


1. Introduction
In addition to environmental impacts, a primary public concern about air pollution is its adverse effects on human health. An extensive body of epidemiological studies has found linkages between air pollution and health (Dockery and Pope, Reference Dockery and Pope1994; Pope and Dockery, Reference Pope and Dockery2006; Fisher et al., Reference Fisher, Bellinger, Cropper, Kumar, Binagwaho, Koudenoukpo, Park, Taghian and Landrigan2021; Fuller et al., Reference Fuller, Landrigan, Balakrishnan, Bathan, Bose-O'Reilly, Brauer, Caravanos, Chiles, Cohen, Corra and Cropper2022). Although the economics literature on the topic is relatively nascent, studies concur that air pollution is detrimental to human health (Chay and Greenstone, Reference Chay and Greenstone2003a, Reference Chay and Greenstone2003b; Currie and Neidell, Reference Currie and Neidell2005; Beatty and Shimshack, Reference Beatty and Shimshack2014; Deryugina et al., Reference Deryugina, Heutel, Miller, Molitor and Reif2019; Balietti et al., Reference Balietti, Datta and Veljanoska2022). Air pollution is associated with high incidences of respiratory and cardiovascular morbidity as well as premature mortality, even at low concentration levels (Currie and Neidell, Reference Currie and Neidell2005; Pope and Dockery, Reference Pope and Dockery2006). For example, studying the impact of the 1970 Clean Air Act in the US, Chay and Greenstone (Reference Chay and Greenstone2003b) find that a 1 per cent decrease in total suspended particles (TSP) translated into a 0.35 per cent decline in infant mortality. Deryugina et al. (Reference Deryugina, Heutel, Miller, Molitor and Reif2019) show that an increment of 1  $\mu $g/m3 PM2.5 concentration is associated with 0.69 additional deaths, 2.7 emergency room admissions and spending of over $16,000 per 1 million elderly population. Similarly, Kim (Reference Kim2021) estimates an increase in respiratory health care costs of $67 million and $70 million in South Korea due to an increase in PM10 (10
$\mu $g/m3 PM2.5 concentration is associated with 0.69 additional deaths, 2.7 emergency room admissions and spending of over $16,000 per 1 million elderly population. Similarly, Kim (Reference Kim2021) estimates an increase in respiratory health care costs of $67 million and $70 million in South Korea due to an increase in PM10 (10  $\mu $g/m3) and O3 (10 ppb), respectively. Recent studies have also found causal impacts of air pollution on obesity among adults and health growth deficiencies in children (Deschênes et al., Reference Deschênes, Wang, Wang and Zhang2020; Balietti et al., Reference Balietti, Datta and Veljanoska2022).
$\mu $g/m3) and O3 (10 ppb), respectively. Recent studies have also found causal impacts of air pollution on obesity among adults and health growth deficiencies in children (Deschênes et al., Reference Deschênes, Wang, Wang and Zhang2020; Balietti et al., Reference Balietti, Datta and Veljanoska2022).
As many places in the world are experiencing rapid growth, there is a growing concern about the health implications of air pollution, especially in areas with dense populations and substandard health infrastructures (Arceo et al., Reference Arceo, Hanna and Olivia2016; UN, 2018). Since health is an essential component of public welfare, understanding different aspects of the health impacts of air pollution becomes a requisite for designing policies to mitigate health damages. To this end, it is imperative to understand the distribution of health burden within the population and design policies to reduce pollution-led health inequity (Kopas et al., Reference Kopas, York, Jin, Harish, Kennedy, Shen and Urpelainen2020; Rao et al., Reference Rao, Kiesewetter, Min, Pachauri and Wagner2021).
A copious amount of studies from developed countries form much of our understanding of air pollution’s health impacts, especially ambient air pollution. The literature on the health impacts of air pollution in developing countries, although gradually expanding, is still scant to answer several important policy questions (Cropper et al., Reference Cropper, Simon, Alberini, Seema and Sharma1997; Duflo et al., Reference Duflo, Greenstone and Hanna2008; Jayachandran, Reference Jayachandran2009; Chen et al., Reference Chen, Ebenstein, Greenstone and Li2013). A major hindrance to studying the health impacts of air pollution in developing countries has been the unavailability (or limited amount) of relevant data (Arceo et al., Reference Arceo, Hanna and Olivia2016; Chen et al., Reference Chen, Guo and Huan2018; Barwick et al., Reference Barwick, Li, Lin and Zou2024). For instance, in Nepal, the Ministry of Population and Environment initiated air quality monitoring by installing six monitoring stations in the capital city of Kathmandu in 2002 but briefly discontinued the measurements in 2007, subsequently affecting air pollution research (Gurung and Bell, Reference Gurung and Bell2012; Mahapatra et al., Reference Mahapatra, Puppala, Adhikary, Shrestha, Dawadi, Paudel and Panday2019).
Given this limitation, one option is to extend results from studies already conducted elsewhere. However, estimates from developed countries may not coherently carry over to developing countries for several reasons. First, given that air pollution concentrations are usually much higher in developing countries, the results from the developed countries may not linearly extend (Cropper et al., Reference Cropper, Simon, Alberini, Seema and Sharma1997; Duflo et al., Reference Duflo, Greenstone and Hanna2008; Arceo et al., Reference Arceo, Hanna and Olivia2016; Chen et al., Reference Chen, Guo and Huan2018). For instance, Arceo et al. (Reference Arceo, Hanna and Olivia2016) compare the dose–response relationship between PM10 and CO and infant mortality in Mexico and the US and find a larger marginal effect of CO in Mexico. They emphasize that the estimates from developed countries may not extend linearly due to a non-linear dose–response relationship and differences in avoidance behaviour costs. Second, issues such as using biomass and traditional open fire stoves, significantly contributing to indoor air pollution, are more salient in developing countries (Duflo et al., Reference Duflo, Greenstone and Hanna2008; Rao et al., Reference Rao, Kiesewetter, Min, Pachauri and Wagner2021). Indoor air pollution accounts for 4.3 million global premature deaths, most occurring in Asian countries (WHO, 2014). Agricultural residue burning is another widespread practice typical of developing countries (Rupakheti et al., Reference Rupakheti, Adhikary, Praveen, Rupakheti, Kang, Mahata, Naja, Zhang, Panday and Lawrence2017; Saikawa et al., Reference Saikawa, Panday, Kang, Gautam, Zusman, Cong, Somanathan, Adhikary, Wester, Mishra, Mekherji and Shrestha2019). Third, given that socioeconomic composition, nutritional levels and access to health facilities widely differ in developing countries, results from developed countries may have limited external validity (Foster and Kumar, Reference Foster and Kumar2011).
Economic studies identify several methodological and estimation challenges in estimating the health impacts of air pollution, mainly due to the biases introduced by measurement error and potential confounders (Chay and Greenstone, Reference Chay and Greenstone2003a, Reference Chay and Greenstone2003b; Deryugina et al., Reference Deryugina, Heutel, Miller, Molitor and Reif2019). Since controlled experiments are not always feasible due to ethical considerations, studies typically rely on observational data (Beatty and Shimshack, Reference Beatty and Shimshack2014). An essential limitation of the aggregate observational data is that they are subject to selection bias and measurement error of exposure and health outcomes at the individual level, particularly in areas with sparse monitoring (Son et al., Reference Son, Bell and Lee2010; Graff Zivin and Neidell, Reference Graff Zivin and Neidell2013). Additionally, they do not provide enough information about individual characteristics, behavioural responses and exposure differences within the population. Several factors can determine personal exposure, making unbiased estimation of health challenging. For example, individuals who live or work close to air pollution sources have higher exposure (Anderson, Reference Anderson2019; Kopas et al., Reference Kopas, York, Jin, Harish, Kennedy, Shen and Urpelainen2020). Some occupations require individuals to spend more time outdoors, exposing them longer to ambient pollution (Foster and Kumar, Reference Foster and Kumar2011; Shakya et al., Reference Shakya, Rupakheti, Aryal and Peltier2016a). Surveys and health diaries are often used to extract individual health information (Evans and Smith, Reference Evans and Smith2005; Gupta, Reference Gupta2008). A definite advantage of surveys is that they allow researchers to obtain in-depth information about individual socioeconomic and behavioural characteristics, which could determine the exposure level. However, one limitation is that survey-based health responses likely suffer from self-reporting and recollection bias (Janke, Reference Janke2014).
Since air pollution exposure has health consequences, individuals have strong incentives to make coping choices to reduce health costs and maximize well-being. In the long run, individuals can choose to locate in areas with better air quality through ‘Tiebout sorting’ (Depro and Timmins, Reference Depro, Timmins and Banzhaf2012). In the short run, they can avoid exposure by restricting outdoor activities (Graff Zivin and Neidell, Reference Graff Zivin and Neidell2009; Ahmad et al., Reference Ahmad, Gibson, Nadeem, Nasim and Razaee2022; Barwick et al., Reference Barwick, Li, Lin and Zou2024), investing in self-protection measures like facemasks and air filters (Sun et al., Reference Sun, Kahn and Zheng2017; Zhang and Mu, Reference Zhang and Mu2018; Ito and Zhang, Reference Ito and Zhang2020), and changing their mode of transportation (Saberian et al., Reference Saberian, Heyes and Rivers2017). When individuals exhibit behavioural responses, the air pollution level does not accurately measure exposure (Neidell, Reference Neidell2009; Janke, Reference Janke2014; Kim, Reference Kim2021).
