Colorectal cancer (CRC) is a prevalent cancer type that ranks third in males and second in females globally(Reference Siegel, Miller and Jemal1). It is also the second leading cause of cancer deaths worldwide(Reference Biller and Schrag2). The probability of developing CRC during an individual’s lifetime is estimated to be around 4–5 %, and this risk can vary based on factors such as age, disease history and lifestyle(Reference Mármol, Sánchez-de-Diego and Pradilla Dieste3).
Upon the diagnosis of CRC, clinical and pathological staging are crucial in determining the local extent, lymph node involvement and the presence of metastases(Reference Quirke, Williams and Ectors4–Reference Chen, Collins and Wang6). Identifying the histopathological characteristics of the tumour is essential for targeting the most suitable oncological treatment and assessing the prognosis(Reference Pătraşcu, Cercelaru and Graure7). Histopathological changes that occur in CRC patients can vary significantly(Reference Park, McMillan and Powell8,Reference Jakubowska, Kisielewski and Kańczuga Koda9) .
Tumour aggressiveness in solid cancers has been linked to the tumour microenvironment, with particular emphasis on desmoplasia. Desmoplasia is a histopathological finding commonly seen in the vicinity of malignant solid tumours such as CRC, where fibrous or connective tissue grows in response to tumour growth(Reference Suarez-Carmona, Lesage and Cataldo10–Reference Kim, Lee and Kim13). In desmoplastic regions, excessive accumulation of extracellular matrix proteins may contribute to tumour progression by altering local cytokine distribution and substrate rigidity(Reference Zeltz, Primac and Erusappan14). Furthermore, the presence of desmoplasia has been associated with tumour invasiveness, increased risk of disease progression and recurrence and reduced overall survival (OS) in patients with CRC(Reference Mochizuki, Ao and Sugiura11,Reference Huang, Lin and Lim15–Reference Wagner, Richter and Hille17) .
Studies investigating the relationship between adiposity levels and desmoplasia in cancer patients remain scarce. Nonetheless, emerging evidence suggests a potential link. For instance, one study reported that obesity is associated with an increase in desmoplastic stromal reaction and a reduced response to chemotherapy in patients with pancreatic cancer, ultimately contributing to tumour progression within an obesogenic microenvironment(Reference Incio, Liu and Suboj18).
In this context, the evaluation of body composition through computed tomography (CT) has become increasingly important in the management of cancer patients(Reference Mourtzakis, Prado and Lieffers19–Reference Cespedes Feliciano, Kroenke and Caan21). Previous studies have established the correlation between fat distribution, lean muscle mass and postoperative complications, hospitalisation duration and mortality(Reference Cespedes Feliciano, Kroenke and Caan21–Reference Fleming, O’Connell and Kavanagh23). Moreover, the prognostic value of adipose tissue radiodensity measured by CT has been explored in some types of cancer(Reference da Cunha Júnior, Silveira and Takahashi24–Reference Feliciano, Winkels and Meyerhardt26). A growing body of evidence suggests that CT-based analysis of adipose tissue radiodensity may serve as a promising prognostic marker in different stages of CRC treatment(Reference Black, Mackay and Ramsay20,Reference Fleming, O’Connell and Kavanagh23,Reference Feliciano, Winkels and Meyerhardt26) . Specifically, decreased radiodensity may indicate larger adipocytes, while increased radiodensity may be indicative of adipocyte atrophy, inflammation or oedema(Reference Feliciano, Winkels and Meyerhardt26).
Therefore, it is essential that studies explore the relationship between adiposity and the histological features of colorectal tumours and their impact on the OS of patients with CRC. Understanding the tumour microenvironment and its possible relationship with body fat distribution may facilitate the development of more targeted and effective therapeutic strategies for the management of CRC. Thus, this study aimed to examine the association between histopathological characteristics and adiposity in CRC patients and assess the prognostic capacity of these factors in predicting survival outcomes.
Methods
Participant recruitment
A retrospective cohort study was conducted at the Brazilian national referral cancer centre between January 2007 and December 2015, with a specific focus on patients diagnosed with CRC. Inclusion criteria encompassed patients aged 20 or above who had undergone surgery as their initial treatment and received confirmation of CRC diagnosis through histopathological analysis. Furthermore, patients were required to have undergone CT imaging at the level of the third lumbar vertebra (L3) within 90 d prior to surgery. Exclusion criteria were established, including patients with a previous cancer diagnosis, absence of laboratory testing, distant metastasis, neoadjuvant treatment or non-curative surgery, active infectious, hematological, chronic or autoimmune inflammatory diseases, hormone therapy, decompensated respiratory pathology, heart failure or acute myocardial infarction within the past 6 months, immunomodulatory drug usage, recent transfusion within the past 3 months, poor-quality CT images or interference artifacts and individuals lacking tumour tissue samples available from the tumour bank. This study adhered to the quality criteria established in the STROBE Statement(Reference Von Elm, Altman and Egger27).
Patients and clinical samples
Demographic and clinical data were extracted from physical and electronic medical records. Researchers, who had received appropriate training, gathered the following information: age, sex, tumour location, staging, degree of differentiation, presence of disease recurrence or metastasis, type of antineoplastic treatment (including exclusive surgery, adjuvant radiotherapy, adjuvant chemotherapy or adjuvant chemotherapy plus radiotherapy) and laboratory test results (blood count: neutrophils and lymphocytes) taken 2 weeks before surgery. The NLR was calculated by dividing the absolute neutrophil count by the absolute lymphocyte count. Additionally, the dates of diagnosis and death were recorded.
Computed tomography imaging data acquisition
The CT scan of the L3 was utilised for body composition assessment. Trained observers analysed the scan, which was subsequently verified by a second observer using SliceOmatic software (version 5.0, Tomovision, Canada). This software facilitates precise delineation of specific tissues and their expression in Hounsfield Units (HU).
