Diabetes is a chronic non-communicable disease that affected approximately 463 million people worldwide in 2019. It is estimated that this number will reach 700 million in 2045, with 90 % of these cases being instances of type 2 diabetes(Reference Saeedi, Petersohn and Salpea1). Type 2 diabetes is a serious condition with a significant impact on individuals’ quality of life, ranking among the top ten causes of death globally(Reference Saeedi, Petersohn and Salpea1,Reference Zurita-Cruz, Manuel-Apolinar and Arellano-Flores2) . The rising prevalence of type 2 diabetes can be attributed in part to population ageing, an increase in obesity rates and a sedentary lifestyle coupled with unhealthy eating patterns(Reference Bellou, Belbasis and Tzoulaki3,Reference Rosen, Kaestner and Natarajan4) . Treatment for type 2 diabetes varies based on factors such as age, duration of the disease and the challenge of metabolic control. It may involve medication and/or insulin use, self-management and lifestyle advice(Reference Yu, Lee and Kim5). Dietary guidance plays a crucial role in the treatment of type 2 diabetes. However, individuals with this condition often exhibit low adherence to dietary management, which can be associated with a poorer prognosis, increased co-morbidities, complications and mortality(Reference Bailey and Kodack6–Reference Katsiki, Anagnostis and Kotsa8). Several factors influence adherence to dietary treatment in these individuals, including challenges in understanding, implementing and maintaining dietary recommendations, food preferences, time since diagnosis, anxiety, depression, stress and eating disorders(Reference Katsaridis, Grammatikopoulou and Gkiouras9–Reference Winston11).
In the context of disordered eating behaviours and type 2 diabetes, another construct that has captured the interest of the scientific and clinical community is food addiction (FA). FA is characterised by the excessive consumption of energy-rich, hyperpalatable and ultra-processed foods, sharing similarities with substance use disorders(Reference Gearhardt, Bueno and DiFeliceantonio12,Reference Gearhardt, Corbin and Brownell13) . Although the concept was initially coined in the 1950s, the number of investigations on the subject has significantly increased in the last 15 years. Part of this heightened interest can be attributed to the development of the Yale Food Addiction Scale (YFAS) in 2009(Reference Gearhardt and Schulte14). This tool adapts diagnostic criteria for substance use disorders to eating behaviour, has been translated and validated in multiple languages and has become the primary instrument for assessing FA globally(Reference Gearhardt, Bueno and DiFeliceantonio12). Recent data from a systematic review encompassing studies conducted in over thirty countries indicate that the global prevalence of FA in the non-clinical population is 14 % in adults, with even higher rates observed in individuals with obesity, reaching approximately 28 % among this group(Reference Praxedes, Silva-Júnior and Macena15).
Prior studies have established positive associations between FA and type 2 diabetes across diverse populations, including the general population, individuals with pre- and post-bariatric and metabolic surgery, and those with mental disorders(Reference Horsager, Bruun and Færk16–Reference Som, Constant and Zayani18). The presence of FA in individuals with type 2 diabetes may pose a challenge to adherence to dietary treatment, making disease control more difficult. This is attributed to the fact that individuals with FA often exhibit a high consumption of ultra-processed, hyperpalatable foods, confectionery, baked sweet products and fast foods(Reference Pursey, Skinner and Leary19,Reference Silva Júnior, Gearhardt and Bueno20) . These food groups are notable for their elevated levels of sugar and refined carbohydrates, serving as risk factors for both the onset and poor control of type 2 diabetes(Reference Bellou, Belbasis and Tzoulaki3,Reference O’Hearn, Lara-Castor and Cudhea21) .
Therefore, investigating the presence of FA in individuals with type 2 diabetes is of great significance in identifying potential factors that impede adherence to dietary treatment for type 2 diabetes. Consequently, this may affect metabolic control and contribute to complications of the disease, offering new avenues for enhancing adherence to dietary treatment among individuals with type 2 diabetes. Given this rationale, the purpose of this systematic review with meta-analysis was threefold: (a) to determine the prevalence of FA in individuals with type 2 diabetes, (b) to assess the association between FA and type 2 diabetes and (c) to establish whether there is a correlation between FA and fasting blood glucose, glycemia, insulinemia, glycated hemoglobin (HbA1c), HOMA indices and complications related to type 2 diabetes.
Material & methods
This systematic review with meta-analysis is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Statement (PRISMA)(Reference Page, Moher and Bossuyt22). The protocol was previously published in the PROSPERO database (https://www.crd.york.ac.uk/prospero/) under registration protocol CRD42023465903.
Eligibility criteria
Cross-sectional studies, case–control studies, cohorts and clinical trials carried out with individuals with type 2 diabetes, regardless of age and sex, were included. Case reports and systematic reviews were not included, and duplicate publications of the included studies were excluded.
Information sources
The searches were carried out until November 2024 in the databases and platforms MEDLINE, EMBASE, Web of Sciences, Latin American and Caribbean Literature in Health Sciences (LILACS), ScienceDirect, Scopus and PsycINFO. We also consulted the grey literature database Open Access Theses and Dissertations (https://oatd.org/). Additionally, we consulted the reference lists of articles included in the full-text reading to select potential studies that were not retrieved by the search strategy.
Search strategy
A broad search strategy was constructed and included terms related to FA and type 2 diabetes, using MeSH terms and free terms. The research had no restrictions regarding the year or language of publication. As an example, the following strategy was used in the MEDLINE database: (((‘food addiction’) OR (‘eating addiction’) OR (‘Yale food addiction Scale’) OR (YFAS) OR (‘modified Yale food addiction scale’) OR (mYFAS) OR (‘Yale food addiction Scale 2·0’) OR (‘YFAS 2·0’) OR (‘modified Yale food addiction scale 2·0’) OR (‘mYFAS 2·0’)) AND ((diabetes) OR (‘diabetes mellitus’) OR (‘type 2 diabetes mellitus’) OR (‘Type 2 Diabetes’) OR (DM) OR (DM2) OR (‘Noninsulin Dependent Diabetes Mellitus’) OR (‘Noninsulin-Dependent Diabetes Mellitus’))).
Selection process
Two independent authors (AESJ and MLM) selected included studies. A third author (NBB) resolved disagreements regarding decisions. The study selection process involved reading the titles and abstracts and the full text of the articles. The Rayyan software (https://rayyan.ai/) was used for this process(Reference Ouzzani, Hammady and Fedorowicz23).
Data collection process
Following the study selection process, the full texts of the selected studies were obtained, and a confirmation of their adherence to the inclusion criteria was made. The data extraction process commenced only after this confirmation. During this stage, two authors (AESJ and MLM) independently conducted the data extraction, and any disparities were resolved through consensus. The collected data were systematically organised in an electronic spreadsheet. In instances where data were not directly available, we reached out to the study authors via email to request the necessary information. Additionally, the GetData Graph Digitizer software, version 2.2.0.20, was employed to extract numerical data from graphical representations.
Data items
The prevalence of FA in individuals with type 2 diabetes and the association between the diagnosis of FA and type 2 diabetes were our main outcomes. The effect measures collected for these outcomes were prevalence, prevalence ratio, OR and/or risk ratio. Additionally, data on fasting blood glucose, blood glucose, insulinemia, HbA1c, HOMA indices and type 2 diabetes complications were collected when available.
