Metabolic syndrome (MetS) is an entity in which a cluster of abnormalities co-exist, including insulin resistance, hypertension, dyslipidemia and central obesity(Reference Nilsson, Tuomilehto and Rydén1). With consideration of the National Cholesterol Education Program Adults Treatment Panel III definition, 38·3 % of the Iranian population suffers from MetS(Reference Tabatabaei-Malazy, Saeedi Moghaddam and Rezaei2), and an incidence rate of 229·9 per 1000 person-years has been observed for it(Reference Hosseini-Esfahani, Alafchi and Cheraghi3).
MetS is accompanied by several clinical implications such as cardiovascular diseases(Reference Guembe, Fernandez-Lazaro and Sayon-Orea4), type 2 diabetes mellitus (T2DM)(Reference Lee, Kim and Kim5) and dementia(Reference Machado-Fragua, Fayosse and Yerramalla6). Moreover, it was observed that MetS is associated with decreased mental health and mental health-related quality of life (HRQOL)(Reference Limon, Lee and Gonzalez7). Mental health is known as the ability to cope and experience a certain degree of stress, anxiety and depression for personal growth and to function productively(Reference Fusar-Poli, Salazar de Pablo and De Micheli8). HRQOL is a manifestation of how the disease and treatment affect disability and daily functioning(Reference Haraldstad, Wahl and Andenæs9).
Various nutritional factors and dietary patterns are related to the incidence of MetS(Reference Rahimlou, Mirzaei and Keshavarz10,Reference Ushula, Mamun and Darssan11) and trigger its mental health consequences, such as stress(Reference Schweren, Larsson and Vinke12) and depression(Reference Rahimlou, Morshedzadeh and Karimi13). Curcumin, probiotics, nutraceuticals(Reference Morshedzadeh, Rahimlou and Shahrokh14), butyrate consumption and adherence to the Mediterranean diet have been suggested for the management of MetS(Reference Fahed, Aoun and Bou Zerdan15). Curcumin is the main bioactive compound that is extracted from Turmeric (Curcuma longa). It was observed that curcumin has the potency to improve major depressive disorder(Reference Ramaholimihaso, Bouazzaoui and Kaladjian16) and anxiety(Reference Khodadadegan, Azami, Guest and Guest17) and alleviate stress(Reference Spanoudaki, Papadopoulou and Antasouras18). Moreover, curcumin supplementation was observed to improve HRQOL(Reference Sadeghian, Rahmani and Jamialahmadi19).
Probiotics are ‘live microorganisms that, when administered in adequate amounts, confer a health benefit on the host’(Reference Hill, Guarner and Reid20). These non-pathogenic microorganisms, which are resistant to digestive enzymes and the gastrointestinal system environment, adhere to the epithelial cells and show health-improving effects(Reference Stavropoulou and Bezirtzoglou21). Their potential beneficial role in mental health improvement through various biochemical and physiological pathways is demonstrated(Reference Johnson, Thurairajasingam and Letchumanan22). Probiotics consumption can relieve stress symptoms(Reference Ma, Jin and Kwok23) and improve HRQOL(Reference Le Morvan de Sequeira, Kaeber and Cekin24). Moreover, it should be noted that in 2021, the probiotic market size was USD 58·17 billion, and it will grow 7·5 % by 2030, according to a report by Grand View Research. For psychobiotics, the probiotics that affect mental health, the market is expected to rise to 201·8 million USD by 2033(Reference Pathak, Tirumalai and Kashyap25).
Although the potential effects of curcumin and probiotics on mental health and HRQOL are well established, there are also some inconsistent results(Reference Le Morvan de Sequeira, Kaeber and Cekin24,Reference Asadi, Gholami and Siassi26,Reference Uchio, Kawasaki and Okuda-Hanafusa27) . Moreover, no previous studies have assessed the co-supplementation of curcumin and probiotics on mental health and HRQOL. However, it should be noted that in a previous study, as a part of a major project, curcumin-probiotic (CurPro) drink powder co-supplementation did not show any promising effect on lipid profile(Reference Mohammadi, Mohsenpour and Sohrabi28). Thus, considering the possible effects of probiotics and curcumin and their combinations on mental health and due to the lack of studies in this regard, the present study aimed to investigate the effect of CurPro co-supplementation in the form of a novel drink powder on mental health and HRQOL in adults with overweight/obesity and MetS.
Methods
Study design and ethical approval
A four-arm, randomised, double-blinded, placebo-controlled clinical trial with factorial design was conducted to examine the effects of curcumin, probiotics, and their combination on mental health and HRQOL. Participants were recruited from outpatient MetS adults of the Imam Reza Clinic, affiliated to Shiraz University of Medical Sciences, Shiraz, Iran, using a convenient sampling method. The study protocol was reviewed and approved by the Institutional Review Board and the ethics committee of Shiraz University of Medical Sciences for being in accordance with the Helsinki Declaration of Ethics for Human Studies (Code: IR.SUMS.REC.1401·592, on 4 December 2022). The study protocol was prospectively registered in the Iranian Registry of Clinical Trials (IRCT.ir) under the registration code: IRCT20220315054289N2 (18 February 2023). The CONSORT guidelines for reporting clinical trials were followed for reporting the study.
