


Early adversity has been associated with negative health outcomes in the young population. Reference Felitti, Anda, Nordenberg, Williamson, Spitz and Edwards1 Among the most potentially pernicious environments in which children and adolescents could grow up, household dysfunction has been described as the most prevalent condition worldwide, with an estimated prevalence of 61.6% in the adolescent population. Reference Broekhof, Nordahl, Bjørnelv and Selvik2 Household dysfunction is a complex construct that refers to exposure to different familial stressors that can include both acute and chronic harmful experiences. These may take the form of the abuse of substances, violent or criminal behaviours, and the presence of severe physical or mental disorders among relatives. In this regard, a study focused on household dysfunction conducted by Broekhof et al Reference Broekhof, Nordahl, Bjørnelv and Selvik2 found that 22.1% of the sample reported witnessing violence, 18.8% reported parental mental health problems and 7.5% reported parental substance misuse.
Diagnosing children with symptoms related to relational trauma can be particularly challenging, as these children often present with a broad spectrum of symptoms. Research has shown that they may receive multiple diagnoses throughout their lives, including behavioural disorders, personality disorders and anxiety−depressive disorders, with corresponding changes in pharmacological treatments during childhood. Reference Marques-Feixa, Palma-Gudiel, Romero, Moya-Higueras, Rapado-Castro and Castro-Quintas3 However, the impact of household dysfunction on these severe clinical outcomes, previously linked to relational trauma, remains underexplored. Although the literature is scarce, early exposure to household dysfunction has also been associated with a higher risk of developing emotional and behavioural problems Reference Bussemakers, Kraaykamp, Schoon and Tolsma4 and a dose–response relationship with internalising and externalising symptoms. Reference Holmes, Darmanthe, Tee and Goodchild5 In fact, household dysfunction seems to be a transdiagnostic risk factor for different mental disorders. According to Kessler et al, Reference Kessler, McLaughlin, Green, Gruber, Sampson and Zaslavsky6 clusters of adversities associated with maladaptive family functioning are linked to the highest risk of any mental disorder. This increased risk for psychopathology has also been identified in children living with relatives with substance use disorders, who have a greater tendency to develop other mental disorders. Reference Lander, Howsare and Byrne7
Exposure to early household dysfunction is believed to disrupt children’s well-being and future health through different pathways, including stress-induced brain changes and less favourable environments for optimal development. Reference Shonkoff, Garner, Siegel, Dobbins, Earls and Garner8 Additionally, household dysfunction may affect and modulate the attachment style and behaviour of children and adolescents, conferring a greater risk of being involved in self-harming actions, such as the use of substances. Reference Craig, Wolff, Pierce, Zettler and Baglivio9 Noticeably, the mentioned loop of risk factors may be at the root of future psychopathology. From an emotion regulation perspective, successful adaptation relies on adaptive strategies like cognitive reappraisal, Reference Gross10 and meta-analytic evidence positions emotional intelligence as the core set of dispositional skills that facilitate these regulatory processes. Reference Salovey and Mayer11 Within resilience frameworks, internal resources like emotional intelligence may counteract the effects of risk. A compelling theoretical rationale exists for examining emotional intelligence as a mediator of household dysfunction’s effects. Chronic stress and disrupted caregiving within dysfunctional households are hypothesised to impede the development of these core emotional skills. Reference Barragán Martín, del Molero Jurado, del Pérez-Fuentes, Oropesa Ruiz, Martos Martínez and del Són Márquez12 In turn, deficits in emotional intelligence may limit adaptive coping and increase vulnerability to emotional distress, thereby elevating the risk for maladaptive outcomes such as substance use and psychopathology. Reference Davis and Humphrey13
In this regard, youths who have had adverse childhood experiences (ACEs) are at a higher risk of early substance use and more severe consumption patterns. Reference Leza, Siria, López-Goñi and Fernández-Montalvo14 In fact, Kessler et al Reference Kessler, McLaughlin, Green, Gruber, Sampson and Zaslavsky6 concluded that 51–65% of childhood-onset substance use disorders could be attributed to psychosocial early-life adversities. Specifically, experiences of interpersonal trauma appear to be particularly influential in this risk. Reference Aas, Sideli, Franceschini, Alameda, Trotta and Coco15 Moreover, early substance use has been established as a reliable predictor of a faster transition to both substance use disorders Reference Degenhardt, Stockings, Patton, Hall and Lynskey16 and other psychiatric disorders. Reference Brownlie, Beitchman, Chaim, Wolfe, Rush and Henderson17
Although the relationship between household dysfunction and the above-mentioned mental health outcomes has been well documented, less is known about the factors that may tip the scale toward resilience or disease. In that sense, there are some environmental conditions that have been proposed as putative mediators of this association, including familial, community, school social support Reference McCoy, Tibbs, DeKraai and Hansen18 and lifetime stressful life events. Reference White and Widom19
In this regard, one of the most important factors believed to confer resilience to ACE is emotional intelligence, defined as the ability to perceive, understand, use and manage emotions. For this reason, individuals with high levels of emotional intelligence may manage their lives more effectively and adapt better to their environment. Emotional intelligence is intrinsically linked to better emotional management, reactivity and regulation, thus being a protective factor for the development of mental health conditions in individuals exposed to stressful situations. Reference Davis and Humphrey13 Furthermore, emotional intelligence could act as a mediator between adversity and the emergence of substance use disorders. Reference Edalati and Krank20
The research in this area has traditionally focused on exploring the role of emotional intelligence in children directly exposed to maltreatment or abuse. Reference Peng, Zhang, Wang, Lee, Wang and Wang21 In contrast, experiences of household dysfunction have been relatively unexplored. Despite previous studies highlighting that the family environment is essential for children’s emotional regulation development, to the best of our knowledge, this is the first study to specifically evaluate the potential role of emotional intelligence in the association between household dysfunction and these mental health outcomes in children and adolescents. Consequently, the present study aims to explore whether childrens’ and adolescents’ emotional intelligence could mediate the consequences of household dysfunction in two essential dimensions of their health status and well-being: substance use and psychopathological outcomes.