Although exposure avoidance has received attention in recent studies, the critical question of whether exposure avoidance translates into health gains is still open for more exploration. Empirical evidence thus far shows that the impact of avoidance behaviours may not be trivial. Neidell (Reference Neidell2009) and Janke (Reference Janke2014) find that pollution warnings, a proxy for avoidance, significantly reduce asthma hospitalization. Although Sun et al. (Reference Sun, Kahn and Zheng2017) do not estimate the health effects of air filters and facemasks, they report that on average, individuals who use facemasks or air filters reduce their PM2.5 exposure by 33 and 92 per cent, respectively. In a cohort study of traffic police in Kathmandu, Nepal, Shakya et al. (Reference Shakya, Rupakheti, Aryal and Peltier2016a) found that traffic police who wore N95 facemasks for three workdays showed improved lung function. A randomized field study conducted in China finds that using facemasks reduces air pollution-related doctor visits by 80 per cent (Chen et al., Reference Chen, Gong and Zhao2024).
This study focuses on Siddharthanagar municipality of Nepal, a growing urban town in the northern edge of the Indo-Gangetic Plain. The municipality is home to 18,763 households with diverse socioeconomic backgrounds (Siddharthanagar Municipality, Nepal, 2019; Khatiwada and Bohara, Reference Khatiwada and Bohara2026). It is on the Nepal side of the second busiest Nepal-India border of Sunauli and a gateway to the world heritage site of Lumbini, the birthplace of the founder of Buddhism, Gautam Buddha. With the completion of the Gautam Buddha International Airport in sight, the municipality is expected to experience further urban growth. The rapid expansion has posed a severe threat to the environment, especially air quality. An air quality measurement study conducted in Lumbini found the air quality in the region to be poor, with the average hourly PM2.5 and PM10 levels of 53.1 ± 35.1  $\mu $g/m3 and 128.9 ± 91.9
$\mu $g/m3 and 128.9 ± 91.9  $\mu $g/m3 respectively, which not only exceed the WHO guidelines (25 and 50
$\mu $g/m3 respectively, which not only exceed the WHO guidelines (25 and 50  $\mu $g/m3) but also the Nepalese standards (40 and 120
$\mu $g/m3) but also the Nepalese standards (40 and 120  $\mu $g/m3) (Rupakheti et al., Reference Rupakheti, Adhikary, Praveen, Rupakheti, Kang, Mahata, Naja, Zhang, Panday and Lawrence2017). Air pollution concentration over the region is affected by the emissions from local industries, mainly from cement and brick factories, domestic biomass burning, crop residue burning and transboundary air pollution from the nearby regions (Rupakheti et al., Reference Rupakheti, Adhikary, Praveen, Rupakheti, Kang, Mahata, Naja, Zhang, Panday and Lawrence2017; Saikawa et al., Reference Saikawa, Panday, Kang, Gautam, Zusman, Cong, Somanathan, Adhikary, Wester, Mishra, Mekherji and Shrestha2019). The deteriorating air quality has placed a burden on public health and welfare. However, in the absence of comprehensive studies, little is known about the extent of the air pollution-related health problems in the municipality.
$\mu $g/m3) (Rupakheti et al., Reference Rupakheti, Adhikary, Praveen, Rupakheti, Kang, Mahata, Naja, Zhang, Panday and Lawrence2017). Air pollution concentration over the region is affected by the emissions from local industries, mainly from cement and brick factories, domestic biomass burning, crop residue burning and transboundary air pollution from the nearby regions (Rupakheti et al., Reference Rupakheti, Adhikary, Praveen, Rupakheti, Kang, Mahata, Naja, Zhang, Panday and Lawrence2017; Saikawa et al., Reference Saikawa, Panday, Kang, Gautam, Zusman, Cong, Somanathan, Adhikary, Wester, Mishra, Mekherji and Shrestha2019). The deteriorating air quality has placed a burden on public health and welfare. However, in the absence of comprehensive studies, little is known about the extent of the air pollution-related health problems in the municipality.
The objectives of this study are twofold. We examine the role of individuals’ exposure to air pollution based on occupation and proximity to local pollution sources on lung function – a biomarker of respiratory health. Second, we investigate the factors influencing exposure avoidance and whether exposure avoidance positively correlates with improved lung function. We consider exposure avoidance through three types of exposure avoidance measures: facemasks, clean cooking stoves and air filters. We employ a simultaneous equation regression model to account for the endogenous choice of exposure avoidance. Further, we use a spatial error regression model to control for the likely spatial spillover of health outcomes. We find that individuals who work outdoors (farmers and daily wage labourers) and reside near brick kilns have lower lung function. Exposure avoidance positively correlates with lung function. However, exposure avoidance is considerably lower among the more exposed outdoor workers and individuals living in polluted areas, further widening the exposure gap.
This study makes several contributions. First, it is among a limited number of economic studies that use a representative sample and direct measures of health to examine individual air pollution exposure and differences across socioeconomic subgroups. Second, this study is among a finite number of studies investigating the process behind the choice of exposure avoidance, the level of exposure and health. Third, this study adds to the current discussion on environmental inequity based on socioeconomic position by identifying exposure avoidance as a mechanism for exposure differential among socioeconomic subgroups.
2. Literature review
Studies conducted in both developed and developing countries find an association between air pollution and health damages (Cropper et al., Reference Cropper, Simon, Alberini, Seema and Sharma1997; Chay and Greenstone, Reference Chay and Greenstone2003a, Reference Chay and Greenstone2003b; Currie and Neidell, Reference Currie and Neidell2005; Ebenstein et al., Reference Ebenstein, Fan, Greenstone, He, Yin and Zhou2015). Economic studies have been able to contribute to the literature by offering new empirical approaches to control for potential confounders and establish causal linkages between air pollution and health outcomes (Chay and Greenstone, Reference Chay and Greenstone2003a, Reference Chay and Greenstone2003b; Currie and Neidell, Reference Currie and Neidell2005; Beatty and Shimshack, Reference Beatty and Shimshack2014; Deryugina et al., Reference Deryugina, Heutel, Miller, Molitor and Reif2019; Balietti et al., Reference Balietti, Datta and Veljanoska2022).
Several noted studies have exploited natural experiments and policy-induced quasi-experiments to isolate exogenous variation in air pollution. A notable case of a natural experiment is the 1997 Indonesian forest fire that affected several areas of Indonesia and nearby regions. Jayachandran (Reference Jayachandran2009) examined the effect of the wildfire on Indonesian fetal, infant and child mortality rates and found that wildfire-induced air pollution was responsible for 15,600 deaths. Chay and Greenstone exploit variation in TSP concentrations across US counties due to the 1980–1982 economic recession (Chay and Greenstone, Reference Chay and Greenstone2003a) and the 1970 Clean Air Act Amendments (Chay and Greenstone, Reference Chay and Greenstone2003b) and find an association between a decline in TSP concentrations and reduction in infant mortality rates. Chen et al. (Reference Chen, Ebenstein, Greenstone and Li2013) use an inadvertently created quasi-experimental setup of China’s Huai River policy of distributing free coal for winter heating in Northern China and find a linkage between the increase in TSP concentrations and decline in life expectancies in the north.
In the absence of policy instruments, studies have often relied on time-invariant fixed-effects and instrumental variable (IV) estimation approaches to control for confounding issues. For example, Currie and Neidell (Reference Currie and Neidell2005) use a rich set of controls for the weather, mothers’ and children’s characteristics, and month, year and zip code fixed effects to examine linkages between CO and PM10 concentrations and infant mortality in California. Studies that have utilized the IV approach have used various instruments. Arceo et al. (Reference Arceo, Hanna and Olivia2016) use temperature inversion, an atmospheric condition where pollutants get trapped above a layer of cold air, to isolate exogenous variation in PM10 and CO in Mexico. Deryugina et al. (Reference Deryugina, Heutel, Miller, Molitor and Reif2019) use wind direction as an instrument for variation in PM2.5 and find significant effects of particulate matter on mortality, hospitalization and medical costs in the elderly population. Kim (Reference Kim2021) gathers data on historical trends in air pollution and takes the average pollution concentration by date as an instrument.
An essential limitation of using aggregate observational data to understand the linkages between air pollution and health is that exposure and health impacts are not observed at an individual level, adding challenges to the estimation of the health impacts. Several studies have examined the association between exposure and health outcomes based on proximity to pollution sources (Brender et al., Reference Brender, Maantay and Chakraborty2011; Anderson, Reference Anderson2019) and occupation (Gurung and Bell, Reference Gurung and Bell2012; Shakya et al., Reference Shakya, Rupakheti, Aryal and Peltier2016a). The impact of individual exposure to air pollution on direct health measures in a representative sample has received little attention in the economics literature (Foster and Kumar, Reference Foster and Kumar2011). An existing relevant study by Foster and Kumar (Reference Foster and Kumar2011) uses spirometry data of a sample of 1,576 households from Delhi, India, to examine the impact of Supreme Court-mandated vehicular and industrial emissions control policy on residents’ lung function using the IV approach. The mandated policy is used as an instrument for PM2.5 variation. The study finds an overall improvement in lung function due to policy-led air quality improvement, with considerable improvement in individuals from the poorest households.
