


Mental health policy has increasingly directed that, whenever possible, people with severe mental health problems should receive treatment ‘in the community’ while living at home. In parallel, legal mechanisms for compulsory out-patient treatment have been introduced in many countries, usually as part of civil mental health laws. Some of the first such regimes for community treatment orders (CTOs, also called ‘out-patient commitment, ‘mandatory out-patient care’ or ‘assisted out-patient treatment’) were developed in the USA and were generally considered to have strengthened civil liberties by enabling treatment outside asylums. Reference Churchill, Owen, Singh and Hotopf1 Over time, concerns have been raised that CTOs contribute to a ‘net widening’ of coercive practices, Reference Churchill, Owen, Singh and Hotopf1 and the proportionality of restricting the liberty of individuals who have not committed a crime was questioned. CTOs typically mandate that the person must adhere to treatment, accept clinical visits and attend appointments or assessments. Some must live at a specified address, or are required to stay away from certain areas, institutions or individuals due to perceived risks to others. Reference Churchill, Owen, Singh and Hotopf1,Reference Dawson2 Should the condition of someone under a CTO deteriorate, they may swiftly be returned to hospital. To enforce this, health professionals sometimes have the power to enter someone’s property or summon police assistance to bring the person to a hospital or clinical setting where they may be administered treatment, using physical force if required. Reference Dawson2,Reference Dawson, Kelly and Donnolly3 Many of those subjected to CTOs report that the regimes are disproportionally coercive and oriented towards psychotropic medication and supervision that they do not want and experience as harmful or burdensome, rather than helping with recovery. At the same time, the safeguard and structure of the order are considered helpful by some. Reference Corring, O’Reilly and Sommerdyk4
The structure and functions of CTO frameworks have been described in different ways. Geller Reference Geller5 outlines five legislative positions on compulsory out-patient care: (a) not permitting such compulsion; (b) allowing it without specific statute or (c) without enforcement powers; (d) permitting in- and out-patient compulsion under the same criteria and with set enforcement powers; and (e) setting a different, usually lower, threshold for out-patient compulsion. The last two positions are relevant to how Churchill and colleagues Reference Churchill, Owen, Singh and Hotopf1 describe different functions of CTO regimes that are used to legitimise their use. ‘Least restrictive’ regimes typically have the same legal criteria as involuntary admission, with the aim to treat a condition already deteriorated in the community, which is presumed less restrictive than the hospital setting. ‘Preventative’ regimes, on the other hand, have lower legal thresholds for out-patient than for in-patient compulsion, with the aim to prevent (further) deterioration or (further) danger, and the CTO is considered a tool in the management of the person. Reference Churchill, Owen, Singh and Hotopf1 Dawson Reference Dawson2 points out several ways in which CTO regimes differ that relate to their restrictiveness. Whereas ‘first-generation’ CTOs tend to specify requirements (such as having to adhere to treatment) and powers (such as whether or how clinicians can enter someone’s house), ‘second-generation’ CTOs rely on treatment plans that tailor specific conditions to the individual, which clinicians then have powers to enforce. Reference Dawson2 Regimes also differ in regard to whether decision-making capacity forms a legal criterion so that only those without it can be subjected to CTOs. There are also differences regarding whether regimes permit CTOs following someone’s first-ever admission or while that person is in the community, which might indicate ambitions for prevention or least restrictive setting, respectively. Although reinforcement mechanisms differ, Dawson argues that all statutes and commentators concur that authorising clinicians to ‘restrain and medicate’ in people’s own homes is a ‘Rubicon not to be crossed’. Reference Dawson2
It is a general legal principle that interventions in the private sphere must be proportional and exercised within a legal framework that promotes accountability and fairness and protects citizens’ rights. Although conceptualisations of CTOs vary, their intrusiveness continues to raise human rights concerns. Reference Dawson, Kelly and Donnolly3 These are reflected in international frameworks, most notably the Convention on the Rights of People with Disabilities (CRPD), which expects governments to minimise, or eradicate, their use because they undermine the right to self-determination. 6 Others argue that the right to treatment in some situations weighs more heavily than freedom from restrictions. Reference Kelly, Kelly and Donnelly7 Ethical analyses of the justification of CTOs differ in their conclusions, with some being more in favour Reference Muntez, Galon and Frese8 than others, Reference Newton-Howes and Matthewson9 although most argue that their ethics are contingent on highly targeted and restricted use. Ethical arguments often hinge on whether CTOs are perceived to confer benefits that outweigh their restrictiveness and potential harm, Reference Churchill, Owen, Singh and Hotopf1 making the evidence base relevant to different positions. Most scholars agree that relevant outcome measures used to assess the beneficial effects of CTO include readmission to hospital and adherence to, and use of, community services. Systematic reviews and meta-studies of the sizeable but heterogenous body of research investigating these outcomes find no advantage of CTOs over ordinary follow-up. Reference Kisely, Campbell and O’Reilly10,Reference Barnett, Matthews, Lloyd-Evans, Mackay, Pilling and Johnson11 Newer individual studies suggest potential benefit to those with non-affective psychoses. Reference Segal12 Some argue, however, that CTOs should be measured on how they manage dangerousness in the community. Reference Kisely, Bull, Newton-Howes, Zirnsak, Edan and Lawn13 Less evidence is available on such outcomes, but one meta-analysis found no beneficial effects on criminal behaviour, violence or aggression. Reference Kisely, Bull and Gill14
