




Introduction
Previous research has suggested that the Iron Age (broadly covering 800 BC to AD 43) to Roman (AD 43 to 410) transition in England was a time of major social and environmental upheaval, which proved detrimental to the health of individuals by increasing pathogen exposure and restricting resources (Redfern & DeWitte Reference Redfern and DeWitte2011; Rohnbogner Reference Rohnbogner2022). Bioarchaeological comparisons of the Roman occupation with the preceding Iron Age and succeeding early medieval period (AD 410 to 1066) suggest that the environment of Roman England was less conducive to health (Rohnbogner Reference Rohnbogner and Smith2018). However, the Iron Age is notoriously understudied, with a limited number of inhumations available for analysis in contrast with large Romano-British cemeteries (Harding Reference Harding2016; Roth Reference Roth2016), which may explain why these earlier communities appear ‘healthier’. Further research is required to contextualise discoveries using pioneering palaeopathological techniques, such as advances in the diagnosis of metabolic conditions (Brickley et al. Reference Brickley, Ives and Mays2020) and childhood tuberculosis (Lewis Reference Lewis2011) and in the ability to differentiate between physiological and pathological subperiosteal new bone formation (Eggington et al. Reference Eggington, Pitt and Hodson2024), to further understand the impact Roman occupation had on communities.
The Iron Age to Roman transition in England
The Iron Age in England marks a period where changing social organisation, land management, production and technological advancements shaped the lives of the wider population, but social traditions fluctuated regionally (Moore Reference Moore2011; Roth Reference Roth2016). Bioarchaeological research is hindered by limited surviving skeletal remains; disarticulated burials and lone inhumations are often dismissed as unrepresentative of common funerary rites, while formal burial grounds have only been identified in specific Late Iron Age regions (Harding Reference Harding2016), obscuring the complexity of burial conventions and complicating health interpretations. The total number of surviving skeletal remains is unlikely to be representative of the general population, with individuals lost through archaeologically invisible funerary rites, taphonomic processes and excavation bias (Roth Reference Roth2016).
Though continental influence was present long before the Roman occupation of Britain in AD 43, prompting the cross-exchange of people, ideas and materials (Haselgrove & Moore Reference Haselgrove, Moore, Haselgrove and Moore2007), it was not until after the Roman administration was implemented that this influence impacted most of the population (Mattingly Reference Mattingly2006). A marked gap between the upper and lower classes became apparent (Esmonde Cleary Reference Esmonde Cleary, Hinton, Crawford and Hamerow2011), a phenomenon that may exaggerate Roman influence due to the archaeological signatures left by those seeking power and status (Gerrard Reference Gerrard2013). Consequently, Romano-British research has focused on ‘rich’ archaeological signatures including elaborate villas and high-status burials, which may mask ephemeral markers of ‘everyday’ community experiences (Pearce Reference Pearce, Millett, Revell and Moore2016), but this imbalance has begun to be addressed by the Rural Settlement of Roman Britain project, highlighting the hardships rural communities felt under Roman regimes (Smith et al. Reference Smith, Allen, Brindle and Fulford2016).
Though the impact of ‘Roman’ culture (itself made up of differing communities and traditions) is debatable and regionally variable (Pitts Reference Pitts, Millett, Revell and Moore2016), bioarchaeological evidence indicates how Roman occupation placed a strain on communities that only eased in the fifth century, once the pressure to feed administrative centres reduced (Esmonde Cleary Reference Esmonde Cleary, Hinton, Crawford and Hamerow2011; Gerrard Reference Gerrard2013). A narrative of hardship for marginalised communities is revealed; one prompted by the introduction of new diseases and class divides that caused dietary stress (Rohnbogner & Lewis Reference Rohnbogner and Lewis2017). Studies on Romano-British populaces (e.g. Lewis Reference Lewis2011; Hodson Reference Hodson2017; Rohnbogner Reference Rohnbogner2022) are building new understandings of infection, metabolic deficiencies and growth disruption that correlate with heightened sociocultural and environmental stressors triggered by changing regimes. Yet, similar research is required on the preceding Iron Age populations to contextualise interpretations.