Air pollution avoidance behaviours are gaining attention in recent economic literature. Studies find evidence of public avoidance behaviours in response to air pollution. For instance, Graff Zivin and Neidell (Reference Graff Zivin and Neidell2009) find that following smog alerts on television and radio, issued when the O3 concentrations in the air exceed 200 PSI (pollution standard index), attendance at the Los Angeles Zoo and Griffith Park Observatory in Southern California was significantly lower. Another study in Sydney, Australia, shows a significant decrease in cycle use following air pollution alerts (Saberian et al., Reference Saberian, Heyes and Rivers2017). Sun et al. (Reference Sun, Kahn and Zheng2017) find that the public living in urban China respond to a rise in the PM2.5 level by purchasing facemasks and air filters. A study by Ito and Zhang (Reference Ito and Zhang2020) also finds increased demand for air purifiers in response to air pollution resulting from the Huai River policy of free coal distribution for heating in Northern China. Lu et al. (Reference Lu, Chen and Cai2023) show that environmental regulation in China, through higher air quality monitoring operations leading to local air quality improvement, decreases health insurance purchases and claims. Barwick et al. (Reference Barwick, Li, Lin and Zou2024) also report higher public avoidance behaviours following increased air quality monitoring and real-time information dissemination.
Neidell (Reference Neidell2009) and Janke (Reference Janke2014) underscore that past studies that have examined the health effects of air pollution have undermined avoidance behaviours; therefore, estimates are likely to have a downward bias. Taking pollution alerts as a proxy measure for restriction on outdoor activities, Neidell (Reference Neidell2009) shows that the effects of O3 in California were much larger on children's asthma hospitalization when controlling for avoidance behaviours. Janke (Reference Janke2014) also finds that air pollution alerts reduce asthma hospitalization in the UK. The study, however, does not see a significant downward bias of the effects of NO2 and O3 on asthma hospitalization when not controlling for the alerts. A recent study by Kim (Reference Kim2021) shows that the estimate of the impact of PM10 on hospital admissions in South Korea can be three times larger when controlling for pollution alerts. Chen et al. (Reference Chen, Gong and Zhao2024) conducted a randomized field study in China on 2,296 participants to evaluate the efficiency of facemasks. They found that while facemasks led participants to spend more time outdoors, potentially increasing exposure risk, their use led to an overall reduction in doctor visits by 80 per cent.
In the context of developing countries, numerous studies have focused on indoor air pollution and shed some light on the positive impact of cleaner cooking technologies (and fuels) on indoor pollution and respiratory health. For example, two randomized controlled trials from Guatemala find that women and children from treatment households that used improved cooking stoves had fewer chronic respiratory symptoms and improved lung function (Smith-Siverten et al., Reference Smith-Siverten, Diaz, Pope, Lie, Díaz, McCracken, Bakke, Arana, Smith and Bruce2009; Smith et al., Reference Smith, McCracken, Weber, Hubbard, Jenny, Thompson, Balmes, Diaz, Arana and Bruce2011). Since these studies involve random assignment of cooking technology, they do not provide information about the factors influencing individuals’ choice of such technology. Stabridis and van Gameren (Reference Stabridis and van Gameren2018) use data from the 2002 Mexican Family Life Survey to study the impact of the endogenous choice of firewood and liquefied petroleum gas (LPG) consumption on health and labour force participation. The study finds that women from households that use firewood are more likely to have respiratory problems and lower labour force participation than those who use LPG. The evidence on the linkages between the endogenous choice of exposure avoidance, the level of air pollution exposure and health outcomes is still limited and warrants further exploration.
3. Theoretical framework
We analyse our objectives using a theoretical framework derived from the Becker-Grossman health production function model, a seminal framework for understanding the economics of health (Becker, Reference Becker1965; Grossman, Reference Grossman1972). The central notion of the model is that health provides utility to individuals and that health at a given time depends on past health inputs. Following Freeman et al. (Reference Freeman, Herringes and Kling2014) and Deschênes et al. (Reference Deschênes, Greenstone and Shapiro2017), we consider health production ( $H$) as a function of individual air pollution exposure (
$H$) as a function of individual air pollution exposure ( $E$) and exposure avoidance (
$E$) and exposure avoidance ( $A$). The model implies that given a level of air pollution, individuals make coping choices to maximize their utility through health production.
$A$). The model implies that given a level of air pollution, individuals make coping choices to maximize their utility through health production.
 \begin{equation}H = H\!\left( {E,{ }A} \right)\end{equation}
\begin{equation}H = H\!\left( {E,{ }A} \right)\end{equation} In the following utility maximization model, individuals gain utility  $(U\!\left( {H,\,X,\,L;C} \right)$ from having good health (
$(U\!\left( {H,\,X,\,L;C} \right)$ from having good health ( $H$), consumption of goods and services (
$H$), consumption of goods and services ( $X$) and leisure (
$X$) and leisure ( $L$), given a set of individual (and household) characteristics (
$L$), given a set of individual (and household) characteristics ( $C$). The given utility function is subject to a budget constraint, as given by
$C$). The given utility function is subject to a budget constraint, as given by  ${p_A}A + X \leq I + {p_w}\left( {T - L} \right)$, where I represents non-labour income, T represents total available time, and
${p_A}A + X \leq I + {p_w}\left( {T - L} \right)$, where I represents non-labour income, T represents total available time, and  ${p_A}$ and
${p_A}$ and  ${p_w}$ are the prices of exposure avoidance and wage rate respectively. The price of
${p_w}$ are the prices of exposure avoidance and wage rate respectively. The price of  $X$ is normalized to 1. For modelling simplicity, we limit our model to air pollution-related health production.
$X$ is normalized to 1. For modelling simplicity, we limit our model to air pollution-related health production.
 \begin{equation}U(H,\,X,\,L;\,C)\,\,subject\,to\,\,{p_A}A + X \leq I + \,{p_w}(T - L)\end{equation}
\begin{equation}U(H,\,X,\,L;\,C)\,\,subject\,to\,\,{p_A}A + X \leq I + \,{p_w}(T - L)\end{equation} Now, assuming an interior solution, we can express the utility maximation problem in the following Lagrangian form, where  $\lambda$ is the Lagrangian multiplier:
$\lambda$ is the Lagrangian multiplier:
 \begin{equation}
\text{max}_{\left\{ {A,X,L} \right\}}\mathcal{L} = U(H,\,X,\,L;\,C)\, +\, \lambda \left[ {I + \,{p_w}(T - L)-X-{p_A}A} \right]
\end{equation}
\begin{equation}
\text{max}_{\left\{ {A,X,L} \right\}}\mathcal{L} = U(H,\,X,\,L;\,C)\, +\, \lambda \left[ {I + \,{p_w}(T - L)-X-{p_A}A} \right]
\end{equation}By solving the utility maximization problem, we can derive the demand function of exposure avoidance. Exposure avoidance is expressed as a function of exposure, income, and prices, given a set of individual characteristics (Freeman et al., Reference Freeman, Herringes and Kling2014):
 \begin{equation}A = A(E,I,{ }{p_A},{ }{p_w};C)\end{equation}
\begin{equation}A = A(E,I,{ }{p_A},{ }{p_w};C)\end{equation} Similarly, the partial derivative of  $H$ with respect to
$H$ with respect to  $E$ can be expressed as follows, where the partial derivative of health with respect to exposure equals the total derivative of health with respect to exposure minus the product of the partial effect of avoidance behaviour on health and the partial effect of exposure on avoidance:
$E$ can be expressed as follows, where the partial derivative of health with respect to exposure equals the total derivative of health with respect to exposure minus the product of the partial effect of avoidance behaviour on health and the partial effect of exposure on avoidance:
 \begin{equation}\frac{{\partial H}}{{\partial E}} = \frac{{dH}}{{dE}} - \left( {\frac{{\partial H}}{{\partial A}}\frac{{\partial A}}{{\partial E}}} \right) \cdot \end{equation}
\begin{equation}\frac{{\partial H}}{{\partial E}} = \frac{{dH}}{{dE}} - \left( {\frac{{\partial H}}{{\partial A}}\frac{{\partial A}}{{\partial E}}} \right) \cdot \end{equation}The expression within the parentheses, which represents the intermediary role of avoidance, is overlooked in most empirical studies. Hence, the partial (biological) effect of exposure on health is inferred from the total derivative, which likely yields biased estimates. In this study, we internalize exposure avoidance behaviours. We assume a positive sign on the partial derivative of health with respect to exposure avoidance. We expect individuals to make behavioural adjustments to maximize their utility through health production. Although the partial effect of exposure on avoidance behaviour is typically assumed to be positive (Deschênes et al., Reference Deschênes, Greenstone and Shapiro2017), we do not make this a priori assumption. We posit that if there is large heterogeneity in exposure and exposure avoidance within the population based on socioeconomic position, exposure avoidance could be low among the more exposed subgroups. In such a case, the relative partial effect of exposure on avoidance would be negative, and the health effect would be overestimated. We model and test these hypotheses in the empirical section.
