


Statement of Research Significance
Research Question(s) or Topic(s): This study examined whether patients with Parkinson’s disease (PD) without cognitive impairment (PD-CU) show subtle visuo-constructional deficits using the qualitative scoring of the Rey–Osterrieth complex figure (ROCF) via the Boston Qualitative Scoring System, and how these relate to cognitive functioning. Main Findings: Both PD-CU and PD with mild cognitive impairment patients showed qualitative alterations in ROCF performance compared to healthy controls. Specifically, in PD-CU, we found reduced planning and neatness, which were associated with executive dysfunction. Furthermore, distinct cognitive profiles were linked to lateralized copying styles. Study Contributions: The study highlights the clinical value of qualitative ROCF analysis in detecting early executive deficits in PD-CU that may not be identified by standard neuropsychological tests. Incorporating qualitative tools into cognitive evaluations could enhance early diagnosis and guide timely interventions. Additionally, identifying asymmetric copying patterns offers a novel, actionable method to stratify patients based on divergent cognitive trajectories and potential progression risk.
Introduction
Constructional apraxia is a cognitive disorder defined by an inability to draw three- or two-dimensional figures, assembling their single elements into a unitary and complete reproduction under the guidance of a perceptual or mental model (Gainotti & Trojano, Reference Gainotti and Trojano2018). Although it is usually considered a unitary cognitive construct, increasing neuropsychological and imaging evidence highlights the involvement of multiple cognitive processes in drawing, including visuospatial processes, planning abilities, and control processes (Bai et al., Reference Bai, Liu and Guan2021; Gainotti & Trojano, Reference Gainotti and Trojano2018).
A neurodegenerative disease in which constructional apraxia is frequently observed is Parkinson’s disease (PD), a progressive, multisystem neurodegenerative disorder characterized by motor and non-motor symptoms (Trojano & Papagno, Reference Trojano and Papagno2018). Among these, cognitive dysfunctions play a relevant role in disease progression (Postuma et al., Reference Postuma, Berg, Stern, Poewe, Olanow, Oertel, Obeso, Marek, Litvan, Lang, Halliday, Goetz, Gasser, Dubois, Chan, Bloem, Adler and Deuschl2015) and have received particular attention due to their consequences in everyday functioning (Leroi et al., Reference Leroi, McDonald, Pantula and Harbishettar2012). At the neural level, these cognitive alterations are the result of two primary processes: the progressive dysfunction of fronto-striatal networks and the accumulation of Lewy body pathology in temporo-parietal regions (Fu & Halliday, Reference Fu and Halliday2025). PD cognitive profile is commonly characterized by executive dysfunctions, although visuospatial deficits, together with language and memory impairments, might also be detected in the early stages of the disease (Barvas et al., Reference Barvas, Mattavelli, Zappini, Giardina, Ottaviani and Papagno2021). Notably, constructional apraxia is recursively reported (Allone et al., Reference Allone, Lo Buono, Corallo, Bonanno, Palmeri, Di Lorenzo, Marra, Bramanti and Marino2018), not only at the stage of overt dementia (Saur et al., Reference Saur, Maier, Milian, Riedel, Berg, Liepelt-Scarfone and Leyhe2012) but also in the stage of mild cognitive impairment (MCI) (Allone et al., Reference Allone, Lo Buono, Corallo, Bonanno, Palmeri, Di Lorenzo, Marra, Bramanti and Marino2018; Saka & Elibol, Reference Saka and Elibol2009; Saur et al., Reference Saur, Maier, Milian, Riedel, Berg, Liepelt-Scarfone and Leyhe2012), suggesting a utility of drawing tasks in terms of screening measures (Lolekha et al., Reference Lolekha, Tangkanakul, Saengchatri and Kulkeartprasert2021), differential diagnosis (Alissa et al., Reference Alissa, Lones, Cosgrove, Alty, Jamieson, Smith and Vallejo2022; Saka & Elibol, Reference Saka and Elibol2009), and detection of subtle cognitive changes (Schejter-Margalit et al., Reference Schejter-Margalit, Kizony, Shirvan, Cedarbaum, Bregman, Thaler, Giladi and Mirelman2021).