Before the participants entered the study, volunteers were verbally informed about the study protocol, its aims and any possible advantages and disadvantages. The research team assured the volunteers of the confidentiality of their personal information. Moreover, it was emphasised that the participants have the right to leave the study at any stage in case of unwillingness to cooperate with the study, while this would not affect their routine clinical care. Finally, the written informed consent was signed by the volunteers.
Study population
Adults aged 30–65 years were eligible to participate if a) were overweight (25 < BMI < 29·9) or obese (BMI ≥ 30), b) suffered from MetS based on National Cholesterol Education Program Adults Treatment Panel III, c) had no renal, hepatic, inborn disease, endocrine or cardiovascular disorders (except for T2DM, dyslipidaemia or hypertension), d) were not pregnant or lactating, e) were not taking antibiotic medications, curcumin, probiotic or other supplements for 3 months before the study initiation and f) were not hospitalised or infected with COVID-19 or any communicable disease for 3 months before the study.
If any participant started insulin therapy, took antibiotics, probiotics or curcumin, reported the diagnosis of any diseases and pregnancy or had low adherence to the interventions, he/she was excluded from the study. Obese or overweight individuals who followed special or any medical diets were omitted at the first visit and not assessed for eligibility. On the other hand, participants who expressed unwillingness to cooperate were free to leave the study, and it did not affect their usual medical care.
Metabolic syndrome diagnosis and anthropometric assessments
After the referral by the collaborator endocrinologist, participants were assessed for anthropometric measurements and referred to the laboratory for blood sampling. Height was measured while the participants had no shoes and hats, stood straight; back, heels and buttocks touched the wall, and their head was in Frankfurt position touching the wall. Height was recorded with an accuracy of 0·1 cm using a stadiometer (Seca, Germany). A bioelectrical impedance analysis device (Tanita, model: BC-418, Japan) was used to measure weight and BMI. Participants were asked to be well hydrated and had no vigorous physical activity before weight and height measurements. Weight and BMI were measured when the participant stood on the bioelectrical impedance analysis device with minimal possible clothing and barefoot. Waist circumference was read on an inelastic tape measure after a normal exhale, while participants stood, and the tape measured the midpoint between the lowest rib and iliac crest with 0·1 cm accuracy.
Blood pressure was assessed three times at 5-minute intervals after 5 min of rest in a sitting position using a sphygmomanometer (Riester Precisa-N, Germany). The final reports for systolic and diastolic blood pressures were the averages of three assessments with 5-minute intervals.
After overnight fasting for 8–10 h, participants were presented at the laboratory for blood tests. A 5-ml venous blood sample was taken and centrifuged. The colorimetric enzymatic method was applied to assess the separated serum for fasting blood sugar (fasting blood sugar; commercial kit: BXC0101A, Biorex Inc. Iran), TAG (commercial kit: BXC0271A, Biorex Inc. Iran) and HDL-cholesterol (commercial kit: BXC0420A, Biorex Inc. Iran) using an autoanalyser (BT-1500, Biotenica, Italy). MetS components were assessed before and after the intervention.
Based on the National Cholesterol Education Program Adults Treatment Panel III, MetS diagnosis was approved if any participant showed three out of five clinical symptoms of 1) waist circumference higher than 88 cm for women and 102 cm for men, 2) elevated TAG over 150 mg/dl, 3) low HDL-cholesterol (less than 50 mg/dl for women or under 40 mg/dl for men), 4) high fasting blood sugar (over 110 mg/dl), and 5) systolic blood pressure ≥ 130 mmHg or diastolic blood pressure ≥ 85 mmHg(Reference Zafar, Khaliq and Ahmad29).
Study protocol
First, the collaborator endocrinologist referred the individuals with MetS to the research team. Volunteers were informed about the study verbally and in written form, and then, in case of willingness to cooperate, the informed consent forms were signed by volunteers. Then, a face-to-face interview was done to record participants’ demographic characteristics including gender, marital, education and job status. Participants’ income was recorded as low (up to minimum wage), middle (minimum wage up to twice minimum wage) or high (more than two minimum wage). Also, being a current smoker, alcohol user and history of T2DM, dyslipidaemia and hypertension were asked. Subsequently, participants entered a 2-week run-in period to stabilise nutritional habits and physical activity levels.
After 14 days, participants were presented at the laboratory for blood sampling. Then participants were visited by the research team for dietary intake, physical activity, mental health and HRQOL assessments. Then, based on a sequence of sealed opaque envelopes, participants were assigned to one of the study groups (three intervention groups and one control group). The sequence of envelopes was prepared by an out-of-study person familiar with the randomisation method prior to study initiation. A balanced-block randomisation method (blocks of 4 with a 1:1:1:1 ratio) was used to determine the random sequence, then codes (A, B, C or D) were assigned to the study groups and concealed in opaque envelopes based on the random sequence. After revealing the study group code, participants received the drink powder sachets of the assigned group for the first half of the study (4 weeks).
At the end of the 4th week, participants were visited by the research team to return the unused drink powder sachets and hand over the quota for the second half of the study (4 weeks).
By the end of the 8th week, participants were recalled to visit the research team for post-intervention dietary intake, physical activity, mental health and HRQOL assessments. Moreover, participants returned the unused sachets of drink powders. In addition, in the 4th and 8th weeks, participants were asked about the possible side effects following the drink consumption by the physician cooperating with the study. Moreover, the physician made physical assessments for any possible signs of side effects. During the study period, periodic phone calls were made with participants to ensure maximum adherence to the study protocol.
