be affected by a multitude of factors such as taste, colour, smell, aftertaste, and texture. Factors reducing drink-based supplement palatability and adherence included thicker textures,(Reference den Boer, Boesveldt and Lawlor16) build-up of a mouthcoating,(Reference Thomas, Van der Stelt, Schlich and Lawlor17) abdominal bloating,(Reference Darmon, Karsegard and Nardo18) alterations in mouthfeel when wearing dentures, and changes in flavour perceptions depending upon medication status.(Reference Regan, Feeney and Hutchings19) Moreover, continual single use of a supplement resulted in monotony and taste fatigue leading to reduced intake.(Reference Nieuwenhuizen, Weenen, Rigby and Hetherington20) Typically, hospital patients are offered drink-based ONS. However, previous research has identified that 56% of older adults (n = 96, 58% female, 28% with malnutrition) in hospital did not like drink-based supplements.(Reference Gosney14) Hence, exploration of adherence to different ONS formats is an important research direction to maximise nutritional intake for malnourished older persons.
Hospitalised older adults with malnutrition should be offered an improved range and provision of ONS to suit personal preferences and maximise intake.(Reference Volkert, Beck and Cederholm9) Research suggests that alternative ONS products such as ice cream are acceptable by hospitalised older adults at risk of malnutrition.(Reference Taib, Ong and Mulvaney21) Yet this is an understudied area, with limited data investigating adherence to alternative ONS products compared to ready-made drinks in hospital, such as powdered ONS and snacks. ONS variations according to flavours and categories need to be considered to improve patients’ adherence. Therefore, this study aimed to investigate the adherence and palatability of a new porridge supplement compared to a standard drink-based supplement and to explore product acceptability in hospitalised older adults at risk of malnutrition.
The specific objectives included:
-
• To determine patient adherence to a new porridge supplement compared to standard drink-based ONS, assessed through measurement of product intake (% of product consumed).
-
• To examine the palatability of a new porridge supplement compared to standard drink-based ONS.
-
• To assess the acceptability of product use on acute medical wards through qualitative semi-structured interviews with participants and healthcare professionals.
Methods
Study design and setting
This was a single-centre multi-method randomised controlled crossover design. A crossover design was chosen to account for heterogeneity in an older patient population (e.g., differences in disease states and oral sensory perceptions), in which participants acted as their own controls to better compare palatability of products. This study was conducted at University Hospital Southampton (UHS) National Health Service (NHS) Foundation Trust on acute trauma and orthopaedic wards. The manuscript follows Consolidated Standards of Reporting Trials (CONSORT) guidance (Supplement 1).
Ethics and data sharing
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human participants were approved by the Health Research Authority (HRA) and Health and Care Research Wales (HCRW) on 6th January 2023 (22/LO/0898). Written informed consent was obtained from all participants. The study was registered on ClinicalTrials.gov (NCT05620082) on 17th November 2022, including access to the protocol and statistical analysis plan (https://clinicaltrials.gov/study/NCT05620082?cond=malnutrition&term=relish&rank=1). De-identified participant data is available on University of Southampton research data repository ‘Pure’.
Patient and public involvement
A public and patient representative provided input into the study protocol, reviewed patient-facing materials, and was a part of the study management group. Before development of the new porridge supplement, palatability and taste of porridge was assessed by a group of older people hospitalised on medical wards at UHS. Flavour preferences were explored with a survey (n = 25; aged 86.23 ± 5.93 (mean ± standard deviation [SD]) years; 56% female). Analyses showed a median likability rating of 5 (IQR 3–6) ‘mildly like’ points for porridge. Participants flavour preferences were golden syrup, strawberry, and apple and cinnamon.
Participant recruitment
Eligible participants on acute medical and orthogeriatric wards were identified by the clinical care team and approached by the research team to obtain informed consent. Inclusion criteria were adults aged 65 years or above, medium-high risk of malnutrition (Malnutrition Universal Screening Tool [MUST] score 1–4),(Reference Cortes, Yanes and Capitan-Moyano22) and able to provide informed written consent. Exclusion criteria were a MUST > 4 (severely malnourished), body mass index (BMI) ≤ 15 kg/m2 requiring specialist dietetics input, chronic liver disease, renal failure (any stage), dysphagia, major surgery within the preceding month, a terminal illness, patients receiving end-of-life care, unable to eat by mouth (Nil By Mouth [NBM]), and requiring alternative ONS as advised by dietetic support. Initially, patients receiving ONS in the previous month were excluded; however, this impacted recruitment rates and was subsequently removed from the exclusion criteria on 31st May 2024.
Eligibility criteria were developed in response to screening and recruitment trials by the study team, in collaboration with the dietetic team to ensure participant safety, and consistent with malnutrition screening policy and management at UHS. All patients admitted to UHS are assessed for risk of malnutrition within 24 hours using MUST.(Reference Cortes, Yanes and Capitan-Moyano22) Patients with a medium (score 1), or high risk (score ≥ 2) of malnutrition receive nutritional support. If a patient has a medium MUST score, oral nutritional supplements can be offered as a part of their nutritional action plan.
Eligible healthcare professionals were approached for interview by the research team. Inclusion criteria were staff able to provide consent and working at UHS on the wards receiving the ONS intervention. A sub-sample of patients participating in the trial were invited for interview. Purposive sampling was used to include staff from a range of roles and a diverse group of patients, including age, sex, and adherence to the tested products.
