



Introduction
About 0.5–1.26% of people worldwide suffer from coeliac disease, a multisystem autoimmune condition with significant regional differences in prevalence patterns.(Reference Kurppa, Mulder, Stordal and Kaukinen1,Reference Saleh, Takruri, Rawashdeh and Ahmad2) The only proven treatment for this genetically caused enteropathy, which is characterised by gluten-induced villous shrinkage and subsequent malabsorption, is lifetime adherence to strictly gluten-free diets.(Reference Husby, Murray and Katzka3,Reference Ludvigsson, Bai and Biagi4)
According to recent epidemiological data, the prevalence of coeliac disease is 1–3% in general populations, but it is significantly higher (10–20%) among first-degree relatives of those who have the condition.(Reference Rostami-Nejad, Asri and Olfatifar5) According to current statistics, incidence is 1.5 times higher in females than in males across a range of populations.(Reference Nadhem, Azeez and Smalligan6) The fact that biopsy-confirmed prevalence is 0.7% but global prevalence based on serological markers approaches 1.4% illustrates the importance of histological confirmation for accurate diagnosis.(Reference Lionetti, Gatti and Pulvirenti7,Reference Singh, Arora and Strand8)
Further data from communities in the Middle East and North Africa put doubts on traditional beliefs regarding the geographic distribution of coeliac disease by demonstrating notable prevalence rates comparable to those observed in Western countries.(Reference Nawaiseh, McKyer and Abdelrahim9) Regional eating habits and a family history of such as higher frequencies of HLA-DQ2 and HLA-DQ8 haplotypes, have an impact on the observed epidemiological patterns showing complex interactions between genetic vulnerability and environmental influences.(Reference Makharia, Mulder and Goh10)
In Jordan, as in many parts of the Middle East, products labelled ‘gluten-free’ are required to comply with international standards – specifically the Codex Alimentarius states that foods labelled as gluten-free should not have more than 20 ppm of gluten in the food as sold.(11,12) Commission Implementing Regulation (EU) No 828/2014 currently governs information given to consumers in the European Union about the presence or absence of gluten.(13) Based on clinical data showing that intake below this range is protective for the majority of coeliac disease patients, this science-based criterion reflects broad expert consensus.(Reference Collin, Thorell and Kaukinen14,Reference Catassi, Fabiani and Iacono15) Regarding oats, the Codex Alimentarius standard specifies that the permissibility of specially processed oats – those not contaminated with wheat, rye, or barley and containing gluten at levels not exceeding 20 mg/kg – in foods labelled as gluten-free is to be determined at the national level by each adopting country.(11) No formal national-level regulatory determination addressing the inclusion of specially produced oats in gluten-free labelled foods has been established in Jordan. Consequently, oat-derived products were not included in the scope of the present study, and all compliance assessments were conducted exclusively against the universally adopted 20 mg/kg threshold for gluten derived from wheat, rye, and barley. With an overall contamination incidence of 15.12% found in commercially labelled gluten-free products worldwide, systematic evaluations show significant hurdles in maintaining the integrity of gluten-free products.(Reference Guennouni, Admou and El Khoudri16) Shared farming equipment, transportation networks, processing plants, and storage settings are examples of cross-contamination mechanisms that may introduce gluten amounts high enough to cause clinical reactions.(Reference Thompson, Dennis and Emerson17,Reference Falcomer, Santos Araújo and Farage18) Even though the majority of contamination investigations have been carried out in high-income nations, new data from middle-income environments also points to a risk of contamination that is clinically significant. For instance, Mehtab et al. found that 10.8% of packaged foods labelled as gluten-free in India had gluten levels over the recommended threshold, underscoring the necessity of market surveillance outside of high-income areas.(Reference Mehtab, Sachdev and Singh19) As a middle-income nation in the Middle East, Jordan‘s changing retail food sector lacks thorough data describing gluten contamination. Therefore, the purpose of this study was to produce information pertinent to regulatory monitoring and public health protection by methodically evaluating gluten contamination in items promoted as gluten-free inside Jordan’s retail food system.