Intervention
Participants received one out of four types of drink powder sachets based on the assigned group along with a low-energy diet. Four study groups and their related sachets were:
-
(1) Probiotic group: sachets containing 109 colony-forming unit freeze-dried probiotics of Lactobacillus acidophilus and Lactobacillus rhamnosus strains (Parsi Lact, Pardis Roshd Mehregan Co., Shiraz, Iran).
-
(2) Curcumin group: sachets containing 1 g spray-dried curcumin (regular curcumin pellet was prepared from Karen Pharma and Food Supplement Co., Tehran, Iran).
-
(3) CurPro group: sachets filled with dry-blended 109 colony-forming unit freeze-dried probiotic (as described previously) and 1 g of spray-dried curcumin.
-
(4) Placebo group: containing maltodextrin.
The dosage of curcumin(Reference Fusar-Poli, Vozza and Gabbiadini30) and probiotics strains(Reference Le Morvan de Sequeira, Kaeber and Cekin24,Reference El Dib, Periyasamy and de Barros31) was determined after a review of the literature. To ensure maximal similarity of drink powders, orange flavouring was added to all sachets. Moreover, food colouring was added to the sachet, which had no curcumin to mimic the curcumin color. Participants were asked to dissolve one sachet of drink powder in water per day and consume it. Sachets were labelled as A, B, C or D in line with the study group codes by the same out-of-study person who prepared random sequences. Sachets were identical in size, colour and weight, and the powders were similar in taste, colour and aroma to blind participants and investigators. All the measures were done for not deviating from the concealment or blinding guidelines. The codes assigned to the sachets and groups remained confidential until after the final analysis of data.
Along with drink powders, participants received a low-energy diet with a reduction of 500 kcal after considering physical activity level and calculating the daily total energy expenditure using Mifflin-St. Jeor equation for each participant(Reference Mahan and Raymond32). The diet consisted of 50–55 % carbohydrate, 15–20 % protein and 25–30 % fat from total energy.
Low adherence to the intervention was defined as consumption of less than 80 % of sachets based on the counting of returned unused sachets at weeks 4 and 8, or low compliance with diet, considering less than 50 % of calorie reduction during the study period in comparison with the pre-intervention diet records.
Outcomes
For the present study, stress was considered as the primary outcome. In addition, other aspects of mental health including anxiety and depression and HRQOL were assessed as the secondary outcomes of the study.
Dietary and physical activity assessments
A 3-day food recall (two weekdays and one weekend) was used to assess the dietary intake of participants before and after the study period. Participants were asked to recall food and drinks along with preparation methods and ingredients for complex foods. Consumptions were reported based on the scales for Iranian households and then converted to grams. Dietary intakes were analysed using the modified version of Nutritionist 4 software for Iranian (N4, First Databank Inc., San Bruno, CA, USA) to extract daily energy and macronutrient intake.
The physical activity of participants was assessed using the 7-item short form of the validated International Physical Activity Questionnaire. This instrument asks for the frequency and duration (minutes) of three levels of physical activity as vigorous, moderate and low intensity for the past 7 days. To calculate the physical activity, the duration of each intensity level (in minutes) for the past 7 days was multiplied by the metabolic equivalent of the intensity level (3·3, 4 and 8 for low, moderate and vigorous, respectively) and summed(Reference Lee, Macfarlane and Lam33).
Depression, anxiety, and stress assessment
The Depression Anxiety Stress Scale-21 was used to assess the symptoms of stress, anxiety and depression of participants, before and after the study(Reference Akin and Çetin34). The validity of the Persian version has been checked previously for the general Iranian adult population(Reference Sahebi, Asghari and Salari35). The Depression Anxiety Stress Scale-21 consists of twenty-one self-reported 4-point scale questions (Online Supplementary Material). Each item scores from 0 (no symptoms at all) to 3 (very severe). The instrument has three subscales for depression, anxiety, and stress with seven questions. The scores for each subscale were summed up and multiplied by two (each subscale scores from 0 to 42), in order to compare them with normative results of the long form of Depression Anxiety Stress Scale-21. A higher score in each subscale shows greater severity of symptoms in the related subscale. Moreover, individuals are categorised based on their score for depression (0–9 = normal, 10–13 = mild, 14–20 = moderate, 21–27 = severe and ≥ 28 = extremely severe), anxiety (0–7 = normal, 8–9 = mild, 10–14 = moderate, 15–19 = severe and ≥ 20 = extremely severe) and stress (0–14 = normal, 15–18 = mild, 19–25 = moderate, 26–33 = severe and ≥ 34 = extremely severe).
Health-Related quality of life assessment
HRQOL was evaluated using the 36-item Short Form Health Survey (SF-36) before and after the intervention (Online Supplementary Material). This instrument asks for the quality of life in eight health-related concepts of physical functioning (physical functioning with ten questions), role limitations due to physical problems (RP with four questions), bodily pain (bodily pain with two questions), general health (general health with five questions), vitality (with four questions), social functioning (social functioning with two questions), role limitations due to emotional problems (RE with three questions) and mental health (mental health with five questions)(Reference Instrument Ware and Sherbourne36). The scores of multiple choice questions of SF-36 in each subdomain are summed up and divided by the number of questions to yield a total score in each subdomain. Moreover, the total score of SF-36 is calculated by summing up the score for each answer and dividing by the total number of questions. Scores for each subdomain and the total score range from zero to 100. Higher scores indicate higher HRQOL(Reference Ware37). The Persian version of SF-36 has been validated previously(Reference Montazeri, Goshtasebi and Vahdaninia38).
