Women account for approximately 50 % of the world’s population; however, in light of the expanded concept of health, social gender discrimination towards them and the overload of responsibilities worsen this population’s well-being and make it more susceptible to illnesses, fact that increases women’s morbidity and mortality rates(1–3). Accordingly, breast neoplasms and complications related to pregnancy and childbirth are among the main causes of mortality in the female population(4).
These and other diseases’ pathophysiology has been related to oxidative stress, which is a mechanism observed when the body presents an imbalance between oxidising and antioxidant compounds. It is worth noticing that the antioxidant defense system comprises endogenous enzymes, including superoxide dismutase, catalase and glutathione peroxidase, as well as exogenous compounds, such as vitamin C and lycopene, that can be ingested through food intake(Reference Chikara, Nagaprashantha and Singhal5). Furthermore, researchers have dedicated themselves to assessing the positive effect of diets rich in antioxidants on diseases’ prevention and progression, as well as in controlling signs and symptoms of these pathologies. Researchers also observed that there is a high correlation between a diet’s total antioxidant capacity (TAC) and plasma TAC in young adults has been already observed(Reference Hajjarzadeh, Nikniaz and Mahdavi6,Reference Wang, Yang and Lee7) .
A diet’s antioxidant status can be assessed through dietary TAC, which is a dietary pattern analysis method. It is adopted to point out a diet’s antioxidant content and its cumulative and synergistic effects since it can show populations’ total antioxidant status(Reference Daneshzad, Tehrani and Bellissimo8,Reference Abshirini, Siassi and Koohdani9) . The concept of dietary TAC was introduced as a new tool to assess dietary antioxidants’ effects since it has proven to be as effective in measuring diet quality as other established diet quality indices because it can report inverse associations between dietary TAC and oxidative stress(Reference Abshirini, Siassi and Koohdani9).
Thus, if one takes into consideration the high prevalence of disorders affecting the female population every year, the association of oxidative stress and dietary TAC with these disorders’ improvement or prevention, and the scarcity of systematic reviews seeking to investigate it, the aim of the present systematic review and meta-analysis was to assess the association between dietary TAC and clinical conditions affecting women’s health, including endocrine conditions with gynecological implications, obstetric outcomes, gynaecological conditions and oncological diseases related to the female reproductive system.
Methods
Protocol and registration
This review was elaborated based on the document proposed by the Meta-analysis of Observational Studies in Epidemiology(Reference Stroup, Berlin and Morton10) reporting checklist. The search for scientific articles, as well as data extraction and methodological quality assessment, was carried out by two independent investigators – disagreements between appraisers were resolved through consensus. Research formal registration was carried out at the PROSPERO database (ID: CRD42024427784).
Search strategy
The search for original observational studies assessing the association between dietary TAC and women’s health outcomes was conducted to identify articles according to previously established inclusion criteria. The search was carried out in the following databases: MEDLINE (via PubMed), EMBASE, LILACS and CINAHL and through the reference list of articles obtained, until 29 February 2024. The following search MESHES were adopted: ‘dietary total antioxidant capacity’, ‘woman’ and ‘women’s health’.
These meshes were selected based on the previous readings of published articles relating diet TAC to health outcomes, as well as on MESHES selected for each assessed clinical condition. It is important to notice that all studies selected through this search were included in the present review. Publication year filters were not used.
Study eligibility criteria
This systematic review applied PICOS (Population, Intervention, Comparison, Outcome and Study Design) criteria, as detailed in Table 1. The following inclusion criteria were adopted: (a) studies assessing diet TAC in pregnant women, in women at reproductive age and women at pre- and post-menopausal periods, be them healthy or carrying diseases related to women’s health – including endocrine conditions with gynaecological implications (e.g. polycystic ovary syndrome (PCOS)), obstetric outcomes (e.g. gestational diabetes mellitus (GDM), preeclampsia (PE), miscarriage), gynaecological conditions (e.g. infertility, menopause) and oncological diseases related to the female reproductive system (e.g. breast, ovarian and endometrial cancers) – ; (b) studies conducted on human beings and (c) manuscripts published in English, Portuguese and Spanish about the herein assessed topic. Studies focused on diseases that are not specific to endocrine, obstetric, gynaecological or oncological outcomes, such as cardiovascular, bone, ocular and psychological diseases, as well as review articles, clinical trials, animal studies, and studies carried out in vitro were excluded from the review.
PICOS criteria for inclusion of studies

Abbreviations: NA, not applicable.
