


Statement of research significance
Research topic:
-
This study examined how depressive symptom severity influences the relationship between global cognitive performance and self-reported everyday functioning in people with HIV (PWH) over time.
Main findings:
-
In a longitudinal sample of PWH, worse cognition was associated with greater functional dependence, but only among those with low to moderate depressive symptom severity.
-
Among those with higher depressive symptom severity, functional dependence was reported regardless of cognitive performance.
-
No significant interaction was found for subjective cognitive difficulties and depressive symptoms.
Study contributions:
-
This study highlights the potential for depressive symptoms to obscure the relationship between cognitive impairment and everyday functioning in PWH.
-
Given the reliance on self-report in diagnosing HIV-Associated Neurocognitive Disorders (HAND), these findings emphasize the importance of considering depression severity in functional assessments.
-
This contributes critical nuance to HAND diagnostic practices and may improve accuracy in distinguishing neurocognitive impairment from mood-related functional complaints.
Introduction
HIV-associated neurocognitive disorders (HAND) can occur due to direct and indirect impacts of human immunodeficiency virus (HIV) on the nervous system, including observed pathology in the brain, spinal cord, and peripheral nerves (Clifford & Ances, Reference Clifford and Ances2013). The advent of combination antiretroviral therapy (cART) has notably reduced the occurrence of severe HAND and significantly enhanced disease management, leading to reductions in medical morbidity and mortality rates (Heaton et al., Reference Heaton, Clifford, Franklin, Woods, Ake, Vaida, Ellis, Letendre, Marcotte, Atkinson, Rivera-Mindt, Vigil, Taylor, Collier, Marra, Gelman, McArthur, Morgello and Simpson2010). Despite these advancements, reports indicate that HAND remains prevalent, with just under 50% of people with HIV (PWH) exhibiting mild to moderate forms of HAND, even when being treated with virally-suppressive cART – mirroring proportions seen in the pre-cART era (Heaton et al., Reference Heaton, Clifford, Franklin, Woods, Ake, Vaida, Ellis, Letendre, Marcotte, Atkinson, Rivera-Mindt, Vigil, Taylor, Collier, Marra, Gelman, McArthur, Morgello and Simpson2010). With PWH experiencing increased life expectancies, susceptibility to declines in everyday functioning due to HAND may also rise (Kordovski et al., Reference Kordovski, Tierney and Woods2021). However, diagnosing the impact of HIV on cognition remains challenging due to the contributions of several co-occurring factors (e.g., aging, potential cART toxicity, comorbidities) and individual differences, necessitating comprehensive assessments (Cody & Vance, Reference Cody and Vance2016; Neigh, Reference Neigh2016).
More specifically, HAND diagnosis require attributing at least some of the neurocognitive impairment and functional decline to the impact of HIV on the brain, independent of comorbidities (Antinori et al., Reference Antinori, Arendt, Becker, Brew, Byrd, Cherner, Clifford, Cinque, Epstein, Goodkin, Gisslen, Grant, Heaton, Joseph, Marder, Marra, McArthur, Nunn, Price and Wojna2007; Heaton et al., Reference Heaton, Clifford, Franklin, Woods, Ake, Vaida, Ellis, Letendre, Marcotte, Atkinson, Rivera-Mindt, Vigil, Taylor, Collier, Marra, Gelman, McArthur, Morgello and Simpson2010; Woods et al., Reference Woods, Moore, Weber and Grant2009).
Given the pivotal role of a patients’ everyday functioning in diagnosing HAND severity and differentiating asymptomatic from symptomatic forms, the accurate and reliable assessment of everyday functioning is critical. Presently, various methods – self-reported, clinician-rated, and performance-based – are available for assessing everyday functioning among PWH; however, no universally agreed-upon gold standard method exists (Kordovski et al., Reference Kordovski, Tierney and Woods2021). Hence, understanding the strengths and weaknesses of each approach is essential in guiding the assessment of functional decline among PWH. Self-report measures, prevalent in literature and clinical settings due to their cost-effectiveness and minimal participant burden, rely on accurate insight into one’s own everyday functioning (Blackstone et al., Reference Blackstone, Moore, Heaton, Franklin, Woods, Clifford, Collier, Marra, Gelman, McArthur, Morgello, Simpson, Rivera-Mindt, Deutsch, Ellis, Hampton Atkinson and Grant2012). Clinician-ratings are limited in most settings given that the clinician may have limited situational access and time to spend with the patient, and therefore may lack adequate knowledge of the participant’s daily life. Standardized, performance-based measures are the most objective; yet, they lengthen the diagnostic process and necessitate specialized testing equipment (Moore et al., Reference Moore, Palmer, Patterson and Jeste2007). These performance-based assessments may be more suitable when a patient meets other HAND criteria but denies declines in everyday functioning on self-reported measures (Antinori et al., Reference Antinori, Arendt, Becker, Brew, Byrd, Cherner, Clifford, Cinque, Epstein, Goodkin, Gisslen, Grant, Heaton, Joseph, Marder, Marra, McArthur, Nunn, Price and Wojna2007).