Statistical analysis
Based on the previous study(Reference Hadi, Sepandi and Marx39), with consideration stress score as the primary outcome, the reduction of 3·49 for stress score in the intervention group in comparison with the control group, a standard deviation of 2·3 and 3·44, a type 1 error of 0·05 and 90 % power, the sample size for each group was calculated to be 26. After consideration of 25 % drop-outs during the study, thirty-two participants were considered for each study group. The G * Power software was used to calculate the sample size.
Statistical Package for Social Sciences (SPSS software, version 16, USA) was used for conducting statistical analysis. Categorical and continuous variables were summarised by frequency and percentage and mean and standard deviation (mean ± sd). The Shapiro–Wilk test, Q-Q, and histogram plots were used to assess the normal distribution of data. Categorical variables were analysed using the χ 2. Changes in dietary intake, physical activity, mental health and HRQOL scores were calculated as [post-intervention – pre-intervention]. Analysis of variance was used for between-group comparisons. The between-group comparisons for changes in mental health and HRQOL scores with adjusting for BMI as a confounder were conducted using analysis of covariance. The Bonferroni test was used for post hoc analyses. Within-group comparisons were done using a paired sample t-test. The per-protocol approach was used for data analysis, and a P-value less than 0·05 was considered significant.
Results
Participant recruitment and follow-up period of the study were carried out from April to September 2023. A total of 682 individuals were assessed for eligibility, which led to the participation of 128 eligible volunteers. Participants were randomly assigned to the study groups. During the study period, ten participants stopped to cooperate with the study due to various reasons. Of the participants who finished the study, fourteen were excluded from the final analysis. Finally, 104 participants (17/87, male/female) entered the final analysis (twenty-six in each group) with a mean age of 48·98 ± 7·27 (mean ± sd). Figure 1 depicts the recruitment and follow-up procedure of the study.
CONSORT flow diagram of the study: From participant recruitment to the final analysis.

Demographic and baseline characteristics of participants
Table 1 shows the demographic and baseline characteristics of the participants. No significant differences were observed considering participants’ demographic characteristics. Moreover, no alcohol consumption was reported by the participants. The between-group comparison did not show any statistical difference between participants in terms of age, height and weight. However, participants in the CurPro group had lower BMI in comparison to the other groups (P = 0·005) (Table 1).
Demographic and baseline characteristics of participants based on the groups

Abbreviations: CurPro, Curcumin\Probiotic; HTN, Hypertension; BMI, Body Mass Index.
* One way ANOVA and the Bonferroni post-hoc test showed significant differences with P-value less than 0.05.
Baseline MetS components
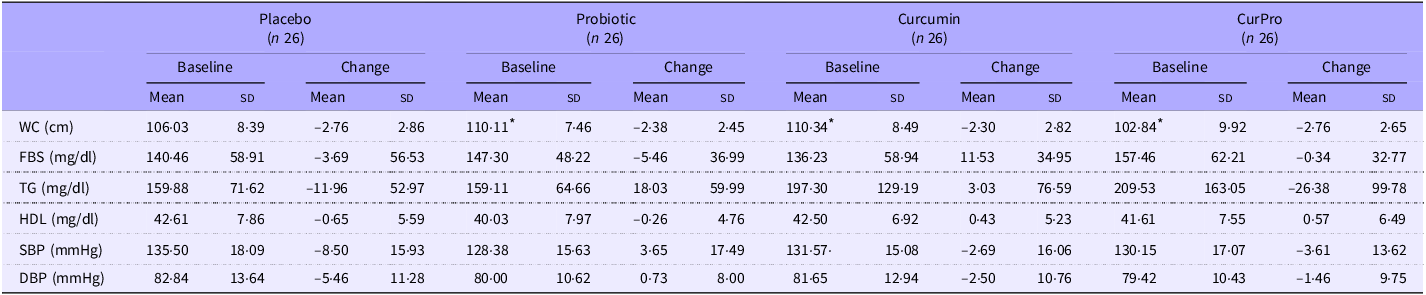
Participants in the study groups had no significant differences regarding fasting blood sugar, TAG, HDL, systolic blood pressure and diastolic blood pressure at baseline. However, participants in the CurPro group (102·84 ± 9·92 cm) had lower waist circumference in comparison with participants in the probiotic (110·11 ± 7·46 cm; P CurPro v. Probiotic = 0·018) and curcumin groups (110·34 ± 8·49 cm, P CurPro v. Curcumin = 0·013) (Table 2). Table 2 summarises baseline assessments of MetS components of participants based on the study groups.
Baseline assessments and changes of MetS components of participants based on the study groups

Abbreviations: MetS, Metabolic Syndrome; CurPro, Curcumin\Probiotic; WC, Waist Circumference; FBS, Fasting Blood Sugar; TG, Triglycerides; HDL, High-density Lipoprotein; SBP, Systolic Blood Pressure; DBP, Diastolic Blood Pressure.
