Childhood is a critical period for the development of healthy eating habits that potentially track into adulthood(Reference Craigie, Lake and Kelly1). Currently, children’s diets have been characterised by a high intake of energy-dense and nutritionally poor foods (as pastry products and soft drinks) and a low consumption of fruit and vegetables(Reference Williams, Buoncristiano and Nardone2). Moreover, the excessive consumption of meat and dairy products, which have a high environmental footprint, coupled with an inadequate intake of plant-based foods, suggests that children’s dietary patterns may not be environmentally sustainable(Reference Stehfest, Bouwman and van Vuuren3).
The Food and Agriculture Organization (FAO) defines sustainable diets as diets that minimise environmental impacts, contribute to food and nutrition security and promote a healthy life for present and future generations. These diets should be nutritionally adequate, safe and health-promoting while optimising natural and human resources(4). Various organisations have recognised the growing importance of sustainability in food policy-making(5,Reference Joseph and Clancy6) . Although there is a general understanding of the environmental impact of dietary patterns, based on a systematic review, there is no established tool for assessing the healthiness and sustainability of diets in the paediatric age group(Reference Teixeira, Afonso and Rodrigues7).
The EAT-Lancet recommendations on healthy diets from sustainable food systems are designed to promote a balanced and nutritious diet while considering the environmental impact of food production, aiming to achieve a sustainable food system for the future(Reference Willett, Rockström and Loken8). Recently, the World Index for Sustainability and Health (WISH) was developed for adults, building upon the EAT-Lancet reference diet(Reference Trijsburg, Talsma and Crispim9).
Family background, and mothers in particular, play an important role in the early development of children’s eating habits(Reference Savage, Fisher and Birch10). This influence is recognised to begin even before birth(Reference Ventura and Worobey11), as the diet of pregnant women, along with their body mass index (BMI), seem to influence the quality of their children’s diet later in life(Reference Biagi, Nunzio and Bordoni12). In addition, some parental feeding practices, defined as specific strategies used by parents to regulate the types and amounts of foods consumed by their children, may interfere with the development of healthy eating habits(Reference Yee, Lwin and Ho13).
Although the association between these family characteristics and healthy dietary patterns has been previously studied(Reference Vidhyashree, Raveendran and Priya14,Reference Favara, Maugeri and San Lio15) , to the best of our knowledge, this association has not been explored in the context of a healthy and, at the same time, environmentally sustainable dietary pattern in paediatric age. Given the importance of prioritising adherence to these specific diets, and understanding the associated health benefits(Reference Willett, Rockström and Loken8), it is crucial to understand the hierarchy of associated factors that may play a role in the acquisition of children’s dietary patterns. This insight is of particular importance for the effective planning of public health initiatives, which aim to enhance the quality of children’s diets(Reference Scaglioni, De Cosmi and Ciappolino16).
The objective of this study was to investigate the association between family characteristics (organised into a hierarchical theoretical framework) and adherence to the EAT-Lancet dietary recommendations in 7-year-old children from a population-based birth cohort.
Material & methods
Study design and population
The present study included participants, who are part of the ongoing population-based birth cohort Generation XXI, which has been described in detail elsewhere(Reference Larsen, Kamper-Jørgensen and Adamson17,Reference Alves, Correia and Barros18) . Mothers’ resident in the Porto Metropolitan area (northern Portugal) who delivered a live-born child, with a gestational age ≥ 24 weeks, in one of the five public maternity units, between April 2005 and August 2006, were eligible for enrolment in this study. Mothers were invited to participate within 24 to 72 hours of delivery and, among those invited, 91·4 % accepted. A total of 8647 infants and 8495 mothers were enrolled in the study. At the ages of 4 and 7, the families of these children were invited to participate in evaluations, with participation proportions of 86 % and 80 %, respectively. Data were collected through face-to-face interviews or via telephone using an abbreviated version of the questionnaire when the family was unable to be physically present (20 % and 15 % at 4 and 7 years old, respectively).
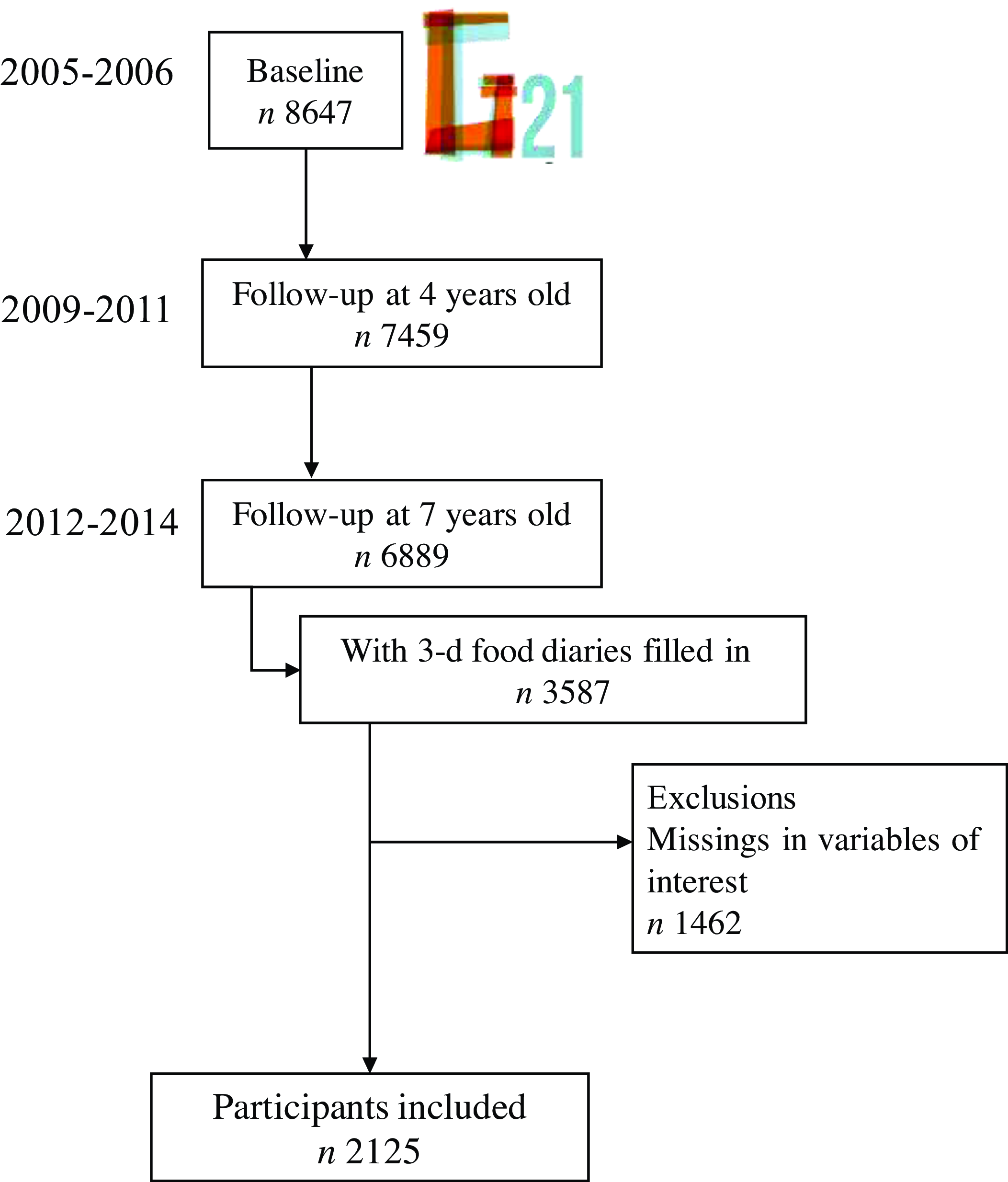
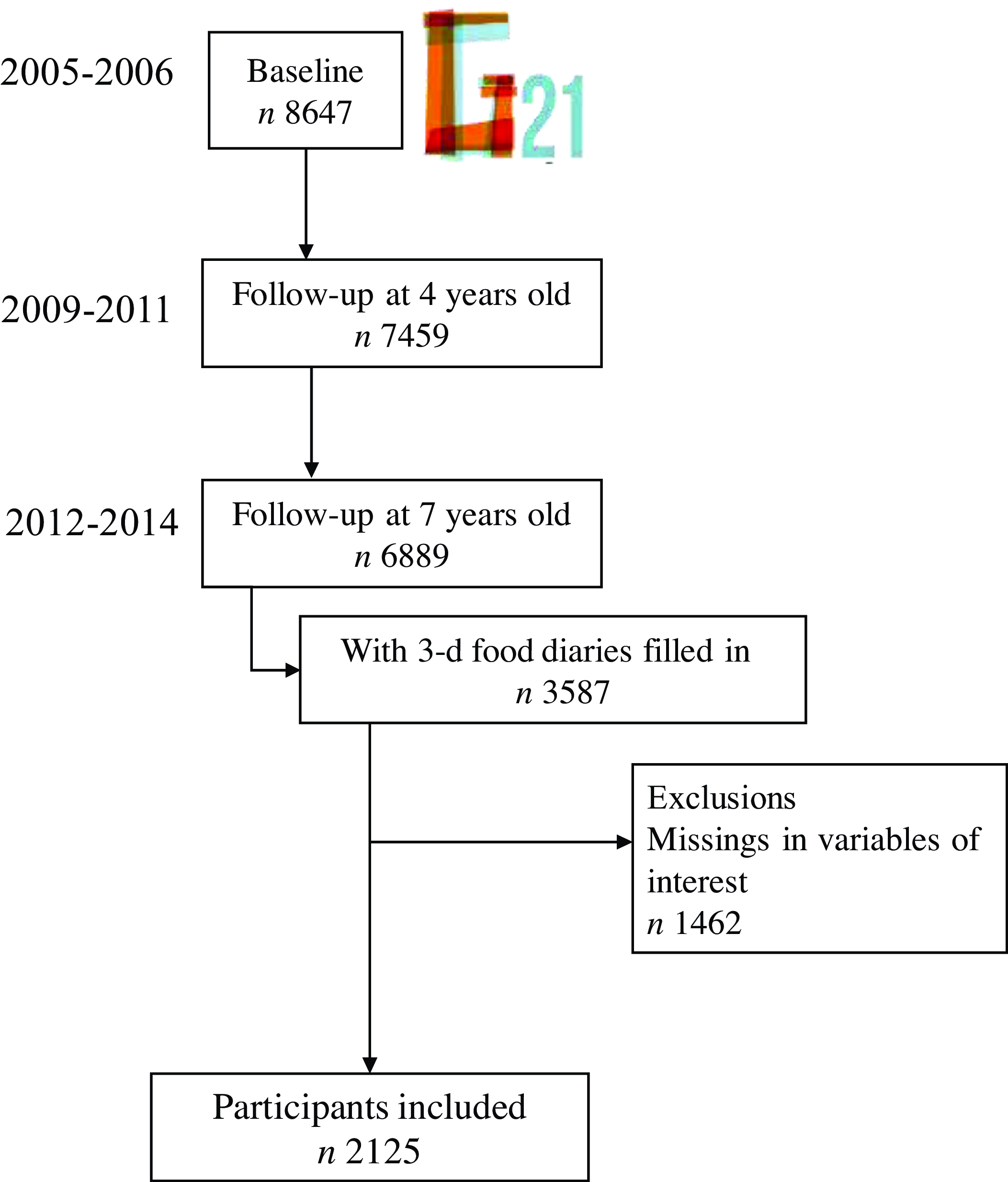
