Irritable bowel syndrome (IBS) is a common gut–brain interaction medical condition, generally identified by chronic and recurring abdominal pain and discomfort, along with changes in bowel habits. These symptoms typically occur without any other underlying organic gastrointestinal (GI) disease(Reference El-Salhy, Hatlebakk and Hausken1). Moreover, it has been linked to a significant decrease in health-related quality of life, concomitant to an increased occurrence of somatisation and a higher likelihood of psychological comorbidities, such as depression and suicidal tendencies. Additionally, IBS can lead to work impairment and result in higher medical and prescription expenses, annually. Furthermore, IBS may have a considerable impact on the costs incurred by both primary and secondary healthcare providers(Reference Oka, Parr and Barberio2).
The prevalence of IBS differs substantially between countries and regions. The most recent worldwide studies on functional GI disorders employed the new Rome IV criteria, which are stringent in identifying IBS. As a result, the current global prevalence of IBS is approximately 4·6 %, which is nearly half of what was previously reported with the use of other Rome criteria(Reference Galica, Galica and Dumitrașcu3). While there is no precise data available for the occurrence of IBS in Iran, various studies have indicated a broad range of prevalence, from 1 to 21 percent, among different population groups in Iran(Reference Mansouri, Rarani and Fallahi4). Further, it is apparent that women and people under the age of 50 years are affected more by this condition, although no consensus has been reported(Reference Galica, Galica and Dumitrașcu3).
Currently, no treatment for this disorder exists, largely due to the limited diagnostic and therapeutic approaches. Pharmacological treatments, psychotherapy, probiotic supplementation and dietary modifications are among the available therapeutic strategies; however, these treatments have not been effective and generalisable across patient groups(Reference Defrees and Bailey5–Reference Ford, Moayyedi and Chey7). Nevertheless, epidemiological studies continue to investigate the pathophysiology of IBS, in an effort to identify suitable treatments. The aetiology of IBS is not completely established; however, numerous factors are thought to play a pivotal role in the pathophysiology of IBS. These factors include genetics, altered gut microbiota, abnormal colonic motility or transit, increased colonic bile acid concentration, intestinal or colorectal sensation and low-grade colonic mucosal inflammation, along with epithelial barrier dysfunction, up-regulation of neurohormones, activation of secretory processes in the epithelial layer, psychological disturbance and diet(Reference Camilleri8,Reference Fukudo, Okumura and Inamori9) . Among these risk factors, dietary factors are regarded as crucial due to the widespread and inevitable impact on the overall health of individuals. The focus of nutritional studies in IBS has primarily been on alleviating symptoms and treatment of the disease, rather than the association of food and disease risk. Numerous studies have examined the nutritional status of IBS patients, as well as the effects of dietary interventions, such as low fermentable oligosaccharides, disaccharides, monosaccharides and polyols, gluten-free and lactose-free diets, elimination diets, probiotics and synbiotics and fibre, in reducing symptoms(Reference Galica, Galica and Dumitrașcu3,Reference Hujoel10,Reference Dionne, Ford and Yuan11) . However, studies investigating the association between diet and the risk of IBS are scarce. For instance, Lari et al. reported that there was no significant association between dietary polyphenols and odds of IBS(Reference Lari, Shidfar and Aminianfar12). Moreover, Roudi et al. showed a significant positive association between caffeine intake and the risk of IBS, although no significant association between fibre and IBS risk was shown(Reference Roudi, Khayyatzadeh and Ghazizadeh13). The aforementioned studies mainly investigate the association of single nutrients and food items with IBS risks, where the interaction between the dietary components and their composite effects on IBS risk was not evaluated. Recently, epidemiological studies have tended to assess the association of dietary indices, such as the dietary quality index-international (DQI-I), healthy eating index, Mediterranean diet Score, dietary approaches to stop hypertension and dietary inflammatory index, with the odds of chronic diseases, such as cancers and cardiometabolic disease, as a new approach for the prediction of the relationship between total diet quality (rather than single nutrients and food groups) and disease risk(Reference Daneshzad, Larijani and Azadbakht14,Reference Du, Li and Su15) . Salari-Moghaddam et al. reported that adherence to proinflammatory diet, examined by the dietary inflammatory index, was associated with higher odds of IBS in a cross-sectional study. Further, Eslampour et al., in a case–control study, showed that a higher inflammatory diet was associated with a higher risk of IBS(Reference Eslampour, Ghanadi and Aghamohammadi16,Reference Salari-Moghaddam, Keshteli and Esmaillzadeh17) . However, the results from Saneie et al. suggested no significant association between dTAC and IBS risk(Reference Saneie, Aminianfar and Shidfar18). Although these studies considered the overall diet in their investigation, they, again, examined a specific aspect, namely the inflammation and oxidative status of the diet. Whereas, other indices, such as DQI-I, take more aspects of diet into account. DQI-I is used as an effective method for cross-national comparisons and has been utilised to quantify the diet quality of populations and evaluate its association with chronic disease(Reference Chan, Wong and Chu19). Identifying dietary issues through the DQI-I could be beneficial in identifying and creating strategies to improve public health prevention programmes(Reference Sharifi, Izadpanah and Hosseini20). Moreover, Ebrahimi et al., in a comparison of diet quality indices use in the Iranian population, indicated that DQI-I is more applicable in the evaluation of nutrient adequacy(Reference Ebrahimi, McNaughton and Leech21). In view of the paucity of evidence pertaining to the relationship between DQI-I and IBS and the relatively high prevalence of IBS in Iran, this study sought to assess the association between DQI-I and IBS odds in a sample of Iranian individuals.