Changes are calculated as: Post intervention – Pre intervention.
Results are shown as mean (sd).
* One way ANOVA and the Bonferroni post-hoc test showed significant differences with P-value less than 0.05.
Dietary intake and physical activity
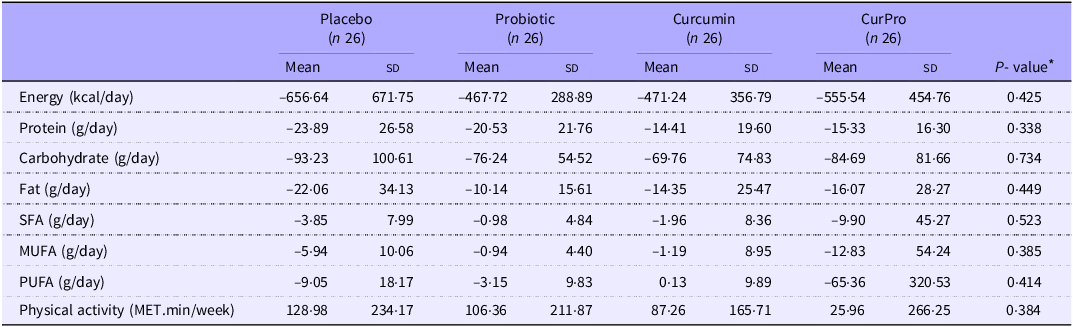
Table 3 indicates changes in dietary intake and physical activity level of the participants during the study period. Participants in all four groups showed a reduction in energy, protein, carbohydrate and fat consumption, but the between-group comparisons were not significant. On the other hand, physical activity increased in all groups, but the differences among the groups were not significant.
Dietary intake and physical activity changes of participants during the study period based on the study groups

Abbreviations: CurPro, Curcumin\Probiotic; SFA, Saturated Fatty Acids; MUFA, Mono Unsaturated Fatty Acids; PUFA, Poly Unsaturated Fatty Acids.
Changes are calculated as: Post intervention – Pre intervention.
Results are shown as mean (sd).
* One-way ANOVA.
A P-value less than 0.05 was considered significant.
Mental health and health-related quality of life
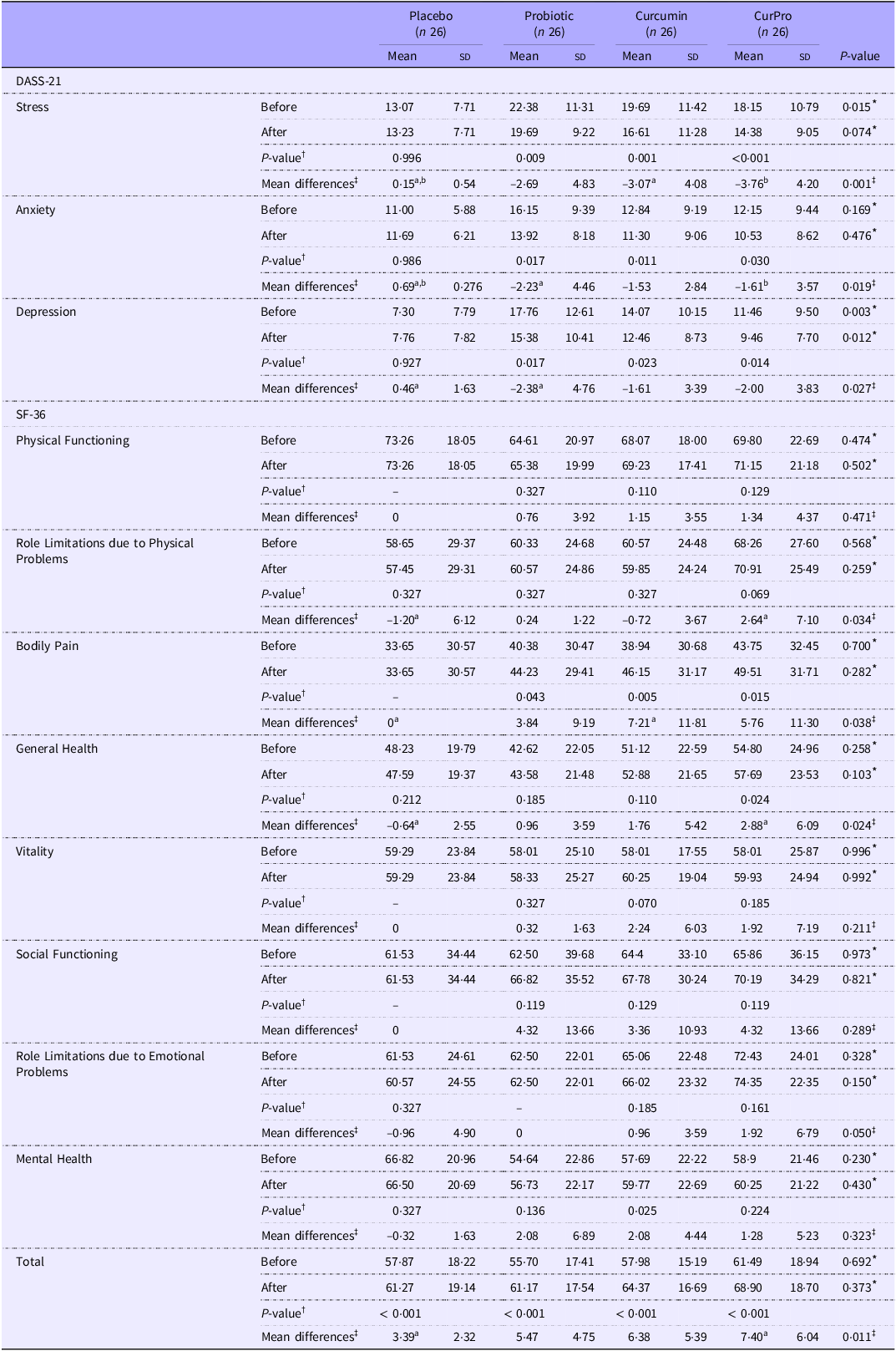
Table 4 shows pre-intervention, post-intervention and changes in mental health and HRQOL subdomain scores. During the study, participants’ stress scores increased in the placebo group (0·15 ± 0·54), this is while scores decreased in the probiotic (–2·96 ± 4·83, P Placebo v. Probiotic = 0·113), curcumin (–3·07 ± 4·08, P Placebo v. Curcumin = 0·031) and CurPro (–3·76 ± 4·20, P Placebo v. CurPro < 0·001) groups. Statistical analysis showed significant differences in changes in stress scores between groups (P = 0·001).
