Heart failure (HF), defined as a clinical syndrome characterised by typical symptoms, such as breathlessness, ankle swelling and fatigue, is increasingly becoming a major global public health problem. Even though the incidence of HF has been declining since 2000, it is still highly prevalent and increases direct and indirect costs to the healthcare system owing to the ageing of the population. It is suggested that there are an estimated amount of 56·19 million people globally suffer from HF(Reference Yan, Zhu and Yin1). The Global Burden of Disease Study suggested that air pollution was responsible for approximately 6·6 million premature deaths in 2019, which was mainly attributed to fine particulate matter (PM2·5). The potential mechanism may be that air pollutants could increase the risk of cardio-metabolic diseases by eliciting inflammatory changes and oxidative stress(Reference Vogli, Peters and Wolf2).
Emerging evidence increasingly indicates that lifestyle factors, such as dietary habits, may influence the relationship between air pollution and human health. For example, a large prospective cohort study conducted in the USA found that adherence to a Mediterranean diet could alter the link between air pollution and cardiovascular disease (CVD) mortality(Reference Lim, Hayes and Ahn3). Participants with higher scores on the alternative Mediterranean Diet Index showed a reduced risk of CVD mortality associated with air pollution exposure. Additionally, several short-term intervention studies have highlighted the potential role of specific foods or nutrients in modifying the impact of air pollution on cardiopulmonary health(Reference Tong4,Reference Tong, Rappold and Caughey5) . Plant foods, usually rich in antioxidant vitamins, flavonoids and polyphenols, play a pivotal role in reducing inflammation and oxidative stress(Reference Aleksandrova, Koelman and Rodrigues6). Previous studies suggested that plant-based dietary patterns might be associated with better neurological health and a reduced risk of cardiovascular risk factors, such as obesity(Reference Liang, Fu and Turner-McGrievy7), hypertension(Reference Díez and Butler8) and diabetes mellitus(Reference Baden, Liu and Satija9). In considering the negative relationship between plant-based dietary patterns and HF and the adverse effect of air pollution and HF, it is plausible to hypothesise that plant-based diet may modify the association between air pollution and HF. Our study aimed to test this hypothesis and add additional dimensions to food, air pollution and HF.
Methods
Study population
The UK Biobank is an ongoing national health resource carried out in the UK aimed at preventing, diagnosing and treating a wide range of diseases and promoting health. This cohort includes over 500 000 participants aged between 40 and 69 years at recruiting time (2006–2010). Participants attended one of twenty-two assessment centres located across England, Scotland and Wales, where they completed a comprehensive baseline assessment. Further details of the study protocol have been described elsewhere(Reference Sudlow, Gallacher and Allen10). For this cohort study, participants who withdrew consent during follow-up had missing data on diet, with uncompleted PM2·5 exposure information, with HF or other CVD at baseline or had implausible energy intakes (> 17 573 or < 3347 kJ for men and > 14 644 or < 2092 kJ for women) were excluded from analyses (online Supplementary Figure S1). The UK Biobank study received ethical approval from the NHS North-West Multi-Centre Research Ethics Committee (Ref. 11/NW/0382), and all participants provided written informed consent for their participation. Finally, a total of 190 092 participants were available for this analysis.
Assessment of heart failure
The assessment of HF was conducted using both linked with hospital inpatient data and death register records according to the International Classification of Disease 10th revision (ICD-10) codes: I11·0, I13·0, I13·2, I50·0, I50·1 and I50·9(Reference Ho, Zhou and Petermann-Rocha11,Reference Liang, Chen and Feng12) . Hospital admissions data were available until October 2022 in England, August 2022 in Scotland and May 2022 in Wales. Participants were followed-up from the date they attended the assessment centre until the date of death, diagnosis or last date of follow-up, whichever came first.