The DOHaD hypothesis
Introducing anthropological and biomedical understanding of the maternal environment into archaeological research can enrich our understanding of stress, diet, immunity and health across a community (Agarwal Reference Agarwal2016). The Developmental Origins of Health and Disease (DOHaD) hypothesis posits that experiences within the first 1000 days after conception (until about two years of age) can contribute to epigenetic changes that influence health parameters for adulthood and subsequent generations (Barker Reference Barker2012). During early life, humans will adjust to positive and negative environmental stimuli to maximise survival, but this can also result in permanent biological changes, which may cause issues in later life (Glover Reference Glover and Antonelli2015). Consequently, the skeletal remains of non-adults, whose growing bodies are susceptible to the external influences of stress (defined in this context as a range of factors influencing development, including infection, nutrition, social, cultural and environmental variables, and genetic predisposition), can reflect generational signatures and environmental factors (Gowland & Halcrow Reference Gowland, Halcrow, Gowland and Halcrow2020). Additionally, infant health can be easily influenced by the disease burden and socioeconomic status of the mother, with experiences passing to the child via the intrauterine environment or breastfeeding (Gowland Reference Gowland, Gowland and Halcrow2020). By viewing non-adult experiences alongside the health of reproductive adults, an impression of the stressors affecting different generations can be gained. Thus palaeopathological changes can be seen to reflect the long-term influence of a changing sociocultural landscape, helping to develop a nuanced understanding of the impact a major event had on population health.
Materials and methods
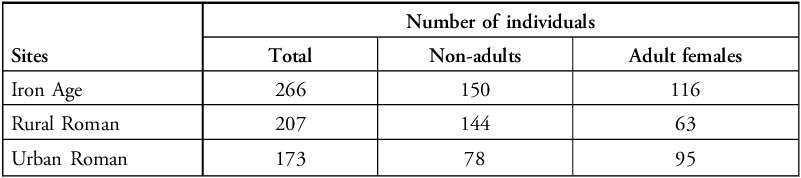
Human skeletal remains were selected from Iron Age and Romano-British sites across England, encapsulating rural and urban settlements dating from the fourth century BC until the fourth century AD. The study sample comprised 646 skeletons (372 non-adults and 274 adult females) from 24 Iron Age and Roman sites (Table 1; see online supplementary materials (OSM) Tables S1 & S2 for detailed breakdown). Variation in the number of individuals available for study resulted from differences in the survival, excavation and accessibility of skeletal remains.
Overview of human skeletal remains from Iron Age (fourth-century BC–first-century AD) and Roman (first–fourth-centuries AD) sites. See OSM for more detailed breakdown of numbers.

Iron Age sites were chosen from across England to capture representative understanding of life during this period. Meanwhile, care was taken when selecting Roman sites to ensure that sampled areas were experiencing similar administrative pressures from Roman occupation. Northern and western sites were avoided as these areas more commonly faced military occupation and thus may have been subjected to differing economic and social regimes (Mattingly Reference Mattingly2006). Instead, this study focused on rural and urban sites from the south and central belt, encapsulating reassessment of commonly researched areas (e.g. Hampshire, Oxfordshire and Dorset) and newly researched areas with excavations published in the past decade (e.g. Northamptonshire and Peterborough). The selected settlements provide an overview of community life, with Middle to Late Iron Age skeletons offering understanding of health prior to the Roman occupation of England for comparison with inhumations buried during the middle to late Roman period (Figure 1). Although the latter consists of a populace that lived hundreds of years after the initial occupation, any health alterations observed reflect a response to the long-lasting impact of living under Roman regimes. Rural sites consist of communities with an agricultural focus (Smith et al. Reference Smith, Allen, Brindle and Fulford2016) and although a handful of villa sites are included, burials thought to be high-status (e.g. placed in family mausoleums, with stone sarcophagi or alongside lavish grave goods) were excluded. Urban sites are characterised by their large settlement size, density, organisation and administrative status, with burials recovered from large, organised cemeteries (Burnham & Wacher Reference Burnham and Wacher1990; Millett Reference Millett2010).
Locations of sites with human skeletal remains selected for analysis; left) Iron Age settlements; right) Roman settlements and their proximity to Roman roads (figure by author).

Skeletal analysis
The biological profiles of all skeletal remains were constructed through age-at-death estimation, health status analysis and, for adults, determination of biological sex. As reliable sexually dimorphic indicators do not manifest prior to puberty (Lewis Reference Lewis2022), the biological sex of non-adults was not determined. Only skeletons with the cranial vault, thoracic spine and long bones preserved for pathological assessment were included in the study.