Method
Design and participants
This case–control study was conducted within the framework of the ISFUN (The Isfahan functional disorders) population-based prospective cohort study. The ISFUN cohort study has a twofold goal: firstly, to explore how genetic and environmental factors interact to influence the features of functional somatic syndromes, and secondly, to investigate the epidemiology, risk factors, course and prognosis of functional somatic syndrome in a sample of Iranian adults. Another aim of the study is to establish a novel definition of functional somatic syndrome that integrates phenotypic and multi-omics data using a multidisciplinary approach. Details about the ISFUN project have been published elsewhere(Reference Adibi, Ani and Vaez22). Briefly, this study was designed to follow a group of apparently healthy individuals aged 18–65 years over a period of 4 years through yearly visits. Exclusion criteria for this cohort study were as follows: pregnant women, individuals with non-communicable diseases, such as cancer or undergoing pharmacological treatment, individuals with chronic diseases in the active phase of the disease and undergoing treatment, individuals with mental disorders (such as severe depression, psychosis, etc.) and house-bound people who were unable to participate and attend the health centre. Questionnaire data (functional symptoms, psychological assessment, lifestyle evaluation, quality of life, dietary assessment, physical activity level and socio-demographic information), physical examination and anthropometric measurements, blood, stool and urine samples were gathered at baseline as well as during subsequent yearly visits. Genomic, microbiota and metabolomics profiling was conducted through DNA genotyping, microbial amplicon sequencing and urine analysis. The study began in September 2017 and concluded in 2022, with 1935 participants initially recruited.
In the current study, 100 IBS cases, as well as 310 healthy controls, were included in the first phase of the cohort. IBS cases were patients, aged 18–50 y, diagnosed with IBS according to ROME IV criteria by gastroenterologists. The control group was randomly selected from the healthy patients from the first phase of the ISFUN cohort. Data on cases and controls were gathered at the same time and in the same setting. This study was conducted according to the guidelines in the Declaration of Helsinki and all procedures involving human subjects/patients were approved by the Research Ethics Committee of Isfahan University of Medical Sciences (IR.MUI.RESEARCH.REC.1401·370). Written informed consent was obtained from all subjects/patients.
Sample size estimation
According to a relatively similar study conducted on IBS by De Graff et al. (Reference de Graaf, Spooren and Hendrix23), and taking into account a type I error rate (α = 5 %), statistical power of 80 % and a minimum detectable standardised effect size of 0·4 (Δ) for DQI-I, with a control group being three times larger than the case group (φ = 3), the required sample size was estimated using the following formula. Accordingly, the necessary sample size for the case group was 100, and the control group was 310.
 $$n={{\left(1+\varphi\over \varphi\right)}}{{(z_{1-\alpha/2}+z_{1-\beta})^2}\over{\Delta^2}}+{{z_{1-\alpha/2}^2}\over{2(1+\varphi)}}$$
$$n={{\left(1+\varphi\over \varphi\right)}}{{(z_{1-\alpha/2}+z_{1-\beta})^2}\over{\Delta^2}}+{{z_{1-\alpha/2}^2}\over{2(1+\varphi)}}$$
Inclusion and exclusion criteria
Inclusion criteria for this case–control study are as follows: (a) adults with the age of 18–50 y, (b) newly diagnosed IBS, (c) having no history of celiac, GI surgery or other chronic GI diseases. Exclusion criteria were as follows: (a) being on a special diet, (b) reporting total daily energy intakes outside the range of 800–4200 kcal/d. As mentioned above, participants were selected in the framework of a cohort study. Therefore, the same screening tools have been used for the assessment of the dependent, independent and confounding variables in cases and controls (which are explained fully in the following sections). The same inclusion and exclusion criteria, except for those suffering from IBS, were used for control selection. Three controls for each confirmed case were considered.
Initially, participants were asked about their medical histories regarding various diseases such as cancers, CVD, diabetes, hypertension, fatty liver, epilepsy, mental disease, etc. and the medications they were currently taking. Additionally, all participants completed questionnaires assessing stress and anxiety, as well as the Rome IV criteria and other GI questionnaires, and underwent medical examinations. Based on this assessment, 721 patients were diagnosed with functional GI disorder and excluded from the control selection process and 1171 participants had no functional GI disorder. For this study, 310 individuals were randomly selected from those 1171 participants. Also, forty-three people were excluded from the study due to missing data and reporting energy outside the expected range.