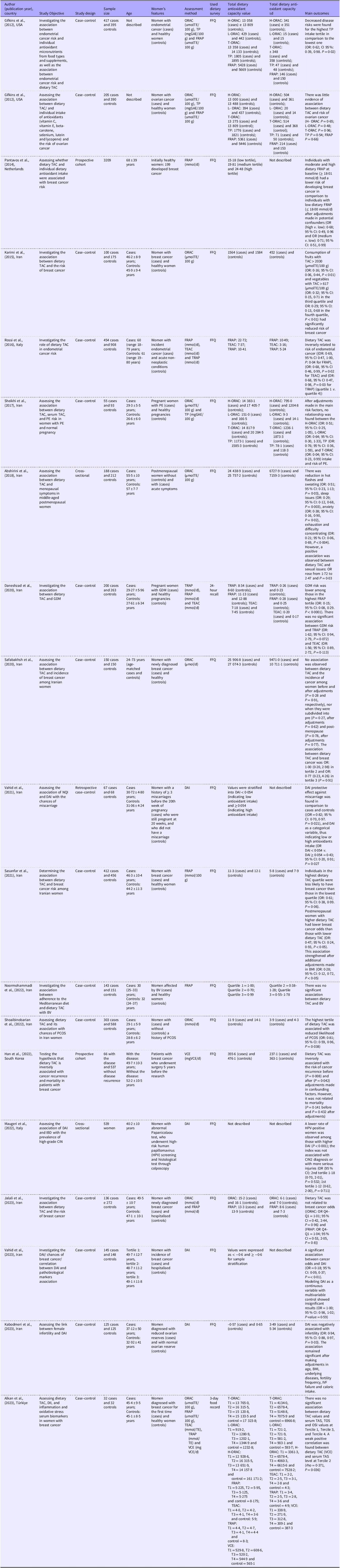
Features of studies assessing diet’s total antioxidant capacity and women’s health outcomes, including endocrine, gynaecological, obstetric and oncological conditions, 2024

Abbreviations: AFD, Antioxidant Food Database; BV, Bacterial vaginosis; CIN, cervical intraepithelial neoplasia; DAI, Dietary antioxidant index; DII, Dietary Inflammatory Index; FRAP, ferric reducing antioxidant potential; GDM, gestational diabetes mellitus; H-ORAC, hydrophilic oxygen radical absorption capacity; HPV, human papillovirus; L-ORAC, lipophilic oxygen radical absorption capacity; NQI, nutritional quality index; ORAC, oxygen radical absorption capacity; PE, pre-eclampsia; TAC, total antioxidant capacity; TAS, total antioxidant status; TE, Trolox equivalents; TEAC, antioxidant capacity equivalent to Trolox; T-ORAC, total oxygen radical absorption capacity; TOS, total oxidant status; TP, total phenolics; TRAP, total radical scavenging antioxidant parameter; T1, before surgery; T2, before chemotherapy; T3, in the 6th month of chemotherapy; T4, in the 12th month of chemotherapy; VCE, vitamin C equivalents.
Study selection and data extraction
Articles selection was carried out through title and abstract analysis and full-text reading by two authors of the current study separately. Duplicates were excluded after combining findings from the adopted bases; subsequently, studies were selected by titles. The selected articles were subjected to abstract reading, and the potentially relevant ones were read in full. The corresponding author was contacted to request access to the full article when it was not available to go on with the assessments.
The following information was extracted from the selected articles: author; publication year and country where the research was carried out; study objective and design; sample size (n); features of women included in the research (whether they were healthy pregnant women, adult women carrying a disease, among others); participants’ mean age; adopted dietary TAC assessment method; dietary TAC mean and standard deviation and main analysed outcomes.
Methodological quality assessment
Methodological quality assessment of the included studies was carried out in JBI’s critical appraisal tool(Reference Aromataris, Fernandez and Godfrey11), which, in turn, is widely recommended for assessing observational studies. It is also worth highlighting that this tool analyzes three main domains and their sub-classifications by taking into consideration aspects linked to sample selection, comparability and determination of exposure/outcome of interest, besides its easy application and interpretation.
Statistical analyses
Meta-analyses were performed with studies that were carried out with similar pathologies and that presented similar methodology features in the evaluation and measuring units of dietary TAC to standardise the collected data. Means and standard deviations were calculated for each investigated dietary TAC analysis methodology by using the inverse variance method and the DerSimonian and Laird random effects model. Data heterogeneity was analysed through the Cochran Q test and I2 statistic. All analyses were carried out in RevMan 5.4 software (The Nordic Cochrane Centre, The Cochrane Collaboration, Denmark).