For non-adults, dental ageing methods based on the formation, development, mineralisation and eruption of each tooth (AlQahtani et al. Reference AlQahtani, Hector and Liversidge2010) were prioritised. Where teeth did not survive, regression equations based on long bone diaphyseal lengths were used to estimate age-at-death within an appropriate degree of error (equations from Scheuer et al. Reference Scheuer, Musgrave and Evans1980 for individuals likely less than 40 gestational weeks (foetal); Primeau et al. Reference Primeau, Friis, Sejrsen and Lynnerup2016 for older individuals). Only those individuals with an age-at-death of below 3.5 years, according to dental ageing, were included in the analysis. This provided a buffer, accounting for the margins of error in ageing methods, to ensure that palaeopathological changes occurring within the first 1000 days after conception were fully captured.
Non-adults were also assessed for growth disruption, indicative of impaired health prompted by environmental stress (Sandman et al. Reference Sandman, Glynn, Poggi Davis, Reissland and Kisilevsky2016; Hodson & Gowland Reference Hodson, Gowland, Gowland and Halcrow2020). Dental age-at-death was compared with an expected diaphyseal long bone length for the corresponding age category to calculate standard deviation from the norm as a Z-score (see Kiserud et al. Reference Kiserud2017 for foetal growth standards; Spake & Cardoso Reference Spake and Cardoso2021 for older non-adults). Individuals with a Z-score of below 0 standard deviation fall below expected growth rates, while those with a Z-score of below -2 standard deviations are classed as having experienced growth faltering. Z-scores were calculated as follows (Sanas et al. Reference Sanas, Umapathi and By Labcorp2021):
 $$ {Z {\hbox-} score={{(long\, bone \,measurement)-(mean\, reference\, measurement)}\over{standard \,deviation \,of \,the \,reference \,population}}}$$
$$ {Z {\hbox-} score={{(long\, bone \,measurement)-(mean\, reference\, measurement)}\over{standard \,deviation \,of \,the \,reference \,population}}}$$