Sample size
A sample size of 50 was chosen based upon guidance from previous literature investigating adherence and palatability of ONS.(Reference Hubbard, Elia, Holdoway and Stratton12,Reference Thomas, Van der Stelt, Schlich and Lawlor17) In a systematic review of 49 studies assessing ONS adherence, studies included 1–4 groups with a median of 30 (interquartile range 23–41) participants in each group.(Reference Hubbard, Elia, Holdoway and Stratton12) Difficulties with recruitment resulted in changes to eligibility criteria, expanding the number of wards involved in the study and extending the study end date. Fifty participants was a target supported by study resources, achievable in the timeframe of the project, and consistent with lower recruitment rates obtained from previous research with older people in hospital.(Reference Meredith, Holt and Varkonyi-Sepp23)
Trial randomisation
Participants were randomised to groups by the lead researcher in a crossover procedure using a computer-generated randomisation tool, ‘Research Randomizer’,(Reference Urbaniak and Plous24) to minimise sequence effects and bias. Participants were allocated to one of two sequences at random in a 1:1 allocation to eliminate bias associated with group assignment while creating similar sized groups. Randomisation was performed before recruitment started, generating a list of participant ID numbers randomly assigned to each group. On recruitment to the study, researchers referred to the randomisation table to assign participants to groups.
Adverse event reporting
Adverse events were reported to the chief investigator (CI) and principal investigator (PI) and recorded on the Case Record Form (CRF) stored in the study site file. All serious adverse events were reported to the study team (CI or PI) and then onto the study sponsor within 24 hours of the investigator becoming aware of the event. All study staff and clinicians in contact with participants were responsible for noting adverse events that were reported by the participant and making them known to appropriate medical staff. Participants were encouraged to contact their research nurse/team at the time of an event occurring.
Intervention
Participants were prescribed ONS twice per day for 4 days, in addition to normal meals, in a crossover design. Two ONS products (Supplement 2) were tested for palatability and adherence including a new porridge supplement (treatment) and standard drink-based ONS (control). Each ONS product was tested over 2 days in a randomised crossover sequence. The products were offered twice per day, in-between breakfast and lunch and after dinner to reduce the detrimental long period of calorie absence experienced overnight.(Reference Correa-Arruda, Vaez and Aguilar-Nascimento25) The porridge (treatment) was powdered and mixed with 170 ml boiling water in a pot using a measuring jug and included a choice of 5 flavours including golden syrup, apple and cinnamon, strawberries and cream, bananas and custard, and chocolate. The drink-based ONS (control) were ready-to-drink milkshakes. Participants were offered the ONS in a screw-topped plastic bottle and choice of a variety of flavours (e.g., vanilla, strawberry, chocolate, banana, mocha). ONS products were prepared and distributed to participants by health care professionals working on the wards.
Data collection
Participant characteristics
Participant characteristics including age (years), domicile status, marital status, care provision, usual residence, reason for admission, frailty (Program of Research to Integrate Services for the Maintenance of Autonomy [PRISMA-7]),(Reference Raiche, Hebert and Dubois26) risk of sarcopenia (Strength, Assistance with walking, Rising from a chair, Climbing stairs, and Falls [SARC-F]),(Reference Ida, Kaneko and Murata27) and appetite (Simplified Nutritional Appetite Questionnaire [SNAQ])(Reference Pilgrim, Baylis and Jameson28) were assessed at baseline. Participant’s C-reactive protein (CRP) (mg/L)(Reference Wener, Daum and McQuillan29) and National Early Warning Score (NEWS)(Reference Treacy, Wong, Odell and Roberts30) were recorded as markers of acute illness (recorded as part of standard care), a potential mediator of older adults’ appetite. Consistent with hospital site screening policy and nutrition management, the MUST tool was used to categorise participants at risk of malnutrition.(Reference Cortes, Yanes and Capitan-Moyano22)
Levels of CRP (mg/L) were measured on admission and used as an inflammatory marker with mild inflammation considered at levels 5–30 mg/L and above 30 mg/L indicating moderate to severe inflammation.(Reference Wener, Daum and McQuillan29) Research suggests a CRP of 30 mg/L is a threshold of acute inflammation leading to reduced food intake.(Reference Pourhassan, Cederholm and Trampisch31) The NEWS system alerts the clinical care team to deteriorating adult patients in hospital through scoring routine bedside measures, such as oxygen saturation and pulse rate, leading to an overall NEWS risk score indicating a specific clinical response (Low: 1–4 aggregated score, Medium: score 5–6, High: score ≥ 7).(32)
SNAQ is a four-item tool comprising items 1, 2, 4 and 6 of the Council on Nutrition Appetite Questionnaire (CNAQ), assessing appetite, satiety, taste of food and number of meals per day respectively. SNAQ has a maximum score of 20, with a score of ≤14 indicating poor appetite.(Reference Pilgrim, Baylis and Jameson28) The SARC-F comprises five components: strength, assistance in walking, rise from a chair, climbing stairs and falls. The scores range from 0 to 10, with a score of equal to or greater than four being predictive of sarcopenia and poor outcome.(Reference Ida, Kaneko and Murata27) The PRISMA-7 contains seven items with a positive score of three or more indicating frailty and has high accuracy in identifying frail older adults.(Reference Raiche, Hebert and Dubois26,Reference Hoogendijk, van der Horst and Deeg33)
Primary outcome measures
Primary outcome measures included adherence to ONS and palatability. Adherence to ONS was assessed via documentation of ONS leftovers at 2 timepoints, including after lunch (for ONS given in the morning) and early morning the following day (for ONS given after dinner). Leftovers were weighed (g) using weighing scales (Seca Model 875 digital weighing scale) and documented by the research team. Adherence was calculated as the percentage of the mean ONS consumed per day. Moreover, the mean intake of ONS energy (kcal/day) and protein (g/day) was calculated.
Palatability ratings, including appearance, smell, taste, sweetness, texture, thickness, aftertaste, mouth feel, and overall likability was assessed with a 7-point hedonic Likert scale (7 = definitely like, 6 = moderately like, 5 = mildly like, 4 = neither like nor dislike, 3 = mildly dislike, 2 = moderately dislike, 1 = definitely dislike). Hedonic scales have been used to assess palatability of ONS supplements across population groups(Reference Hébuterne, Frin and Lefevere15,Reference Taib, Ong and Mulvaney21) and have good reliability.(Reference McGough, Peacock and Hackett34) Palatability ratings (score 1–7) were completed on initial introduction of each ONS, on day 1 and day 3.