Method
Participants
A total of 187 children and adolescents aged 7–17 years, from our multicentre study EPI-Young-Stress Project, were included in the present study. Of these participants, 116 had been diagnosed with a current psychiatric disorder, and 71 were healthy controls. Those with current psychopathology were recruited from six child and adolescent psychiatry units of Spanish hospitals (in-patient clinics, partial hospital admission programmes and out-patient clinics). Children without psychopathology were recruited from advertisements, primary healthcare centres, schools and other community facilities in the same geographical areas. The case and control groups were comparable in terms of age and gender distribution, and were recruited from similar geographical areas and educational stages.
Experienced psychologists and psychiatrists conducted face-to-face interviews to collect information regarding socioeconomic status, maltreatment history, medical/psychiatric history and substance use. These interviews were conducted separately with minors and with their parents or legal guardians. Other sources, such as school or social service reports, were used when needed. Additional information regarding the sample has been reported elsewhere. Reference Marques-Feixa, Palma-Gudiel, Romero, Moya-Higueras, Rapado-Castro and Castro-Quintas3
Measures
Household dysfunction
A maltreatment history was thoroughly gathered through a semi-structured interview, validated by professionals from the Spanish Social Services, and made available online. 22 This instrument differentiates among all five types of direct maltreatment: physical abuse, emotional abuse, sexual abuse, physical neglect and emotional neglect. Additionally, the Tool for Assessing the Severity of Situations in which Children are Vulnerable (TASSCV) includes the assessment of other types of maltreatment, such as prenatal maltreatment of the mother, abandonment of the child and household dysfunction. Following the TASSCV criteria, each child maltreatment type was coded as either (a) absent, (b) suspected (if significant signs of neglect or abuse emerged during the evaluation) or (c) confirmed (with clear evidence from social services or family). Suspected and confirmed cases were categorised into the maltreatment group. The severity index was computed by multiplying its severity and frequency scores of the different types of direct maltreatment, which were rated on a four-point Likert scale according to TASSCV criteria. Maltreatment severity was coded according to the characteristics of the experience suffered, as low (1), moderate (2), severe (3) or very severe (4); frequency was coded according to whether child maltreatment had occurred once (1), sometimes (2), often (3) or frequently (4).
Briefly, the concept of household dysfunction refers to circumstances where the domestic environment is deemed to be inappropriate and incompatible with the optimal development of the individual, exhibiting antisocial or deviant patterns. The presence of household dysfunction was defined as the existence of at least one of the following familial conditions: (a) maladaptive behaviour such as aggression or discrimination (including gender-based or intra-family violence); (b) criminal behaviour (theft, drug trafficking or other crimes that cause harm to others); (c) allowing or encouraging the minor’s misuse of drugs; (d) engaging in prostitution in a home in which the minor is present, or proposing prostitution to the minor; and (e) engaging in episodes of drug misuse that are often perceived by the minor.
Emotional intelligence
Emotional intelligence was measured using the parent- or guardian-administered Trait Emotional Intelligence Questionnaire for Children Short Form (TEIQue-CSF). This test provides comprehensive coverage of emotion-related facets of children’s personality, including adaptability, addictive tendencies, emotion expression, emotion perception, emotion regulation, low impulsivity, peer relations, self-esteem and self-motivation. The questionnaire comprises 36 short statements on a five-point Likert scale (ranging from 1 = completely disagree, to 5 = agree completely), yielding scores ranging from 36 to 180. The scale has demonstrated good internal consistency in previous research (e.g. Cronbach’s α = 0.88). Reference Petrides and Furnham40
Substance use
The consumption of tobacco, alcohol, cannabis, cocaine, ecstasy and other substances was evaluated in face-to-face interviews, following the Spanish version of the Schedule for Affective Disorders and Schizophrenia for School-Age Children: Present and Lifetime Version DSM-5 (K-SADS-PL-5). Age of substance use initiation was a study variable of interest regardless of the type of drug used. Additionally, an index of severity of substance use was created by multiplying the number of substances used more than once by the frequency of use (once or more per year (1), one or more per month (2), once per week (3), two to three times per week (4), four to six times per week (5) and daily (6)). The result is a continuous variable (between 0 and 30) that measures substance use, considering both the number of different types and frequency of use.