Despite all high-level evidence pointing in the same direction, debates about CTO effectiveness, and its ethical justification, continue. Nonetheless, more than 80 CTO regimes form part of mental health legislation worldwide. Most jurisdictions in North America and Australia have such provision, along with a number of European countries. Reference Rugkåsa, Molodynski, Burns, Molodynski, Rugkåsa and Burns15 CTOs also exist in countries as diverse as Gibraltar, Taiwan, Samoa and Uganda, Reference Rugkåsa, Molodynski, Burns, Molodynski, Rugkåsa and Burns15 and are under consideration in others, such as Hong Kong. Given their widespread use, it is somewhat surprising that very little research has compared the content of CTO statutes. Our literature search to identify studies comparing European regimes (see the supplementary material available at https://doi.org/10.1192/bjo.2026.12015) found that four European regimes (England & Wales, Israel, Scotland and Switzerland) have been included in previous comparisons. This included a 2007 systematic review comparing international regimes, Reference Churchill, Owen, Singh and Hotopf1 and several legal analyses of Commonwealth regimes. Reference Dawson2,Reference Dawson, Kelly and Donnolly3,Reference Dawson16
We found no up-to-date study describing the availability and restrictiveness of CTO regimes across several European countries. To clarify, by restrictiveness we mean how, and the degree to which, a CTO limits the person’s actions, rights or freedoms. This is, in turn, relevant for assessing the proportionality of such orders, which implies that restrictions or negative consequences should not outweigh potential benefits. In the present analysis we seek to address gaps in the literature in this regard. Through this, we aim to shape future empirical work on the functioning, effect and ethics of out-patient compulsion, and to inform current debates and policy-making in contexts where CTOs are being considered.
Specifically, we aim to ascertain (a) which countries permit CTOs, and a range of issues related to CTO restrictiveness as enshrined in law, including (b) procedures and legal thresholds for initiation and renewal, (c) specified restrictions placed on the person and (d) powers to enforce them. Our focus is on how CTOs are conceived in law – that is, the letter of the law, and not its interpretation or application.
Method
We report from the Fostering and Strengthening Approaches to Reducing Coercion in European Mental Health Services (FOSTREN) Law and Policy Project, conducted by the EU-funded European Cooperation in Science and Technology (COST)-Action (ref. no. 19133). This was a network of clinicians and researchers established across 33 member countries, dedicated to understanding the dynamics surrounding the use of coercive practices. We constructed a survey to collect information on relevant legislation and policy across these countries. This was piloted (in Portugal, Finland and Montenegro) and amended before being sent to country representatives to arrange completion locally. Details about the development and methodology, including the full survey, are reported elsewhere. Reference Aluh, Lantta, Lourenço, Birkeland, Castelpietra and Dedovic17
Data collection took place between July 2023 and September 2024. In our letter to respondents, it was clear that participation was voluntary. The return of a completed survey was considered implicit consent to participate. We encouraged respondents to involve local experts in completing the survey, and to provide weblinks to relevant documents. We obtained data on the full survey from 28 countries. For the purposes of the present analysis, we subsequently contacted people in the network from the remaining five countries to ascertain whether CTOs were part of their legislation, and obtained data where it was. The analysis is thus based on all 33 eligible countries.
We defined CTO regimes as mechanisms, specified in the letter of the law, for compulsory community care of adults with severe mental health problems. We excluded regimes based on case law or legal interpretation. We also excluded forensic CTOs, under which having committed a crime is a reason for the restrictions. Regimes that commit the person to live in community-based residential care, but where they cannot freely take part in community life and activities, were also excluded.
Data on CTO regimes included year of introduction and, where relevant, year of last amendment; legal criteria for using CTOs and whether these differ from the criteria for involuntary admission; whether CTOs can be initiated when the person resides in the community and after their first-ever admission; the duration of the initial order; whether renewals are possible and, if so, for how long and by which procedures; whether legal safeguards for CTOs are the same as those for involuntary admissions; and how CTOs can be terminated. We further asked whether the law specifies that the person must make themselves available for assessments; attend regular meetings with clinicians; take medication; and live on a specified address. We also asked whether conditions tailored to the individual may be specified in the order or in a treatment plan and, if so, whether adherence to this plan is a specified requirement. Finally, we asked how the laws specify enforcement powers.
Law texts are drafted in specific contexts and legal traditions. On occasion, this made it difficult for respondents to classify items into pre-specified categories. To enhance data quality we accessed available legal frameworks online, translated relevant sections using online tools (Google Translate and ChatGPT) and consulted the existing literature. We then conducted a thorough member check of draft results by getting respondents to help clarify information, correct apparent errors or provide additional contextual information.
The study is based at Akershus University Hospital, Norway. Following the decision of the Regional Ethics Committee that the study was outside the scope of the Norwegian Health Research Act (ref. no. 616738), the protocol was approved by the hospital’s Privacy Ombudsman (ref. no. 2023_85).