Secondary outcome measures
Secondary outcome measures included acceptability of ONS products, total caloric intake (kcal/day), and the gap (%) in energy and protein intake compared to personal requirements. Existing literature suggests that the effectiveness of ONS in improving energy intake can be compromised by partial displacement of normal meals.(Reference Fiatarone Singh, Bernstein and Ryan35) Therefore, total energy intake was assessed through completion of patient food charts, including estimated proportion of meals consumed. Food charts were a part of standard care and were completed by the nursing team. Energy intake (kcal) was calculated from diaries via nutritional data supplied by hospital catering (Serco). The food diary was completed 2 days before the start of testing to estimate normal total energy intake and then completed daily during the 4-day testing period.
Acceptability of ONS products was explored with semi-structured interviews. The interviews explored the views of hospitalised older adults and healthcare professionals, exploring the acceptability of the ONS products and the factors influencing implementation (Supplement 3). The interviews were audio-recorded for data collection purposes and took place one-to-one with the researcher (SJM) within UHS in-person, or remotely via telephone, or Microsoft Teams. Patients were interviewed following completion of 4 days of ONS intervention.
Data analysis
Statistical analysis was conducted using the statistical software SPSS (V.29). Descriptive statistics (median (interquartile range [IQR]); mean (standard deviation [SD]); number (%)) were used to analyse ONS ingested (%), intake of energy (kcal/day), intake of protein (g/day), gaps to dietary requirements (%), and palatability Likert scores (score 1–7). Normality tests, including skewness and kurtosis, were conducted to determine suitable statistical analyses for measures (i.e., non-parametric vs. parametric tests). Primary outcome measures were compared between groups (treatment vs. control) using a related-samples Wilcoxon signed-rank test with asymptomatic significance (2-sided test), and differences in ONS intake (g) were compared between morning and evening supplements. Total daily energy intake (kcal) was compared between ONS groups and control (i.e., before testing) with a related-samples Friedman’s Two-Way Analysis of Variance (ANOVA) by Ranks summary to assess the impact of ONS on normal meal intake, using adjusted significance for pairwise comparisons. Participant’s energy and protein requirements were calculated using European guidelines recommending older people consume 1 g/kg of body weight protein and 30 kcal/kg of body weight energy daily.(Reference Volkert, Beck and Cederholm8) Participants absolute gap in energy (kcal) and protein (g) intake compared to their requirements was calculated and converted into a percentage before comparing between timepoints (baseline, porridge and drink-based) with a general linear model repeated measures ANOVA. Mauchly’s test of sphericity was used and Greenhouse-Geisser correction applied for data where sphericity was not assumed. Pairwise deletion was used to handle missing data.
Interviews were transcribed verbatim and analysed using reflexive thematic analysis (RTA).(Reference Braun and Clarke36) RTA is a method for identifying, analysing, and reporting patterns or themes within data. Organisation of qualitative data was conducted using NVIVO. Transcribed text was read and coded by SJM. The codes were analysed to generate concepts and ideas to determine the acceptability of ONS products and to identify facilitators and barriers to their implementation. The codes acted as tags or labels to help catalogue key concepts embedded within the raw data. From the codes, themes were developed to reflect the views and experiences of the patients and healthcare professionals regarding the intake and use of ONS products in hospital. Using an iterative approach, SERL acted as a ‘critical friend’, helping SJM to reflect and sense-make, interpret the barriers and facilitators to supplement adherence, and support the lead author as she reflected on her beliefs and assumptions.
Results
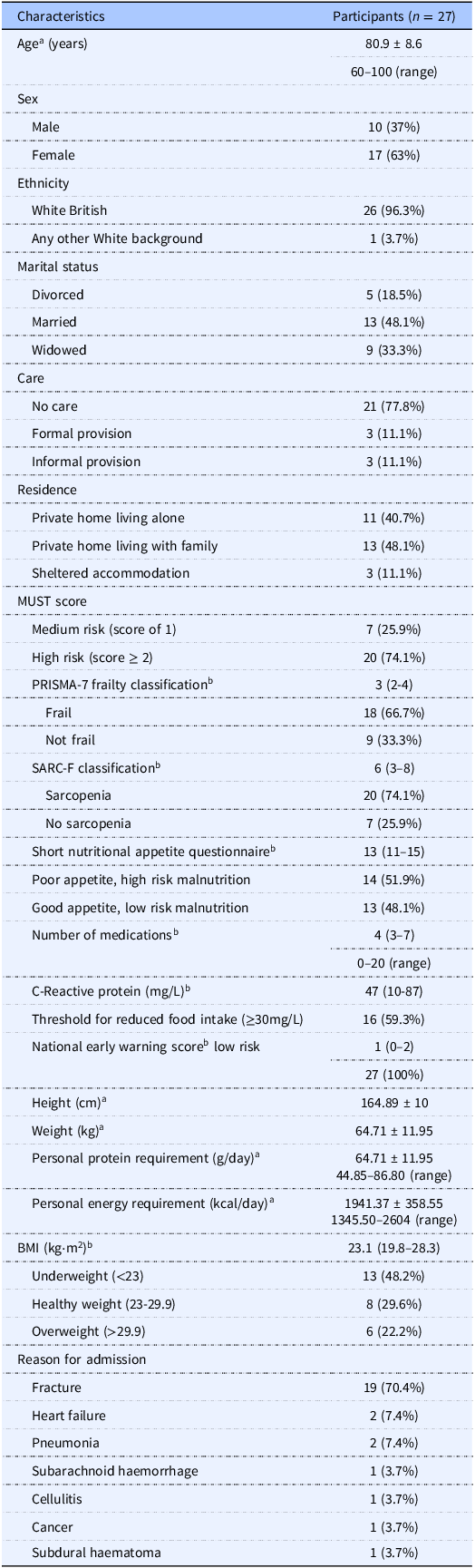
Four hundred and sixty-nine participants were screened, 114 participants were approached, and 27 consented to participate in the study (Figure 1). Participant characteristics are presented in Table 1. Participants were mainly female (63%), had a mean age of 80 years, had poor appetite (52%), were frail (67%), and were at risk of sarcopenia (74%). Based on MUST scores, 74.1 % of participants were at high risk of malnutrition. No adverse events were caused by the nutritional products studied.