For subcutaneous adipose tissue, CT attenuation thresholds of –190 to –30 HU were employed, while thresholds of –150 to –50 HU were used for visceral adipose tissue. Accurate segmentations of muscle and fat were obtained, and the following quantitative measures were recorded: skeletal muscle index (SMI), visceral adipose tissue radiodensity (VATd) and subcutaneous adipose tissue radiodensity (SATd). Adipose tissue was quantified using HU, whereas SMI was measured in square centimeters per square meter (cm2/m2)(Reference Mourtzakis, Prado and Lieffers19).
To categorise VATd, SATd and SMI, we first separated the sample into men and women, respecting the biological differences in body composition between both sexes. Within each sex group, these variables were divided into tertiles based on their radiodensity values. Subsequently, the first, second and third tertiles of men and women were aggregated (first tertile men + first tertile women; second tertile men + second tertile women; third tertile men + third tertile women) for statistical analysis purposes. The SMI area stratified into lower tertiles is associated with lower muscle mass, while the upper tertiles mean higher amounts of muscle mass. In contrast, the interpretation of the VATd and SATd analyses follows an inverse pattern: the first tertile denotes low radiodensity (high fat content), the second tertile represents intermediate radiodensity (intermediate fat content) and the third tertile indicates high radiodensity fat (low fat content).
Histological categorisation
Tissue samples from surgeries, embedded in paraffin, were dehydrated overnight at 60°C, then deparaffinised in xylene and rehydrated through graded alcohols in water. Endogenous peroxidase activity was blocked by incubating with 3 % hydrogen peroxide for 10 min. Antigen retrieval was performed using EDTA for 20 min at a temperature of 65·98°C, heated in a microwave oven. A blocking agent was applied for 10 min at room temperature. The deparaffinised sections were stained with Mayer’s hematoxylin for 10 min (to stain the nuclei) and washed with water before being stained with eosin for 10 min (to stain the cytoplasm). The stained sections were dehydrated in 70 % ethanol, 80 % ethanol, 90 % ethanol, 100 % ethanol and finally cleared in xylene.
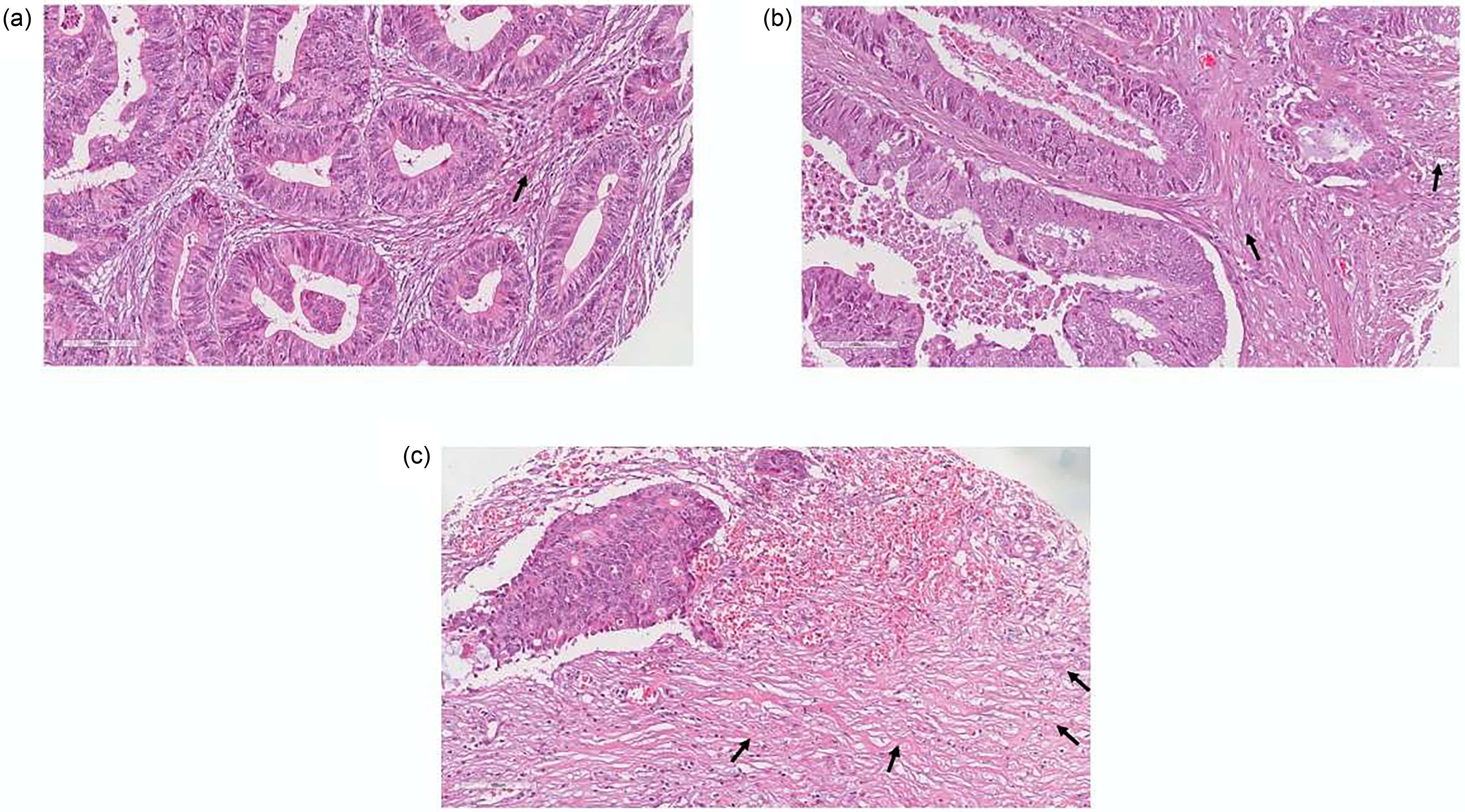
Next, an experienced pathologist (F.R.R.) analysed the slides. The material was examined for lymph node infiltration (absent v. confirmed), perineural invasion (absent v. confirmed), tumour size (in cm) and desmoplastic reaction. To measure tumour size, we utilised the largest horizontal diameter of the tumour obtained from the pathological analysis(Reference Saha, Shaik and Johnston28–Reference Yasui, Takemasa and Miyake30). The presence of desmoplastic reaction was semiquantitatively classified as follows: mild fibrous stroma (desmoplasia poorly present/< 25 %), moderate fibrous stroma (desmoplasia moderately present/25–75 %) or accentuated fibrous stroma (desmoplasia strongly present/> 75 %).