4. Data and key variables
The data comes from a primary household survey conducted in Siddharthanagar municipality of Nepal. The survey was conducted in the summer (June–July) of 2019 on a sample of 610 randomly selected households from all 13 wards. The survey respondents from each household were 18 years and above. This study focuses on the association between individual exposure to air pollution and respiratory health. Past studies have proposed several methods to measure individual exposure. One is individual air quality monitoring to assess individual exposure. Individual monitoring, however, is costly, labour-intensive and not always feasible to execute in a relatively large sample for an extended period (Son et al., Reference Son, Bell and Lee2010; Graff Zivin and Neidell, Reference Graff Zivin and Neidell2013). Another proposed method is to use data from several monitoring stations and interpolate the data to finely capture air pollution variation across space (Son et al., Reference Son, Bell and Lee2010). Studies have also utilized remote sensing satellite data to assess air quality (Balietti et al., Reference Balietti, Datta and Veljanoska2022; Barwick et al., Reference Barwick, Li, Lin and Zou2024). However, at the time of this study, there were no air quality monitoring stations in the municipality. There was also a lack of high-resolution remote sensing data – ideally with a resolution of 1 km × 1 km – necessary to accurately capture the air quality variation within the study area. Therefore, we rely on three proxies for individual exposure: occupational exposure, residential proximity to the brick kilns and nearest major roads.
Table A1 (online appendix) presents detailed descriptive statistics of the variables used in the study. The survey included questions about both individual and household characteristics. The individual part included lung function measurement, occupation, smoking behaviour, sex and age. Household information included residential location (longitude and latitude), duration of residence, use of avoidance measures, household wealth, education of the household head, air quality perception and awareness about the health impacts of air pollution. We created a composite index of household wealth that includes 18 household assets, such as cell phones, fans, radios, televisions and motorcycles, and divided households into five wealth quintiles.
4.1. Lung function
Spirometry tests were conducted on respondents from 305 randomly chosen households (final sample) to assess their lung function. We used portable spirometer devices (EasyOne Spirometer Model 2000) for the tests. Lung function is a sensitive measure of respiratory health in response to different air pollutants, such as particulate matter and O3, and is commonly used in epidemiological studies (Dockery and Pope, Reference Dockery and Pope1994; Bellia et al., Reference Bellia, Pistelli, Giannini, Scichilone, Catalano, Spatafora, Hopps, Carrozzi, Baldacci, Di Pede, Paggiaro and Viegi2003; Paulin and Hansel, Reference Paulin and Hansel2016). An advantage of spirometry tests is that they can objectively measure the variations in respiratory health within the representative sample and help eliminate the likely self-reporting and recollection bias associated with survey-based health responses and selection bias in hospital data (Janke, Reference Janke2014; Kim, Reference Kim2021).
We gathered data on two indicators of lung function: forced vital capacity (FVC) and forced expiratory volume in 1 second (FEV1). FVC measures the total amount of exhaled air, and FEV1 measures the amount of air exhaled in the first 1 second. The ratio of FEV1 to FVC provides information about respiratory obstruction – the ratio is lower among individuals with obstructive lung conditions. The spirometer device also calculated the percentage of predicted normal values of FVC and FEV1, accounting for an individual’s sex, age, height and smoking habit, which we entered in the device before taking the measurements. To ensure data quality, we only retained data from a session quality of ‘A’ or ‘B’ reported in the device (Shakya et al., Reference Shakya, Rupakheti, Aryal and Peltier2016a). Additionally, we only conducted spirometry tests in the morning (between 9 a.m. and 12 p.m.) to reduce any influence of diurnal variations in air pollution on the test results.
Following Foster and Kumar (Reference Foster and Kumar2011), we use the FEV1/FVC ratio as our health outcome variable in regression analyses. The FEV1/FVC ratio is a continuous variable with a mean value of 0.76 and a standard deviation of 0.14.Footnote 1 The mean value is comparable to other past studies from the region. Foster and Kumar (Reference Foster and Kumar2011) report a mean of 0.70 in a representative sample from Delhi, India. Gurung and Bell (Reference Gurung and Bell2012) report mean values of 0.80 for traffic police and indoor office workers in Kathmandu, Nepal. The respondents were also asked if they had air pollution-related illness symptoms, such as coughing, eyes, nose, and throat irritation, during the 30 days before the survey. The FEV1/FVC ratio is consistent with the self-reported illness symptoms – the mean for those with no symptom (0.77) was higher than those with at least one (0.74) and two or more symptoms (0.73) (online appendix Figure A2). A T-test confirms significant differences (at the 5 per cent level) between the means of those with no symptoms and those with one or more symptoms.
4.2. Occupation and residential location
For exposure based on occupation, we consider two occupation groups required to work outdoors for an extended number of hours: farmers and daily wage labourers. We consider the time spent outdoors as an indicator of the amount of exposure to ambient air pollution. The data shows that 14.4 per cent of the respondents are farmers or daily wage labourers.Footnote 2 As many as 40 per cent reported that they remain outdoors for more than 6 hours, and 66 per cent remain outdoors for more than 3 hours (appendix Figure A3). In comparison, only 22 per cent of respondents in other occupations spend 6 hours outdoors, and 47 per cent remain outdoors for more than 3 hours. A Chi-squared test confirms that farmers and labourers spend significantly more time outdoors than the comparison group at the 1 per cent significance level. Preliminary analysis shows that the subgroup has a lower lung function (mean FEV1/FVC ratio of 0.70) as compared to the comparison group (0.77) (appendix Figure A4).
We consider proximity to the brick kilns and distance to the nearest major road for exposure based on residential location. We use secondary ward-level data on the brick kiln provided by the Ministry of Urban Development of Nepal in 2017. The proximity to the brick kilns indicates whether a household lives in a ward with brick kilns. Brick kilns are present in wards 1 and 4 of the municipality, and 19.5 per cent of the sample live there. We calculated the distance to road variable by georeferencing the major roads in the municipality, taking longitude and latitude data of the surveyed households, and calculating the distance to the nearest major road using the ArcGIS 10.7.1 software. Major roads are defined using the municipality’s road map for 2017.
4.3. Air pollution exposure avoidance
Individuals can limit their air pollution exposure through avoidance measures. Exposure avoidance can create ‘a wedge between potential and realized exposure’ (Graff Zivin and Neidell, Reference Graff Zivin and Neidell2013). We consider exposure avoidance through two types of self-protection – facemasks and air filters – and one type of pollution prevention measures – clean cooking stoves.Footnote 3 While individuals can invest in facemasks to protect themselves against outdoor air pollution, clean cooking stoves and air filters can help reduce indoor air pollution. The use of facemasks for self-protection is increasing in developing countries, especially in urban areas, since they are cheaper and accessible (Zhang and Mu, Reference Zhang and Mu2018; Ahmad et al., Reference Ahmad, Gibson, Nadeem, Nasim and Razaee2022). Despite being relatively expensive, studies have also shown public demand for air filters (Sun et al., Reference Sun, Kahn and Zheng2017; Ito and Zhang, Reference Ito and Zhang2020). The contributions of traditional cooking stoves and solid fuels to indoor pollution in developing countries are well known in the literature (Duflo et al., Reference Duflo, Greenstone and Hanna2008; Pattanayak et al., Reference Pattanayak, Jeuland, Lewis, Usmani, Brooks, Bhojvaid, Kar, Lipinski, Morrison, Patange, Ramanathan, Rehman, Thadani, Vora and Ramanathan2019; Balietti et al., Reference Balietti, Datta and Veljanoska2022).
We generate an index for the avoidance measures,Footnote 4 ranging from 0 to 2, by adding them, where 0 means no measure, 1 means at least one measure, and 2 means two or more measures.Footnote 5 Individuals can also reduce their exposure by restricting outdoor activities (Neidell, Reference Neidell2009, Graff Zivin and Neidell, Reference Graff Zivin and Neidell2009) and changing their mode of transportation (Saberian et al., Reference Saberian, Heyes and Rivers2017). However, we limit our investigation to the use of avoidance measures. Nearly one-third of the households (32.8 per cent) do not use any measure, while 45.2 per cent reported using one, and 22.0 per cent reported using two or more measures. Investment in air filters is extremely low (1.6 per cent). The percentage of the sample using avoidance measures is comparable to those found in Bresnahan et al. (Reference Bresnahan, Dickie and Gerking1997) and Ullah et al. (Reference Ullah, Ullah, Rajper, Ahmad and Li2021). Preliminary analysis suggests a positive correlation between exposure avoidance and lung function. The mean FEV1/FVC ratio increases with the number of measures – the mean for no measure, one measure and two or more measures are 0.72, 0.76 and 0.81, respectively.
5. Empirical strategy
5.1. Simultaneous equations model
We estimate the health outcome using the following two-equation system that allows for a non-zero contemporaneous correlation across the equations.
Health outcome equation:
 \begin{equation}
Lung\,Function_{i} = \beta_{0} + \beta_{1}\,\,Avoid_{i} + \beta_{2}\,\,Occupation_{i} + \beta_{3}\,\,Residence_{i} + \delta X_{i} + u_{i}
\end{equation}
\begin{equation}
Lung\,Function_{i} = \beta_{0} + \beta_{1}\,\,Avoid_{i} + \beta_{2}\,\,Occupation_{i} + \beta_{3}\,\,Residence_{i} + \delta X_{i} + u_{i}
\end{equation}Exposure avoidance decision equation:
 \begin{equation}
\begin{gathered}
Avoid_{i} = \alpha_{0} + \alpha_{1}\,Perception_{i} + \alpha_{2}\,Awareness_{i} + \alpha_{3}\,Occupation_{i} \\
+\,\,\alpha_{4}\,Residence_{i} + \theta\,X_{i} + v_{i}
\end{gathered}
\end{equation}
\begin{equation}
\begin{gathered}
Avoid_{i} = \alpha_{0} + \alpha_{1}\,Perception_{i} + \alpha_{2}\,Awareness_{i} + \alpha_{3}\,Occupation_{i} \\
+\,\,\alpha_{4}\,Residence_{i} + \theta\,X_{i} + v_{i}
\end{gathered}
\end{equation}where  $Cov\!\left({{u_i},{ }{v_i}} \right) \ne 0$ and
$Cov\!\left({{u_i},{ }{v_i}} \right) \ne 0$ and  $\varepsilon = [{u_i},\,{v_i}]{\sim} {\textrm N}\left( {0,\,\,{\Sigma}} \right),$ where
$\varepsilon = [{u_i},\,{v_i}]{\sim} {\textrm N}\left( {0,\,\,{\Sigma}} \right),$ where  $\mathop \sum = \left[ {\begin{array}{*{20}{c}}
{\sigma_1^2}&{{\sigma_{12}}} \\
{{\sigma_{21}}}&{\sigma_2^2}
\end{array}} \right]$.
