


Introduction
Nearly 80% of patients admitted to an intensive care unit post-cardiac arrest are comatose because of hypoxic ischemic brain injury (HIBI). Sixty percent of these patients die following withdrawal of life-sustaining therapies (WLST) because of a predicted poor neurological outcome.Reference Nolan, Sandroni and Böttiger1 Consistent, objective, evidence-based, and accurate neuroprognostication of patients is crucial to avoid inappropriate WLST or prolonged, invasive, and costly therapies that could perpetuate patient and family suffering when there is no realistic chance of an acceptable functional neurological recovery.
A growing body of evidenceReference Sandroni, D’Arrigo and Cacciola2,Reference Sandroni, D’Arrigo and Cacciola3 and several guidelines exist Reference Nolan, Sandroni and Böttiger1,Reference Geocadin, Callaway and Fink4–Reference Fordyce, Kramer and Ainsworth9 for assisting clinicians in assessment of neurological prognosis. Ideally, neuroprognostication should be undertaken after confounding factors have been excluded and sufficient time has elapsed. Guidelines outline recommendations for neurological examination, diagnostic imaging, neurophysiologic tests, and biomarker findings that predict a poor prognosis. Due to the risk of “false-positive” prediction of poor outcome and resultant “self-fulfilling prophecies,” a multimodal approach to neuroprognostication is recommended.Reference Nolan, Sandroni and Böttiger1,Reference Geocadin, Callaway and Fink4 Canadian guidelinesReference Wong, van Diepen and Ainsworth10 for the care of the post-cardiac arrest patient are available, and Canadian guidelines for neuroprognostication postarrest have recently been published.Reference Fordyce, Kramer and Ainsworth9
Despite this large body of literature, guideline recommendations are based on relatively low-quality evidence, which likely contributes to variability of practices.Reference Bray, Cartledge and Finn11 Potential areas of controversy include what constitutes a confounding factor, the minimum amount of time that is needed to definitively conclude that a patient’s prognosis is poor, how best to approach multimodal prognostication, and what false-positive rate (FPR) is acceptable when determining prognosis. Furthermore, institutional protocols, perceptions of practitioners regarding accuracy of diagnostic modalities, and access to tests may influence neuroprognostication practices.
In view of this uncertainty, we conducted a cross-sectional survey of Canadian healthcare providers to investigate current practices and opinions regarding neuroprognostication in comatose post-cardiac arrest patients.
Methods
This study was approved by the University of Calgary Conjoint Health Research Ethics Board. The survey was designed based on recent recommendations.Reference Burns and Kho12,Reference Burns, Duffett and Kho13 The survey was endorsed and distributed by the Canadian Critical Care Society (CCCS), the Canadian Cardiovascular Society (CCS), the Canadian Neurological Sciences Federation (CNSF), and through program contacts from the University of Calgary.
Our sampling frame consisted of intensivists, cardiologists, and neurologists who regularly care for adult (≥18 years old) post-cardiac arrest patients. We specifically targeted physicians practicing in academic (with affiliated Royal College of Physicians and Surgeons of Canada certified training programs) or nonacademic Canadian hospitals, to obtain a breadth of opinions and practices. Both English- and French-speaking physicians were surveyed.
Survey development was led by two investigators (CMB and JAK) based on a MEDLINE review of relevant literature. Feedback from other neurocritical care specialists (AHK and PC) was obtained. Domains that were considered important included: (1) demographics, experience, and confidence with postarrest neuroprognostication; (2) use of guidelines or institutional protocols; (3) timing of prognostic assessments; (4) confounders that may interfere with neuroprognostication; (5) interpretation and perceived utility of neurological examination findings; (6) availability, interpretation, and perceived utility of diagnostic tests; (7) multimodal neuroprognostication considerations; and (8) provider distress during neuroprognostication. For the survey, a poor neurological prognosis was defined as a cerebral performance category (CPC) of 3–5 (severe neurological disability, persistent vegetative state, and death).
Based on these domains, possible questions were generated (CMB), which were, in turn, reviewed by a panel of neurocritical care specialists (JAK, AHK, and PC). Redundant questions, or those considered irrelevant by unanimous agreement, were removed to achieve a manageable number. Formatting was completed by a panel of three individuals (CMB, MM, and JAK), with attention to strategic ordering of questions to avoid influencing responses. The survey was designed to ensure respondents could not return to previous questions to adjust their answers.
Pretesting of the survey was undertaken by a group of experts from centers across Canada, who reviewed questions to ensure adequate clarity, relevance, and consistency in interpretation of the questions.
Pilot testing was completed by intensivists, cardiologists, and neurologists from a single Canadian center (University of Calgary), who were asked to comment on flow, salience, clarity, and administrative ease of the questionnaire. Modifications were made accordingly.