Methods
Study design and setting
Using a stratified market-based sampling technique, a cross-sectional market surveillance study was carried out throughout Jordan’s retail food industry between August 2022 and November 2024. The study’s methodology was based on established food safety monitoring principles and international best practices for evaluating gluten contamination in order to promote the representation of commercially accessible gluten-free branded foods in the Jordanian market including both products manufactured locally and others imported from various countries around the world.(Reference Thompson and Simpson20)
Sample collection and preparation
Based on an anticipated contamination prevalence of 15% derived from global meta-analyses,(Reference Guennouni, Admou and El Khoudri16) with a 95% confidence level and 5% precision, a minimum of 196 products were required for the sample size calculation. A total of 182 products were analysed, representing 93% of the planned sample size and providing enough statistical power (β = 0.80) to detect notable differences in contamination rates across product categories.
The sampling sites included traditional bakeries, individual grocery stores, large supermarket chains, and vendors of specialist health foods from several governorates, including Amman, Irbid, and Zarqa. Online businesses were excluded from the study period. Products were kept in compliance with manufacturer instructions before analysis. label was used to record the brand name, ingredient list, food category, expiration date, and manufacturing information, including the country of manufacture if available, for each sampled product. Product categories, such as cookies, biscuits, rice-based products, seasoning products, milk products, nuts, and nutrition/snack bars, were designated based on the advertised item’s primary form and intended usage.
In order to prepare the sample, solid and semi-solid goods were homogenised using a home blender until a fine, homogenous powder was produced, with about 75% of the material going through a 20-mesh stainless steel screen. Before subsampling, liquid items were well mixed. After homogenisation, representative 5 g subsamples were collected for gluten extraction and analysis. Sample-contact surfaces and blender components were cleaned with alkaline enzyme washing detergent, rinsed with 70% ethanol, and dried between samples to minimise carryover contamination.
Analytical methods
Gluten quantification was performed at the Food Chemistry Laboratory, Clinical Nutrition Department, University of Petra, using a validated double-antibody-sandwich ELISA (SENSISpec INgezim GLUTEN R5®, Madrid, Spain, version 3.0, 2023). This assay uses R5 monoclonal antibodies with demonstrated specificity for the QQPFP amino acid sequence found in potentially toxic prolamin epitopes from wheat, barley, and rye.(21,Reference Valdés, García and Llorente22) Samples were processed in accordance with the manufacturer’s protocol, and gluten concentrations were determined from the assay calibration curve.
Method validation
The R5 sandwich ELISA demonstrated the following validated analytical performance parameters: limit of detection, 1.5 mg/kg; limit of quantification, 3.0 mg/kg; recovery, 95–105% for spiked samples at 10, 20, and 50 mg/kg; reproducibility, 8.7%; repeatability, 7.7%; and inter-assay CV, <10%.(Reference Valdés, García and Llorente22) All samples underwent duplicate analysis, and positive and negative controls were included in each analytical run. Standard curve parameters were verified (R 2 > 0.995) for each analytical batch to ensure measurement accuracy.
Statistical analysis
Descriptive statistical analyses were performed using SPSS version 29.0 and R software version 4.3.0. Products were categorised as compliant (≤20 mg/kg) or non-compliant (>20 mg/kg) according to the internationally used regulatory threshold (11). Contamination rates were calculated with 95% CI using Wilson score intervals. Associations between product categories and contamination status were assessed using chi-square tests. Risk ratios with 95% CI were calculated to quantify contamination risk across product categories. Statistical significance was set at p < 0.05.