Survival outcome
The calculation of OS in this study involved measuring the duration from the date of histopathological diagnosis to the date of death from any cause. Patients who survived beyond the 5-year period or discontinued medical follow-up were classified as censored cases.
Data analysis
Variable distribution symmetry was assessed using the Kolmogorov–Smirnov test, and categorical variables were presented as absolute or relative frequencies. Tertiles obtained from the sample analysis were used to define classification ranges for variables (NLR, SMI, VATd and SATd).
The association between desmoplasia and the independent variables investigated in this study, as well as tumour aggressiveness, was analysed using logistic regression. Logistic regression analysis was employed to calculate the OR along with its corresponding 95 % CI and P-value.
For multivariate analyses, we employed a stepwise selection method to identify the most significant factors influencing the results. This approach iteratively adds or removes variables based on their statistical significance. We established predefined criteria: variables with an entry probability equal to or less than 0·05 (indicating a 5 % or less chance of being irrelevant) were included, while variables with an exit probability equal to or greater than 0·10 (indicating a higher probability of being irrelevant) were excluded. All variables with a P-value < 0·200 in the univariate analyses were considered for inclusion in the final multivariate model. Additionally, variables with demonstrated biological plausibility (e.g. age and sex) were incorporated based on their potential relevance to the study objectives. The selection of these variables was guided by the hypothesised associations between adipose tissue distribution, histopathological alterations and overall 5-year survival in patients with CRC. Survival functions were estimated using the Kaplan–Meier method, and the Log-rank test was employed to assess and compare survival probabilities based on the stratification of the selected variables. Hazard ratios (HR) with 95 % CI for the analysed variables were also estimated using both univariate and multivariate Cox proportional hazards models.
All statistical analyses were performed using IBM SPSS Statistics for Windows (version 25). Statistical significance was considered when P< 0·05.
Results
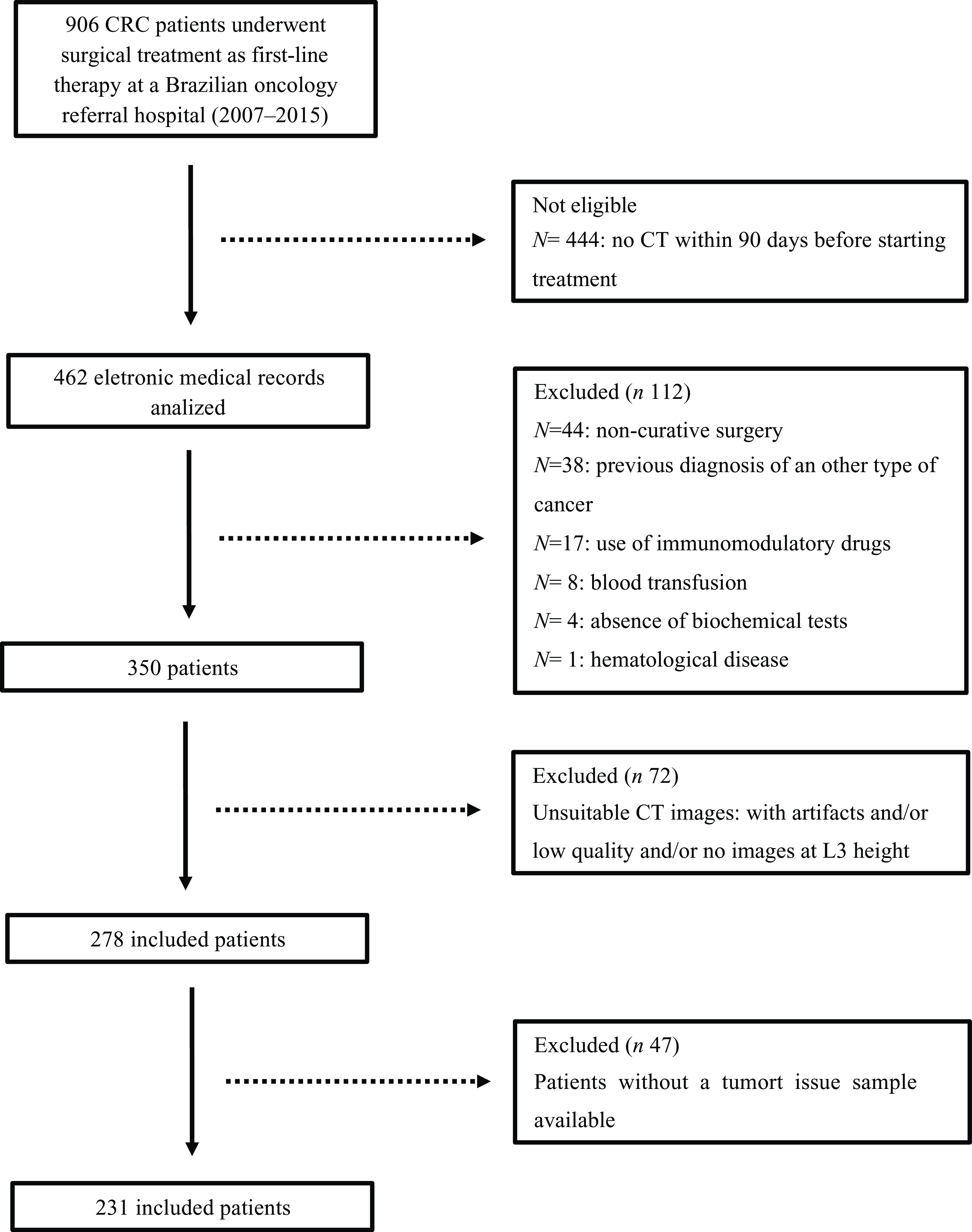
During the designated data collection period, a total of 906 patients underwent surgical treatment as first-line therapy for CRC. Of these, a subset of 231 individuals met the eligibility criteria and were included in the study, as shown in Figure 1.