Psychopathological outcomes
Emotional and behavioural problems
The Achenback’s Child Behavior Checklist (CBCL) was used to evaluate emotional and behavioural problems in the entire sample. The CBCL has well-established psychometric properties, including high internal consistency for its broad band scales. Reference Achenbach and Rescorla23 This parent-report inventory assesses internalising symptoms (anxious/depressed, withdrawn and somatic complaints), externalising symptoms (rule-breaking behaviour and aggressive behaviour) and other symptoms (social problems, thought problems and attention problems), in children aged 6–18 years. For the purpose of this study, a ‘total problems’ score was employed for the whole sample (CBCL-TP), to summarise the aforementioned domains on a continuum spectrum.
Number of lifetime psychiatric diagnoses and subtypes of prescribed drugs
Psychopathology was ascertained for the entire sample, using the K-SADS-PL-5. Reference Kaufman, Birmaher, Brent, Rao, Flynn and Moreci24 This is a semi-structured diagnostic interview with demonstrated good to excellent reliability and validity for assessing DSM-5 disorders in children and adolescents. Clinicians reported psychiatric diagnoses for each participant, both currently and throughout the participant’s life, following DSM-5 criteria. All major diagnostic categories were covered and were categorised into the following groups: attention-deficit/hyperactivity disorder, affective disorders, trauma and stress-related disorders, anxiety disorders, behavioural disorders, psychotic disorders and eating disorders. The number of lifetime psychiatric diagnoses was considered as a main variable for the present study. To better characterise the sample, a classification of the current main diagnosis is reported in Table 1.
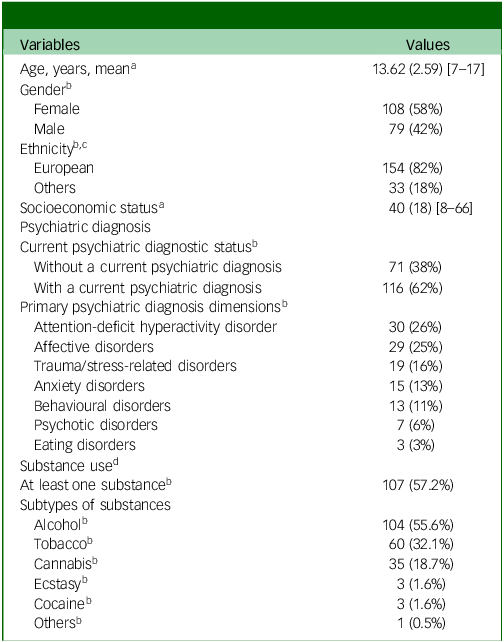
Descriptive data of our sample (N = 187)

Table 1 Long description
The table presents descriptive data for a sample of 187 individuals. It includes variables such as age, gender, ethnicity, socioeconomic status and psychiatric diagnoses. The mean age is 13.62 years with a standard deviation of 2.59, ranging from 7 to 17 years. Gender distribution shows 108 females (58 percent) and 79 males (42 percent). Ethnicity is divided into European (154 individuals, 82 percent) and others (33 individuals, 18 percent). Socioeconomic status has a mean value of 40 with a standard deviation of 18, ranging from 8 to 66. Psychiatric diagnostic status indicates 71 individuals (38 percent) without a current psychiatric diagnosis and 116 individuals (62 percent) with a current psychiatric diagnosis. Primary psychiatric diagnosis dimensions include attention-deficit hyperactivity disorder (30 individuals, 26 percent), affective disorders (29 individuals, 25 percent), trauma and stress-related disorders (19 individuals, 16 percent), anxiety disorders (15 individuals, 13 percent), behavioral disorders (13 individuals, 11 percent), psychotic disorders (7 individuals, 6 percent), and eating disorders (3 individuals, 3 percent). Substance use is reported by 107 individuals (57.2 percent), with subtypes including alcohol (104 individuals, 55.6 percent), tobacco (60 individuals, 32.1 percent), cannabis (35 individuals, 18.7 percent), ecstasy (3 individuals, 1.6 percent), cocaine (3 individuals, 1.6 percent) and others (1 individual, 0.5 percent).
ADHD, attention-deficit hyperactivity disorder.
a. Values are reported as mean (s.d.) [range].
b. Refers to any use of any of the listed substances. Values are reported as n (%).
c. Other ethnicities were Latin American (66%), Maghrebin (16%), sub-Saharan (9%) and others (9%).
d. Data available for n = 177.
Furthermore, the pharmacological treatments currently prescribed were categorised into six types (hypnotics/anxiolytics, antidepressants, antipsychotics, mood stabilisers, anticholinergics, psychostimulants and others). The number of prescribed drugs was calculated as the sum of the different types of drugs prescribed daily.
Global functioning
The Children’s Global Assessment Scale (CGAS) was used to evaluate the overall functioning and impairment, serving as a complementary instrument to syndrome-specific scales. Reference Shaffer, Gould, Brasic, Ambrosini, Fisher and Bird25 The assessment encompasses multiple domains of functioning, including academic performance, social relationships, self-care skills and overall psychological well-being. Specifically, the CGAS was utilised to evaluate children’s lifetime worst global functioning. Scores ranged from 1 to 100, with lower scores indicating a more severe impairment and higher scores indicating better functioning.