$\mathop \sum = \left[ {\begin{array}{*{20}{c}}
{\sigma_1^2}&{{\sigma_{12}}} \\
{{\sigma_{21}}}&{\sigma_2^2}
\end{array}} \right]$.
The health outcome variable in Equation (6),  $Lung\,Fun{c_i},$ represents an individual’s FEV1/FVC ratio, and it is a continuous variable. We specify
$Lung\,Fun{c_i},$ represents an individual’s FEV1/FVC ratio, and it is a continuous variable. We specify  $Lung\,Fun{c_i}$ as a function of individual’s exposure to air pollution based on occupation (
$Lung\,Fun{c_i}$ as a function of individual’s exposure to air pollution based on occupation ( $Occupatio{n_i}$) and residential location (
$Occupatio{n_i}$) and residential location ( $Residenc{e_i}$), individual’s (and household’s) response to air pollution to reduce exposure
$Residenc{e_i}$), individual’s (and household’s) response to air pollution to reduce exposure  $(Avoi{d_i})$, and other socioeconomic and behavioural controls
$(Avoi{d_i})$, and other socioeconomic and behavioural controls  $({X_i})$ – duration of residence, smoking behaviour, sex, age, education of the household head and household wealth.
$({X_i})$ – duration of residence, smoking behaviour, sex, age, education of the household head and household wealth.
The endogenously determined exposure avoidance is a categorical variable, ranging from 0 to 2. Equation (7) presents the determinants of exposure avoidance. Our identifying assumption is that perception of air quality near where the individuals live ( $Perceptio{n_i})\,$and the awareness that air pollution causes illness (
$Perceptio{n_i})\,$and the awareness that air pollution causes illness ( $Awarenes{s_i})$, along with exposure and other socioeconomic and behavioural traits
$Awarenes{s_i})$, along with exposure and other socioeconomic and behavioural traits  $({X_i})$, influence individuals to avoid air pollution exposure, which translates into positive health outcomes. Therefore, air quality perception and awareness about air pollution’s health impacts enter the health production function through exposure avoidance.
$({X_i})$, influence individuals to avoid air pollution exposure, which translates into positive health outcomes. Therefore, air quality perception and awareness about air pollution’s health impacts enter the health production function through exposure avoidance.
We simultaneously estimate the mixed-process systemFootnote 6 using the maximum likelihood estimation method, assuming a multivariate normal distribution for the error terms (Roodman, Reference Roodman2011). We expect a positive correlation between lung function and exposure avoidance  $({\beta_1} \gt 0)$ as individuals can reduce their exposure level by using avoidance measures. Similarly, we expect lower function among outdoor workers exposed to ambient air pollution for an extended period. Two variables that capture residential exposure include proximity to the brick kilns and distance to the nearest road. Given that individuals living closer to local pollution sources are more likely to have higher exposure, we expect the coefficient on proximity to the brick kilns to be negative and distance to the nearest road to be positive – lung capacity improves as the distance to the road increases.
$({\beta_1} \gt 0)$ as individuals can reduce their exposure level by using avoidance measures. Similarly, we expect lower function among outdoor workers exposed to ambient air pollution for an extended period. Two variables that capture residential exposure include proximity to the brick kilns and distance to the nearest road. Given that individuals living closer to local pollution sources are more likely to have higher exposure, we expect the coefficient on proximity to the brick kilns to be negative and distance to the nearest road to be positive – lung capacity improves as the distance to the road increases.
5.2. Spatial analyses
5.2.1. Identification of spatial patterns
Given that air pollution exposure is likely to be correlated across space, estimates of health outcomes are likely to be influenced by the presence of this spatial autocorrelation. Jerrett et al. (Reference Jerrett, Burnett, Kanaroglou, Eyles, Finkelstein, Giovis and Brook2001) and Goodman et al. (Reference Goodman, Wilkinson, Stafford and Tonne2011) show that the estimates of air pollution exposure can be biased without accounting for the spatial dependence. We utilize several spatial techniques to detect and control for the spatial dependence of the health outcome. We first identify the spatial patterns of the FEV1/FVC ratio and the main independent variables using two statistical approaches: Moran’s I and Getis-Ord ( $G_i^*$). Understanding the spatial distribution of exposure and health outcomes is helpful in identifying regions highly affected by pollution. The Moran’s I test is used to examine the global spatial autocorrelation of the variables (Moran, Reference Moran1950). The test provides a broad indication of whether values of the variables are similar for the nearby features across the spatial location. The Getis-Ord (
$G_i^*$). Understanding the spatial distribution of exposure and health outcomes is helpful in identifying regions highly affected by pollution. The Moran’s I test is used to examine the global spatial autocorrelation of the variables (Moran, Reference Moran1950). The test provides a broad indication of whether values of the variables are similar for the nearby features across the spatial location. The Getis-Ord ( $G_i^*$) statistic, a commonly used LISA (Local Indicators of Spatial Association), is used to identify local spatial clusters of hot and cold spots (Getis and Ord, Reference Getis and Ord1992; Ord and Getis, Reference Ord and Getis1995). The
$G_i^*$) statistic, a commonly used LISA (Local Indicators of Spatial Association), is used to identify local spatial clusters of hot and cold spots (Getis and Ord, Reference Getis and Ord1992; Ord and Getis, Reference Ord and Getis1995). The  $G_i^*$ statistic is calculated by
$G_i^*$ statistic is calculated by
 \begin{equation}G_i^* = \frac{{\mathop\sum_{j = 1}^n {w_{ij}}{x_j} - \mathop\sum_{j = 1}^n ({w_{ij}})\bar X}}{{{{\hat \sigma }_x}\sqrt {\frac{{\mathop\sum_{j = 1}^n w_{ij}^2\, - \,{{(\mathop\sum_{j = 1}^n {w_{ij}})}^2}}}{{n - 1}}} }},\end{equation}
\begin{equation}G_i^* = \frac{{\mathop\sum_{j = 1}^n {w_{ij}}{x_j} - \mathop\sum_{j = 1}^n ({w_{ij}})\bar X}}{{{{\hat \sigma }_x}\sqrt {\frac{{\mathop\sum_{j = 1}^n w_{ij}^2\, - \,{{(\mathop\sum_{j = 1}^n {w_{ij}})}^2}}}{{n - 1}}} }},\end{equation}where  ${w_{ij}}$ represents the spatial weight between feature
${w_{ij}}$ represents the spatial weight between feature  $i$ and
$i$ and  $j$;
$j$;  ${x_j}$ represents individual value for feature
${x_j}$ represents individual value for feature  $j$;
$j$;  $\bar X$ represents sample mean; and
$\bar X$ represents sample mean; and  ${\hat \sigma_x}$ represent sample standard deviation. We use the values obtained from
${\hat \sigma_x}$ represent sample standard deviation. We use the values obtained from  $G_i^*$ statistics (given as Z-scores) to visually identify clusters of significantly high and low values of the variables of interest. Further, we use the discrete values obtained from
$G_i^*$ statistics (given as Z-scores) to visually identify clusters of significantly high and low values of the variables of interest. Further, we use the discrete values obtained from  $G_i^*\,$statistics for Kriging interpolation of unknown values across the study area.
$G_i^*\,$statistics for Kriging interpolation of unknown values across the study area.
5.3. Spatial error model with endogeneity
We then employ a spatial error regression modelFootnote 7 to control for the likely spatial dependence while estimating the health outcomes (Drukker et al., Reference Drukker, Egger and Prucha2013). The choice of a spatial error model, instead of a spatial dependent variable lag model, stems from our postulation that the outcome variable in spatial location ( $i$) is not directly affected by the outcome variable in location (
$i$) is not directly affected by the outcome variable in location ( $j$) – the spatial dependence exists through the interaction of the error terms (Anselin, Reference Anselin1988).
$j$) – the spatial dependence exists through the interaction of the error terms (Anselin, Reference Anselin1988).
Health outcome equation (with spatially autocorrelated error term):
 \begin{equation}
Lung\,{Function}_{i} = \gamma_{0} + \gamma_{1}\,{Avoid}_{i} + \gamma_{2}\,{Occupation}_{i} + \gamma\,{Residence}_{i} + \lambda\,\,X_{i} + e_{i}
\end{equation}
\begin{equation}
Lung\,{Function}_{i} = \gamma_{0} + \gamma_{1}\,{Avoid}_{i} + \gamma_{2}\,{Occupation}_{i} + \gamma\,{Residence}_{i} + \lambda\,\,X_{i} + e_{i}
\end{equation}where  ${e_i} = \,\,{W_{ij}}{e_j} + {\in_i}.$
${e_i} = \,\,{W_{ij}}{e_j} + {\in_i}.$
Equation (9) is equivalent to Equation (6) except for the spatial autoregressive process in the error term  $({e_i})$.