Results
Population-level gluten contamination assessment
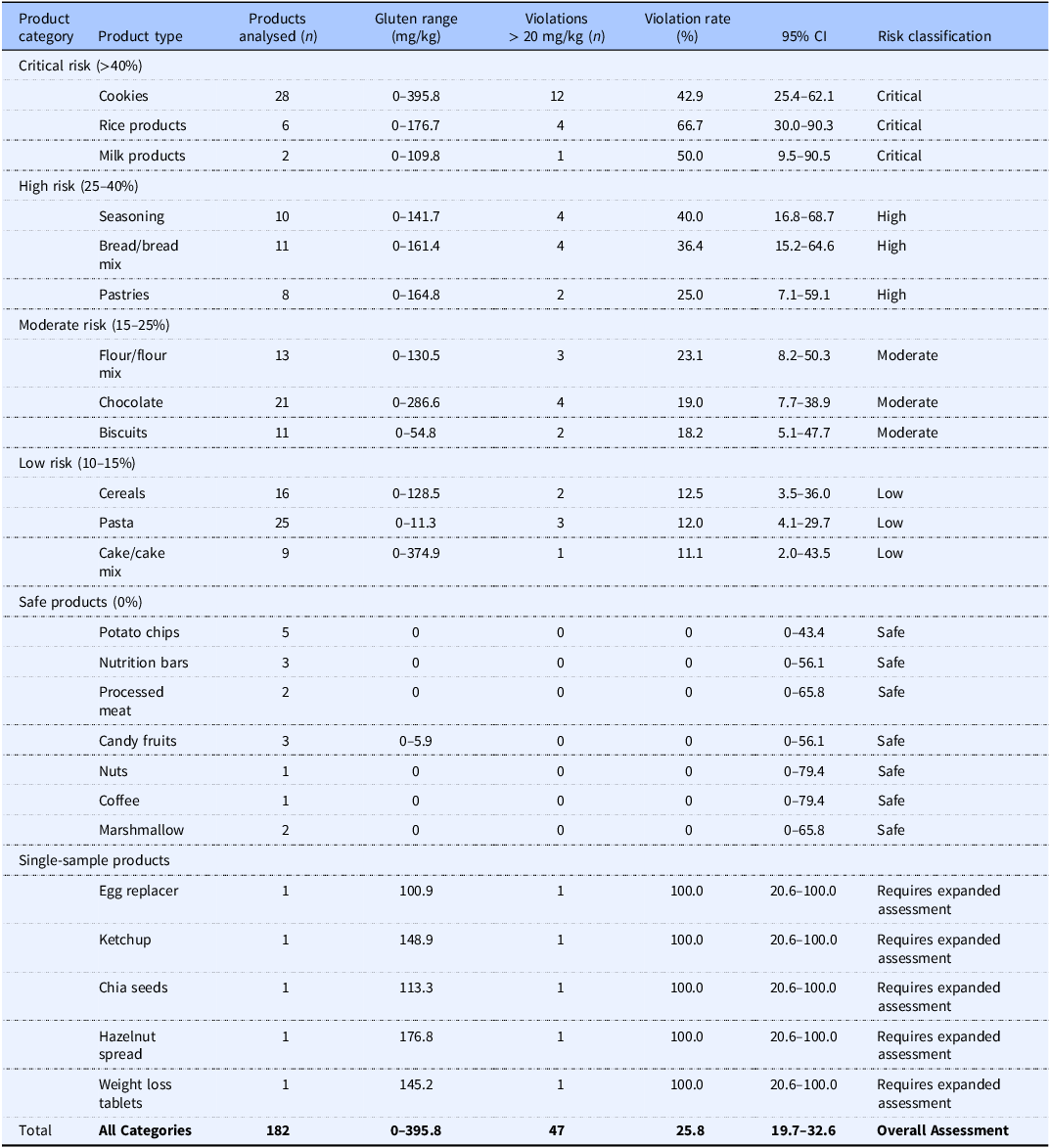
Among the 182 commercially available products labelled as gluten-free that were analysed and shown in Table 1, 47 products (25.8%; 95% CI: 19.7–32.6%) exceeded the accepted threshold of 20 mg/kg gluten, whereas 135 products (74.2%) were compliant. Contamination patterns differed significantly across product categories (χ2 = 45.23, df = 24, p < 0.001), with measured gluten concentrations ranging from undetectable levels to 395.8 mg/kg, substantially above the accepted regulatory threshold.(11)
Gluten contamination analysis and risk stratification of gluten-free labelled products in Jordan

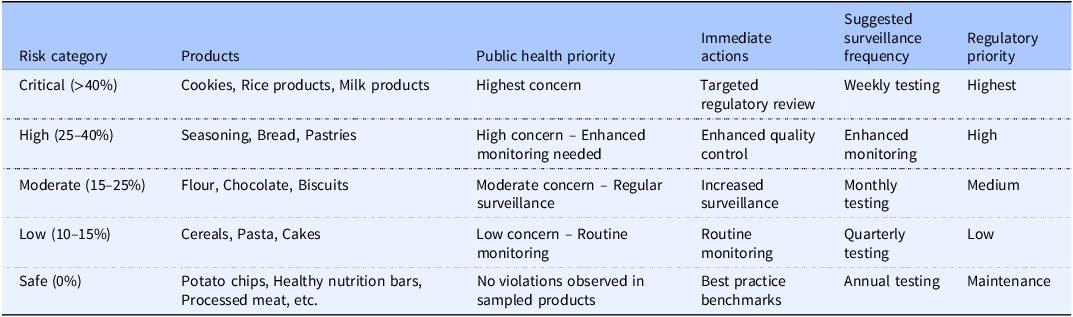
Risk stratification analysis
Category-specific contamination rates are summarised in Table 2. The highest non-compliance rates were observed in rice-based products (66.7%), milk products (50.0%), and cookies (42.9%). Additional elevated rates were observed in seasoning products (40.0%), bread and bread mixes (36.4%), and pastries (25.0%). Intermediate non-compliance was observed in flour and flour mixes, chocolate products, biscuits, cereals, pasta, and cake and cake mixes. No violations were observed in potato chips, healthy nutrition bars, processed meats, crispy candy fruits, nuts, coffee, or marshmallows; however, several of these categories were represented by small sample sizes and should therefore be interpreted cautiously.