Healthful plant-based dietary patterns
The Oxford WebQ tool was adopted to evaluate the healthful plant-based diet index (hPDI) based on mean food intakes taken from a minimum of two 24-hour dietary assessments(Reference Heianza, Zhou and Sun13,Reference Satija, Bhupathiraju and Spiegelman14) . The hPDI consisted of seventeen food groups(Reference Heianza, Zhou and Sun13): whole grains, fruits, vegetables, nuts, legumes and vegetarian protein alternatives, tea and coffee, fruit juices, refined grains, potatoes, sugar-sweetened beverages, sweets and desserts, animal fat, dairy products, eggs, fish or seafood, meat and miscellaneous animal-derived foods. The seventeen food groups were divided into quintiles based on consumption levels, with scores assigned either positively (Q1 = 1 to Q5 = 5) or in reverse (Q5 = 1 to Q1 = 5). Healthy foods were assigned positive scores, while less healthy foods were assigned reverse scores. For positive scoring, the highest quintile received a score of 5, decreasing incrementally to a score of 1 for the lowest quintile. For reverse scoring, this pattern was flipped (details in online Supplementary Table S1). The scores for all seventeen food groups were then summed to calculate the hPDI for each individual. A higher hPDI reflects a diet characterised by greater consumption of healthy plant-based foods, along with lower intake of less healthy plant-based foods and animal products, indicating better overall dietary quality. We categorised the participants into three groups based on the tertile cut-off values of hPDI as low, moderate and high hPDI, respectively. Previous research demonstrated stable food intake levels over 4 years following the baseline assessment in this cohort(Reference Bradbury, Young and Guo15). Additionally, a strong correlation (Pearson correlation coefficient = 0·88; P < 0·0001) was found between the baseline hPDI and the averaged hPDI based on repeated measurements from 2009 to 2012(Reference Heianza, Zhou and Sun13). Therefore, the earliest dietary intake data were used in this study to maximise follow-up time for participants who completed more than one dietary assessment.
Assessment of ambient air pollution
The annual average concentrations of PM2·5 were estimated with a land use regression model developed from the European Study of Cohorts for Air Pollution Effects project(Reference Wang, Zhou and Song16,Reference Gao, Huang and Guo17) . The spatial variations of annual average air pollutant concentrations were calculated using the land use regression model including the geospatial predictor variables generated from the geographic information system such as traffic, land use and topography. Air pollution exposures of all participants in the UK Biobank were linked to the records through residential addresses given at the baseline visit. The exposure data for PM2·5 were collected in 2010. The annual average concentrations of PM2·5 in 2010 for each participant were linked to their residential addresses provided at the baseline visit (2006–2010). Both the continuous data (per 10 µg/m3) and categorical data (defined as low, moderate and high by the tertile cut-off points) for PM2·5 were used for data analysis.
Covariates
Covariates were selected a priori, mainly based on a literature review(Reference Heianza, Zhou and Sun13,Reference Thompson, Candussi and Tresserra-Rimbau18) . Anthropometric measurements and biological samples were collected from all study participants by trained staff. In this study, several covariates were considered, including age, sex(Reference Zhu, Qi and Bos19), ethnicity, educational level, BMI (in kg/m2), smoking status(Reference Lu, Xu and Georgakis20), alcohol consumption(Reference Larsson, Burgess and Mason21), physical activity(Reference Larsson, Tektonidis and Gigante22) and employment.
Statistical analysis
The baseline characteristics of the study population were presented by incident HF. Continuous variables were expressed as mean (sd) and categorical variables were presented as number (percentage), respectively.
Multivariable Cox regression models were used to analyse the relationships of hPDI and PM2·5 with the risk of incident HF. Three models were used: Model 1 was the crude model; Model 2 was adjusted for age and sex and Model 3 was further adjusted for ethnicity, educational level, BMI, smoking status, drinking status, physical activity and employment. To evaluate the combined effects of hPDI and PM2·5, participants were categorised into nine groups according to hPDI and PM2·5 exposure level: low hPDI-high PM2·5, low hPDI-moderate PM2·5, low hPDI-low PM2·5, moderate hPDI-high PM2·5, moderate hPDI-moderate PM2·5, moderate hPDI-low PM2·5, high hPDI-high PM2·5, high hPDI-moderate PM2·5 and high hPDI-low PM2·5. The hazard ratios with their 95 % CI of HF in model 3 were calculated with low hPDI and high PM2·5 exposure as the reference. The interaction effects of PM2·5 exposure and hPDI were analysed using both additive and multiplicative interaction models. For additive interactions, a new variable was constructed to categorise individuals into nine groups based on combinations of PM2·5 exposure levels (low, moderate and high) and hPDI levels (low, moderate and high), with individuals in the low hPDI and high PM2·5 groups serving as the reference. The relative excess risk due to interaction (RERI) was calculated to quantify the interaction: RERI = 0 indicated no additive interaction, RERI < 0 suggested a negative additive interaction and RERI > 0 reflected a positive additive interaction. In this study, a significant positive RERI suggested that hPDI could influence the effects of PM2·5 exposure on HF risk. For multiplicative interactions, the likelihood ratio test was performed by comparing models with and without an interaction term between PM2·5 and hPDI. A P-value for interaction below 0·05 was considered evidence of a significant multiplicative interaction.