Results
Availability of CTO regimes in the 33 countries surveyed
Figure 1 shows that the following countries have CTO regimes: Belgium, Bulgaria, France, Israel, Malta, the Netherlands, Norway, Portugal, Slovenia and Sweden. The UK is divided into three jurisdictions, of which two, England & Wales and Scotland, have CTOs. In Switzerland CTOs are permitted by federal law (which is what is referred to below, unless otherwise specified), but the 26 cantons have legislative power to specify the detail and power of local regimes. Counting Switzerland as one jurisdiction, there are 13 CTO regimes across the 33 countries.
Availability of community treatment order (CTO) regimes across 33 eligible FOSTREN (Fostering and Strengthening Approaches to Reducing Coercion in European Mental Health Services) countries.

Fig. 1 Long description
The map of Europe highlights countries with and without community treatment orders (CTOs) in their mental health law. The 33 participating European countries are marked in dark blue if they have CTO legislation, and those without are marked in light green. This visual representation helps to understand the distribution of CTO legislation across Europe.
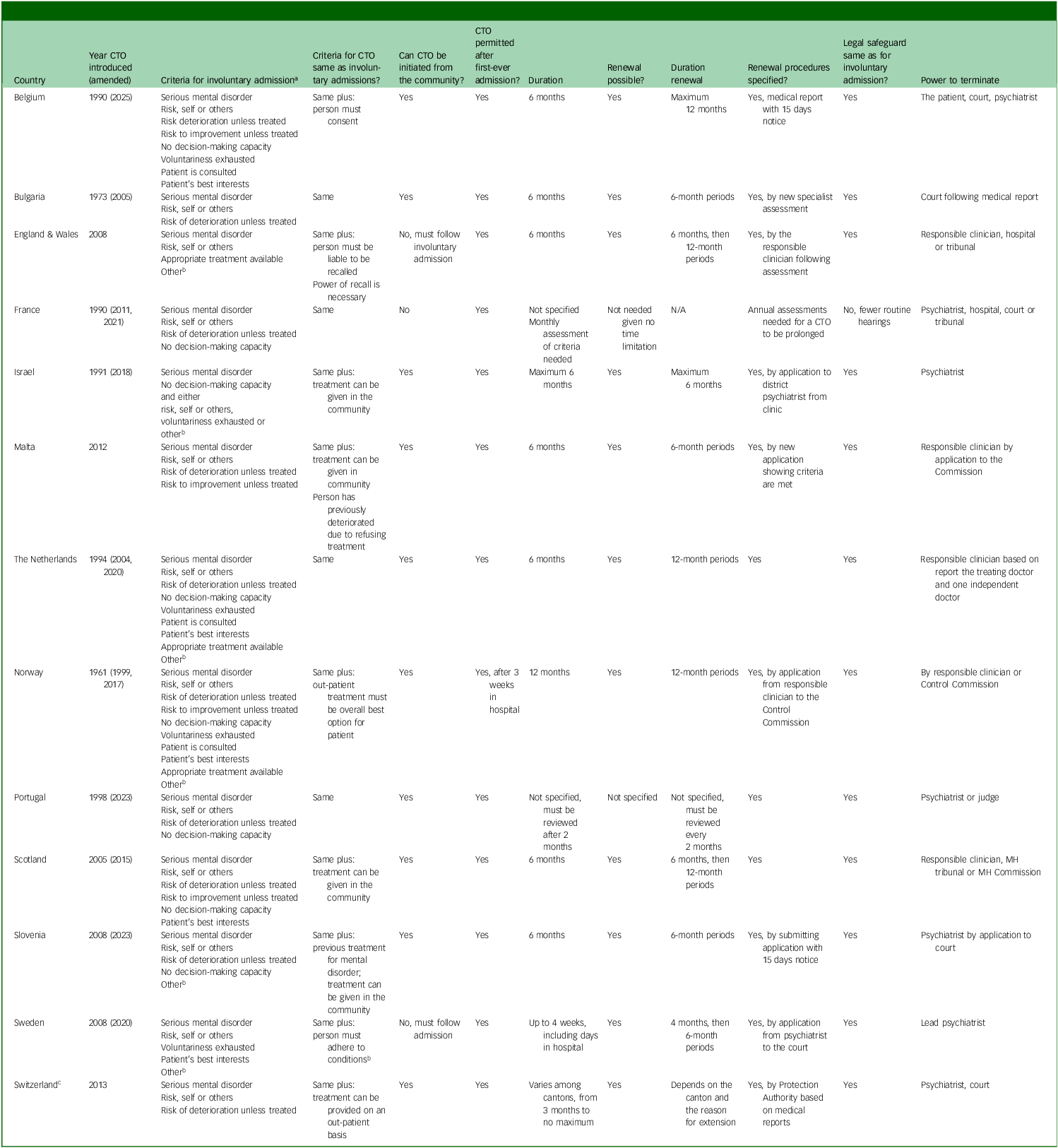
As shown in Table 1, Bulgaria and Norway were early adopters (1973 and 1961, respectively), with others following suit in the 1990s and the remaining half between 2005 and 2012. CTOs were introduced in Swiss federal law in 2013, although some cantons had arrangements prior to that. Most regimes have been amended since their introduction, ten within the past decade.