Results
Search
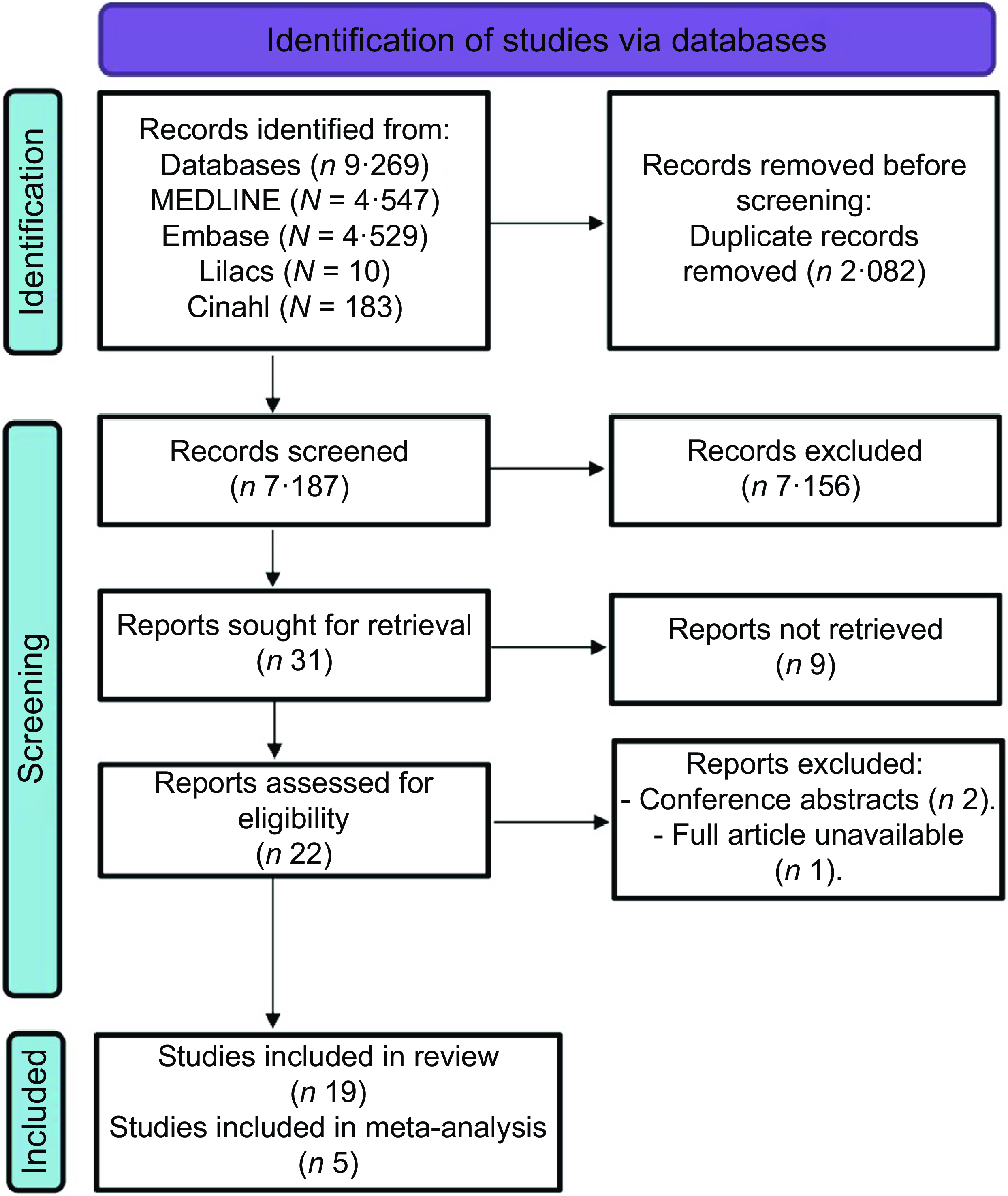
Search in the databases led to 9269 studies and 2082 of them were duplicates. In total, 7156 of the remaining 7187 studies were excluded from the review at the title-reading stage. The reviewers’ analysis included twenty-two studies in the full-text assessment. Two (2) texts were excluded from the study after the reading because they were conference abstracts, and one text was excluded because its full-text access was not allowed, not even after request to the corresponding author. In total, nineteen studies met the eligibility criteria defined for this systematic review and they remained in the study. Five (5) of them had their data included in the meta-analysis (Figure 1).
Flow chart of search and selection process.