The direct copy of the Rey–Osterrieth complex figure (ROCF) (Caffarra et al., Reference Caffarra, Vezzadini, Dieci, Zonato and Venneri2002) is often used for assessing drawing skills in individuals with cognitive decline. This test allows for the evaluation of both copying accuracy and the qualitative aspects of the procedure, providing more detailed insights into the patient’s difficulties. Remarkably, the qualitative analysis of patients’ production and errors allows the identification of distinctive features in copying performance and their association with other cognitive dysfunctions that may contribute to constructional apraxia in these patients (Trojano & Gainotti, Reference Trojano and Gainotti2016). The Boston Qualitative Scoring System (BQSS) (Stern et al., Reference Stern, Singer, Duke, Singer, Morey, Daughtrey and Kaplan1994) represents a structured method for qualitative assessment that provides multiple scores developed to measure executive (e.g., planning, fragmentation, neatness, perseveration) and visuospatial (e.g., rotation, symmetry) aspects of the ROCF production.
In PD patients with cognitive deficits, qualitative drawing alterations have been previously reported, often associated with executive dysfunctions (Freeman et al., Reference Freeman, Giovannetti, Lamar, Cloud, Stern, Kaplan and Libon2000). Furthermore, Scarpina et al. (Reference Scarpina, Ambiel, Albani, Pradotto and Mauro2016) used the BQSS to explore these deficits, showing that PD patients without dementia exhibited greater difficulties in ROCF planning, as well as impulsive and visuospatial errors (i.e., spatial rotation) (Scarpina et al., Reference Scarpina, Ambiel, Albani, Pradotto and Mauro2016). However, no studies have investigated the possible presence of subtle qualitative alterations in PD without overt cognitive impairment (PD-CU) that might represent a complementary source of information to the quantitative standard assessment.
Therefore, this study aims to evaluate qualitative alterations at the ROCF copy in PD-CU individuals compared to those mild cognitively impaired (PD-MCI) and healthy controls (HCs), and to evaluate their relationship with cognitive performance in executive and visuospatial tasks.
Materials and methods
Participants
Seventy patients with PD diagnosed according to the Movement Disorders Society criteria (Postuma et al., Reference Postuma, Berg, Stern, Poewe, Olanow, Oertel, Obeso, Marek, Litvan, Lang, Halliday, Goetz, Gasser, Dubois, Chan, Bloem, Adler and Deuschl2015) were recruited at the Center for Neurocognitive Rehabilitation of the Center for Mind/Brain Sciences (University of Trento). Inclusion criteria were a diagnosis of idiopathic PD (Postuma et al., Reference Postuma, Berg, Stern, Poewe, Olanow, Oertel, Obeso, Marek, Litvan, Lang, Halliday, Goetz, Gasser, Dubois, Chan, Bloem, Adler and Deuschl2015), Hoehn and Yahr score ≤ 4, age above 60 years, and being under L-dopa medication. Patients with evidence of dementia or other neuropsychiatric disorders were excluded, as well as patients with visual or motor limitations preventing the full neuropsychological assessment. All patients underwent a baseline clinical evaluation performed by experienced neurologists and neuropsychologists and were tested while on their medication regimen.
Fifty-six HCs, matched for demographic variables to the patient group, were enrolled for statistical comparison at the drawing task. HCs were included based on the absence of positive neuropsychiatric history, neurological disorders, or cognitive impairment evaluated through the Italian version of the Montreal Cognitive Assessment (MoCA) and a brief neuropsychological assessment. The study was conducted following the ethical guidelines of the local ethics committee (University of Trento Research Ethics Committee) and the Declaration of Helsinki, and written informed consent was signed by all participants.
Neuropsychological assessment
All participants underwent a standard neuropsychological evaluation, including a screening test of global cognitive functioning (MoCA) and two tests for each cognitive domain according to MDS criteria (Litvan et al., Reference Litvan, Goldman, Tröster, Schmand, Weintraub, Petersen, Mollenhauer, Adler, Marder, Williams-Gray, Aarsland, Kulisevsky, Rodriguez-Oroz, Burn, Barker and Emre2012). Attentional matrices and Trail Making Test B-A were selected for attention, Rey’s 15 words test delayed recall and ROCF delayed recall for long-term memory, Stroop error index and phonemic verbal fluency for executive functions, semantic verbal fluency and picture naming for language, and Judgment of Line Orientation and Benton Facial Recognition Test for visuospatial abilities. Based on the Italian normative cut-off scores, patients were classified as MCI (n = 24) or CU (n = 46) following the MDS Level II criteria (Litvan et al., Reference Litvan, Goldman, Tröster, Schmand, Weintraub, Petersen, Mollenhauer, Adler, Marder, Williams-Gray, Aarsland, Kulisevsky, Rodriguez-Oroz, Burn, Barker and Emre2012). According to these criteria, a patient is classified as MCI when showing impairments in at least two neuropsychological tests (i.e., either one impaired test in two different cognitive domains or two impaired tests in a single cognitive domain). In our sample, no PD-CU patient met these criteria, as they did not perform in the pathological range in any administered test according to Italian normative data.