Statistical analysis
Descriptive analyses were performed using IBM SPSS Statistics version 23 for Windows (IBM Corp., Armonk, NY, USA; https://www.ibm.com/products/spss-statistics), and mediation analyses were performed with PROCESS macro version 4.2 for SPSS (Andrew F. Hayes, The Ohio State University, Columbus, OH, USA; https://www.afhayes.com/spss-sas-and-mplus-macros-and-code.html). In alignment with the objectives of this study, a simple mediation model was employed. Reference Zhao, Lynch and Chen26,Reference Hayes27 Only variables exhibiting a substantial correlation with each other were incorporated into the model.
Household dysfunction was used as the explanatory or independent variable (X), and emotional intelligence was the mediating variable (M). Six dependent variables (Y) were successively tested in our approach: (a) age of substance use initiation, (b) substance use severity index, (c) emotional and behavioural problems (CBCL-TP), (d) number of lifetime psychiatric diagnoses, (e) number of different prescribed drugs and (f) global functioning (CGAS score). For a better understanding of the results, the mentioned dependent variables were grouped in two domains: substance use and psychopathological outcomes. For the dichotomous predictor household dysfunction, the partially standardised coefficients reported represent the change in the outcome variable, expressed in standard deviation units, associated with the presence (coded as 1) versus the absence (coded as 0) of household dysfunction.
This statistical approach enables us to study whether the mediation effect of emotional intelligence is indirect-only or complementary. Indirect-only mediation indicates that the direct effect of X on Y becomes insignificant when M is introduced into the model. Conversely, a complementary mediation effect indicates the presence of both direct and indirect effects from X to Y, and so when M is incorporated into the model, statistical significance is maintained, although it can be reduced.
To account for multiple comparisons, the Bonferroni correction was applied across the six mediation models, adjusting the significance threshold to p < 0.0083. Accordingly, the statistical significance of the indirect effects was tested using a bootstrapping procedure with 10 000 samples and a bias-corrected 99% confidence interval. The indirect effect was accepted as statistically significant only if its bias-corrected 99% confidence interval excluded zero. Reference Hayes27 Standardised coefficients for dichotomous X, coded by a unit difference, were in a partially standardised form. For dichotomous variables, the interpretation of the partially standardised coefficient centres around the change in the outcome variable (M or Y), expressed in standard deviations, associated with a one-unit change in the predictor (X).
The Cribari–Neto heteroscedasticity-consistent standard error and covariance matrix estimator was employed. For each mediation analysis, the proportion mediated was estimated. This measure estimates the extent to which the pathway accounts for the total effect through the mediating variable.
Ethics approval and consent to participate
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013.
The study received approval from the Ethical Review Board of the participating hospitals, as well as the Bioethics Commission of the University of Barcelona, serving as the coordinating centre (Institutional Review Board approval number: IRB00003099). Families were explicitly informed about the voluntary nature of the study, their rights and the procedures, risks and potential benefits associated with it. Written consent was required from all parents or legal guardians, and the children themselves provided written assent after the nature of the procedure had been fully explained.
Results
Variables and sample description
The total sample comprised 187 minors, the majority of whom (82%) were of European origin. There was a slightly greater number of girls (58%). A total of 38% of the sample had no psychiatric diagnosis, whereas 62% had at least one. The most prevalent primary diagnoses were affective disorders and attention-deficit hyperactivity disorder. Further, 44.3% of the sample demonstrated contact with at least one substance. Alcohol was the most commonly used substance, observed in 55.6% of individuals with a history of substance use. See Table 1 for additional information.
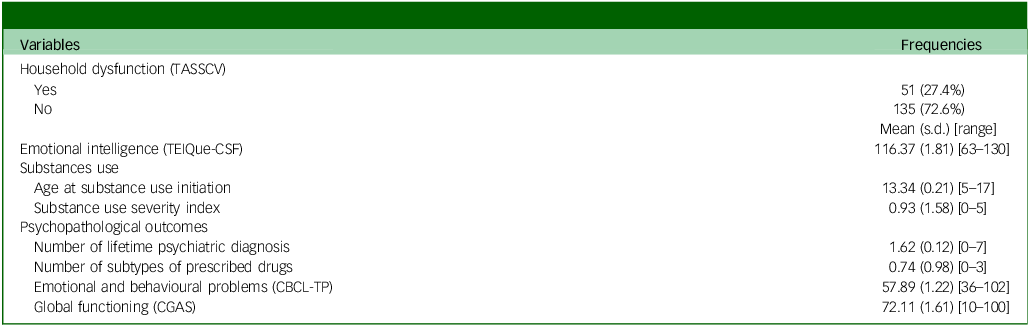
A description of the variables included in the mediation analyses is provided in Table 2. According to the TASSCV scale, 27.4% had household dysfunction. See Table 2 for the descriptive statistics of our sample regarding emotional intelligence and the outcomes of interest: (a) age at substance use initiation, (b) substance use severity index, (c) emotional and behavioural problems (CBCL-TP), (d) number of lifetime psychiatric diagnoses, (e) number of different prescribed drugs and (f) global functioning (CGAS).