The survey was then disseminated nationally. Purposive sampling was utilized as individuals were invited to participate by the CCCS, CCS, and CNSF. The CCCS sent the survey by email to physician members for participation, the CCS posted the survey to its member’s board for participation, and the CNSF shared the survey for participation on their website for all members. In addition, the study team contacted physicians in each respective specialty at major academic institutions who were then asked to distribute the survey to others. Between two and three subsequent reminder emails were sent at approximately 2-week intervals in accordance with each professional association’s survey policies.
The survey was anonymous, self-administered by respondents, voluntary, and completed online using REDCap (see online appendix for a copy of the survey).Reference Harris, Taylor, Thielke, Payne, Gonzalez and Conde14 The survey required approximately 20 minutes to complete and was available in both English and French. No monetary or other incentive was offered for completion or participation.
Data were exported from REDCap into Excel.Reference Harris, Taylor, Thielke, Payne, Gonzalez and Conde14 Statistical analysis was performed (MM) using IBM SPSS Statistics for Windows, version 25.15 Results were reported as numbers and percentages of individuals who answered each question completely. The data were analyzed using Fisher’s exact test.
Results
Physician Demographics
The survey was distributed to 397 members of the CCCS, 1174 physicians from the CCS, and 1200 members of the CNSF. At least a portion of the survey was completed by 134 physicians. All surveys with responses to questions beyond the demographic section were included in the analysis.
There were responses from across the country, 91 (71%) of which were from Western Canada (British Columbia, Alberta, Saskatchewan, and Manitoba) followed by Ontario (n = 24, 19%), Quebec (n = 11, 9%), and Atlantic Canada (n = 2, 1.6%). There were no respondents from Northern territories. Respondents most often identified their specialty as critical care (n = 97, 72%), followed by neurology (n = 22, 16%), and cardiology (n = 15, 11%). Most respondents practice in academic centers (n = 109, 90%), with 500 or more beds (n = 85, 70%), that admit up to 100 postarrest patients per year (n = 62, 52%). There was a relatively equal distribution of early (0–10 years; n = 53, 42%), mid (11–20 years; n = 32, 25%), and late (>20 years; n = 43, 33%) career physicians. Most physicians (n = 89, 74%) prognosticated between 1 and 15 postarrest patients per year (Table 1, Supplement Table S1).
Demographics of survey respondents

‡Valid percentages; *for those patients not following commands. †All respondents indicated until patient wakes or is discharged from intensive care unit; % – (valid) percentage; # – number; AAN – American Academy of Neurology; AHA – American Heart Association; ERC – European Resuscitation Council; ANZCOR – Australian and New Zealand Committee on Resuscitation; °C – degrees Celsius; hrs – hours; NA – not applicable; % academic versus nonacademic is reflective of valid % within each type of center.
Use of Guidelines or Institutional Protocols
The majority (n = 72, 54%) of respondents utilize the American Heart Association (AHA) guidelinesReference Geocadin, Callaway and Fink4 followed by European Resuscitation Council (ERC)/European Society of Intensive Care MedicineReference Nolan, Sandroni and Böttiger1 (n = 39, 29%) and American Academy of Neurology (AAN)Reference Wijdicks, Hijdra, Young, Bassetti and Wiebe7 (n = 39, 29%) guidelines. Of the physicians who utilize the AAN Reference Wijdicks, Hijdra, Young, Bassetti and Wiebe7 guidelines published in 20067, 92% (n = 36) practice in academic centers. The majority of physicians who reported use the AAN Reference Wijdicks, Hijdra, Young, Bassetti and Wiebe7 guidelines are from Western Canada (n = 36, 92%) and Quebec (n = 4, 10%). Of the total number of respondents from each discipline who participated in the survey, there was a total of 27 (69%) critical care physicians, 11 (28%) neurologists, and 1 (50%) neurocritical care physician who identified that they use the AAN Reference Wijdicks, Hijdra, Young, Bassetti and Wiebe7 guidelines to guide postarrest management and neuroprognostication. Most physicians (n = 70, 63%) reported having no institutional protocols to guide postarrest neuroprognostication practices (Table 1).
When asked about targeted temperature management (TTM) for postarrest patients with a depressed level of consciousness, most physicians identified that they target euthermia (n = 57, 49%). There were 39 (33%) and 5 (4%) academic and 5 (4%) and 2 (2%) nonacademic respondents who target 34–36°C and 32–34°C, respectively (p = 0.24). Of those physicians who specified a specific temperature target, the majority (n = 77, 66%) maintained this target for 24–48 hours. Only a small number (n = 5, 4%) of physicians do not target a specific temperature in any postarrest patient (Table 1).