Factors, beyond changes in neuropsychological functioning among PWH, such as depressive and medical symptoms, may influence self-reported everyday functioning (Carter et al., Reference Carter, Rourke, Murji, Shore and Rourke2003; Jacob et al., Reference Jacob, Fazeli, Crowe and Vance2022). Furthermore, studies suggest that PWH may accurately identify the presence of functional decline in everyday functioning but may struggle to differentiate between physical, affective and cognitive causes (Obermeit et al., Reference Obermeit, Beltran, Casaletto, Franklin, Letendre, Ellis, Fennema-Notestine, Vaida, Collier, Marra, Clifford, Gelman, Sacktor, Morgello, Simpson, McCutchan, Grant and Heaton2017). Depressive symptoms have also been found to strongly associate with a patient’s self-reported assessment of everyday function, independent of cognitive impairment among PWH (Laverick et al., Reference Laverick, Haddow, Daskalopoulou, Lampe, Gilson, Speakman and Rodger2017). Acknowledging the impact of significant depression on biasing functional decline assessments, the Frascati criteria emphasize that self-report alone is insufficient in such cases (Antinori et al., Reference Antinori, Arendt, Becker, Brew, Byrd, Cherner, Clifford, Cinque, Epstein, Goodkin, Gisslen, Grant, Heaton, Joseph, Marder, Marra, McArthur, Nunn, Price and Wojna2007).
Some longitudinal studies have been done, but limited in regards to examining within-person or visit-specific relationships. General findings from these studies have shown that individuals who have steeper declines in cognition over time exhibit steeper declines in subjective cognition/functioning over time, compared to peers (McArdle & Nesselroade, Reference McArdle and Nesselroade2003). However, less is known about how subjective cognition and objective cognition covary within an individual (Burmester et al., Reference Burmester, Leathem and Merrick2016; Srisurapanont et al., Reference Srisurapanont, Suttajit, Eurviriyanukul and Varnado2017). In a large sample of older adults in the general population, Hülür et al., (Reference Hülür, Hertzog, Pearman, Ram and Gerstorf2014) found a within-person relationship between subjective functioning and objective cognition, such that participants reported worse cognitive symptoms on visits when they also had worse cognitive performance, even when covarying for occasion-specific depressive symptoms (Hülür et al., Reference Hülür, Hertzog, Pearman, Ram and Gerstorf2014). These within-person longitudinal relationships have not yet been evaluated in the context of HIV.
Therefore, the current study aimed to examine longitudinal relationships among objective global cognition, depressive symptom severity, and self-reported everyday functioning outcomes among PWH. The aims of the study were to examine i) the within- and between-person influence of depressive symptoms on everyday functioning (IADL dependence and self-report of cognitive difficulties), ii) the average within- (random slope) and between-person influence of objective cognitive performance on everyday functioning, and iii) to explore the influence of depressive symptoms on the relationship between objective cognitive performance and everyday functioning. Given that depression may precede cognitive decline (Koenig et al., Reference Koenig, Bhalla and Butters2014) and literature has noted that the effect of depression on cognitive function influences daily function in the long term (Gonda et al., Reference Gonda, Pompili, Serafini, Carvalho, Rihmer and Dome2015), we hypothesized that higher visit-specific depressive symptoms and worse visit-specific cognitive performance would independently relate to poorer self-reported everyday functioning within persons. Furthermore, we hypothesized that individuals with higher mean levels of depressive symptoms would exhibit a reduced influence of visit-specific cognitive performance on everyday functioning such that depressive symptoms may obscure the observable impact of cognition on everyday functioning. Thus, we anticipated that the within-person association between objective cognition and self-reported everyday functioning would depend on a person’s mean depression symptoms level over time, showing a stronger negative relationship between cognition and everyday functioning among participants with lower mean depression symptoms levels than those with higher mean depression symptom levels.