Study flowchart. CRC, colorectal cancer; CT, computed tomography; L3, third lumbar vertebra; n, number of observations.

Demographic and clinicopathological characteristics
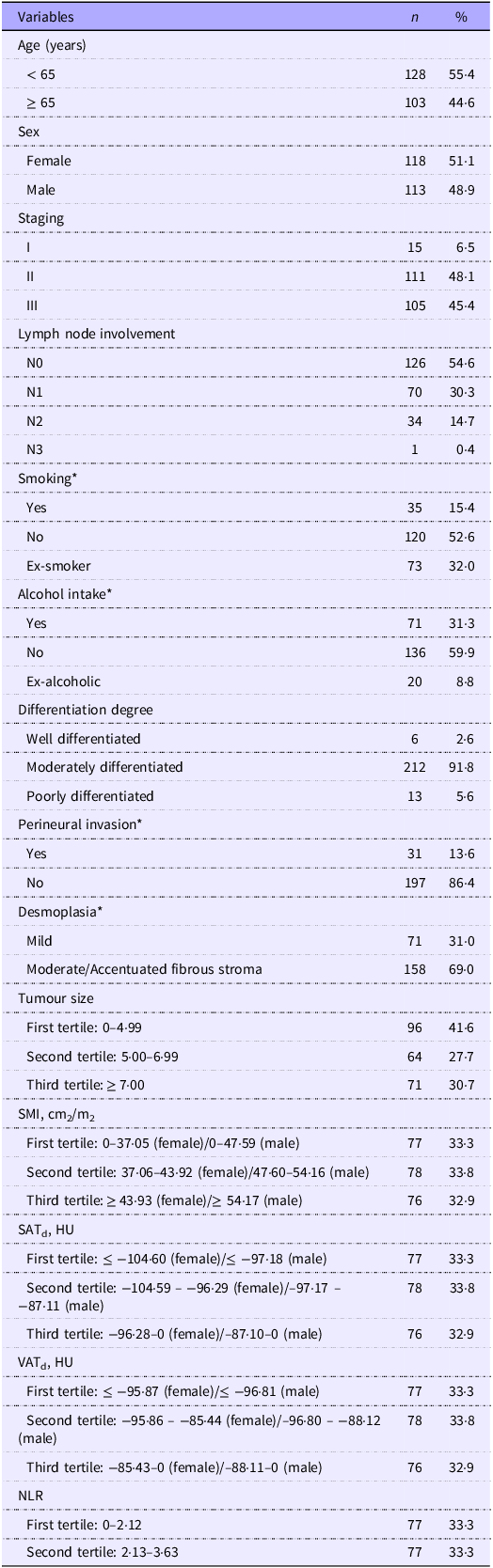
In our cohort, the predominant segment was composed of individuals under 65 years of age (55·4 %). The distribution by sex showed a higher percentage of female patients (51·1 %), while 48·9 % were male. Regarding CRC staging, the predominant stages were classified as II and III, representing a substantial proportion (93·6 %) of cases, and a significant majority (91·8 %) also had moderate differentiation. Notably, approximately 69 % of patients had moderate to accentuated fibrous stroma, as outlined in Table 1.
Epidemiological and clinicopathological profiles of the patients with colorectal cancer (n 231) (Number and percentages)

Note: N, number of observations; %, frequency; HU, Hounsfield units; SMI, skeletal muscle index; SATd, subcutaneous adipose tissue radiodensity; VATd, visceral adipose tissue radiodensity; NLR, neutrophil-to-lymphocyte ratio.
Variables with missing data (≤ 2 %).
SATd was associated with lower tumour size in the tumour aggressiveness analyses
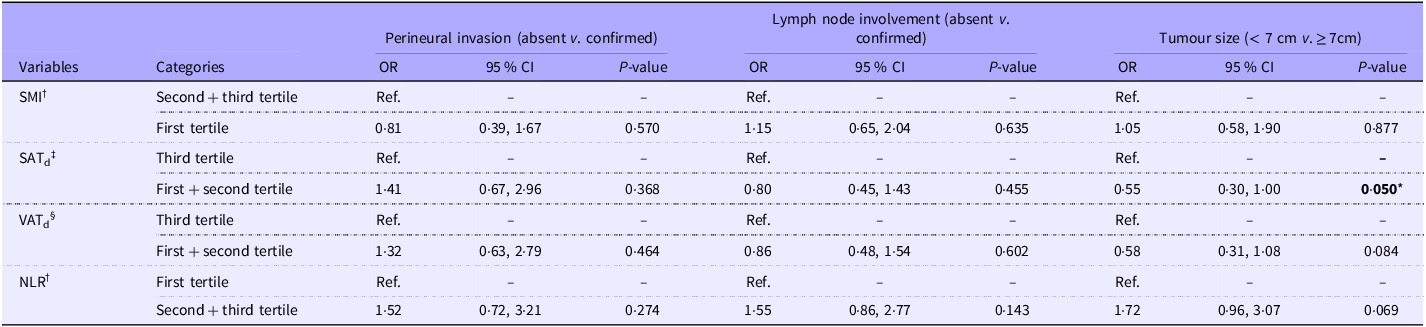
In the univariate analysis, several factors potentially linked to tumour aggressiveness were evaluated, with the degree of differentiation, VATd and SATd showing a significant association with tumour size. However, none of the analysed variables showed a significant correlation with perineural invasion or lymph node involvement (online Supplementary Table 1). Subsequently, a multivariate logistic regression analysis was performed to further explore the relationships of body composition, systemic inflammation (NLR) and other clinicopathological characteristics with tumour aggressiveness. Despite initial univariate findings, no body composition component was significantly associated with critical aggressive tumour features such as perineural invasion or lymph node involvement. However, SATd emerged as a potential protective factor. In this analysis, SATd was inversely associated with tumour size (OR = 0·55, 95 % CI: 0·30, 1·00), suggesting that higher levels of subcutaneous fat may be associated with smaller tumour size (Table 2).
