


Hyperprolactinaemia is a common adverse effect of antipsychotic medication, with reported prevalence reaching up to 47% in women and around 18% in men treated with antipsychotics. Reference Bushe, Yeomans, Floyd and Smith1 The agents most commonly implicated are those with high dopamine D2 potency molecules, Reference Markianos, Hatzimanolis and Lykouras2 such as the first-generation antipsychotics along with amisulpride, risperidone and paliperidone; the last of these has the higher risk ratio for prolactin elevation according to a recent meta-analysis. Reference Huhn, Nikolakopoulou, Schneider-Thoma, Krause, Samara and Peter3 The pathophysiological mechanism involves the blockade of dopamine D2 receptors located on the membrane of lactotroph cells in the anterior pituitary gland, which are the primary targets of the tubero-infundibular pathway, resulting in the loss of dopaminergic inhibition of prolactin secretion. Reference Haddad and Wieck4
Hyperprolactinaemia can lead to a spectrum of clinical symptoms, including headache, sexual dysfunction, menstrual disturbances, gynaecomastia and galactorrhoea. Of particular concern, long-term exposure (>5 years) to prolactin-raising antipsychotics may result in an increased risk of osteoporosis and breast cancer. Reference Taipale, Solmi, Lahteenvuo, Tanskanen, Correll and Tiihonen5
Adjunctive aripiprazole for managing antipsychotic-induced hyperprolactinaemia
When switching towards a prolactin-sparing antipsychotic is not feasible (such as in cases of intolerance, history of poor response or poor adherence), the adjunctive use of aripiprazole has emerged as a validated strategy to mitigate hyperprolactinaemia without compromising antipsychotic efficacy. Reference Besag, Vasey and Salim6 Following a first report, Reference Wahl and Ostroff7 several studies have confirmed that the addition of aripiprazole can reduce hyperprolactinaemia when induced by risperidone Reference Kane, Correll, Goff, Kirkpatrick, Marder and Vester-Blokland8 (including the long-acting injection form), Reference Ziadi Trives, Bonete Llacer, Garcia Escudero and Martinez Pastor9 paliperidone Reference Qiao, Yang, Li, Guo, Wen and Zhu10 and haloperidol. Reference Shim, Shin, Kelly, Jung, Seo and Liu11 However, its efficiency is reduced when it is used with amisulpride. Reference Paulzen and Grunder12,Reference Chen, Huang, Ree and Hsiao13 Aripiprazole is a potent dopamine D2 partial agonist that stimulates D2 receptors to approximately 60% of the maximal effect of dopamine (i.e. 60% of intrinsic activity). This high level of intrinsic activity results in a decreased prolactin level in monotherapy, Reference Peuskens, Pani, Detraux and De Hert14–Reference Wada, Iwamoto, Yoshimi, Hida, Hotta and Noda16 and appears sufficient to restore the inhibitory dopaminergic tone on prolactin secretion suppressed by another antipsychotic agents.
Comparative prolactin-sparing effects between brexpiprazole and aripiprazole
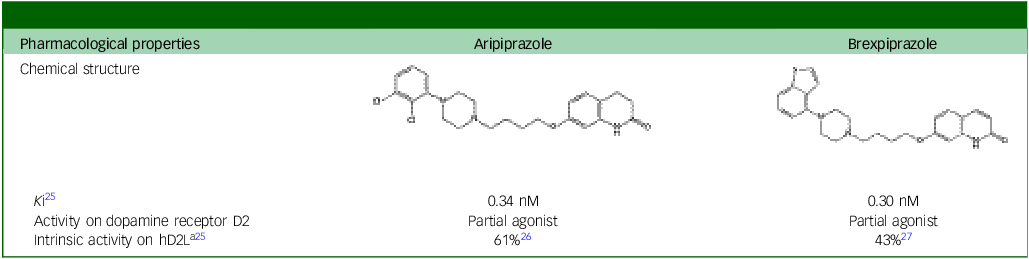
Brexpiprazole, a novel atypical antipsychotic structurally related to aripiprazole (see Table 1), also exhibits partial agonist activity at D2 receptors, but with lower intrinsic activity compared with aripiprazole (approximately 43%). Consequently, brexpiprazole has less impact on serum prolactin levels than aripiprazole. Reference Huhn, Nikolakopoulou, Schneider-Thoma, Krause, Samara and Peter3,Reference Leucht, Leucht, Huhn, Chaimani, Mavridis and Helfer15,Reference Nakamura and Nagamine17 In a retrospective study of youths with psychiatric disorders, aripiprazole was associated with hypoprolactinaemia whereas brexpiprazole significantly increased prolactin levels. Reference Wada, Iwamoto, Yoshimi, Hida, Hotta and Noda16 Nevertheless, this increase remained minimal, and brexpiprazole is considered a prolactin-sparing antipsychotic similar to quetiapine, clozapine, cariprazine or aripiprazole. Accordingly, in a study evaluating the effect of brexpiprazole on prolactin in patients with schizophrenia, prolactin-related adverse effects occurred in 1.8% for brexpiprazole-treated patients versus 0.6% on placebo, leading the authors to propose that brexpiprazole could have potential as a prolactin-stabilising agent in schizophrenia, but that more research was needed before clinical implementation. Reference Ivkovic, Lindsten, George, Eriksson and Hobart18 Indeed, lower intrinsic activity of brexpiprazole at D2 receptors – compared with aripiprazole – introduces a reasonable pharmacological uncertainty regarding its capacity to reverse established hyperprolactinaemia.