Timing of Neuroprognostication
The use of TTM had no significant effect on the time point where physicians were comfortable concluding that patients had a poor prognosis (Figure 1, Supplement Table S2). The number of definitive findings needed to conclude that the prognosis is poor affected the timing when physicians were comfortable and certain in decision-making. Over 50% preferred to wait beyond 5 and 8 days when only 1 or 0 definitive findings suggestive of a poor prognosis were present, respectively. When only one definitive finding suggested a poor prognosis post-rewarming if TTM was performed, 17% (n = 16) of physicians expressed uncertainty as to when they conclude that the prognosis is poor. In contrast, when there were two or more definitive findings suggestive of a poor prognosis post-TTM rewarming, 61% (n = 57) of physicians were comfortable determining a poor neurological prognosis between day 3 and 5. Additionally, when two or more definitive findings suggestive of a poor prognosis are present without the use of TTM, 55% (n = 51) of physicians were comfortable determining a poor neurological prognosis between day 3 and 5. Only one (1%) physician expressed uncertainty as to when they could conclude a poor prognosis under these circumstances (Figure 1, Supplement Table S2).
Percentage* of respondents indicating the earliest time point they are comfortable concluding a comatose patient with an unconfounded assessment has a poor neurologic prognosis (CPC 3–5) based on clinical scenarios. A: Earliest time point post-TTM‡ rewarming to normothermia that physicians are comfortable concluding a poor neurological prognosis (CPC 3–5) in unconfounded comatose** patients. B: Earliest time point post-ROSC when no TTM performed that physicians are comfortable concluding a poor neurological prognosis (CPC 3–5) in unconfounded comatose** patients. *Reported as valid percentages; ‡ TTM – Targeted Temperature Management 32–36∘C; ** Comatose defined as GCS ≤ 8; Confounders – see Table 2; Definitive findings – Exam: bilaterally absent pupillary light reflexes, bilaterally absent corneal reflexes, absent oculocephalic reflex, bilaterally absent vestibulo-ocular reflex, bilaterally absent gag reflex, absent cough reflex, lack of eye opening to painful stimuli, lack of purposeful motor response / EEG: status myoclonus, isoelectric background (<2 uV), suppressed background (<10 uV), highly epileptiform BS, non-epileptiform BS, GPDs on suppressed background, electrographic seizures, absent reactivity / SSEP: bilaterally absent N20 potentials / CT: subjective loss of gray-white, GM/WM <1.15 / MRI: extensive restricted diffusion of deep gray matter, extensive restricted diffusion of cerebral cortex, extensive restricted diffusion of cortex and deep gray matter / Serum Biomarkers: NSE (>33 ug/L, >60 ug/L), Protein S-100B, Creatine Kinase BB, Tau, Neurofilament Light Chain, GFAP, UCH-L1.

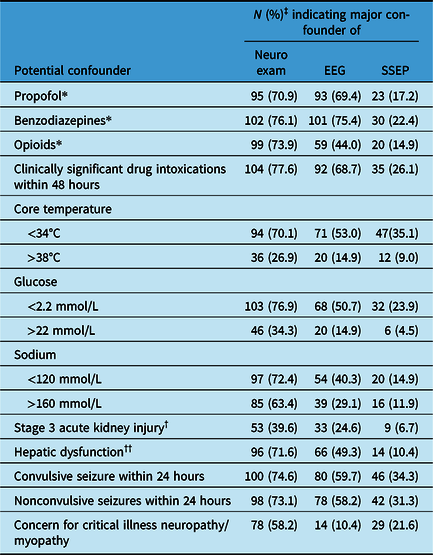
Number (percentage)‡ of respondents identifying major confounders of the neurologic examination, electroencephalography, and somatosensory evoked potentials

‡Valid percentages; * defined as ongoing infusion or impaired clearance with infusion discontinued within 48 hours; † defined as Cr≥3 times the upper limit of normal; †† defined as evidence of synthetic dysfunction.
The earliest time point physicians were comfortable concluding a patient has a poor prognosis with two or more definitive findings was less than 24 hours post-return of spontaneous circulation (ROSC) if no TTM was performed (n = 4, 4%). A small proportion (n = 6, 7%) of physicians identified that less than 24 hours postarrest is the earliest time points postarrest that they would be comfortable clinically determining death by neurological criteria (DNC) (Supplement Table S3).
Confounders
The proportion of respondents who agreed on potential confounders is shown in Table 2. Over 60% of respondents agreed on the following major confounders to the neurological exam: ongoing infusions or impaired clearance of propofol, benzodiazepines, or opioids; clinically significant drug intoxication within 48 hours; core temperature <34°C; glucose <2.2 mmol/L; Na <120 and >160 mmol/L; severe hepatic dysfunction; and both convulsive and nonconvulsive seizures within 24 hours. With electroencephalography (EEG), over 60% agreed that ongoing infusions or impaired clearance of propofol or benzodiazepines, as well as clinically significant drug intoxications within 48 hours would confound interpretation. No potential confounder reached over 60% agreement for somatosensory evoked potentials (SSEPs).