The complete data extracted were: country in which the study was carried out, year of publication, type of study, number of individuals evaluated, age, sex, weight, presence of co-morbidities, age of participants, FA symptom score and prevalence of type 2 diabetes.
In addition, we collected the reported adjusted OR derived from two different models: one model adjusted by age and sex, and the other adjusted by age, sex and BMI. Both the crude and adjusted OR were extracted as reported by the authors in their respective papers or via email contact with them, with no further statistical procedure performed by us.
Study risk of bias assessment
The assessment of the risk of bias in the included studies was carried out by two independent researchers (AESJ and MLM) using The Joanna Briggs Institute Critical Appraisal Checklist for Analytical Cross-Section Studies(Reference Moola, Munn, Tufanaru, Aromataris and Munn24). In instances of disagreement between researchers, a third researcher (NBB) was consulted for resolution. The employed checklist consisted of inquiries about the clarity of inclusion criteria, sample description, assessments of exposures and outcomes, consideration of confounding factors and other relevant domains. Responses to these questions were categorised as ‘yes’, ‘no’, ‘unclear’ or ‘not applicable’. The scoring system was based on the ratio of ‘yes’ responses to the total number of applicable items, as carried out by Migliavaca et al. (Reference Migliavaca, Stein and Colpani25) and Macena et al. (Reference Macena, Silva Júnior and Melo26). Consequently, studies were classified into three risk categories: high risk (up to 49 %), moderate risk (50–69 %) and low risk (70 % or greater) of bias.
Effect measures