The present study included children at the age of 7, who completed 3-day food diaries (n 3587). From the initial sample, children with incomplete information on variables of interest (such as maternal feeding practices and dietary intake) were excluded from the study (n 1462), resulting in a final sample size of 2125 children. The flowchart of the participant’s selection is available in Figure 1. A comparison of baseline characteristics between the included participants and the remaining cohort (n 6522) showed that participating mothers were slightly older (mean = 30·4 years; sd = 4·8 v. mean = 28·5, sd = 5·8) and more educated (mean = 11·8 years of complete schooling years; sd = 4·3 v. mean = 10·0, sd = 4·2). However, the magnitude of the differences was not substantial, as indicated by Cohen’s effect size values (0·36 and 0·42, respectively)(Reference Husted, Cook and Farewell19). This means that the reported significant differences were likely a result of the large sample size rather than variations in the participants’ characteristics.
Flow chart of participant’s selection (Generation XXI).
All phases of the study complied with the Ethical Principles for Medical Research Involving Human Subjects expressed in the Declaration of Helsinki. The baseline and follow-up evaluations at 4 and 7 years of age were approved by the University of Porto Medical School/S. João Hospital Centre Ethics Committee. Each participant’s legal representative received a comprehensive explanation of the study’s objectives and methodology, and written informed consent was obtained at the baseline and subsequent follow-up assessments. The baseline evaluation was approved by the Data Protection National Commission, and the study follows the present EU General Data Protection Regulation under close supervision of the Data Protection Office of ISPUP.
Data collection
A wide range of characteristics were assessed, including socio-economic status, healthcare utilisation and lifestyle behaviours, at the child’s birth and 4 and 7 years of age. These data were retrieved from clinical records or collected through in-person interviews and physical examinations, performed by trained professionals. A detailed description of the data included in this study can be found below.
At the child’s birth
Birth data such as the child’s sex, gestational age (in weeks) and birth weight (in grams) were retrieved from clinical records at baseline. Maternal age and completed years of schooling were asked to mothers, as well as marital status, household income and employment status. Maternal marital status was assessed as married or cohabiting v. single, divorced or widowed. Monthly household income was categorised as ≤ 1000 €, 1001–2000 € and > 2000 €. Maternal current employment status was defined as working (part or full-time, student and working student) v. not working (unemployed, retired and housewife) at the time the questionnaire was completed.
At the child’s birth, data on smoking habits during pregnancy were collected, categorising mothers as smokers or non-smokers. Information on self-reported gestational diabetes during the current pregnancy was also gathered, along with maternal height and pre-pregnancy weight to calculate BMI, as weight divided by the squared height (kg/m2).
At the child’s 4 years of age
Maternal weight was measured and recorded to the nearest 0·1 kg, and height was measured without shoes to the nearest 0·1 cm to calculate maternal BMI when the child was 4 years of age.
Maternal dietary intake was evaluated using a qualitative food frequency questionnaire (FFQ), adapted from a previously validated questionnaire for the Portuguese adult population(Reference Lopes, Aro and Azevedo20). This FFQ assesses consumption over the past 12 months and comprises eighteen items with response options on a nine-point frequency scale, ranging from ‘never’ to ‘≥ 4 times per day’. The consumption frequencies were converted into daily frequencies (e.g. one instance per week was converted to 1/7 of a day or 0·14 instances per d).
Definition of a maternal diet quality score
Based on maternal dietary intake at the child’s 4 years of age, a diet quality score previously described(Reference Durão, Severo and Oliveira21) was calculated in this study. The score was defined based on eight food components: milk, fish, red and processed meat, bread, fruit, vegetables, cakes and salty pastries, and sugar-sweetened beverages. Each component was divided into quartiles, and a scoring system was applied. Scores were assigned on a scale of 1–4, according to increasing quartiles of consumption (milk, fish, bread, fruit and vegetables) or decreasing quartiles of consumption (red and processed meat, cakes and salty pastries, and sugar-sweetened beverages). The total points assigned were summed up to derive a continuous score of diet quality, which could range from 8 to 32 points. A higher score indicates a better diet quality.