Frequencies and means of the clinical or dependent variables in the studied sample of the present study

Table 2 Long description
The table presents data on various clinical variables in a studied sample. It includes two columns: Variables and Frequencies. The Variables column lists categories such as household dysfunction, emotional intelligence, substances use and psychopathological outcomes. The Frequencies column provides corresponding data, including percentages, means, standard deviations, and ranges. Household dysfunction is reported in 27.4% of cases. Emotional intelligence has a mean score of 116.37 with a standard deviation of 18.1 and a range from 63 to 130. Substances use details include age at initiation, substance use severity index and various psychopathological outcomes such as the number of lifetime psychiatric diagnoses, number of prescribed drugs, emotional and behavioral problems, and global functioning scores.
TASSCV, Tool for Assessing the Severity of Situations in which Children are Vulnerable; TEIQue-CSF, Trait Emotional Intelligence Questionnaire for Children Short Form; CBCL-TP, Achenback’s Child Behavior Checklist - Total Problems score; CGAS, Children’s Global Assessment Scale.
Mediation analyses results
Household dysfunction was significantly related to all the clinical variables studied. The relationship with substance use was negative with age at onset (Z = −3.267; p < 0.001) and positive with the severity of use (Z = 3.063; p = 0.002). The correlation was also significantly positive with the number of psychiatric disorders (Z = 5.227; p < 0.001), with emotional and behavioural problems (Z = 6.027; p < 0.001) and with the number of prescribed drugs (Z = 4.293; p < 0.001). Conversely, a negative correlation was observed with global functioning (Z = −5.718; p < 0.001). We also examined the possibility of competitive mediation (suppression), which occurs when direct and indirect effects have opposite signs. No evidence of this pattern was found in our models; all significant direct and indirect paths were consistent in direction.
Substance use
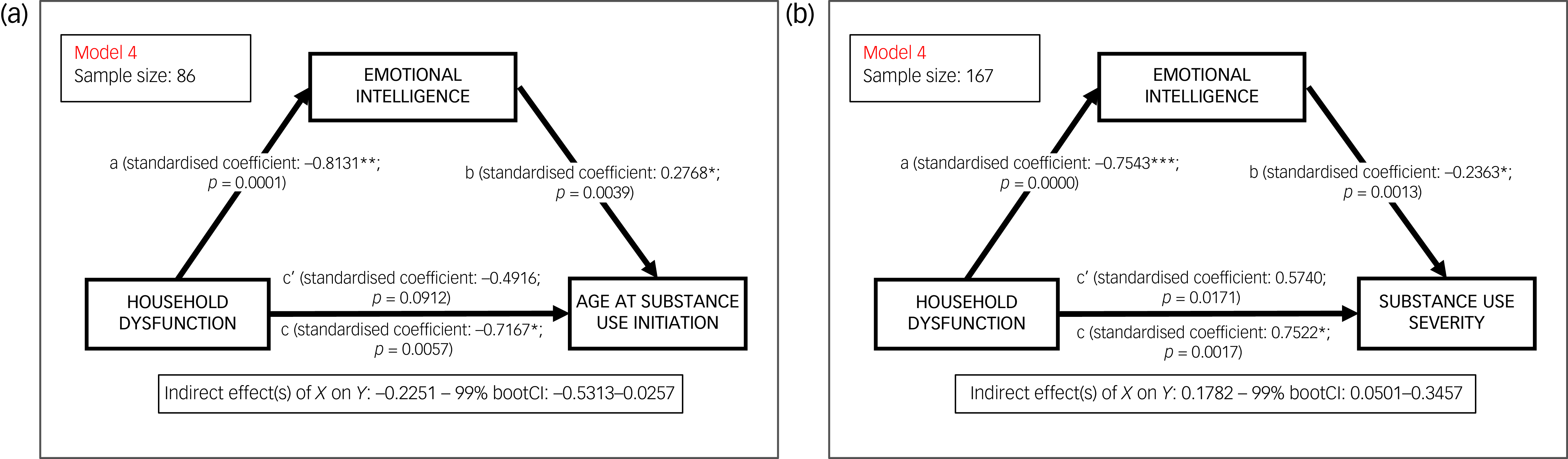
Results of the mediation analyses, including household dysfunction, emotional intelligence and outcomes related to substance use, are depicted in Fig. 1.
Simple mediation model of emotional intelligence in the relationship between household dysfunction and substance use outcomes. (a) Age at substance use onset. (b) Substance use severity index. Standardised path coefficients and significance levels (indicated with asterisks) are shown on each arrow. *p < 0.0083, **p < 0.0001, ***p < 0.00001.

Fig. 1 Long description
A diagram illustrating the relationship between household dysfunction, emotional intelligence, and substance use outcomes. Panel A: A mediation model showing the relationship between household dysfunction and age at substance use onset, mediated by emotional intelligence. The model includes standardized coefficients and significance levels on each arrow. Household dysfunction negatively affects emotional intelligence, which in turn affects the age at substance use onset. Panel B: A mediation model showing the relationship between household dysfunction and substance use severity index, mediated by emotional intelligence. The model includes standardized coefficients and significance levels on each arrow. Household dysfunction negatively affects emotional intelligence, which in turn affects the substance use severity index.