$({e_i})$.  ${W_{ij}}$ represents the spatial weighting matrix, which we create by taking the inverse distance between the households as the spatial weights – households that are spatially close to each other have higher spatial weights and vice versa. Similarly,
${W_{ij}}$ represents the spatial weighting matrix, which we create by taking the inverse distance between the households as the spatial weights – households that are spatially close to each other have higher spatial weights and vice versa. Similarly,  ${W_{ij}}{e_j}{ }\,$represents the spatial lag for the error term and
${W_{ij}}{e_j}{ }\,$represents the spatial lag for the error term and  $\rho $ represents the parameter that captures the scale of spatial autocorrelation. A positive
$\rho $ represents the parameter that captures the scale of spatial autocorrelation. A positive  $\rho \,\left( {\rho \,\,0} \right)$ would indicate that the error in spatial location (
$\rho \,\left( {\rho \,\,0} \right)$ would indicate that the error in spatial location ( $i$) positively correlates with the error in location (
$i$) positively correlates with the error in location ( $j$), and a negative
$j$), and a negative  $\rho \,(\rho \lt 0)$ would indicate that the error in spatial location (
$\rho \,(\rho \lt 0)$ would indicate that the error in spatial location ( $i$) negatively correlates with the error in location (
$i$) negatively correlates with the error in location ( $j$). The parameters on the explanatory variables in the health outcome equation represent the coefficients to be estimated after controlling for the spatial dependence.
$j$). The parameters on the explanatory variables in the health outcome equation represent the coefficients to be estimated after controlling for the spatial dependence.
6. Results
6.1. Simultaneous equations model estimates
Regression results from ordinary least squares (OLS) estimates without accounting for endogeneity are presented in Model 1 in appendix Table A2. We find a positive coefficient on composite avoidance measures. The coefficient value of 0.035 indicates that the FEV1/FVC ratio increases by 0.035 units with an additional measure. This finding suggests that individual avoidance behaviours positively correlate with respiratory health. Next, we find that outdoor workers have a 0.059 unit lower FEV1/FVC ratio, implying that more exposure to ambient pollution corresponds to lower lung function. We also find that higher residential exposure correlates with lower lung function, as the coefficient on proximity to brick kilns (–0.056) is negative and statistically significant at the 5 per cent level. We run a separate regression to examine the role of facemasks and clean cooking stoves (Model 2 in appendix Table A2) and find positive associations of both measures on the FEV1/FVC ratio at the 10 per cent level.Footnote 8 Intriguingly, we do not see significant coefficients on proximity to major roads in both models.
Appendix Table A3a presents the estimates of the FEV1/FVC ratio after accounting for endogeneity in the choice of exposure avoidance. In Model 1, the FEV1/FVC ratio is regressed on just the composite avoidance measures. The estimated coefficient of using an additional measure on the FEV1/FVC ratio is 0.071, reinforcing the positive association between avoidance behaviour and respiratory health. In Model 2, occupational and residential exposure variables are added. Results indicate that individuals residing near the brick kilns have a 0.050 unit lower FEV1/FVC ratio. The coefficient on the outdoor occupation variable is negative and (weakly) significant at the 15 per cent level. In Model 3, we also add the socioeconomic and other controls. The sign and significance of the coefficient on occupation do not vary, although the significance of the coefficient on brick kiln becomes slightly weaker. The magnitude of the coefficient on composite exposure avoidance increases (from 0.073 to 0.114 units) with additional control variables. Using the minimum sample size corrected Akaike Information Criterion, Model 3 has the highest predictive power. Therefore, we use Model 3 as our preferred model. Given our relatively small sample size, we also bootstrapped each regression for 200 replications; the results did not change significantly.
Appendix Table A3b shows the estimates of composite avoidance measures (full model in Table A3a). The estimates are useful for identifying factors that influence exposure avoidance. The correlation between the two equations is significant at the 10 per cent level, indicating endogeneity in exposure avoidance. The coefficient on air quality perception is negative, suggesting that those who perceive air quality to be good are less likely to use avoidance measures. The coefficient on awareness is positive, indicating that awareness about air pollution's health impacts positively correlates with exposure avoidance. The relevance condition is satisfied for two reasons. First, both identifying variables are significant at the 1 per cent level. Second, the joint significance test confirms the validity of identifying variables at the 1 per cent level. Hansstein and Echegaray (Reference Hansstein and Echegaray2018) use the Theory of Planned Behaviour framework to investigate the motivation behind use of facemasks and highlight factors, including perception and awareness, that shape the intention to use facemasks, leading to behavioural action to limit health impacts. Therefore, we posit that air quality perception and awareness enter the health production function, but through behavioural channels. People who perceive higher levels of air pollution and are more aware of its health effects are likely to engage in avoidance behaviours to reduce their exposure, which can improve respiratory health. To investigate this further, we conducted a falsification test using a subsample of households that do not use any avoidance measures 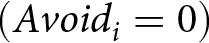 $(Avoi{d_i} = 0)$ and performed a reduced-form regression.Footnote 9 We found that perception and awareness do not predict lung function within the subsample, suggesting that these variables primarily influence lung function through avoidance behaviour.
$(Avoi{d_i} = 0)$ and performed a reduced-form regression.Footnote 9 We found that perception and awareness do not predict lung function within the subsample, suggesting that these variables primarily influence lung function through avoidance behaviour.
An intriguing finding is that labourers and farmers and individuals who live in wards containing brick kilns, although more affected, are significantly less likely to invest in avoidance measures. This result implies that exposure avoidance behaviours can further widen the exposure differential. We also find that the use of avoidance measures increases with education level and household wealth, and the use is higher among males, younger individuals and non-smokers.
6.2. Spatial analyses
The univariate Moran's I test suggests global spatial autocorrelation for labourers and farmers and exposure avoidance variables (appendix Table A4). We did not find a global spatial autocorrelation in the FEV1/FVC ratio variable. The hotspot and Kriging interpolation, nonetheless, suggest that the FEV1/FVC ratio has local spatial autocorrelation, as is evident from the significant hot spot and cold spot patches (appendix Figures A7–A9). Intriguingly, a consistent pattern emerges from these spatial analyses. Individuals living in the centre of the city are mostly non-labourers and farmers, exhibit higher exposure avoidance, and have significantly better lung function. In contrast, those who live in wards containing brick kilns, which are on the southern and western outskirts of the municipality, are least protected and have significantly lower lung function.
Before employing the spatial error model, we ran Moran’s tests to check for any spatial dependence in our two OLS models from appendix Table A2. The tests suggest significant spatial lags in the error terms (at 10 per cent), justifying the relevance of the spatial model (appendix Table A5). Results from the spatial error model, which does not account for endogeneity, and the spatial-IV model are presented in appendix Table A6. The signs on all coefficients are the same in spatial models. The significances, however, are more robust after controlling for the spatial autoregressive process in the error term. We also find the spatial lag parameter in the error term significant in both spatial error and spatial-IV models, suggesting a spatial association through the residual term. Table A6 compares estimates from all four models (OLS, simultaneous, spatial error and spatial-IV). The results are (more or less) consistent across the models, although we find that the occupation and brick kiln coefficients become smaller after accounting for endogeneity. Conversely, the coefficients on avoidance are moderately larger after accounting for endogeneity.
7. Discussion
The world is heading towards rapid urban growth. Currently, 55 per cent of the world’s population lives in urban areas, compared to 30 per cent in 1950, and most of the growth is happening in developing countries (UN, 2018). Without adequate regulations and policy controls, environmental degradation accompanying swift growth – including air pollution – threatens public health and welfare (Ebenstein et al., Reference Ebenstein, Fan, Greenstone, He, Yin and Zhou2015). Moreover, the burden of environmental degradation is disproportionately shared among the population, with the largest impacts falling on the marginalized groups (Duflo et al., Reference Duflo, Greenstone and Hanna2008; Anderson, Reference Anderson and Banzhaf2012; Rao et al., Reference Rao, Kiesewetter, Min, Pachauri and Wagner2021).
This study uses a representative household survey from Siddharthanagar municipality, a growing urban town in southern Nepal, to examine the association between individual air pollution exposure and respiratory health. To this end, we use direct measures of individual lung function as a biomarker of respiratory health. Our individual (and household) level dataset and empirical approaches allow us to shed some light on the exposure differential within the population and identify subgroups more exposed to air pollution, as reflected in the health outcome. While our study concurs with findings from several past studies, it also brings new results to light.
One-sixth of the respondents are primarily engaged in farming and daily wage labour. The nature of these occupations requires them to be exposed to ambient air pollution for a longer time. Sun et al. (Reference Sun, Kahn and Zheng2017) note that in China, the average outdoor time for office workers is only 64 per cent compared to all workers. In many cases, outdoor workers work near roads, factories and other adverse conditions, which expose them to dust, fumes and gases. We find that 7 per cent of individuals engaged in the two occupations remain outdoors for more than 9 hours, and 33 per cent spend 6–9 hours outdoors, significantly higher than the comparison group (Figure A3). We find evidence of lower lung function among outdoor workers – 5.2 percentage points lower. This finding aligns with past studies showing that the amount of outdoor time affects exposure and health outcomes (Foster and Kumar, Reference Foster and Kumar2011; Gurung and Bell, Reference Gurung and Bell2012). This crucial evidence has important policy implications for many developing areas, including Nepal, where many people rely on outdoor work for economic sustenance but face the severe risk of higher air pollution exposure.