The FA prevalence data determined by a version of the YFAS in individuals with type 2 diabetes and the OR values (individuals with and without FA x individuals with and without type 2 diabetes) were considered measures of effect in the present review.
Data analysis
Data analysis was based on a quantitative study of variables. For this investigation, Stata v.15 software (StataCorp) was used, using the metaprop command(Reference Nyaga, Arbyn and Aerts27), with DerSimonian and Laird random effects model using the Freeman–Tukey arcsine transformation to stabilise variances. Furthermore, data relating to the OR were also meta-analysed, when available, using the metan command with a DerSimonian and Laird random effects model. Heterogeneity was assessed using the I 2 statistic, which is considered high when I 2 is greater than 50 %. Egger’s test was used to assess publication bias with the metabias command with graphical representation, and a P-value of 0·10 was adopted to indicate a possible bias.
Results
Study selection
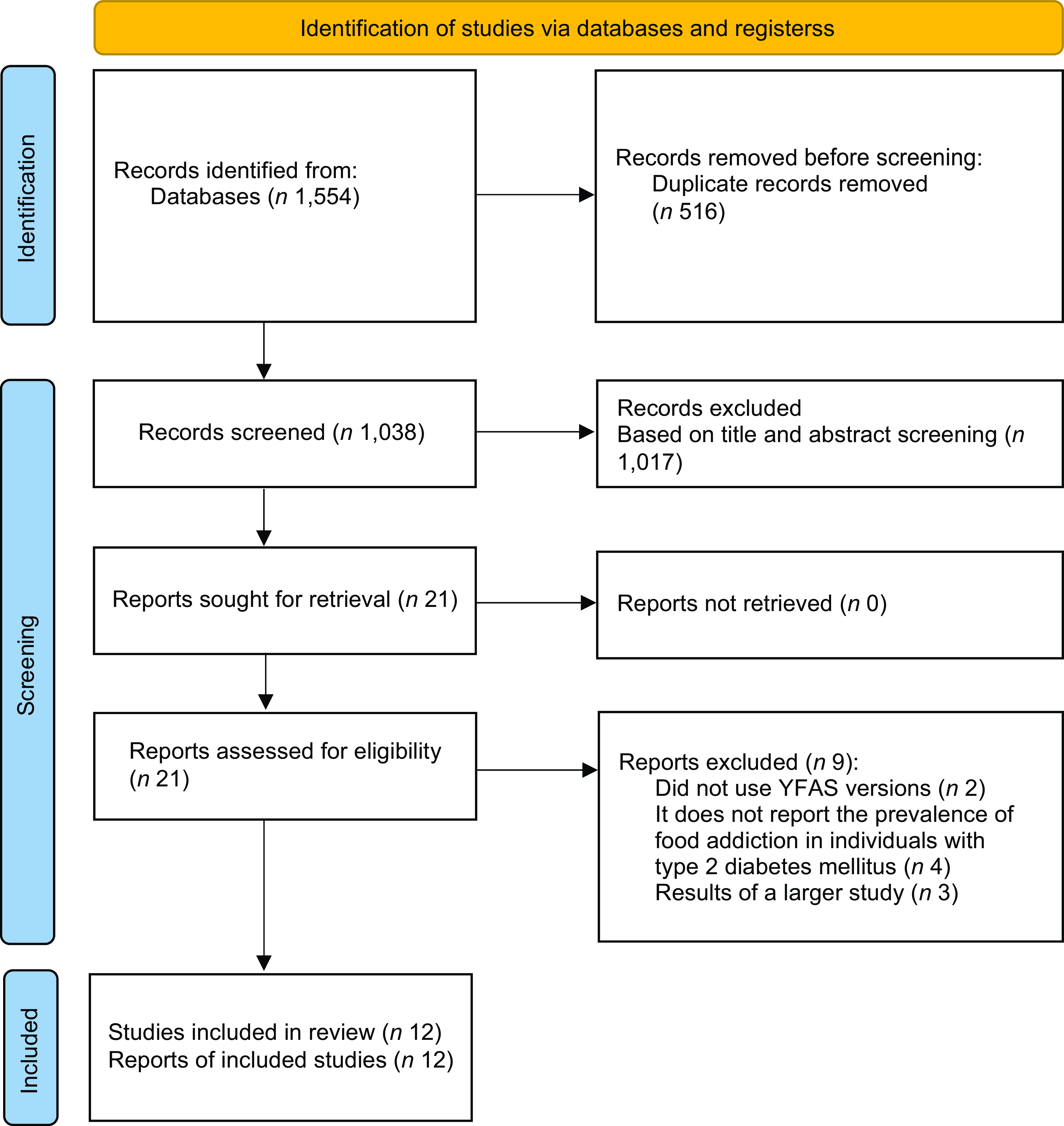
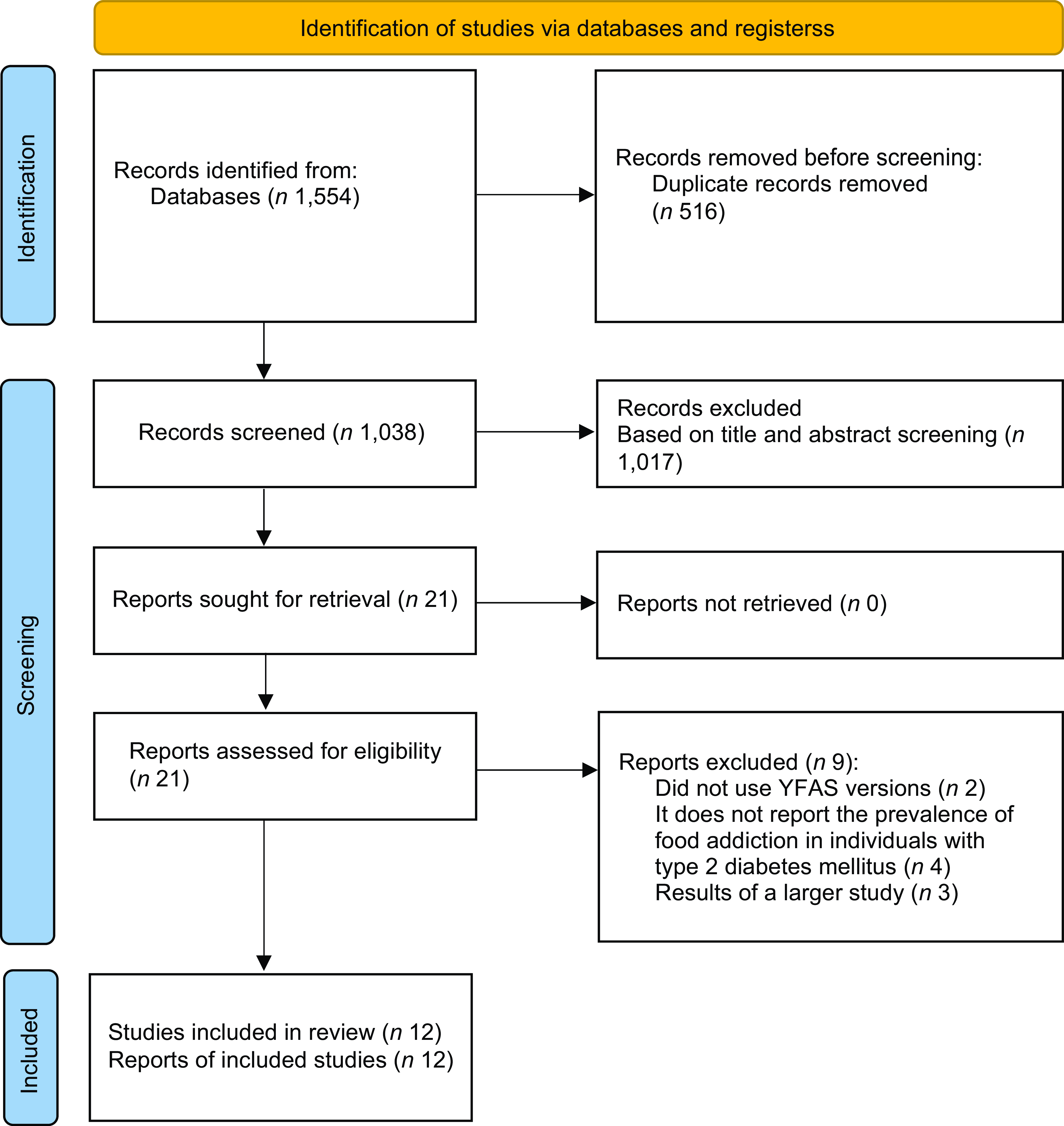
In total, 1437 occurrences were identified in the evaluated databases. Of these, seventeen were selected to read the full texts. Finally, twelve studies were included for qualitative and quantitative evaluation(Reference Horsager, Bruun and Færk16–Reference Som, Constant and Zayani18,Reference Flint, Gearhardt and Corbin28–Reference Smeltzer36) . Details of the study selection can be seen in Fig. 1.
Flow chart of study selection. YFAS, Yale Food Addiction Scale.
Study characteristics
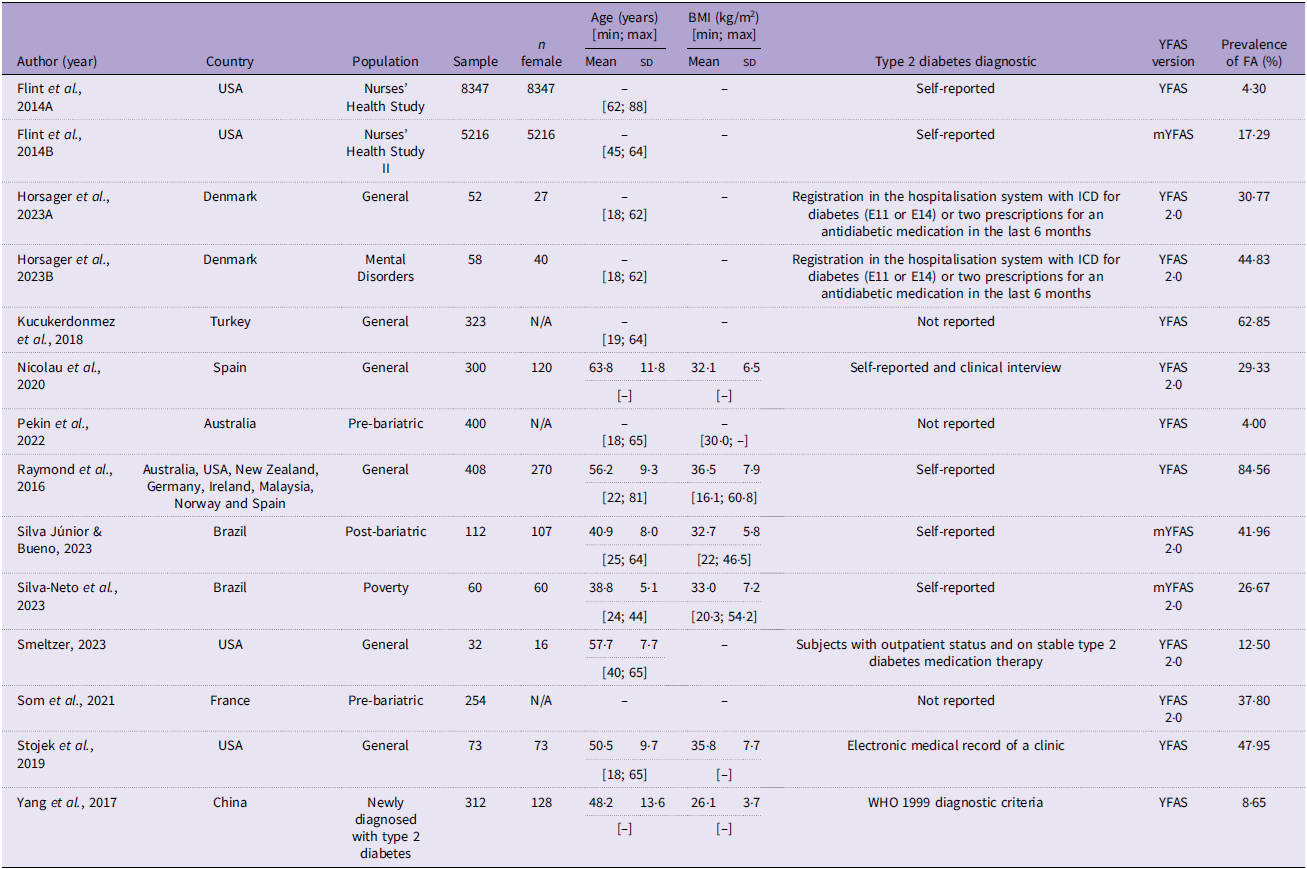
Of the total number of studies included in the present review (n 12), all studies were cross-sectional. Among the tools to diagnose FA, the YFAS was the most used (n 6), while for the diagnosis of type 2 diabetes, self-reporting was the most common way among studies (n 5). The other characteristics of the included studies can be seen in Table 1.