Comparative activity on the human dopamine D2 receptor

hD2L, human dopamine D2 receptor long isoform; K i, equilibrium constant, i.e. nanomolar amount of the antipsychotic needed to occupy 50% of the human dopamine D2 receptor in vitro.
a. The precise value may be debated; intrinsic activity can vary from 20 to 90% depending on in vitro assay. Reference Burris, Molski, Xu, Ryan, Tottori and Kikuchi26,Reference Maeda, Sugino, Akazawa, Amada, Shimada and Futamura27
Despite the favourable prolactin profile of brexpiprazole when used as monotherapy, its potential to reverse hyperprolactinaemia induced by other antipsychotic agents – particularly paliperidone, the most prolactin-elevating agent Reference Huhn, Nikolakopoulou, Schneider-Thoma, Krause, Samara and Peter3,Reference Leucht, Leucht, Huhn, Chaimani, Mavridis and Helfer15 – remains to be addressed.
Here we present a case illustrating the off-label use of brexpiprazole in reducing paliperidone-induced hyperprolactinaemia in a patient who experienced a skin reaction to aripiprazole.
Case report
Ms M is a young adult female, aged 26 years and suffering from paranoid schizophrenia and cannabis addiction, who was admitted to hospital for a psychotic episode and remained hospitalised for 1 month. In the weeks before admission she presented with insomnia and persecutory and grandiose delusions, accompanied by auditory hallucinations. Episodes of agitation and conflict occurred with her family, linked to cannabis use. On the day of admission her speech was characterised by logorrhoea and thought processes were disorganised. Despite these clinical features, she did not exhibit significant agitation or hostility during her stay. She did not report any suicidal ideation.
Before admission she had undergone multiple antipsychotic trials. Given the patient’s history of poor adherence, the selection of a long-acting injectable antipsychotic with combined antipsychotic and mood-stabilising properties was required. Paliperidone treatment had been initiated at a low dose during out-patient follow-up, and gradually increased in hospital with the patient’s agreement, up to a dosage of 12 mg daily. The other medication prescribed was hydroxyzine 25 mg at bedtime and lorazepam 1 mg four times daily as required. The patient showed rapid clinical improvement, with a reduction in hallucinations and delusional thoughts along with improved therapeutic engagement and greater awareness of illness. Twenty-six days after treatment initiation a satisfactory plasma paliperidone level of 42 ng/mL was achieved (therapeutic range 20–60 ng/mL). Reference Hiemke, Bergemann, Clement, Conca, Deckert and Domschke19 However, Ms M developed galactorrhoea 4 weeks following paliperidone initiation. Two serial prolactin measurements, at weeks 4 and 5 after treatment onset, revealed persistent elevation of prolactin above the upper limit of normal, at 130 μg/L (physiological range 5–23 μg /L).
Because of the positive clinical response, the continuation of paliperidone was deemed appropriate by the medical team, a decision supported by the patient. Given the established efficacy of adjunctive aripiprazole for treating antipsychotic-induced hyperprolactinaemia, the addition of aripiprazole at low dose was considered. However, Ms M reported a prior skin reaction apparently due to aripiprazole, characterised by a cutaneous eruption. During hospitalisation a cautious challenge was attempted (2.5 mg/day, increased at 5 mg/day on day 3) but, again, 1 week later this resulted in a reproducible disabling skin eruption, puffy face and newly reported drowsiness and sedation, confirming intolerance and precluding the further use of aripiprazole. In light of these constraints, and given the similarities with aripiprazole, adjunctive low-dose brexpiprazole (1 mg) was introduced as an off-label treatment to counteract hyperprolactinaemia. Brexpiprazole has an elimination half-life of approximately 90 h, leading to steady-state concentration being reached at around 20 days. Reference Lundbeck20
Three weeks following the introduction of brexpiprazole at 1 mg, a prolactin assay demonstrated a marked reduction in serum prolactin, from 130 to 37 μg/L (normal range 5–23 μg/L) and the galactorrhoea resolved. One month later the prolactin level remained at 39 μg/L. Notably, the patient’s periods subsequently returned to a regular pattern. The patient did not develop any skin reaction but complained of somnolence. Importantly, there was no recurrence or exacerbation of psychotic symptoms during this period.