Parental child feeding practices
Parental child feeding practices were assessed using a combined version of the Child Feeding Questionnaire (CFQ)(Reference Birch, Fisher and Grimm-Thomas22) and the scales measuring overt and covert control(Reference Ogden, Reynolds and Smith23). These were completed by the caregivers themselves (95·3 % of mothers). The maternal feeding practices subscales included the following dimensions: restriction (the extent to which parents control the child’s access to foods or opportunities to consume those foods) (three items), pressure to eat (parents’ insistence or demands that their children eat more food) (four items), monitoring (the extent to which parents track what and how much the child is eating) (three items), overt control (represented by a firm attitude from parents about what, how much, where and when the child eats, which can be perceived by the child) (five items) and covert control (in which the child is unable to detect the control; e.g. avoiding buying energy-dense foods) (four items). Participants were assigned mean scores for each dimension if they provided at least 50 % of the answers. The scores ranged from 1 to 5, with higher scores indicating a greater degree of practice. CFQ has previously been adapted and validated in Portuguese children from the Generation XXI cohort(Reference Real, Oliveira and Severo24). Furthermore, the dimensions of this questionnaire have demonstrated satisfactory reliability in a previous study(Reference Durão, Andreozzi and Oliveira25).
Definition of patterns of maternal child feeding practices
Previously, principal component analysis identified three patterns of maternal child feeding practices(Reference Moreira, Severo and Oliveira26), considering the CFQ subscales dimensions. The three patterns of maternal child feeding practices identified by principal component analysis were labelled: ‘perceived monitoring’ (identifying mothers with higher levels of monitoring, perceived responsibility and overt control), ‘restriction’ (describing mothers with higher covert control, concern about child’s weight and restriction) and ‘pressure to eat’ (defining mothers with higher levels of pressuring the child to eat more and overt control). The scores for these factors were on a standard deviation scale, ranging from –3 to 3. A score of 0 represented mothers’ ratings that were close to the sample’s average, while a score of –2 corresponded to maternal ratings that were 2 sd below the sample mean(Reference Moreira, Severo and Oliveira26). These scores were subsequently calculated to each participant in the study.
At the child’s 7 years of age
The family structure was classified into two types of families: ‘family with both parents’ and ‘single-parent family’ (meaning living only with the mother or the father) at the age 7. Information about whether they lived or not with siblings was also obtained. Monthly household income was updated and categorised as ≤ 1000 €, 1001–2000 € and > 2000 €. In addition, information on children’s lifestyles, such as their engagement in regular sports activities, were collected.
A physical examination of the children was performed, including their height and weight, measured by trained professionals following standard procedures(Reference Gibson27). Weight was measured to the nearest tenth of a kilogram (Tanita® digital scale, Arlington Heights) in light clothing and without shoes, and height was measured to the nearest tenth of a centimetre (Seca® wall stadiometer). BMI was calculated, and children were classified according to age- and sex-specific BMI z-scores (BMIz) developed by the World Health Organization (WHO). Overweight (pre-obesity plus obesity) was defined as a BMI for age z-score >+1 sd (Reference Onis, Onyango and Borghi28).
At the age of 7, dietary intake of children were collected by a 3-day food diary (2 weekdays and 1 weekend day), completed by parents or other main caregivers, prior to the face-to-face interview, as previously described(Reference Moreira, Severo and Oliveira29). Data were collected throughout all four seasons (winter, autumn, spring and summer) from 2012 to 2014. Oral (by telephone) and written instructions were provided for the correct completion of the food diaries and for the quantification of food portions. Parents were instructed on the use of household measures and standard units for the quantification of food portions, and photographic examples were provided for more accurate assessment. They were also asked to provide detailed descriptions of each food and drink consumed by the child, including the method of preparation, recipes and place of consumption, whenever possible. It was advised to let children follow their usual diet and to ask for the help of other caregivers in case the child was out of the home during the day. During the face-to-face interview, the fieldwork team was responsible for receiving and thoroughly inspecting the food diaries to ensure their completeness. In cases where any information was missing, the team would request a revised report to be sent by mail at a later time.