Flow diagram illustrating participant screening, recruitment, and analysis. Recruitment took place 29/04/24–31/12/24.

Participant characteristics

Note: a, mean ± standard deviation; b, median and interquartile range; MMSE, mini-mental state examination; MUST, Malnutrition Universal Screening Tool; BMI, body mass index. Personal protein and energy requirements were calculated based on ESPEN guideline on clinical nutrition and hydration in geriatrics, comprising 1 g/kg of body weight for daily protein intake and 30 kcal/kg of body weight for daily energy intake.
Adherence
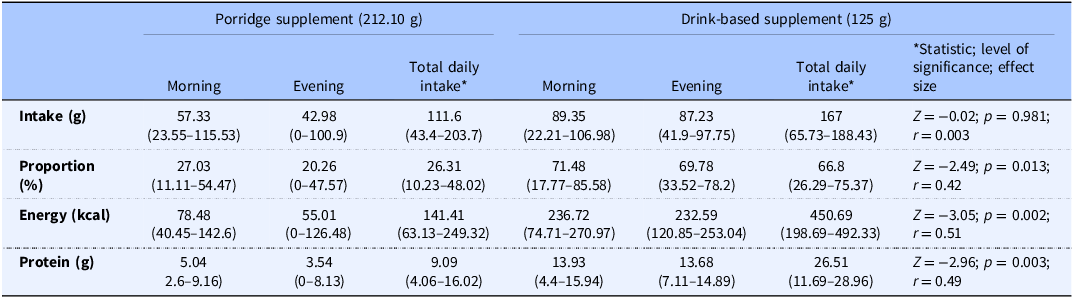
There were no significant differences in the absolute volume of product consumed between the porridge (median 111.6 g [IQR 43.4–203.7]) and drink supplement (median 167 g [IQR 65.73–188.43]) (p = 0.981; r = 0.003). However, the daily percentage of porridge consumed (median 26.31% [IQR 10.23–48.02]) and energy (kcal/day) and protein (g/day) intake were significantly lower compared to the drink supplement (median 66.8% [IQR 26.29–75.37]) (Table 2). There were no differences in porridge intake (g) between morning (median 57.05 [IQR 14.44–108.59]) and evening (median 42.98 [IQR 0–100.9]) supplements (Z = −0.60; p = 0.546), and there were no differences in drink-based intake (g) between morning (median 90.95 [IQR 37.08–107.78] and evening (median 92.55 [IQR 50.98–105.3]) supplements (Z = −0.17; p = 0.862).
Adherence to porridge and drink-based supplements (n = 18). Values are presented as median and interquartile range

Palatability
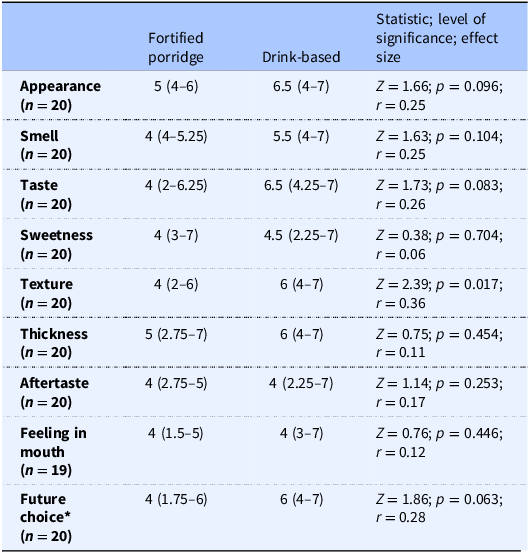
Participants found the drink-based ONS more palatable than the porridge (Table 3). Specifically, the texture of the porridge (median score 4 [IQR 3–7]) was significantly disliked compared to the drink-based control (median score 6 [IQR 4–7]) (Z = 2.39; p = 0.017; r = 0.38). Though not significant, 71% of participants agreed they liked the drink-based ONS and would be happy to choose it in future, compared to 45% for the porridge (Z = 1.86; p = 0.063; r = 0.28).
Palatability of fortified porridge and drink-based oral nutritional supplements (values are expressed as median and interquartile range)

Note: 7, definitely like; 6, moderately like; 5, mildly like; 4, neither like nor dislike; 3, mildly dislike; 2, moderately dislike; 1, definitely dislike. *7, strongly agree; 6, largely agree; 5, agree somewhat; 4, neither agree nor disagree; 3, disagree somewhat; 2, largely disagree; 1, strongly disagree.
Daily energy and protein intake
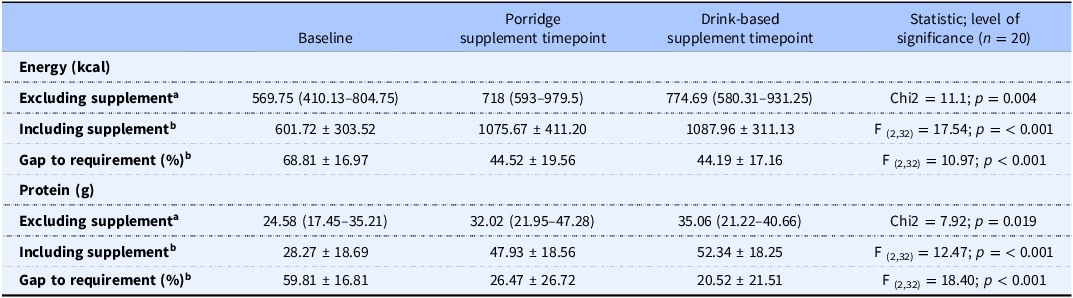
Friedman’s Two-Way ANOVA showed a significant difference in daily energy (kcal) (Chi2 = 11.1; p = 0.004) and protein (g) intake (Chi2 = 7.92; p = 0.019) between baseline, porridge, and drink-based timepoints (excluding ONS intake). Pairwise comparisons using adjusted significance indicated a significantly higher energy (kcal) and protein (g) intake at the porridge timepoint compared to baseline (p = 0.003 and p = 0.017, respectively). Therefore, supplements did not reduce normal dietary intake (Table 4).