Criteria for community treatment order (CTO) placement and legal specification for initiating and maintaining orders in 13 European jurisdictions

Table 1 Long description
A table comparing criteria for community treatment order (CTO) placement and legal specifications for initiating and maintaining orders in 13 European jurisdictions. The table includes columns for year CTOs commenced, how criteria for CTO placement match criteria for involuntary admission, whether CTO can be initiated from the community and following someone’s first ever admission, CTO duration, renewal provisions, and formal procedures for termination. The table has 13 rows, each representing a different jurisdiction, and 7 columns detailing specific criteria and legal specifications. Notable trends include variations in the year CTOs commenced, with Bulgaria and Norway being early adopters in 1961 and 1973, respectively, and other countries following in the 1990s and 2000s. The table also shows differences in the criteria for CTO placement, duration, and renewal provisions across jurisdictions.
N/A, not available.
a. Criteria for involuntary admission are phrased differently across contexts. We asked respondents to classify these in the following categories: 1, evidence of serious mental disorder; 2, risk of harm to self or others; 3, substantial risk of serious deterioration in the patient’s condition if treatment is not given; 4, risk of reducing the likelihood of substantial improvement in the patient’s condition if treatment is not given; 5, the patient lacks decision-making capacity; 6, voluntariness has been exhausted/is futile; 7, the patient has been consulted; 8, the admission is considered in the patient’s best interest; 9, appropriate treatment is available; 10, other.
b. Other: Israel, ability to look after basic needs is severely impaired; causing anguish to others; causing severe damage to property. The Netherlands, no less restrictive option to prevent harm is available. Portugal, the criteria related to risk specify that these are connected to the refusal of medically prescribed treatment. Sweden, indispensable need for psychiatric care that can be met only in a hospital setting is required for involuntary admission, and for CTOs this is replaced with a criterion that the person needs to comply with specific conditions to accept the necessary psychiatric care. Slovenia, for involuntary admission there must be no less restrictive option available to prevent harm, such as voluntary admission, out-patient treatment or CTO.
c. Federal law, within which the 26 cantons have their own specified CTO regimes.
The remaining countries surveyed that do not have CTO legislation, as conceptualised here, are Austria, Bosnia & Herzegovina, Croatia, Cyprus, Czech Republic, Denmark, Estonia, Finland, Germany, Greece, Ireland, Italy, Latvia, Moldova, Montenegro, North Macedonia, Northern Ireland (the third UK jurisdiction), Poland, Romania, Slovakia, Spain and Turkey. Two of these previously had CTO legislation: in Latvia, CTOs were part of mental health legislation between 1997 and 2007 and in Denmark between 2010 and 2019. Whereas Italian legislation does not include CTOs, in some regions Trattamento Sanitario Obbligatorio Extraospedaliero are used in exceptional cases to administer medication in the community, based on permissive interpretation of mental health laws. Similarly in Spain, legal interpretation by several provincial courts allows the operation of ad hoc schemes. Forensic CTOs and compulsory community residential care also exist in some of the surveyed countries.
Criteria and regulations for making and renewing CTOs
As shown in Table 1, the criteria for CTO placement are the same as those for involuntary admissions, but nine countries have additional criteria. Most of these specify that community treatment must be available or feasible. Previous contact with services is an additional requirement in Malta, and also in Slovenia where the 2023 amendment changed the relevant threshold from ‘previous admission’ to ‘previous service use’. The Belgian regime was amended in 2024 (effective from 2025), with CTOs here entitled Traitement volontaire sous conditions, and these require the person’s consent.
Evidence of ‘mental disorder’ and risk of harm to self or others are criteria across all legislations. There must also be a need for treatment to prevent deterioration or enable substantial improvement, except in Sweden and Israel. Eight jurisdictions specify lack of decision-making capacity as a criterion for CTOs. CTOs may be initiated from the community setting, except in Sweden, England & Wales and France, where the order must follow from an involuntary admission. A CTO following someone’s first-ever admission is permitted in all jurisdictions.
CTOs may commonly last up to 6 months, with some countries setting a limit to around 1 month and others not specifying a period. Renewing or prolonging the order is possible in all countries. Six-month renewal periods are the most common, and renewals may typically continue indefinitely. Procedures for renewals, where specified, involve clinical assessments – in some places in conjunction with a court decision.
Legal safeguards are the same for CTOs as for involuntary admissions in all jurisdictions, except in France where there are fewer routine hearings. CTO termination usually requires a clinical assessment, but in some places it is a court or tribunal decision either based on clinical reports or following appeals from the person or interested parties. In several countries, CTOs may be ended by some or all of these means and in Belgium, the person may withdraw consent and end the order that way (unless there is imminent risk).
Restrictions imposed by CTOs and powers to enforce them
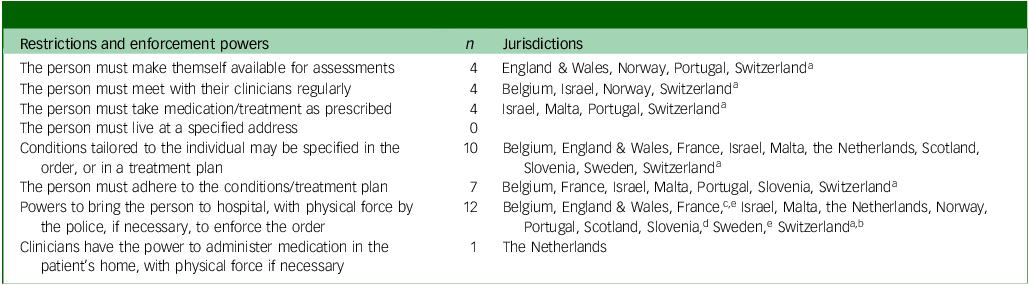
As shown in Table 2, the stipulated obligations on persons subjected to a CTO, and the powers vested in clinicians to ensure that this happens, vary across countries. Bulgaria is the only country where this is not specified.
