



Introduction
Individuals affected by neuromuscular diseases (NMDs) represent a clinically heterogeneous population with hereditary or acquired disorders involving muscles, neuromuscular junctions, peripheral nerves, or lower motor neurons. The predominant and common symptoms are muscle weakness and atrophy, fatigue, and pain. In addition, dysphagia, dysarthria, respiratory disorders, and multisystem involvement (i.e., gastrointestinal and cardiovascular system, liver and central nervous system) may be associated(Reference Salera, Menni, Moggio, Guez, Sciacco and Esposito1). These factors significantly and progressively affect the mobility and autonomy of NMD patients, and the quality of life of both patients and their family members/caregivers(Reference Jones, Hawke, Newman, Miller, Burns and Jakovljevic2–Reference Dangouloff, Boemer and Servais4).
NMD patients are at increased risk of malnutrition: undernutrition may arise from reduced appetite and subsequent decrease in food intake, leading to inadequate energy and macronutrient and/or micronutrient intake(Reference Amzali, Wilson, Bommart, Picot, Galas and Mercier5). Conversely, some patients may experience overnutrition due to excessive caloric intake (with or without micronutrient deficiency), developing overweight and obesity, which can even be promoted by physical impairment, reduced activity, and pharmacological treatments, such as steroid drugs(Reference Billich, Evans, Truby, Ryan, Kornberg and Davidson6).
In this population, gastrointestinal disorders are frequently observed: constipation, gastroesophageal reflux disease, dysphagia, and delayed gastric emptying contribute to maintaining or even worsening an inappropriate nutritional status(Reference Chou, Lindeback, D’Silva, Sampaio, Neville and Farrar7,Reference Dipasquale, Morello and Romano8) .
Common pathophysiological mechanisms in NMDs may include chronic inflammation, increased oxidative stress, autophagy, and mitochondrial dysfunction, which contribute to progressive muscle atrophy, neural damage, and functional decline(Reference Forgues, Fortin, Gagnon, Brisson, Mathieu and Brais9–Reference Zhang, Qi, Wang, Yang, Shen and Yang11).
Current therapy of most NMDs is mainly symptomatic, with analgesic and corticosteroid therapy supplementing motor rehabilitation courses; the assessment of how diet and lifestyle can affect the condition of these patients should not be overlooked. Despite extensive evidence on the role of lifestyle – defined as diet, physical activity, quality of personal and social relationships, sleep hygiene, and smoking and alcohol addictions – in the prevention and management of chronic diseases, there is still inconclusive literature assessing the potential effects of these factors on the clinical course and on the quality of life (QoL) of patients with NMDs(Reference Choi, Ow, Yang and Taneja12–Reference Zhang, Devlin, Smith, Imperatore, Thomas and Lobelo14).
Few aspects of lifestyle have been studied in NMDs, and most of these were individual studies. Regarding physical activity, although the mobility of these patients varies greatly according to the type of NMD and the progression of the disease, monitoring and promoting physical activity can positively affect the overall clinical outcome(Reference Voet, van der Kooi, van Engelen, Lindeman, van Engelen and Geurts15,Reference Bettio, Banchelli, Salsi, Vicini, Crisafulli and Ruggiero16) .
There are currently few works in which the role of diet in this pathological context has been evaluated; the Mediterranean diet is among the most studied beneficial dietary patterns. The Mediterranean diet, rich in vitamins, fibres, and phytochemicals, and low in sugars, salt, and ultra-processed foods, could provide valuable support in counteracting the oxidative and inflammatory damage associated with NMDs(Reference Serra-Majem, Tomaino, Dernini, Berry, Lairon and Ngo de la Cruz17,Reference Petrella, Di Certo, Gabanella, Barbato, Ceci and Greco18) .
The Mediterranean model is not only a dietary pattern, but encompasses many other aspects of lifestyle, such as daily physical activity, balance of daily activities and nightly rest, conviviality and care of social relationships. Sharing experience of meals, not only in terms of consumption but also of preparation, as well as the choice of seasonal and locally sourced foods, are distinctive factors of this model(Reference Petrella, Di Certo, Gabanella, Barbato, Ceci and Greco18,Reference Bakırhan, Özkaya and Pehlivan19) .
The purpose of this systematic review is to evaluate the state of art of the recent scientific evidence on the role of diet and nutrition, with particular focus on the Mediterranean diet and lifestyle, in affecting the clinical course of NMDs and the QoL of these patients.
Methods
This systematic review meets criteria of the Preferred Reporting Items for Systematic Reviews and Meta-Analyse (PRISMA)(Reference Page, Mckenzie, Bossuyt, Boutron, Hoffmann and Mulrow20).
Eligibility criteria
We included cross-sectional, prospective, and retrospective cohort studies, as well as randomised and non-randomised clinical trials, investigating the relationship between lifestyle or diet and these neuromuscular conditions, published in the past five years in peer-reviewed scientific journals. We included articles published in the last five years to provide an updated overview of recent evidence, reflecting current clinical practice. Articles were excluded if they were not published in English, were preprints or unpublished, were preclinical studies (including in vitro or animal-model studies), reviews, systematic reviews, meta-analyses, brief communications, letters to the editor, case reports, case series, guidelines, or conference abstracts. Additionally, articles that did not evaluate any aspect of the patients’ lifestyle, or those that did not provide a diagnosis of neuromuscular disease at baseline or follow-up, were excluded.
Information sources and search strategy
An electronic search was conducted on 24 September 2024 to identify published articles that mentioned ‘neuromuscular disorders’, ‘muscular dystrophy’, ‘peripheral neuropathy’, ‘myopathy’, ‘motor neuron disease’, or ‘myasthenia’ in combination with ‘diet’, ‘nutrition’, ‘lifestyle’, or ‘Mediterranean diet’. The following electronic databases were utilised, along with their respective search strings:
-
- PubMed: Title/Abstract: ((‘neuromuscular disorders’[Title/Abstract] OR ‘muscular dystrophy’[Title/Abstract] OR ‘peripheral neuropathy’[Title/Abstract] OR ‘myopathy’[Title/Abstract] OR ‘motor neuron disease’[Title/Abstract] OR ‘myasthenia’[Title/Abstract]) AND (diet[Title/Abstract] OR nutrition[Title/Abstract] OR lifestyle[Title/Abstract] OR ‘Mediterranean diet’[Title/Abstract])) AND (English[Language]).
-
- Web of Science: Title/Abstract: ((TI=((‘neuromuscular disorder’ OR ‘muscular dystrophy’ OR ‘peripheral neuropathy’ OR myopathy OR ‘motor neuron disease’ OR myasthenia) AND (diet OR nutrition OR lifestyle OR ‘Mediterranean diet’))) OR AB=((‘neuromuscular disorder’ OR ‘muscular dystrophy’ OR ‘peripheral neuropathy’ OR myopathy OR ‘motor neuron disease’ OR myasthenia) AND (diet OR nutrition OR lifestyle OR ‘Mediterranean diet’))) AND LA=(English).
-
- Scopus: Title/Abstract: (TITLE((‘neuromuscular disorders’ OR ‘muscular dystrophy’ OR ‘peripheral neuropathy’ OR myopathy OR ‘motor neuron disease’ OR myasthenia) AND (diet OR nutrition OR lifestyle OR ‘Mediterranean diet’))) OR ABS((‘neuromuscular disorders’ OR ‘muscular dystrophy’ OR ‘peripheral neuropathy’ OR myopathy OR ‘motor neuron disease’ OR myasthenia) AND (diet OR nutrition OR lifestyle OR ‘Mediterranean diet’))) AND LANGUAGE(English) AND PUBYEAR > 2019 AND (LIMIT-TO(EXACTKEYWORD, ‘Humans’)).
Selection and data collection process
A team consisting of one researcher and one associate professor in nutrition science from the Department of Clinical and Experimental Sciences at the University of Brescia, Italy (SM, BZ), and a research fellow from the same department (GG), reviewed the abstracts of selected studies and independently evaluated articles according to the established inclusion criteria, removing duplicates. The team members, along with a master’s student in dietetics from the University of Brescia (DC), collected and synthesised data by thoroughly reviewing each selected article. Neurological data were subsequently evaluated by an associate professor of neurology at the Department of Clinical and Experimental Sciences at the University of Brescia, an expert in the field of neuromuscular diseases (MF). Disagreements or uncertainties were resolved through group discussions. No automated tools or artificial intelligence resources were employed during this process.
Data items
For each selected article, information regarding authorship, year of publication, journal, study period and location, World Health Organization (WHO) region, and study design were recorded in a purpose-built Excel sheet, organised in three sections. The first section of the database contains baseline data about patients, including their number and, where available, the number and type of control subjects, demographics (age, sex, ethnicity), education level, employment status, family situation (caregivers), specific diagnosis of neuromuscular disease and associated pharmacological treatments, most affected body areas, movement limitations, comorbidities, and the use of additional medications and/or supplements. Information on gastrointestinal issues (e.g., vomiting, gastroesophageal reflux, dysphagia, bowel irregularities) and feeding methods (oral or artificial nutrition) was also included, along with weight, body mass index (BMI), body composition data (specifically lean mass and fat mass), and nutritional status and related assessment methods. The second section of the database includes information regarding diet, nutrition, and lifestyle aspects of patients with NMDs, as assessed by relevant questionnaires: in addition to dietary habits, we evaluated other lifestyle factors if addressed in the selected articles, such as physical activity, substance use (alcohol and smoking), emotional perception and care, and sleep quality. Data or investigations related to the microbiota were included, if available. Finally, the last section includes study duration, primary and secondary endpoints, interventions, QoL, changes in endpoints, and dropout rates. For missing or unclear data, ‘not available-NA’ was recorded.