Other potential confounders that were highlighted by physicians included cardiorespiratory instability, hypercapnia, hypoxemia, severe acidosis, cervical spine injury, additional concomitant cerebral pathology (e.g., subdural hemorrhage and hydrocephalus), neuromuscular blockade, and profound hypophosphatemia.
Neurological Examination
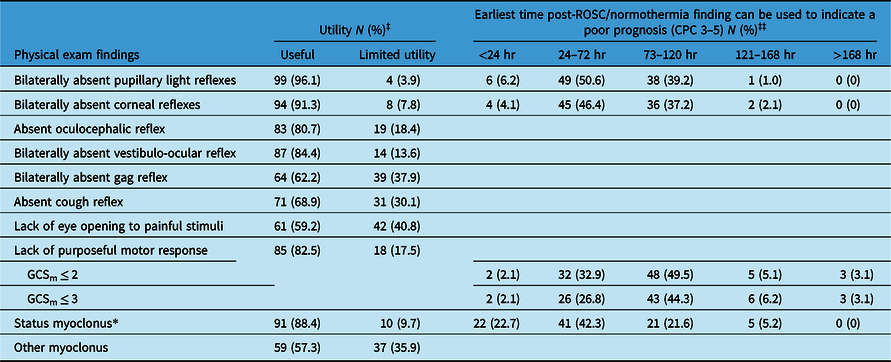
Regarding the neurological exam, 85, 80, and 75% (n = 88, 82, and 77) of physicians identified bilaterally absent pupillary light reflexes (PLR), bilaterally absent corneal reflexes (CR), and status myoclonus (SM, ≥30 min of sustained, diffuse myoclonus) respectively, as useful in determining that a patient has a poor prognosis (Table 3, Supplement Table S4).
Perceived utility and earliest time post-ROSC and return of normothermia that physical exam findings can be used to predict a poor neurologic prognosis (CPC 3–5)

‡Valid percentages reported – missing percentages are of those who indicated “unsure” to the question of utility; ‡‡ valid percentages reported – missing percentages are those who either indicated the finding was “not reliably predictive of a poor prognosis” or “unsure” to the question regarding timing; * defined as ≥30 min sustained, diffuse myoclonus.
Opinions regarding the timing of when exam findings could be used to predict a poor prognosis varied widely (Table 3, Supplement Table S5). A large proportion of respondents indicated that extensor (n = 87, 90%) or flexor (n = 77, 79%) posturing could be reliably used to predict a poor prognosis before 7 days postarrest. Only 40% (n = 39) and 39% (n = 38) of physicians indicated that the bilateral absence of PLR and CR, respectively, could be used to predict a poor prognosis on postarrest day 3 and beyond, with the majority of other respondents indicating these findings could be used earlier in a patient’s course to conclude a poor prognosis.
Test Availability, Interpretation, and Perceived Utility
Twenty percent (n = 19) of respondents indicated that a FPR of <5% for a diagnostic test is necessary for it to be considered definitive in neuroprognostication. Of these physicians, 79% (n = 15) practice in academic centers and 32% (n = 6, p = 0.045) have been practicing less than 5 years as an independent licensed physician. Thirty-two percent (n = 31) of physicians indicated that an FPR of <2.5% was preferable. Of these physicians, 87% (n = 27) practice in academic centers and 13% (n = 4, p = 0.045) have been practicing less than 5 years as an independent licensed physician. Of the physicians who chose an FPR of <1% (49%, n = 47), 92% (n = 43) practice in academic centers and 23% (n = 11, p = 0.045) have been practicing less than 5 years as an independent licensed physician.
Neuroprognostication test accessibility, perceived utility, and the time point at which specific findings can be used to conclude a poor prognosis are outlined in Table 4. Computed tomography (CT), magnetic resonance imaging (MRI), and routine (not continuous) electroencephalography (EEG) are easily available to 98, 87, and 82% (n = 98, 87, and 82) of physicians, respectively. SSEPs are available to 73% (n = 73) of physicians, but logistical challenges must often be navigated when trying to organize this test. The majority of physicians indicated that serum biomarkers [neuron-specific enolase (NSE), protein S-100B, creatinine kinase BB, tau, neurofilament light chain, glial fibrillary acidic protein (GFAP), and ubiquitin C terminal hydrolase-L1 (UCH-L1)] are not available at their centers (Supplement Table S6).