Public health risk assessment and management recommendations by product category

Note: Special consideration required for paediatric coeliac patients who are particularly exposed to contamination effects on growth and development.
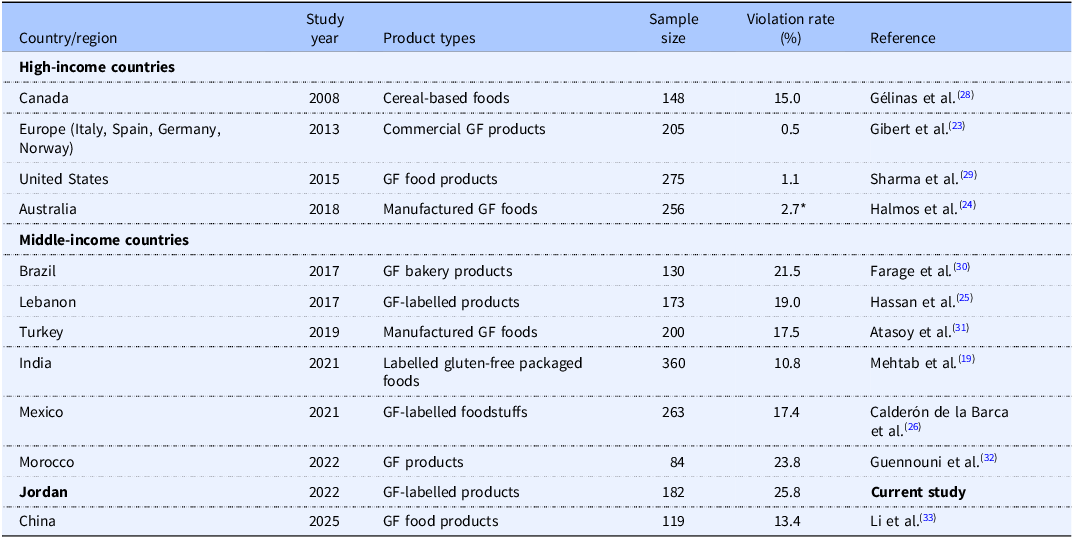
International comparative context
Jordan’s observed non-compliance rate of 25.8% was higher than that reported in several other settings included in Table 3. For direct comparison, emphasis was placed on studies evaluating commercially labelled gluten-free products rather than naturally gluten-free foods. Using this approach, the contamination rate observed in Jordan exceeded those reported in India (10.8%), Mexico (17.4%), Lebanon (19.0%), Europe (0.5%), and Australia (2.7%).
International comparison of gluten contamination rates in labelled gluten-free (GF) products

Note: *2.7% exceeded the Australian gluten-free standard of no detectable gluten (<5 ppm); however, only 0.78% of products analysed were greater than the 20 ppm international standard.
Discussion
In this market surveillance study of commercially available products labelled as gluten-free in Jordan, 25.8% of sampled products exceeded the accepted threshold of 20 mg/kg gluten.(11) The highest non-compliance rates were observed in rice-based products, milk products, and cookies, and the maximum measured concentration reached 395.8 mg/kg. These findings indicate that a substantial proportion of products marketed as gluten-free in Jordan may expose consumers to clinically meaningful gluten contamination.