Synthesis methods
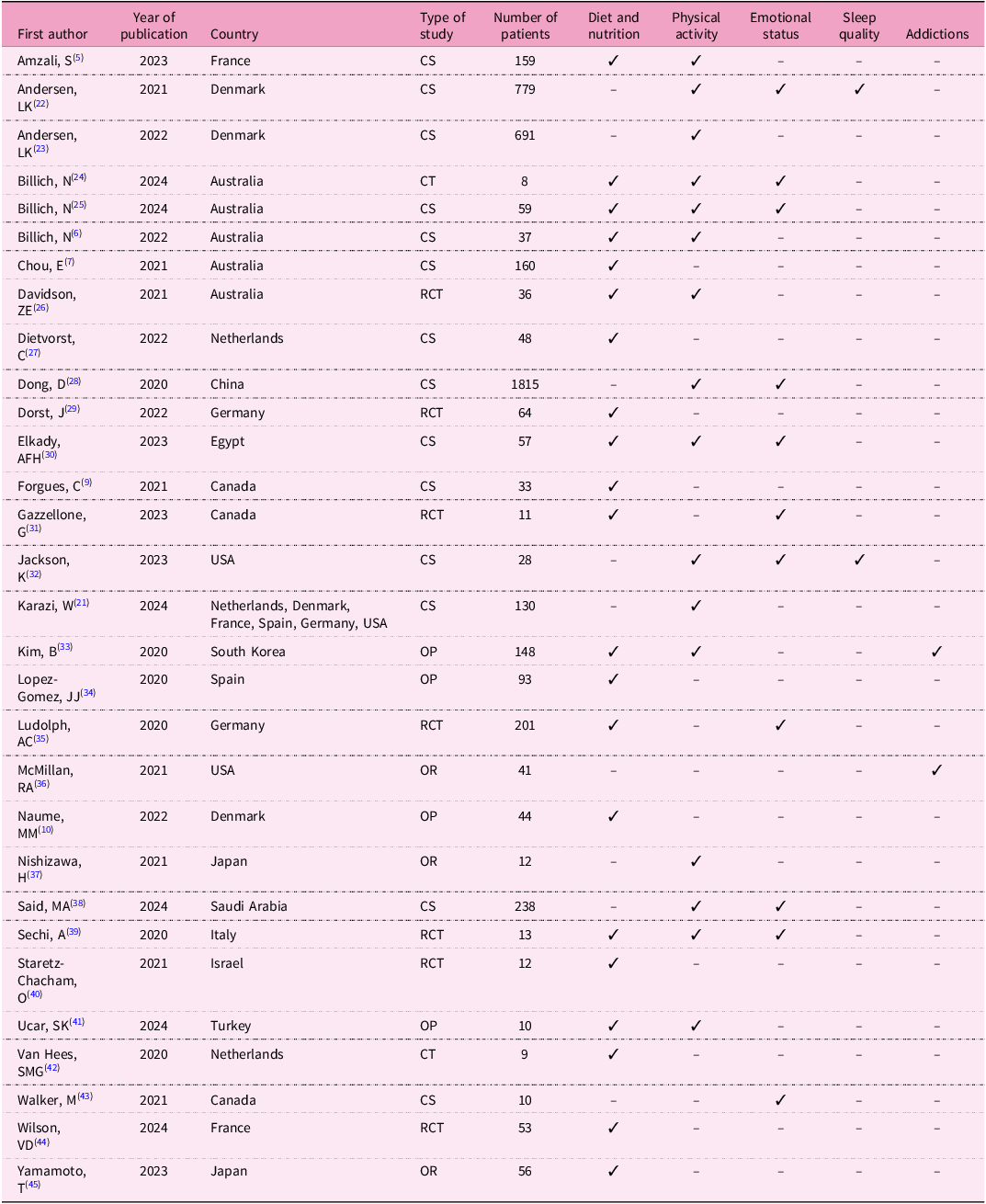
All collected data were summarised into six tables for ease of analysis. Table 1 describes the types of articles selected, the publication year, and the country in which the study was conducted. Demographic data of patients (number, age, sex, ethnicity, education level, and employment status) are summarised in Table 2, while clinical data (type of NMD, steroid treatment, supplements, feeding method, gastrointestinal problems, and comorbidities) and microbiota analysis are presented in Table 3. Table 4 includes anthropometric measurements (BMI or BMI z-score, waist circumference, body composition, malnutrition screening, and nutritional status). Lifestyle aspects are summarised in Table 5: the number of patients evaluated in relation to dietary habits and other different lifestyle aspects (physical activity, sleep quality, addictions, and emotional perception and care) are reported. Finally, Table 6 lists the individual studies included in the review, detailing the first author, publication year, country, study design, sample size, and lifestyle aspects investigated. Percentages were calculated based on the available data for each specific characteristic.
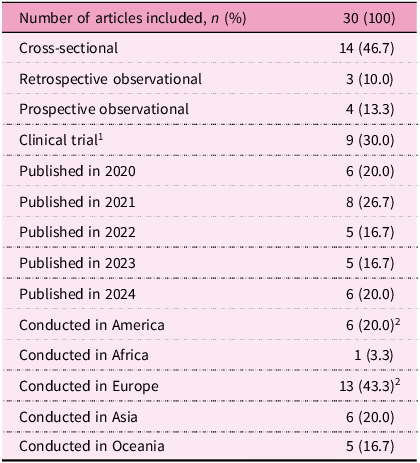
Type of articles included

Notes:
1. Seven randomised controlled trials and two non-randomised.
2. The study by W. Karazi et al.(Reference Karazi, Coppers, Maas, Cup, Bloemen and Voet21) recruited patients from both Europe and America, and was counted in both subgroups.
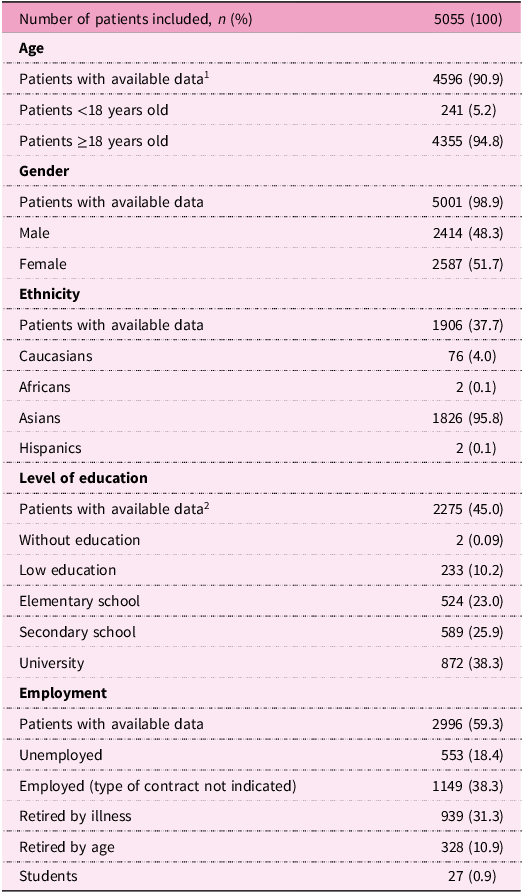
Demographic data

Notes:
1. The total count included only those patients for whom age was expressed as a mean and standard deviation; the count excluded those items with median and classes/age groups.
2. Included 55 patients whose level of education was not specified and 12 children attending elementary school.
Clinical data

Anthropometric data and nutritional status

Lifestyle aspects

List of selected studies with first author, year of publication, country, type of study, number of patients, and investigated aspects of lifestyle

Note: CS, cross-sectional; OR, observational retrospective; OP, observational prospective; RCT, randomised clinical trial; CT, clinical trial.
Bias and certainty assessment
Given the considerable heterogeneity in study design, populations, and assessment tools, this review was conducted as a narrative systematic review with qualitative analysis of the results and narrative synthesis, in line with PRISMA-S and Cochrane recommendations.
Percentages were calculated based on the available data for each considered element. This article does not represent a meta-analysis; therefore, as per the latest PRISMA guidelines(Reference Page, Mckenzie, Bossuyt, Boutron, Hoffmann and Mulrow20), no models were applied to assess statistical heterogeneity or sensitivity analyses to evaluate the robustness of the synthesised results. To enhance the methodological rigour of this narrative review and address potential sources of bias, the quality of all included studies was independently assessed by two authors (SM and GG) using the Mixed Methods Appraisal Tool (MMAT), version 2018. For each study, the two screening questions were first evaluated, followed by the five core criteria appropriate to the study design category. Each criterion was rated as ‘Yes’, ‘No’, or ‘Can’t tell’. Disagreements between authors were resolved through discussion and consensus. In accordance with MMAT guidance, no overall quality score was calculated; instead, the detailed ratings for each criterion are presented to allow readers to evaluate strengths and limitations transparently. The results of this appraisal are reported in Supplementary Table S1.
Results
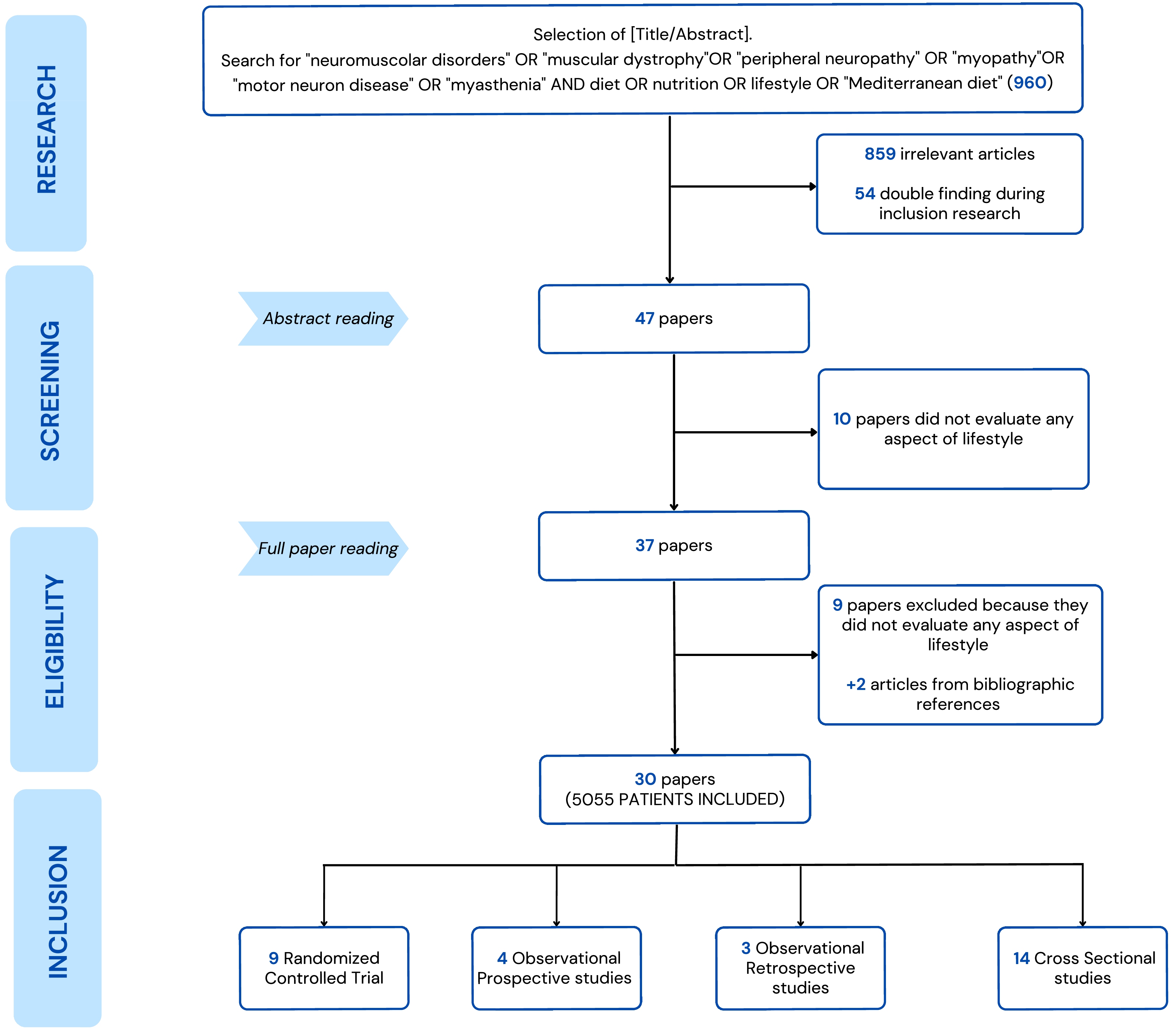
The search conducted across the three databases led to an initial number of 960 articles: 272 from PubMed, 478 from Web of Science, and 210 from Scopus. After applying the inclusion and exclusion criteria, 101 articles were selected. After removal of duplicates, the number decreased to 47. Out of these papers, ten articles were excluded for not aligning with the objective of the current project. Full-text reading of the remaining 37 articles led to the exclusion of those that did not address any aspect of diet, nutrition, or lifestyle, or that focused only on caregivers rather than patients. Eventually, 30 studies were selected for the purpose of the review, inclusive of two more articles manually identified from the reference lists of the other papers(Reference Amzali, Wilson, Bommart, Picot, Galas and Mercier5–Reference Chou, Lindeback, D’Silva, Sampaio, Neville and Farrar7,Reference Naume, Jørgensen, Høi-Hansen, Born, Vissing and Borgwardt10,Reference Zhang, Qi, Wang, Yang, Shen and Yang11,Reference Karazi, Coppers, Maas, Cup, Bloemen and Voet21–Reference Yamamoto, Mori-Yoshimura, Oya, Komaki and Takahashi45) . The article selection and screening process is detailed in Figure 1.