Features of analysed studies
Fifteen of the nineteen selected articles followed the case–control design(Reference Daneshzad, Tehrani and Bellissimo8,Reference Gifkins, Olson and Demissie12–Reference Vahid, Rahmani and Khodabakhshi25) , two of them were cohort studies(Reference Han, Chung and Park26,Reference Pantavos, Ruiter and Feskens27) and two were cross-sectional research(Reference Abshirini, Siassi and Koohdani9,Reference Maugeri, Barchitta and Magnano San Lio28) . The sample size ranged from 64 to 3·209 women. Twelve (12) studies were carried out with Iranian participants(Reference Daneshzad, Tehrani and Bellissimo8,Reference Abshirini, Siassi and Koohdani9,Reference Jalali, Heidari and de Courten14–Reference Noormohammadi, Eslamian and Kazemi17,Reference Safabakhsh, Imani and Shab-Bidar19,Reference Sasanfar, Toorang and Maleki20,Reference Shoaibinobarian, Eslamian and Noormohammadi22–Reference Vahid, Rahmani and Khodabakhshi25) , two with Italian women(Reference Rossi, Tavani and Ciociola18,Reference Maugeri, Barchitta and Magnano San Lio28) , two studies were carried out with American women(Reference Gifkins, Olson and Demissie12,Reference Gifkins, Olson and Paddock13) , one research comprised Korean women(Reference Han, Chung and Park26), one article regarded residents in the Netherlands(Reference Pantavos, Ruiter and Feskens27) and one comprised women from Turkey(Reference Alkan, Artaç and Aksoy21). The main characteristics of the included studies are shown in Table 2.
Eleven (11) studies assessed dietary TAC among women with neoplasms, seven studies assessed women with breast cancer(Reference Jalali, Heidari and de Courten14,Reference Karimi, Bahadoran and Abedini16,Reference Safabakhsh, Imani and Shab-Bidar19,Reference Sasanfar, Toorang and Maleki20,Reference Vahid, Rahmani and Khodabakhshi25–Reference Pantavos, Ruiter and Feskens27) , three research assessed women with endometrial cancer(Reference Gifkins, Olson and Demissie12,Reference Rossi, Tavani and Ciociola18,Reference Maugeri, Barchitta and Magnano San Lio28) , and one article regarded women with ovarian cancer(Reference Gifkins, Olson and Paddock13). One study analysed women with bacterial vaginosis(Reference Noormohammadi, Eslamian and Kazemi17), one research assessed women with menopausal participants(Reference Abshirini, Siassi and Koohdani9) and one research involved women with PCOS(Reference Shoaibinobarian, Eslamian and Noormohammadi22). Two studies analysed pregnant women (one was about women with PE(Reference Sheikhi, Sharifi-Zahabi and Paknahad23) and the other about mothers with GDM(Reference Daneshzad, Tehrani and Bellissimo8)), one study assessed women with a history of miscarriage(Reference Vahid, Rahmani and Davoodi24) and another analysed female infertility(Reference Kabodmehri, Sadat and Alami15). One study related diet TAC to inflammation and oxidative stress serum markers in women with breast cancer(Reference Alkan, Artaç and Aksoy21). The studies used clinical examinations and diagnoses to identify the assessed comorbidities.
Five studies used oxygen radical absorption capacity (ORAC) assays to determine dietary TAC(Reference Abshirini, Siassi and Koohdani9,Reference Karimi, Bahadoran and Abedini16,Reference Safabakhsh, Imani and Shab-Bidar19,Reference Shoaibinobarian, Eslamian and Noormohammadi22,Reference Sheikhi, Sharifi-Zahabi and Paknahad23) , four studies used the dietary antioxidant index (DAI) to do so(Reference Kabodmehri, Sadat and Alami15,Reference Vahid, Rahmani and Davoodi24,Reference Vahid, Rahmani and Khodabakhshi25,Reference Maugeri, Barchitta and Magnano San Lio28) , two studies used the total radical capture antioxidant parameter (TRAP) in this analysis, as well as ferric reducing antioxidant power (FRAP) and Trolox equivalent antioxidant capacity(Reference Daneshzad, Tehrani and Bellissimo8,Reference Rossi, Tavani and Ciociola18) , three studies only used FRAP assays(Reference Noormohammadi, Eslamian and Kazemi17,Reference Sasanfar, Toorang and Maleki20,Reference Pantavos, Ruiter and Feskens27) , three studies analysed the combination of FRAP and ORAC methods(Reference Gifkins, Olson and Demissie12–Reference Jalali, Heidari and de Courten14), one study adopted the vitamin C equivalent antioxidant capacity (VCE) method(Reference Han, Chung and Park26) and one article analysed all the aforementioned methods, except for DAI(Reference Alkan, Artaç and Aksoy21). In addition, twelve of the nineteen included studies showed a close association between dietary TAC and the outcomes of interest(Reference Abshirini, Siassi and Koohdani9,Reference Gifkins, Olson and Demissie12,Reference Kabodmehri, Sadat and Alami15,Reference Karimi, Bahadoran and Abedini16,Reference Rossi, Tavani and Ciociola18,Reference Sasanfar, Toorang and Maleki20,Reference Shoaibinobarian, Eslamian and Noormohammadi22,Reference Vahid, Rahmani and Davoodi24–Reference Maugeri, Barchitta and Magnano San Lio28) .