Accessibility, perceived utility, and earliest time post-ROSC/normothermia ancillary tests can be used to predict a poor neurological prognosis

‡Vaild percentages ‡‡ valid percentages – missing percentages are of those who indicated “unsure” to the question of utility; ‡‡‡ valid percentages – missing percentages are those who either indicated the finding was “not reliably predictive of a poor prognosis” or “unsure” to the question regarding timing; hr – hours; EEG – electroencephalography; uV – microvolts; BS – burst suppression; GPD – generalized periodic discharge; SSEP – somatosensory evoked potentials; CT – computer tomography; GM – gray matter; WM – white matter; MRI – magnetic resonance imaging; NSE – neuron specific enolase; ug/L – micrograms per liter; GFAP – glial fibrillary acidic protein; UCH-L1 – ubiquitin C terminal hydrolase-L1.
SSEP (n = 76, 76%), MRI (n = 75, 75%), CT (n = 62, 62%), and EEG (n = 61, 61%) were considered the most useful tests for neuroprognostication. Despite this, a variable number of physicians indicated certain findings on MRI, CT, and EEG (that are proven in the literature to predict a poor prognosis) were not reliable (Table 4, Supplement Table S7). Most indicated that they were unsure of the utility of serum biomarkers. Opinions regarding the timing by which test findings could be used to predict a poor prognosis varied widely (Table 4, Supplement Table S8).
Multimodal Neuroprognostication Considerations
Eighty-nine percent (n = 85) of respondents agreed if there are no definitive findings on the neurological exam, electrophysiologic tests, neuroimaging, or biomarkers, the prognosis is unclear. Most (n = 76, 79%) believed that ≥2 definitive findings on either the neurological exam, neurophysiologic tests, neuroimaging, and/or biomarkers is required to conclude that a patient has a poor prognosis (CPC 3–5) with reasonable certainty (FPR<5%). There was no consensus regarding whether a single definitive finding could be used to conclude a poor prognosis with adequate certainty (n = 25, 26% agreed, n = 40, 42% neutral, and n = 31, 32% disagreed). Most respondents (n = 83, 87%) agreed that when utilizing ≥2 definitive findings to predict a poor prognosis (CPC 3–5), these should be from different categories (Figure 2).
Multimodal approach to neuroprognostication. A: If no definitive findings from the neurological exam, electrophysiologic tests, neuroimaging, or biomarkers are present, the prognosis is unclear. B: 1 definitive finding on either neurological exam, electrophysiologic tests, neuroimaging, or biomarkers indicates a poor prognosis (CPC 3–5) with adequate certainty (FPR <5%). C: ≥2 definitive findings on either neurological exam, electrophysiologic tests, neuroimaging, and/or biomarkers are required to conclude a patient has a poor prognosis (CPC 3–5) with adequate certainty (FPR <5%). D: Ideally, when using ≥2 definitive findings to predict a poor prognosis (CPC 3–5), these should be from different testing categories (i.e., neuroimaging and exam or neuroimaging and electrophysiologic tests, etc.). E: When ≥2 definitive findings are present, it is not necessary to obtain additional tests.

In addition to the medical information obtained through multimodal neuroprognostication, respondents also indicated several other factors that should be taken into consideration when discussing goals of care. These included patient and family values, including religious and cultural beliefs, and expressed wishes such as those documented in advanced directives, the patient’s age, preexisting conditions, baseline functional status, the level of disability/length of rehabilitation that the patient and/or family would be willing to accept and donation considerations (i.e., donation after death determination by circulatory criteria) as appropriate.
Provider Confidence and Distress
Approximately 57% (n = 64) of physicians indicated feeling confident with accurately identifying patients with good (CPC 1–2) versus poor (CPC 3–5) outcomes at day 3–5 postarrest. (Supplement Figure S1a). However, 70% (n = 64) of physicians indicated some level of distress (mild n = 39, 42%, moderate n = 23, 25%, and severe n = 2, 2%) when determining a patient’s neurological prognosis (Supplement Figure S1b). Of the physicians who expressed mild and moderate distress, the majority were critical care physicians (80 and 58%, respectively) and for those who expressed severe distress, the responses were equally distributed between cardiologists (50%) and neurologists (50%). In addition, 51% (n = 47) of physicians frequently requested a second opinion from a colleague or external expert (neurology, n = 43; critical care/ICU, n = 39; neurocritical care, n = 32).