Flowchart summarising the systematic approach of article selection.

The total number of patients investigated in this literature review was 5055. Regarding the subjects for whom age data were available (90.9%), 94.8% were adults (aged ≥18 years) and 5.2% were paediatric patients. The female population represented 51.7% (2587 out of 5001 people with available data), and out of the 1906 patients with available ethnicity data 95.8% were Asian, 4% Caucasian, while African and Hispanic ethnicities represented 0.1%. Education level data were available for 45% of patients (2275/5055) and out of these 10.2% had a low level of education, limited to elementary school, 23% completed elementary school (middle school), 25.9% completed secondary school (equivalent to high school in some educational systems), and 38.3% completed higher school. Two patients (0.1%) reported having no formal education. Regarding employment status, data were available for 59.3% of the study population (2996/5055): 18.4% were unemployed, while 38.3% were currently employed (whether full-time or part-time was not specified), 31.3% had to quit work activities because of the disease, 10.9% were retired, and 0.9% (a total of 27 patients) were students. All demographic data for the study population are summarised in Table 2.
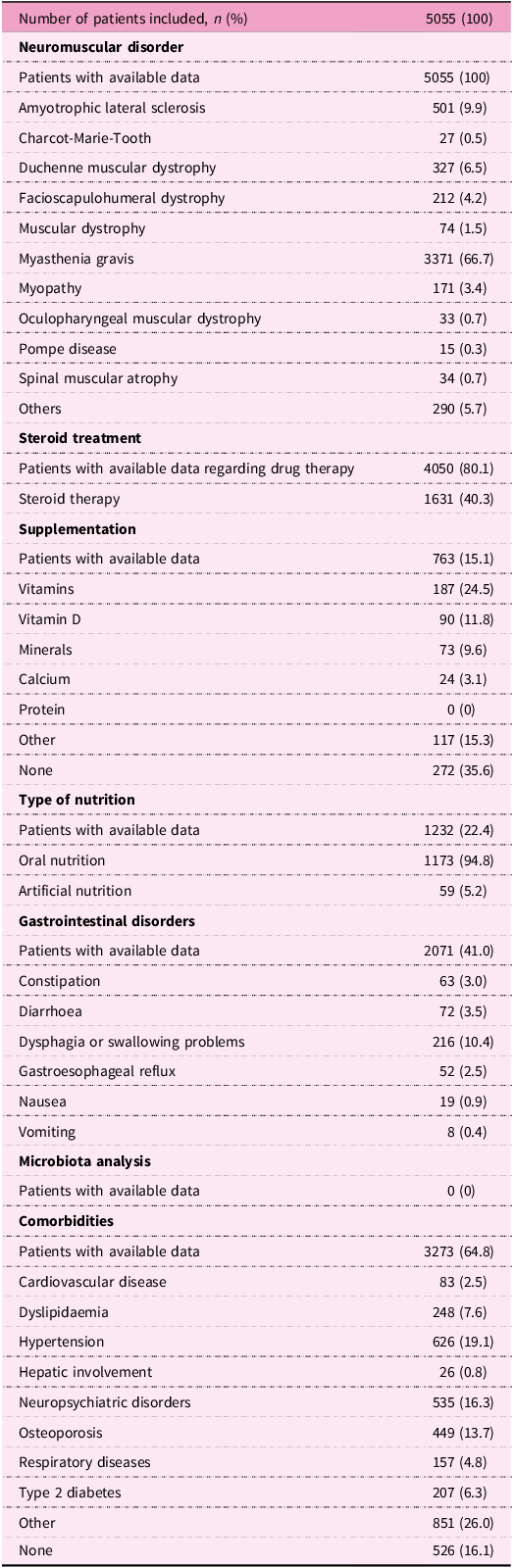
Most patients were affected by myasthenia gravis (MG; n = 3371; 66.7%), followed by those with amyotrophic lateral sclerosis (ALS; n = 501; 9.9%), Duchenne muscular dystrophy (DMD; n = 327; 6.5%), and facioscapulohumeral dystrophy (FSHD; n = 212; 4.2%). In addition, patients with myopathies of different origins (3.4%), spinal muscular atrophy (SMA; 0.7%), oculopharyngeal muscular dystrophy (0.7%) and other muscular dystrophies (MD; 1.5%), Charcot-Marie-Tooth pathology (CMT; 0.5%), and Pompe disease (0.3%) were included. Patients with other rare neuromuscular conditions were grouped in the ‘other’ category, accounting for 5.7% of the whole study population.
Drug therapy data were available for 4050 patients and among them 40.3% (n = 1631) were on steroid treatment. Moreover, 15.1% of all patients (n = 763) reported data about supplementation; among them, 24.5% were supplemented with vitamins, of which 11.8% were with vitamin D, 9.6% with minerals, especially calcium (3.1%), and 15.3% with other types of supplements. No patients were on protein supplementation and 35.6% did not report supplements intake.
Data on type of nutrition were available for 1232 patients (22.4%), of whom 94.8% were fed orally, while 5.2% relied on artificial nutrition. Evaluation of gastrointestinal disorders was available for 2071 patients (41% of the sample); among them, 10.4% reported dysphagia or difficult swallowing. Other reported gastrointestinal complaints included diarrhoea (3.5%), constipation (3.0%), gastroesophageal reflux (2.5%), nausea (0.9%), and vomiting (0.4%).
No data related to microbiota were identified in any included studies.
Regarding comorbidities, data were collected for 3273 patients (64.7%). Among them, 19.1% suffered from hypertension, 16.3% from neuropsychiatric disorders, 13.7% from osteoporosis, and 7.6% from dyslipidaemia. Other less frequent comorbidities included type 2 diabetes (6.3%), respiratory disease (4.8%), cardiovascular disease (2.5%), and liver disease (0.8%). The least frequently reported comorbidities were grouped in the ‘other’ category (26.0%). In some studies, comorbidities were an exclusion criterion; these patients accounted for 16.1% of the total.
All clinical data for the 5055 patients included in this systematic review are summarised in Table 3.
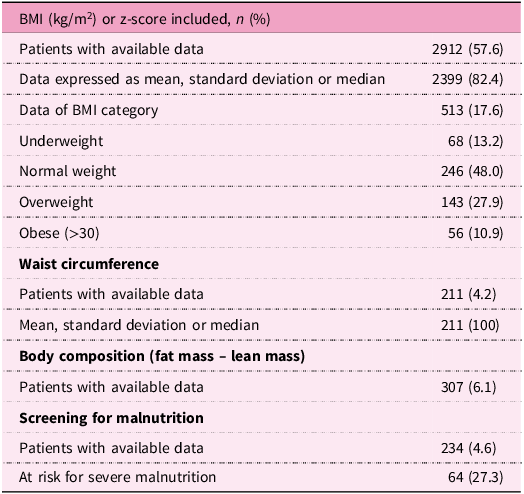
Anthropometric data and nutritional status
The anthropometric data collected are shown in Table 4. Most of the selected studies (22/30) assessed weight, height, and BMI: information was available for 2912 patients (57.6%), and among them 82.4% were described by mean and standard deviation or median and with z-score assessment. Regarding nutritional status, 513 patients (10.1%) were classified according to WHO criteria(46) as: underweight (13.2%), normal weight (48.0%), overweight (27.9%), and obese (10.9%). Waist circumference data were collected in the cross-sectional study by Amzali and collaborators(Reference Amzali, Wilson, Bommart, Picot, Galas and Mercier5) and in the clinical trial by Billich et al.(Reference Billich, Bray, Truby, Evans, Carroll and de Valle24); data were available for 211 patients (4.2%), expressed as mean and standard deviation or median. In Nishizawa’s observational study(Reference Nishizawa and Nakamura37), the circumference of the lower limb was assessed as an instrument to quantify muscle mass. In eight studies, data about body composition were available: five studies used bio-impedance(Reference Amzali, Wilson, Bommart, Picot, Galas and Mercier5,Reference López-Gómez, Ballesteros-Pomar, Torres-Torres, De la Maza, Penacho-Lázaro and Palacio-Mures34,Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39,Reference van Hees, Knuijt, Dicke, Groothuis, Raaphorst, Satink and Cup42,Reference Wilson, Bommart, Passerieux, Picot, Mercier and Laoudj-Chenivesse44) and three used dual-energy X-ray absorptiometry (DEXA) instruments(Reference Billich, Evans, Truby, Ryan, Kornberg and Davidson6,Reference Zhang, Qi, Wang, Yang, Shen and Yang11,Reference Davidson, Hughes, Ryan, Kornberg, Cairns and Jones26) . Analyses of body composition, discriminating between fat mass and lean mass, involved a total of 307 patients (6.1%). Finally, malnutrition risk screening was conducted in four studies(Reference Naume, Jørgensen, Høi-Hansen, Born, Vissing and Borgwardt10,Reference Zhang, Qi, Wang, Yang, Shen and Yang11,Reference López-Gómez, Ballesteros-Pomar, Torres-Torres, De la Maza, Penacho-Lázaro and Palacio-Mures34) for a total of 234 patients (4.6%), of whom 27.3% (n = 64) were found to be at risk of severe malnutrition. The most detailed results on malnutrition risk were obtained by Forgues and colleagues(Reference Naume, Jørgensen, Høi-Hansen, Born, Vissing and Borgwardt10), using the Seniors in the Community Risk Evaluation for Eating and Nutrition (SCREEN II) score, and by Lopez-Gomez(Reference López-Gómez, Ballesteros-Pomar, Torres-Torres, De la Maza, Penacho-Lázaro and Palacio-Mures34), using the Subjective Global Assessment (SGA) screening tool according to GLIM criteria.