Comparison of mental health and quality of life scores of participants based on the study groups

Abbreviations: CurPro, Curcumin\Probiotic; DASS-21, Depression, Anxiety, and Stress Scale 21; SF-36, 36-Item Short Form Survay.
Changes are calculated as: Post intervention – Pre intervention.
Results are shown as mean (sd).
* One-way ANOVA.
† Paired sample t-test.
‡ ANCOVA adjusted for BMI, in case of significant results the Bonferroni post-hoc test was conducted for Post Hoc analysis. Results with the same super-script letter showed significant differences.
A P-value less than 0.05 was considered significant.
Similar trends were observed for anxiety (P = 0·019) and depression (P = 0·027) scores. Anxiety score increased in the Placebo group (0·69 ± 0·27) and decreased in Probiotics (–2·23 ± 4·46, P Placebo v. Probiotic = 0·049), curcumin (–1·53 ± 2·84 P Placebo v. Curcumin = 0·249) and CurPro (–1·61 ± 3·57 P Placebo v. CurPro = 0·034) groups. The scores for depression symptoms reduced in probiotic (–2·38 ± 4·76), curcumin (–1·61 ± 3·39) and CurPro (–2·00 ± 3·83) groups. This is while the depression score increased in the placebo group (0·46 ± 1·63; P Placebo v. Probiotic = 0·048, P Placebo v. Curcumin = 0·316, P Placebo v. CurPro = 0·066).
Among HRQOL subdomains’ scores, between-group comparisons for changes in physical functioning, vitality, social functioning, RE and mental health scores did not show any significant differences. This is while changes in RP (P = 0·034), bodily pain (P = 0·0·38), general health (P = 0·024) scores and the total score of SF-36 (P = 0·011) were significantly different between groups. Post hoc analyses showed differences for RP score (P = 0·040), general health score (P = 0·017) and total score (P = 0·007) of HRQOL between Placebo and CurPro groups, while for bodily pain score, a difference was seen between Placebo and Curcumin groups (P = 0·49). No side effect was reported by the participants in the visits with the physician.
Discussion
In the present study, the possible synergistic effect of CurPros co-supplementation in the form of drink powder was assessed on the mental health and HRQOL response. For the present study, a newly formulated drink powder containing curcumin and probiotics was prepared and used for 8 weeks by the adults with overweight/obesity and MetS. Results of the present study indicated that CurPro drink powder could possibly reduce stress and anxiety and improve the HRQOL of participants. However, no beneficial effect was observed for depression symptoms.
In the current study, an 8-week intervention showed promising effects of CurPros co-supplementation on reducing stress and anxiety symptoms, but the result was not significant for depression. However, probiotic consumption showed a promising effect on the reduction of depression symptoms in comparison with the placebo. Moreover, curcumin supplementation improved stress and anxiety. A previous study indicated that turmeric extract improved mental health in healthy individuals with overweight(Reference Uchio, Kawasaki and Okuda-Hanafusa27). To support the results of the present study, 1 g/d of curcumin for 30 days improved anxiety but not depression in individuals with obesity(Reference Esmaily, Sahebkar and Iranshahi40). In contrarily, 80 mg/d nano-curcumin supplementation in patients with diabetes and peripheral neuropathy did not improve stress but reduced anxiety and depression(Reference Asadi, Gholami and Siassi26). The discrepancy in the observed effect on stress could be due to the lower dosage of curcumin used in the study conducted by Asadi et al. (Reference Asadi, Gholami and Siassi26).
In contrast with the findings of the current study, it is believed that curcumin could improve depression(Reference Ramaholimihaso, Bouazzaoui and Kaladjian16). Curcumin could affect depression symptoms through various pathways. First, it could decrease monoamines and increase the serotonergic and dopaminergic transmission. In addition, the antidepressant effect of curcumin could be due to its action on the glutamatergic system that increases the levels of brain-derived neurotrophic factor(Reference Ramaholimihaso, Bouazzaoui and Kaladjian16). However, the reason for the lack of effects of curcumin on depression scores could be possibly due to the short duration of the study, the study population, and the fact that the participants of our study did not have severe depression at the baseline.