Methods
Participants
Participants included 894 PWH who were enrolled in NIH-funded cohort studies at the University of California San Diego (UCSD) HIV Neurobehavioral Research Program (HNRP). The major cohort studies included the NIH-funded HIV Neurobehavioral Research Center, the Translational Methamphetamine AIDS Research Center, and the California NeuroAIDS Tissue Network. Study visits occurred approximately every 6 months to 1 year between July 1, 2002 and April 10, 2016. All participants provided informed consent for participation in these cohort studies and agreed for their data to be used for future studies assessing the impact of HIV on the nervous system. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the UCSD Institutional Review Board. Exclusion criteria across all studies included history of neurological (e.g., seizure disorders) or severe psychiatric (e.g., schizophrenia) conditions. Inclusion criteria for the current analyses were: 1) having HIV, and 2) having at least two study visits with valid neurobehavioral data.
Measures
Everyday functioning
Participants completed two self-report measures of everyday functioning at each visit. The first, to assess the increased dependence in instrumental activities of daily living (IADLs) and, the second, to assess subjective cognitive difficulties (Patient’s Assessment of Own Functioning Inventory [PAOFI]).
For the first measure (IALD), study participants were classified as either IADL-dependent or IADL-independent based on their responses on a modified version of an Activities of Daily Living scale (Heaton, Marcotte, Mindt, Sadek, Moore, Bentley, McCutchan, Reicks, & Grant, Reference Heaton, Marcotte, Mindt, Sadek, Moore, Bentley and Grant2004). The adapted Activities of Daily Living scale assesses 16 functional domains encompassing both basic (e.g., bathing, dressing) and instrumental (e.g., managing finances, cooking) activities of daily living. Participants were instructed to rate their ability to independently complete each functional task both currently and when they were “functioning at their best.” Individuals were classified as IADL Dependent if their self-rated current level of independence had declined from their highest level of independence for at least two of the following functional domains: 1) housekeeping, 2) managing finances, 3) buying groceries, 4) cooking, 5) transportation, 6) using the telephone, 7) home repairs, 8) shopping for clothes and other non-food goods, 9) laundry, and 10) taking/keeping track of medication. This operationalization of IADL dependence was informed by published recommendations for determining functional impairment in HIV-associated neurocognitive disorders (Antinori et al., Reference Antinori, Arendt, Becker, Brew, Byrd, Cherner, Clifford, Cinque, Epstein, Goodkin, Gisslen, Grant, Heaton, Joseph, Marder, Marra, McArthur, Nunn, Price and Wojna2007; Heaton, Marcotte, Mindt, Sadek, Moore, Bentley, McCutchan, Reicks, et al., Reference Heaton, Marcotte, Mindt, Sadek, Moore and Bentley2004; Woods et al., Reference Paul Woods, Morgan, Dawson, Cobb Scott and Grant2006; Obermeit et al., Reference Obermeit, Beltran, Casaletto, Franklin, Letendre, Ellis, Fennema-Notestine, Vaida, Collier, Marra, Clifford, Gelman, Sacktor, Morgello, Simpson, McCutchan, Grant and Heaton2017).
For the second measure, participants completed the PAOFI self-report measure of subjective cognitive difficulties (Chelune et al., Reference Chelune, Heaton and Lehman1986). The PAOFI is a 34-item questionnaire in which participants report the frequency (from 0 – almost never to 5 – almost always) with which they have difficulties with memory, language and communication, use of hands, sensory-perception, and higher level cognitive and intellectual functions. A total score was derived by summing items that were rated as “fairly often” or “almost always” (range = 0–34), with higher scores indicating more reported cognitive difficulties.
Depression
All participants completed the Beck Depression Inventory-II (BDI-II) at each visit. The BDI-II is a 21-item self-report measure of depression symptom severity (Beck et al., Reference Beck, Steer and Brown1996) on which participants provide ratings of their experience of depression symptoms over the previous two weeks. The total score (range = 0–63) represents the sum of item ratings, with higher scores indicating greater number and severity of depression symptoms. The Composite International Diagnostic Interview (World Health Organization, 1998) was also administered to all participants to establish presence of current and lifetime major depressive disorder (MDD) based on the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2000).