After, the information was handled by a team of trained nutritionists. Energy and nutrient intake were calculated using the methodology of the software eAT24 (Electronic Assessment Tool for 24-h recall)(Reference Goios, Severo and Lloyd30). This software was previously validated(Reference Goios, Severo and Lloyd30) and includes the harmonised food classification and description system proposed by the European Food Safety Authority (EFSA) – the FoodEx2 classification system(31) and food composition tables from Portugal and other sources to allow the conversion into nutrients(Reference Lopes, Torres and Oliveira32).
Definition of the World Index for Sustainability and Health (WISH) dietary pattern
To measure the adherence to the EAT-Lancet recommendations, an adapted version for paediatric age of the WISH score(Reference Teixeira, Afonso and Severo33) was applied to the food consumption data. The WISH, originally developed for adults(Reference Trijsburg, Talsma and Crispim9), consists of thirteen food groups: grains, vegetables, fruits, dairy products, red and processed meat, fish, eggs, chicken and other poultry, legume grains, nuts, unsaturated fats, saturated fats, soft drinks and added sugars. Scores for each component can range from 0 to 10, reflecting adherence to the EAT-Lancet dietary recommendations. The total score, ranging from 0 to 130, indicates the overall health and environmental sustainability of the diet, with higher scores indicating a healthier and more environmentally sustainable diet(Reference Trijsburg, Talsma and Crispim9). WISH was estimated for each participant based on the individual consumption of each food group and the recommended thresholds of the EAT-Lancet Commission. The details of each component, scoring criteria and their respective recommendations are presented in Table A of online Supplementary material.
Statistical analysis
Continuous variables were summarised by means and sd and categorical variables by counts and proportions.
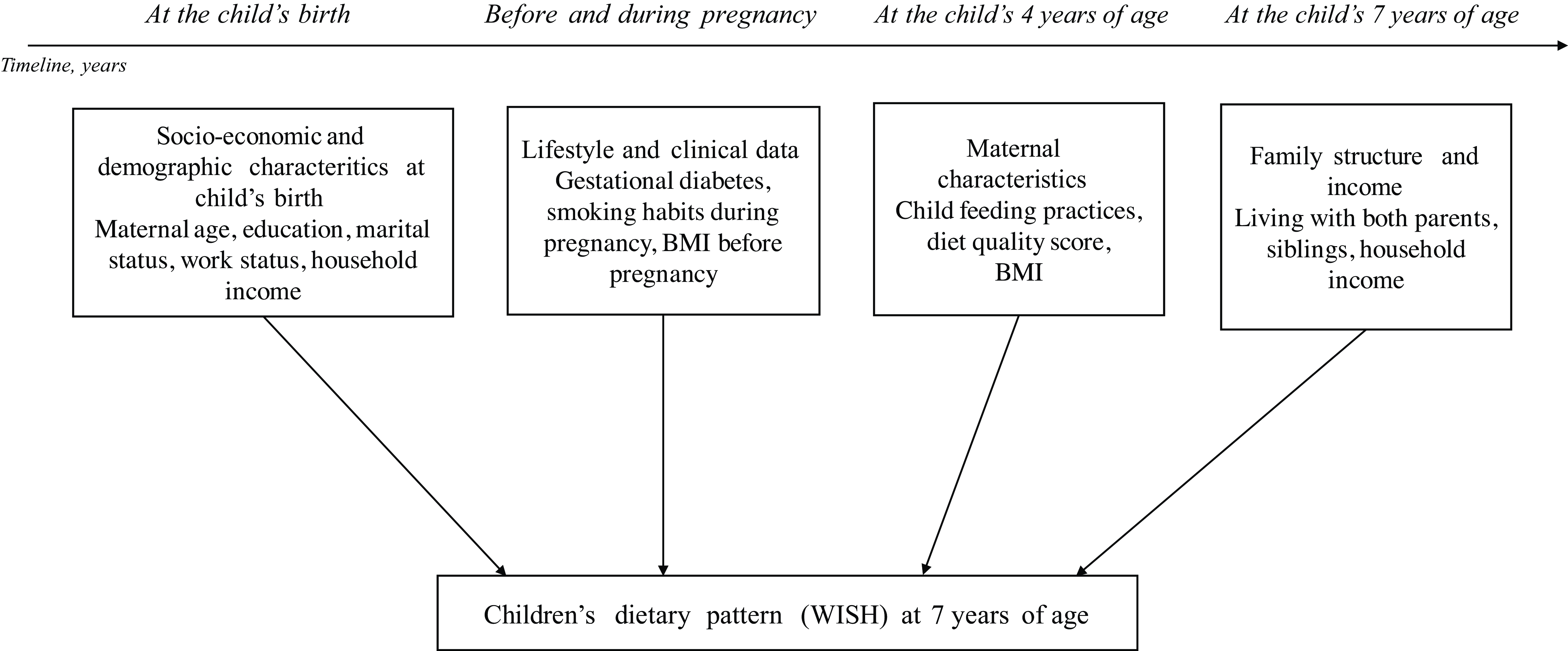
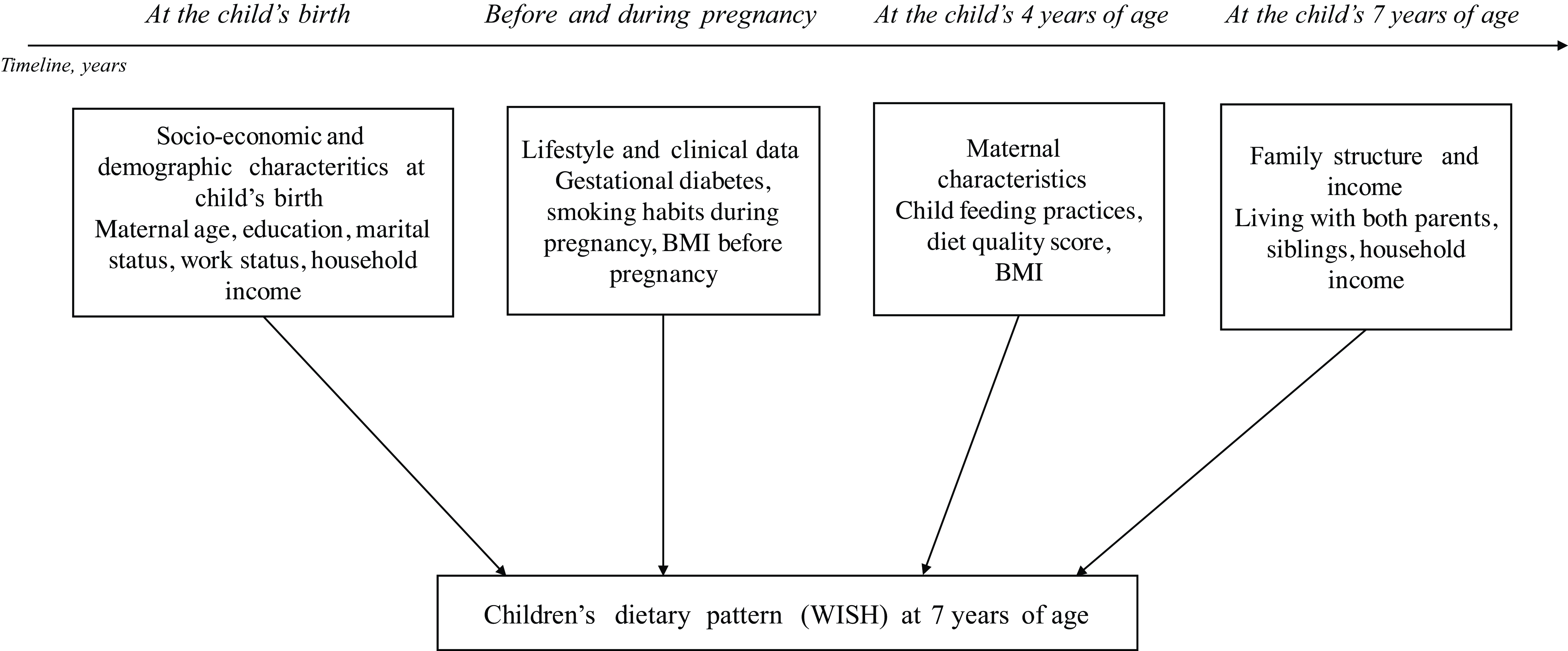
To address the aim of this study more effectively, a theoretical framework (Figure 2) based on previous models(Reference Victora, Huttly and Fuchs34–36) and ensuring time precedence between blocks of variables was established. First, we conducted a comprehensive review of the literature to identify relevant variables related to adherence to a healthy diet in childhood(Reference Biagi, Nunzio and Bordoni12,Reference Yee, Lwin and Ho13,35,Reference Wen, Kong and Eiden37,Reference Suzuki, Ando and Sato38) . Then, we checked which variables were available within the Generation XXI cohort with potential to be included in this framework, based on the theoretical and empirical relevance found. This predefined theoretical framework was based on (a) socio-economic characteristics at the child’s birth, (b) maternal characteristics before and during pregnancy, (c) maternal diet and feeding practices at the child’s 4 years of age and (d) family characteristics at the child’s 7 years of age. Variables were organised to reflect temporal precedence, ensuring that socio-economic characteristics at the child’s birth influence maternal characteristics during pregnancy, which in turn impact feeding practices and, finally, family characteristics at 7 years of age.
Theoretical framework of maternal and other family determinants of children’s dietary pattern. This theoretical framework was based on previous works (34, 35, 36). WISH, World Index for Sustainability and Health.
Associations between exposures (mother and other family characteristics) and adherence to the adapted WISH at 7 years of age were measured through hierarchical linear regressions models, obtaining crude and adjusted β regression coefficients and the respective 95 % confidence intervals (95 % CI). A step-by-step approach was used. Firstly, univariate models were applied for each variable considered in the framework. Only variables that reached statistical significance were then conceptually grouped into blocks (blocks a, b, c and d previously described). Multivariable models were then fitted for these blocks, with variables within each block being mutually adjusted. Considering a high correlation between maternal education years and the household income both at baseline and when the child reached 7 years of age, the inclusion of maternal education was chosen for the adjusted models as it yielded the highest improvement in Negelkerke’s R2. Models were further adjusted for child’s sex and sports practice at the age of 7. No significant child’ sex interaction was observed in the associations under study; hence, stratification was not applied in the models.
The hierarchical linear regression analysis used the coefficient of determination, Negelkerke’s R2, to evaluate the factors (i.e. characteristics) with the greatest relevance for the children’s dietary pattern, meaning a higher score (greater adherence) to the WISH(Reference Nagelkerke39).
A sensitivity analysis was conducted to examine the associations between mother and other family characteristics and the WISH score into quartiles (instead of a continuous variable), using a multinomial logistic regression, where all four blocks were mutually adjusted.
A significance level of 5 % was assumed, as well as independence between observations. Analyses were performed in the IBM® SPSS® Statistics version 28.