Age at substance use initiation
There is an indirect-only mediation effect of emotional intelligence on the age at onset of substance use, since the effect of household dysfunction on the age at onset of substance use is no longer significant when emotional intelligence is introduced into the model (see Fig. 1(a)). When household dysfunction is present, emotional intelligence decreases. Additionally, as emotional intelligence decreases, the age at substance use initiation is also reduced. Thus, emotional intelligence exerts an opposite-direction effect, suppressing the effect of household dysfunction on substance use onset age. The percentage of the age at onset of substance use that is related to both household dysfunction and emotional intelligence was 17.32% (R 2). The proportion mediated, or the proportion of the total effect explained by the pathway through the mediating variable, was 31.40%.
Substance use severity
There is an indirect-only mediation effect of emotional intelligence between household dysfunction and substance use severity. Thus, the influence of household dysfunction on substance use severity becomes non-significant when emotional intelligence is incorporated into the model, as illustrated in Fig. 1(b). Therefore, emotional intelligence exerts an opposite-direction effect, suppressing the negative effect of household dysfunction. The proportion of the severity of substance use variable that is attributable to the household dysfunction and emotional intelligence combined was 15.54% (R 2), and the proportion mediated was 23.69%.
Psychopathological outcomes
Results of the mediation analyses, including household dysfunction, emotional intelligence and outcomes related to psychopathological outcomes, are depicted in Fig. 2.
Simple mediation model of emotional intelligence in the relationship between household dysfunction and clinical/functional outcomes. (a) Emotional/behavioural problems (Achenback’s Child Behavior Checklist (CBCL) Total Problems score). (b) Number of lifetime psychiatric diagnoses. (c) Number of prescribed psychiatric drugs. (d) Global functioning (Children’s Global Assessment Scale score). Path coefficients and statistical significance are displayed directly in the figure. *p < 0.0083, **p < 0.0001, ***p < 0.00001.

Emotional and behavioural problems (CBCL-TP)
There is a complementary mediation of emotional intelligence between household dysfunction and the CBCL-TP score (see Fig. 2(a)). Thus, the influence of household dysfunction on emotional and behavioural problems remains significant when introducing emotional intelligence into the model, although the effect size reduces. Household dysfunction decreases emotional intelligence, which is associated with increases in the CBCL-TP score. The proportion of the CBCL-TP attributable to the household dysfunction and emotional intelligence combined was 60.54% (R 2), and the proportion mediated was 56.37%.
Number of lifetime psychiatric diagnoses
There is an indirect-only mediation effect of emotional intelligence between household dysfunction and the number of different lifetime psychiatric diagnoses received. Consequently, when emotional intelligence is incorporated into the model, the impact of household dysfunction on the number of lifetime psychiatric diagnoses is suppressed, as seen in Fig. 2(b). Specifically, a negative correlation was observed between emotional intelligence and the number of psychiatric diagnoses. The proportion of the number of psychiatric diagnoses variable attributable to household dysfunction and emotional intelligence combined was 37.12% (R 2), and the proportion mediated was 39.46%.
Number of drugs prescribed (polypharmacy)
There is an indirect-only mediation effect of emotional intelligence between household dysfunction and the number of drugs prescribed to psychiatric patients, since the influence of household dysfunction ceases to be significant when emotional intelligence is added to the model (see Fig. 2(c)). As emotional intelligence decreases, the quantity of prescribed psychiatric drugs increases. The proportion of the number of different types of prescribed drugs that are attributable to household dysfunction and emotional intelligence combined was 30.21% (R 2), and the proportion mediated was 48.75%.
Global functioning (CGAS)
A complementary mediation effect of emotional intelligence was identified between household dysfunction and the lifetime worst CGAS score, since the influence of household dysfunction on CGAS remained significant when emotional intelligence was incorporated into the model, but the effect size was diminished (see Fig. 2(d)). Specifically, our results indicate that, as emotional intelligence decreases, the global functioning of the participants also decreases. The proportion of the global functioning variable attributable to household dysfunction and emotional intelligence combined was 50.16% (R 2), and the proportion mediated was 54.20%.
All indirect effects remained statistically significant even under these stricter criteria, further supporting the robustness of the proposed model.
Discussion
As expected, our findings indicate that children exposed to elevated household dysfunction tend to present with lower levels of emotional intelligence. This underscores the importance of a stable and functional family environment in fostering the emotional competence necessary for healthy development.
Interestingly, in our study, emotional intelligence emerges as a putative protective factor against the negative consequences that household dysfunction has on youths’ risk for substance use, emotional and behavioural problems, and clinical psychiatric conditions. Actually, our results indicate that emotional intelligence has a protective effect against all the explored outcomes.
