


Highlights
-
• We distributed a survey to Canadian neurosurgeons about their recommendations for the return to driving after a craniotomy.
-
• Recommendations were highly variable.
-
• Most Canadian neurosurgeons recommend at least 1–2 months seizure-free before resuming driving after a craniotomy for higher-risk conditions like gliomas or high-grade meningiomas, in otherwise seizure-naïve patients.
Introduction
Driving is a fundamental component of independence. Restrictions on driving following surgery can have profound implications for patients’ quality of life. Reference Lai and Du1–Reference Bergot, Cuchard, Mazeaud, Magro and Seizeur4 In recent years, there has been growing recognition of the need for standardized guidelines regarding driving restrictions following craniotomy.Reference Charmley, Kimber, Mahant and Lehn3, Reference Cho and Olson5, Reference Giraldi, Vinsløv Hansen, Wohlfahrt, Fugleholm, Melbye and Munch6 Such guidelines would aim to balance the safety of both patients and the public, while also ensuring that patients regain independence and autonomy in a timely manner.
It is well established in the literature that patients with neurological impairments or a prior history of seizures should abstain from driving for a specified duration.Reference Classen, Crizzle, Winter, Silver and Eisenschenk7–Reference Yale, Hansotia, Knapp and Ehrfurth12 Among patients who undergo craniotomy without a history of seizures, there is currently no consensus within the literature regarding the appropriate timing for resuming driving (Bergeron et al. joint submission).Reference Bergeron, Moshref, MacLean, Rizzuto, Walling and Christie13 There is a well-known risk of de novo epilepsy in seizure-naïve patients who undergo a craniotomy.Reference Giraldi, Vinsløv Hansen, Wohlfahrt, Fugleholm, Melbye and Munch6 The United Kingdom (UK) has developed an extensive list of driving recommendations for patients undergoing craniotomy for various neurosurgical conditions.14 In Canada, no equivalent set of standardized guidelines or recommendations exists (Bergeron et al. joint submission).Reference Bergeron, Moshref, MacLean, Rizzuto, Walling and Christie13 As a result, Canadian clinicians bear the responsibility of providing return to driving recommendations for their patients in the absence of supporting evidence. We anticipated this would yield marked variability in recommendations across provinces and even within healthcare institutions. Furthermore, factors such as patient demographics, geographical considerations and institutional policies may influence the decision-making process regarding driving restrictions post-craniotomy.Reference Cho and Olson5, Reference Xu, Shanthosh and Zhou15, Reference Lossius, Kinge and Nakken16
Prior to the establishment of nationwide guidelines for return to driving following craniotomy in patients without a prior history of seizures, a thorough understanding of current Canadian practice patterns is warranted. To bridge this knowledge gap, a survey was created and subsequently conducted among neurosurgeons affiliated with the Canadian Neurosurgical Society (CNSS) to assess the attitudes and practices of Canadian neurosurgeons regarding their recommendations on driving restrictions for patients undergoing craniotomy surgery.
Methods
The Canadian Neurosurgery Research Collaborative (CNRC)Reference Dakson, Tso and Ahmed17 developed a self-administered cross-sectional survey to assess the Canadian practice patterns regarding return to driving following craniotomy in patients without a history of seizures.
Survey development
We developed a survey with the objective of capturing the heterogeneity of clinicians’ recommendations for seizure-naïve, neurologically intact patients who undergo cranial procedures for various conditions. We constructed small scenarios to emphasize frequent conditions requiring a cranial procedure. We included conditions known to have a higher risk of post-operative seizures (glioma and high-grade meningioma) and conditions at low risk of post-operative seizures (pituitary adenoma and posterior fossa tumor) to evaluate how this affects clinicians’ recommendations. We added some modifiers to the scenarios, focusing on modifiers that are known to affect the risk of post-operative seizures (meningioma grade and temporal location of a glioma). For all scenarios, we mentioned that “The patient has no history of seizures and no post-operative deficit” to exclude these confounders from clinicians’ recommendations. We added a scenario with a patient who had seizures pre-operatively as a control question: in this situation, we expected all clinicians to answer “6 months without seizure” as it is clearly indicated in Canadian law. At the end of the questionnaire, we asked clinicians about their rationale regarding return to driving and their knowledge of existing guidelines. We tried to limit the length of the questionnaire to 5–10 minutes maximum (16 questions total; Appendix A).