Results
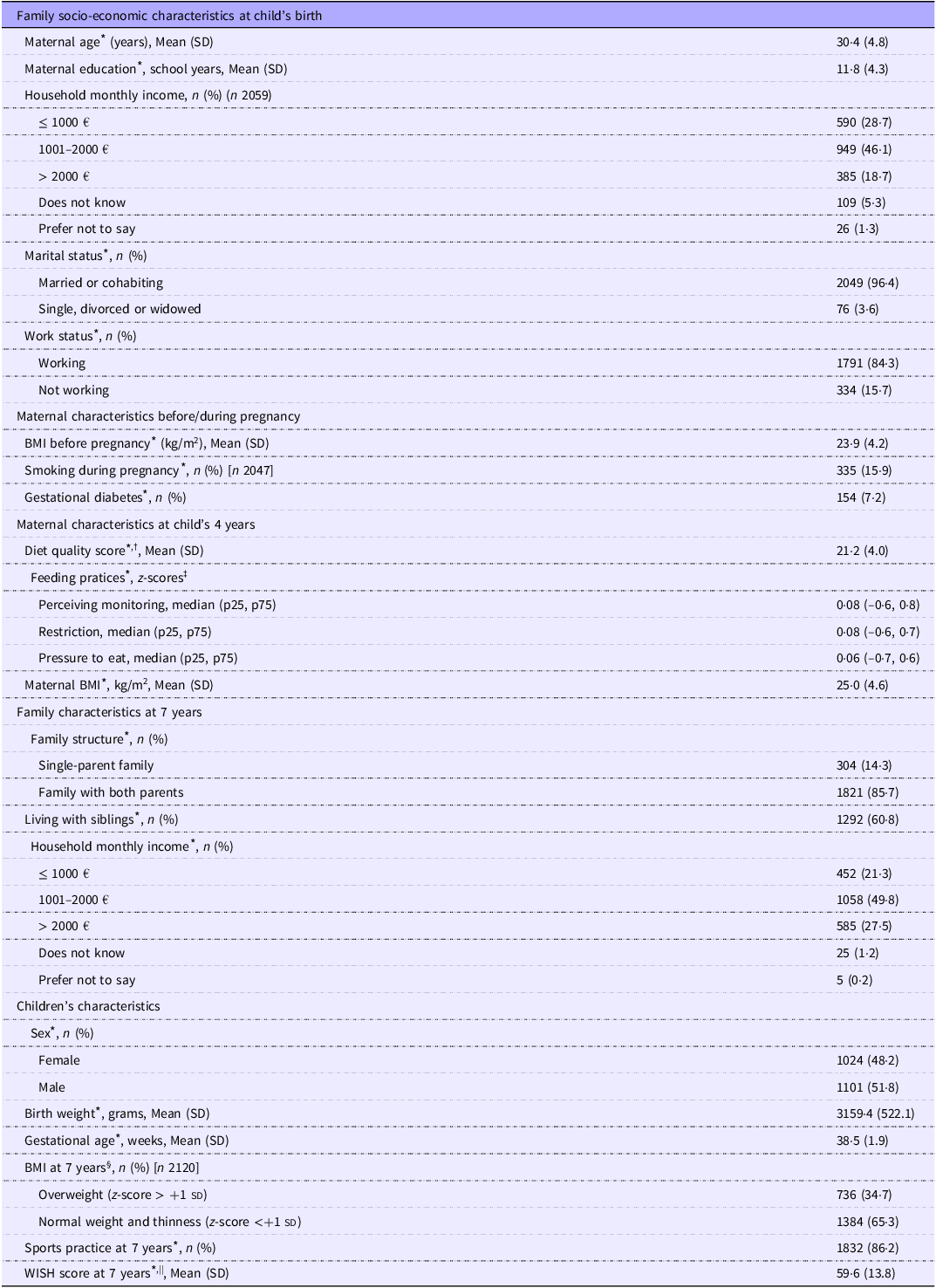
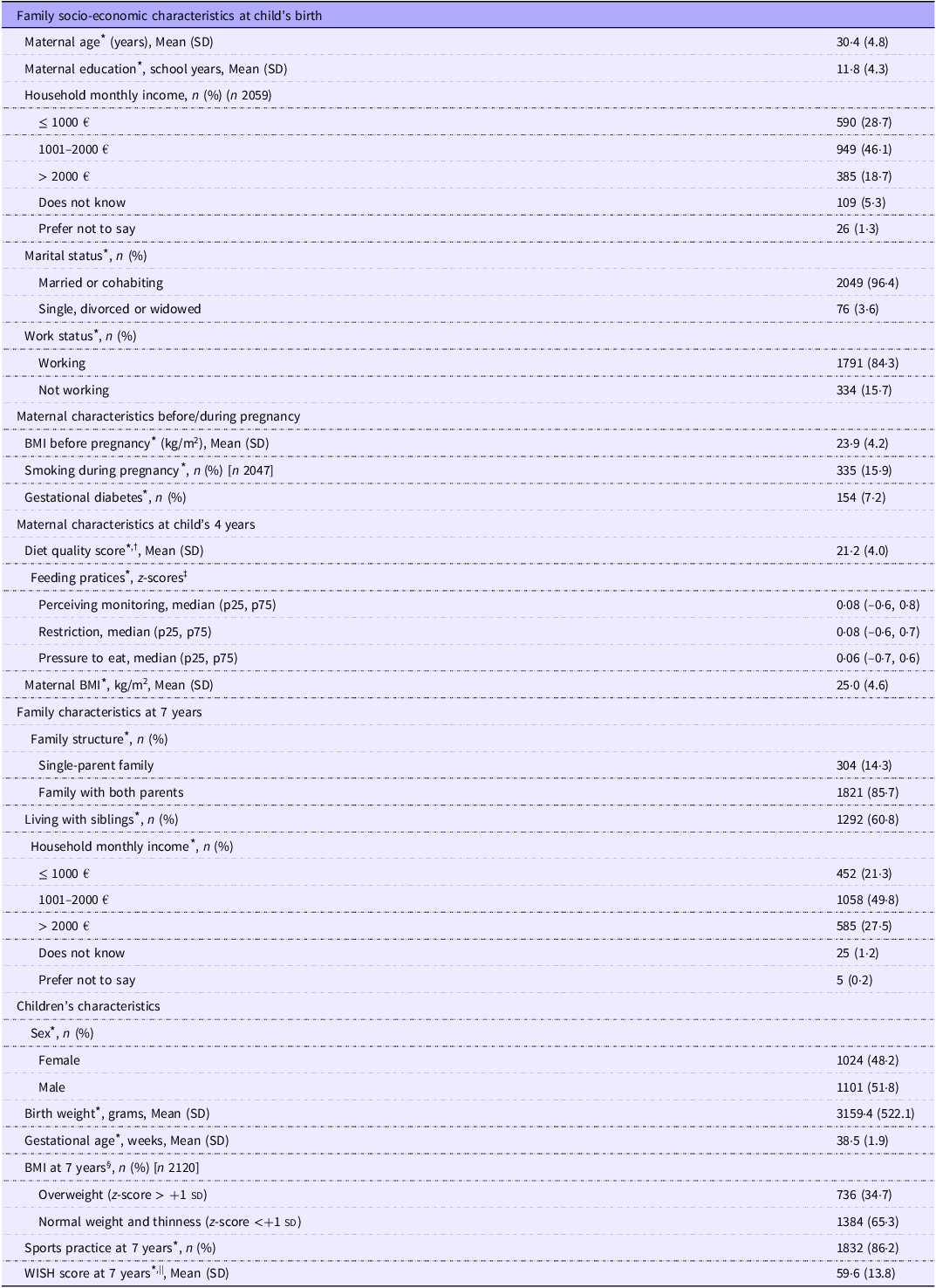
At baseline, mothers had a mean age of 30·4 years (sd = 4·8) and 11·8 years of schooling (sd = 4·3). The majority of mothers were married or cohabiting (96·4 %) and employed (84·3 %). Before pregnancy, mothers had a mean BMI of 23·9 kg/m2 (sd = 4·2), and 15·9 % smoked during pregnancy. At the child’s 4 years of age, mothers had a mean diet quality score of 21·2 points (sd = 4·0, ranging from 8 to 31; possible range 8–32). Approximately half of the children were males (51·8 %), and at 7 years of age the majority of them lived with both parents (85·7 %) and had siblings (60·8 %). The average WISH score was 59·6 points (sd = 13·8, ranging from 10·6 to 100; possible range 0–130) (Table 1).
Characteristics of families and their 7-year-olds from the Generation XXI birth cohort with 3-d food diaries and complete data in variables of interest (n 2125)
p, percentile; SD: stadard deviation; WISH, World Index for Sustainability and Health.
* Data on these variables are available for all the participants in this analysis (n 2125).