A total of four sensitivity analyses were carried out to examine the robustness of the relationships by (1) excluding individuals with less than 2 years of follow-up to minimise the reverse casualty; (2) restricting analyses among the participants without hypertension, diabetes and cancer at baseline to minimise the potential influence of comorbidities; (3) restricting analyses among the male participants to determine if the relationships were consistent across different sexes; (4) excluding participants aged less than 60 years old to investigate whether the results were consistent across different age-groups and (5) further adjusting for diabetes, hypertension, dyslipidaemia and cancer at baseline minimise the potential influence of health status on diet habits.
All statistical analyses were conducted using R (version 4.0.3). A two-tailed P < 0·05 was considered as statistical significance.
Results
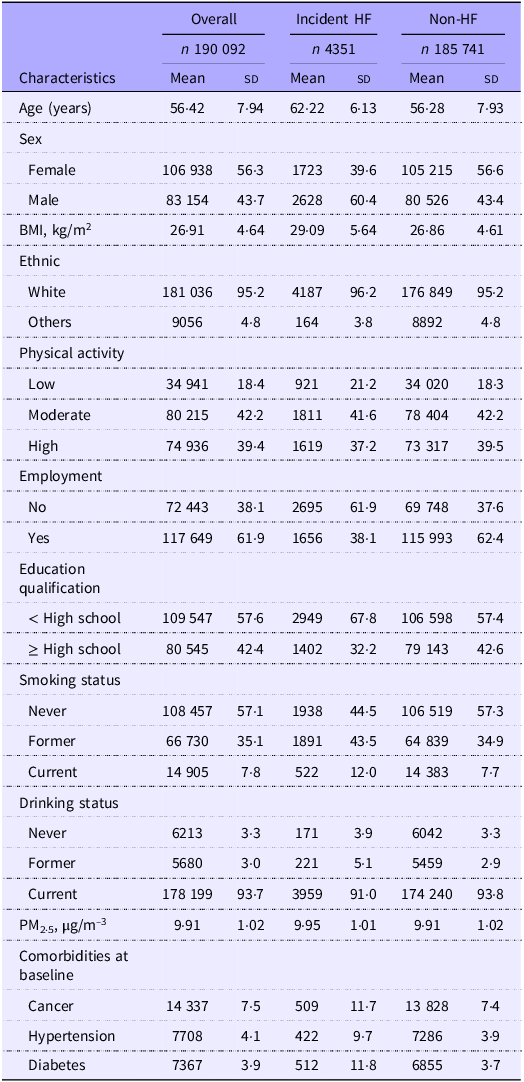
Table 1 presents the baseline characteristics of 190 092 study participants by HF status. The mean age of the participants at baseline was 56·42 years (sd: 7·94 years) and 48·7 % were males; 4351 cases of HF were identified during the follow-up. Participants who developed HF were older and more likely to be male, unemployed and current smokers in comparison with those without depression.
Baseline characteristics of the study participants by heart failure

HF, heart failure; PM2·5, particulate matter with aerodynamic diameter < 2·5 μm.