Multivariate logistic regression of associated factors to tumour aggressiveness in surgical patients with colorectal cancer (OR and 95 % CI)

SMI, skeletal muscle index; SATd, subcutaneous adipose tissue radiodensity; VATd, visceral adipose tissue radiodensity; NLR, neutrophil-to-lymphocyte ratio.
P< 0·05.
†OR for multivariate logistic analyses were adjusted by age (< 65 v. ≥ 65 years), sex (female v. male), differentiation degree (well differentiated v. moderately differentiated, poorly differentiated), SMI (second tertile + third tertile v. first tertile), NLR (first tertile v. second tertile + third tertile).
‡SATd (third tertile v. first tertile + second tertile).
§VATd (third tertile v. first tertile + second tertile).
Bold values are statistically significant (P < 0.05).
VATd was associated with desmoplastic reaction (moderate to accentuated fibrous stroma) occurrence
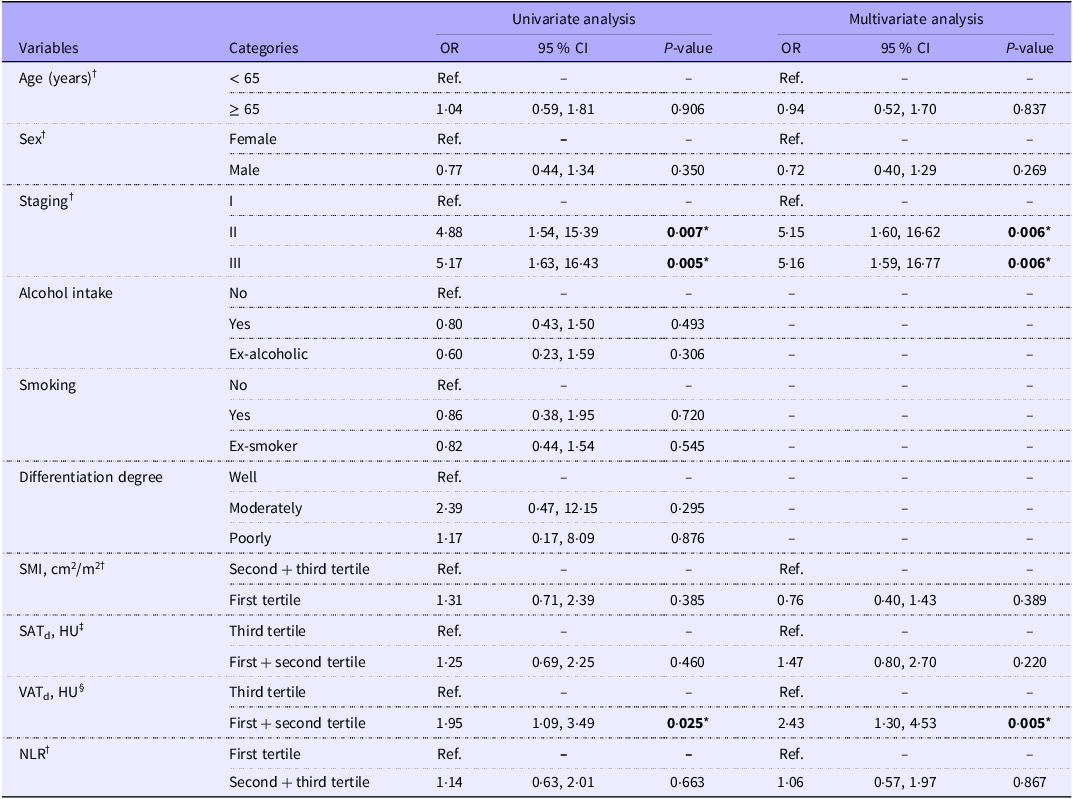
Based on the results presented in Table 3, univariate analysis identified CRC stages II and III, as well as the lower tertiles of VATd (first and second tertiles), as significant predictors of desmoplastic reaction. Specifically, these factors were strongly associated with the presence of fibrous stromal remodelling in the tumour microenvironment, a key feature of tumour aggressiveness. In the multivariate analysis, after adjusting for potential confounders, including age, sex, SMI and NLR, these associations remained statistically significant. Both CRC stages II and III were independently associated with an increased likelihood of desmoplastic reaction (OR = 5·15, 95 % CI: 1·60, 16·62 and OR = 5·16, 95 % CI: 1·59, 16·77, respectively). Additionally, lower VATd (i.e. the 1st and 2nd tertiles) was found to be independently associated with the presence of moderate to accentuated fibrous stroma (OR = 2·43, 95 % CI: 1·30, 4·53). This suggests that reduced visceral fat may be a contributing factor to the desmoplastic response in CRC, highlighting a potential link between adipose tissue distribution and tumour progression.
Univariate and multivariate logistic regression of associated factors to moderate to accentuated fibrous stroma in patients with colorectal cancer (OR and 95 % CI)

HU, Hounsfield units; VATd, visceral adipose tissue radiodensity; SATd, subcutaneous adipose tissue radiodensity; SMI, skeletal muscle index; NLR, neutrophil-to-lymphocyte ratio.
P< 0·05.
†OR for multivariate logistic analyses were adjusted by age (< 65 v. ≥ 65 years), sex (female v. male), staging (I v. II, III), SMI (second tertile + third tertile v. first tertile), NLR (first tertile v. second tertile + third tertile).
‡SATd (third tertile v. first tertile + second tertile).
§VATd (third tertile v. first tertile + second tertile).
Bold values are statistically significant (P < 0.05).
Furthermore, Figure 2 presents representative histological images of tumour samples illustrating varying intensities of the desmoplastic reaction, thereby capturing the morphological spectrum of stromal remodeling observed in our CRC specimens.