First, regarding substance use, our findings suggest that children and adolescents exposed to dysfunctional households are at a greater risk of consuming substances at earlier stages and with a higher severity. This is in great accordance with Broekhof et al, Reference Broekhof, Nordahl, Bjørnelv and Selvik2 who report that children exposed to household dysfunction present a higher lifetime risk of substance use. Furthermore, other researchers have described an earlier onset and a higher severity of substance use among people exposed to ACE and recurrent trauma. Reference Aas, Sideli, Franceschini, Alameda, Trotta and Coco15 Unfortunately, these authors do not explore emotional intelligence as a mediator in this association. Our data, however, clearly detected the protective effect of emotional intelligence on the age at initiation of substance use, where we found an indirect-only mediation effect of emotional intelligence and a proportion mediated of 31.40%, showing that emotional intelligence accounts for nearly a third of the effect of household dysfunction on substance use onset. This suggests that children exposed to household dysfunction and low emotional intelligence may be more likely to engage in substance use, possibly as a means of managing or regulating their negative emotions. However, the findings of this study demonstrate that if emotional intelligence is fostered, even in the presence of household dysfunction, the onset of substance use may not be altered, thereby acting as a clear protective factor for substance use onset. According to our results, emotional intelligence also has a protective effect on the severity of substance use. Although the proportion mediated is somewhat smaller (approximately 24%), it remains substantial. It indicates that a considerable part of the more severe and frequent use pattern associated with household dysfunction is explained by lower emotional intelligence. These results are in line with former research indicating that emotional intelligence plays a key role in the development of substance use and behavioural addictions. Reference Henning, Crane, Taylor and Parker31 Since emotional intelligence appears to be related to impulse control and stress management, it is not surprising that it exerts a pivotal influence on early-onset substance use and severity.
Concerning emotional and behavioural outcomes, our study points out that youths exposed to household dysfunction present a higher risk of developing behavioural and emotional problems. According to our findings, the research by Holmes et al Reference Holmes, Darmanthe, Tee and Goodchild5 evidences that household dysfunction experiences mediate over half (56%) of household dysfunction’s effect on both externalising and internalising behaviours, a relationship that has already been well described for other ACEs. Furthermore, two recent studies claimed that household dysfunction predicts higher rates of deviant behaviours such as illicit drug use or stealing. Reference Bussemakers, Kraaykamp, Schoon and Tolsma4 In this regard, a recent study highlights that the co-occurrence of ACE predicts a higher risk of maladaptive behaviours, including the commitment of felonies and a higher risk of juvenile arrest. Reference Giovanelli, Mondi, Reynolds and Ou32 However, the authors did not discriminate between abuse and household dysfunction. Interestingly, household dysfunction is believed to affect youths’ future global functioning by means of the mentioned behavioural deviations, which have been, in turn, associated with reduced childhood well-being, poorer academic performance and later mental health outcomes. Reference Higgins and McCabe35
Regarding the role of emotional intelligence, our findings suggest that emotional intelligence acts as a protective factor against the aforementioned behavioural and emotional deviations. This protective relationship has been previously highlighted in the literature, with higher levels of emotional intelligence reducing adolescents’ involvement in risky behaviours. Additionally, different dimensions of emotional intelligence have been negatively associated with internalising and externalising behaviours, with self-control being a predictor of lower externalising problems and well-being a predictor of lower internalising problems. Reference Marques-Feixa, Palma-Gudiel, Romero, Moya-Higueras, Rapado-Castro and Castro-Quintas3
Second, regarding mental health outcomes, our study demonstrates the existence of an indirect-only mediation effect between household dysfunction and the number of lifetime psychiatric diagnoses received and global functioning, with a proportion mediated of nearly 40%. In this regard, the relationship between ACEs and adverse mental health outcomes has been extensively reported in the literature, both for direct forms of maltreatment Reference Marques-Feixa, Palma-Gudiel, Romero, Moya-Higueras, Rapado-Castro and Castro-Quintas3 and household dysfunction. Reference Negriff33 Furthermore, our findings suggest an indirect-only mediation effect between household dysfunction and the number of pharmacological treatments prescribed, showing that nearly half of household dysfunction’s effect on polypharmacy could operate through emotional intelligence. Actually, ACEs have been clearly associated with both a higher risk of mental disorders and a worse clinical prognosis. Reference Lippard and Nemeroff34 However, the evidence of a worse prognosis among individuals solely exposed to household dysfunction is scarce, although a previous study identified a poorer adjustment among individuals living in suboptimal familial environments. Reference Higgins and McCabe35
The R 2 values indicate that the combined effect of household dysfunction and emotional intelligence explains a meaningful share of the variability in key outcomes – from about a sixth of the severity in substance use to nearly two-thirds of the variance in broad emotional/behavioural problems. This reinforces that, although other factors are involved, targeting the familial environment and emotional skills (as captured by our model) could address a core component of risk for these conditions in youth.
Finally, the fact that emotional intelligence acts as a mediator of the number of psychiatric diagnoses and the clinical prognosis is not surprising, considering previous evidence supporting emotional intelligence as a protective factor for mental health problems in adolescents. Reference Davis and Humphrey13 Indeed, classical studies determined that emotional intelligence moderates the relationship between stress and mental health, since individuals with higher levels of emotional intelligence can mitigate the harmful effects of adverse situations and diminish the levels of perceived emotional distress. Reference Gohm, Corser and Dalsky36 Moreover, according to our findings, emotional intelligence enhances psychological adjustment in adolescents. In this regard, emotional intelligence is believed to contribute to personal resilience after stress, since it is related to a more optimal emotional reactivity and less emotional dysregulation, two factors that have been observed to be underlying transdiagnostic mental disorders. Reference Reyes-Wapano37 In fact, emotional intelligence is associated with better use, understanding and management of emotions, which leads to healthy choices for personal growth and well-being. Indeed, the indirect-only mediating effect found between household dysfunction and pharmacological treatments suggests that increasing emotional intelligence in children exposed to household dysfunction could help reduce the psychiatric polypharmacy associated with them.