In detail, Forgues et al.(Reference Naume, Jørgensen, Høi-Hansen, Born, Vissing and Borgwardt10) found that 82% of patients with oculopharyngeal muscular dystrophy were at risk for malnutrition, often associated with dysphagia. Lopez-Gomez(Reference López-Gómez, Ballesteros-Pomar, Torres-Torres, De la Maza, Penacho-Lázaro and Palacio-Mures34), in his research on ALS patients, noted that nearly half of patients (48%) were screened for malnutrition and that those with worsened nutritional status had a lower life expectancy than those in optimal nutritional condition.
In such heterogeneous and progressive diseases, nutritional status changes greatly, and in observational studies performed by Naume and by Chou(Reference Chou, Lindeback, D’Silva, Sampaio, Neville and Farrar7,Reference Zhang, Qi, Wang, Yang, Shen and Yang11) , more than 50% of patients had inadequate body weight, ranging from overweight and obesity in Duchenne muscular dystrophy in paediatric patients, to underweight in other conditions such as motor neuron disease, muscular spinal atrophy, and myotonic dystrophy type 1.
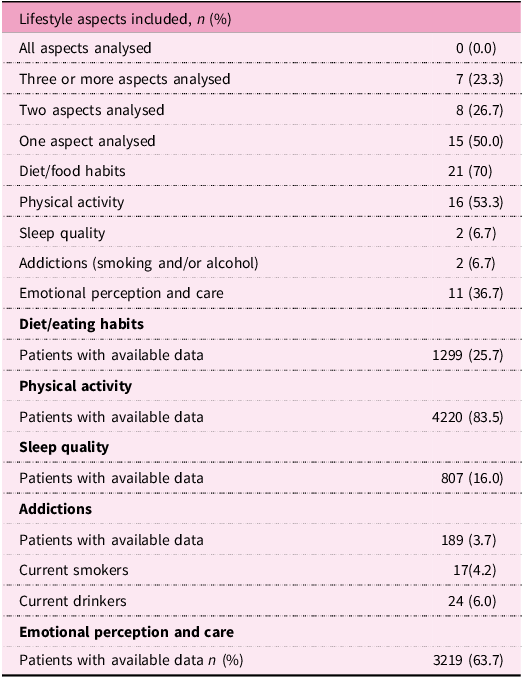
Table 5 details data about diet and nutrition and all the other available lifestyle factors, if addressed (physical activity, smoking and/or alcohol dependence, sleep quality, psychological and emotional conditions, and patients’ perceptions). Seven studies (23.3%) examined three or more aspects of lifestyle, eight studies (26.7%) focused on two aspects, and 15 articles (50.0%) examined a single aspect of lifestyle. None provided a comprehensive analysis of all relevant lifestyle factors in these conditions.
The summary of key information extracted from selected articles, such as the type of study, country, sample size, and all aspects of lifestyle investigated, is reported in Table 6. The evaluation of the methodological quality of the selected studies is reported in Supplementary Table S1.
A descriptive analysis of diet and nutrition and of any other addressed lifestyle factors (including physical activity, sleep quality, smoking and alcohol consumption habits, and emotional perception and care) was performed.
Diet and nutrition
Diet and/or nutrition were investigated in 21 studies (12 observational and 9 clinical trials), with data from 1299 patients (25.7% of the selected total sample). In five intervention studies(Reference Dorst, Doenz, Kandler, Dreyhaupt, Tumani and Witzel29,Reference Gazzellone, Lanteigne, Gammage, Fajardo and Ditor31,Reference Ludolph, Dorst, Dreyhaupt, Weishaupt, Kassubek and Weiland35,Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39,Reference Staretz-Chacham, Pode-Shakked, Kristal, Abraham, Porper and Wormser40) the authors investigated the effect of special dietary patterns on patients’ symptoms and/or life expectancy. Specifically, in the work of Dorst et al. and Ludolph et al.(Reference Dorst, Doenz, Kandler, Dreyhaupt, Tumani and Witzel29,Reference Ludolph, Dorst, Dreyhaupt, Weishaupt, Kassubek and Weiland35) , the effect of a high-calorie diet was evaluated in comparison to a control group without supplementation, while in the study of Gazzellone et al.(Reference Gazzellone, Lanteigne, Gammage, Fajardo and Ditor31) the ‘Mad Dog Diet’, an anti-inflammatory diet programme, was tested. In the study of Sechi et al.(Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39), the effect of a high-protein diet combined with exercise was compared to the exercise programme alone, without any nutritional intervention. The work conducted by the Staretz-Chacham(Reference Staretz-Chacham, Pode-Shakked, Kristal, Abraham, Porper and Wormser40) research group evaluated the effect of a restrictive ketogenic diet on a small group of patients. Specific supplementations evaluated in patients with DMD or FSHD were effective in improving motor performance, and in the second group of patients, at a statistically significant threshold(Reference Davidson, Hughes, Ryan, Kornberg, Cairns and Jones26,Reference Wilson, Bommart, Passerieux, Picot, Mercier and Laoudj-Chenivesse44) . The family-centred intensive lifestyle and weight management programme specifically studied for DMD patients by Billich and collaborators(Reference Billich, Bray, Truby, Evans, Carroll and de Valle24) has been very successful both in terms of patients’ satisfaction and QoL.
None of the selected studies considered adherence to the Mediterranean diet or proposed an intervention based on a Mediterranean dietary pattern. Only the Mad Dog Diet proposed by Gazzellone’s group(Reference Gazzellone, Lanteigne, Gammage, Fajardo and Ditor31) shares common elements with the Mediterranean diet, such as the use of plant-based foods rich in antioxidants, fibre, and omega-3, and a reduced intake of refined and ultra-processed foods. However, this is not an intervention based on the Mediterranean diet.
Dietary intakes, expressed as energy and macro- and micronutrient composition, collected through food diaries, food frequencies questionnaires, or interviews, were evaluated in 13 observational studies(Reference Amzali, Wilson, Bommart, Picot, Galas and Mercier5,Reference Billich, Evans, Truby, Ryan, Kornberg and Davidson6,Reference Naume, Jørgensen, Høi-Hansen, Born, Vissing and Borgwardt10,Reference Zhang, Qi, Wang, Yang, Shen and Yang11,Reference Andersen, Aadahl and Vissing23,Reference Billich, Bray, Truby, Evans, Carroll and de Valle24,Reference Dietvorst, Bot, Van Der Holst and Niks27,Reference Kim, Jin, Kim and Park33,Reference López-Gómez, Ballesteros-Pomar, Torres-Torres, De la Maza, Penacho-Lázaro and Palacio-Mures34,Reference Uçar, Altınok, Mansuroglu, Canda, Yazıcı and Çelik41,Reference van Hees, Knuijt, Dicke, Groothuis, Raaphorst, Satink and Cup42,Reference Yamamoto, Mori-Yoshimura, Oya, Komaki and Takahashi45) . Dietvost(Reference Dietvorst, Bot, Van Der Holst and Niks27) found that intake of fibre, nuts, and dairy products, as well as liquids, was significantly lower than in a healthy population and below the recommended thresholds; these data were confirmed, especially with regard to protein and fibre, by van Hees and collaborators(Reference van Hees, Knuijt, Dicke, Groothuis, Raaphorst, Satink and Cup42). Billich and Yamamoto(Reference Billich, Bray, Truby, Evans, Carroll and de Valle24,Reference Yamamoto, Mori-Yoshimura, Oya, Komaki and Takahashi45) evaluated patients’ refusal or avoidance behaviour with respect to certain foods or textures, and Chou(Reference Chou, Lindeback, D’Silva, Sampaio, Neville and Farrar7) investigated how many of the recruited subjects had received dietary advice from a nutrition specialist. Finally, Billich(Reference Billich, Bray, Truby, Evans, Ryan and Carroll25) reported that, according to caregivers, patients experienced an increased appetite and often ate discretionary foods.
In clinical trials based on targeted dietary interventions, in which caloric and macro- and micronutrient intakes were optimised, an improvement of motor skills, expressed as increased fatigue tolerance, was observed in different pathologic conditions. In the presence of overweight and/or obesity, an improvement in BMI was observed, as well as a reduction of waist circumference(Reference Billich, Bray, Truby, Evans, Carroll and de Valle24,Reference Davidson, Hughes, Ryan, Kornberg, Cairns and Jones26,Reference Dorst, Doenz, Kandler, Dreyhaupt, Tumani and Witzel29,Reference Gazzellone, Lanteigne, Gammage, Fajardo and Ditor31,Reference Ludolph, Dorst, Dreyhaupt, Weishaupt, Kassubek and Weiland35,Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39,Reference Wilson, Bommart, Passerieux, Picot, Mercier and Laoudj-Chenivesse44) . Specific dietary intervention, such as a high-protein diet or a ketogenic diet, was found to be effective in improving some metabolic parameters and motor functions(Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39–Reference Uçar, Altınok, Mansuroglu, Canda, Yazıcı and Çelik41). However, none of the clinical trials examined observed a significantly positive correlation between dietary intervention and survival. The study by Gazzellone and co-workers, a randomised controlled trial performed with 11 patients with different pathologic conditions, found a significant correlation between an anti-inflammatory diet, based on the consumption of fresh and minimally processed food, and improvement in depression(Reference Gazzellone, Lanteigne, Gammage, Fajardo and Ditor31).