Daily energy (kcal) and protein (g) intake at baseline, at porridge timepoint, and drink-based supplementation timepoint excluding and including supplements, and the percentage gap to personal nutrition requirements

Note: a, median and interquartile range; b, mean ± standard deviation. Baseline data were collected 5.56 ± 4.34 (mean ± SD) days after patient admission.
There was a significant difference in the gap (%) between total daily energy and protein intake (including supplements) and personal energy and protein requirements between timepoints (p < 0.001). Pairwise comparisons showed significant differences in gaps to energy and protein requirements (%) between baseline and porridge timepoints (p = 0.002, p < 0.001, respectively) and between baseline and drink-based supplement timepoints (p < 0.001), however, there were no significant differences in the gap (%) to energy and protein requirements between porridge and drink-based supplement timepoints (p = 0.958, p = 0.401, respectively) (Table 4).
Acceptability of nutritional supplements
Nine older adults (aged 65–95 years; 7 female), 2 nurses, 1 health care assistant, 1 dietetic assistant, and 1 dietitian were interviewed. Mean interview length was 22.64 minutes. Four main themes showcased the factors influencing food intake and acceptability of supplements, illustrated in Figure 2, and described below. Supporting quotations for each theme are presented in Table 5.
Main themes showing the factors influencing food intake, supplement palatability, and compliance.

The main themes and subthemes influencing the acceptability of nutritional supplements have been displayed with supporting quotations

Food traditions and lifelong preferences
Participants reported hospital food often did not meet their personal food preferences, reducing intake. Family traditions and eating cultures guided food intake and etiquette. For instance, most older people ate 3 small meals a day without snacks in-between meals, and they preferred whole foods to artificial supplements. Some participants grew up eating porridge in their families and preferred porridge as a traditional breakfast food rather than a snack. Staff reported porridge as an inappropriate supplement during the summer, where hot weather reduced calorie intake. Needing a specialist diet to manage disease symptoms (e.g., coeliac disease, diabetes) was perceived as a barrier to altering calorie and protein intake for some participants who were concerned about exacerbation of illness symptoms, especially if they consumed anything unfamiliar. Moreover, the association of supplements with end of life and illness deterred some participants from consumption.
The interplay between age-related changes in physical ability and appetite and the consequences of illness and treatment influenced food intake
Reduced appetite due to medications and feeling ill impacted participant’s food intake, including adherence to supplements. Participants also noticed a slow decline in their appetite over time associated with their age and often reported preferring smaller portion sizes. Supplements with a smaller volume, a thinner texture, and drink-based, were easier to consume when participants had a reduced appetite. Weight loss and reduced strength motivated participants to increase their calorie intake. However, the presence of co-morbidities, poor dental health, constipation, impaired eyesight, fatigue, and pain changed some participants physical ability to prepare and eat food. Participants relied on food delivery services and family at home to assist with shopping and cooking and required assistance with choosing from the menu and cutting up food in hospital. Some participants required softer textures and had a slow eating pace, which resulted in cold unpalatable food. Supplements were often perceived as a good replacement for whole foods when a participant’s appetite was poor post-surgery and when eating was a struggle. Staff reported dementia as a significant risk for malnutrition, influencing appetite and ability to eat and becoming a barrier to understanding why they needed supplements.
Hospital culture impacted food intake and supplement adherence
-
1. Hospital food services influenced the availability and provision of palatable food
The hospital provided a large variety of food options to meet patients’ food preferences and participants were pleasantly surprised by the quality of the food, especially given the large amounts of people that the hospital catered for. Only one participant disliked the food, and another found the food was served too cold, which reduced food intake. The hospital catered well for individuals requiring vegetarian and gluten-free options. However, participants reported a lack of ‘lighter’ food options, which they would have preferred post-surgery and with a poorer appetite. Staff explained the structure of three large meals a day conflicted with the dietetic teams’ advice to consume smaller more frequent meals throughout the day for older people with poor appetite. While biscuits were readily available as snacks, participants reported a lack of healthier snacks, such as fruit, and staff highlighted that improved access to hospital snacks was needed, offering a better variety of snacks and more often.
-
2. Social expectations in hospital and coping with difficult emotions
Participants reported feeling lonely on the wards and found the ward a depressing environment. Participants felt they had to stick to social hospital norms, including staying in bed and within their bay, which reduced feelings of well-being, increased sedentary behaviour, reduced physical activity and reduced appetite. Individuals who made social connections on the wards, had regular visitors, and were able to leave their bay, reported a stronger sense of well-being, which they believed enhanced their recovery. Families were pivotal to improving food intake, bringing in participants’ favourite food, helping with hospital food choices, and assisting at mealtimes. Patients who were not visited frequently and who were reluctant to ask for nutritional support from staff for fear of being a burden had reduced intake.
-
3. Staff attitudes and behaviours on a busy ward – beyond the written role
Nursing, health care support worker, and allied health care professional staff kindness and compassion improved patient recovery, but sometimes staff did not have the capacity to fulfil patient’s optimum nutritional needs. Patients with dementia disproportionately impacted on staff time that had an impact on other patients who reported feeling neglected. This influenced a negative view of staff attitudes to an ageing population where staff did ‘the basics to keep us alive’ but did not allow them to flourish. Most staff perceived ONS as an important part of malnutrition management. However, staff with negative perceptions of ONS influenced prescription and patient perspectives. Often the reasons for prescribing nutritional supplements and specialist nutritional advice were not readily available to patients; subsequently patients were unclear on the benefits of using supplements.