Quantitative and qualitative evaluation of constructional praxis through the ROCF copy
All participants performed the direct copy of the ROCF, which was scored from a quantitative point of view following the Italian normative procedures (Caffarra et al., Reference Caffarra, Vezzadini, Dieci, Zonato and Venneri2002). A score of 0 to 2 points was assigned for each of the 18 elements constituting the figure. Specifically, a score of 2 was given when the element was present, accurate, and well placed; a score of 1 if the element was present, but dislocated or inaccurate; a score of 0.5 if the element was both inaccurate and dislocated; a score of 0 when the element was absent. The overall score ranges from 0 to 36.
Qualitative aspects were assessed using the BQSS, which provides a fully structured and standardized approach to ROCF qualitative evaluation. Unlike other observational methods used especially in the developmental field, such as the Developmental Scoring System (DSS-ROCF) (Bernstein & Waber, Reference Bernstein and Waber1996) and (Lang et al., Reference Lang, Roberts, Harrison, Lopez, Goddard, Khondoker, Treasure and Tchanturia2016 Reference Lang, Roberts, Harrison, Lopez, Goddard, Khondoker, Treasure and Tchanturia), the BQSS can be applied to a wide range of populations (neurological, geriatric and psychiatric) and provides detailed criteria and replicable scoring procedures, thereby enhancing psychometric properties. In fact, the BQSS shows good inter-rater reliability, test–retest reliability, and discriminant validity between patients’ groups and HC, and among different patient groups (traumatic brain injury, dementia, human immunodeficiency virus, attention-deficit/hyperactivity disorder, and alcohol abuse) (Stern et al., Reference Stern, Javorsky, Singer, Singer Harris, Sommerville and Duke1992; Stern et al., Reference Stern, Singer, Duke, Singer, Morey, Daughtrey and Kaplan1994). Besides, while normative values are not formally defined (Stern et al., Reference Stern, Singer, Duke, Singer, Morey, Daughtrey and Kaplan1994), previous studies have reported BQSS scores distribution, validating its use to differentiate typical from atypical drawing patterns (Freeman et al., Reference Freeman, Giovannetti, Lamar, Cloud, Stern, Kaplan and Libon2000; Scarpina et al., Reference Scarpina, Ambiel, Albani, Pradotto and Mauro2016; Somerville et al., Reference Somerville, Tremont and Stern2000).
The qualitative parameters of the BQSS (Stern et al., Reference Stern, Singer, Duke, Singer, Morey, Daughtrey and Kaplan1994) include fragmentation, planning, neatness, perseverations, and confabulations aspects. Specifically, fragmentation refers to the segmentation of elements into smaller parts, planning to the organization of the production, neatness to the waviness of the lines; perseveration to the presence of repeated elements in the figure, and confabulations to the addition of elements absent in the ROCF model (Somerville et al., Reference Somerville, Tremont and Stern2000). Furthermore, the BQSS allows for the evaluation of visuospatial alterations such as asymmetry, as well as vertical and/or horizontal expansion, reduction, and rotation, analyzed by using transparency templates (Stern et al., Reference Stern, Singer, Duke, Singer, Morey, Daughtrey and Kaplan1994).
In our study, two expert raters (C.L. and R.B.), blind to clinical evaluation, assessed ROCF copy performance according to BQSS guidelines (Stern et al., Reference Stern, Singer, Duke, Singer, Morey, Daughtrey and Kaplan1994). As provided by the BQSS, a score from 0 (poor) to 4 (good) was assigned for each type of feature. Then, an aggregate score (0–4) was obtained for each qualitative aspect. Asymmetry was assessed by analyzing the presence of fewer details or more distortions on one side of the figure than the other based on BQSS guidelines (Stern et al., Reference Stern, Javorsky, Singer, Singer Harris, Sommerville and Duke1992), obtaining a three-level nominal variable (left asymmetry, right asymmetry, no asymmetry).
Statistical analysis
First, preliminary statistical analyses were performed to assess data distribution (Shapiro–Wilk test) and to compare demographic, clinical, and cognitive variables between groups using parametric or non-parametric (Kruskal–Wallis) one-way ANOVA and Chi-squared tests.