Global neurocognitive functioning
Participants completed a comprehensive neurocognitive test battery (administration time: 2 to 2.5 hours) that assesses seven neurocognitive domains consistent with Frascati recommendations for neuroAIDS research (Antinori et al., Reference Antinori, Arendt, Becker, Brew, Byrd, Cherner, Clifford, Cinque, Epstein, Goodkin, Gisslen, Grant, Heaton, Joseph, Marder, Marra, McArthur, Nunn, Price and Wojna2007). The seven neurocognitive domains included speed of information processing, learning, memory (delayed recall), executive functioning, verbal fluency, working memory, and fine motor functioning; details on the specific test battery are provided elsewhere (Heaton et al., Reference Heaton, Clifford, Franklin, Woods, Ake, Vaida, Ellis, Letendre, Marcotte, Atkinson, Rivera-Mindt, Vigil, Taylor, Collier, Marra, Gelman, McArthur, Morgello and Simpson2010). Raw test scores were transformed into scaled scores adjusted for repeated testing but not demographic characteristics using a published normative data (e.g., Norman et al., Reference Norman, Moore, Taylor, Franklin, Cysique, Ake, Lazarretto, Vaida and Heaton2011). The normative set used US census (2000)-matched proportions of race/ethnicity categories: 68.7% Caucasian, 13.5% African American, 13.0% Hispanic, and 4.8% other race/ethnicities. Raw scores for the total subject group were converted into quantiles and were mapped into the corresponding quantiles of a standard normal distribution. These scores were then converted into normalized scaled scores with a mean of 10 and standard deviation of 3. We applied published practice-effect corrections (Cysique et al., Reference Cysique, Franklin, Abramson, Ellis, Letendre, Collier, Clifford, Gelman, McArthur, Morgello, Simpson, McCutchan, Grant and Heaton2011) to individual test scaled scores to account for potential learning from multiple exposures to the cognitive testing. In this study, demographic adjustments were not included in the transformation process to maintain consistency with our analytic goals and population focus, but adjustments for repeated testing ensured the validity of longitudinal comparisons.
The scaled scores were then averaged to provide a global scaled score (M = 10, SD = 3 in normative sample), which was used for primary analyses. To characterize neurocognitive functioning in the current sample, HIV-associated neurocognitive disorders (HAND) diagnoses were also established using the Frascati criteria (Antinori et al., Reference Antinori, Arendt, Becker, Brew, Byrd, Cherner, Clifford, Cinque, Epstein, Goodkin, Gisslen, Grant, Heaton, Joseph, Marder, Marra, McArthur, Nunn, Price and Wojna2007).
Neuromedical evaluation
HIV/ Acquired immunodeficiency syndrome (AIDS) disease status and related measures including disease duration, CD4 cell count (as a measure of immune system health), and engagement with HIV treatment, were determined by clinical interview and review of available clinical and immunological data. AIDS diagnoses were defined as has having a history of CD4+ T cell count <200 cells/μL or presence of an AIDS-indicating clinical condition utilizing the Centers for Disease Control and Prevention AIDS classification system. Quantification of current and lowest CD4+ T cells (flow cytometry) were performed at a Clinical Laboratory Improvement Amendments (CLIA)-certified, or CLIA equivalent, laboratory. Also, HIV RNA (active virus) levels in plasma were measured by reverse transcriptase polymerase chain reaction (Roche Amplicor, v. 1.5; lower limit of quantitation, 50 copies per milliliter).
Statistical analyses
Multilevel models are suitable to explore how visit-specific (within-person) variations in depressive symptoms and cognitive performance influences self-reported everyday functioning over time, while also accounting for average (between-person) differences in these predictors across individuals. Two multilevel models were conducted to examine within- and between-person predictors of self-reported everyday functioning outcomes: 1) a multilevel logistic regression model examined predictors of likelihood of IADL dependence, and 2) a multilevel linear regression model examined predictors of cognitive difficulties (i.e., PAOFI score). Primary within-person predictors for each model were visit-specific depressive symptom severity (i.e., person-centered BDI-II score), visit-specific global cognition (i.e., person-centered global scaled score), and time (i.e., years since baseline). The effect of visit-specific global cognition on everyday functioning was modeled as a random slope to allow the relationship to vary across participants and to permit the examination of mean depressive symptoms as a cross-level moderator of this relationship. Primary between-person predictors for each model were mean BDI-II score (i.e., mean within individuals across visits) and mean global cognition (i.e., global scaled score mean within individuals across visits).
Covariates for each multilevel model were determined by examining univariable relationships with the outcome variables (i.e., IADL dependence and PAOFI score). Any demographic or HIV disease characteristic that was related to either outcome at p < 0.05 was included in the models. Thus, two time-invariant covariates were included at the between-person level of each model: years of education and nadir CD4 (included as a dichotomous variable nadir CD4 < 200 [yes vs. no]). All analyses were conducted using R, version 4.4.2. Multilevel models were examined using the “lme4” package (Bates et al., Reference Bates, Mächler, Bolker and Walker2015).