Characteristics of the included studies (n 12)
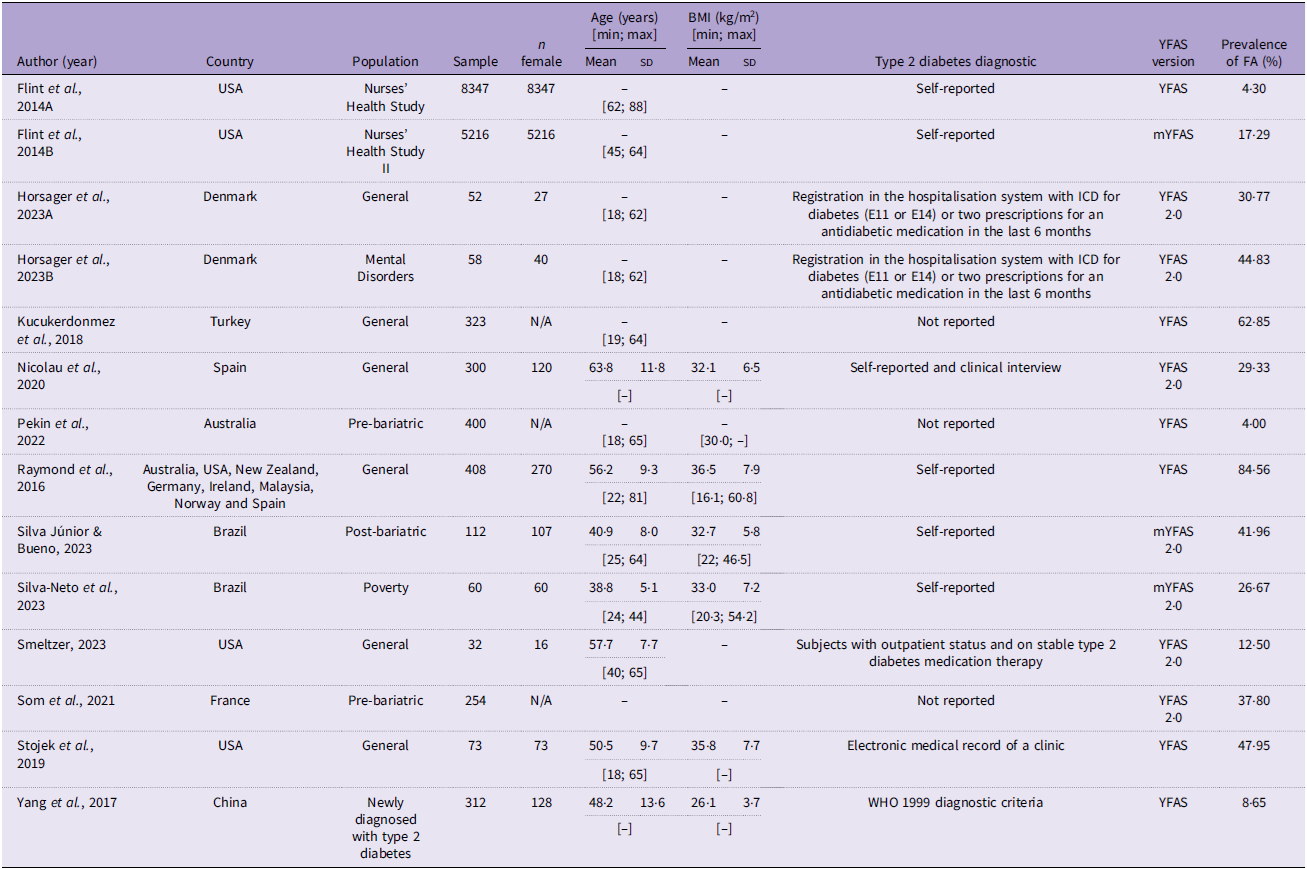
YFAS, Yale Food Addiction Scale; FA, food addiction.
Risk of bias in studies
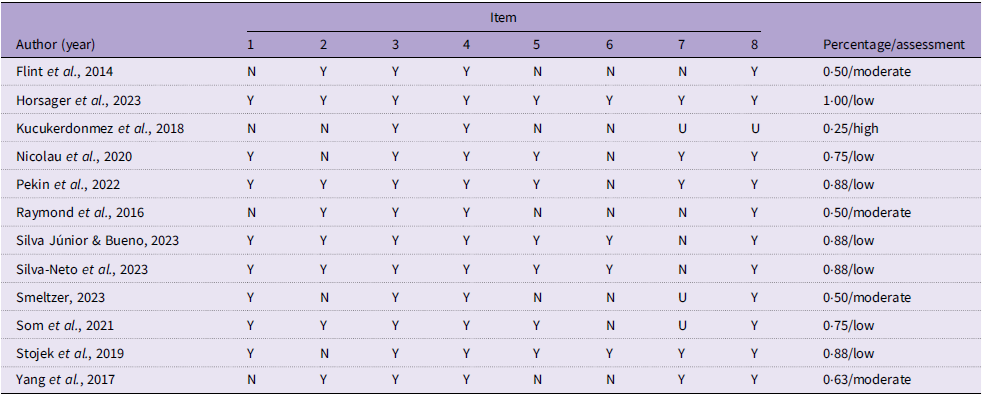
Among the studies included, seven were considered to have low bias(Reference Horsager, Bruun and Færk16–Reference Som, Constant and Zayani18,Reference Nicolau, Romerosa and Rodríguez30,Reference Pekin, McHale and Seymour31,Reference Silva-Neto, Silva Júnior and Bueno33,Reference Stojek, Maples-Keller and Dixon34) , four with moderate risk of bias(Reference Flint, Gearhardt and Corbin28,Reference Raymond, Kannis-Dymand and Lovell32,Reference Yang, Liu and Li35,Reference Smeltzer36) , and one with high risk of bias(Reference Kucukerdonmez, Seckiner and Meseri29). The main domains that presented non-conformities with ‘unclear’ or ‘no’ answers were regarding reporting strategies and whether the outcomes were measured validly and reliably (Table 2).
Risk of bias assessment
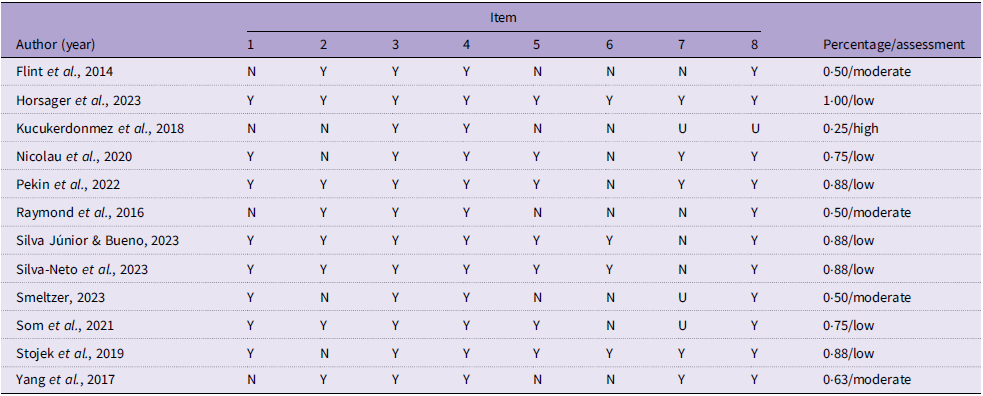
Y, yes; N, no; U, nuclear.