Post hoc analyses were carried out through the Games–Howell (for parametric statistics) and Dwass–Steel–Critchlow–Fligner tests (for non-parametric statistics) to analyze possible significant differences between the performance of PD-MCI compared to PD-CU and HC, but also between PD-CU and HC. In the analyses of BQSS parameters, preliminary correlations were performed to compare raters’ evaluations (all correlations p < 0.001), and average scores were then computed for each BQSS variable (i.e., fragmentation, planning, neatness, perseverations, reduction, rotation, vertical/horizontal expansion, and confabulations) to be considered for the subsequent analysis. For asymmetry, each rater evaluated in all images the absence (N) or the presence of asymmetric copy with the lack of details on the right (R) or on the left (L) part of the figure. Discordant judgments (12%) were jointly reviewed by the raters until consensus was reached. Next, non-parametric one-way ANOVAs were computed to compare ROCF qualitative performances between groups based on the BQSS. Differences in the frequency of asymmetric copy patterns between groups were analyzed through Chi-square statistics.
Since a significant percentage of patients showed an asymmetric copy pattern, ANCOVAs were also performed to compare attentional-executive and visuospatial abilities between groups defined based on the ROCF asymmetry (i.e., N/L/R), considering the ROCF overall scores as nuisance variable. Furthermore, a Chi-square test was performed to assess whether motor lateralization at evaluation (symmetrical, right or left) was associated with ROCF asymmetry copy patterns (neutral, left, or right). Finally, partial correlation analyses (Spearman, r) controlling for global cognitive status (i.e., MoCA) were performed to assess the relationship between qualitative aspects at ROCF copy and cognitive performance at executive or visuospatial tasks. Finally, receiver operating characteristic (ROC) curve analyses were conducted to determine the discriminative ability of quantitative and qualitative ROCF measures in differentiating HC from patients’ groups. Specifically, ROC curves were performed for HC versus PD-MCI and for HC versus PD-CU on BQSS variables in which significant differences were found in group comparisons. Then, performance at the neuropsychological battery was compared in PD-CU divided based on ROC-defined cut-off scores in order to highlight possible differences in cognitive performance between sub-groups. Statistical analyses were conducted using Jamovi 2.3.21.
Results
Comparison between PD-CU, PD-MCI, and controls at ROCF performance
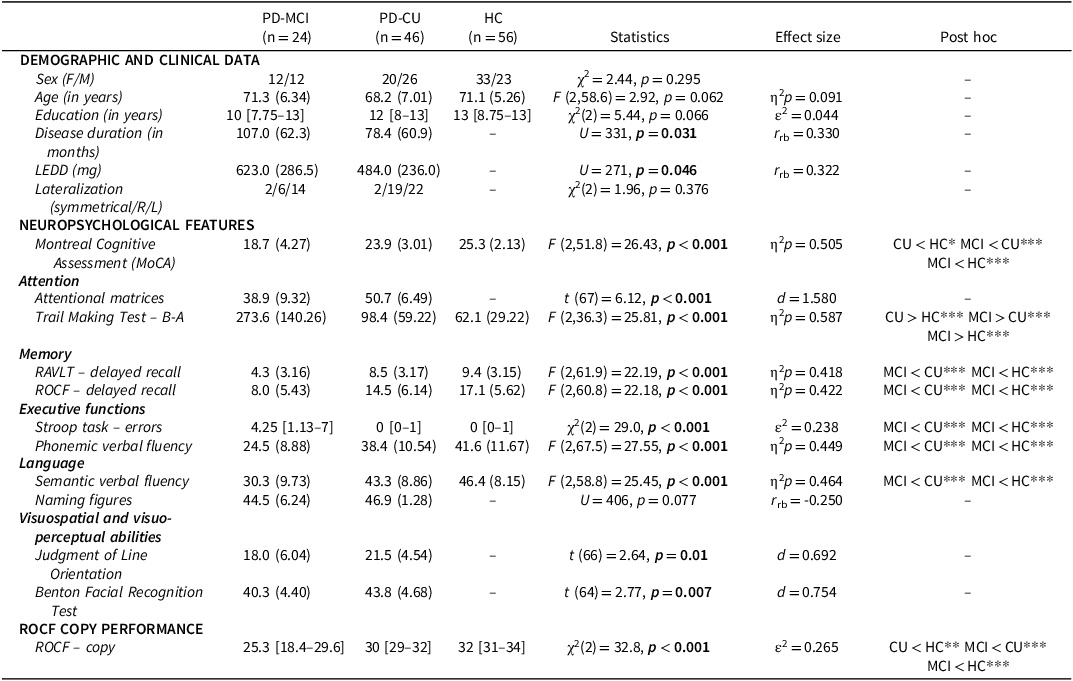
Preliminary statistical analyses showed no significant differences when comparing demographic variables between groups (see Table 1). However, significant differences emerged when comparing the neuropsychological performance. In detail, PD-MCI patients showed lower scores than both the control and the PD-CU groups in all the tests administered. Furthermore, significant differences were found between PD-CU and HC in the MoCA and Trail Making Test B-A, although all PD-CU patients performed within Italian norms. A comparison of performance on the quantitative ROCF copy scores revealed a statistically significant difference between the three groups (χ2[2] = 31.8, p < 0.001), with MCI showing the worst performance, followed by PD-CU and then HC (Table 1).