Results
Demographic and clinical characteristics from participants’ baseline visit are displayed in Table 1. The sample of 894 PWH were about 46 years of age with 13 years of education on average, were predominantly male (83%) and non-Hispanic White (51%). Participants had an average of about 6 visits (SD = 3.6) over an average of 5 years (SD = 3.7). At baseline, they had high rates of past MDD (57%) with lower rates of current MDD (16%). Over half (55%) of participants also met Frascati criteria for HAND, with ANI being the majority (65%) of HAND diagnoses. Only 25% of participants were employed. In terms of HIV disease characteristics, most participants had a history of AIDS (75%) and were on ART (78%), and almost half had undetectable HIV viral loads (48%). A bivariate logistic regression showed that the likelihood of an undetectable viral load at the baseline visit was significantly positively related to the year that the baseline visit occurred (from 2002 to 2015: OR = 1.11 [per one year increase], 95%CI = 1.06–1.16, p < 0.001).
Baseline demographic and clinical characteristics

Note: Values are displayed as mean (SD), median [IQR] or n (%). BDI-II = Beck Depression Inventory – Second Edition, MDD = major depressive disorder, HAND = HIV-associated neurocognitive disorder, ANI = asymptomatic neurocognitive impairment, MND = mild neurocognitive disorder, HAD = HIV-associated dementia, IADL = instrumental activities of daily living, PAOFI = Patient’s Assessment of Own Functioning Inventory, AIDS = acquired immune deficiency syndrome, HIV = human immunodeficiency virus, ART = antiretroviral therapy.
an = 211, bn = 214; psychiatric diagnostic interviews were not consistently administered to all participants in all studies included until 2006.
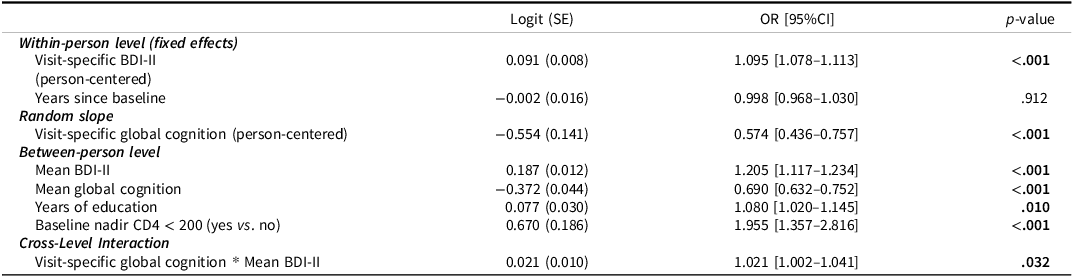
At the within-person level, there was a main effect of visit-specific BDI-II score (p < 0.001) and a conditional main effect of visit-specific global cognition (p < 0.001), such that higher depressive symptom severity and worse global cognitive performance related to higher likelihood of reported IADL dependence at that visit. Significant main effects at the between-person level showed that worse mean global cognition (p < 0.001), higher years of education (p = 0.010), and having a baseline nadir CD4 less than 200 (p < 0.001) were predictive of greater likelihoods of reported IADL dependence on average across visits. There was also a conditional main effect of mean BDI-II score (p < 0.001) such that greater mean BDI-II score related to greater likelihood of IADL dependence when global cognitive performance was at each person’s mean. Results of the multilevel logistic regression model showed a significant cross-level interaction, where mean depressive symptoms moderated the random slope of the relationship between visit-specific global cognitive performance and likelihood of IADL dependence (p = 0.032; Table 2). Probing this interaction at different levels of mean BDI-II score revealed that participants with lower mean levels of depressive symptoms displayed a stronger relationship between global cognition and likelihood of IADL dependence compared to participants with higher mean levels of depressive symptoms (Figure 1). Participants with higher mean depressive symptoms levels had greater likelihoods of IADL dependence regardless of their cognitive performance.
Interaction between visit-specific global cognition and mean BDI-II score on likelihood of IADL dependence. Intercepts, slopes, and 95%CI bands were derived from multilevel model estimates. A person-centered global scaled score of 0 represents an individual’s mean level of global cognition, with negative and positive values representing cognitive performances worse than and better than their mean, respectively. Each line represents a quintile of the mean BDI-II distribution. Note. IADL = instrumental activities of daily living, BDI-II = Beck Depression Inventory.