When analysing the main outcomes of the included studies, it is possible to note that, for the most part, dietary TAC showed an influence on the prevention of the most diverse diseases related to women’s health in general. In this context, four of the seven studies assessing breast neoplasia found that women with this cancer type recorded reduced dietary antioxidants intake in comparison with those without this disease. There was a significant inverse correlation between dietary TAC and breast cancer after adjustments made in the main confounding factors, yet, a significantly lower consumption of TAC was also found among women who had a recurrence of the disease(Reference Vahid, Rahmani and Khodabakhshi25,Reference Han, Chung and Park26) .
Furthermore, three studies showed that the inverse association between dietary TAC and breast cancer risk became non-significant, after controlling the potential confounding factors, even if women are divided into pre- and post-menopausal states(Reference Jalali, Heidari and de Courten14,Reference Karimi, Bahadoran and Abedini16,Reference Safabakhsh, Imani and Shab-Bidar19) . Around endometrial neoplasia, only one of the three analysed studies observed an association between antioxidant index and endometrial lesions(Reference Maugeri, Barchitta and Magnano San Lio28), and one author did not find an association through the FRAP method, despite there being a reduction in the risk of cancer in the group with higher intake of total phenolic compounds(Reference Gifkins, Olson and Demissie12).
On endometrial cancer, Rossi et al.(Reference Rossi, Tavani and Ciociola18) observed that diet TAC is inversely related to the risk of the disease. In turn, Gifkins et al.(Reference Gifkins, Olson and Paddock13) found little evidence of the association between dietary TAC and ovarian neoplasia development. Alkan et al.(Reference Alkan, Artaç and Aksoy21) only observed a weak positive association between dietary and serum TACs in women with breast cancer, before chemotherapy.
Studying PCOS, Shoaibinobarian et al.(Reference Shoaibinobarian, Eslamian and Noormohammadi22) concluded that there is an association between those recording higher dietary TAC and with lower chance of having PCOS in comparison to female participants with and without PCOS diagnosis. Regarding infertility, Kabodmehri et al.(Reference Kabodmehri, Sadat and Alami15) also showed that women with higher DAI had a lower risk of infertility, with an inversely significant association. Around postmenopausal women, the highest TAC level were less likely to experience symptoms, such as sleep issues, anxiety, hot flashes and sweating, whereas those accounting for the lowest level were more likely to experience sexual issues(Reference Abshirini, Siassi and Koohdani9). Furthermore, a study evaluated the influence of dietary TAC and the occurrence of bacterial vaginosis; however, no relationship was observed between them(Reference Noormohammadi, Eslamian and Kazemi17).
Regarding diseases of the gestational period, the study of the relationship between the occurrence of abortion and dietary TAC observed a significant protective effect in women who have shown the highest level of dietary TAC(Reference Vahid, Rahmani and Davoodi24). Furthermore, one study looked at pregnant women and assessed those with and without GDM, where they observed that the occurrence of the disease was greater in women with lower antioxidant intake, just as a similar finding was found in cases of “PE”(Reference Daneshzad, Tehrani and Bellissimo8,Reference Sheikhi, Sharifi-Zahabi and Paknahad23) .
Studies’ methodological quality
About assessing the methodological quality of articles analysed in JBI’s critical appraisal tool, all studies about neoplasms, infections, PCOS, GDM, PE, infertility and serum biomarkers met the tool’s requirements, so their quality was considered adequate. On the other hand, one study24 did not meet important tool requirements; therefore, it was considered a low-quality article. It did not make the exemption of the exposure of interest in the control group clear, and it would have directly interfered with the recorded results, besides not reflecting the results’ complete reliability.