The health implications of living close to pollution sources, such as major roads and industries, are well-established (Brender et al., Reference Brender, Maantay and Chakraborty2011; Anderson, Reference Anderson2019; Kopas et al., Reference Kopas, York, Jin, Harish, Kennedy, Shen and Urpelainen2020). Studies identify brick kilns as a major contributor of air pollution in the region around Siddharthnagar (Rupakheti et al., Reference Rupakheti, Adhikary, Praveen, Rupakheti, Kang, Mahata, Naja, Zhang, Panday and Lawrence2017; Saikawa et al., Reference Saikawa, Panday, Kang, Gautam, Zusman, Cong, Somanathan, Adhikary, Wester, Mishra, Mekherji and Shrestha2019). Emissions from brick kilns contribute to SO2, NOx, Black Carbon, Organic Compounds and PM. The brick kiln industry is swiftly growing to address the rising demand for bricks due to rapid urbanization. We show that individuals living near the brick kilns have lower lung function. A more interesting finding is the locations of these brick kilns. Brick kilns are in wards on the outskirts of the municipality, away from the central part of the city. Ward 1 is on the southernmost part and is closest to the bustling Nepal–India border. Likewise, Ward 4 is on the western outskirts and is on the route to Lumbini. The residents of the two wards are at the lower end of the wealth and education ladders (appendix Figure A6). Residents of these two wards also reported less awareness about air pollution – 64 per cent versus 85 per cent for the comparison group. The findings provide some indication of residential sorting based on proximity to pollution sources – households with higher socioeconomic status reside away from local pollution sources (Goodman et al., Reference Goodman, Wilkinson, Stafford and Tonne2011; Depro and Timmins, Reference Depro, Timmins and Banzhaf2012). However, with the information available in our dataset, we are unable to precisely identify whether the marginalized households are located near brick kilns, possibly due to lower land and housing prices, or if the brick kilns moved to those areas.
Our analysis does not show significant differences in the lung function of individuals living near major roads. Several studies indicate that individuals who live (or work) near roads are likely to have higher pollution exposure (Shakya et al., Reference Shakya, Rupakheti, Aryal and Peltier2016a). For instance, Anderson (Reference Anderson2019) finds that the elderly population living within 50 to 600 meters of highways have higher chances of premature mortality. Some studies do not find significant effects of road exposure on health. A case in point is Gurung and Bell (Reference Gurung and Bell2012), who do not find differences in lung function between traffic police and indoor workers. Similarly, Bowatte et al. (Reference Bowatte, Lodge, Knibbs, Erbas, Perret, Jalaludin, Morgan, Bui, Giles, Hamilton, Wood-Baker, Thomas, Thompson, Matheson, Abramson, Walters and Dharmage2018) do not find differences in lung function of individuals residing less (and more) than 200 meters away from major roads.
Our findings suggest a weak inverse quadratic (inverted U-shape) relationship between distance to road and the FEV1/FVC ratio (appendix Figure A5). The FEV1/FVC ratio initially improves with distance at a diminishing rate and then declines. We find a similar relationship between the FEV1/FVC ratio and two other traffic exposure indicators: the density of roads and open areas in the wards. Our survey coincided with the open agricultural (wheat) residue burning period, which ominously contributes to air pollution in the region (Rupakheti et al., Reference Rupakheti, Adhikary, Praveen, Rupakheti, Kang, Mahata, Naja, Zhang, Panday and Lawrence2017). We hypothesize that the immediate exposure to emissions from agricultural residue burning could affect individuals living away from the road near farmlands, which could also partly explain the lower lung function of farmers. We are, however, unable to validate these hypotheses with our dataset.
Individuals can reduce their air pollution exposure through avoidance measures. Exposure avoidance, however, involves a trade-off between the costs and the benefits of avoidance. Janke (Reference Janke2014) argues that behavioural response relies on an individual's assessment of the costs and benefits of response – if individuals perceive clear benefits and lower costs, responses are typically higher. When air pollution information is not readily available, perception about air quality based on visibility or smell can help people to make necessary adjustments, especially when the pollution levels are high and inferring the level of air pollution is easy (Graff Zivin and Neidell, Reference Graff Zivin and Neidell2013; Barwick et al., Reference Barwick, Li, Lin and Zou2024). However, given that some pollutants are colourless and odourless, public perception may not be an adequate indicator.
Ignoring individuals’ coping choices could underestimate the social welfare gain of pollution reduction, considering that some measures are highly costly. Confirming past studies (Graff Zivin and Neidell, Reference Graff Zivin and Neidell2009; Sun et al., Reference Sun, Kahn and Zheng2017; Zhang and Mu, Reference Zhang and Mu2018), we find that the public does react to the risk of air pollution exposure to create a safer personal environment. Two-thirds of the households use at least one avoidance measure. In line with the recommendations made in Graff Zivin and Neidell (Reference Graff Zivin and Neidell2013), we estimate the health production function using avoidance behaviour as a health input. Our findings indicate that the number of exposure avoidance actions positively correlates with lung function, indicating that individuals who use more measures are more protected. A caveat of this result is that we do not account for other types of avoidance actions, such as restricting outdoor activities, which risk-averse individuals may take. Our results advance the discussion on the health implications of exposure avoidance at a time when economic literature is paying attention to public preferences for exposure avoidance.
Despite being a new phenomenon, facemasks are gaining popularity in developing countries, especially in urban areas (Zhang and Mu, Reference Zhang and Mu2018; Ahmad et al., Reference Ahmad, Gibson, Nadeem, Nasim and Razaee2022). Amazon India saw one-year sales of facemasks increase by thirteenfold in 2016 compared to the year before (Choudhury, Reference Choudhury2016). Shakya et al. (Reference Shakya, Noyes, Kallin and Peltier2016b) evaluate the effectiveness of four commercially available cloth and surgical masks and two expensive N95 masks in Kathmandu, Nepal. They find that N95 masks are the most effective, followed by disposable surgical masks (filtration efficiency of 78–94 per cent), cloth masks with exhaust valves (80–90 per cent), and cloth masks with no exhaust valves (39–65 per cent). Cherrie et al. (Reference Cherrie, Apsley, Cowie, Steinle, Mueller, Lin, Horwell, Sleeuwenhoek and Loh2018) evaluate the efficiency of nine commercially available masks in Beijing, China, and find a penetration range of 0.26 per cent to 29 per cent for PM2.5 and BC, depending on the mask type and flow rate. Sun et al. (Reference Sun, Kahn and Zheng2017) report that air filters can reduce PM2.5 exposure by 92 per cent.
Traditional open fire stoves and solid fuels are extensively used in developing countries to meet domestic energy requirements, with up to 3 billion people relying on them (Duflo et al., Reference Duflo, Greenstone and Hanna2008; Pattanayak et al., Reference Pattanayak, Jeuland, Lewis, Usmani, Brooks, Bhojvaid, Kar, Lipinski, Morrison, Patange, Ramanathan, Rehman, Thadani, Vora and Ramanathan2019). Cleaner stoves are desired mostly for their better cooking efficiency. Recent studies emphasize that pollution concerns also significantly influence households’ preference for cleaner cooking technology (Pattanayak et al., Reference Pattanayak, Jeuland, Lewis, Usmani, Brooks, Bhojvaid, Kar, Lipinski, Morrison, Patange, Ramanathan, Rehman, Thadani, Vora and Ramanathan2019; Jeuland et al., Reference Jeuland, Pattanayak, Soo and Usmani2020).
7.1. A case of exposure differential and environmental inequity
One critical finding of this study is that the effects of air pollution are inequitably distributed among socioeconomic subgroups (see Fig. 1). Moreover, individuals and households more exposed to air pollution are less likely to adopt avoidance measures. We find labourers and farmers who work outdoors and remain more exposed to ambient air pollution are significantly less likely to adopt avoidance measures. The same is true for households that live in relatively more polluted areas. These findings suggest that exposure avoidance behaviours could widen the exposure gap between socioeconomic subgroups. We show limitations in the notion that avoidance behaviours invariably positively correlate with exposure.
A potential mechanism by which low socioeconomic position can lead to exposure and health inequality.

Income level is an essential factor behind differences in avoidance behaviours, as affluent households can afford expensive avoidance measures. Sun et al. (Reference Sun, Kahn and Zheng2017) highlight that the average price of air filters in China is $490, while facemasks requiring frequent disposal cost $0.9. People in the top 25 per cent in the income category accounted for 31.9 and 47.9 per cent of the total sales of facemasks and air filters, respectively. Rao et al. (Reference Rao, Kiesewetter, Min, Pachauri and Wagner2021) show that wealth-based socioeconomic status plays a big role in adopting clean cooking technology; marginalized households are less likely to own clean stoves. Additionally, wealthier households can live in better-insulated homes in less polluted areas, engage in indoor occupations, and have better health through good nutrition and medical care (Jayachandran, Reference Jayachandran2009; Foster and Kumar, Reference Foster and Kumar2011; Graff Zivin and Neidell, Reference Graff Zivin and Neidell2013). We concur with these findings, as our results show a significant positive role of wealth in the adoption of avoidance measures. Among households not using any avoidance measure, 29 per cent identified the lack of money as a significant barrier. Our data also reveal that occupation and residence-based marginalized groups fall in the lower wealth quintiles (Figure A6). These marginalized groups are also at the lower end of the education and awareness ladders.