Discussion
Our findings demonstrate significant variability exists across Canada in neuroprognostication practices following cardiac arrest that are often inconsistent with recommendations from current guidelines.Reference Nolan, Sandroni and Böttiger1,Reference Geocadin, Callaway and Fink4,5,Reference Wijdicks, Hijdra, Young, Bassetti and Wiebe7–Reference Wong, van Diepen and Ainsworth10 While previous post-cardiac arrest prognostication surveys have been published,Reference Bray, Cartledge and Finn11,Reference Zhou, Barden and Gilmore16–Reference Lanfang, Zheng and Feng20 our study assesses more in-depth neuroprognostication considerations, including multimodal aspects, and describes opinions from academic and nonacademic intensivists, neurologists, and cardiologists from across Canada.
We identified that approximately 30% of respondents utilize the AAN guidelines. These were published in 2006 and have yet to be updated with contemporary evidence.Reference Sandroni, D’Arrigo and Cacciola2,Reference Sandroni, D’Arrigo and Cacciola3 This finding suggests that almost a third of Canadian physicians performing neuroprognostication may be doing so based on outdated guidance. Over 60% of facilities where respondents are employed do not have institutional protocols for postarrest care or neuroprognostication. Literature suggests that standardized critical care management protocols improve patient outcomes, streamlines care, and facilitate continuing medical education.Reference Lellouche, Mancebo and Jolliet21–Reference McCredie, Alali, Scales, Rubenfeld, Cuthbertson and Nathens24 Protocols may influence consistency across providers regarding timing of prognostication, exclusion of confounders, pertinent examination findings, useful diagnostic tests and relevant findings, as well as multimodal neuroprognostication considerations. In addition, protocols may help improve relative lack of confidence and variable levels of distress that 43 and 70% of physicians reported, respectively.
Timing of neuroprognostication is discussed at length throughout the literature, and AHA,Reference Geocadin, Callaway and Fink4 ERC,Reference Nolan, Sandroni and Böttiger1 and AANReference Wijdicks, Hijdra, Young, Bassetti and Wiebe7 guidelines recommend deferring definitive neuroprognostication for at least 72 hours post-ROSC or return of normothermia when TTM is utilized. Despite this, our results show that the use of TTM had no statistically significant impact on the timing of neuroprognostication. A small proportion of physicians expressed comfort determining a definitive prognosis for patients 24 hours or less postarrest. Utilizing suboptimal time points during the process of neuroprognostication in this patient population is a modifiable factor that, if addressed, may improve accuracy.
A small proportion of physicians (7%) indicated comfort declaring DNC 24 hours or less post-ROSC. Many guidelinesReference Greer, Shemie and Lewis25,Reference Shemie, Doig and Dickens26 caution against clinically declaring DNC within 24–48 hours postarrest, while others do not.Reference Wijdicks, Hijdra, Young, Bassetti and Wiebe7 The recently published Canadian guidelinesReference Shemie, Wilson and Hornby27 suggest delaying the clinical assessment for DNC for at least 48 hours from ROSC, unless there is imaging evidence consistent with devastating brain injury.Reference Shemie, Wilson and Hornby27 If there is radiographic evidence of devastating brain injury, the new guidelines suggest earlier determination of DNC is appropriate. In these circumstances where earlier DNC is suspected, it is important to consider that confounders may be present. Our survey results show that 57% of physicians currently are comfortable declaring death within 48 hours from an arrest. While our survey did not specify neuroimaging findings in the question, this suggests that significant knowledge translation may be required to ensure practices are aligned with updated guidelines.
Guidelines stress the importance of ensuring potential confounders are excluded during the process of neuroprognostication but do not provide more specific recommendations. To our knowledge, this survey is the first to ask detailed questions regarding possible confounders. The median threshold to define consensus based on Delphi criteriaReference Diamond, Grant and Feldman28,Reference Jaworska, Makuk and Krewulak29 is ≥75%. Our results highlight the lack of consensus surrounding what factors should be considered confounders of not only the neurological exam, but also EEG and SSEPs. Further research and consensus building efforts in this area are warranted.
Similar to other surveysReference Bray, Cartledge and Finn11,Reference Zhou, Barden and Gilmore16–Reference Lanfang, Zheng and Feng20 Canadian respondents placed high utility on several elements of the neurological examination. Over 90% indicated that bilaterally absent PLR or CR had some level of utility (53 and 44% very useful, 32 and 36% useful, 11 and 12% somewhat useful for PLR and CR, respectively) for neuroprognostication. While this is congruent with guidelines, at least 30 and 40% indicated that bilaterally absent PLR and CR, respectively, could be used to accurately predict a poor prognosis earlier than guideline recommendations of 72 hours. Respondents also indicated utility of other elements of the neurological exam that have not been validated as predictors. Specifically, over 80% of respondents indicated some utility (22% very useful, 28% useful, and 32% somewhat useful) of a lack of purposeful motor response when evaluated in insolation and more than 70% indicated this could be used within 5 days post-ROSC. This is despite evidence suggesting an unacceptably high FPR for both extensor and flexor posturing.Reference Lellouche, Mancebo and Jolliet21 The perceived differences in utility between SM and other forms of myoclonus suggests increasing awareness by Canadian physicians of the varying clinical implications of different types of postarrest myoclonus.Reference Kramer30,Reference Chakraborty, Braksick, Rabinstein and Wijdicks31
Our results highlight important discrepancies in access to diagnostic tests for neuroprognostication across Canada. Over 10, 15, and 75% of physicians indicated a lack of access or logistical challenges when arranging MRI, EEG, and SSEPs, respectively. Considering multimodal prognostication is recommended in guidelines, this highlights major access inequities within the Canadian health system that require attention. In particular, access to SSEPs should be increased.