Demographic, clinical, and neuropsychological features of PD patients with (PD-MCI) and without (PD-CU) mild cognitive impairment and healthy controls (HC)

Note: ROCF = Rey–Osterrieth complex figure. Data are reported as mean (standard deviation) for parametric statistics and median [25–75th percentile] for nonparametric statistics. Raw scores are used for neuropsychological tests. Bold font – significant p-value, *p < 0.05, **p < 0.01, ***p < 0.001.
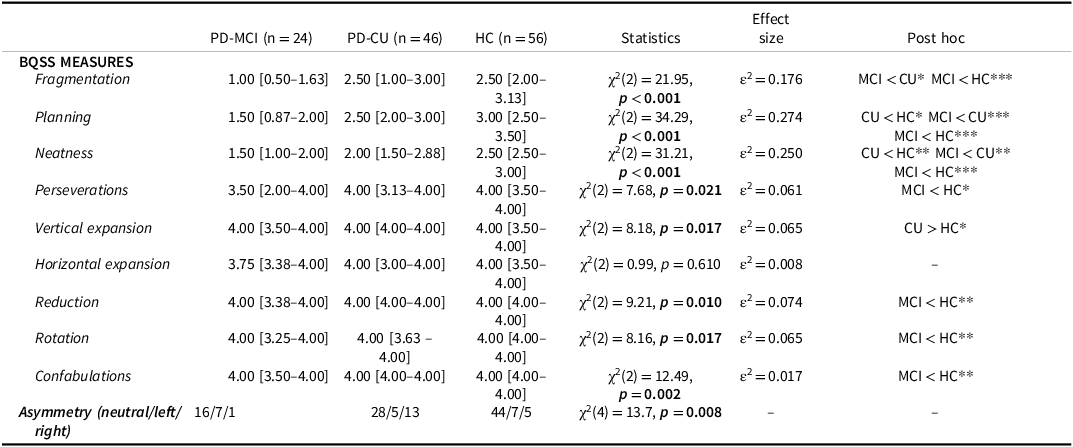
When considering ROCF qualitative aspects (see Table 2 and Figure 1A), PD-MCI were characterized, as expected, by lower performance in all BQSS measures compared to HCs except for horizontal expansion, and in fragmentation, planning, and neatness compared to the PD-CU group. Notably, PD-CU individuals were also characterized by a significant reduction in planning and neatness compared to the HC group.
(A) ROCF copy performance example for HC (a), PD-CU (b), and PD-MCI (c). (B) ROCF copy performance example of left (L) and right (R) asymmetry. Note: HC = healthy control; PD-CU = Parkinson’s disease without cognitive impairment; PD-MCI = Parkinson’s disease with mild cognitive impairment; ROCF = Rey–Osterrieth complex figure.

Comparison at the Boston Qualitative Scoring System (BQSS) scores between PD patients with (PD-MCI) and without (PD-CU) mild cognitive impairment and healthy controls (HC)

Note: Data are reported as median [25–75th percentile]. Bold font – significant p-value, *p < 0.05, **p < 0.01, ***p < 0.001. Raw scores from 0 to 4 are used for BQSS measures.
Finally, a different distribution of an asymmetric pattern of copy was found between groups.