Results of multilevel logistic regression model examining within- and between-person effects of depression and global cognition on likelihood of self-reported IADL dependence. Outcome: likelihood of self-reported IADL dependence

Note: Bolded p-values are significant at p < 0.05. IADL = instrumental activities of daily living, BDI-II = Beck Depression Inventory.
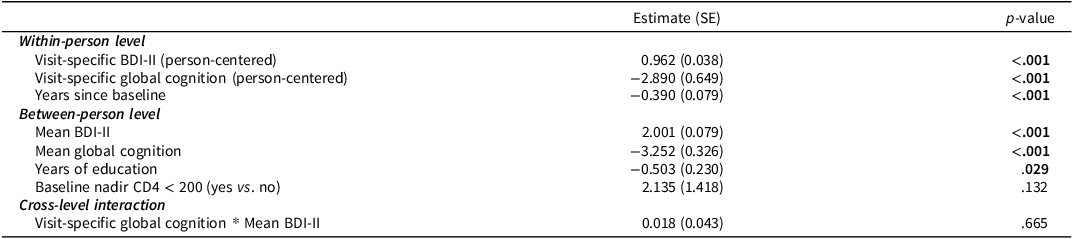
In contrast, the interaction between visit-specific global cognition and mean BDI-II score on self-reported cognitive difficulties (i.e., PAOFI score) was not statistically significant (p > 0.05; Table 3; Figure 2). Significant main effects at the within-person level showed that higher visit-specific BDI-II score (p < 0.001) and worse visit-specific global cognitive performance (p < 0.001) related to higher (worse) PAOFI scores. PAOFI scores also appeared to decrease within persons over time (p < 0.001). Significant main effects at the between-person level showed that higher mean BDI-II score (p < 0.001), lower mean global cognition (p < 0.001), and lower years of education (p < 0.05) related to worse PAOFI scores on average across visits.
Additive main effects of visit-specific global cognition and mean BDI-II score on self-reported cognitive difficulties (i.e., PAOFI score). Intercepts, slopes, and 95%CI bands were derived from multilevel model estimates. A person-centered global scaled score of 0 represents an individual’s mean level of global cognition, with negative and positive values representing cognitive performances worse than and better than their mean, respectively. Each line represents a quintile of the mean BDI-II distribution. Note. PAOFI = Patient’s Assessment of Own Functioning Inventory, BDI-II = Beck Depression Inventory.

Results of multilevel linear regression model examining within- and between-person effects of depression and global cognition on self-reported cognitive difficulties (PAOFI score). Outcome: self-reported cognitive difficulties (PAOFI score)

Note: Bolded p-values are significant at p < 0.05. PAOFI = Patient’s Assessment of Own Functioning Inventory, BDI-II = Beck Depression Inventory.
Discussion
Given that assessment of everyday functioning is an essential component in the diagnostic criteria for HAND, a longitudinal examination of within- and between-person predictors of self-reported everyday functioning is needed to support appropriate use of self-reported functioning among PWH. Consistent with our first hypothesis, we found significant, independent, within-person associations of visit-specific depressive symptom severity and visit-specific global cognition on both IADL dependence and cognitive difficulties. That is, fluctuations in depressive symptoms and cognitive performance related to respective changes in self-reported everyday functioning outcomes over time within persons. Additionally, and partially consistent with our second hypothesis, results also showed that the average within-person relationship between cognitive performance and likelihood of reported IADL dependence was moderated by participants’ mean depressive symptom level such that the relationship was strongest among those with low mean depression symptoms. More specifically, participants with low mean depressive symptoms were more likely to report IADL dependence when they also had below-mean cognitive performance. In contrast, participants with high mean depressive symptoms were likely to report IADL dependence regardless of their global cognitive performance.
The interaction between mean depressive symptom severity and visit-specific cognitive performance on reported IADL dependence is a novel analysis and result within this population and with longitudinal data in general. The evidence that high levels of depressive symptoms negatively bias self-reported everyday functioning, however, is consistent with the majority of literature in HIV (Atkinson et al., Reference Atkinson, Grant, Kennedy, Richman, Spector and McCutchan1988; Kamat et al., Reference Kamat, Morgan, Marcotte, Badiee, Maich, Cherner, Almeida, de Pereira, Ribeiro, Barbosa, Atkinson and Ellis2013) and other clinical populations (e.g., schizophrenia, Alzheimer’s) (Clare et al., Reference Clare, Whitaker, Quinn, Jelley, Hoare, Woods and Wilson2012; Mausbach et al., Reference Mausbach, Depp, Bowie, Harvey, McGrath, Thronquist and Patterson2011). The guidelines and criteria for HAND advise against relying solely on self-reported everyday functioning, especially in instances of elevated depressive symptoms (Antinori et al., Reference Antinori, Arendt, Becker, Brew, Byrd, Cherner, Clifford, Cinque, Epstein, Goodkin, Gisslen, Grant, Heaton, Joseph, Marder, Marra, McArthur, Nunn, Price and Wojna2007). These recommendations underscore the potential bias that heightened depressive symptoms can introduce into self-reported assessments of daily functioning in individuals affected by HAND.