Overall, observational studies revealed that macro- and micronutrient intakes were frequently far from international recommended levels(Reference Elkady, Ahmed and Abd El- Naby30,47) , especially for protein(Reference Amzali, Wilson, Bommart, Picot, Galas and Mercier5,Reference Billich, Evans, Truby, Ryan, Kornberg and Davidson6,Reference Naume, Jørgensen, Høi-Hansen, Born, Vissing and Borgwardt10,Reference Zhang, Qi, Wang, Yang, Shen and Yang11,Reference Elkady, Ahmed and Abd El- Naby30,Reference Kim, Jin, Kim and Park33,Reference López-Gómez, Ballesteros-Pomar, Torres-Torres, De la Maza, Penacho-Lázaro and Palacio-Mures34) and lipid intakes(Reference Amzali, Wilson, Bommart, Picot, Galas and Mercier5,Reference Kim, Jin, Kim and Park33,Reference López-Gómez, Ballesteros-Pomar, Torres-Torres, De la Maza, Penacho-Lázaro and Palacio-Mures34) . Vitamin C, zinc, calcium, and vitamin E were frequently insufficient too(Reference Amzali, Wilson, Bommart, Picot, Galas and Mercier5,Reference Billich, Evans, Truby, Ryan, Kornberg and Davidson6,Reference Davidson, Hughes, Ryan, Kornberg, Cairns and Jones26) . Reduced consumption of fresh fruit and vegetables emerged in several studies(Reference Amzali, Wilson, Bommart, Picot, Galas and Mercier5,Reference Billich, Evans, Truby, Ryan, Kornberg and Davidson6,Reference Naume, Jørgensen, Høi-Hansen, Born, Vissing and Borgwardt10,Reference Elkady, Ahmed and Abd El- Naby30) and, as a consequence, levels of dietary fibre were often found to be far below optimal intake levels(Reference Chou, Lindeback, D’Silva, Sampaio, Neville and Farrar7,Reference Naume, Jørgensen, Høi-Hansen, Born, Vissing and Borgwardt10,Reference Dietvorst, Bot, Van Der Holst and Niks27,Reference Elkady, Ahmed and Abd El- Naby30) . Moreover, the analysis of diet quality revealed that many patients consumed foods high in calories, but low in nutrients, and that at least 30% of calories were derived from discretionary foods and drinks(Reference Billich, Evans, Truby, Ryan, Kornberg and Davidson6).
In ten studies, the use of supplements was reported: four were clinical trials as part of the intervention(Reference Billich, Bray, Truby, Evans, Carroll and de Valle24,Reference Davidson, Hughes, Ryan, Kornberg, Cairns and Jones26,Reference Staretz-Chacham, Pode-Shakked, Kristal, Abraham, Porper and Wormser40,Reference Wilson, Bommart, Passerieux, Picot, Mercier and Laoudj-Chenivesse44) , while in the other contexts both commercial multivitamins and targeted supplements, such as vitamin D, calcium, and omega-3, were independently consumed(Reference Billich, Evans, Truby, Ryan, Kornberg and Davidson6,Reference Naume, Jørgensen, Høi-Hansen, Born, Vissing and Borgwardt10,Reference Zhang, Qi, Wang, Yang, Shen and Yang11,Reference Kim, Jin, Kim and Park33,Reference Uçar, Altınok, Mansuroglu, Canda, Yazıcı and Çelik41) .
In the intervention study conducted by Wilson and colleagues, a supplementation of vitamin C, vitamin E, zinc, and selenium significantly improved muscle volume and function in patients with FSHD(Reference Wilson, Bommart, Passerieux, Picot, Mercier and Laoudj-Chenivesse44).
Finally, nutrition education interventions, in which both patients and caregivers or targeting groups were involved, were found to be effective in improving eating habits and the management of daily meals(Reference Billich, Bray, Truby, Evans, Ryan and Carroll25,Reference van Hees, Knuijt, Dicke, Groothuis, Raaphorst, Satink and Cup42) .
Other lifestyle factors
In addition to diet and nutrition, all other lifestyle factors that emerged in this literature review were analysed.
Physical activity (PA) was analysed in 16 studies (53.3%), including 3 clinical trials and 13 observational studies, and involving a total of 4220 patients out of 5055 (83.5%) (Table 5).
The studies by Amzali et al.(Reference Amzali, Wilson, Bommart, Picot, Galas and Mercier5), Andersen et al.(Reference Andersen, Aadahl and Vissing23), Billich et al.(Reference Billich, Evans, Truby, Ryan, Kornberg and Davidson6), Davidson et al.(Reference Davidson, Hughes, Ryan, Kornberg, Cairns and Jones26) Dong et al.(Reference Dong, Chong, Wu, Kaminski, Cutter and Xu28), Elkady et al.(Reference Elkady, Ahmed and Abd El- Naby30), Jackson et al.(Reference Jackson, Parthan, Lauher-Charest, Broderick, Law and Barnett32), Karazi et al.(Reference Karazi, Coppers, Maas, Cup, Bloemen and Voet21), Kim et al.(Reference Kim, Jin, Kim and Park33), Nishizawa et al.(Reference Nishizawa and Nakamura37), Said et al.(Reference Said and Alhumaid38), and Ucar et al.(Reference Uçar, Altınok, Mansuroglu, Canda, Yazıcı and Çelik41) collected data on participants’ actual physical activity and/or motor function, using assessment tools and scales not always comparable.
Assessment of PA has been conducted through questionnaires, interviews, and/or rating scales in 13 studies; more specific instruments, such as accelerometers(Reference Andersen, Aadahl and Vissing23), tests conducted with health professionals(Reference Billich, Evans, Truby, Ryan, Kornberg and Davidson6,Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39) , and the ‘6-Minute Walk Distance (6MWD)’(Reference Billich, Bray, Truby, Evans, Carroll and de Valle24,Reference Davidson, Hughes, Ryan, Kornberg, Cairns and Jones26,Reference Uçar, Altınok, Mansuroglu, Canda, Yazıcı and Çelik41) were used in six papers.
Three intervention studies(Reference Billich, Bray, Truby, Evans, Carroll and de Valle24,Reference Davidson, Hughes, Ryan, Kornberg, Cairns and Jones26,Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39) examined motor function and physical activity in patients with neuromuscular diseases. The pilot study by Billich et al. showed a trend toward improved motor function and fatigue tolerance, although not statistically significant, after a lifestyle and weight management programme(Reference Billich, Bray, Truby, Evans, Carroll and de Valle24).
In the work of Davidson et al., a significant increase in 6MWD test performance and an improvement of daily activity parameters were observed after the use of an enhanced supplement. Body composition and quality of life of these DMD patients did not change(Reference Davidson, Hughes, Ryan, Kornberg, Cairns and Jones26). Sechi’s group observed that an exercise programme combined with a high-protein diet improved aerobic function, lung capacity, and QoL in late-onset Pompe disease patients. In this intervention study, a personalised exercise training programme, combined with a high-protein diet, could significantly improve maximal muscular performance, exercise tolerance, vitality, and general health in comparison to the control group(Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39).
Data from observational studies showed that, even taking into account different disease conditions, the physical activity level of most patients with neuromuscular diseases was overall lower than the minimum level of WHO recommendations(48). In addition, this tendency toward a reduced physical activity was more pronounced among females than males(Reference Andersen, Aadahl, Vissing and Knak22,Reference Andersen, Aadahl and Vissing23,Reference Dong, Chong, Wu, Kaminski, Cutter and Xu28,Reference Said and Alhumaid38) . The extensive observational study performed by Dong and co-workers found that women with MG had a significantly worse physical quality of life and a lower level of active lifestyle in comparison to men with the same clinical condition (p < 0.001 and p < 0.01, respectively)(Reference Dong, Chong, Wu, Kaminski, Cutter and Xu28). Andersen et al. observed that 53% of patients with MG had a low level of PA, especially among females. Authors found a significant correlation between poor PA and higher BMI, older age, presence of comorbidities, reduced QoL, sleep disorders, and increased levels of fatigue(Reference Andersen, Aadahl, Vissing and Knak22). In a subsequent study by Andersen and collaborators, conducted by accelerometer and IPAQ test, it was observed that 48% of patients with MG did not meet the moderate intensity recommendations(Reference Andersen, Aadahl and Vissing23). Jackson et al. observed that participation in sports was challenging for patients with MG, and symptoms often induced withdrawal of PA(Reference Jackson, Parthan, Lauher-Charest, Broderick, Law and Barnett32). In the work of Amzali, 84% of patients with FHSD reported low level of PA, and in women it was significantly lower than in men. Simultaneously, PA was positively related to younger age, daily energy intake, and zinc blood level(Reference Amzali, Wilson, Bommart, Picot, Galas and Mercier5). The study of Billich et al.(Reference Billich, Evans, Truby, Ryan, Kornberg and Davidson6) reported a weak positive correlation between motor performance and energy intake (p < 0.01) and Nishizawa and collaborators observed that a more sedentary lifestyle and lack of PA significantly decreased motor performance of patients with DMD(Reference Karazi, Coppers, Maas, Cup, Bloemen and Voet21,Reference Nishizawa and Nakamura37) . In the observational transversal study of Karazi, 47% of the patients with myopathy did not perform vigorous PA, 29% of the patients did not perform moderate PA, and 13% did not walk for at least ten minutes a day(Reference Karazi, Coppers, Maas, Cup, Bloemen and Voet21,Reference Kim, Jin, Kim and Park33) , while in the study of Kim on ALS patients, 61% of subjects were reported to do exercise more than once a week(Reference Kim, Jin, Kim and Park33).
In the prospective study by Ucar et al.(Reference Uçar, Altınok, Mansuroglu, Canda, Yazıcı and Çelik41), it was observed that a diet high in protein and fat led to increased exercise tolerance and motor function in paediatric patients with glycogen storage disease. Moreover, the daily activity questionnaire scores significantly improved in comparison to the initial self-evaluation(Reference Uçar, Altınok, Mansuroglu, Canda, Yazıcı and Çelik41). Finally, Said and collaborators observed that more than 60% of patients, especially men, with different disabilities involved in the observational study, met the minimum standard of PA specified by WHO. Authors also observed that PA was significantly related to education level, type of disability (poliomyelitis exhibited the highest level of PA), and self-rated health(Reference Said and Alhumaid38).
With regard to other lifestyle factors that emerged from this review, sleep quality was assessed in two observational studies, both conducted on patients suffering from MG(Reference Andersen, Aadahl, Vissing and Knak22,Reference Jackson, Parthan, Lauher-Charest, Broderick, Law and Barnett32) . Self-reported sleep quality and sleep disturbance during the previous two weeks were measured by Andersen and colleges using the Insomnia Severity Index, with 55% of patients reporting insomnia. In addition, significantly more sleep problems were reported in the group of patients with lower physical activity. Insomnia also correlated with general fatigue, reduced activity and motivation, and mental fatigue(Reference Andersen, Aadahl, Vissing and Knak22).
Jackson and co-workers conducted structured interviews, and the common symptoms identified by patients revealed that the main sleep problems were caused by respiratory problems or preoccupation with illness(Reference Jackson, Parthan, Lauher-Charest, Broderick, Law and Barnett32).
Alcohol consumption and tobacco use were investigated in two articles(Reference Kim, Jin, Kim and Park33,Reference McMillan, Bowen, Bayan, Kasperbauer and Ekbom36) : in the papers by Kim et al. and by McMillan et al., alcohol consumption and smoking status were obtained by interviews and reported in the results as ‘current’, ‘former’, or ‘never’ drinking or smoking. Notably, in both studies, authors did not look for any correlation between tobacco use or alcohol consumption and pathological condition, QoL, or survival(Reference Kim, Jin, Kim and Park33,Reference McMillan, Bowen, Bayan, Kasperbauer and Ekbom36) .
No data on abuse of substances were identified in the articles selected in this systematic review.