†Possible range from 8 to 32 (21); ‡possible range from −3 to 3 (26); §defined according to the WHO (28); ||possible range from 0 to 130 (33).
The food consumption of this sample, in g/day, according to the thirteen food groups evaluated in the WISH score, is presented in Table B of online Supplementary material. The high children’s consumption (in grams) of red and processed meats (median = 65·2, percentile 25–75 = 41·6–89·6) and dairy products (median = 504·4, percentile 25–75 = 385·2–626·7) is highlighted, as well as the low consumption (in grams) of legume grains (median = 6·5, percentile 25–75 = 0·0–14·4) and nuts (median = 0·0, percentile 25–75 = 0·0–0·0).
The consumption of these thirteen food groups according to the distribution of the WISH score by quartiles is also described in Table C of the online Supplementary material. In addition, the sample characteristics according to the WISH quartiles are described in online Supplementary Table D.
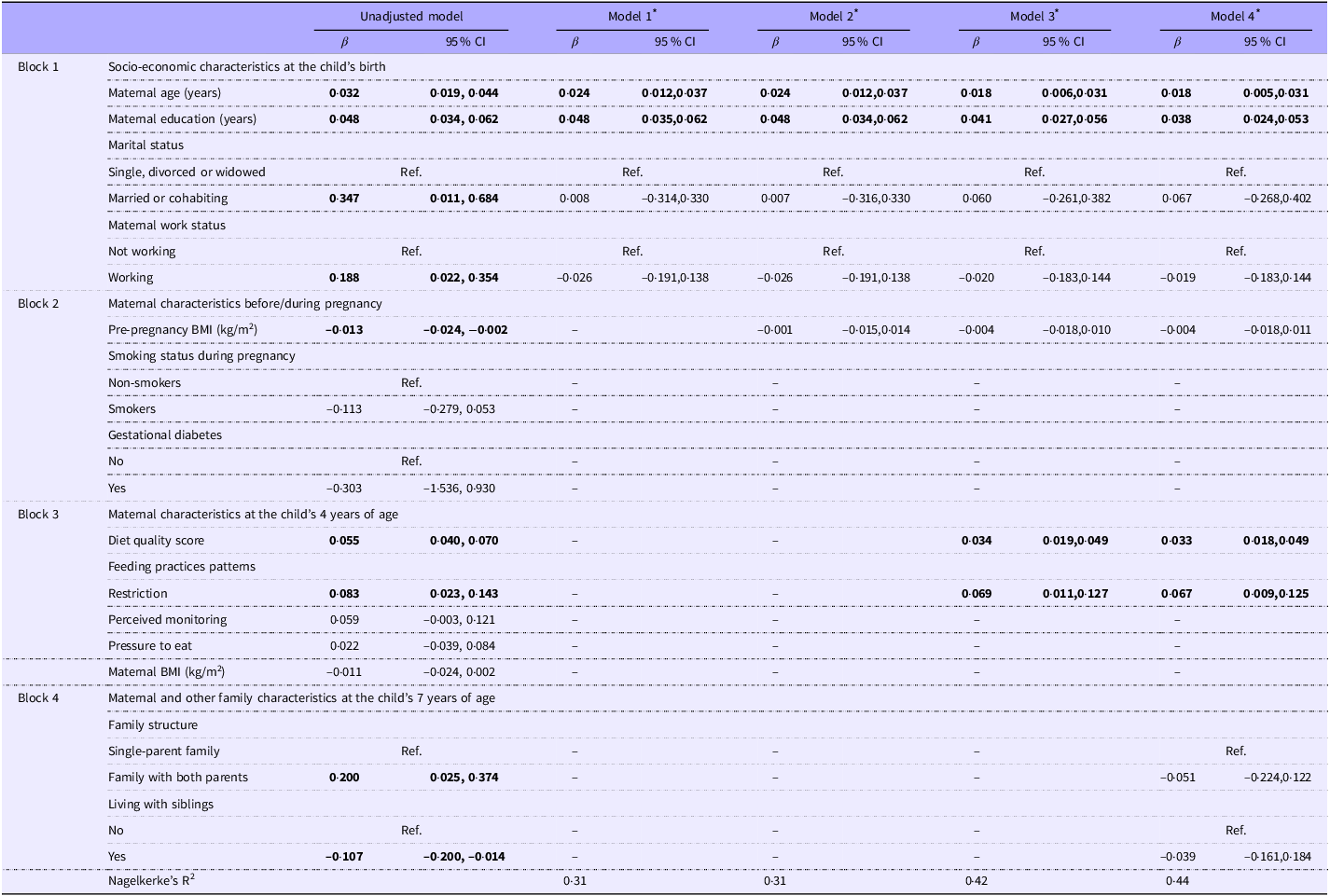
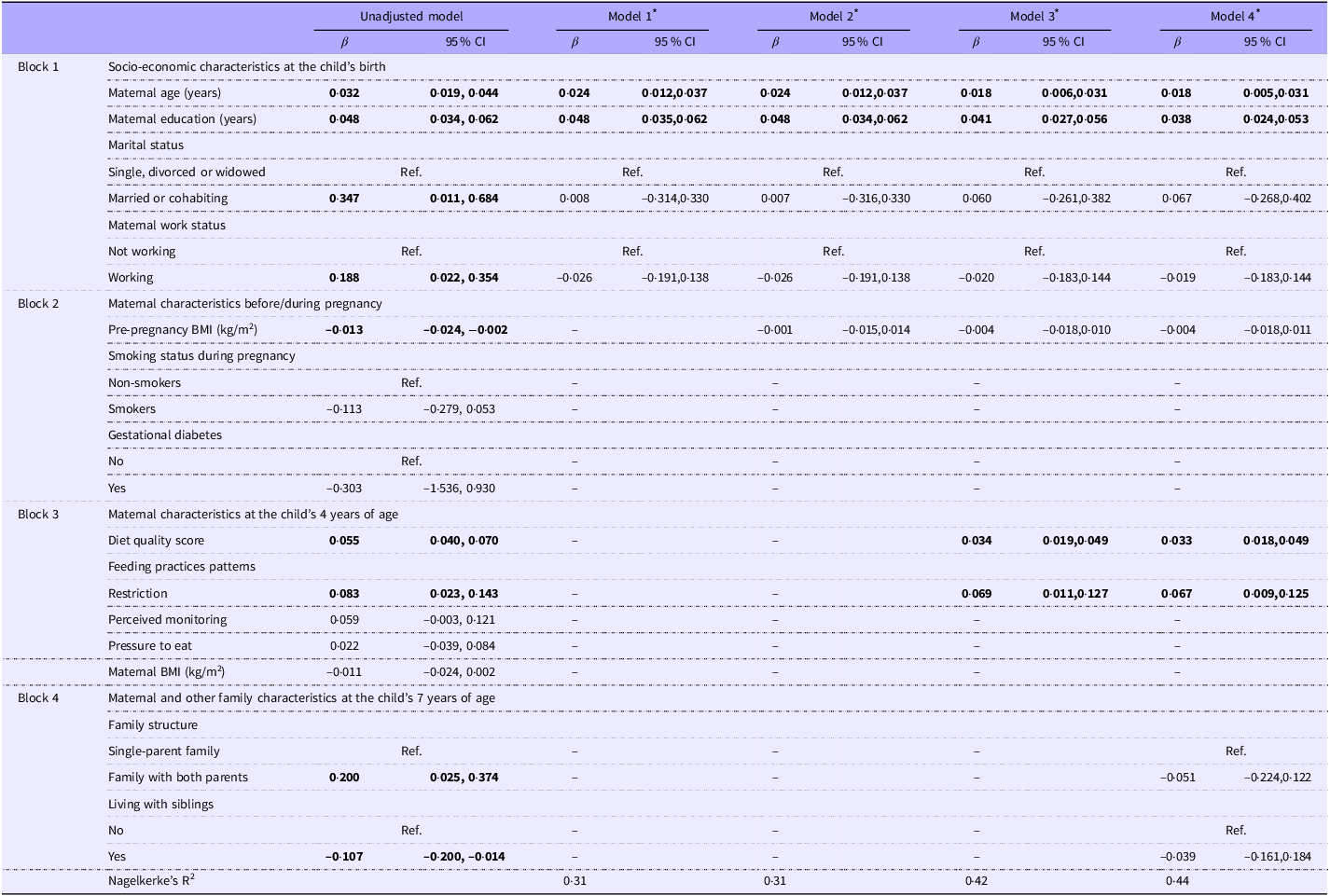
Table 2 presents the associations between maternal and other family characteristics and adherence to the adapted WISH at the age of 7. In statistical analysis, a predefined theoretical framework (Figure 2) was followed by the sequential addition of blocks of variables into the model. First, the socio-economic characteristics at the child’s birth were analysed (model 1). It was found that maternal age and education had a significant overall effect, with increasing age and education, resulting in a significantly higher score of the adapted WISH at the age of 7. These characteristics (maternal age, education, marital status and work status) collectively accounted for 31 % of the variance of the outcome under study (WISH score), as determined by the Nagelkerke’s R2. The inclusion of pre-pregnancy BMI did not yield significant effects on the associations under study, as the previous estimates remained unchanged (model 2). The addition of maternal diet and feeding practices at the age of 4 years (model 3) showed positive associations between the maternal diet quality score and the use of restrictive feeding practices and adherence to the adapted WISH at the age of 7. The inclusion of this set of variables led to an 11 % increase in the model’s explanatory power (Nagelkerke’s R2 = 42 %). Lastly, family characteristics at 7 years old were added (model 4). However, the inclusion of these variables did not result in any significant changes in the model estimates.