Assessment of dietary intakes and dietary quality index international measurement
Dietary data over the past year were obtained through a Willett-format dish-based 106-item semi-quantitative FFQ (DB-FFQ) that was developed and validated for the Iranian population. Comprehensive information about the design, the food items included and the validity of the questionnaire was published somewhere else(Reference Keshteli, Esmaillzadeh and Rajaie24). Briefly, the questionnaire contained five categories of foods and dishes: (1) mixed dishes (twenty-nine items of mixed cooked or canned dishes) (2) grains (ten items: different types of bread, cakes, biscuits and potatoes); (3) dairy products (nine items: low-fat milk, high-fat milk, yoghurt, dough (a fermented yoghurt drink), curd, butter, cheese and cream); (4) vegetables and fruits (twenty-two items) and (5) miscellaneous food and beverages (thirty-six items: sweets, fast foods, desserts, nuts and beverages). Participants were asked to indicate how often they ate each food item using six to nine frequency response options, ranging from “never or less than once a month” to “12 or more times per day. The frequency response option was not constant for all foods and was defined according to the common frequency of the items’ consumption. For infrequently consumed foods, the high-frequency categories were eliminated. In the case of frequently consumed common foods, the number of multiple-choice categories was increased to nine. For instance, the frequency consumption for tuna had six options and for tea, nine options, respectively. Eventually, the food items were converted into grams by calculating the portion size using the “household measures” booklet. The amount of intake was then determined by taking into account the frequency of consumption for each food item. A customised version of Nutritionist IV software for Iranian foods was utilised to acquire the nutrient intakes of each participant.
DQI-I was calculated based on the criteria proposed by Kim et al. (Reference Kim, Haines and Siega-Riz25). DQI-I assesses the overall quality of a diet based on its nutritional variety, adequacy, moderation and balance together. Variety score ranges between 0 and 20. It consists of an overall variety of five food groups (0–15 points) and protein variety (0–5). The adequacy component score ranges between 0 and 40 and consists of vegetables, fruit, grain, fibre, protein, Fe, Ca and vitamin C that are necessary to ensure a healthy diet (0 and 5 points awarded for each). The moderation component score ranges between 0 and 30 and evaluates total fat, saturated fat, cholesterol, Na and empty-calorie foods that are associated with chronic diseases. Empty calorie percent is estimated based on the portion of added sugar, discretionary fat and alcohol, as a proportion of total energy. Balance component considers macronutrients ratio to energy intake ratios (0–6 points awarded) and fatty acid ratio according to three types of fatty acids including SFA, MUFA and PUFA (0–4 points awarded). Lastly, each component score in four categories is summed to measure the final DQI score. The total score could range from 0 to 100 with higher DQI-I scores indicating higher dietary quality. In this study after calculating DQI-I scores, participants were classified in tertiles (<58, 58–64·66, > 64·66).
Assessment of irritable bowel syndrome
Diagnosis of IBS was made using ROME IV criteria via a self-report questionnaire and then approved by associated gastroenterologists. A fixed medical team interviewed the participants and made sure that all the questions were understood and answered. Furthermore, interview-based diagnosis were recorded as well. According to these criteria, an individual was considered as having IBS if they experienced recurrent abdominal pain, occurring at least 1 day a week during the past 3 months, associated with at least two or more of the following: a. defecation; b. change in frequency of stool; c. change in stool appearance(Reference Yang, Wei and Liu26).
Assessment of other variables
Data on demographic characteristics including sex, age, education, marital status, smoking status (former and current smoker), past medical history, chronic disease history were gathered via a standard questionnaire. socio-economic status was assessed using Persian validated socio-economic status short-form questionnaire(Reference Roohafza, Feizi and Gharipour27). Dietary habits (meal pattern, chewing sufficiency and fluid consumption) were assessed through a pretested questionnaire(Reference Adibi, Hassanzadeh Keshteli and Esmaillzadeh28).
Depression and anxiety symptoms were evaluated using the Hospital Anxiety and Depression Scale questionnaire that has been validated in Iran(Reference Montazeri, Vahdaninia and Ebrahimi29). This questionnaire consists of fourteen items, divided into two separate subscales assessing symptoms of depression and anxiety. Each section has a four-point rating scale. Hence, the overall score ranges from 0 to 21 (0 showing the lowest and 21 showing the highest degree of depression and anxiety). In this study, a score of ≤7 in each subscale was regarded as ‘not having anxiety and depression and scores of ≥8 were regarded as ‘having’ the conditions.
Anthropometric measurements were administered by trained staff. Height was measured using a nonelastic tape measure to the nearest 0·5 cm, when standing barefoot in a normal position. Participants’ weight was measured to the nearest 100 g using a digital scale, with participants in light clothing. BMI was calculated by dividing weight (kg) by height (m2), and waist circumference was measured at a level midway between the lower rib margin and the iliac crest using a tape horizontally fixed around the body. Hip circumference was measured by an inelastic meter, at maximum circumference over the buttocks. Physical activity was assessed using the International Physical Activity Questionnaire, which consists of 27 questions with 5 domains (work time activity, housework, leisure time, transportation and sitting). It asks about individuals’ physical activity intensity in the past 7 days as a part of daily life. Data from International Physical Activity Questionnaire were converted to metabolic equivalent minutes/week using existing guidelines(Reference Booth30).