Desmoplastic reactions categorised as (a) mild fibrous stroma (desmoplasia poorly present/< 25 %), (b) moderate fibrous stroma (desmoplasia moderately present/25–75 %) or (c) accentuated fibrous stroma (desmoplasia strongly present/> 75 %). Magnification 40×. Black arrows indicate areas of desmoplastic reaction.

Kaplan–Meier analysis and overall survival prognosis
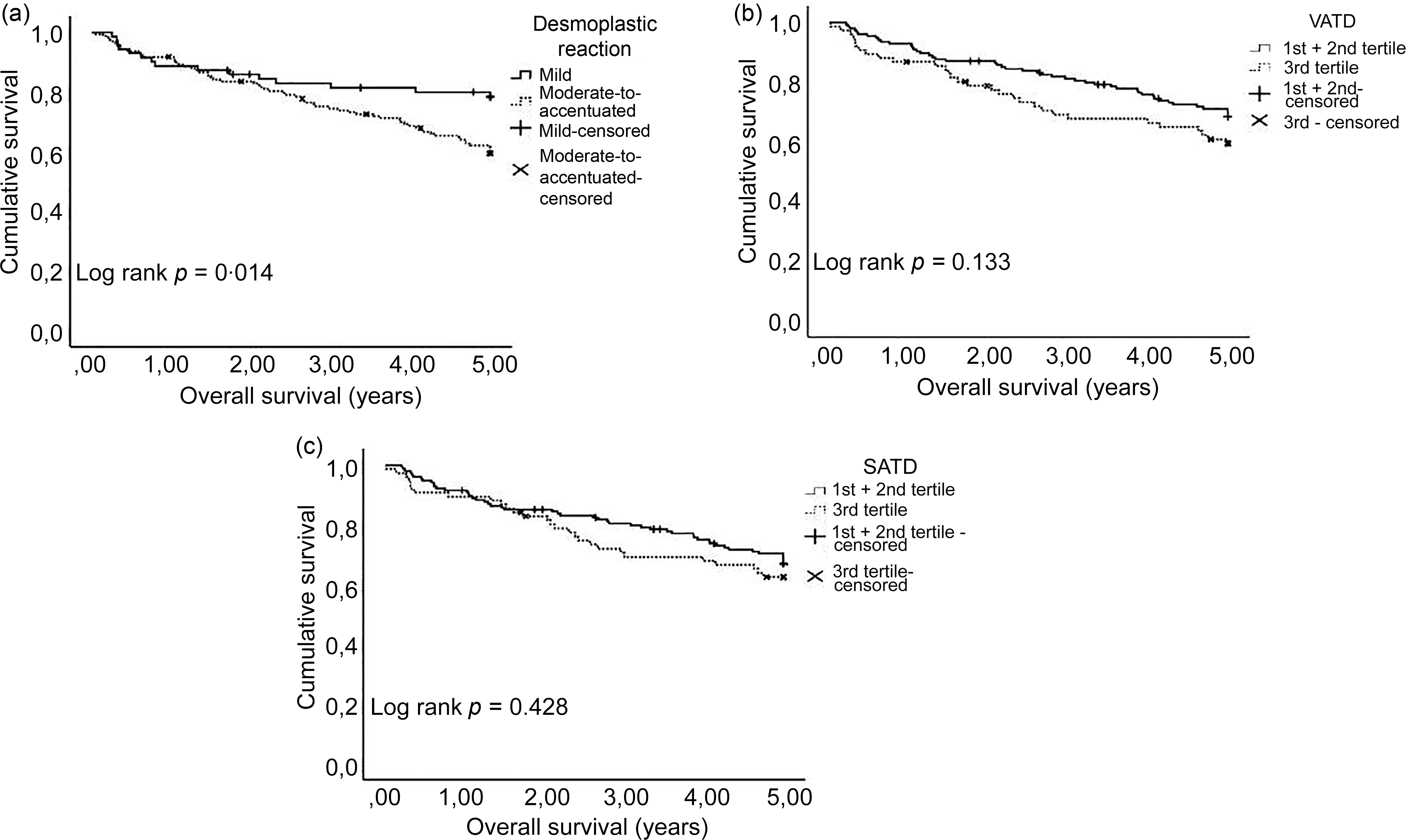
Kaplan–Meier analysis revealed a statistically significant difference across the levels of desmoplastic reaction (P= 0·014) (Figure 3(a)). In contrast, the body composition parameters related to adipose tissue compartments did not demonstrate significant differences among the tertile groups (P= 0·133 for VATd and P= 0·428 for SATd) (Figure 3(b) and (c)).
Kaplan–Meier survival curves were employed to stratify surgical patients with colorectal cancer based on (a) desmoplastic reaction; (b) VATd and (c) SATd. VATd (Hounsfield units): first tertile: ≤ −95·87 (female)/≤ −96·81 (male); second tertile: −95·86 to −85·44 (female)/–96·80 to −88·12 (male); third tertile: −85·43–0 (female)/–88·11–0 (male) SATd (Hounsfield units): first tertile: ≤ −104·60 (female)/≤ −97·18 (male); second tertile: −104·59 to −96·29 (female)/–97·17 to −87·11 (male); third tertile: −96·28–0 (female)/–87·10–0 (male). VATd, visceral adipose tissue radiodensity; SATd, subcutaneous adipose tissue radiodensity.