Meta-Analysis
FRAP: Two studies were included in the meta-analysis: 548 women with breast cancer (case group) and 728 healthy women as the control group. FRAP was not significantly different between studied groups (mean difference: −0·76, CI 95 % (–1·56, −0·05), P = 0·07; I2 = 0 % and P = 0·84) (Figure 2).
Forest plot of studies using the FRAP method to assess diets’ total antioxidant capacity, expressed in mmol/d. FRAP, ferric reducing antioxidant power.

ORAC: Two studies were included in the meta-analysis: 182 women with breast cancer in the case group and 182 healthy women in the control group. No significantly different ORAC value was observed in the groups (standard mean difference: −0·31, CI 95 % (–0·79, 0·17), P = 0·20; I2 = 68 % and P = 0·08) (Figure 3).
Forest plot of studies using ORAC method to assess diets’ total antioxidant capacity expressed in umolTE/100 g. ORAC, oxygen radical absorption capacity.

VCE: Two studies were included in this analysis: 98 women with breast cancer in the case group and 569 healthy women in the control group. Vitamin C equivalents’ levels were significantly lower in the case group than in the group of individuals without diseases (mean difference: −110·53, CI 95 % (–171·53, −49·52), P < 0·001; I2 = 0 % and P = 0·38) (Figure 4).
Forest plot of studies using the Vitamin C Equivalent method to assess diet’s total antioxidant capacity.

Discussion
This systematic review, complemented by meta-analysis, provides a comprehensive view of the association between dietary TAC and various health conditions affecting women. Although not all studies were included in the quantitative analysis due to methodological reasons, the findings demonstrate that dietary TAC levels are significantly lower in women with diseases compared to the control group. This outcome reinforces dietary antioxidant intake’s influence on preventing conditions affecting women’s health. In addition, diversity in study designs highlights the broad approach adopted to explore this association, as well as sample size extension – ranging from 64 to 3209 women – which raises questions about the general profile and robustness of the current findings. These results make it crucial to take into consideration the representativeness of the assessed population.
Studies’ geographic distribution shows the majority of research was carried out with Iranian participants, as well as with Italian, American and Korean women and with residents in the Netherlands and Turkey, which raises questions about cultural and environmental factors’ influence on the diet TAC/female health association. Accordingly, the analysis applied to the assessed populations highlights the global exploration of the association between dietary TAC and several women’s health conditions, such as the history of miscarriage, bacterial vaginosis, menopause, PCOS, complicated pregnancies (PE and GDM), infertility and cancer (breast, endometrium and ovary).
Four of the seven studies assessing breast neoplasia found that women with this cancer type recorded reduced dietary antioxidants intake in comparison to those without this disease. There was a significant inversed correlation between dietary TAC and breast cancer after adjustments made in the main confounding factors, yet, a significantly lower consumption of TAC was also found among women who had a recurrence of the disease(Reference Vahid, Rahmani and Khodabakhshi25,Reference Han, Chung and Park26) . Furthermore, the number of participants in the highest dietary TAC quartile was 0·39 times less likely to have the aforementioned disease than those in the lowest quartile(Reference Sasanfar, Toorang and Maleki20). Pantavos et al.(Reference Pantavos, Ruiter and Feskens27), in their turn, noticed that moderate and high dietary FRAP (≥18·01 mmol/d) led to a lower risk of developing breast cancer than low dietary FRAP after adjustments made to potential confounding factors.
However, three studies showed that the inversed association between dietary TAC and breast cancer risk became non-significant, after controlling the potential confounding factors, even if women are divided into pre- and post-menopausal states(Reference Jalali, Heidari and de Courten14,Reference Karimi, Bahadoran and Abedini16,Reference Safabakhsh, Imani and Shab-Bidar19) . Only one of the three analysed studies on endometrial neoplasia observed an association between antioxidant index and endometrial lesions(Reference Maugeri, Barchitta and Magnano San Lio28). Another author has not found this association through the FRAP method, but cancer risk was reduced among the highest tertile of total phenolic compound intake in comparison to the lowest one, after using the ORAC database and making adjustments in the main covariates(Reference Gifkins, Olson and Demissie12).
Rossi et al.(Reference Rossi, Tavani and Ciociola18) also found correlations, such as diet TAC inversely related to the risk of endometrial cancer and risk between the lowest and highest quartile, in all analysed methods (FRAP, Trolox equivalent antioxidant capacity and TRAP). However, Gifkins et al.(Reference Gifkins, Olson and Paddock13) found little evidence of an association between dietary TAC and ovarian neoplasia development. Alkan et al.(Reference Alkan, Artaç and Aksoy21) only observed a weak positive association between dietary and serum TACs in women with breast cancer, before chemotherapy, when it comes to the association among dietary TAC and inflammation serum biomarkers (tumour necrosis factor alpha, interleukin 1β and interleukin 6) and oxidative stress (malondialdehyde, protein carbonyl and total oxidising state).