The emotional and psychological status of patients was investigated in 11 studies (36.7%), 4 clinical trials(Reference Billich, Bray, Truby, Evans, Carroll and de Valle24,Reference Gazzellone, Lanteigne, Gammage, Fajardo and Ditor31,Reference Ludolph, Dorst, Dreyhaupt, Weishaupt, Kassubek and Weiland35,Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39) and 7 observational studies(Reference Andersen, Aadahl, Vissing and Knak22,Reference Billich, Bray, Truby, Evans, Ryan and Carroll25,Reference Dong, Chong, Wu, Kaminski, Cutter and Xu28,Reference Elkady, Ahmed and Abd El- Naby30,Reference Jackson, Parthan, Lauher-Charest, Broderick, Law and Barnett32,Reference Said and Alhumaid38,Reference Walker, Mistry, Amin, McAdam, Kalnins and Lui43) , with data available for 3219 of 5055 patients (63.7%). The most frequently investigated emotional aspects involved conditions of anxiety and depression, which were examined in the work of Andersen et al., Billich et al., Dong et al., Gazzellone et al., Jackson et al., and Ludolph et al.(Reference Andersen, Aadahl, Vissing and Knak22,Reference Billich, Bray, Truby, Evans, Carroll and de Valle24,Reference Dong, Chong, Wu, Kaminski, Cutter and Xu28,Reference Gazzellone, Lanteigne, Gammage, Fajardo and Ditor31,Reference Jackson, Parthan, Lauher-Charest, Broderick, Law and Barnett32,Reference Ludolph, Dorst, Dreyhaupt, Weishaupt, Kassubek and Weiland35) . Other studies explored the relationship between emotions and eating behaviours or focused attention on stress management, emotional well-being, and vitality of patients(Reference Billich, Bray, Truby, Evans, Ryan and Carroll25,Reference Elkady, Ahmed and Abd El- Naby30,Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39) . Among clinical trials, of note was the work of Gazzellone and collaborators, where an anti-inflammatory diet succeeded in significantly improving depression status measured by the Centre for Epidemiological Studies Depression Scale (CES-D)(Reference Gazzellone, Lanteigne, Gammage, Fajardo and Ditor31). Sechi et al. also observed a trend in improvement in emotional state following a combined diet and physical activity intervention, although none of these studies reached statistical significance, probably due to a small sample size(Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39). In the study of Ludolph, 3% of the sample reported depression, and the dietary intervention did not significantly change their perceived QoL(Reference Ludolph, Dorst, Dreyhaupt, Weishaupt, Kassubek and Weiland35). Finally, in Billich’s well-being intervention trial, the impact on anxiety, reported at baseline in three out of eight DMD patients, was not evaluated(Reference Billich, Bray, Truby, Evans, Carroll and de Valle24).
Data on emotional condition and perception, collected in the different observational studies mainly at baseline, vary greatly, even in similar pathological conditions. In the article of Andersen, 8% of patients with MG reported depression or anxiety, and this condition significantly correlated with fatigue (general, physical, and mental) and reduced activity and motivation(Reference Andersen, Aadahl, Vissing and Knak22). In the large observational study performed by Dong and co-workers on Chinese patients with MG, depression was reported by 10.1% of men and 10.6% of women, and anxiety by 12.7% of men and 12.5% of women. Authors observed that MG also affected the emotional status in the female population more than in males(Reference Dong, Chong, Wu, Kaminski, Cutter and Xu28).
In the study by Jackson et al.(Reference Jackson, Parthan, Lauher-Charest, Broderick, Law and Barnett32), conducted in patients with MS, anxiety and depression affected 82% and 75% of the population, respectively. Moreover, frustration (64% of patients), stress (32%), and discomfort (18%) were reported, and patients referred to difficulties in interpersonal relationships, a sense of misunderstanding by friends and family, anxiety related to social occasions, and a tendency to avoid relational events. Reduced sociality and difficulties in managing relationships both within and outside the family emerge as factors that severely affect the QoL perceived(Reference Jackson, Parthan, Lauher-Charest, Broderick, Law and Barnett32). Elkady recorded, with the health promotion behaviour scale test, an intermediate level of stress management and self-actualisation among MG patients(Reference Elkady, Ahmed and Abd El- Naby30,Reference Said and Alhumaid38) .
In the study by Said and collaborators, where patients with different NMDs were enrolled, health perception was significantly better in those who were physically active (p < 0.001)(Reference Said and Alhumaid38).
In projects involving both patients and caregivers in small groups, it was also possible to investigate correlations between pathology, emotions, and eating habits: sadness, depression, anger, boredom, and pleasure were associated with food consumption in 14% of patients with DMD(Reference Billich, Bray, Truby, Evans, Ryan and Carroll25). In the qualitative study of Walker, through semi-structured interviews on weight management, the psychosocial well-being of boys with DMD and families was discussed, and the importance of an integrated and multidisciplinary approach was highlighted. A higher level of engagement among mothers also emerged(Reference Walker, Mistry, Amin, McAdam, Kalnins and Lui43).
Primary and secondary endpoints
Among the 30 studies evaluated in this narrative review, 11 enrolled paediatric patients (< 18 years; 36.7%)(Reference Billich, Evans, Truby, Ryan, Kornberg and Davidson6,Reference Chou, Lindeback, D’Silva, Sampaio, Neville and Farrar7,Reference Naume, Jørgensen, Høi-Hansen, Born, Vissing and Borgwardt10,Reference Billich, Bray, Truby, Evans, Carroll and de Valle24–Reference Dietvorst, Bot, Van Der Holst and Niks27,Reference Nishizawa and Nakamura37,Reference Staretz-Chacham, Pode-Shakked, Kristal, Abraham, Porper and Wormser40,Reference Uçar, Altınok, Mansuroglu, Canda, Yazıcı and Çelik41,Reference Walker, Mistry, Amin, McAdam, Kalnins and Lui43) , 9 enrolled young to middle-aged adults (age 18–50 years; 30%)(Reference Amzali, Wilson, Bommart, Picot, Galas and Mercier5,Reference Dong, Chong, Wu, Kaminski, Cutter and Xu28,Reference Elkady, Ahmed and Abd El- Naby30,Reference Jackson, Parthan, Lauher-Charest, Broderick, Law and Barnett32,Reference Said and Alhumaid38,Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39,Reference van Hees, Knuijt, Dicke, Groothuis, Raaphorst, Satink and Cup42,Reference Wilson, Bommart, Passerieux, Picot, Mercier and Laoudj-Chenivesse44,Reference Yamamoto, Mori-Yoshimura, Oya, Komaki and Takahashi45) , and 10 enrolled adults (mean age >50 years; 33.3%)(Reference Forgues, Fortin, Gagnon, Brisson, Mathieu and Brais9,Reference Karazi, Coppers, Maas, Cup, Bloemen and Voet21–Reference Andersen, Aadahl and Vissing23,Reference Dorst, Doenz, Kandler, Dreyhaupt, Tumani and Witzel29,Reference Gazzellone, Lanteigne, Gammage, Fajardo and Ditor31,Reference Kim, Jin, Kim and Park33–Reference McMillan, Bowen, Bayan, Kasperbauer and Ekbom36) . This age distribution reflects the natural course of these heterogeneous conditions: genetic dystrophies (DMD, SMA) typically manifest during childhood; myopathies and limb-girdle muscular dystrophies tend to manifest in early adulthood; MG, ALS, and inclusion body myositis are predominantly diseases that affect middle-aged and elderly adults.
In this narrative review, we also search for possible correlations of lifestyle on disease course (19 studies) and on QoL (nine studies, four as primary and five as secondary endpoint).
As for changes in pathology-related parameters, the studies vary greatly according to different diseases: in patients with ALS, a higher body weight was positively correlated with a prolonged survival rate, and an increased intake of protein, fats, and meat was positively associated both with long-term survival and symptoms delay(Reference Kim, Jin, Kim and Park33). A fat-rich diet, even if effective in improving weight gain, caused gastrointestinal side effects in several ALS patients(Reference Dorst, Doenz, Kandler, Dreyhaupt, Tumani and Witzel29). In the intervention study of Ludolph and collaborators, a high-caloric nutrition programme did not increase the survival time, nor the vital capacity and functionality of ALS patients(Reference Ludolph, Dorst, Dreyhaupt, Weishaupt, Kassubek and Weiland35).
In MG patients, higher physical activity seems to improve symptoms and fatigue resistance and, globally, these patients registered a better health condition and quality of life(Reference Andersen, Aadahl, Vissing and Knak22,Reference Andersen, Aadahl and Vissing23) . One third of the MS patients involved in the observational study of Elkady achieved a low level of healthy promotion behaviours, including reduced physical activity(Reference Karazi, Coppers, Maas, Cup, Bloemen and Voet21,Reference Elkady, Ahmed and Abd El- Naby30) . Lower physical activity was related to worst parameters and, overall, to a poorer quality of life, also in patients with McArdle disease(Reference Karazi, Coppers, Maas, Cup, Bloemen and Voet21). Physical activity is one of the aspects of the lifestyle that also affects the disease parameters in patients with DMD. Nishizawa and colleagues observed a significant reduction of motor function in patients with DMD in relation to the movements and travel restriction imposed during Covid-19 pandemic(Reference Nishizawa and Nakamura37).
Improved functional outcomes and ambulation in patients with DMD were achieved by antioxidant supplementation and higher protein intake(Reference Amzali, Wilson, Bommart, Picot, Galas and Mercier5,Reference Davidson, Hughes, Ryan, Kornberg, Cairns and Jones26) . Personalised dietary interventions, associated with lifestyle for weight management, have been reported by both DMD patients and caregivers to improve physical function and satisfaction(Reference Billich, Evans, Truby, Ryan, Kornberg and Davidson6,Reference Billich, Bray, Truby, Evans, Carroll and de Valle24,Reference Billich, Bray, Truby, Evans, Ryan and Carroll25) . Multidisciplinary interventions, involving both patients and caregivers, created a healthier environment and improved clinical outcomes(Reference Said and Alhumaid38,Reference van Hees, Knuijt, Dicke, Groothuis, Raaphorst, Satink and Cup42,Reference Walker, Mistry, Amin, McAdam, Kalnins and Lui43) . In studies of different types of patients with neuromuscular diseases, it has been observed that a personalised dietary intervention and a multidisciplinary approach over time can improve health condition, including improving depression or mobility(Reference Gazzellone, Lanteigne, Gammage, Fajardo and Ditor31,Reference Uçar, Altınok, Mansuroglu, Canda, Yazıcı and Çelik41) .