Restrictions and enforcement powers as specified in community treatment order (CTO) legislation in 13 European jurisdictions

Table 2 Long description
The table compares restrictions and enforcement powers specified in community treatment order (CTO) legislation across 13 European jurisdictions. It lists various obligations for persons under CTOs and the powers given to clinicians to ensure compliance. The table has 7 rows and 3 columns. The first column lists different restrictions and enforcement powers, the second column shows the number of jurisdictions that apply each restriction, and the third column lists the specific jurisdictions. Notable trends include the variation in the number of jurisdictions applying each restriction, with some restrictions being more commonly applied than others. Bulgaria is the only country where these restrictions are not specified.
a. Varies among cantons.
b. Only by decision of the protection authority.
c. If the CTO is initiated by the regional administration, the patient may be brought to hospital by force when a psychiatrist’s recall order has been made. If the order is initiated by the person’s family, the police are not involved and, although a certificate may authorise the use of force, health professionals are not in a position to put this into effect.
d. If the situation is not urgent, rather than bringing the person to hospital by force, a proposal for an involuntary admission can be made, including a second opinion assessment, for the court to consider.
e. Specifies only when there is risk or following a judicial order. Non-compliance with conditions does not give sufficient cause to intervene with force.
Four regimes stipulate that a person under a CTO must stay in contact with their treatment team, and four specify when the person must make themselves available for assessments (e.g. when renewal is considered or to seek a second opinion). None of the regimes states that the person must live at a specified address. Four laws specify an obligation to accept treatment or medication as prescribed, whereas the Norwegian regime requires a separate involuntary treatment order, additional to the CTO, to insist on medication.
In ten regimes, restrictions are tailored to the person, either as specified conditions of the order (such as in England & Wales and Sweden) or as part of individual treatment plans, but only seven regimes specify that these plans must be adhered to. The specificity of care plans varies. The Maltese regime provides an example of how detailed plans must accompany a CTO application, specifying named personnel tasked with follow-up, the medicines prescribed, appointment schedules and other aspects of care. In Belgium the person must be involved in making the treatment plan to which they consent. Regular review of treatment plans is required in many countries. In England & Wales, the responsible clinician has authority to alter the individualised conditions without consultation.
In all countries, the person subjected to CTO may be ordered to return to hospital when deemed clinically necessary. Some regimes, such as the French and the Swedish, state that non-compliance per se is an insufficient ground for return: instead, clear signs of deterioration must be documented. Eleven countries specify that the police may be involved if needed to return the person to a clinical setting or safe place. Some regimes (e.g. Malta and England & Wales) include powers for brief recall (for up to 24 and 72 h, respectively) for assessment when there is concern, after which the person either returns to the community under the CTO or is admitted to hospital. As the only jurisdiction, and following a legal change in 2020, Dutch law states that all coercive measures permissible in the hospital setting are also permissible in the homes of those under a CTO, including clinicians administering medication by physical force.
Discussion
Among the 33 surveyed countries, all 5 legislative positions on compulsory out-patient care described by Geller Reference Geller5 are represented. First, 20 countries do not have a provision for CTOs according to our definition. Second, some areas of Italy and Spain appear to practise community compulsion based on legal interpretation. Third, Bulgaria has CTO provision but enforcement powers are not specified. Fourth, 11 regimes permit both hospital and community compulsion under the same criteria, although additional criteria surrounding appropriateness and feasibility apply in 9 of these. In regard to the fifth position, the Belgian regime can be interpreted as having different standards for out-patient compared with in-patient compulsion, in that patients need to consent to a CTO, suggesting a higher threshold.
We examined different aspect of legislation related to CTO restrictiveness, including legal criteria, duration, safeguards, obligations on the person and enforcement mechanisms. The legal criteria for CTO generally match those for involuntary admission and are similar across the 13 identified regimes (counting Switzerland as one jurisdiction); this aligns with previous international studies. Reference Churchill, Owen, Singh and Hotopf1–Reference Dawson, Kelly and Donnolly3 Regarding whether a lack of decision-making capacity is a criterion for CTO, five countries in our sample permit CTOs for people with such capacity and eight do not. Following the CRPD, decision-making capacity has emerged as a key point of contention in debates about the justification of coercive practices. Reference Dawson, Kelly and Donnolly3,6,Reference Kelly, Kelly and Donnelly7 Capacity-based regimes are often considered better aligned with the CRPD because they protect the autonomy of those with capacity but also ensure the right to care for those without. It is far from clear, however, that having a capacity criterion implies the same thresholds for compulsion. Whereas Belgian, Israeli, Scottish and Slovenian laws state that significantly impaired capacity suffices, Norwegian law specifies that the lack of capacity must be ‘manifest’, and the French regime presumes that the mental disorder prevents the person from giving valid consent.