Nearly 60% of individuals indicated similar concerns for access to continuous EEG. The recently published TELSTAR trialReference Ruijter, Keijzer and Tjepkema-Cloostermans32 suggests no improvement in outcomes when rhythmic and periodic EEG activity is suppressed with antiseizure medications. The characteristics of patients enrolled (nearly 60% with myoclonus and 30% lacking N20 potentials); only 56% success in achieving the treatment goal (48 hours of suppressed activity); and a high WLST rate (including within the first 24 hours) limit the external validity of this trial. Other studies suggest aggressive treatment of carefully selected individuals with rhythmic and periodic EEG activity or electrographic seizures may have benefits.Reference Beretta, Coppo and Bianchi33 Therefore, access to continuous EEG for select postarrest patients who may benefit from aggressive treatment is needed. While not all institutions will be able to implement this, there should be clear pathways in place that allows for triaging and transferring of patients who may benefit from aggressive treatment to centers with continuous EEG capabilities.
When assuming all tests are available, Canadian physicians placed similar importance on EEG and neuroimaging tests despite established and stronger evidence for SSEPs.Reference Sandroni, D’Arrigo and Cacciola2 Most respondents indicated uncertainty regarding the utility of biomarkers that matches the evolving literature in this area.Reference Fordyce, Kramer and Ainsworth9,Reference Hoiland, Rikhraj and Thiara34
Despite evidence and guidelines specifying time points at which certain test findings accurately indicate a poor prognosis, several physicians utilize them at time points of lower yield or may utilize findings that are not yet fully proven to definitively suggest a poor prognosis. Much of the EEG literature suggests a high FPR for certain patterns detected less than 24 hours post-ROSC (e.g., nonsynchronous burst suppression), likely related to acute confounders (such as sedation, metabolic derangements, or hypothermia) that may influence the EEG during this time. Nevertheless, approximately 10% of respondents indicated that such EEG patterns detected less than 24 hours post-ROSC definitively suggested a poor prognosis. Only one-third of individuals responded that EEG reactivity is not a reliable predictor of prognosis. Evolving literature that suggests more objective means of both testing and measuring EEG reactivity need to be established.Reference Zhou, Maciel, Ormseth, Beekman, Gilmore and Greer35–Reference Noirhomme, Lehembre, del and etal47
Another important consideration in diagnostic test interpretation is that of ensuring tests are interpreted by individuals not only with expertise within the modality but also with content expertise in integrating various findings and multimodal neuroprognostication. For example, while existing literature does not identify a critical threshold for volume of restricted diffusion on MRI to conclude a poor prognosis, no standardized reporting format has been suggested in the literature to guide reporting of neuroimaging for these patients. Thus, similar wording may be used to describe scans with a large or small burden of HIBI. It would therefore be advisable, when possible, for physicians, performing neuroprognostication, to review all test results, in addition to the reports themselves. The survey did not allow us to infer practitioner’s comfort at interpreting tests independently and their relative reliance on written diagnostic reports within this context. Further assessment of physician comfort with interpretation of prognosticating tests in this clinical context would be prudent.