Results of individual studies
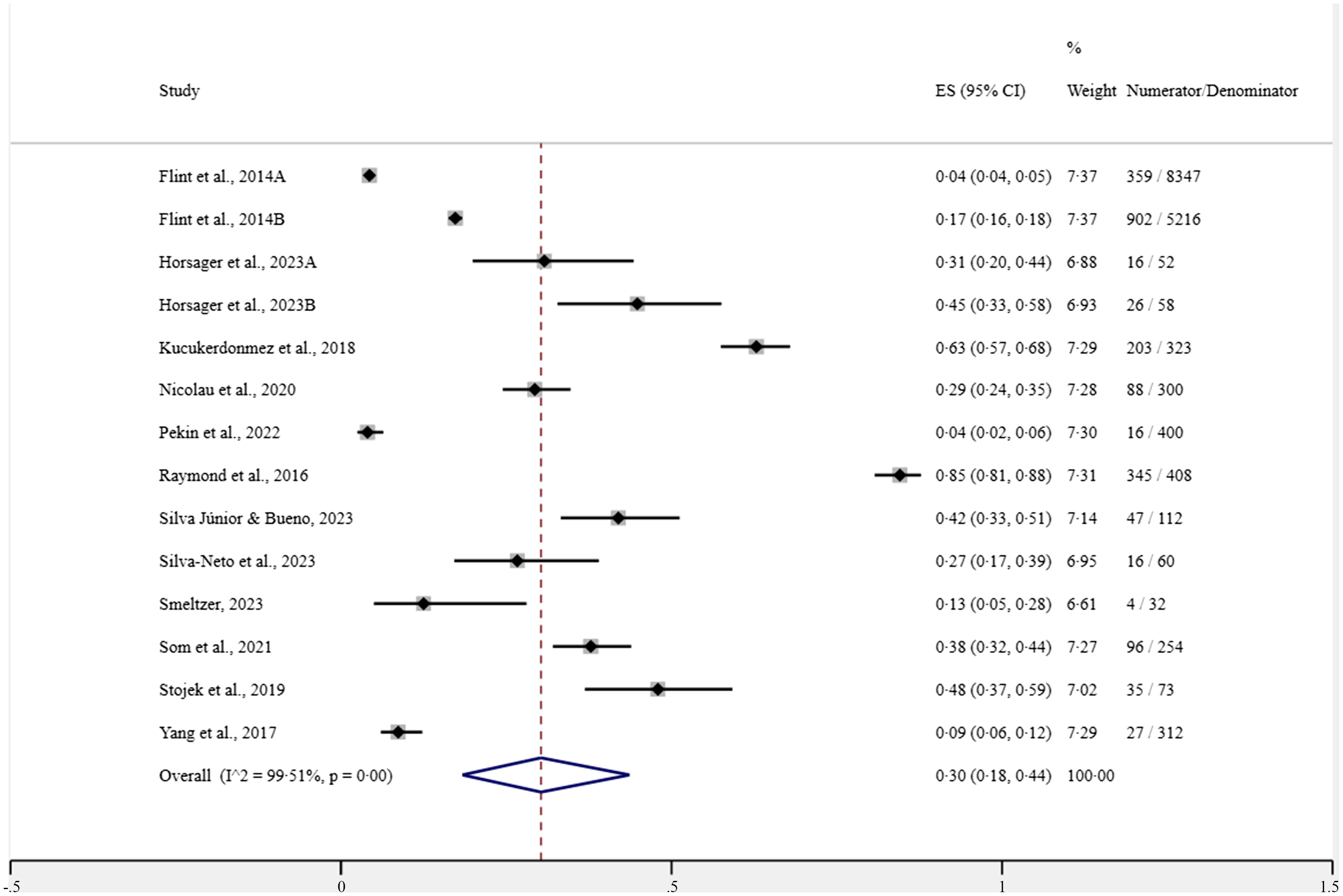
The studies by Raymond et al. (Reference Raymond, Kannis-Dymand and Lovell32) and Kucukerdonmez et al. (Reference Kucukerdonmez, Seckiner and Meseri29) had the highest prevalence of FA in individuals with type 2 diabetes (84·56 and 62·85 %, respectively). In contrast, Pekin et al. (Reference Pekin, McHale and Seymour31) presented a prevalence of 4·00 % of FA in individuals with type 2 diabetes before bariatric surgery, similar to the study conducted by Flint et al. (Reference Flint, Gearhardt and Corbin28) using the YFAS with data collected between 2008 and 2011, which showed a prevalence of 4·30 % of FA.
Regarding the average number of FA symptoms, only four studies report this information. The studies by Silva-Neto et al. (Reference Silva-Neto, Silva Júnior and Bueno33) and Raymond et al. (Reference Raymond, Kannis-Dymand and Lovell32) presented similar means in individuals diagnosed with FA (mean: 4·75; sd: 2·51 and mean: 4·70; sd: 2·22 symptoms, respectively). Yang et al. (Reference Yang, Liu and Li35) show an average of symptoms of 3·6 (sd: 0·8), which is lower than the finding in Brazilian individuals after bariatric surgery observed in the study by Silva Júnior & Bueno(Reference Silva Júnior and Bueno17), which is 6·34 (sd: 2·86).
In the biochemical assessment of glycemic levels during the fasting period, Nicolau et al. (Reference Nicolau, Romerosa and Rodríguez30) show that individuals with type 2 diabetes with a positive diagnosis of FA have a significantly higher average than those individuals without a diagnosis of FA (mean: 164·6; sd: 72·8 mg/dl v. mean: 140·5; sd: 38·8 mg/dl). These findings corroborate the study presented by Yang et al. (Reference Yang, Liu and Li35) with individuals newly diagnosed with type 2 diabetes in northeastern China. However, studies by Yang et al. (Reference Yang, Liu and Li35) and Stojek et al. (Reference Stojek, Maples-Keller and Dixon34) differ in their findings when evaluating the increase in blood glucose after performing the oral glucose tolerance test, in which the first does not observe any difference between having or not having a diagnosis of FA. In contrast, in the second, when evaluating only African-American women, this increase is greater in those diagnosed with FA. As for the evaluation of the Hb1Ac indicator, individuals with FA show slightly higher values, as shown in the study by Nicolau et al. (Reference Nicolau, Romerosa and Rodríguez30) (mean: 7·9; sd: 4·4 % v. mean: 7·6; sd: 1·4 %) and also by Stojek et al. (Reference Stojek, Maples-Keller and Dixon34) (8·9 % v. 7·6 %). Finally, when evaluating the HOMA-IR index, patients with FA showed higher means in the study by Yang et al. (Reference Yang, Liu and Li35) (mean: 8·37; sd: 5·81) compared with individuals without FA (mean: 4·89; sd: 2·67), which is similar to the data presented by Stojek et al. (Reference Stojek, Maples-Keller and Dixon34) (24·21 v. 6·95).