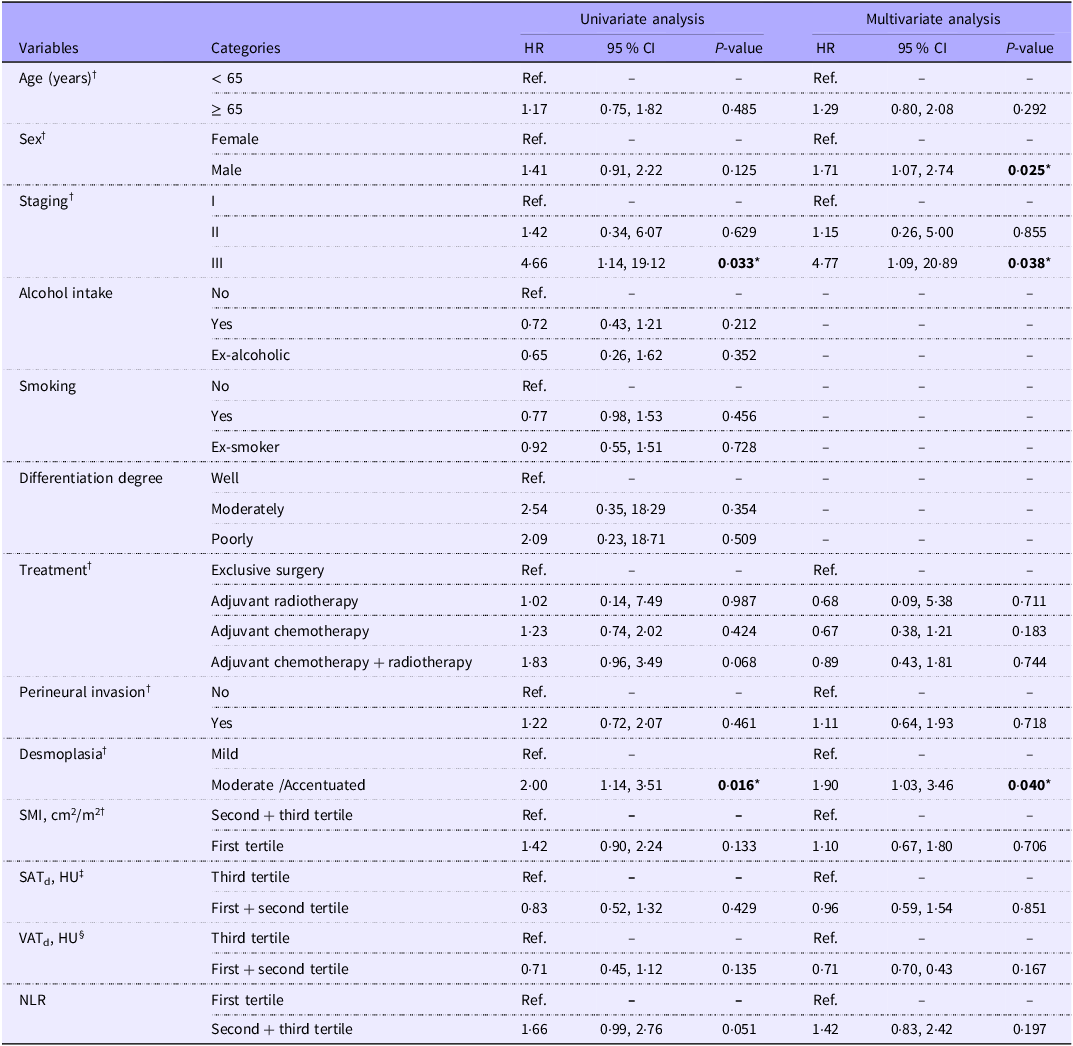
As shown in Table 4, univariate Cox regression analysis for OS indicated that stage III disease (HR = 4·66, 95 % CI: 1·14, 19·12) and the presence of moderate to accentuated fibrous stroma (HR = 2·00, 95 % CI: 1·14, 3·51) were associated with shorter survival. In the multivariate Cox regression model, male sex (HR = 1·71, 95 % CI: 1·07, 2·74), stage III disease (HR = 4·77, 95 % CI: 1·09, 20·89) and moderate to accentuated fibrous stroma (HR = 1·90, 95 % CI: 1·03, 3·46) emerged as independent predictors of reduced OS.
Univariate and multivariate Cox regression of predictive factors of overall survival in 5 years in surgical patients with colorectal cancer (hazard ratios and 95 % CI)

HR, hazard ratio; HU, Hounsfield units; VATd, visceral adipose tissue radiodensity; SATd, subcutaneous adipose tissue radiodensity; SMI, skeletal muscle index; NLR, neutrophil-to-lymphocyte ratio.
P< 0·05.
†HRs for multivariate logistic analyses were adjusted by age (< 65 v. ≥ 65 years), sex (female v. male), staging (I v. II, III), SMI (second tertile + third tertile v. first tertile), NLR (first tertile v. second tertile + third tertile), perineural invasion (no v. yes), desmoplasia (mild v. moderate + accentuated).
‡SATd (third tertile v. first tertile + second tertile).
§VATd (third tertile v. first tertile + second tertile).
Bold values are statistically significant (P < 0.05).
Discussion
Our findings revealed that lower radiodensity levels of visceral adipose tissue, indicative of higher fat content, were associated with the presence of moderate to accentuated desmoplasia. Furthermore, desmoplastic reaction in CRC has emerged as an independent risk factor for a worse 5-year prognosis.
To the best of our knowledge, no previous study has specifically investigated the association between body composition, particularly VATd, and the development of desmoplasia in patients with CRC. However, prior randomised experimental studies in rodent models have demonstrated that the accumulation of dysfunctional, hypertrophic adipocytes within visceral adipose tissue contributes to the onset of a localised desmoplastic response characterised by fibrosis and chronic inflammation, particularly in the context of pancreatic cancer. These studies further suggested that high body adiposity-induced inflammation plays a pivotal role in shaping a desmoplastic tumour microenvironment, which facilitates tumour progression and aggressiveness(Reference Incio, Liu and Suboj18,Reference Okumura, Ohuchida and Sada31,Reference Okumura, Ohuchida and Kibe32) .
In line with these findings, our study identified a significant association between increased visceral fat content – indirectly inferred through decreased radiodensity – and the presence of desmoplasia in CRC patients, thereby suggesting a potential mechanistic link between adipose tissue characteristics and stromal remodelling in CRC progression.