Quality of life was measured through validated and standardised questionnaires, which allowed the assessment of various aspects, including physical, psychological, and emotional well-being: PedsQL, tailored for the paediatric population, was used by Billich(Reference Billich, Bray, Truby, Evans, Carroll and de Valle24) and Davidson(Reference Davidson, Hughes, Ryan, Kornberg, Cairns and Jones26); for the adult population affected by MG, the specific MGQoL-15 was used by Andersen and by Dong(Reference Andersen, Aadahl, Vissing and Knak22,Reference Dong, Chong, Wu, Kaminski, Cutter and Xu28) ; and the SF-36 questionnaire, able to assess eight different areas of daily life, was used by Sechi and Wilson(Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39,Reference Wilson, Bommart, Passerieux, Picot, Mercier and Laoudj-Chenivesse44) . Due to the different and not comparable assessment methodologies, a comprehensive statistical analysis was not permitted. Improved QoL was observed in some intervention studies: Sechi et al. highlighted that individualised exercise programmes, in combination with tailored nutrition, have led to significant improvements not only in physical function but also in quality of life, particularly with regard to general health (p = 0.031) and vitality (p = 0.031)(Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39,Reference Wilson, Bommart, Passerieux, Picot, Mercier and Laoudj-Chenivesse44) . Wilson and colleagues observed that antioxidant supplementation, with vitamin C, vitamin E, zinc, and selenium for 17 weeks, significantly improved the QoL of FSHD patients in terms of physical functioning, general health, vitality, emotional role functioning, and mental score. In the clinical trial of Staretz-Chacham, although not significant, a general trend of an increased QoL was observed in the ketogenic diet group(Reference Staretz-Chacham, Pode-Shakked, Kristal, Abraham, Porper and Wormser40), while in the work of Davidson and Ludolph, performed on patients affected by DMD and ALS respectively, no meaningful improvements in QoL score were detected(Reference Davidson, Hughes, Ryan, Kornberg, Cairns and Jones26,Reference Ludolph, Dorst, Dreyhaupt, Weishaupt, Kassubek and Weiland35) . Observational studies have provided different results regarding QoL: Dong et al. identified that risk factors that could worsen QoL included female sex (p < 0.05), a high number of comorbidities (p < 0.05), and unemployment (p < 0.001), while an active lifestyle had a positive impact on HRQoL (p < 0.001)(Reference Dong, Chong, Wu, Kaminski, Cutter and Xu28). In the study of Andersen (2021) the MGQoL-15 score was significantly higher in patients regularly involved in PA (p < 0.01)(Reference Andersen, Aadahl, Vissing and Knak22), a trend also observed in patients with low motor capacity(Reference Billich, Bray, Truby, Evans, Carroll and de Valle24,Reference Kim, Jin, Kim and Park33) . The importance of physical activity as a component of lifestyle has also emerged in the work of Elkady et al. and Ucar et al.(Reference Uçar, Altınok, Mansuroglu, Canda, Yazıcı and Çelik41), who explored the effect of a high-protein diet and physical activity on increased motor capacity and QoL, with promising although not statistically significant results(Reference Elkady, Ahmed and Abd El- Naby30,Reference Uçar, Altınok, Mansuroglu, Canda, Yazıcı and Çelik41) . QoL is closely related also to the emotional state of patients: negative emotions, such as anxiety, depression, sadness, and frustration, have a direct impact on the quality of social relationships, negatively affecting patients’ overall well-being(Reference Billich, Bray, Truby, Evans, Ryan and Carroll25,Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39) . Impacts on social functioning, reported by the 96% of patients with MG enrolled in the study of Jackson, which included difficulties in dating, feeling misunderstood by friends and family, feeling uncomfortable/anxious in social situations, and skipping or avoiding social events, have been identified as significantly affecting the perceived QoL(Reference Jackson, Parthan, Lauher-Charest, Broderick, Law and Barnett32).
Disease-stratified endpoints
In the present narrative review, the findings on diet, physical activity, and QoL could also be presented separately for the three most represented disease groups (MG, ALS, DMD), which together account for 83.1% of the total study population (n = 4,199 of 5,055). In patients affected by MG, physical activity and lifestyle management emerged as the most clinically actionable parameters, with PA consistently associated with lower fatigue (MFI-20) and better QoL (MG-QoL15) across multiple observational studies(Reference Chou, Lindeback, D’Silva, Sampaio, Neville and Farrar7,Reference Andersen, Aadahl, Vissing and Knak22,Reference Andersen, Aadahl and Vissing23,Reference Dong, Chong, Wu, Kaminski, Cutter and Xu28) . In patients affected by ALS, nutritional status and caloric support were central, but randomised clinical trial evidence has not demonstrated survival benefit even with high-caloric fat-rich supplementation(Reference Dorst, Doenz, Kandler, Dreyhaupt, Tumani and Witzel29,Reference Kim, Jin, Kim and Park33,Reference Ludolph, Dorst, Dreyhaupt, Weishaupt, Kassubek and Weiland35) . In DMD, the nutritional picture is dominated by corticosteroid-driven weight gain, low fibre intake, and vitamin D deficiency, with interventional data suggesting a trend toward functional benefit from multicomponent supplementation(Reference Billich, Evans, Truby, Ryan, Kornberg and Davidson6,Reference Naume, Jørgensen, Høi-Hansen, Born, Vissing and Borgwardt10,Reference Davidson, Hughes, Ryan, Kornberg, Cairns and Jones26,Reference Dietvorst, Bot, Van Der Holst and Niks27) .
Discussion
Patients with neuromuscular disorders frequently experience nutritional imbalances, from undernutrition and muscle atrophy to overweight and obesity, often exacerbated by disease progression(Reference Dipasquale, Morello and Romano8,Reference Deenen, Horlings, Verschuuren, Verbeek and van Engelen49,Reference Wernio, Wasilewska, Czaja-Stolc, Śledzińska, Wierzba and Szlagatys-Sidorkiewicz50) .
While pharmacological treatments are essential for symptom management, and in some settings are changing the course of pathology (i.e., spinal muscular atrophy)(Reference Oskoui, Day, Deconinck, Mazzone, Nascimento and Saito51), the role of various lifestyle factors, in particular nutrition and dietary habits, remains underexplored. Despite growing evidence on the impact of an unhealthy lifestyle on chronic diseases, such as cardiovascular and metabolic conditions and cancer, its influence on the clinical course and QoL of NMD patients has not been systematically evaluated.
In the present qualitative systematic review, for the first time, we addressed diet, nutrition, and Mediterranean diet as lifestyle factors affecting the clinical course and QoL of different NMD conditions. The heterogeneity in the clinical conditions and in the measurement methods of lifestyle aspects do not allow a quantitative analysis, but, overall, better management of diet and lifestyle and a higher level of health-promoting behaviours promoted symptom stability and improved general health, vitality, and QoL(Reference Andersen, Aadahl, Vissing and Knak22,Reference Billich, Bray, Truby, Evans, Carroll and de Valle24,Reference Billich, Bray, Truby, Evans, Ryan and Carroll25,Reference Jackson, Parthan, Lauher-Charest, Broderick, Law and Barnett32,Reference Kim, Jin, Kim and Park33,Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39) .
Among NMD patients, anthropometric dynamics and nutritional status exhibit great differences according to the pathological conditions and their progression(Reference Salera, Menni, Moggio, Guez, Sciacco and Esposito1,Reference Chou, Lindeback, D’Silva, Sampaio, Neville and Farrar7) . Although this population is at elevated risk for malnutrition, either by excess or deficiency, only 10% of the patients underwent nutritional screening, and, among them, less than 50% exhibited a normal weight according to WHO criteria(46). This result highlights a critical gap in clinical practice, as timely nutritional assessment could facilitate early interventions to optimise dietary intake and prevent complications. Malnutrition-specific screenings were performed in a small percentage of patients, of whom approximately one third were found to be at risk for severe malnutrition. Moreover, both the collection of waist circumference data, and even arm or calf circumference detection – quick and non-invasive methods to assess metabolic risk-related overweight and obesity, and malnutrition and muscle loss, respectively – were performed in a negligible proportion of subjects(Reference Amzali, Wilson, Bommart, Picot, Galas and Mercier5,Reference Billich, Bray, Truby, Evans, Carroll and de Valle24,Reference Nishizawa and Nakamura37) . These data emphasise how anthropometric and malnutrition risk assessments are still poorly investigated, despite the well-documented consequences on health status, hospitalisation duration, and overall QoL. International guidelines, such as the GLIM criteria for malnutrition diagnosis, advocate for a more comprehensive assessment of nutritional risk, yet their implementation in NMDs remains limited(Reference Cederholm, Jensen, Correia, Gonzalez, Fukushima and Higashiguchi52). Another aspect that is still underestimated is the assessment of body composition in terms of lean and fat mass. Dual-energy X-ray absorptiometry, widely used as a reference method in research, provides accurate measurements but is costly and not always accessible. Bioimpedance analysis, thanks to the technological improvements and increasing reliability of devices, represents a more practical and feasible approach for routine clinical settings, and may complement DEXA in the monitoring of patients with neuromuscular disorders(Reference Ellegard, Aldenbratt, Svensson and Lindberg53). The estimation of total body fat, the infiltration of fatty deposits between muscle fibres, and the amount of total muscle mass, are parameters that can monitor the progression of many NMDs and the effects of targeted interventions(Reference Amzali, Wilson, Bommart, Picot, Galas and Mercier5,Reference López-Gómez, Ballesteros-Pomar, Torres-Torres, De la Maza, Penacho-Lázaro and Palacio-Mures34,Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39,Reference Wilson, Bommart, Passerieux, Picot, Mercier and Laoudj-Chenivesse44) ; these rapid and very low-cost methods could be implemented.
Gastrointestinal conditions, such as gastroesophageal reflux disease, dysphagia, swallowing difficulties, constipation, and other impairments, heavily affect both the nutritional status and the QoL of NMD patients. After a timely assessment of the anthropometric measurements, the gastrointestinal function should also be evaluated as soon as possible, and, although no specific recommendations for all the NMDs are currently available, should be taken into account in the treatment pathway(Reference Dipasquale, Morello and Romano8). In the present systematic review, gastrointestinal function was assessed in about 40% of subjects, thus representing an additional aspect to be implemented.