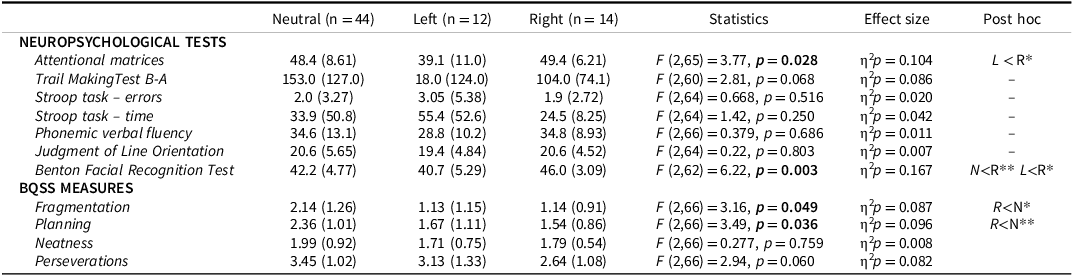
By grouping patients according to the ROCF asymmetry (Table 3 and see Figure 1B for examples), ANCOVAs showed significant differences in the performance at the attentional matrices (F[2,65] = 3.77, p = 0.028) and at the Benton Facial Recognition Test (F[2,62] = 6.22, p = 0.003). Post hoc comparisons revealed that patients with left-sided asymmetry performed significantly worse in the attentional matrices (p = 0.022) and in a visuo-perceptual task (i.e., Benton’s facial recognition test) (p = 0.004) compared to those with right-sided asymmetry. On the other hand, patients with right-sided asymmetry showed significant alterations in planning and fragmentation indices compared to patients with a symmetric performance. No other significant differences were found for the remaining neuropsychological tests analyzed (Table 3). The Chi-square test performed to evaluate possible differences in the distribution of asymmetric copy pattern based on motor lateralization revealed no significant difference (χ2[4] = 1.34, p = 0.855).
Performance comparison at neuropsychological tests and BQSS variables between patients based on ROCF copy asymmetry patterns

Note: BQSS = Boston Qualitative Scoring System; ROCF = Rey–Osterrieth complex figure. Data are reported as mean (standard deviation). Raw scores are used for neuropsychological tests. Bold font – significant p-value, *p < 0.05, **p < 0.01, ***p < 0.001.
Correlations between BQSS scores and performance in other cognitive domains
Partial correlations between PD patients’ performance and BQSS indices showed a positive association between planning and neatness scores and tests evaluating executive functions. In detail, a positive correlation was found between the scores of planning and neatness and phonemic verbal fluency – FAS (planning: r = 0.245, p = 0.042; neatness: r = 0.310, p = 0.010), while a significant negative association was found between neatness and the Stroop error index (r = −0.256, p = 0.036). In addition, positive significant correlations emerged between BQSS variables and visuospatial measures, specifically between the scores at the Judgment of Line Orientation and the indices of fragmentation (r = 0.291, p = 0.017), planning (r = 0.293, p = 0.016), and perseveration (r = 0.326, p = 0.007).
ROC analyses
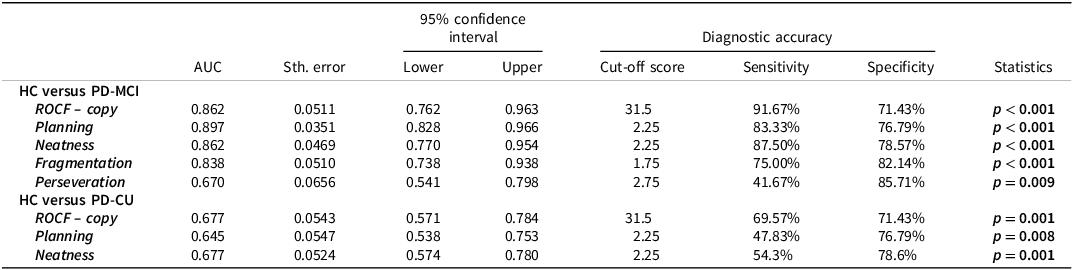
ROC analyses were then conducted to determine the ability of ROCF copy performance and BQSS indices to discriminate between HC and patients’ groups (Table 4). For HC versus PD-MCI, ROCF copy showed good discriminative accuracy (AUC = 0.862). Among the BQSS qualitative scores, planning (AUC = 0.897), neatness (AUC = 0.862), fragmentation (AUC = 0.838), and perseveration (AUC = 0.670) also had modest-to-good discriminative accuracy. For HC versus PD-CU, ROCF copy (AUC = 0.677, p = 0.001), planning (AUC = 0.645), and neatness (AUC = 0.677) showed similar discriminative accuracy.
Summary of receiver operating characteristic curve analyses in the comparisons between PD-MCI and HC and PD-CU and HC

Note: HC = healthy control; PD-CU = Parkinson’s disease without cognitive impairment; PD-MCI = Parkinson’s disease with mild cognitive impairment; ROCF = Rey–Osterrieth complex figure. Bold font – significant p-value.
PD-CU performing below cut-off at ROCF copy showed exclusively reduced verbal fluency on phonemic cue (t(44) = −2.881, p = 0.006) compared to PD-CU performing above the cut-off score, while PD-CU patients showing scores below the ROC-defined cut-off score in planning were characterized by a reduced performance at MoCA (U = 162, p = 0.024), ROCF delayed recall (t(44) = −2.283, p = 0.021), Stroop task errors (U = 168, p = 0.045) and verbal phonemic fluency (t(44) = −1.509, p = 0.034). No significant differences were instead found when comparing PD soubgroups based on neatness scores (i.e., impaired vs unimpaired) (all p > 0.05).