Statistical analysis
In this study, participants were categorised based on tertile cut-off points of DQI-I score. Normality of continuous variables was evaluated using the Kolmogorov–Smirnov test and Q–Q plot. Data on general characteristics and energy-adjusted dietary intakes of study participants in cases and controls, and also across tertiles of the DQI-I score, are shown as means ± sd for continuous variables and frequencies and percentages for categorical variables. Comparisons of continuous basic characteristics between cases and controls were performed using independent samples t-tests, while one-way ANOVA was used for comparisons across tertiles of DQI-I. Categorical variables were compared using the chi-squared test. Comparisons of dietary intake between cases and controls were conducted using independent samples Hotelling’s T2, and multivariate analysis of variance (MANOVA) was used for comparisons across tertiles of DQI-I score.
Binary logistic regression was utilised to estimate OR and 95 % CI for the association of DQI-I and IBS odds in total and sex-stratified populations in the crude and multivariable-adjusted models. Potential confounding variables in multivariable models were selected if they had a biological or statistical association with both dependent and independent variables or at least with dependent variable at P < 0·1. We examined all potential confounders based on the above criteria, and finally, we included age, sex, BMI, socio-economic status, chronic disease, dietary habits including regular meal pattern, chewing sufficiency, fluid consumption and energy intake which affect the results effectively. We fitted five models including crude model, model 1: adjustment was made for age and sex, model 2: additionally, adjustment was made for BMI, socio-economic status, chronic disease (at least one disease including depression and anxiety), model 3: more adjustment was done by entering dietary habits (regular meal pattern, chewing sufficiency, fluid consumption) and finally in model 4, energy intake was added to previous confounders. We performed stratified logistic regression analysis by sex after observing a significant interaction effect