Shoaibinobarian et al.(Reference Shoaibinobarian, Eslamian and Noormohammadi22) concluded that there is an association between those recording higher dietary TAC and with lower chance of having PCOS in comparison to female participants with and without PCOS diagnosis. Kabodmehri et al.(Reference Kabodmehri, Sadat and Alami15) also showed that women with higher DAI had a lower risk of infertility, with an inversely significant association. Likewise, a cross-sectional study carried out with postmenopausal women assessed the dietary TAC/menopausal symptoms association and observed that women presenting the highest TAC level were less likely to experience symptoms, such as sleep issues, anxiety, hot flashes and sweating, whereas those accounting for the lowest level of it were more likely to experience sexual issues(Reference Abshirini, Siassi and Koohdani9).
Researchers have shown a positive association between menopausal symptoms and increased risk of chronic diseases and oxidative stress, mainly due to oestrogen deprivation. This outcome highlights the importance of controlling these symptoms through likely modifiable factors, such as diet and overall intake of antioxidant nutrients(Reference Abshirini, Siassi and Koohdani9,Reference Abshirini, Siassi and Koohdani29,Reference Cagnacci, Cannoletta and Palma30) . The possible explanation for such mechanisms linking antioxidant intake to menopausal symptoms reduction lies in higher antioxidant status caused by diets rich in these nutrients, which leads to increased dietary TAC. Furthermore, these diet types count on abundant amounts of phytoestrogens lignans and isoflavones, which are plant-derived oestrogens less powerful than estradiol, but that are capable of binding to the oestrogen receptor and reducing hot-flashes severity and frequency(Reference Abshirini, Siassi and Koohdani9,Reference Thompson, Boucher and Liu31,Reference Canivenc-Lavier and Bennetau-Pelissero32) .
PCOS is primarily an endocrine disorder with gynaecological implications, where oxidative stress plays a key role its development, due to insulin resistance and hyperglycaemia commonly associated with this condition(Reference Shoaibinobarian, Eslamian and Noormohammadi22). Therefore, researchers have pinpointed that oxidative stress decrease is positively related to more mature oocytes in infertile PCOS women. Thus, food types rich in antioxidants can protect the body from oxidative damage in these patients. Recent data also suggest that high dietary TAC can reduce PCOS changes(Reference Shoaibinobarian, Eslamian and Noormohammadi22,Reference Combelles, Gupta and Agarwal33,Reference Noormohammadi, Eslamian and Malek34) .
A case–control study aimed at assessing the DAI/chances of miscarriage association and observed significant protective effects in women who showed the highest level of dietary TAC in comparison to those who did not, after crude and multivariate data adjustments were made(Reference Vahid, Rahmani and Davoodi24). Regarding PE, women with the disease had significantly lower dietary TAC than pregnant women without this comorbidity, after adjustments made to the main risk factors, such as energy and pre-pregnancy BMI. Nonetheless, no association was observed between TAC intake and PE risk(Reference Sheikhi, Sharifi-Zahabi and Paknahad23).
The literature points out that women with GDM present increased oxidative stress biomarkers and reduced antioxidant activity after the analysis of the association between gestational disorders, such as PE and GDM, and dietary TAC. This finding suggests an imbalance during pregnancy, as shown in the study by Mandani et al. in 2021(Reference Mandani, Badehnoosh and Jalali-Mashayekhi35). Two studies looked at pregnant women and assessed those with and without GDM. They found that FRAP intake was significantly lower in the case group than in the control and that GDM risk was 85 % lower among women in the highest FRAP tertile. However, there was no significant association between GDM risk and TRAP and Trolox equivalent antioxidant capacity methods(Reference Daneshzad, Tehrani and Bellissimo8).
Another case–control study sought to investigate the dietary TAC/bacterial vaginosis association. However, vaginosis odds were not associated with total antioxidant intake. This finding disregarded age, BMI, waist circumference, number of cigarettes per day, pregnancy frequency and exercise(Reference Noormohammadi, Eslamian and Kazemi17).
These results raise important reflections to help better understand dietary TAC and its implications for women’s health outcomes, to provide a solid starting point for more in–depth discussions about this complex association and its clinical outcomes. Furthermore, the whole variety of assessed conditions highlights the complexity of dietary TAC’s influence on women’s health, and it suggests that different antioxidant mechanisms may play specific roles in distinct contexts.