Only the study by Nicolau et al. (Reference Nicolau, Romerosa and Rodríguez30) reported the differences between individuals with and without FA and the complications of type 2 diabetes. In this study, increased prevalences of retinopathy (25·0 % v. 13·2 %), nephropathy (32·0 % v. 22·3 %), and neuropathy (29·5 % v. 21·8 %) were observed in individuals with a positive diagnosis of FA compared with individuals without this diagnosis.
Results of syntheses
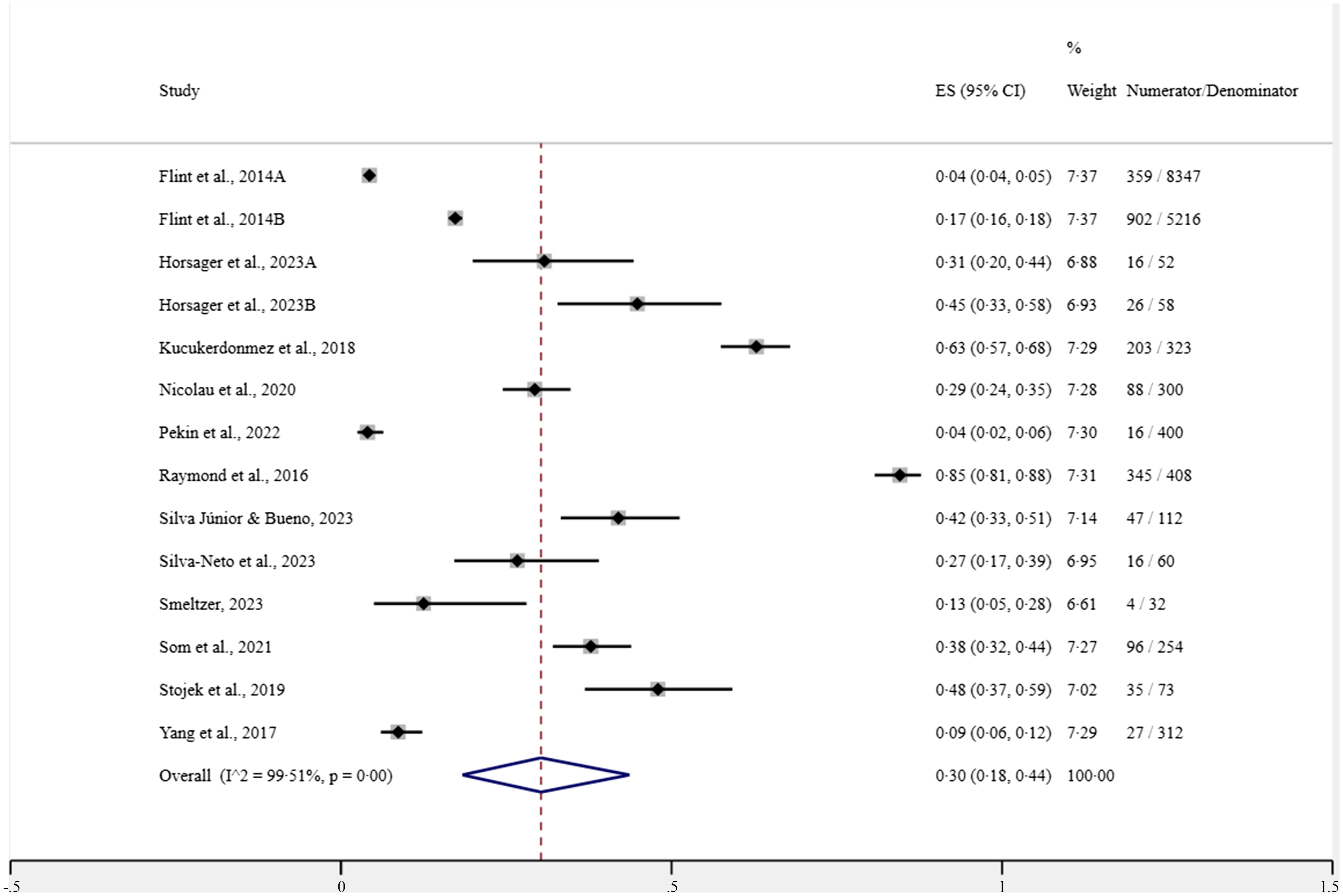
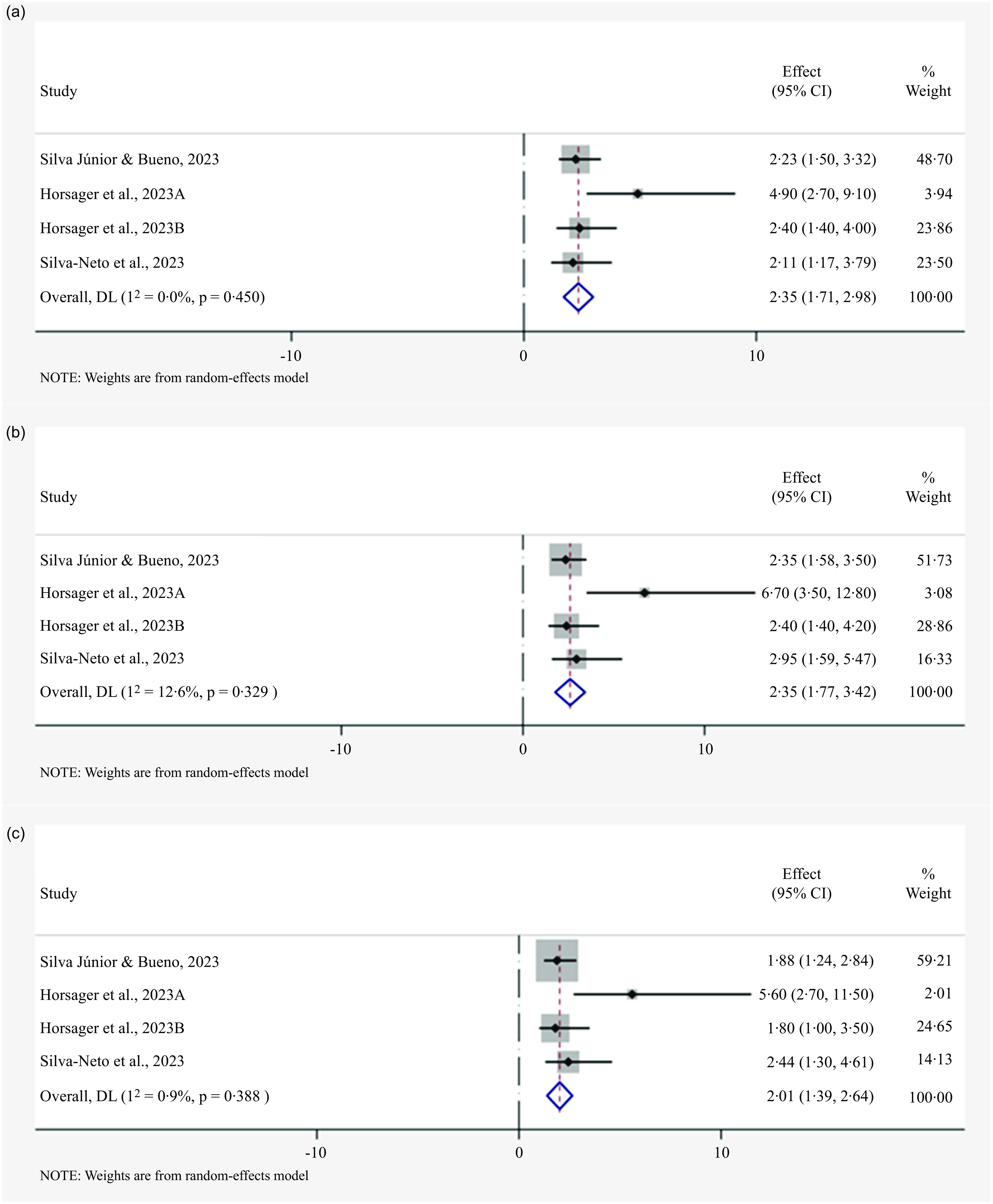
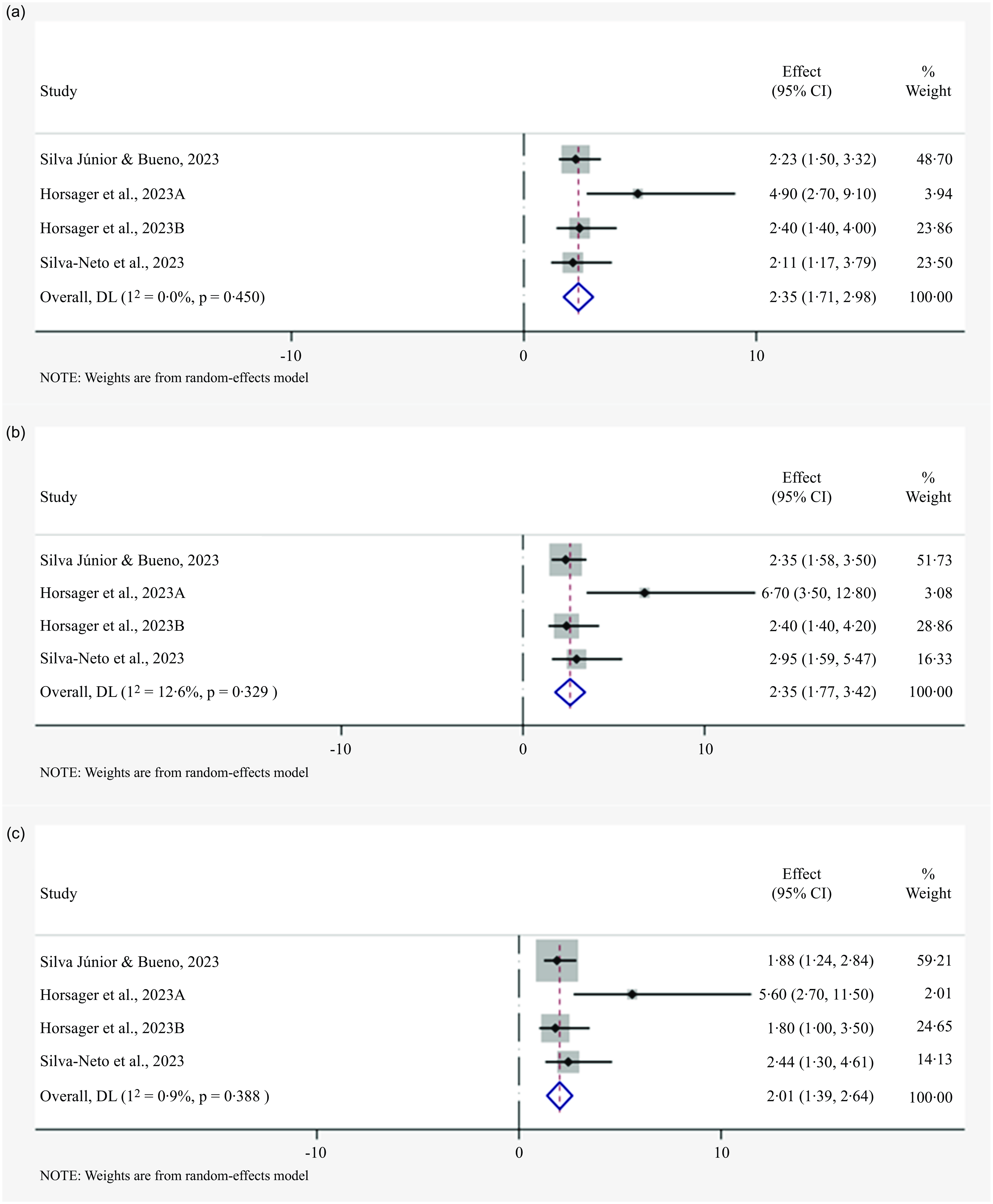
The crude and adjusted ORs of the studies by Silva-Neto et al. (Reference Silva-Neto, Silva Júnior and Bueno33) and Silva Júnior & Bueno(Reference Silva Júnior and Bueno17) were obtained through contact with the authors, since these were not exposed in the publications. In the meta-analyses carried out, a pooled prevalence of 30 % (95 % CI (18, 44) with estimated predictive interval (0; 85); I 2 = 99·51; 12 studies; 15 947 participants) can be seen in Fig. 2. When evaluating the meta-analyses for the crude OR presented by the studies, we found the grouped value of 2·35 (95 % CI (1·71, 2·98); I 2 = 12·6; 3 studies; 282 participants with diabetes in the studies). The pooled OR adjusted for age and sex was 2·60 (95 % CI (1·77, 3·42); I 2 = 12·6; 3 studies; 282 participants with diabetes in the studies) (Fig. 3). Finally, as shown in Fig. 3(c), the pooled age, sex and BMI-adjusted OR was 2·01 (95 % CI (1·39, 2·64); I 2 = 0·09; 3 studies; 282 participants with diabetes in the studies).
Forest plot for the prevalence of food addiction in individuals with type 2 diabetes.
Forest plots for the crude and adjustments OR for the association between type 2 diabetes and food addiction. (a) Crude OR for the association between type 2 diabetes and food addiction. (b) OR or the association between type 2 diabetes and food addiction adjustment by age and sex. (c) OR or the association between type 2 diabetes and food addiction adjustment by age, sex and BMI.
Publication bias
We found some evidence of publication bias in the studies included in the meta-analysis with the prevalences found (bias = 4·15 (0·29; 8·01), P = 0·03) (online Supplementary Fig.1). Similarly, we found publication bias in the studies included in our meta-analyses performed with data related to adjusted OR (bias = 2·00 (–0·13; 4·14); P = 0·05) (online Supplementary Fig.2).