Basic help with eating and sourcing good nutrition was sometimes challenging in a busy ward environment. For instance, staff did not always have time to encourage patients to sit out of their beds to receive meals. Moreover, some patients reported staff frequently forgetting to give them fresh water, and staff were unavailable and/or unaware of participants that needed assistance with feeding, such as cutting food smaller to make chewing easier. When staff spent more time with patients to find out their personal needs, they were able to improve access to preferred foods and break hospital misconceptions. For example, advising on the importance of movement in hospital and if they were able, the opportunity for patients to leave the ward with a family member. Many patients did not want to bother busy staff, which sometimes compromised their optimum nutrition needs.
-
4. Nutrition care pathways and established staff practices influenced nutrition management
The dietetic team provided expert nutritional support. However, they were not available for every patient that needed them, and nutrition was often overlooked by the clinical care team or was perceived as a lower clinical priority. Nurses and health care assistants had key roles within a patients’ nutritional care, such as systematically monitoring weight and food intake. Nevertheless, wards were understaffed and there was poor capacity to implement optimal nutritional strategies. Staff outside the dietetic team required specialist nutritional training. However, high turnover of nurses and health care support workers due to shift work patterns typical on an acute ward created barriers to good nutritional support. Staff were encouraged to work at mealtimes to assist with feeding, though some nurses reported a clash with their duty to dispense medication at mealtimes. Participants recognised the value of family and volunteers, such as meal-time assistants to promote good nutrition. However, wards lacked implementation of such interventions.
Nutritional supplementation, including drink-based supplements and soups, were an established practice for malnourished patients in hospital. Supplements are given equal importance and were prescribed with usual medicines to facilitate administration. Moreover, clinical pathways, such as those for patients who have sustained a fractured neck of femur incorporate routine daily drink-based supplementation to reduce risk of malnutrition post-surgery. However, staff did not have capacity to monitor supplement adherence and offer alternative options for supplement refusals. Moreover, there were limited ONS options in hospital, in which a larger variety of ONS was needed to support a tailored approach. Drink-based supplements were perceived as convenient to provide compared to real food snacks and cheap to supply in hospital. Nursing staff wanted more input from the dietetic team to develop a nutritional care plan for patients on the wards and to review these plans before discharge, incorporating food fortification as well as ONS and arranging nutrition care follow-up in the community.
Interaction between supplement texture, flavours, and presence of artificial ingredients influenced palatability and adherence
Five out of the nine participants interviewed enjoyed the taste of the drink-based supplement, 2 participants found the supplement too sweet, 1 participant said palatability would have improved with the drink served cold, and another disliked the smell and consistency of the supplement. Only 2 participants enjoyed the taste of the porridge, with golden syrup being the preferred flavour. The porridge was served hot, which was perceived as a facilitator to adherence. However, the thickness and texture of the porridge was frequently reported as a barrier to adherence, especially for individuals who found swallowing difficult. Having to prepare the powdered porridge created additional issues. For example, one participant reported the porridge was not mixed well enough and had powdered clumps, and another explained they preferred eating real oats rather than an artificial supplement. Some participants wanted to add other foods to the porridge to improve palatability including honey and Greek yoghurt.
Generally, staff reported that patients did not like the taste of supplements on offer in hospital, highlighting that they were often too sweet and that artificial ingredients used to increase shelf life impacted taste and palatability. Drink-based supplements were best served cold but there was not enough space in fridges on the wards. Staff liked the concept of porridge as an additional option as an ONS, as it looked and tasted less artificial. Additionally, their view was that supplements closest to the consistency and palatability to normal food improved patient adherence. Smaller supplement volumes and thinner, smoother consistencies were advocated in hospital to suit patients with poor appetite and difficulties eating. Having a better range of flavours and supplement types, including alternatives to milk-based options, was encouraged by staff, especially to combat supplement fatigue, i.e., boredom of consuming the same supplements.
Discussion
This single-centre multi-method randomised controlled crossover study aimed to evaluate the adherence and palatability of a new porridge supplement compared to a drink-based supplement traditionally offered in hospital and to assess the acceptability of products with older people and healthcare professionals. Adherence was significantly higher with standard drink-based ONS (median 66.8% [IQR 26.29–75.37]; median 450.69 kcal [IQR 198.69–492.33]) compared to a new porridge supplement (median 26.31% [IQR 10.23–48.02]; median 141.41 kcal [IQR 63.13–249.32]) in hospitalised older people with medium-high risk of malnutrition. Overall, participants found the drink-based ONS more palatable than the porridge. Specifically, the texture of the porridge was significantly disliked compared to the drink-based control (Table 3). Four main themes were interpreted from interviews as influencing the acceptability of ONS and impacting participants’ food intake, including 1) food traditions and lifelong preferences, 2) the interplay between age-related changes in physical ability and appetite and the consequences of illness and treatment, 3) hospital culture, comprising hospital food services, social expectations in hospital, nutrition care pathways, and staff attitudes and behaviours on busy wards, and 4) interaction between supplement texture, flavours, and presence of artificial ingredients.