between sex and our predictor variable in association with the dependent variables. Variance inflation factor was used for detecting multicollinearity, and a value of more than 5 was considered as evidence of its’ presence(Reference Vatcheva, Lee and McCormick31). Statistical significance was accepted at P < 0·05. All presented P-values in multiple logistic regression were adjusted for multiple testing using Benjamini–Hochberg correction(Reference Benjamini, Hochberg and JotRsss32). SPSS software (version 20; IBM Corp. Released 2011, IBM SPSS Statistics for Windows, Version 20·0. Armonk, NY: IBM Corp.) was used for performing statistical analysis.
Results
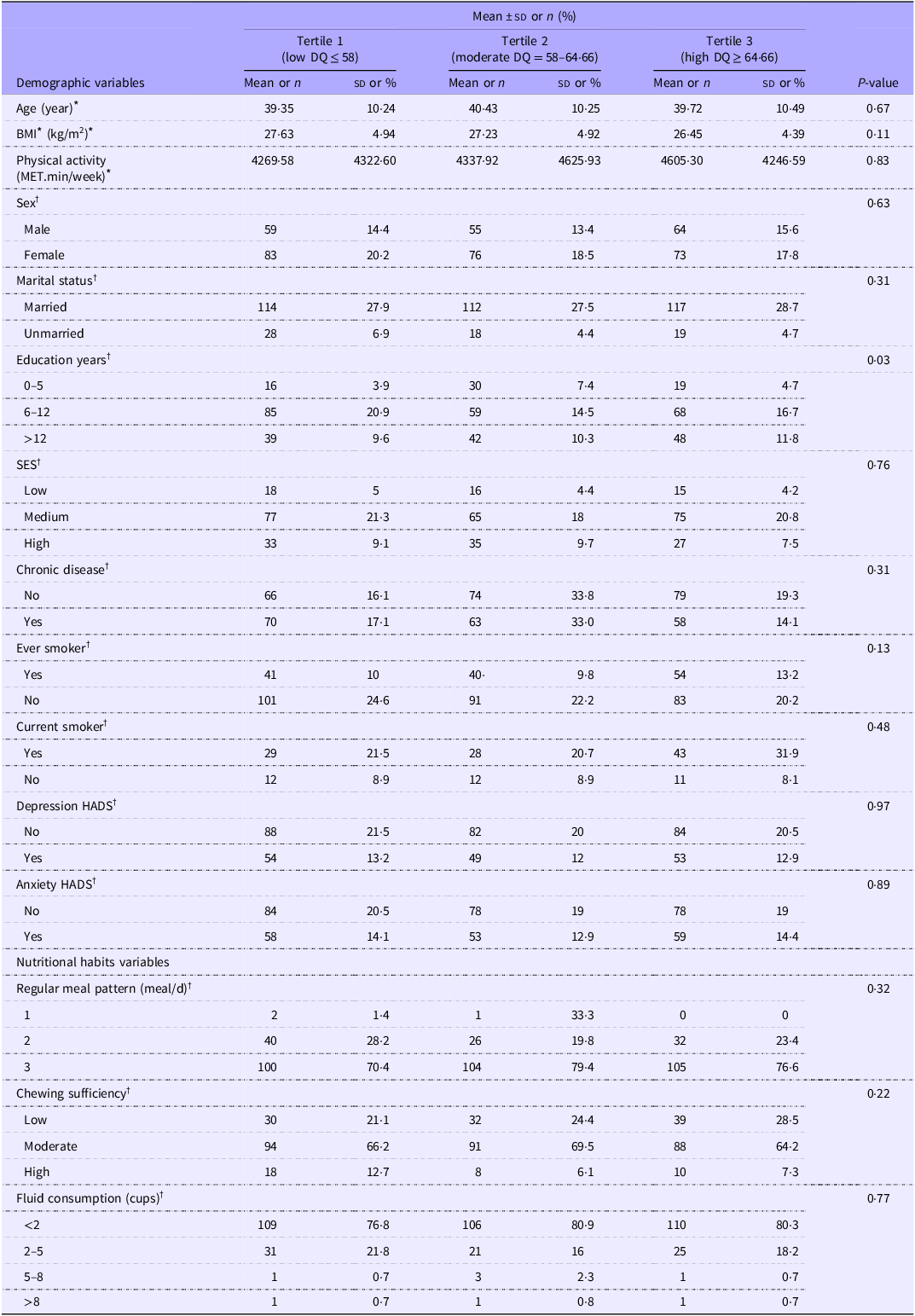
Overall, data from 100 IBS cases and 310 healthy controls were analysed. Table 1 presents the general characteristics of study participants separately by cases and controls. The cases of IBS had higher BMI levels, a history of at least one chronic disease, a history of smoking, depression, anxiety and lower levels of socio-economic status and physical activity and chewing sufficiency. However, only BMI (P = 0·04), chronic disease (P = 0·01), depression (P < 0·001) and anxiety P < 0·001) were significantly different between groups.
Comparing the basic demographic, lifestyle and clinical characteristics of study participants between case and control group

SES, socio-economic status; HADS, Hospital Anxiety and Depression Scale.
* Continuous data is shown as mean ± sd and was analysed by independent two samples t-test.
† Categorical data are presented as numbers (%) and were analysed by χ 2 test.
P < 0.05 was considered as statistically significant.
Table 2 shows the general characteristics of participants across tertiles of DQI-I. Comparing tertiles of DQI-I showed a higher percentage of individuals with more than 12 years of education in the highest tertile of DQI than in the lowest tertile (P = 0·03). Moreover, no significant difference was seen in the distribution of participants in terms of age, education, marital status, gender, BMI, socio-economic status, history of chronic disease, smoking, depression, anxiety and having regular meal patterns, chewing sufficiently and fluid consumption across categories of DQI-I.