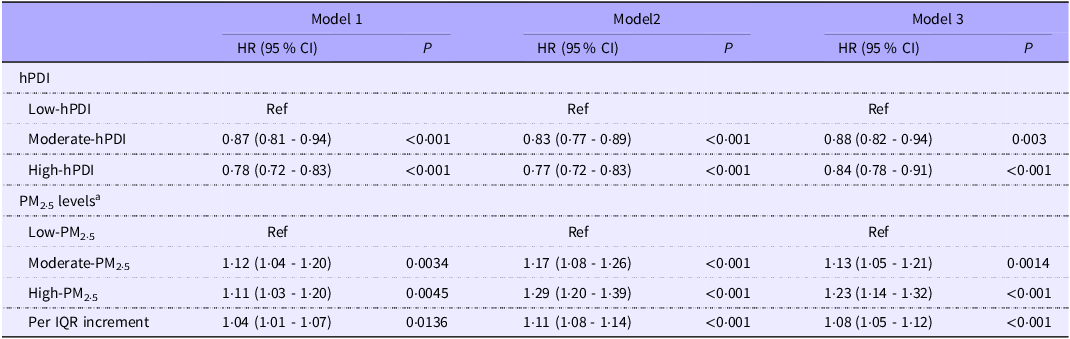
The main effects of hPDI and chronic PM2·5 exposure on incident HF are depicted in Table 2. A higher hPDI was related to a lower risk of incident HF. Compared with the low hPDI levels, the hazard ratio (95 % CI) of incident HF was 0·88 (95 % CI: 0·82, 0·94) and 0·84 (95 % CI: 0·78, 0·91) for moderate and high levels of hPDI, respectively. Whereas, individuals exposed to higher levels of PM2·5 were associated with a higher risk of HF. Compared with the low-PM2·5 groups, the moderate- and high-PM2·5 groups had hazard ratio of 1·13 (95 % CI: 1·05, 1·21) and 1·23 (95 % CI: 1·14, 1·32), respectively.
Associations of plant-based diet and long-term PM2·5 exposure and risk of HF

PM2·5, particulate matter with aerodynamic diameter < 2·5 μm; HF, heart failure; HR, hazard ratio; hPDI, healthful plant-based diet index.
Model 1 was a crude model; Model 2 was adjusted for age and sex and Model 3 was further adjusted for ethnicity, physical activity, education, smoking status, drinking status and BMI.
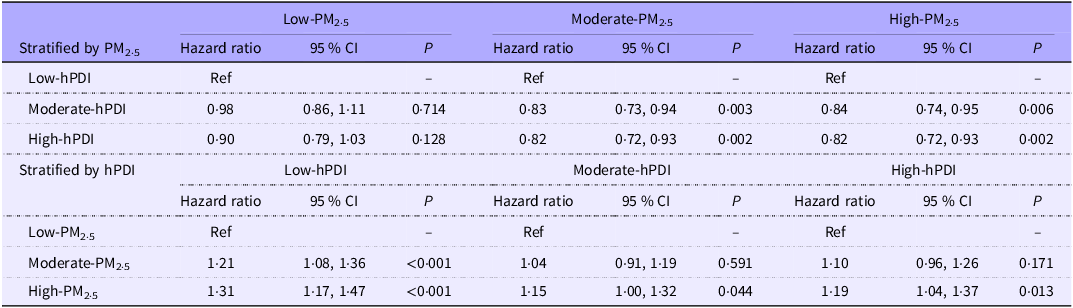
The results of the subgroup analysis are shown in Table 3. A higher hPDI was associated with a lower HF risk in moderate and high PM2·5 exposure, whilst a higher level of PM2·5 exposure was associated with a higher HF risk in each hPDI stratum.
Subgroup analyses on the association of HF with hPDI and PM2·5 exposure stratified by the categories of PM2·5 or hPDI

HF, heart failure; hPDI, healthful plant-based diet index; PM2·5, particulate matter with aerodynamic diameter < 2·5 μm; HR, hazard ratio; .
The results were adjusted by age, sex, ethnicity, physical activity, education, smoking status, drinking status and BMI.