An 8-week probiotics supplementation was observed to improve mental health(Reference Lee, Hong and Kim41). The finding of the present study was in line with another study in which 8 weeks of supplementation with probiotics enhanced depression in major depressive disorder patients(Reference Kazemi, Noorbala and Azam42). Moreover, anxiety was observed to improve after probiotics supplementation(Reference Haghighat, Mohammadshahi and Shayanpour43). In addition, petrochemical industry employees have also benefited from the consumption of probiotics in order to improve their mental health(Reference Mohammadi, Jazayeri and Khosravi-Darani44). Contrary to our result, a recent meta-analysis indicated a stress-reducing effect of probiotic supplementation(Reference Zhang, Zhang and Li45). Subgroup analysis in the above-mentioned meta-analysis showed that long duration (12 weeks) of probiotic intervention reduced stress levels(Reference Zhang, Zhang and Li45).
Probiotics are known to amend mental health status by modulating proteins and neurotransmitters such as glutamate, serotonin and γ-aminobutyric acid(Reference Sharma and Bajwa46). Moreover, as probiotics ameliorate dysbiosis and amend gut microbiota, they could affect mental health through the gut–brain axis(Reference Sharma and Bajwa46). Mental health could also be improved after the production of short-chain fatty acids by probiotics and affecting G-protein-coupled receptors. Moreover, during sickness, the hypothalamic–pituitary–adrenal axis becomes dysfunctional, which leads to the production of stress hormones. Probiotics are able to amend hypothalamic–pituitary–adrenal axis activity by lowering cortisol and stress hormones(Reference Sharma and Bajwa46). All of the aforementioned mechanisms could explain the beneficial effects of probiotics on mental health.
The present investigation observed a promising effect of CurPro on stress and anxiety, but not depression. As positive results were observed in the Probiotic group for depression, non-significant results could be possibly due to the low dosage of curcumin (1 g per day or lower)(Reference Al-Karawi, Al Mamoori and Tayyar47) and the short duration of the study. However, it was seen that curcumin supplementation with dosages higher than 500 mg/d and for durations more than 6 weeks had positive effects on depression(Reference Fusar-Poli, Vozza and Gabbiadini30). Moreover, it was seen that curcumin supplementation could affect depression in patients with major depression, but the results were not significant for depression resulting from other medical conditions(Reference Fusar-Poli, Vozza and Gabbiadini30). Thus, the non-significant result for depression in the present study could be justified by the fact that the participants were not suffering from major depression, which mean score for depression in the study participants was under 21, and they did not suffer from severe depression at the beginning of the study.
As another finding of the current study, after 8 weeks of intervention, in comparison with the placebo group, CurPros consumption improved quality of life, general health and role limitation due to physical problems. However, no beneficial effects were observed for physical functioning, bodily pain, vitality, social functioning and role limitation due to emotional problems. It should be mentioned that curcumin supplementation improved bodily pain. In line with the present findings, turmeric extract consumption for 12 weeks did not improve the quality of life in healthy participants with overweight(Reference Uchio, Kawasaki and Okuda-Hanafusa27). Nouri-Vaskeh et al. (Reference Nouri-Vaskeh, Afshan and Malek Mahdavi48) observed improvements in HRQOL after 12 weeks of intervention with curcumin that supported the results of the present study in this regard. A recent meta-analysis also showed a strong quality-of-life-promoting effect of curcumin(Reference Sadeghian, Rahmani and Jamialahmadi19).
Various mechanisms were proposed for the effects of curcumin on quality of life. Curcumin could show a beneficial effect on HRQOL by decreasing calcitonin gene-related peptide, which is expressed by keratinocytes. Calcitonin gene-related peptide is known to be associated with chronic pain(Reference Sadeghian, Rahmani and Jamialahmadi19). In addition, it could reduce inflammation by down-regulating inflammatory and proinflammatory cytokines(Reference Sadeghian, Rahmani and Jamialahmadi19). Thus, through these effects, curcumin could possibly reduce perceived pain and improve the perception of the quality of life. Moreover, this could justify our observation on improving bodily pain in the curcumin group. Also, curcumin is believed to control various diseases such as metabolic(Reference Johnston, Korolenko and Pirro49), gastrointestinal(Reference Karolin Kamel and Sciences50) and bone(Reference Rohanizadeh, Deng and Verron51) disorders. It is suggested that curcumin could possibly ameliorate HRQOL through controlling these conditions. In addition, it is speculated that curcumin diminishes symptoms of chronic conditions, which finally improves HRQOL(Reference Sadeghian, Rahmani and Jamialahmadi19,Reference Vollono, Falconi and Gaziano52) .