Distribution of study sample’s characteristics across tertiles of dietary quality index international (DQI)

DQ, dietary quality; SES, socio-economic status; HADS, Hospital Anxiety and Depression Scale.
* Continuous data is shown as mean ± sd and was analysed by analysis of variance.
† Categorical data are shown as numbers (%) and were analysed by χ 2 test.
P < 0.05 was considered as statistically significant.
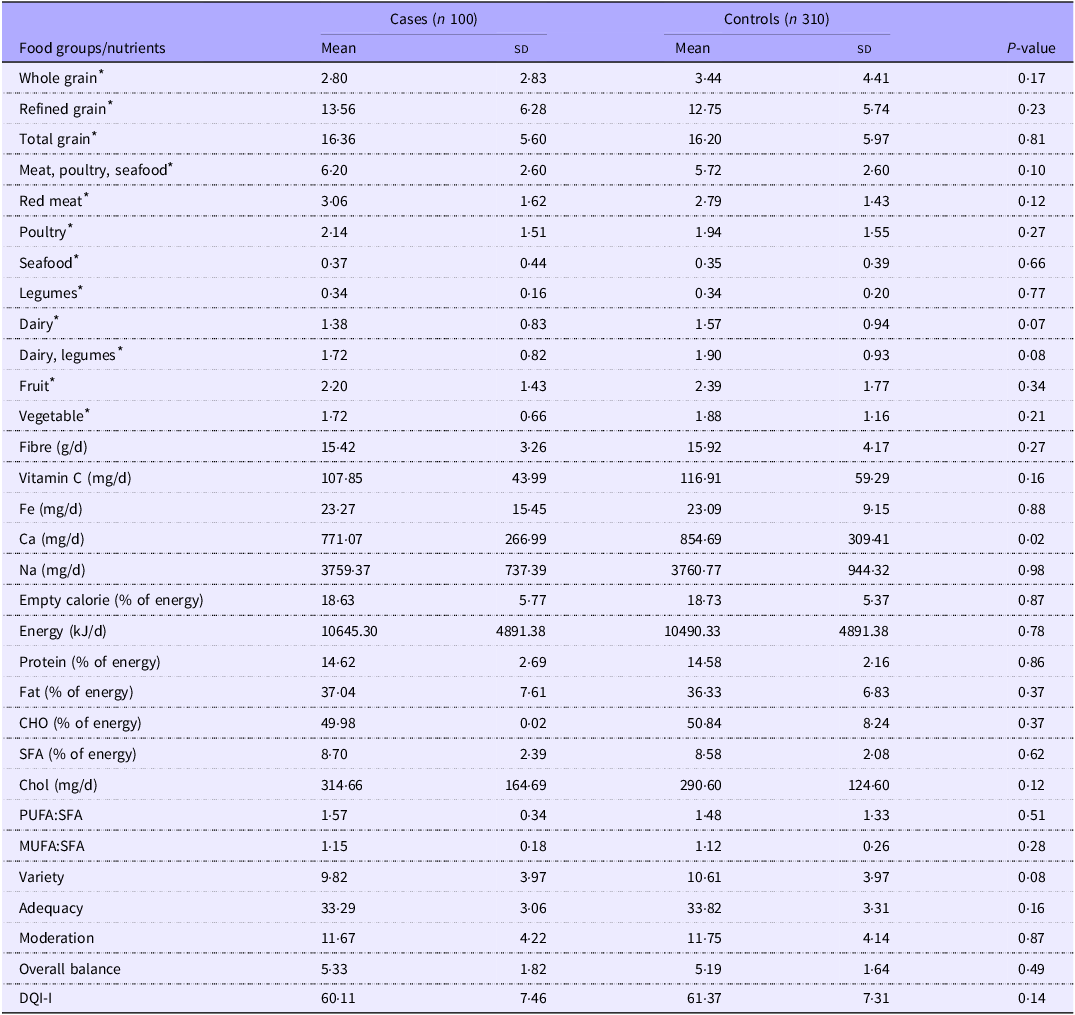
The average dietary intakes of participants separately by cases and controls are summarised in Table 3. These nutrients and food groups are those which have been used in calculating the DQI-I score. The patients with IBS had higher intakes of refined grains, total grains, meat, poultry, sea food, red meat, iron, energy, protein, total fat, SFA and cholesterol. Also, PUFA:SFA and MUFA:SFA were higher in IBS cases. However, these differences did not reach statistically significant levels. Although controls had higher intakes of whole grains, dairy products, fruit, vegetables, fibre, vitamin C, calcium, variety, adequacy, moderation and DQI-I total score, the difference between the two groups was not significant.
Distribution of selected dietary intakes between case and control groups

CHO, carbohydrate; DQI-I, diet quality index international; nutrients and food groups used in calculating DQI-I overall score.
Data are shown as mean ± sd and were analysed by two independent samples Hotelling t-test.
All the food groups and nutrients are energy-adjusted.
* are represented as servings/day.
P < 0.05 was considered as statistically significant.
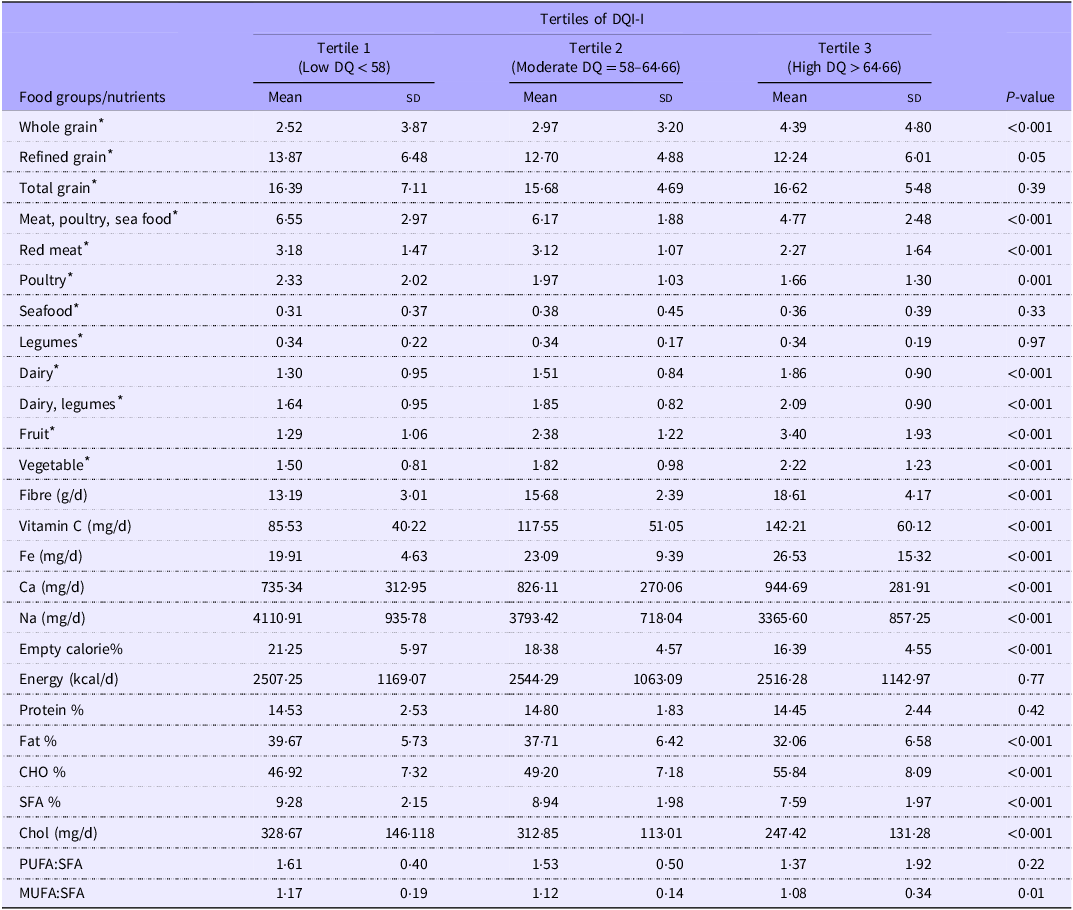
Table 4 shows the dietary intake of participants across tertiles of DQI-I. The consumption of whole grain, dairy and legumes, fruits, vegetables, fibre, vitamin C, Fe, Ca, CHO and PUFA to SFA ratio was increased significantly with an increase in DQI-I tertiles. Furthermore, mean intakes of refined grains, meat, poultry, seafood group, red meat, poultry, sodium, empty calories, fat, SFA, cholesterol and MUFA to SFA ratio decreased significantly with an increase in tertiles of DQI-I (P < 0·05).