Survey distribution
Survey design was iterative and completed by the primary investigators (DJNS and DB). The initial survey draft was assessed for redundancy and clarity by the steering committee of the CNRC. Face and content validity were assessed via board-certified neurosurgeons at multiple sites. The survey was electronically disseminated via the SurveyMonkey (San Mateo, United States) platform and distributed to neurosurgeons via the CNSS mailing list (totalling 120 staff neurosurgeons) between March 1st and December 30th, 2023 (sent three times total). CNRC residents were encouraged to solicit their mentors at their training hospitals to increase the response rate. Participation in the survey was voluntary and completely anonymous. Neurosurgical residents were not included as participants in this survey.
Data analysis
Descriptive analysis was employed to depict the characteristics of our cohort. Categorical variables were summarized using frequencies, percentages and charts.
Results
Forty-eight (40%) out of the 120 Canadian neurosurgeons on the CNSS mailing list responded to the survey. Nearly half of the respondents were from Quebec (n = 21; 44%), followed by Ontario (n = 9; 19%), British Columbia (n = 6; 13%) and other Provinces (Alberta, Nova Scotia, Saskatchewan). In terms of practice, 45 (94%) of the respondents indicated that they had an academic practice compared to three (6%) who were community-based. Thirty-five (73%) respondents reported not being aware of the existence of specific guidelines regarding return to driving after a craniotomy.
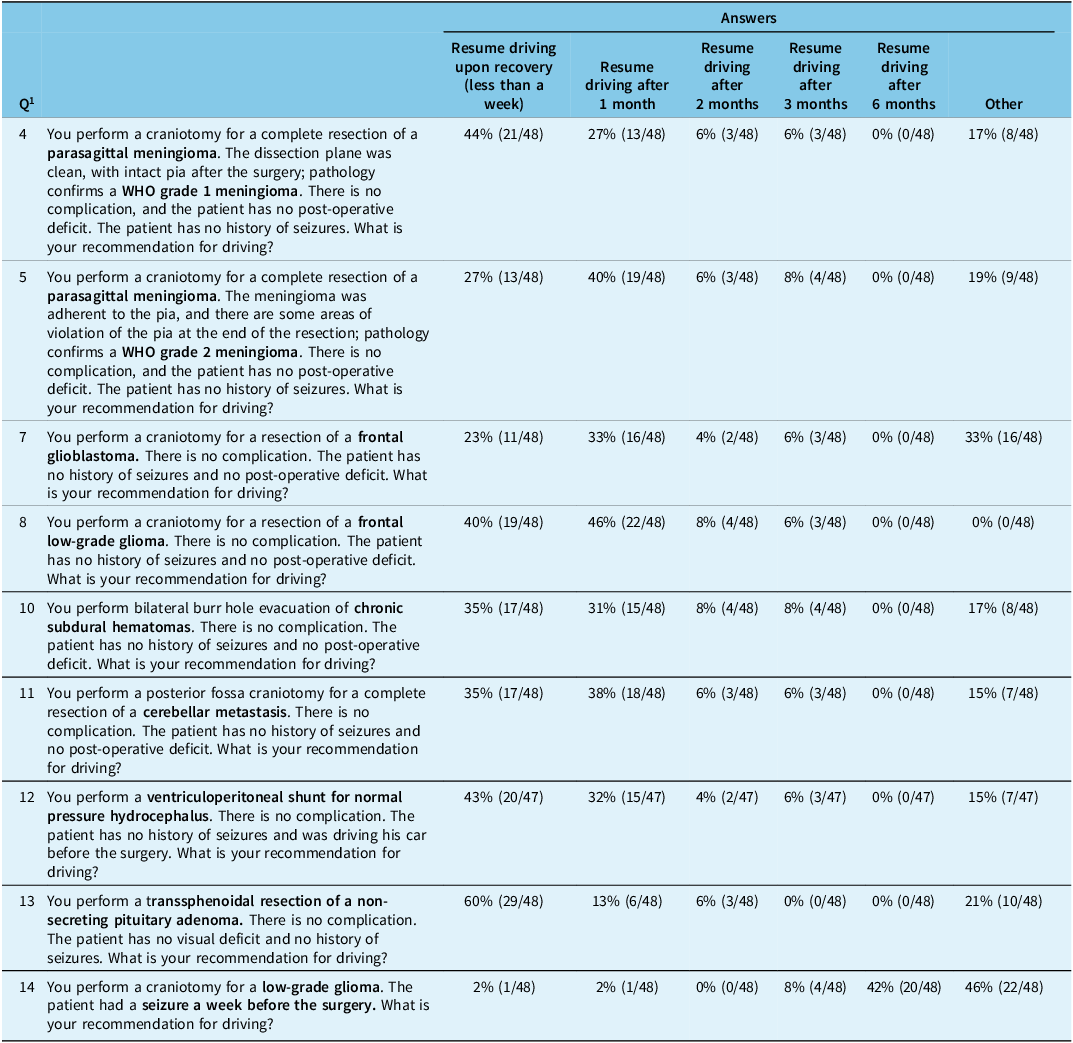
When physicians were questioned about their driving recommendations following the complete resection of a parasagittal World Health Organisation (WHO) grade 1 meningioma in patients who had an uneventful surgery and no history of seizures, 21 (44%) of the respondents indicated they would allow the patient to resume driving upon recovery (less than a week), while 13 (27%) respondents indicated one month (Table 1 – Q4). In contrast, if the patient had a parasagittal WHO grade 2 meningioma, 19 (40%) of the respondents would suggest the patient not drive for 1 month, while 13 (27%) of the respondents would allow the patient to resume driving upon recovery (i.e., less than 1 week) (Table 1 – Q5). Five respondents indicated that they would advise the patient not to drive until their post-operative outpatient visit (4–6 weeks post-operative). Forty-seven (98%) of the respondents reported that their recommendations would not change based on the location of the meningioma. A single respondent expressed that their recommendation would change as tumors located near the epileptogenic areas carry greater risk for post-operative seizures (Appendix – Q6).