Even after controlling for wealth and other factors like education, air quality perception and awareness, we still find exposure avoidance low among the marginalized groups, suggesting that other unaccounted factors may hinder adoption. In the survey, households identified the unavailability of resources near where they live as another barrier. Cooking fuel like LPG, for example, is difficult to transport and requires a robust supply chain to maintain a regular supply. It is also important to concede that people may simply resist behavioural changes. A relevant example is the long-held socio-cultural practice of cooking in open fire cookstoves (Pattanayak et al., Reference Pattanayak, Jeuland, Lewis, Usmani, Brooks, Bhojvaid, Kar, Lipinski, Morrison, Patange, Ramanathan, Rehman, Thadani, Vora and Ramanathan2019). Moreover, 44 per cent of households that do not use any measures find exposure prevention unnecessary. A plausible case is that these households cannot assess their exposure level and risk. Second, they may have incomplete knowledge about avoidance measures (Zhang and Mu, Reference Zhang and Mu2018). Third, adoption could be low when the benefits are not clear, given the cost of these measures (Janke, Reference Janke2014). Although the visibility of air pollution may reduce the cost of learning about the pollution level, adoption could be low when people permanently adapt to high pollution or do not consider averting the risk of exposure as an immediate priority. Lastly, individuals may evaluate the disutility of avoidance, especially facemasks, which could be discomforting for people engaged in physical toil, such as farmers and labourers (Zhang and Mu, Reference Zhang and Mu2018; Chen et al., Reference Chen, Gong and Zhao2024).
The health damages could be reduced by limiting air pollution through governmental regulations or by privately reducing individual exposure. While the regulations-led pollution reduction could have pervasive benefits, only a fraction of the population can benefit from private investments, exacerbating differences in pollution exposure within the population (Sun et al., Reference Sun, Kahn and Zheng2017). Moreover, regulations-led pollution reduction can greatly benefit people who can afford avoidance measures. Zhang and Mu (Reference Zhang and Mu2018) report that $187 million of private investment in facemasks alone could be saved if heavy pollution days in China were reduced by 10 per cent. The disproportionate burden of poor environmental quality on already marginalized groups calls for environmental justice actions (Goodman et al., Reference Goodman, Wilkinson, Stafford and Tonne2011; Anderson, Reference Anderson and Banzhaf2012; Tessum et al., Reference Tessum, Apte, Goodkind, Muller, Mullins, Paolella, Polasky, Springer, Thakrar, Marshall and Hill2019). The call is more salient at a time when income inequality and its consequences, including differential pollution exposure-led health inequality, are garnering much public concern (Piketty, Reference Piketty2014).
Our findings from Siddharthanagar municipality, a growing urban town in southern Nepal with 18,763 households, are likely applicable to other urban areas in South Asia with similar settings, pollution levels, pollution sources, income levels and awareness. Rupakheti et al. (Reference Rupakheti, Adhikary, Praveen, Rupakheti, Kang, Mahata, Naja, Zhang, Panday and Lawrence2017) report that particulate matter and O3 concentrations in the nearby Lumbini region are comparable to those in cities like Kathmandu, Nepal and Kanpur, India. Saikawa et al. (Reference Saikawa, Panday, Kang, Gautam, Zusman, Cong, Somanathan, Adhikary, Wester, Mishra, Mekherji and Shrestha2019) discuss the many similarities in socioeconomic conditions, pollution trends, and sources across urban cities in South Asia. Consistent with our findings, previous studies in the region have shown unequal exposure among different socioeconomic subgroups based on occupation in Kathmandu (Gurung and Bell, Reference Gurung and Bell2012; Shakya et al., Reference Shakya, Rupakheti, Aryal and Peltier2016a) and New Delhi, India (Foster and Kumar, Reference Foster and Kumar2011) and residential exposure across India (Kopas et al., Reference Kopas, York, Jin, Harish, Kennedy, Shen and Urpelainen2020; Rao et al., Reference Rao, Kiesewetter, Min, Pachauri and Wagner2021). Additionally, Ullah et al. (Reference Ullah, Ullah, Rajper, Ahmad and Li2021) report comparable air pollution-related health awareness and the use of exposure avoidance measures in the Malakand division of Pakistan.
8. Conclusion and policy recommendation
Taking the case of Siddharthanagar municipality of Nepal, this study finds an association between air pollution exposure and respiratory health. The study identifies socioeconomic position as an essential factor for individual exposure and exposure differential among the subgroups, mainly through three mechanisms – occupational exposure, residential exposure and exposure avoidance behaviours. The study underscores the role that endogenous choice of exposure avoidance can play in widening the exposure gap, suggesting that private investment in self-protection could lead to suboptimal social gain.
Our findings emphasize the need for government intervention to reduce air pollution exposure inequality. The government’s long-term priority should be reducing pollution by strictly regulating emissions from local sources such as industries, vehicles and agricultural residue burning. In the immediate future, the government can design policy actions to reduce exposure differences among marginalized groups. We find that marginalized households living near prominent pollution sources, like brick kilns, are affected. Although the Government of Nepal has initiated policies to regulate industries in the Lumbini-Siddharthanagar region since 2009, non-compliance with such policies is ubiquitous, resulting in higher emissions (IUCN, 2012). As Siddharthnagar municipality and the nearby big cities of Lumbini and Butwal are experiencing swift urban growth, careful industry-related environmental planning is much warranted to ensure a healthy living environment in the region. In line with the IUCN (2012) report, policymakers should frequently monitor emissions from the local industries and allow emissions as per the national standard. Policymakers should also promote the adoption of cleaner technology and energy sources in the local industries, especially in highly polluting industries like brick kilns.
Air quality monitoring is urgently required to gather data on air pollution and precisely identify pollution hotspots. Frequent dissemination of air quality information can also help the public to assess their exposure level and make necessary behavioural adjustments (Sun et al., Reference Sun, Kahn and Zheng2017; Kim, Reference Kim2021; Ahmad et al., Reference Ahmad, Gibson, Nadeem, Nasim and Razaee2022; Lu et al., Reference Lu, Chen and Cai2023). Subsidizing and providing financing options for avoidance measures and maintaining a robust supply may also increase adoption (Pattanayak et al., Reference Pattanayak, Jeuland, Lewis, Usmani, Brooks, Bhojvaid, Kar, Lipinski, Morrison, Patange, Ramanathan, Rehman, Thadani, Vora and Ramanathan2019). Awareness about the health effects of air pollution also positively correlates with avoidance actions. These recommendations are in the spirit of the UN Sustainable Development Goals (SDGs) that highlight the importance of good health and well-being (SDG goal 3), reducing inequality (SDG goal 10), and creating sustainable communities (SDG goal 11) (UN, 2015).
This study has several limitations. The most important limitation is that we rely on several individual exposure proxies. Therefore, we are not able to accurately measure individual exposure to different air pollutants. The study also considers residential location exogenous, despite gathering some indication of residential sorting based on proximity to pollution sources, which could bias our estimates. Another crucial limitation is that we do not know how frequently individuals use avoidance measures or their total expenditure on these measures. We have also not considered other forms of defensive behaviours, such as limiting outdoor activities and purchasing health insurance. Lastly, this study uses a cross-sectional dataset, which provides only a snapshot of air pollution exposure and respiratory health. Air pollution may have temporal variation throughout the year, mainly due to the meteorological conditions and the biannual practice of anthropogenic open-crop residue burning in the region.
Future research could address these limitations using long-term data on air pollution exposure and health outcomes. More specific to the case of Siddharthanagar and the Indo-Gangetic Plain, future studies could examine health and behavioural differences during pre- and post-crop residue burning periods and different seasons. The economics literature on the impacts of avoidance behaviours on health outcomes, mainly in the context of developing settings, is still scarce; therefore, more evidence is needed to establish causal linkages. In line with Sun et al. (Reference Sun, Kahn and Zheng2017) and Ahmad et al. (Reference Ahmad, Gibson, Nadeem, Nasim and Razaee2022), future studies can use an experimental design to study the effects of air quality information and knowledge about avoidance measures on adoption. Another experimental study can examine the impact of subsidizing avoidance measures on adoption. The experiments can help determine whether the differences in avoidance behaviour are due to air quality information and knowledge gap versus wealth disparities, which may have important policy implications.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1355770X26100539.
Acknowledgements
We are grateful to the South Asian Network for Development and Environmental Economics (SANDEE) for funding this research. We are thankful to our local collaborating institution Pratiman-Neema Memorial Foundation (PNMF), Nepal for their assistance with the survey logistics. We are also thankful to Mohammad Mashiur Rahman for the help in conducting the survey. We would also like to extend our utmost gratitude to the Atmosphere programme and Livelihoods theme of ICIMOD for hosting this research and providing technical assistance.
Author contributions
Niraj Khatiwada: Writing – Original draft preparation, Conceptualization, Formal analysis, Funding acquisition Alok K. Bohara: Supervision, Conceptualization, Methodology, Formal analysis, Funding acquisition
Completing interests
The authors declare none.
Ethical approval and informed consent
This research has been approved by the concerned Office of the Institutional Review Board. Further, informed consent was obtained from all participating households before the survey.



 Open access
Open access