Interestingly, depressive symptoms were found to negatively bias the IADL outcome, but not the PAOFI outcome. The PAOFI outcome showed more consistency with additive main effects of cognition and depressive symptoms. As previously stated, this evidence regarding the IADL measure reinforces recommendations to not rely on self-report of functional impairment in instances of heightened depressive symptom levels. Also, our results are consistent with previous studies of state-dependent biases in self-reports, where depression can skew perceptions towards feeling worse off, potentially influencing self-reported functional abilities (Thames et al., Reference Thames, Becker, Marcotte, Hines, Foley, Ramezani, Singer, Castellon, Heaton and Hinkin2011). This insight suggests a need to consider treating depression to address reported functional challenges, especially for individuals have minimal or no cognitive impairments. It is important to note that heightened depression may contribute to poorer IADL dependence not only through neurocognitive difficulties but also through physical symptoms such as fatigue and reduced energy, underscoring the need for multidimensional assessments of everyday functioning in PWH.
Results also show within-person independent main effects of both cognitive function and depressive symptoms. Notably, this offers support for the notion that alterations in cognition continue to exert influence on self-reported everyday functional outcomes, even when controlling for changes in depressive symptom levels. Despite previous work showing a relation between cognition and depression (Paolillo et al., Reference Paolillo, Pasipanodya, Moore, Pence, Atkinson, Grelotti and Moore2020), our model highlighted their independent effects on everyday functioning. This distinction holds particular significance concerning the PAOFI measure, emphasizing that the relative shifts in PAOFI scores within an individual might carry more clinical relevance than the absolute score at any single point in time. This insight underscores the dynamic interplay between cognitive function, depressive symptoms, and their individual impacts on perceived functional outcomes.
It is also worth noting that IADL dependence did not show improvement over time, as the nature of the IADL measure reflects tangible and concrete daily activities, which tend to decline naturally with age unless there is recovery from a specific acute disability episode. In contrast, the PAOFI is a more subjective measure, potentially influenced by mood and cognitive appraisal, which could explain its decrease over time.
These differing patterns between IADL dependence and PAOFI scores may reflect the distinct nature of these measures. IADL dependence captures objective functional activities and is more closely tied to cognitive performance, while PAOFI scores are subjective and more influenced by mood states, such as depression. The lack of interaction between cognition and depressive symptoms in predicting PAOFI scores suggests that subjective cognitive difficulties may be driven more by depressive symptomatology than actual cognitive changes, consistent with prior findings that depression can negatively bias self-perceived functioning (Atkinson et al., Reference Atkinson, Grant, Kennedy, Richman, Spector and McCutchan1988; Kamat et al., Reference Kamat, Morgan, Marcotte, Badiee, Maich, Cherner, Almeida, de Pereira, Ribeiro, Barbosa, Atkinson and Ellis2013).
Examination of covariates within our study revealed a time-related decrease in PAOFI over time, akin to the general decline noted in BDI scores over time, as indicated in Paolillo et al. (Reference Paolillo, Pasipanodya, Moore, Pence, Atkinson, Grelotti and Moore2020). Moreover, we also note the impact of education and nadir CD4 levels as covariates. These factors surfaced as potentially influential variables in understanding observed changes in IADL dependence.
Limitations
The study has several limitations, including the absence of an HIV-negative control group (Nweke et al., Reference Nweke, Mshunqane, Govender, Akinpelu and Ukwuoma2022), however the focus of the study was on HAND so the absence of a control group for HIV may not significantly impact our outcomes. Participant selection bias (e.g., relatively low percent of women) could limit the generalizability to the broader HIV population. We acknowledge that a limitation of our study is the reliance on self-report measures (e.g., depression and everyday functioning), which may introduce the potential for self-report bias. This bias may arise from shared variance due to mood or perception at the time of response, potentially inflating the observed associations. However, the measures utilized in this study are widely validated, which likely mitigated some of this bias. Also, reported IADL dependence may result in depression (bidirectional influences) so our results may be overestimating its impact. Furthermore, we acknowledge that a limitation of our study is the absence of informant-report data. Previous research (e.g., Becker et al., Reference Becker, Solbrig, Michaelis, Faust, Brockmann and Liepelt-Scarfone2022) indicates that informant reports can offer valuable additional perspectives, especially when patient self-awareness may be affected. Future studies should consider including informant assessments to provide a more comprehensive evaluation of daily functioning. Finally, PAOFI scores showed a decrease over time within persons, which may reflect sample retention bias, as individuals with higher scores were more likely to drop out in long follow-ups. Additionally, missing data were handled using complete case analysis, which could introduce bias into the findings.