Discussion
This case report describes the successful introduction of brexpiprazole to counteract hyperprolactinaemia induced by paliperidone, without recrudescence of psychotic symptoms and without reappearance of the skin reaction previously experienced with aripiprazole.
Absence of reaction with brexpiprazole following aripiprazole-induced skin rash
Aripiprazole-induced cutaneous reactions, such as rash or urticaria, are rare but have been reported in both the literature Reference Park, Kim and Lee21–Reference Parker24 and product information. The aetiopathogenesis is largely unknown. Brexpiprazole is a derivative of aripiprazole with an added thiophene ring (see Table 1). To our knowledge there is no evidence of immunological cross-reactivity between aripiprazole and brexpiprazole, despite their structural similarities. In the present case, the patient experienced a reproducible cutaneous reaction to aripiprazole but tolerated brexpiprazole without any hypersensitivity reaction. This observation, if replicated by others, may indicate that the risk of cross-reactivity between these two agents may be low regarding skin reaction. This would be a potentially valuable consideration for clinical practice in cases where aripiprazole intolerance is a barrier to treatment.
Intrinsic activity at dopamine D2 receptors and implications for hyperprolactinaemia
Brexpiprazole, like aripiprazole, is a potent dopamine D2 partial agonist but with lower intrinsic activity at this receptor (43%; see Table 1). The reduction of antipsychotic-induced hyperprolactinaemia relies on the restoration of dopaminergic tone at the D2 receptor, counteracting the prolactin-elevating effects of D2 antagonists. However, the minimal level of intrinsic D2 activity required to achieve a clinically meaningful reduction in prolactin remains to be determined. Moreover, some reports, albeit rare, have described hyperprolactinaemia induced by aripiprazole Reference Joseph28 and brexpiprazole. Reference Fernando, Gan, Xiao and Yun29 Thus, it was uncertain whether brexpiprazole would effectively lower prolactin in this context. In the case of our patient, adjunctive brexpiprazole led to a significant decrease in prolactin levels without a resurgence of psychotic symptoms, indicating that its potency (equilibrium constant (K i) = 0.30 v. 1.6 nM for paliperidone), Reference Gray and Roth30 and its partial agonist activity, were sufficient to counteract the effect of paliperidone on D2 receptors localised on the lactotroph cells of the pituitary gland. We could also have tried cariprazine, the third available partial agonist, which has a high affinity for the D2 receptor (K i = 0.49 nM) Reference Mohr, Masopust and Kopecek25 but displays even lower intrinsic activity than brexpiprazole (∼30%). Reference Kiss, Horvath, Nemethy, Schmidt, Laszlovszky and Bugovics31
Normalisation of prolactin
Spontaneous normalisation of prolactin over time without the introduction of brexpiprazole cannot be entirely ruled out. Indeed, partial tolerance during chronic treatment may cause prolactin levels to trend towards normalisation. Nevertheless, elevated prolactin levels persist in most patients despite prolonged exposure to neuroleptic. Accordingly, prolonged exposure to prolactin-increasing antipsychotics has been associated with a decline in bone mineral density and the development of osteoporosis, Reference Bushe, Yeomans, Floyd and Smith1 and may elevate the risk of breast cancer. Reference Taipale, Solmi, Lahteenvuo, Tanskanen, Correll and Tiihonen5 Furthermore, symptoms such as galactorrhea, gynaecomastia, menstrual irregularities, infertility and sexual dysfunction can be distressing for the individual. Consequently, treatment may be indicated with the aim of minimising both hyperprolactinaemia and the symptomatic burden.
To our knowledge, the off-label use of brexpiprazole to mitigate paliperidone-induced hyperprolactinaemia has not previously been described. If this finding is replicated by others, it may be clinically useful for managing antipsychotic-induced hyperprolactinaemia in patients who are intolerant to aripiprazole and for whom switching to a prolactin-sparring molecule is not possible.
Author contributions
Drafting of the initial manuscript, interpretation of the data and literature search: M.H.-C. Conception of the design: T.B., M.K. Case data acquisition and analysis and detailed examination of electronic medical records: T.B., M.-C.I. Supervision and interpretation of the data: M.K., O.T.K., D.L.-T. Critical revision: A.-L.B., N.W. Supervision of writing of the manuscript: N.W. Final approval of the version to be published: all authors. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
This study received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.
Ethical standards
The participant has been fully anonymised by the author. Written informed consent was obtained from the patient, who authorised her physicians to anonymously disclose relevant clinical information for the publication of a pharmacological case report.

 Open access
Open access
eLetters
No eLetters have been published for this article.