Legal oversight and safeguards are present in all regimes, usually the same as for admissions. Although tribunals/courts and/or oversight bodies are often instrumental in determining when an order should be renewed or terminated, decisions are based on clinical assessments typically made by the treating or lead psychiatrists. Previous studies have found close alignment between clinical recommendations and tribunal decisions, which may be interpreted as agreement on the threshold for CTOs Reference Rugkåsa, Yeeles, Koshiaris and Burns18 or that clinicians’ views usually prevail. Reference Zetterberg, Sjostrom and Markstrom19
The lack of specified duration of a CTO in some jurisdictions, and with no limits to the potential number of renewals in most, indicates that individuals, on clinical discretion, can remain under this form of compulsion for very long periods. Studies show that CTOs often last for years. Reference Barkhuizen, Cullen, Shetty, Pritchard, Stewart and McGuire20 From the viewpoint of clinicians, fear of (legal) ramifications of not imposing or maintaining a CTO for someone who might represent present or future danger could lead to ‘defensive practice’ Reference Fisk21 and thereby a driver for a prolonged CTO. From the perspective of those with lived experience of being under a CTO, not knowing how long the order – and its restrictions – are going to last is reported as an additional burden. Reference Stensrud, Høyer, Granerud and Landheim22 The stress associated with such uncertainty might therefore have implications for assessing the proportionality of the measure.
Half of the regimes investigated specify obligations on the person to adhere to clinical follow-up. Ten regimes in addition, or instead, tailor restrictions based on the individual situation. The limited number of studies on such tailored restrictions suggests that these mainly concern medication and contact with services, and to a lesser extent residency (distance to institutions or named individuals were not mentioned). Reference Rugkåsa, Yeeles, Koshiaris and Burns18,Reference Zetterberg, Sjostrom and Markstrom19 Second-generation regimes can be seen as better aligned with human rights frameworks because they do not impose blanket restrictions on everyone under a CTO. At the same time, having restrictions specified in treatment plans means that their implications on personal liberty, and thus their proportionality, are less transparent and open to scrutiny. Reference Dawson2
Most regimes allow enforcement of CTOs by ordering the person to attend hospital, with police assistance if necessary, which adds to their coercive nature. As the only regime, the Dutch have ‘crossed the “Rubicon”’ Reference Dawson2 of authorising clinicians to use physical force outside of a clinical setting. Prior to the 2020 legal change that introduced this, views among clinicians were mixed and concerns were raised regarding the practicalities and safety of applying such powers. Reference de Waardt, van der Heijden, Rugkåsa and Mulder23 The limited research that has subsequently been conducted shows that force occasionally is used in people’s homes, and this is described by those with lived experience as violating the sanctitude of a safe home. Reference de Waardt, Mulder and Widdershoven24
While CTO restrictiveness in terms of legal criteria, oversight and enforcement seems to be clearly set out in law, how this is interpreted in practice could impact de facto restrictiveness (see below). The specific restrictions on the individual are not, however, fully specified in most law texts. This is also the case regarding the length of time that restrictions will be in place, because the possibilities for renewal means that CTO duration can be ascertained only in retrospect. Combined, this precludes an assessment of overall restrictiveness, which might have implications for how the proportionality of a CTO can be judged.
We found no patterns of CTO regimes that are clearly preventative or least restrictive; rather, as reported in a previous study, most regimes include both preventative and least restrictive elements. Reference Churchill, Owen, Singh and Hotopf1 With the same criteria as involuntary admission, CTO placement from the community might be considered less restrictive than admitting the person to hospital involuntarily, and is permitted in most regimes. However, the same countries also allow CTO following a person’s first-ever admission, presumably as a preventative measure to reduce future risk. Reference Dawson2 As argued by Dawson, this means that for some individuals there is no established pattern of non-compliance, relapse or readmissions, making it difficult to suggest that such use of CTOs represents the least restrictive approach. Reference Dawson, Kelly and Donnolly3 This might be of concern, given that as many as a fifth of those experiencing their first episode of psychosis have been reported to be subjected to a CTO. Reference Morandi, Golay, Lambert, Schimmelmann, McGorry and Cotton25 To mitigate such concern over proportionality, some regimes, such as the Maltese, require a history of deterioration. Several Canadian regimes go further, including Saskatchewan, where CTO criteria are linked to hospitalisation over the previous 2 years. Reference Dawson2
Future direction of CTO legislation
Based on our findings and the wider literature, it appears that European CTO legislation moves in different directions: some countries have reigned in legal powers by removing the provision altogether. In Latvia this was due to human rights concerns, lack of safeguards and insufficient community care; the country is now developing community-based care Reference Wijker, Sillitti and Hewlett26 without the option of using CTOs. Denmark introduced and abandoned CTO legislation in the context of a well-developed community care system. This abandonment was due to concerns over proportionality in light of limited observed benefits, and because the orders were relevant to a very small population. 27 We have not observed calls for the reintroduction of CTOs in either country. In England & Wales, a current White Paper explicitly seeks to curtail CTO use by requiring consultation with community services prior to initiating orders, shorten their duration and involve tribunals in assessment of individual conditions. 28
In other countries, developments appear to be going in the opposite direction. Permitting ‘restrain and treat’ in the Dutch regime clearly widens their enforcement powers. We also noted how Slovenia lowered the threshold by changing requirements from ‘previous admissions’ to ‘previous service contact’. In Norway, the introduction of capacity-based law in 2017 sought to limit the use of coercion. A recent legal change will, from 2026, alter the degree of certainty when assessing the lack of capacity, from ‘manifest’ to ‘on the balance of probabilities’, explicitly lowering the threshold. 29 The 2024 amendment in Belgium widened the scope for CTOs (it was previously restricted to family care) while simultaneously raising the threshold compared with compulsory admissions, by requiring the person’s consent.