Hierarchical multivariable liner regression associations between maternal and other family characteristics and adherence to the World Index for Sustainability and Health (WISH) in 7-year-olds from the Generation XXI birth cohort (n 2125)
Statistically significant associations are highlighted in bold.
Nagelkerke’s R2: explained variance of each model in the step-by-step approach (block of variables sequentially added).
* Blocks of variables (1. Socio-economic characteristics of mothers before the child’s birth; 2. maternal characteristics before/during pregnancy; 3. maternal characteristics at the child’s 4 years of aged; 4. family characteristics at the child’s 7 years of age) were sequentially added into the analysis, if significantly associated with the WISH score in the unadjusted model. Maternal age, education, marital and work status (Block 1), were added do model 1. Pre-pregnancy BMI (Block 2) was added to model 2. Mothers’ diet quality score and restrictive feeding practices (Block 3) were added to model 3. Family structure and living with siblings (Block 4) at the child’s 7 years of age were added to model 4. Child’s sex and practice of sports at 7 years old were added as additional covariates in all models.
In the final model, maternal age and education at baseline (i.e. child’s birth) were associated with a higher adherence to the adapted WISH at the age of 7 years (β = 0·018, 95 % CI 0·005, 0·031; β = 0·038, 95 % CI 0·024, 0·053, respectively). Also, when the child was 4, the maternal diet quality score and the use of more restrictive feeding practices were associated with increased scoring in the adapted WISH at the age of 7 (β = 0·033, 95 % CI 0·018, 0·049; β = 0·067, 95 % CI 0·009, 0·125, respectively). Despite the absence of a sex interaction in the associations under study, particularly in this analysis, distinct results were exhibited for females and males, with more restrictive feeding practices being significantly associated with a healthier and more environmentally sustainable dietary pattern only in females (β = 0·093, 95 % CI 0·014, 0·172) (results only shown in text).
In a sensitivity analysis, associations were tested considering the WISH score distributed into quartiles (instead of a continuous variable) and results are summarised in online Supplementary Table E D. Similar results were obtained for the upper quartile of the WISH score, giving robustness to our findings.
To identify the key factors influencing the children’s dietary pattern, variables significantly associated with the WISH in model 4 were systematically removed one by one from the final model. Maternal education (assessed at baseline, in completed years of schooling) and the maternal diet quality (at the child’s 4 years old) were the key factors associated with the adherence to the adapted WISH at the age of 7. The removal of these variables from the final model produced the biggest drop in Nagelkerke’s R2 (full v. reduced model: R2 = 42 % v. R2 = 33 % and R2 = 42 % v. R2 = 37 %, respectively) (results presented only in text).
Discussion
The main findings from this study suggest that maternal characteristics were associated with greater adherence to a healthy and environmentally sustainable diet at the age of 7. Maternal age and education at the child’s birth were positively associated with the adapted WISH score. At the age of 4, the maternal diet quality score and the use of more restrictive feeding practices (including dimensions of covert control, i.e. a type of control not perceived by the child, concerns about the child’s weight and food restriction) were associated with a higher adherence to the WISH when they were 7 years old. A methodology of consecutive addition of blocks of variables into the models suggests that maternal education at the child’s birth and maternal diet quality at the child’s 4 years of age were the key factors associated with children’s adherence to the adapted WISH.
According to the WHO, socio-economic characteristics significantly influence lifestyles and overall well-being(35). Individuals’ socio-economic status determines their exposure and vulnerability to health-compromising conditions(35). Similarly, it is well documented that maternal sociodemographic characteristics, including age, education level and income, are positively correlated with the promotion of healthier dietary habits during childhood(Reference Scaglioni, De Cosmi and Ciappolino16). Indeed, in this study, these characteristics account for approximately one-quarter of the variance of the WISH score. Specifically, mothers who are older and more educated have children with healthier and more environmentally sustainable diets at school age. Additionally, maternal education at the child’s birth was identified as one of the key factors influencing children’s diet. These findings are consistent with those reported in the literature regarding healthy dietary patterns(Reference Durão, Severo and Oliveira21,Reference Wen, Kong and Eiden37) .
A recent systematic review(Reference Mannino, Sarapis and Moschonis40) has showed that a higher pre-pregnancy BMI in mothers has been associated with an increased risk of their children developing unhealthy eating habits. These include consuming a diet high in ultra-processed foods, added sugars and unhealthy fats, which are typically considered foods with a high environmental footprint. In this study, a higher pre-pregnancy BMI was associated with a lower adherence to the EAT-Lancet dietary recommendations. However, in the adjusted model, this result lost both magnitude and significance, suggesting that the initial association might be explained by maternal age and education at baseline (covariates in the adjusted model).
In the present study, there was an inverse association between smoking during pregnancy and adherence to the adapted WISH at the age of 7, although this result was not statistically significant. According to the literature, smoking during pregnancy has been associated with childhood obesity(Reference Suzuki, Ando and Sato38) which, in turn, is known to be closely linked to inadequate eating habits(Reference Liberali, Kupek and Assis41). Despite this, this effect appears to be greater in children up to 5 years old(Reference Suzuki, Sato and Ando42). Considering pregnancy-related events, children born from mothers with gestational diabetes mellitus are at a high risk of developing various health problems, including obesity(Reference Dugas, Perron and Kearney43). In this study, no significant association was found between maternal smoking during pregnancy and the dietary patterns of children at 7 years of age. Further studies are necessary to elucidate these associations.
Maternal diet quality after pregnancy can have a significant impact on the dietary pattern of the child as they grow. Mothers who maintain a healthy and balanced diet and good eating behaviours are more likely to have children who adopt similar dietary patterns(Reference Juton, Lerin and Homs44). Indeed, in this study, the maternal diet quality at the child’s 4 years of age was identified as one of the key factors influencing a greater adherence to the WISH at the age of 7. Despite not assessing children or mothers’ dietary patterns, a previous studies has showed similar associations considering only some food groups(Reference Johnson45).