Conclusions
These results highlight the importance of considering both depressive symptoms and cognitive performance in assessing everyday functioning in PWH, particularly when diagnosing symptomatic HAND. It reveals that cognitive abilities and IADL dependence are linked in individuals with low to moderate depressive symptom levels, but in those with higher depressive symptom levels, IADL dependence is likely to be reported irrespective of cognitive status. These findings are of clinical relevance as they stress the importance of relying on diverse assessment methods, including self-reports and informant- or performance-based evaluations, to assess an individual’s everyday functioning.
Acknowledgements
Competing interests: Dr Raeanne Moore is a co-founder of KeyWise AI and NeuroUX.
This work was supported by the National Institute on Drug Abuse (C.R.S. and M.R.P., TRAIN T32 grant number 5T32DA031098), (J.M. grant number NIDA K23DA051324), (M.A.H., T32 DA031098); the National Institute on Aging (R.M., grant number NIA R01AG62387); and the Veterans Affairs MIRECC fellowship (M.A.H., Department of Veterans Affairs, Veterans Health Administration, Office of Academic Affiliations, VISN22 Desert Pacific Mental Illness Research, Education and Clinical Centers MIRECC Advanced Postdoctoral Fellowship).
The HIV Neurobehavioral Research Center (HNRC) is supported by Center award P30MH062512 from NIMH. The San Diego HIV Neurobehavioral Research Center [HNRC] group is affiliated with the University of California, San Diego, the Naval Hospital, San Diego, and the Veterans Affairs San Diego Healthcare System, and includes: Director: Robert K. Heaton, Ph.D., Co-Director: Igor Grant, M.D.; Associate Directors: Ronald J. Ellis, M.D., Ph.D., and Scott Letendre, M.D.; Center Manager: Jennifer Iudicello, Ph.D.; Donald Franklin, Jr.; Cheryl Kelley; NeuroMedical Core: Ronald J. Ellis, M.D., Ph.D. (Director/NeuroMedical Unit Head), Scott Letendre, M.D. (Co-I./Laboratory Unit Head), Christine Fennema-Notestine, Ph.D., (Co-I./Neuroimaging Unit Head); Debra Rosario, M.P.H., Neurobehavioral & Psychiatry Core: David J. Moore, Ph.D. (Co-Director/Neurobehavioral Unit Head), Murray B. Stein, M.D. (Co-Director/Psychiatry Unit Head), Erin E. Morgan, Ph.D. (Co-I./Psychiatric Coordinator), Andrew H. Miller, Matthew Dawson, NeuroVirology & Biology Core: Sara Gianella Weibel, M.D. (Co-Director/NeuroVirology Unit Head), Sarah A. LaMere, D.V.M., Ph.D. (Associate Unit Head, NeuroVirology Unit), Cristian Achim, M.D., Ph.D. (Co-Director/Neurobiology Unit Head), Ana Sanchez, Ph.D. (Co-I./Neurobiology Unit), Adam Fields, Ph.D.(Associate Unit Head, Neurobiology Unit); Microbiome Core: Rob Knight, Ph.D. (Co-Director), Pieter Dorrestein, Ph.D. (Co-Director); Developmental Core: Scott Letendre, M.D. (Director), Ajay Bharti, M.D. (Co-I.), J. Allen McCutchan, M.D., Christine Fennema-Notestine, Ph.D.; Administrative Core: Robert K. Heaton, Ph.D. (Director/Coordinating Unit Head), Participant Accrual and Retention Unit: J. Hampton Atkinson, M.D. (Unit Head), Jennifer Marquie-Beck, M.P.H.; Data Management and Information Systems Unit: Ian Abramson, Ph.D. (Unit Head), Clint Cushman; Statistics Unit: Florin Vaida, Ph.D. (Unit Head), Anya Umlauf, M.S., Bin Tang, Ph.D.
“The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.”




 Open access
Open access