The majority of physicians indicated a FPR of <1–2.5% was preferable in order to rely on diagnostic tests to predict a poor prognosis. A recent international survey that involved few Canadians and found medical providers preferred a FPR of <0.1% for recommending WLST.Reference Steinberg, Callaway and Arnold18 Our survey did not allow respondents to choose a percentage lower than 1%. The FPRs of all individual post-cardiac arrest diagnostic tests have confidence intervals that exceed these limits, therefore highlighting the importance of multimodal approaches. Most respondents agreed that ≥2 congruent predictive findings are required to definitively conclude that a patient has a poor neurological prognosis during the first week postarrest, and that these two findings should be from different categories (neurological exam, neuroimaging, EEG, SSEP, and/or biomarkers). Over 50% of respondents commonly request a second opinion. Clinicians practicing in centers with access to expertise in neuroprognostication and neurocritical care may predict functional outcomes more accurately and help alleviate provider reported distress.Reference Finley Caufield, Mlynash and Eyngorn48 In addition to medical information obtained through multimodal neuroprognostication, one of the factors that physicians indicated should be taken into consideration when discussing goals of care were donation after cardiac death (DCD). It is very important to note that one of the key concepts of DCD is that goals of care should not be influenced by DCD availability.Reference Shemie, Baker and Knoll49,Reference Weiss, Balamuth and Hensley50
This survey was designed with careful attention to recommended methodology and comprises a large representative cohort of Canadian physicians involved in neuroprognostication of postarrest patients. The release of the TTM2Reference Dankiewicz, Cronberg and Lilja51 trial results coincided closely with the circulation of our postarrest survey. Therefore,Reference Weiss, Balamuth and Hensley50 the impact of the trial on physician practice is likely not reflected in the collected responses. This survey was distributed while Canadian guidelines for post-cardiac arrest neuroprognostication were in development. It is possible that some respondents were part of the guideline working group, and this may have impacted the survey responses. Survey validity is directly correlated with response rate and completion of the survey. Our sampling frame was selected specifically to target critical care physicians, neurologists, and cardiologists who routinely care for adult postarrest patients; however, we did not capture opinions from other relevant team members including nurse practitioners or medical trainees. In addition, the overall response rate was low, as with most surveys.Reference Burns, Duffett and Kho13 However, this response rate may be an underestimate since many of the physicians the survey was distributed to do not regularly care for postarrest patients. The length and complexity of the questionnaire may have influenced the completion rate. Despite efforts to balance survey completion with capturing sufficient information to understand practices, only 69% who initiated the survey completed it.
Conclusions
Significant variability exists in post-cardiac arrest neuroprognostication practices among Canadian physicians. Practices that are inconsistent with current guidelines are relatively common. Standardized neuroprognostication protocols based on best evidence regarding optimal timing of assessments, exclusion of confounding factors, use of the most pertinent findings of neurological examination, use of additional diagnostic tests, and implementation of multimodal considerations may improve consistency and accuracy. Access to evidence-based tests and second opinions from experts in this field are important considerations to address current inequities within the Canadian healthcare system and ensure that all postarrest patients undergo individualized, evidence-based neuroprognostication. Further research is warranted to continue to advance this field and incorporate best evidence into practice.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/cjn.2023.261.
Acknowledgments
We acknowledge and thank the Canadian Cardiovascular Society, the Canadian Critical Care Society, the Canadian Neurological Sciences Federation, Dr Dan Zuege (Department Head – Department of Critical Care Medicine – Calgary, Canada), Dr Lara Cooke (Section Chief – Department of Clinical Neurosciences, Division of Neurology – Calgary, Canada), and Dr Carlos Morillo (Section Chief – Department of Cardiac Sciences, Division of Cardiology – Calgary, Canada) for endorsing and distributing our survey.
Funding
-
Caralyn M. Bencsik has no disclosures or funding to declare.
-
Dr Andreas H. Kramer was the co-chair of the Canadian Cardiovascular Society Position Statement for Neuroprognostication of the post-cardiac arrest patient. He is the Medical Director of the Southern Alberta Organ & Tissue Donation Program.
-
Dr Philippe Couillard has no disclosures or funding to declare.
-
Maarit MacKay has no disclosures or funding to declare.
-
Dr Julie A. Kromm was the lead for the electrophysiology section of the Canadian Cardiovascular Society Position Statement for Neuroprognostication of the post-cardiac arrest patient.
Competing interests
-
Caralyn M. Bencsik has no conflict of interest to declare.
-
Dr Andreas H. Kramer has no conflict of interest to declare.
-
Dr Philippe Couillard has no conflict of interest to declare.
-
Maarit MacKay has no conflict of interest to declare.
-
Dr Julie A. Kromm has no conflict of interest to declare.
Statement of authorship
-
Caralyn Bencsik contributed to the conception and design of the study, acquisition, and interpretation of data, drafting, and critically revising the manuscript for intellectual content and approved the final version of the manuscript.
-
Andreas Kramer contributed to the conception and design of the study, acquisition, and interpretation of data, drafting, and critically revising the manuscript for intellectual content and approved the final version of the manuscript.
-
Philippe Couillard contributed to the conception and design of the study, acquisition, and interpretation of data, drafting, and critically revising the manuscript for intellectual content and approved the final version of the manuscript.
-
Maarit Mackay contributed to the acquisition, analysis, and interpretation of the data, and critically revising the manuscript for intellectual content and approved the final version of the manuscript.
-
Julie Kromm contributed to the conception and design of the study, acquisition, and interpretation of data, drafting, and critically revising the manuscript for intellectual content and approved the final version of the manuscript.







 Open access
Open access