This study provided insight into the adherence and acceptability of a novel form of nutritional support in practice. Previous research has focused largely on drink-based ONS effectiveness and adherence, demonstrating average adherence rates of 67% in hospital.(Reference Hubbard, Elia, Holdoway and Stratton12) Of the few studies that have investigated other forms of supplementation in an older population, adherence rates have varied, such as 48.1% with homemade porridge and soup supplements,(Reference Bunout, Barrera and de la Maza37) and 84.4% with an ice-cream-based supplement.(Reference Taib, Ong and Mulvaney21) Existing research demonstrated various reasons for poor adherence to ONS, including reduced palatability influenced by medications and dentures altering the mouthfeel of products.(Reference Regan, Feeney and Hutchings19) In the present study, aversion to the texture of the porridge likely contributed to poor adherence. Moreover, porridge (212.1 g) was a larger volume than the drink-based supplement (125 g) meaning a larger proportion of the porridge needed to be consumed to achieve daily energy and protein recommendations.(Reference Volkert, Beck and Cederholm8) Participants highlighted difficulties consuming supplements during hospitalisation caused by various factors such as reduced appetite due to illness, medications, and alterations in physical ability to eat. Therefore, our findings are consistent with recommendations of lower-volume energy-dense ONS in older people living with illness.(Reference Hubbard, Elia, Holdoway and Stratton12,Reference Lombard, van Steijn and Schuur38) Nevertheless, patients and staff indicated a desire for a better range of ONS in hospital, including supplements with fewer artificial ingredients. This presents challenges for industry to produce low-volume energy-dense products that do not compromise on taste.
Baseline daily energy intake (534.25 kcal) was lower (p = 0.004) compared to daily energy intake at porridge (790 kcal) and drink-based supplement (703.25 kcal) timepoints (excluding supplements), showing supplements did not replace normal dietary intake and indicating patient recovery over time. Total energy and protein intake across all timepoints in the current cohort was considered low even with the addition of supplements. Participants were not meeting nutritional requirements with a gap of 44–69% off daily energy requirements and 20–60% off protein requirements across study timepoints (i.e., baseline and supplementation). Interestingly, when comparing between porridge and drink-based supplement timepoints the gap to energy and protein requirements was similar despite lower adherence to the porridge supplement. Overall, the daily intake of supplements was not sufficient to improve participants’ energy and protein requirements.
Protein and energy intakes lower than requirements are associated with a range of negative health outcomes, including longer hospital stays, higher readmission rates, hospital-associated infections, frailty, and mortality.(Reference Agarwal, Ferguson and Banks39,Reference Thibault, Makhlouf and Kossovsky40) Consistent with our findings, decreased food intake in hospital is a prevalent and significant issue for older inpatients worldwide.(Reference Sanson, Bertocchi and Dal Bo41) For example, older adults (n = 81 age 81.5 ± 11.5 [mean ± SD] years) with malnutrition, or at risk of malnutrition in hospital in Italy, had a mean energy intake of 669.0 ± 573.9 (SD) kcal/day and mean protein intake of 30.7 ± 25.8 (SD) g/day during their first 5 days of hospital admission.(Reference Sanson, Bertocchi and Dal Bo41) This equated to 60% of patients who ingested ≤ 50% of their calculated energy and protein requirements.(Reference Sanson, Bertocchi and Dal Bo41)
In line with existing literature, our interview findings highlighted various factors influencing older people’s food intake in hospital, including the impact of acute illness and medication on appetite, alterations in ability to eat (e.g., difficulties cutting food), oral problems (e.g., forgetting to bring dentures into hospital), catering limitations in hospital (e.g., restrictions on food serving times), reduced physical activity, and poor staff capacity to provide optimal nutritional support at meal times.(Reference Pourhassan, Cederholm and Trampisch31,Reference Sanson, Bertocchi and Dal Bo41–Reference Cass and Charlton43) Considering the multifactorial influences on patient appetite, participants’ gap to meeting energy and protein requirements, and the challenges associated with ONS consumption (e.g., dislike of textures and taste of artificial ingredients), our interview findings revealed the importance of additional nutritional strategies in hospital to manage and prevent malnutrition, including accessibility of snacks and the availability of family or volunteers to act as mealtime assistants. In a systematic review of 10 studies, alternative strategies, such as energy- and protein-based food fortification (e.g., protein-enriched bread or yoghurt) and snacks (e.g., cake, pastries, cheese sandwiches) were employed as an effective, acceptable, and cost-effective intervention to improve dietary intake among older people in hospital (546 patients), including a significant increase in energy (250–450 kcal per day) and protein intake (12–16 g per day).(Reference Mills, Wilcox and Ibrahim44) However, the feasibility of implementing such interventions is unclear. Indeed, our findings highlight the important impact of hospital food systems and ward culture on the availability and accessibility of nutritious food for patients. For instance, the hospital had limited snack choice and strict meal serving times, and ward staff often had limited time to deliver nutrition support, corroborated in previous literature showcasing poor nurse capacity to prioritise mealtimes above competing clinical demands.(Reference Naughton, Simon and White45) Future research is needed to assess the feasibility of adapting hospital food systems, including enrichment of hospital food menus and improving flexibility of mealtime services for older people with malnutrition.
Consistent with previous research,(Reference Brunner, Mayer and Qin46) we showed that basic nutrition training was needed for a range of staff roles (e.g., health care assistants and nurses). Due to lower staff capacity and high staff turnover, the hospital adopted a ‘blanket’ approach to ONS prescription in certain clinical cohorts, such as automatically prescribing ONS to patients sustaining a neck-of-femur fracture, to overcome restricted access to the dietetic team and ensure patients at higher risk of malnutrition were receiving sufficient energy and protein pre- and post-operatively. However, staff reported drink-based ONS being discarded as they did not have the time to monitor adherence and offer alternative options to suit patient preferences. Therefore, to improve nutritional intervention effectiveness and sustainability, hospital departments need to consider person-centred strategies, catering for personal preferences, enabling eating pleasure, and being adaptable to different eating patterns.(Reference Brunner, Mayer and Qin46) One such solution advocated by staff was assistance from family or volunteer mealtime assistants, which has a burgeoning evidence base that demonstrates improved dietary intake in hospitalised older people at risk of malnutrition.(Reference Brunner, Mayer and Qin46,Reference Zhang, Tay and Lim47) Enhanced staff training is also an important intervention, including educating on the importance of energy (calorie) and protein-first approach through food but complemented by the provision of ONS, ensuring good oral hygiene and that dentures are cleaned and fit well, comfortable positioning at mealtimes (e.g., encouraging patients to sit out of their bed), nursing assistance and supervision, and family involvement.(Reference Zhang, Tay and Lim47) Additionally, the concept of protected mealtimes should be prioritised where all health care professionals should refrain from clinical interventions, i.e., ward rounds, therapy.