Distribution of dietary intakes across tertiles of dietary quality index international (DQI-I)

DQ, dietary quality; CHO, carbohydrate.
Data are shown as mean ± sd and were analysed by MANOVA.
All the food groups and nutrients are energy-adjusted.
* are represented as servings.
P < 0.05 was considered as statistically significant.
Crude and multivariable-adjusted OR and 95 % CI for the association of DQI-I with IBS in total and gender-stratified samples across tertile are presented in Table 5. Compared to those in the highest tertile of DQI-I scores, participants in the lowest tertile had higher odds of suffering from IBS in the crude model (OR: 1·81; 95 % CI: 1·03, 3·20, P = 0·03). After controlling for age and gender the association remained significant (OR: 1·80; 95 % CI: 1·02, 3·18, P = 0·04) but in three other adjusted models, we found no significant association between DQI-I scores and IBS odds. In addition, when gender stratified analysis was done, no significant association was observed between DQI-I score and IBS odds in men and women.
OR and 95 % CI IBS risk across categories of the DQI-I score in total sample and gender-stratified population

Tertile 1 indicates the lowest levels of DQI-I score and Tertile 3 indicates the highest levels of DQI-I score.
* Adjusted for age-sex and adjusted only for age in gender-stratified model.
† Adjustment was made for age, sex, BMI, socio-economic status, chronic disease (at least one disease including depression and anxiety).
‡ Adjustment was made for age, sex, BMI, socio-economic status, chronic disease, dietary habits (regular meal pattern, chewing sufficiency, fluid consumption).
§ Adjustment was made for age, sex, BMI, socio-economic status, chronic disease, dietary habits including regular meal pattern, chewing sufficiency, fluid consumption and energy.
Discussion
To the best of our knowledge, this is the first study to investigate the association between DQI-I and the odds of IBS. Accordingly, in this case–control study, we found that, although higher DQI-I scores were associated with lower odds of IBS in crude and age-sex-adjusted models, no significant association was observed between DQI-I and IBS when we adjusted the results for multiple confounders. Moreover, the results were not significant in sex-stratified models.
Considering the uncertainty about the aetiology of IBS, recognizing and altering its contributing factors could be useful in ascertaining a beneficial treatment and management approach. Although there has not been a similar study that specifically investigated the relationship between DQI-I and IBS, the association between other dietary quality indices with GI disorders including IBS has been explored in some recent studies. Indeed, in a cross-sectional study by Soltani et al., it was reported that higher adherence to dietary approaches to stop hypertension diet was associated with lower odds of IBS(Reference Soltani, Keshteli and Esmaillzadeh33). Zito et al., in a survey from southern Italy, demonstrated an inverse association between adherence to a mediterranean diet and IBS prevalence and GI symptoms(Reference Zito, Polese and Vozzella34). Nevertheless, Chen et al. in a case–control study expressed that adherence to the MED diet was not correlated with IBS symptoms(Reference Chen, Mahurkar-Joshi and Liu35). Moreover, Sanie et al. showed no association between dTAC and IBS risk(Reference Saneie, Aminianfar and Shidfar18), whilst Nourimajd et al. observed no significant association between Mind diet adherence and IBS(Reference Nouri-Majd, Salari-Moghaddam and Keshteli36). Similar to our study, Mobasheri et al. indicated that the association of dietary acid load was only significant with IBS in the crude model(Reference Mobasheri, Shidfar and Aminianfar37). The discrepancy between the findings could be due to the different design of studies and varied applied/considered factors. Indeed, the majority of previously mentioned studies utilised a cross-sectional design. Moreover, although the noted studies reported the use of a healthy dietary pattern, this was defined differently in each study. For instance, in one study, a healthy dietary pattern is characterised by higher intakes of whole grains and lower consumption of dairy products, whereas others considered a diet rich in grain and dairy as a healthy pattern(Reference Soltani, Keshteli and Esmaillzadeh33). Thus, there is limited comparable data to establish a potential association between DQI-I and the odds of IBS.