The combined effects of hPDI and long-term exposure to PM2·5 on HF risk are shown in Table 4 and online Supplementary Figure S1. Individuals with a high level of hPDI and exposed to a low level of PM2·5 exhibited the lowest risk of incident HF, whilst those who were in the low hPDI group and exposed to a high level of PM2·5 were associated with the highest risk of HF. Compared with participants who were in the low hPDI group and exposed to a high level of PM2·5, those with a high level of hPDI and exposed to a low level of PM2·5 had a hazard ratio of 0·68 (95 % CI: 0·60, 0·78). The trend patterns of the effects of hPDI and PM2·5 exposure were evident in each stratum of PM2·5 exposure or hPDI. A significant positive RERI was observed, indicating the existence of positive additive interactions. For individuals with moderate hPDI and low PM2·5 exposure, the RERI were 0·15 (95 % CI: 0·01, 0·29), suggesting that a 0·11 relative excess risk was due to the additive interaction. However, no significant additive interactions for participants with high hPDI and low PM2·5 exposure.
Combined effects of hPDI, PM2·5 and the risk of HF

hPDI, healthful plant-based diet index; PM2·5, particulate matter with aerodynamic diameter < 2·5 μm; HF, heart failure; RERI, relative excess risk due to interaction; HR, hazard ratio.
The results were adjusted by age, sex, ethnicity, physical activity, education, smoking status, drinking status and BMI.
The estimates of RERI were calculated based on the reference group with low hPDI and high PM2·5.
Bolding indicates that the results are statistically significant.
The sensitivity analysis generally yields similar results (online Supplementary Tables S2–S5).
Discussion
To the best of our knowledge, this is the first study to evaluate both the independent and combined effects of adherence to healthy plant-based dietary patterns and long-term PM2·5 exposure on the risk of HF. Our study found that higher hPDI was associated with a lower risk of HF. Whilst, living in areas with higher PM2·5 was associated with a higher risk of HF. PM2·5 exposure may increase the risk of HF more greatly in individuals with low hPDI than those with high hPDI. Our findings indicated that higher adherence to the plant-based dietary pattern might be beneficial to the risk of HF induced by chronic exposure to PM2·5. The negative relationships between a plant-based diet and HF can be attributed to several factors. First, plant-based diets are typically rich in dietary fibre, which has been consistently associated with a reduced risk of CVD, including HF. The high fibre content in these diets promotes satiety, helps maintain healthy body weight and reduces the risk of obesity and metabolic disorders, all of which are risk factors for HF(Reference Craig, Mangels and Fresán23,Reference Wastyk, Fragiadakis and Perelman24) . Second, plant-based diets are abundant in antioxidant compounds, such as vitamins C and E, carotenoids and flavonoids, that have been shown to possess anti-inflammatory and cardioprotective properties(Reference Ketnawa, Reginio and Thuengtung25). These antioxidants help minimise oxidative stress and inflammation, which play crucial roles in the development and progression of HF. Elevated serum levels of inflammation increase risk factors for HF, as well as incident HF(Reference Sanders-van Wijk, Tromp and Beussink-Nelson26,Reference Murphy, Kakkar and McCarthy27) . Plant-based diets decrease serum levels of inflammation and may be protective. One potential explanation is the differing factors related to the reduction of oxidative stress and inflammation(Reference Lau, Roshandelpoor and Zarbafian28,Reference Kumar, Lim and Poh29) . Furthermore, the consumption of plant-based proteins instead of animal-based proteins in a plant-based diet may contribute to its beneficial effects on heart health. Plant-based proteins, derived from sources like legumes, soyabean and nuts, are typically lower in saturated fat and cholesterol compared with animal-based proteins. Substituting animal proteins with plant-based proteins has been associated with improved lipid profiles, decreased blood pressure and reduced cardiovascular risk, which may ultimately lower the risk of HF(Reference Richter, Skulas-Ray and Champagne30).
Moreover, our study investigated the potential role of PM2·5 exposure in HF risk. It is well known that PM2·5 exposure is associated with a higher risk of incident HF. Our results reported a positive association between PM2·5 exposure and HF, which is in line with previous studies(Reference Zhang, Chen and Cheng31,Reference Jia, Lin and He32) . Several potential mechanisms might be underlying the observed relations between air pollution and HF. For instance, exposure to air pollution can lead to oxidative stress, systemic inflammation and autonomic imbalance and then increase blood pressure(Reference Rajagopalan, Al-Kindi and Brook33) and decrease cardiac output(Reference Bai, Shin and Burnett34). Prolonged or repeated stimulation of these pathways may further result in the progression of endothelial dysfunction, atherosclerosis, diastolic dysfunction, left ventricular hypertrophy and myocardial fibrosis(Reference Hu, Nie and Ou35–Reference Wang, Ran and Xia37), which could eventually increase the risk of HF. In addition, a randomised controlled study of HF showed that a filter intervention might reduce endothelial dysfunction and B-type natriuretic peptide increases associated with short-term exposure to diesel exhaust exposure in patients with HF.(Reference Hayes, Lim and Zhang38,Reference Zhang, Qian and Chen39) Existing evidence suggests the potential mechanisms for the risk of HF associated with a higher PM2·5 exposure strengthened by a low hPDI score.