No amending effects of probiotics on HRQOL were observed in the present study. Haghighat et al. (Reference Haghighat, Mohammadshahi and Shayanpour43) also did not observe any effect of probiotics on HRQOL in patients undergoing haemodialysis. This study used lower dosages of probiotics but had a longer duration(Reference Haghighat, Mohammadshahi and Shayanpour43). On the other hand, probiotic supplements were observed to increase quality of life(Reference Venkataraman, Jose and Jose53,Reference Arnold, Luna and Williams54) . A recent meta-analysis indicated that probiotics could slightly improve quality of life(Reference Le Morvan de Sequeira, Kaeber and Cekin24). These differences in results could be due to differences in participants, who were with T2DM(Reference Venkataraman, Jose and Jose53), autism(Reference Arnold, Luna and Williams54) and irritable bowel syndrome(Reference Le Morvan de Sequeira, Kaeber and Cekin24). Moreover, using different species of probiotics, including Lactobacillus and Bifidobacterium (Reference Arnold, Luna and Williams54), could possibly justify the contrasting results. In addition, although participants in Venkataraman’s(Reference Venkataraman, Jose and Jose53) study had the most similarity with those of the present study (T2DM which is a MetS component), differences in methodologies between studies such as duration (12 weeks v. 8 weeks) and using various strains in Venkataraman study(Reference Venkataraman, Jose and Jose53) could describe sources of discrepancies in the results. It should be noted that subgroup analysis based on the duration in the meta-analysis conducted by Le Morvan de Sequeira et al. (Reference Le Morvan de Sequeira, Kaeber and Cekin24) indicated that probiotic supplementation for 4 to 6 weeks could improve quality of life, but longer duration could not affect HRQOL which emphasises on the importance of the duration of probiotic supplementation.
Various health issues are amended by probiotic consumption, which could affect HRQOL. It is proposed that probiotics could reduce constipation, increase fecal short-chain fatty acids, gastrointestinal mucosal integrity, intestinal tight junctions and oral health, which can improve HRQOL(Reference Ale and Binetti55). However, the reason for achieving no positive results following probiotic supplementation could be due to the strains used in our study, study duration and possibly the relatively good quality of life in our study participants.
Results of the present study indicated that CurPro supplementation could possibly improve HRQOL. However, the results were not promising for probiotics. This could be due to using a few strains of probiotics. Moreover, duration could be a reason for insignificant results.
In Asian ethnic foods, curcumin is widely used due to its health-promoting effects. Also, there is a great insight into including probiotics in the daily intakes(Reference Abd El-Hack, El-Saadony and Swelum56). On the other hand, psychiatric problems are becoming prevalent worldwide(57), and the world is searching for novel natural and dietary methods for relieving psychiatric problems. Hence, considering the practical aspects of these combinations, it seems that curcumin and probiotics (especially their combinations) could possibly help improve mental health.
Limitations and strengths
The current study had some strengths. First, the CurPro co-supplementation in the form of drink powder was used to investigate their synergistic effect as an innovation. As another strength, relatively high dosages of probiotics and curcumin can be mentioned. However, there are some limitations as well. First, the small sample size and the short duration of the study could possibly affect the observed results. Moreover, it was better to use multi-strains of probiotics instead of two strains. Although spray-dried curcumin was used to improve its water solubility, using other water-soluble curcumin types, such as nano-curcumin or curcumin-piperine with higher bioavailability could better exert the drink powder’s possible effects. In addition, at the beginning of the study, participants showed low levels of anxiety, stress and depression, which could affect the final results of the study.
Conclusion
An 8-week supplementation of CurPro co-supplementation along with a low-energy diet in adults with overweight/obesity and MetS could possibly improve stress, anxiety and HRQOL. Curcumin supplementation lowered stress symptoms, while probiotic supplementation has shown promising effects on anxiety and depression. Nevertheless, curcumin and probiotic supplementation did not improve the HRQOL score. However, further studies in different populations with various dosages or probiotic strains and longer durations are warranted to reach robust results regarding depression and to better elucidate the mechanisms of action.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114525000923
Acknowledgements
This study was a part of a major project and extracted from Mohammad Ali Mohsenpour’s PhD dissertation in Nutrition (ID: 24422). The authors would like to thank the collaborators and participants of the study for taking part in this research. We send warm regards to the Vice-chancellor of Research of Shiraz University of Medical Sciences, Shiraz, Iran, for the financial support of the study (Grant number: 26818). The research team thanks the Department of Food Sciences and Technology, Shiraz University, for the dedicated support in using laboratories and facilities.
The study was supported by the Vice-chancellor for Research of Shiraz University of Medical Sciences with the grant number: 26 818.
M. A. M.: Research idea, study design, data acquisition, data interpretation and writing and preparation of the manuscript and critical revision of the manuscript. F. M.: Research idea, data acquisition and writing and preparation of the manuscript. Z. S.: Study design, data interpretation and critical revision of the manuscript. M. N.: Research idea, study design, data acquisition, data interpretation and critical revision of the manuscript. M. J.: Study design, data acquisition, data interpretation and critical revision of the manuscript. M. H. E.: Research idea, study design, data acquisition, data interpretation and critical revision of the manuscript.
Competing interests
There are no conflicts of interest.
Ethical statement
The study protocol was reviewed and approved by the Institutional Review Board and ethics committee of Shiraz University of Medical Sciences for being in accordance with the Helsinki Declaration of Ethics for Human Studies (Code: IR.SUMS.REC.1401·592, on 4 December 2022). The study protocol was prospectively registered in the Iranian Registry of Clinical Trials (IRCT.ir) under the registration code: IRCT20220315054289N2 (18 February 2023). All participants were informed about the study and signed informed consent form before participation in the study.