The contamination frequency observed in the present study was higher than that reported in several other settings included in our comparison table, including Europe, Australia, Lebanon, Mexico, and India.(Reference Mehtab, Sachdev and Singh19,Reference Gibert, Kruizinga and Neuhold23–Reference Calderón de la Barca, Luna-Alcocer, Valenzuela-Miranda and Mejía-León26) This pattern may reflect differences in manufacturing controls, raw material sourcing, supply-chain segregation, regulatory oversight, and market maturity across settings. However, due to variations in sampling contexts, product categories, analytical procedures, and market structures, direct comparisons between research should be regarded with caution.
Since rice is naturally gluten-free, the unusually high contamination found in rice-based goods is noteworthy. According to this research, cross-contact during processing, storage, transportation, or packaging may cause contamination instead of the raw item itself.(Reference Guennouni, Admou and El Khoudri16–Reference Falcomer, Santos Araújo and Farage18) In categories including spice products, flour blends, and bakery-type goods, where ingredient complexity and shared production settings may raise the risk of unintentional gluten exposure, similar mechanisms may also lead to contamination.
These findings are significant from a clinical and public health standpoint because correct gluten-free labelling is essential to the long-term care of coeliac disease.(Reference Husby, Murray and Katzka3,Reference Ludvigsson, Bai and Biagi4) In populations with limited access to low-risk product alternatives or specialised dietary counselling, repeated exposure to contaminated items could negatively impact mucosal repair, symptom control, and dietary adherence.(Reference Rostami-Nejad, Asri and Olfatifar5,Reference Collin, Thorell and Kaukinen14,Reference Catassi, Fabiani and Iacono15) These difficulties may also have a detrimental effect on more general patient-centred outcomes, such as the health-related quality of life of individuals with coeliac disease.(Reference Elsahoryi, Ibrahim and Alhaj27) Therefore, the current findings emphasise the necessity of better manufacturing controls and increased market surveillance in product categories with greater contamination frequencies.
This study has a number of advantages. It uses a validated R5 sandwich ELISA method for gluten quantification, covers a variety of retail food categories, and offers one of the first organised evaluations of gluten contamination in commercially labelled gluten-free items in Jordan.(21,Reference Valdés, García and Llorente22) However, a number of restrictions should be taken into account. Sample sizes were uneven across categories, some categories were represented by only a small number of products, and sampling was conducted at a single market level rather than through repeated lot-based testing over time. In addition, product origin was not analysed in sufficient detail to support robust comparisons between locally manufactured and imported foods, and the presence of oat-specific cross-contact risk was not systematically evaluated. These issues should be addressed in future surveillance studies.
Larger numbers within specific product categories, repeated batch-level sampling, and more thorough subgroup analysis by retail channel, ingredient profile, and manufacturing nation should all be included in future studies. To promote the creation of context-specific regulatory and quality assurance measures for gluten-free goods in Jordan and similar regional markets, more work is also required.
Conclusion
The present findings indicate that a substantial proportion of commercially labelled gluten-free products in Jordan exceed the accepted threshold for safe gluten-free claims. Higher contamination frequencies were observed in selected product categories, particularly rice-based products, milk products, and cookies, highlighting the need for strengthened surveillance and improved manufacturing controls. These data provide an initial evidence base for enhancing regulatory oversight, supporting consumer protection, and guiding future gluten-free market surveillance in Jordan and the broader Middle Eastern region.
Acknowledgements
The authors would like to thank the Deanship of Scientific Research at the University of Petra for its support and assistance throughout this work.
Authorship contributions
L.M.A., N.A.E., O.A.A., O.D.A.M., A.A.A., F.F.A., H.K., A.D.A., and Q.K.F. contributed to the conception and/or design of the study, data acquisition, analysis and interpretation of data, and drafting or critical revision of the manuscript. All authors approved the final version and agreed to be accountable for all aspects of the work.
Funding statement
This research was supported by the Dean of Scientific Research and Graduate Studies at the University of Petra, Jordan (Grant number 21/4/2023). The funding organisation had no role in study analysis, interpretation, or manuscript preparation.
Competing interests
The authors declare no conflicts of interest.
Ethical standards
This study did not involve human participants or animal subjects. It was based on laboratory analysis of commercially available food products.

 Open access
Open access