Five articles were suitable for the quantitative meta-analysis because they presented similar, or likely standardisation methodologies and pathologies. The included studies produced current evidence of the association between dietary TAC and breast cancer. Breast cancer demonstrated strong epidemiological evidence when dietary TAC was assessed using vitamin C equivalents, showing that the total antioxidant intake in women with the disease is significantly lower than in healthy women. This suggests that a low consumption of antioxidant-rich foods may be associated with a higher risk of developing this oncological condition. Conversely, when dietary TAC was evaluated using the FRAP and ORAC methods, no significant associations were observed.
The findings highlight a critical relationship between dietary TAC and breast cancer risk, underscoring the potential role of antioxidants in disease prevention. These dietary TAC/neoplasms association is well established in the literature. The meta-analysis carried out with twenty-one studies, and another one conducted with nineteen studies, have concluded that high dietary TAC has a protective effect against these diseases, since it reduces the incidence of breast, endometrial, colon, gastric and lung cancer(Reference Abbasalizad Farhangi and Vajdi36,Reference Parohan, Sadeghi and Mahdavi37) . The pathophysiology of neoplasms can explain this association, since it involves the secretion of cytokines and inflammatory mediators, such as TNF-α and leptin. This process increases oxidative stress and tissue damage(Reference Lopes, Cruz and Rocha Sobrinho38); therefore, antioxidant vitamins act in ruling out/neutralising reactive oxygen species, increasing antioxidant capacity and reducing cellular oxidative damage(Reference Phan, Paterson and Bucknall39).
The observed lower dietary TAC in women with breast cancer could reflect dietary patterns characterised by insufficient consumption of fruits, vegetables and other antioxidant-rich foods. This underscores the importance of dietary quality in cancer prevention strategies and highlights a potential area for public health interventions aimed at promoting antioxidant-rich diets. Moreover, the results may also suggest that vitamin C equivalents capture relevant aspects of antioxidant intake more effectively than other methods, such as FRAP and ORAC, again raising questions about the variability of these assays in assessing dietary antioxidants, as they focus on distinct chemical reactions and target compounds. These discrepancies also could highlight the complexity of the antioxidant system, where interactions between multiple compounds and pathways influence the overall protective effect.
Future research should delve deeper into the methodological differences between these assessments to determine which most accurately reflects biologically active antioxidant capacity related to cancer risk. In addition, longitudinal studies and intervention trials are needed to explore whether increased consumption of antioxidant-rich foods reduces the incidence or progression of other diseases related to women’s health, as few studies have been conducted on this topic, limiting scientific knowledge on the subject.
These findings also emphasise the need for personalised dietary recommendations, as individual variations in metabolism, genetics and lifestyle can modify the impact of antioxidants on cancer risk. Understanding these nuances may pave the way for more targeted approaches to prevention, ensuring that dietary strategies are effective and tailored to individual needs.
It is crucial to recognise and consider some limitations inherent to the assessed studies, such as the diversity of methods used to determine dietary TAC, including assays like ORAC, DAI, TRAP, FRAP, Trolox equivalent antioxidant capacity and VCE, after analysing the results in the present systematic review, complemented by meta-analysis. This finding underscores the need for methodological standardisation, as the chosen methods can influence the consistency of results and comparability between studies.
Conclusion
It is possible to conclude that, despite methodological differences used in studies included in the present literature review, dietary TAC was lower in individuals in the disease groups than in those belonging to the control group. This finding reflects the consequences of eating habits based on low fruit and vegetable consumption, which are the main antioxidant-source food types and it also highlights the relevance of ingesting these compounds in regular diets to prevent conditions affecting health, both in the short- and long terms.
Furthermore, it is recommended that further studies focus on a deeper understanding of the mechanisms underlying the effects of dietary TAC on women’s health conditions and that health policies be developed to promote adequate consumption of foods that are sources of antioxidants, aiming to improve health and prevent diseases.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114525000443
Acknowledgements
This work was supported by the Alagoas State Research Support Foundation (FAPEAL); the Brazilian public resources from the National Council for Scientific and Technological Development (CNPq) and the Coordination for the Improvement of Higher Education Personnel (CAPES).
A. R. B., M. B. T. F., T. A. D. and T. M. W. performed data extraction and analysis and wrote the manuscript. A. C. M. O. and N. B. B. contributed to the study conception and design and manuscript writing. All authors contributed to the article’s critical review and final manuscript approval.
The authors declare no conflict of interest.