Clinical scenarios and driving recommendations from the 48 Canadian neurosurgeons who completed the survey

1 Note: Questions with clinical scenarios are represented in the following table. Questions 1 to 16 from the survey distributed to Canadian neurosurgeons can be found in Appendix A. Answers in the “others” category were free text where clinicians expressed nuance (“it depends on […]”) or a distinct non-listed answer (“after follow-up appointment 6 weeks post-op”). They were analyzed separately by grouping into themes.
The following was observed regarding driving recommendations following complete resection of a frontal glioblastoma, for patients who had an uneventful surgery and no history of seizures: 16 (33%) respondents indicated they would recommend against driving until 1 month after surgery (Table 1 – Q7). One respondent indicated that the patient should not drive until radiation therapy was completed, even if the patient had no neurological impairment. In scenarios involving the resection of a frontal low-grade glioma, 22 (46%) of the respondents would recommend against driving until 1 month after the surgery, whereas 19 (40%) would allow the patient to drive within 1 week, provided their surgical recovery was uneventful (Table 1 – Q8). Moreover, 43 (90%) of the respondents said their recommendations would not change regardless of the location of the glioma. The remaining respondents (n = 5; 10%) indicated they would change their recommendation if the tumor involved the visual field area (Appendix – Q9). As a control question, we asked for driving recommendations if the same patient had a seizure one week pre-operatively: 42 (88%) respondents recommended to stop driving until 6 months of seizure-freedom, or demand an evaluation by a neurologist, consistent with Canadian guidelines (Table 1 – Q14).
Following surgeries, including craniotomy for evacuation of chronic subdural hematoma, cerebellar metastasis resection or ventriculoperitoneal shunt for normal pressure hydrocephalus, the majority of respondents indicated they would allow the patient to drive without restriction after surgery (less than 1 week) or one-month post-operative (Table 1 – Q10-12). In the setting of transsphenoidal resection of non-secreting pituitary adenoma without post-operative complications, 29 (60%) of the respondents would allow driving if they do not have significant neurological or visual deficits and do not take opioid medication. Of the 10 (21%) respondents who indicated “other” as their recommendations, 50% reported they do not perform skull base surgery, while the other half preferred that the patient undergo evaluation by neuro-ophthalmology to confirm the absence of visual defects prior to return to driving (Table 1 – Q13).