Limitations
The present study has some limitations. First, it is highly probable that household dysfunction coexists with other subtypes of childhood maltreatment. Moreover, employing a dichotomous variable of household dysfunction does not allow us to explore the potential effects of the severity and accumulation of different experiences, included in this construct. In fact, this study defined household dysfunction as the presence of severe familial conditions, including episodes of substance use, maladaptive and violent behaviours, or prostitution witnessed by minors. It should be noted that the definition of household dysfunction varies across studies, with other authors including additional experiences such as parental divorce.
Additionally, the sample size of 187 youth is modest for a multiple mediation model that includes six dependent variables and various covariates. Nevertheless, the results remained significant even after applying the Bonferroni correction.
Concerning the possibility of reverse causation, such as psychiatric symptoms affecting emotional intelligence, this cannot be completely dismissed in a cross-sectional design. Nevertheless, the directionality outlined in the model – from household dysfunction to emotional intelligence and, subsequently, to various outcomes – is rooted in well-established theoretical frameworks and bolstered by other longitudinal studies. Reference Danese and Widom28–Reference Nweze, Ezenwa, Ajaelu and Okoye30 Therefore, the current findings align with a theoretically and clinically valid pathway, offering preliminary evidence that justifies further exploration in prospective longitudinal studies.
The generalisability of our findings may be limited by the specific cultural and healthcare context of Spain and the predominantly European origin (82%) of our sample. Future studies in more diverse cultural and ethnic populations are needed.
In conclusion, household dysfunction is a form of early-life stress that increases the risk of youths’ mental health conditions, including the onset and severity of substance use, emotional and behavioural problems, and clinical psychiatric outcomes such as comorbidity and polypharmacy. In our study, emotional intelligence appears to be a protective factor against the negative consequences of household dysfunction. The findings of this study suggest several potential implications for practice and policy, which warrant consideration for future research and implementation efforts. First, regarding prevention, our results underscore the potential value of enhancing early identification of household dysfunction in settings frequented by children, such as primary care and schools. Incorporating brief, non-stigmatising screenings for familial adversity into routine assessments could facilitate earlier connection to support services, potentially mitigating risk before more severe outcomes emerge. Second, concerning intervention, the consistent mediating role of emotional intelligence suggests that interventions designed to bolster these skills may be particularly beneficial for youth exposed to household dysfunction. Existing evidence-based programmes, such as the school-wide Social and Emotional Learning (SEL) curricula (e.g. the RULER programme (recognizing, understanding, labeling, expressing, regulating) developed by the Yale Center for Emotional Intelligence Reference Brackett, Rivers, Reyes and Salovey38 ), provide a viable model for universal promotion of emotional competencies. For youth showing early signs of difficulty, integrating emotional intelligence-focused modules into therapeutic approaches could directly target the psychological mechanism identified here. Third, at the policy level, public health and educational strategies could benefit from a greater integration of emotional skills promotion. This includes supporting the implementation of SEL programmes and training for child-facing professionals to recognise adversity and its emotional correlates. Reference Durlak, Weissberg, Dymnicki, Taylor and Schellinger39 Positioning emotional competence as a developmental asset within health and education policy frameworks represents a promising, proactive approach to building resilience.
Data availability
The data that support the findings of this study are available from the corresponding author, A.G.-P., upon reasonable request.
Acknowledgements
The authors thank the EPI-Young-Stress GROUP for their collaborative work in participant recruitment, data collection and clinical assessments: María Martín, Eulalia Anglada, Pilar Santamarina-Pérez, María José Lobato María Mayoral, Iría Méndez.
Author contributions
M.R., N.S.M., L.M.-F., A.G.-P., I.Z. and L.F. conceptualised the study. M.R., L.M.-F., S.R., J.L.M.-G., A.M., M.R.-C., M.M.-V., H.B.-F., M.J.M. and I.Z. conducted data collection. M.R. performed the statistical analyses. N.S.M., L.M.-F., A.G.-P., L.F. and I.Z. collaborated on interpretations. M.R., L.M.-F., A.G.-P. and L.F. prepared tables and wrote the initial draft of the manuscript. All authors contributed to the review and approval of the final manuscript.
Funding
The study was supported by the Spanish Ministry of Economy and Competitiveness; the Network Center for Biomedical Research in Mental Health (CIBERSAM; Instituto de Salud Carlos III) and the Comissionat per a Universitats i Recerca del DIUE, of the Generalitat de Catalunya regional authorities (grants 2017SGR1577 and 2021SGR00706). We received two grants from ‘Fondo de Investigaciones Sanitarias – FIS’ (grants PI15/00097 and PI22/01245) from the Spanish Ministry of Health for the funding of this multicentric project co-founded by the ‘Fondo Europeo de Desarrollo Regional (FEDER) – Una manera de hacer Europa’. This study was facilitated by a pre-doctoral research grant from the Spanish Ministry of Universities to N.S.M.-G. (grant FPU21/03927).
Declaration of interest
None.


 Open access
Open access
eLetters
No eLetters have been published for this article.