Discussion
Constructional apraxia is a cognitive disorder observed in PD, particularly in patients with cognitive impairment (Trojano & Gainotti, Reference Trojano and Gainotti2016). Copying complex figures requires multiple cognitive functions, including visuospatial processing, executive control, and motor planning, which may be differentially affected depending on patients’ cognitive profile (Barvas et al., Reference Barvas, Mattavelli, Zappini, Giardina, Ottaviani and Papagno2021). In this study, we provide evidence of early qualitative changes in PD patients without overt cognitive impairment, thus contributing to a better understanding of the relationship between clinical-cognitive phenotypes and drawing abilities in this neurodegenerative condition.
While previous studies have confirmed qualitative alterations in drawing tasks among PD patients with cognitive impairment (Allone et al., Reference Allone, Lo Buono, Corallo, Bonanno, Palmeri, Di Lorenzo, Marra, Bramanti and Marino2018; Saur et al., Reference Saur, Maier, Milian, Riedel, Berg, Liepelt-Scarfone and Leyhe2012; Scarpina et al., Reference Scarpina, Ambiel, Albani, Pradotto and Mauro2016), to the best of our knowledge, no evidence is currently available regarding such alterations in well-characterized cognitively unimpaired individuals (PD-CU).
In this study, we report, for the first time, reduced neatness and altered planning abilities in PD patients without clinically detectable cognitive deficits on standard neuropsychological assessments.
A recent study by Caselli et al. (Reference Caselli, Langlais, Dueck, Chen, Su, Locke, Woodruff and Reiman2020) suggested that subtle alterations in ROCF copying may serve as an early marker of cognitive decline, potentially appearing up to 20 years before symptom onsetReference Caselli, Langlais, Dueck, Chen, Su, Locke, Woodruff and Reiman. Similar findings have been reported in Lewy Body Disease, where qualitative alterations in drawing tasks are described in prodromal stages (Cagnin et al., Reference Cagnin, Bussè, Jelcic, Gnoato, Mitolo and Caffarra2015), and in patients with REM sleep behavior disorder (Galbiati et al., Reference Galbiati, Carli, Dodich, Marelli, Caterina, Cerami, Zucconi and Ferini-Strambi2019).
The findings of the current study thus suggest that qualitative alterations in drawing tasks may reflect early cognitive inefficiencies in PD patients who do not exhibit overt cognitive impairment.
Although PD-CU patients showed lower performance at group level compared to HC in the ROCF copy when considering the quantitative parameter, all these patients scored within normative range based on the Italian normative cut-offs. This apparent discrepancy could be explained by the significant differences observed in planning and neatness, which contribute to affect the overall performance. Thus, qualitative information, and particularly planning, might be a useful parameter to be added in the clinical assessment, as it might represent the presence of subtle cognitive alterations. These results are overall in line with previous evidence showing the presence of subtle cognitive dysfunctions also in PD-CU individuals, who do not meet the criteria for MCI according to MDS criteria (Litvan et al., Reference Litvan, Goldman, Tröster, Schmand, Weintraub, Petersen, Mollenhauer, Adler, Marder, Williams-Gray, Aarsland, Kulisevsky, Rodriguez-Oroz, Burn, Barker and Emre2012), and with the results of the ROC analyses.
In fact, when comparing PD-CU to HCs, the quantitative and qualitative indices showed similar discriminative accuracy. However, PD-CU patients performing below the cut-off score on planning based on ROC results demonstrated lower scores across multiple executive function tasks compared to the other PD-CU subgroup. This supports the hypothesis that assessing planning strategies in PD-CU may help in detecting early signs of selective executive dysfunctions, even though these patients are still clinically classified as cognitively unimpaired. Thus, qualitative measures may provide complementary information about executive changes in PD patients, poorly detected by quantitative scores representing the overall visuo-constructive performance. Future longitudinal studies should be devoted to disentangling the possible role of these subtle alterations in predicting conversion to MCI. Early MCI detection is crucial, as it is linked to an increased risk of developing dementia, which carries significant social and economic burdens (Aarsland et al., Reference Aarsland, Batzu, Halliday, Geurtsen, Ballard, Ray Chaudhuri and Weintraub2021). Therefore, incorporating qualitative assessments into longitudinal studies may help identify PD patients at higher risk for cognitive deterioration.