It is important to highlight that not only the maternal diet during pregnancy plays a pivotal role in the optimal growth and development of the child(Reference Biagi, Nunzio and Bordoni12). This importance persists over time. The preschool period is a period of heightened vulnerability and dependence for parents, particularly mothers, who serve as important role models(Reference Savage, Fisher and Birch10). During this period of vulnerability and importance, children not only learn social and behavioural cues from their parents, particularly their mothers, but they also consolidate their relationship with food(Reference Scaglioni, De Cosmi and Ciappolino16). The dietary choices and eating behaviours observed and adopted by children from their caregivers can have a long-lasting impact on their future eating habits and overall approach to nutrition(Reference Scaglioni, De Cosmi and Ciappolino16). Consequently, it is recommended that intervention strategies be implemented to improve the dietary habits of mothers, with the objective of promoting better dietary habits over time.
It is well established that parental child feeding practices are closely related to eating habits in childhood(Reference Yee, Lwin and Ho13). The present study observed that children whose mothers employed more restrictive feeding practices at 4 years of age exhibited a higher score on the adapted WISH at 7 years of age. In a previous study conducted in Generation XXI, it was observed that restricting the child’s access to unhealthy foods, using covert control, a kind of control not perceived by the child, and expressing concerns about the child’s weight at the age of 4 were inversely associated with the ”energy-dense foods’ dietary pattern (a dietary pattern with foods typically characterised by a high environmental footprint) after 3 years old(Reference Barbosa, Lopes and Costa46). These findings are consistent with those of a Dutch birth cohort study that observed that following a restrictive feeding practice was associated with a lower consume of sweets, cookies and chocolates, and a higher intake of fruits and vegetables(Reference Gubbels, Kremers and Stafleu47). This dietary pattern aligns with a more environmentally sustainable pattern. In light of the potential for a sex interaction in the associations under study, previous research has documented that parents tend to employ more restrictive practices with females than with males(Reference Gubbels, Kremers and Stafleu48). In this study, when this analysis was stratified by sex, this association remained as statistically significant only among females, suggesting a sex modification effect on this association in particular, as previously reported in the literature.
Nevertheless, research on the relationship between parental restriction and children’s diet has yielded conflicting results, suggesting a complex nature. When critically analysing this association, it is important to mention that some studies have found an association between restriction and higher childhood BMI(Reference Quah, Ng and Fries49). In other words, it has been proposed that mothers are more likely to adopt these feeding practices in response to their child’s BMI, rather than the other way around(Reference Quah, Ng and Fries49). The practice of restriction may originate from parental concerns about unhealthy weight development in children(Reference Beckers, Karssen and Vink50). However, its potential beneficial effects remain uncertain, and it has been linked to the emergence of disordered eating behaviours in adolescence, particularly among females(Reference Loth, MacLehose and Fulkerson51). Consequently, while these practices may have a positive impact on children’s diets in the short term, they may also have adverse effects in the long term.
When interpreting the results of this study, it should be taken into account several limitations. The exclusion of participants due to missing data could introduce a selection bias. However, we conducted a sensitive analysis comparing participants and non-participants and the Cohen’s effect size values were not particularly high(Reference Husted, Cook and Farewell19). This leads us to conclude that the significance of differences between this sample and the remaining cohort are likely due to the large sample size rather than substantial differences between participants. Indeed, when compared with the national data from the National Institute of Statistics, the mean age of women at the time of birth is close to the average age of mothers in this study (29·2 v. 30·4 years)(52). Conversely, this sample exhibits a slightly higher level of education than the national data for women aged 25–34 years (35·3 % v. 33·1 % with higher education)(53). It should be noted that this sample is not representative of Portuguese children; thus, caution should be taken when extrapolating the results. Also, it is important to note that the cohort was recruited in 2005/2006, and the assessment at 7 years old took place over 10 years ago. Therefore, the socio-economic characteristics of postpartum women in 2024 may differ, and it is also possible that infant feeding practices have changed. As such, the results of this study should be interpreted carefully.
In addition, it is important to acknowledge the limitation of using a short-list FFQ to assess maternal diet, which relies heavily on participants’ memory and trustworthiness, potentially leading to recall bias and inaccurate reporting. FFQ typically offer a limited range of food items, potentially omitting fewer common foods and underestimating true consumption. However, it is important to note that the FFQ used in this study was adapted from a previously validated questionnaire(Reference Lopes, Aro and Azevedo20,Reference Pinto, Severo and Correia54) , and its food groups were combined, with less desegregation than the original FFQ, but covered the same food groups, which makes its usage acceptable. Notably, the CFQ consists of parent-report measures, which could also introduce measurement error owing to social desirability effects and inherent subjectivity(Reference Kimberlin and Winterstein55). However, the questionnaire has shown good psychometric properties in children from this cohort(Reference Real, Oliveira and Severo24).
Finally, despite several variables have been tested in the multivariable analysis, we cannot fail to exclude any residual confounding. For instance, the influence of the school environment on children’s diet was not assessed, and we know that schools play a crucial role in developing healthy eating habits during childhood(Reference Cohen, Hecht and McLoughlin56).
This study is notable for its robust methodology, including a relatively large sample size and comprehensive assessment of potential confounding variables. Furthermore, the study is prospective, which ensures temporal sequence between variables. A significant benefit of this study is the use of a predefined theoretical framework for analysis and the assessment of children’s diets through a reference method, such as the 3-day food records. This approach has been described as one of the most accurate methods for estimating food consumption in children(Reference Burrows, Martin and Collins57). Moreover, to the best of our knowledge, this study is the first to assess maternal and other family determinants influencing a healthy and environmentally sustainable dietary pattern in childhood, specifically aligned with the EAT-Lancet reference diet on healthy diets from sustainable food systems. Given the growing importance of sustainability in shaping food policies(Reference Joseph and Clancy6), this study contributes valuable insights for policymakers and researchers seeking to promote sustainable and healthy dietary habits among children. However, further research with larger and more diverse samples is necessary to confirm and extend our findings.
In conclusion, this study suggests that a higher maternal education (at the child’s birth) and the maternal diet quality (at the child’s 4 years of age) were the key factors associated with increased adherence to the EAT-Lancet dietary recommendations on healthy diets from sustainable food systems at the age of 7. Given the longitudinal nature of these data, it would be interesting in future studies to analyse the main determinants of children’s diets as they grow, as it is expected that the contextual determinants will change throughout the life course.
Our results seem to emphasise the importance of promoting better maternal dietary habits, particularly among less educated mothers, to foster healthier dietary patterns in school-age children.
Acknowledgement
The authors gratefully acknowledge the families enrolled in Generation XXI for their kindness, the participating hospitals and their staff for their help and support, and all previous and current members of the research and field team for their enthusiasm and perseverance.
Generation XXI was funded by Programa Operacional de Saúde–Saúde XXI, Quadro Comunitário de Apoio III and Administraçao Regional de Saúde Norte (Regional Department of Ministry of Health). It has support from the Portuguese Foundation for Science and Technology (FCT) through the projects with references UIDB/04750/2020 and LA/P/0064/2020 and DOI identifiers ·https://doi.org/10·54499/UIDB/04750/2020 and ·https://doi.org/10·54499/LA/P/0064/2020. The first author (BT) had a PhD grant 2021.05133.BD (··https://doi.org/10·54499/2021·05133.BD), funded by the Foundation for Science and Technology (FCT) and FSE (Fundo Social Europeu) Program. The authors also acknowledge the SYSTEMIC project (n°696295), a knowledge hub on Nutrition and Food Security, in collaboration with JPI-HDHL (Healthy Diet for a Healthy Life), FACCE-JPI (Joint Programming Initiative for Agriculture, Climate Change and Food Security) and JPI-OCEANS (Joint Programming Initiative Healthy and Productive Seas and Oceans).
B. T.: Conceptualisation, formal analysis, investigation, methodology and writing – original draft; C. A.: investigation, methodology, supervision, validation, visualisation and writing – review and editing; A. O.: Conceptualisation, formal analysis, investigation, methodology, project administration, supervision, validation, visualisation and writing – review and editing. All authors read and approved the final version of the manuscript.
The authors declare none conflitct of interests.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114525000157