Based on the above considerations, diet management and eating habits play a crucial role in the disease progression, symptoms improvement, and QoL in NMDs, and most of the articles included in the present review have investigated this aspect of lifestyle. Overall, observational studies detected both quantitative and qualitative deficiencies: calories, proteins, lipids, and fibres were often low in comparison to dietary recommendations, as well as vitamin C, vitamin E, zinc, selenium, and calcium. The analysis of diet quality showed a reduced consumption of fruit and vegetables, legumes, nuts, and seeds, substituted by discretionary foods. Clinical trials based on dietary interventions, mainly aimed at improving energy and macro- and micronutrient intakes, were found to be overall quite effective in improving motor skills, fatigue tolerance, and quality of life, although they have not significantly increased life expectancy(Reference Billich, Bray, Truby, Evans, Carroll and de Valle24,Reference Davidson, Hughes, Ryan, Kornberg, Cairns and Jones26,Reference Dorst, Doenz, Kandler, Dreyhaupt, Tumani and Witzel29,Reference Gazzellone, Lanteigne, Gammage, Fajardo and Ditor31,Reference Ludolph, Dorst, Dreyhaupt, Weishaupt, Kassubek and Weiland35,Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39,Reference Wilson, Bommart, Passerieux, Picot, Mercier and Laoudj-Chenivesse44) . High caloric diets adopted in all conditions characterised by severe malnutrition, such as ALS, provided reasonable results, but, due to low sample sizes and a high rate of drop-out, no statistically significant benefits were identified(Reference Dorst, Doenz, Kandler, Dreyhaupt, Tumani and Witzel29,Reference Ludolph, Dorst, Dreyhaupt, Weishaupt, Kassubek and Weiland35,Reference Prado, Pedro and Adiao54) . Protein supplementation has shown benefits in improving muscle mass and strength, stimulating muscle protein synthesis and counteracting the anabolic resistance in a population of frail individuals, and even in such a heterogeneous population the tendency is in favour of high-protein diets(Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39,Reference Yoshimura, Matsumoto, Inoue, Okamura and Kuzuya55) . However, none of the selected papers used a protein supplement. The ketogenic diet (KD), a dietary pattern effectively proposed in some neurological patients, mainly those suffering from drug-resistant epilepsy(Reference Wickstrom, Taraschenko, Dilena, Payne, Specchio and Nabbout56), has been used in small studies of patients with NMDs. The ability to protect neurons from free radical damage and reduce oxidative stress and neuroinflammatory responses made KD a potential therapeutic adjuvant also in NMDs(Reference Tao, Leng and Zhang57). The small number of patients following a KD in this systematic review only allows us to observe a trend toward improvement of exercise tolerance(Reference Uçar, Altınok, Mansuroglu, Canda, Yazıcı and Çelik41) and QoL(Reference Staretz-Chacham, Pode-Shakked, Kristal, Abraham, Porper and Wormser40). One of the aspects explored in this narrative review was the potential role of the Mediterranean diet in the context of neuromuscular disorders. None of the studies identified assessed adherence to the Mediterranean diet or proposed interventions based on a Mediterranean dietary pattern. A study assessed the potential of a dietary intervention based on foods rich in antioxidants, plant-based foods, and omega-3 fatty acids, which involved reducing the intake of sugars and refined foods. Although this intervention shares some characteristics with the Mediterranean diet, it represents a different dietary approach(Reference Gazzellone, Lanteigne, Gammage, Fajardo and Ditor31).
Diet quality is another aspect that should be carefully investigated in the context of NMDs: increasing scientific evidence correlates diets rich in ultra-processed foods with alterations at the gut–brain axis level and a possible neurotoxic effect(Reference Cai, Song, Xu, Yang, Wei and Chen58,Reference González Olmo, Butler and Barrientos59) . In the context of improving dietary fat quality, the replacement of ultra-processed snacks with whole, nutrient-dense foods such as nuts or nut-based spreads, may offer additional metabolic and cardiovascular benefits. A recent systematic review with Bayesian meta-analysis demonstrated that hazelnut consumption significantly improves blood lipid profiles, particularly by reducing total and LDL cholesterol, without negatively affecting body weight. These findings support the potential role of nut consumption as part of a Mediterranean dietary pattern in patients with neuromuscular disorders(Reference Perna, Giacosa, Bonitta, Bologna, Isu and Guido60). A poor diet quality, characterised by great consumption of high caloric food, rich in sugars and fats and poor in vegetables, legumes, and whole grains, has been detected among young DMD patients, thus promoting an inappropriate nutritional status. Given the increasing evidence linking ultra-processed foods to neurotoxicity and gut–brain axis dysfunction, dietary patterns rich in minimally processed, nutrient-dense foods, such as the Mediterranean diet, may offer a protective effect in NMDs(Reference Dietvorst, Bot, Van Der Holst and Niks27,Reference van Hees, Knuijt, Dicke, Groothuis, Raaphorst, Satink and Cup42) . Moreover, abundance of fibre could also improve gut function and glycaemic control. A greater adherence to a healthy dietary pattern, rich in antioxidants, polyphenols, and fibre, represents a promising approach also in neuromuscular disorders where oxidative stress plays a predominant role(Reference Petrella, Di Certo, Gabanella, Barbato, Ceci and Greco18,Reference Bakırhan, Özkaya and Pehlivan19) . The Mediterranean lifestyle is also integrated by regular practice of physical activity and muscle-strengthening activities, adequate rest, and socialisation during meals(Reference Serra-Majem, Tomaino, Dernini, Berry, Lairon and Ngo de la Cruz17). Exhaustive studies focused on the effects of Mediterranean diet and lifestyle on NMD progression and QoL are still lacking. This gap highlights a promising avenue for future research aimed at integrating nutritional and lifestyle strategies into NMD management.
In addition to diet quality interventions, the involvement of both caregivers and patients appears to be more effective in increasing adherence, participant satisfaction, and QoL(Reference Billich, Bray, Truby, Evans, Ryan and Carroll25,Reference van Hees, Knuijt, Dicke, Groothuis, Raaphorst, Satink and Cup42) .
With regard to the other lifestyle-related aspects among those identified in this literature review, physical activity appears to be a cornerstone in health promotion even in patients with NMDs: despite the many barriers to exercise these subjects may face, an overall positive correlation between PA and improved motor function and QoL has been observed. More active patients reported significantly increased fatigue tolerance from daily activity, although different pathological settings and different methods of investigation did not allow a uniform result to be derived. Overall, these findings underscore the importance of considering exercise as a key lifestyle factor that can positively influence the evolution of these complex and disabling diseases(Reference Bettio, Banchelli, Salsi, Vicini, Crisafulli and Ruggiero16).
Increasing evidence suggests that insomnia, sleep loss, or circadian sleep disturbance may act as neurobiological stressors which directly contribute to neuroinflammation by increasing pro-inflammatory cytokines and negatively influencing neural plasticity, causing neuron loss, neural death, and neural injury(Reference Palagini, Manni, Aguglia, Amore, Brugnoli and Girardi61). In patients suffering from NMDs, respiratory problems, movement limitations, and worry about illness affect the sleep quality and duration, with a further impairment of general fatigue, motivation, and mental well-being. However, this aspect has been evaluated only marginally in this review, given the small number of articles selected, as was the case with smoking habits and addictions, did not allow exhaustive conclusions to be reached on the matter.
Data on emotional perception and care are available for a considerable proportion of patients selected for this systematic review: a better quality of diet, including specific supplements, greater involvement in physical activity, and better sleep hygiene are all factors that, in different studies, have been related to better emotional condition and a lower risk of developing depression or anxiety. On the other hand, negative emotional status, like anxiety, depression, and stress, are common in these patients, heavily affecting their QoL. This trend emphasises how different aspects of lifestyle have a synergistic effect and how they should therefore be analysed altogether. Social occasions and interpersonal relationships are referred to as difficult situations to manage and indeed generate concern; however, multidisciplinary approaches, through the involvement of caregivers and patient groups, have improved patient perception and engagement.
This review underscores how, even in the most complex neuromuscular disease settings, taking charge of nutrition, diet quality, and some lifestyle factors such as physical movement and emotional conditions could support the patient both in the course of the pathology and especially regarding QoL. Moreover, the active involvement of caregivers in both healthy behaviour knowledge and tailored interventions could also improve the QoL of these families.
Our results should be considered in the light of some limitations. First, the research methodology was more oriented towards diet and nutrition and less specific with regard to other aspects of lifestyle, such as sleep, smoking, alcohol consumption, anxiety, or depression. Moreover, heterogeneities among the selected studies, including study design, methods and reporting, sample size, type of disease, and endpoints, allowed a qualitative systematic descriptive analysis, and highlight the gaps in this research area. The randomised controlled trials identified cover only four conditions (ALS(Reference Dorst, Doenz, Kandler, Dreyhaupt, Tumani and Witzel29,Reference Ludolph, Dorst, Dreyhaupt, Weishaupt, Kassubek and Weiland35) ; DMD(Reference Davidson, Hughes, Ryan, Kornberg, Cairns and Jones26); FSHD(Reference Wilson, Bommart, Passerieux, Picot, Mercier and Laoudj-Chenivesse44); rare metabolic NMD(Reference Sechi, Zuccarelli, Grassi, Frangiamore, De Amicis and Marzorati39,Reference Staretz-Chacham, Pode-Shakked, Kristal, Abraham, Porper and Wormser40) ) and address different interventions (hypercaloric diets, multicomponent supplements, ketogenic diet, exercise combined with diet), making design-based subgrouping methodologically inappropriate. Our search was restricted to studies published in the last five years, which may have excluded relevant earlier evidence. Furthermore, a considerable proportion of the collected data is related to patients with myasthenia gravis, while no studies were found that met the inclusion criteria dedicated to patients with Guillain-Barré syndrome, despite it being a well-known neuromuscular disorder, and this may influence overall outcomes. Moreover, the majority of patients were of Asian ethnicity, limiting external validity and generalisability.
However, to our knowledge this is the first systematic review offering a more comprehensive view of the complex interrelationship between diet, nutrition, Mediterranean diet, lifestyle, and pathological parameters and QoL in NMD patients. This review emphasises that the assessment of nutritional status, body composition, and gastrointestinal function are elements that should be systematically explored within clinical practice in order to develop nutritional interventions adapted to each patient.
Given the multiple benefits of the Mediterranean diet in several neurological conditions(Reference Zuliani, Gianfredi, Veronese, Volpe, Maggi and Onder62), the role it plays in neuromuscular disorders remains largely unexplored, both in terms of adherence to the Mediterranean diet and the implementation of dietary interventions based on the Mediterranean model. Future research should aim to standardise dietary and lifestyle assessment tools, implement multidisciplinary interventions, and explore the long-term impact of lifestyle modifications on both disease progression and patient-reported outcomes.
Conclusion
In conclusion, given the heterogeneity and disabling nature of these disorders, it is crucial to consider the interplay of diet and lifestyle according to multidisciplinary and personalised approaches in order to significantly improve health outcomes and quality of life for patients and their families. A comprehensive, multidisciplinary approach to diet and lifestyle, including regular nutritional screening, promotion of physical activity adapted to individual functional capacity, psychological support, and family/caregiver involvement, appears to be the most promising strategy for improving clinical outcomes and QoL in these patients. Future research should prioritise adequately powered intervention trials, standardised nutritional assessment protocols, and the study of Mediterranean diet adherence and its potential neuroprotective effects in NMDs.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954422426100420
Acknowledgements
The authors thank Dr. Daria Cattaneo for her contribution during the initial stages of the project.
Authorship
S.M., G.G., B.Z., and M.F. conceived the idea for the study, and developed the rationale and research questions. S.M. and G.G. wrote the first draft of the manuscript. B.Z., M.F., M.M, G.M., B.R., A.P., and M.C. provided critical review and feedback at each stage of the process. A.P., M.C., B.Z., and M.F. supervised the project. All authors critically revised the manuscript for intellectual content and agreed and approved the final manuscript. S.M. is the guarantor of the review.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The authors declare none.



 Open access
Open access