In terms of good clinical practice, hospital policies and procedures should be reviewed and implemented in line with current clinical/research perspectives consistent with expert consensus. In the current study hospital screening policy advocated MUST to assess risk of malnutrition and guide patient nutrition plans. Evidence suggests MUST is a valid and reliable tool for screening malnutrition in hospital settings.(Reference Cortes, Yanes and Capitan-Moyano22) However, there is increasing credibility worldwide for the diagnosis of malnutrition using the Global Leadership Initiative on Malnutrition (GLIM) criteria, working towards a common malnutrition ‘language’ to ensure malnutrition prevalence, interventions, and outcomes can be compared globally.(Reference Alves, de Jesus and Britto48) Working towards the endorsement of malnutrition diagnostic criteria and management is needed for standard application in clinical settings. The ESPEN guideline on nutrition and hydration in geriatrics provides 82 recommendations to guide good clinical practice, including routine screening for malnutrition, ongoing systematic assessment of nutritional therapies, and individualising energy and protein requirements.(Reference Volkert, Beck and Cederholm8) In the current study optimal nutritional management was restricted by poor staff capacity and training, reduced availability of dietetic support, poor adherence to ONS, and inflexible hospital food systems. Interventions to improve food intake and ONS adherence should be individualised, comprehensive and part of a multimodal and multidisciplinary team approach,(Reference Volkert, Beck and Cederholm8) however wider hospital pressures and overarching health policies impact clinical practice and nutritional care, such as overcoming challenges related to staffing, equipment and funding.(Reference Freedman and Wolf49)
Strengths and limitations
A strength of the study was objectively weighing the difference between prescribed and consumed ONS rather than relying on patient recall or estimating the proportion of ONS consumed. Moreover, the crossover design accounted for heterogeneous groups, such as differences in oral sensory perceptions and disease states. However, the small sample size, exclusion of individuals without capacity to consent, and single-centre design limit the generalisability of findings. Only 33% of patients approached participated in the study, which is consistent with recruitment challenges often experienced in an older population within health care research and points to the importance of reviewing and considering research processes to enhance inclusion of older people in clinical trials.(Reference Goodwin, Low and Quinn51) Nevertheless, the qualitative interviews provided an in-depth exploration of factors influencing the acceptability and implementation of ONS products in hospital, meaningful insight into the barriers and facilitators of ONS consumption and showcased the complexity of appetite in acutely unwell older people and nutrition management in hospital systems.
There is a high prevalence of cognitive impairment secondary to dementia and delirium in hospitalised older people.(Reference Wu, Chang, Tranyor and Chiu52) These confer a higher malnutrition risk and present barriers to ONS adherence.(Reference Deeth, Stevens, Bell and Mudge53) Hence, future research investigating ONS adherence and palatability should include individuals without capacity to consent to ensure better representation of findings in practice. Furthermore, participants were mainly white British; hence, future research should improve recruitment strategies to include a wider diversity of older people. Consistent with previous research investigating adherence of innovative products,(Reference Taib, Ong and Mulvaney21) each product in the current study was tested over 2 days, which provided sufficient early insight into adherence and palatability allowing the development of products while saving resources. Nevertheless, further research examining adherence over a longer duration is needed to explore the possible effects of supplement fatigue, including re-measuring palatability after a longer consumption period for each product.
Conclusion
Our findings highlight that adherence was significantly higher for standard drink-based ONS compared to a new porridge product. Older people at risk of malnutrition disliked the texture of the porridge and were unlikely to meet ONS energy and protein recommendations with a larger product volume given the impact of acute illness on reduced appetite compared to a smaller energy-dense drink-based supplement. Multifaceted influences on nutritional intake highlight the need for a multi-component approach to nutritional care in hospital, considering patient-centred care rather than relying on a ‘one-size fits all’ approach. To improve patient-centred nutritional care, participants requested a wider in-hospital range of ONS products with natural ingredients, enhanced training for staff in nutritional care, involvement from family and staff during mealtimes, and consideration of ‘real food’ options, such as food fortification and snacks. Future research is needed to develop in-hospital ONS options and to explore the feasibility of implementing wider nutritional care changes for hospitalised older people with malnutrition.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/jns.2026.10108.
Acknowledgements
The authors thank the wonderful research participants and the amazing research team for making the project possible and Kate Adams from ADAMS Clinical Nutrition Ltd. for her passion and expertise in developing products to support older peoples’ health and well-being and for providing the porridge for the study. The authors also thank UKRI for funding the project.
Author contribution
SJM, HPP and SERL conceived and designed the trial and provided critical intellectual content. SERL and PCC obtained the funding. SERL was the chief investigator responsible for the overall conduct and management of the study. KAS led recruitment and data collections, and SJM monitored study processes and analysed the data. SJM drafted the manuscript. All authors contributed to the preparation of the final manuscript.
Funding statement
This research was funded by the UKRI i-NutriLife Open Innovation Research Club Hub (Hub grant reference BB/X010821/1). SL is funded by NIHR Advanced Fellowship Scheme.
HPP is supported by the NIHR Southampton Biomedical Research Centre, Nutrition, and the University of Southampton. This report is independent research, and the views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. These funding bodies had no role in writing of the manuscript or decision to submit for publication. For the purpose of Open Access, the author has applied a Creative Commons Attribution (CC BY) licence to any Author Accepted Manuscript version arising from this submission.
Competing interests
Harnish P Patel has received lecture fees from Abbott, Pfizer, and HC-UK conferences outside of the submitted work. Other authors have no competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.






 Open access
Open access