When neurosurgeons were questioned about the rationale guiding their driving recommendations, 18 (38%) did not provide an answer. Of those who did respond, the majority indicated that they did not know of specific guidelines. Rather, they base their recommendations depending on the patient’s physical and neurological condition following surgery. Finally, we attempted to evaluate interest in participating in the development of standardized Canadian driving guidelines. Sixteen respondents answered “yes,” expressing a willingness to contribute to the formulation of the first Canadian driving guidelines for returning to driving following craniotomy for those patients who have no history of seizures.
Discussion
The aim of this study was to gain a better understanding of the current Canadian practice patterns regarding return to driving recommendations for patients having undergone craniotomy with no prior history of seizures. Forty-eight Canadian neurosurgeons completed the survey, which demonstrated a lack of consensus regarding return to driving restrictions following craniotomy in patients with no seizure history across Canada. The majority of respondents stated that they allowed patients to resume driving after the craniotomy as soon as one week post-operatively (given they are not on opioid medication or have a new post-operative neurological deficit), or after 1 month without seizure. These recommendations are more lenient than those identified in other jurisdictions such as the UK (Bergeron et al. joint submission).Reference Bergeron, Moshref, MacLean, Rizzuto, Walling and Christie13 They are also more lenient than recommendations identified through a similar survey performed in Australia and New Zealand: most neurosurgeons advised against driving for 6 months without seizures, in concordance with the Austroads guidelines for private vehicles following craniotomy, irrespective of underlying pathology.Reference Cho and Olson5
The main strength of this study is its national reach, with a sample of 48 neurosurgeons across Canada. The inclusion of a diverse range of clinical scenarios helped us capture nuances in the surgeons’ recommendations. As in most survey studies, there is a risk of a sample bias; in other words, it is plausible that neurosurgeons who did not participate in the survey have driving recommendations and rationales that differ from those observed in this study. With an estimated 339 neurosurgeons in Canada in 2019,18 our 48 respondents represent approximately 14% of the National neurosurgeon population. Surgeons practicing in an academic hospital were over-represented in our sample, due to the outreach through the CNSS mailing list and through the neurosurgery residents of the CNRC distributing the survey to their mentors at academic teaching hospitals. Also, neurosurgeons from the Province of Quebec were over-represented, representing 21/48 (44%) respondents in our sample compared to 80/339 (24%) of the Canadian neurosurgeon population. Although the sample is not perfectly representative of the Canadian neurosurgeon population, the variability in recommendations regarding return to driving after a craniotomy in our study highlights the need for more guidance or guidelines on this issue in Canada. We are working toward a set of evidence-based recommendations to guide Canadian neurosurgeons in their counseling of patients after a craniotomy (Bergeron et al. joint submission).Reference Bergeron, Moshref, MacLean, Rizzuto, Walling and Christie13
Conclusion
This Canadian study provides valuable insight into the lack of consensus on recommendations regarding return to driving following craniotomy in patients without a history of seizures in Canada. It is part of a broader effort to provide evidence-based recommendations to guide Canadian neurosurgeons in their counseling of patients after a craniotomy.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/cjn.2025.10525.
Acknowledgements
We thank all the neurosurgery staff and residents across Canada for making this work possible. We would like to acknowledge the funding support from the CNSS for the general operations of the CNRC.
Author contributions
DB and DJNS participated equally in the project. DB and DJNS drafted the initial version of the manuscript. DB, DJNS, TD, MR, MAM, MAR, MR and NP contributed to data collection and analysis. SW and SDC supervised the project. All authors approved the final version of the manuscript.
Funding statement
No funding was obtained for this study.
Competing interests
The authors report no conflict of interest in the writing of this study.
Ethical standards
The ethical committee approval was not required, given the article type.



 Open access
Open access
Target article
Assessment of Driving Restrictions Following Craniotomy: A Survey of Canadian Neurosurgeons
Related commentaries (1)
Reviewer Comment on Ndongo Sonfack et al. “Assessment of Driving Restrictions Following Craniotomy: A Survey of Canadian Neurosurgeons”