Two-thirds of the surveyed countries have no provision for CTOs. The move towards community-based care, which was a precursor of CTOs in many countries, Reference Churchill, Owen, Singh and Hotopf1 is now in its early stages in others. Whether CTOs will be added to these systems remains to be seen. In Moldova, a 2024 legal reform introduced new national quality standards and a restructuring focused on the development of community-based care that emphasises voluntariness and better alignment with the CRPD, 30 and CTOs have not so far been considered. In other countries, including Montenegro 31 and Cyprus, 32 discussions about CTOs are ongoing as part of policy plans for community-based services. In Spain most psychiatrists reportedly favour the introduction of CTOs, but draft legislation has not passed into law. Reference Lippi, Campanozzi, D’Andrea, Morena, Orsini and Damato33 This suggests a disagreement on the way forward, and that the ad hoc schemes founded in liberal legal interpretation might be likely to continue. Calls for testing of CTOs in Italian services have been made. Reference Lippi, Campanozzi, D’Andrea, Morena, Orsini and Damato33 In Germany, the Federal Constitutional Court recently decided that limiting involuntary care to the in-patient setting is partly unconstitutional. By instructing the development of new legal accommodations, this reflects a view of the community as a least restrictive setting. 34
Limitations
The study benefited from an international, cross-disciplinary research team. In addition, the active participation of representatives from participating countries in supplying and verifying data strengthened its quality. Nonetheless, given the complexities of legal texts we cannot, despite rigorous data-checking, rule out occasional inaccuracies or that our classification does not fully account for details or particularities in individual regimes.
Implications for further research
We found that law texts per se are insufficient to determine overall CTO restrictiveness, due to a lack of specificity of the content and duration of restrictions placed on the person. We believe systematic empirical studies within and between jurisdictions are necessary as a prerequisite for assessing this, and also the proportionality of limiting the personal liberty of individuals who have not committed a crime. Specifically, we recommend five areas for investigation to inform mental health policy and legislation surrounding CTOs.
First, we need studies that explore how CTO restrictiveness can be shaped by the interpretation and application of legal frameworks. The letter of the law, which was our concern, does not necessarily reflect practice and ‘implementation gaps’ between statute and practice are not uncommon. Reference van der Baaren35 Interpretations in the form of clinical guidelines or legal precedence might play a role. For example, although the legal text in the Israeli regime states that the same criteria apply for both in- and out-patient compulsion, there is a reported precedent for lower thresholds in determining risk related to CTOs. Reference Bauer, Rosca, Grinshpoon, Khawaled, Mester and Yoffe36 Additionally, discrepancies in how decision-making capacity is determined in practice could affect de facto thresholds. It has been demonstrated that capacity assessment procedures can be unclear, that clinicians find such assessments difficult Reference Jorem, Forde, Husum, Dahlberg and Pedersen37 and that these might be poorly documented. Future studies should examine the relationship between statute and its interpretation and practice across these areas.
Second, we must continue to investigate whether CTOs deliver benefits to people’s lives in both the short and longer term. This should, given the negative appraisals from those with personal experiences, include potential harms as outcome measures. Reference Kisely, Zirnsak, Corderoy, Ryan and Brophy38
Third, it has been argued that, in light of the current evidence base, an ethically balanced way forward would be to make CTOs subject to individual consent. Reference Szmukler39 While this is part of some Canadian laws, Reference Dawson16 Belgium was the only jurisdiction in our sample with such provision, effective from 2025. How voluntary or coercive individuals experience such regimes, and how freely their consent is given that the alternative is likely to be involuntary admission, should be examined.
Fourth, CTO use could relate to the dimensioning of services. Policies of reducing bed numbers and expectations of shorter hospital admissions could be a driver for earlier discharge by placing people on CTOs. Reference Dawson, Kelly and Donnolly3 This would suggest that the use of coercion to some extent is driven by service factors and not clinical need, which poses ethical concerns. Reference Hofstad, Husum, Rugkåsa and Hofmann40 The interaction between use of CTOs and both in-patient and community service configurations needs exploration.
Fifth, given that most countries in our sample manage without CTO regulation, future studies should examine how they do this. This could include investigation of the scope of their mental health systems and the role of families and networks, as well as cultural issues related to stigma and public attitudes towards risk and inclusiveness. Particular attention should be paid to contexts in which CTOs have been tried but abandoned, or where authorities seek to curtail their use.