The results of the correlational analyses confirmed a significant association between planning and neatness scores and executive functioning across the entire group, rather than with visuospatial impairments. These results once again support the hypothesis that executive alterations, rather than pure visuospatial deficits, contribute to impaired performance when copying complex drawings in PD, at least in the early stages (Allone et al., Reference Allone, Lo Buono, Corallo, Bonanno, Palmeri, Di Lorenzo, Marra, Bramanti and Marino2018; Freeman et al., Reference Freeman, Giovannetti, Lamar, Cloud, Stern, Kaplan and Libon2000; Saka & Elibol, Reference Saka and Elibol2009). Notably, patients with poor neatness predominantly exhibited overwritten lines, which have previously been interpreted as a symptom of impulsivity (Scarpina et al., Reference Scarpina, Ambiel, Albani, Pradotto and Mauro2016), and the significant correlation between neatness and loss of inhibitory control (i.e., Stroop error index), also supported by similar observations in atypical Parkinsonism (Tommasini et al., Reference Tommasini, Bonaccorsi, Del Prete, Cintoli, Pagni, Mazzucchi, Palermo, Morganti, Frosini, Siciliano, Tognoni and Ceravolo2023), suggests that inhibitory deficits may manifest as difficulties in suppressing current movements beyond the appropriate request.
Another relevant finding of the current study is the presence of asymmetric drawing patterns in these patients. Although these alterations were not linked to motor lateralization, significant differences were observed in the cognitive profiles of patients with left versus right asymmetry. Patients who exhibited omissions in the copy of the right ROCF portion also demonstrated poorer planning abilities and a higher degree of fragmentation in the figure elements compared to other patients. Conversely, patients with a left-sided asymmetry showed reduced visuo-perceptual and attentional abilities, as evidenced by their performance at the neuropsychological tasks. Given previous evidence linking drawing disabilities to lower planning abilities in patients with left brain damage (Hécaen & Assal, Reference Hécaen and Assal1970) and to impairments in visuo-perceptual tasks in those with right brain damage (Trojano et al., Reference Trojano, Fragassi, Chiacchio, Izzo, Izzo, Di Cesare, Cristinzio and Grossi2004), as well as the known right lateralization of the attentional network (Corbetta & Shulman, Reference Corbetta and Shulman2002), these differences between individuals with left/right asymmetries might likely correspond to asymmetric vulnerabilities at the brain level (Raimo et al., Reference Raimo, Boccia, Di Vita, Cropano, Guariglia, Grossi and Palermo2021). However, it cannot be excluded that the neuropsychological correlate of this asymmetry could reflect the different prevalence of left/right asymmetry in PD-MCI (i.e., higher prevalence of left asymmetry) and PD-CU (i.e., higher prevalence of right asymmetry). Besides, the absence of a significant difference in motor lateralization distribution between PD patients and ROCF asymmetry does not fully support this hypothesis. Since no imaging data is available to evaluate the association between lateralized performance and functional/structural degeneration to the contralateral hemisphere, we cannot exclude that the asymmetry detected might be due to poor global planning or deficient sustained attention. Future studies incorporating imaging techniques, as well as quantitative data about omissions and asymmetrical alterations, are needed to evaluate the potential impact of asymmetric neurodegeneration on drawing performance in PD or to define whether these phenotypes might be representative of specific underlying pathologies (e.g., vascular disease).
This study is not exempt from other limitations. First, the sample size is relatively small, and the findings should be replicated in a larger group of patients. Additionally, the absence of neuroimaging biomarkers limits our ability to link cognitive performance with the underlying neurodegenerative patterns, which could provide valuable insights into behavioral differences, such as those observed in ROCF asymmetry. Although no relationship was found between motor lateralization and drawing asymmetry, it is important to note that this information was derived from clinical records. Future studies should incorporate quantitative measures of motor dysfunction (e.g., UPDRS part III) to assess in depth this relationship, as well as the qualitative production of the ROCF delayed recall. In fact, to the best of our knowledge, no study on neurodegenerative conditions has yet assessed the applicability of qualitative indices in detecting executive and visuospatial alterations in the delayed recall performance. Finally, it is important to acknowledge that the BQSS is not an open-access tool, which might limit its availability for clinical or research use.
In conclusion, qualitative alterations in ROCF copy performance might characterize PD individuals without clinically detectable cognitive decline and could be linked to subtle executive dysfunctions. These results open a new perspective in the investigation of early cognitive indices of progression in PD and invite further investigation of these aspects in longitudinal studies including biomarkers.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing interests
None.


 Open access
Open access