Discussion
The present study provides the results of a systematic review with a meta-analysis of the prevalence and associations of FA with the diagnosis of type 2 diabetes, fasting blood glucose, blood glucose, insulinemia, HbA1c, HOMA indices, and complications of the disease. Twelve studies were included, and the results of the meta-analysis indicated a 30 % prevalence of FA in individuals with type 2 diabetes. Furthermore, it was possible to observe that the associations between FA and type 2 diabetes remained relatively high even after adjusting for age and sex, and age, sex, and BMI. Finally, we highlight that few studies have evaluated the associations between FA and the biochemical parameters of disease control and complications, highlighting that this is a fruitful niche for the development of future research.
The meta-analysis revealed a prevalence of 30 % for FA in individuals with type 2 diabetes. This figure was slightly higher than the rate found in Praxedes et al. (Reference Praxedes, Silva-Júnior and Macena15) meta-analysis for individuals with obesity (28 %) and comparable to those in the pre-operative period of bariatric and metabolic surgery (32 %)(Reference Praxedes, Silva-Júnior and Macena37). Type 2 diabetes stands out as one of the most severe consequences linked to obesity, with both conditions seemingly sharing similar pathophysiological mechanisms. Despite the acknowledged association between a high BMI and an increased prevalence of FA, it is essential to recognise that they are distinct entities and should not be used interchangeably. It is important to note that only a limited number of studies included in this review provided BMI data for individuals with type 2 diabetes, both with and without FA, making it impractical to delve further into this relationship.
The presence of FA in individuals with type 2 diabetes may constitute an additional factor complicating adherence to dietary recommendations. Neuroimaging studies have demonstrated that foods rich in simple carbohydrates and fats seem to activate regions associated with reward in a manner akin to addictive drugs. This stimulation can result in a loss of control, consequently prompting an increased pursuit and consumption of this particular type of food(Reference Volkow, Wang and Fowler38–Reference Volkow, Wang and Tomasi40). Additionally, it was also observed that individuals are more likely to show signs of FA related to foods rich in refined carbohydrates and fats(Reference Schulte, Avena and Gearhardt41). The studies included in this review reveal that individuals with FA had higher levels of fasting blood glucose, HOMA-IR, HbA1c and a greater occurrence of microvascular complications(Reference Nicolau, Romerosa and Rodríguez30,Reference Stojek, Maples-Keller and Dixon34,Reference Yang, Liu and Li35) , which would support the hypothesis that this diagnosis of FA in individuals with type 2 diabetes may have a relevant clinical impact, given its potential to reduce adherence to dietary recommendations.
The eating patterns observed in individuals with FA seem to be characterised by the high consumption of ultra-processed, hyperpalatable foods, confectionery and baked sweet products. This pattern is recognised for being rich sources of refined carbohydrates and sugar and, in turn, is associated with the worst glycemic control of individuals with type 2 diabetes(Reference Pursey, Skinner and Leary19,Reference Silva Júnior, Gearhardt and Bueno20) . Eating habits characterised by high consumption of ultra-processed foods may be related to a higher risk of type 2 diabetes, as shown in the NutriNet-Santé Prospective Cohort(Reference Srour, Fezeu and Kesse-Guyot42). The mechanisms underlying the impact of these foods are not fully understood. However, upon examining their nutritional composition, elements such as high sugar and sweetener content, as found in sugar-sweetened beverages, for example, a high glycemic index and low amounts of fibre, appear to contribute significantly to metabolic impacts in individuals with type 2 diabetes(Reference Allison43). Similarly, this type of food is also associated with the mechanisms proposed for FA symptoms, as has already been observed in animal models(Reference Lennerz and Lennerz44). Therefore, the convergence between the high prevalence of FA and its symptoms in individuals with type 2 diabetes appears to be the high consumption of ultra-processed foods.
The present systematic review with meta-analysis presents limitations that must be considered in its interpretation. Most of the included studies use the diagnosis of type 2 diabetes through self-report, which may lead to an increase in false-negative diagnoses for the condition that would not be included in our analyses, thus underestimating the prevalence of type 2 diabetes. However, studies evaluating the validity of self-report for the diagnosis of type 2 diabetes show reasonable sensitivity and high specificity, thus being useful and applicable in population studies(Reference Fontanelli, Teixeira and Sales45,Reference Paddison, Saunders and Abel46) . The heterogeneity in our results should be considered in the studies included in this review. The studies included in our review encompassed populations from various geographical locations, age groups and socio-economic backgrounds. However, the diversity of demographic characteristics can influence the prevalence of FA, and our pooled analyses might not accurately reflect the true burden of FA in the type 2 diabetes population. It was not possible to carry out subgroup analyses to try to mitigate this due to the fact that the studies did not present this data. That is, while the results of our meta-analyses provide valuable insight into the prevalence of FA in individuals with type 2 diabetes, the representativeness and potential misrepresentation of specific subgroups highlight the need for further research in more diverse populations. Previous systematic reviews have already highlighted that studies carried out on the topic of FA are very heterogeneous and that they seem to have this characteristic even when evaluating smaller subgroups(Reference Praxedes, Silva-Júnior and Macena15,Reference Pursey, Skinner and Leary19,Reference Praxedes, Silva-Júnior and Macena37) . Another point that must be highlighted is the lack of reports on the number of FA symptoms, the relationship between the positive diagnosis of FA and metabolic parameters (e.g. HbA1c, HOMA indices, fasting blood glucose, blood glucose and insulinemia), and complications resulting from type 2 diabetes, which made it impossible for us to meta-analyse such data. Furthermore, only some studies reported the OR of the relationship between type 2 diabetes and FA, which meant that few participants were included in the meta-analyses carried out, which suggests caution in its interpretation. Finally, it is possible to notice that the majority of our meta-analyses show a high I 2 value, which reveals a high heterogeneity in the analysis of the studies, which may be due to the varied sample sizes, the clinical variability in the samples of the included studies and of the different quality of the studies about the risk of bias.
In conclusion, the results of the meta-analyses showed a high prevalence of FA in individuals with type 2 diabetes and that the associations between these two conditions remained even after adjustment for age, sex and BMI, although with a high heterogeneity among individual estimates. Furthermore, few studies have evaluated the associations between FA and the biochemical parameters controlling the disease and its complications. Therefore, we highlight the need for future investigations that can elucidate the possible relationships between FA and type 2 diabetes, characterising a new line of research that should investigate the potential clinical impacts of the relationship between these two relationships.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S000711452500008X
Acknowledgements
The authors would like to acknowledge Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brazil (CAPES) and Conselho Nacional de Desenvolvimento Científico e Tecnológico – CNPq.
A. E. S. J. is supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brazil (CAPES) research fellowships (grant number: 88 887·805029/2023-00). MLM is supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brazil (CAPES) research fellowships (grant number: 88 887·679721/2022-00). NBB is supported by a research grant from the Conselho Nacional de Desenvolvimento Científico e Tecnológico – CNPq (grant number: 311401/2022-8). The sponsors had no role in the design and analysis of the study or the writing of this article.
A. E. S. J. conceived the study, wrote and reviewed the manuscript. M. L. M. and N. B. B. participated in the writing and review of the manuscript. All authors read and approved the final version of the manuscript.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.