In conclusion, this is the first study to compare the availability and restrictiveness of community compulsion across European countries. We found that 13 jurisdictions in the 33 surveyed countries have CTO statutes, and that legal criteria largely match those for compulsory in-patient care. Restriction of citizens’ liberties requires clearly defined regulations and legal safeguards. For CTOs, the principle of proportionality of restrictions and the use of the least restrictive option represent key legal, and ethical, concerns. Reference Dawson, Kelly and Donnolly3 We found that the restrictiveness of CTOs cannot be ascertained from law texts (de jure) alone, because many statutes function in ways that prevent scrutiny of the content and duration of restrictions. This, and other aspects of how CTOs are applied in practice, should be investigated to establish their de facto restrictiveness. The lack of (or, at the very least, contested) evidence for patient benefits further adds to the uncertainties regarding the role of CTOs in balancing individuals’ rights to autonomy and their rights to care. Two-thirds of our sample, including both countries with and without community-based services, do not use CTOs. Policy drives to extend community mental healthcare across European countries should therefore not automatically lead to new provisions for CTOs. We would argue, in line with the Danish Government’s conclusions when abandoning their regime, 27 that until their restrictiveness and outcomes are better understood, new CTO regimes are difficult to justify.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjo.2026.12015
Data availability
Data availability is not applicable because no new data were created or analysed in this study.
Acknowledgements
The FOSTREN Law and Policy Project was a joint venture involving researchers from seven countries, who developed the survey upon which this paper is based. The group consisted of Giulio Castelpietra (Italy); Jovo Dedovic (Montenegro); Tânia Lourenço, José Miguel Caldas de Almeida and Deborah Oyine Aluh (Portugal); Søren Fryd Birkeland (Denmark); Andrés Fontalba Navas (Spain); Tella Lantta (Finland); and Jorun Rugkåsa (Norway). The work formed part of the COST-Action FOSTREN. The network grant was funded by the European Cooperation in Science and Technology (ref. no. CA19133), and all team members have received travel reimbursement during the course of this work. We are extremely grateful to Richard Whittington, who led the FOSTREN network that made this work possible. We thank those (totalling more than 80) who participated in data collection and quality assurance across the FOSTREN countries. In addition to some who did not wish to be named, these included the following: Austria: Joachim Scharfetter, Joy Ladurner, Matthäus Fellinger, Monika Nowotny. Belgium: Evi Verbeke, Stijn Vanheule. Bulgaria: Vladimir Nakov, Michail Okoliyski. Croatia: Dunja Degmečić, Slađana Štrkalj- Ivezić. Cyprus: Andreas Chatzittofis, Theano Mavromoustaki. Czech Republic: Jaroslav Pekara; Petr Winkler (policy data). Denmark: Frederik Alkier Gildberg, Søren Fryd Birkeland. Estonia: Aneth Tuurmaa, Mari Ader, Ingrid Ots-Vaik, Ülle Kumm, Jane Idavain, Reet Nestor, Katrin Tomson, Anne Randväli. Finland: Tella Lantta, Aila Vokkolainen, Satu Tuovinen, Irkku Höök. France: Yvonne Quenum, Magali Coldefy, Stéphanie Wooley, Dominique Friard. Germany: Sophie Hirsch, Jakov Gather, Tilman Steinert. Greece: Stelios Stylianidis, Eugenie Georgaca, Aikaterini Nomidou, Maria Samakouri, Panagiota Bali. Ireland: Jim Maguire, Ciaran Corcoran. Israel: Ronen Shmilovitz, Alexander Shestiperov, Yoav Kohn. Italy: Gian Maria Galeazzi, Davide Elia Bertani, Giulio Castelpietra, Tommaso Bonavigo, Antonello Leogrande, Luca Pingani. Latvia: Marina Loseviča. Montenegro: Jovo Dedovic. Moldova: Jana Chihai, Mădălina Bivol, Radislav Coșulean. The Netherlands: Dieuwertje Anna de Waardt (CTO data). Norway: Roger Almvik, Bjørn Kristian Soknes, Olav Nyttingnes, Jorun Rugkåsa. Poland: Jakub Lickiewicz, Łukasz Cichocki, Łukasz Kaczka, Tomasz Rowiński. Portugal: José Miguel Caldas de Almeida, Deborah Oyine Aluh, Tânia Lourenço. Romania: Adriana Mihai. Slovakia: Dagmar Breznoscakova, Barbora Maliarova, Katarina Kohylova. Slovenia: Juš Škraban, Matej Vinko, Katarina Ficko Mauch, Andreja Čelofiga. Sweden: Anna Björkdahl, Lars Kjellin. Switzerland, Sabine Hahn, Stephane Morandi. Turkey: Hulya Bilgin, Merve Aydın. UK: Alina Haines-Delmont, Sian Cooper, Faye McLoughlin (England & Wales), Patrick Callaghan, Brodie Paterson (CTO data, Scotland).
Author contributions
J.R., S.F.B. and D.O.A. were part of the team that conceptualised the study and created the data collection form used. J.R. and D.O.A. had overall responsibility for data entry, handling and verification. J.R. led the analysis, with contributions from the other authors, and all were involved in both quality control and contacting respondents for clarification. J.R. was project principal investigator and wrote the article. J.R., D.O.A., J.C., S.F.B. and A.C. contributed critical assessment of the draft manuscript in several rounds and have accepted publication of the final version.
Funding
All team members have received travel reimbursement during the course of this work, from FOSTREN (funded by COST grant no 19133). In addition, D.O.A.’s participation was in part funded by the Norwegian Research Council (grant no. 273546).
Declaration of interest
None.
Use of artificial intelligence
We used Google Translate and Chat GPT to translate details of legal frameworks in languages unfamiliar to the author team. We checked the resulting information with respondents from the respective countries. Artificial intelligence was not used in the writing of any parts of the manuscript.




 Open access
Open access
eLetters
No eLetters have been published for this article.