We observed a synergistic interaction on the additive scale between hPDI and PM2·5 exposure in relation to HF risk. The RERI is widely regarded as the standard metric for assessing additive interactions, as it better represents biological interaction compared to measures on the multiplicative scale(Reference de Mutsert, de Jager and Jager40). Assessing interactions on the additive scale is particularly useful for determining whether two risk factors act synergistically – meaning their combined excess risk exceeds the sum of their individual excess risks – and is especially relevant for evaluating public health implications(Reference Knol and VanderWeele41). In this study, the significant RERI suggested that moderate hPDI combined with low PM2·5 exposure reduced HF risk more than expected based on their independent effects. These findings imply that hPDI may modify the relationship between PM2·5 exposure and HF risk, potentially attenuating the negative impact of air pollution in individuals with higher hPDI scores. Further research is required to confirm and expand upon these observations. To our knowledge, this is the first study to evaluate the combined effects of plant-based dietary patterns and PM2·5 on HF risk. The prospective study design and the large sample size were the two main strengths of this study. The current study also has several potential limitations. First, the results from our observational study were based on a retrospective sub-analysis of the data from the UK Biobank. Thus, the causality of the results should be interpreted with caution. Second, the dietary assessment was based on 24-hour recall, which might be subjected to measurement error and lead to misclassification(Reference Wang, Zhou and Song16). Third, only seventeen food groups were used to construct the PDI due to the unavailability of vegetable oils in the current study, which was included in the original paper describing the PDI by Satija et al.(Reference Satija, Bhupathiraju and Rimm42). Fourth, the PDI treat all animal-based foods equally without discrimination by assigning opposite scores, which may ignore benefits from some food components, such as dairy products and seafood. However, the results of our sensitivity analyses were stable by considering dairy products and seafood as healthful food groups. Fifth, only a single measurement of air pollution is available in the UK Biobank since the home addresses of the participants are unavailable during follow-up. Further studies with repeated measurements are needed to confirm the findings. Sixth, even though we had controlled the majority of confounders, the residual confounding from unmeasured or unknown factors might remain. Finally, our analyses were conducted among Europeans, limiting the extrapolation of our findings to other ethnic groups.
In conclusion, our findings from the UK Biobank Study suggested that the association between long-term PM2·5 exposure and the risk of developing HF was lower among the participants with higher hPDI. Our findings suggest that higher adherence to the plant-based dietary pattern may benefit the risk of HF induced by long-term PM2·5 exposure. Promoting the plant-based dietary pattern may be a strategy to reduce the effects of PM2·5 on CVD.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114525000698
Acknowledgements
The UK Biobank data was utilised under application no. 93398.
The work was supported by Henan Medical Science and Technology Research Program Joint Construction Project (No. LHGJ20220277), the Open Research founded by the National Health Commission Key Laboratory of Birth Defects Prevention and the Henan Key Laboratory of Population Defects Prevention (ZD202303, ZD202301), the 2022 International Postdoctoral Exchange Fellowship Program (Talent-Introduction Program) (No. YJ20220181) and Henan Medical Science and Technology Research Program (No.232102310069).
Y. J. Z. and L. L. designed research. Y. J. Z. conducted the data cleaning and data analysis. S. S. Z., X. Q. Z. and Y. J. Z. drafted the manuscript. Z. K. W., Y. F. J., W. D. W., J. X. Z., X. L. Z. and Y. C. B. revised the manuscript. Y. J. Z. and L. L. had primary responsibility for the final content. All authors read and approved the final manuscript.
None of the authors has any conflicts of interest to declare.