Interestingly, the observed relationship between desmoplasia and elevated levels of visceral fat was independent of systemic inflammation, as measured by the NLR. The existing scientific literature suggests that high body adiposity plays a crucial role in promoting desmoplasia, which, in turn, accelerates tumour progression and reduces the efficacy of chemotherapy. This phenomenon is largely attributed to hypoxia resulting from the formation of aberrant blood vessels and impaired tissue perfusion, which are consequences of adipose tissue expansion. Dysfunctional adipocytes, along with the recruitment of immune cells, further exacerbate this process. The accumulation of hypertrophic and dysfunctional adipocytes in visceral adipose tissue may trigger a stromal desmoplastic response, characterised by fibrosis and a dense stromal reaction(Reference Incio, Liu and Suboj18,Reference Okumura, Ohuchida and Kibe32,Reference Kuziel, Moore and Arendt33) .
Despite our results regarding desmoplasia, additional analyses of tumour aggressiveness have failed to demonstrate significant associations between VATd and key markers of tumour progression, including perineural invasion, lymph node metastasis or tumour size. Notably, SATd exhibited an inverse correlation with tumour size. This finding may be attributed to the relationship between tumour burden and increased production of proinflammatory cytokines, which in turn could have a detrimental effect on both lean mass and adipose tissue. Consequently, it can be inferred that smaller tumours may result in less pronounced nutritional deficits(Reference Daas, Rizeq and Nasrallah34).
Nevertheless, in contrast to visceral adipose tissue, which has been more directly implicated in tumour aggressiveness, partly due to its elevated production of proinflammatory cytokines, subcutaneous adipose tissue appears to play a less prominent role in tumour progression. These findings lend support to the hypothesis that the quality of adipose tissue, particularly within distinct anatomical compartments, may differentially modulate tumour behaviour(Reference Han, Liu and Tang35,Reference Lazarchuk, Plizga and Stołecka36) .
In recent years, researchers have proposed the use of adipose tissue radiodensity as a promising prognostic biomarker for patients diagnosed with multiple myeloma and breast cancer(Reference da Cunha Júnior, Silveira and Takahashi24,Reference Cheng, Caan and Chen25) . Furthermore, a study demonstrated that adipose tissue radiodensity is an independent predictor of overall mortality in patients with non-metastatic CRC, regardless of BMI or weight fluctuations(Reference Feliciano, Winkels and Meyerhardt26). It is important to emphasise that increased radiodensity of adipose tissue may reflect reduced lipid content and alterations in the tissue’s structural properties(Reference Ebadi, Dunichand-Hoedl and Rider37). However, in our study, no statistically significant association was found between SATd, VATd and OS over a 5-year period. These findings align with conclusions from larger population-based studies, which have similarly reported no direct correlation between adipose tissue radiodensity and long-term survival outcomes(Reference Cheng, Caan and Chen25,Reference Anyene, Caan and Williams38) .
Studies involving other types of tumours also did not report a significant association between fat compartments and OS. In a retrospective cohort study involving 2868 patients with non-metastatic breast cancer, neither low SATd nor VATd demonstrated significant associations with overall mortality. On the other hand, it was found that high SATd at the time of diagnosis was significantly associated with an increased risk of overall mortality. The authors proposed several potential underlying mechanisms for this association, including accelerated depletion of subcutaneous fat, increased vascularity indicative of more aggressive tumour behaviour, extracellular matrix deposition leading to desmoplasia and an amplified inflammatory response(Reference Cheng, Caan and Chen25).
Although our results highlight the significant impact of tumour morphology on body composition, other studies have demonstrated that host phenotypic characteristics, such as skeletal muscle attenuation and adipose tissue composition, can significantly influence clinical outcomes, independently of tumour-specific factors. Van Dijk et al. (2017) reported that low skeletal muscle radiodensity attenuation and visceral adiposity were associated with increased risk of surgical site infections and reduced OS in patients with pancreatic cancer(Reference Van Dijk, Bakens and Coolsen39). Furthermore, in a separate cohort of patients with colorectal liver metastases, it was found that body composition metrics were predictive of OS regardless of tumour biology, underscoring the prognostic importance of host-related factors in oncologic outcomes(Reference Van Dijk, Bakens and Coolsen40). These findings collectively support the notion that body composition plays a pivotal role in shaping cancer prognosis and warrants deeper investigation in the context of personalised treatment approaches.
The present study yielded promising results regarding the association between adipose tissue radiodensity, desmoplasia and prognosis in CRC. Furthermore, while the findings underscore the significance of desmoplasia as a notable pathological alteration within the adipose tissue microenvironment, the underlying mechanisms and key factors driving desmoplasia formation remain inadequately understood. Nonetheless, our study is subject to certain limitations. First, as is typical of retrospective studies, data collection biases may be inherent. Additionally, the relatively small sample size in our study necessitates validation of our findings in a larger cohort. Therefore, further research is essential to better elucidate the identified associations.
Conclusion
The results suggest that a decrease in VATd, which reflects an increase in visceral fat content, may play a significant role in the pathogenesis of desmoplasia in CRC. This finding highlights the potential biological interaction between visceral fat accumulation and tumour progression. Moreover, higher levels of desmoplasia, but not VATd, were found to be associated with a marked reduction in survival rates over a 5-year follow-up period, underscoring the clinical relevance of desmoplastic response in predicting patient prognosis.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114525103784
Acknowledgements
We sincerely thank everyone involved in this research, especially the patients whose participation was crucial to advancing scientific knowledge.
This study was funded by Carlos Chagas Filho Foundation for Research Support of the State of Rio de Janeiro (E-26203·250/2017) and National Council for Scientific and Technological Development (CNPq) (312399/2020–0).
J. C. S. A., L. B. M. and W. A. F. P. designed the study. J. C. S. A., T. V. M., G. S. V. S., L. C. O., G. V. C. and L. B. M. collected and analysed the data. J. C. S. A., G. S. V. S., L. C. O., G. V. C., L. B. M. and W. A. F. P. prepared and drafted the manuscript. All authors read and approved the final manuscript.
The authors declare that there are no conflicts of interest.
This study was conducted in accordance with the guidelines outlined in the Declaration of Helsinki. All procedures involving human participants received approval from the Ethics and Research Committee of the Brazilian National Cancer Institute (protocol number: 00994818.4.0000.5274/2018), and written informed consent was obtained from all participants.