Some foods, such as legumes, vegetables and fruits, are considered as symptom onset contributors in IBS patients in some studies. Furthermore, most diets with higher quality generally contain some high fermentable oligosaccharides, disaccharides, monosaccharides and polyol content which induce symptoms in IBS patients. Therefore, the null findings in this study could be explained by the high contribution of foods containing fermentable oligosaccharides, disaccharides, monosaccharides and polyol in calculating the DQI-I score too(Reference de Roest, Dobbs and Chapman38). On the other hand, some other evidence has indicated that the incidence of IBS was higher in individuals with insufficient consumption of fibre. Also, the high fibre content in some diets such as dietary approaches to stop hypertension diet has been reported to confer a protective association in IBC-C patients(Reference Soltani, Keshteli and Esmaillzadeh33,Reference Guo, Zhuang and Kuang39) . Yet, in our study, although cases had lower intakes of whole grains, fruits, vegetables and fibre, the difference between cases and controls did not reach statistical significance.
It should be noted that the results of this study did not show any association between DQI-I and IBS in gender-stratified models. It is widely accepted that IBS is more prevalent in women than in men, and it has been assumed that this is related to hormonal modulatory effects and slower GI transit time, delay in gastric emptying and decreased colonic transit time(Reference Meleine and Matricon40). Also, it has been reported that women are more likely to consult a physician for their symptoms(Reference Khayyatzadeh, Esmaillzadeh and Saneei41). Another issue which should be considered is that, in this study, we included all sub-types of IBS in total and gender-stratified logistic regression models to reduce the likelihood of relatively low numbers of individuals in tertiles, which may have an impact on results. Nevertheless, our results, as well as the extant literature, confirm that IBS is a complex disorder and due to bearing a gut–brain interaction nature, numerous unknown factors may play a role in IBS aetiology and its risk, so, there is a demand for more prospective and clinical trials to clarify the role of diet quality in odds of IBS.
This study had several strengths that warrant consideration. First, this is, to our knowledge, the first case–control study on the association of the DQI-I score with IBS. Second, the selection of cases and controls was done using the framework of a well-conducted cohort study, which reduces the selection bias that case–control studies are prone to., i.e., controls were selected from the community which were representative of the real population. Third, the analyses controlled for a wide range of potential confounders to minimise confounding bias in results. Fourth, dietary data was gathered through a valid and reliable FFQ. Nevertheless, despite the noted strengths, our study had some limitations as well. There is not a definite biochemical marker for IBS diagnosis and, so, we used ROME IV criteria for the identification of cases. The questionnaire-based data is prone to misclassification bias; however, along with diagnosis with ROME IV, patients were consulted and clinically examined by gastroenterologists for more precise diagnosis and to reduce selection bias. Another limitation of the study is that FFQ relies on individual’s memory and also it is prone to over- or under-estimation of intake reports which results in recall bias. To reduce this bias, a dietician trained participants on how to complete the FFQ to minimise the errors in the process. Another point that should be noted is that in this study, post hoc stratified analyses by gender were conducted due to the significant interaction found between sex and the predictor variable. However, it should be noted that these analyses may lack sufficient statistical power, primarily due to the relatively low sample sizes within each gender group. This limitation must be considered when interpreting the results. Despite the nearly equal distribution of genders in our study sample, the post hoc nature of these analyses underscores the need for cautious interpretation and highlights the importance of larger, prospective studies to robustly confirm these findings. Finally, despite taking several confounders into account, residual confounding factors could not be avoided. For instance, we did not have data regarding the alcohol consumption of participants due to the prohibition of alcohol intake in Iran. Nevertheless, alcohol is a potential risk factor for IBS and could be considered as a confounder.
Conclusion
Although DQI-I represents a healthy diet, the results of the current case–control study demonstrated that a higher DQI-I score was not associated with reduced odds of IBS in fully adjusted regression models. Moreover, considering inherent limitations as well as the scarce evidence regarding the association between DQI-I and the odds of IBS, further large-scale, prospective studies are required to confirm our findings and elucidate the role of diet quality in IBS odds. Considering the complex nature of IBS and the exclusive response of every patient to the same foods maybe using a modified version of DQI-I could be beneficial in investigating the association of this index with IBS. Also, considering the different manifestations and symptoms between sub-types of IBS, subtype-specific analysis would be beneficial in understanding the role of diet quality in IBS odds.
Acknowledgements
The authors thank the staff, the fieldworkers and ISFUN cohort participants, without whom this study would not have been possible.
This study was part of a PhD thesis of Saeede Jafari Nasab and was financially supported by Isfahan University of Medical Sciences.
Author contributions: P. A., M. H. E. and S. J. N. developed the study design and provided feedback on methods, results and discussion parts of manuscript. S. J. N., P. H. and C. C. T. C. contributed to the writing of the first draft of the manuscript and the reviewing and editing of the final manuscript. A. F. conducted data analysis and contributed to the reviewing and editing of the final manuscript. S. J. N. and A. F. designed and developed tables. H. S., A. A., P. H. and H. R. contributed to the management, data collection or administration of the study. All authors read and approved the final manuscript.
None of the authors had any personal or financial conflicts of interest.