Only females aged between 18 and 45 years were included in the adult analysis to ensure that the sample encapsulated adult females who were likely to have become mothers (Pilkington Reference Pilkington2013; Murphy Reference Murphy2021). Biological sex was assessed through visual examination of pelvic traits and characteristics of the skull (Phenice Reference Phenice1969; Walker Reference Walker2008). Age-at-death was estimated through the assessment of pelvic morphological features, including the pubic symphysis (Brooks & Suchey Reference Brooks and Suchey1990) and the auricular surface (Lovejoy et al. Reference Lovejoy, Meindl, Pryzbecker and Mensforth1985).
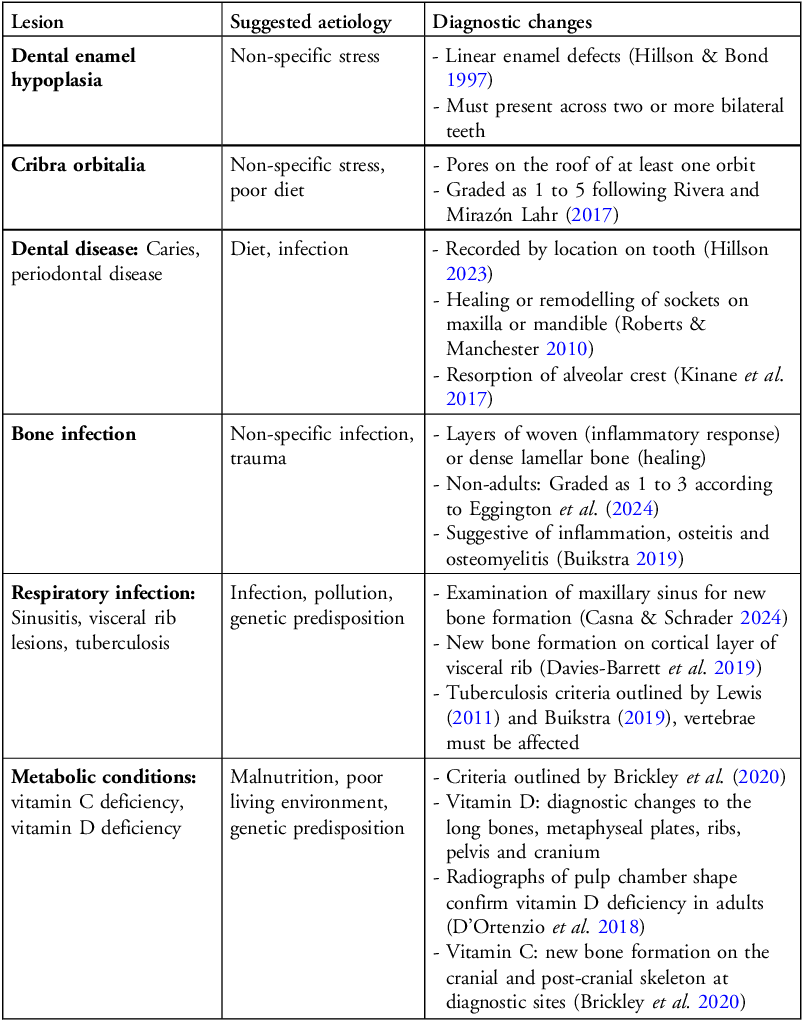
Dental and skeletal lesions were assessed macroscopically and recorded by location, type and whether active or healed (Buikstra Reference Buikstra2019; see Table 2 for further details). The frequencies of different lesions are presented as crude prevalence rates, which express the number of individuals with lesions as a percentage of individuals for whom the relevant skeletal element was available for assessment.
Criteria used for the identification of pathological lesions on non-adult and adult skeletons.

Statistical analysis
Chi-squared tests were applied to assess differences between the Iron Age, rural Roman and urban Roman cohorts. All statistical analyses were conducted using Microsoft Excel and IBM SPSS Statistics 27.
Results
Non-adult palaeopathology
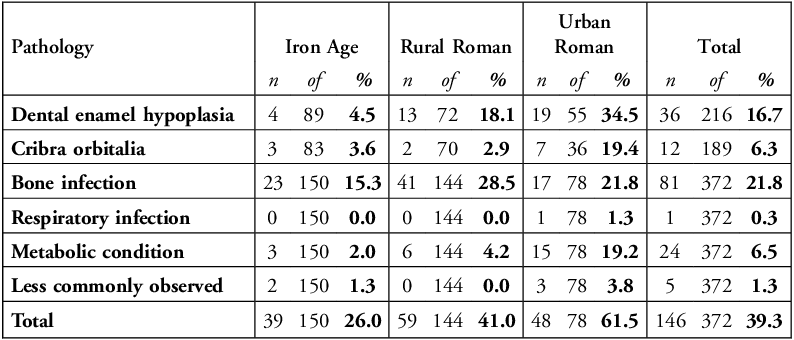
A total of 146 out of 372 non-adults (39.3%) display one or more palaeopathological lesion (see Table 3 and Figure 2). In general, dental enamel hypoplasia and bone infections are the most common lesions. The category ‘less commonly observed’ includes lesions that did not fit into other commonly identified palaeopathological categories (i.e. lytic lesions or congenital changes).
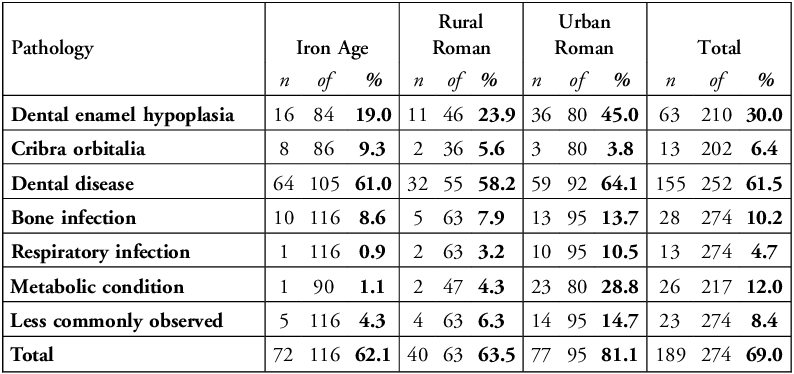
Number (n) and percentage prevalence (%) of non-adults with palaeopathological changes; ‘of’ indicates the number of individuals with relevant skeletal elements for examination.

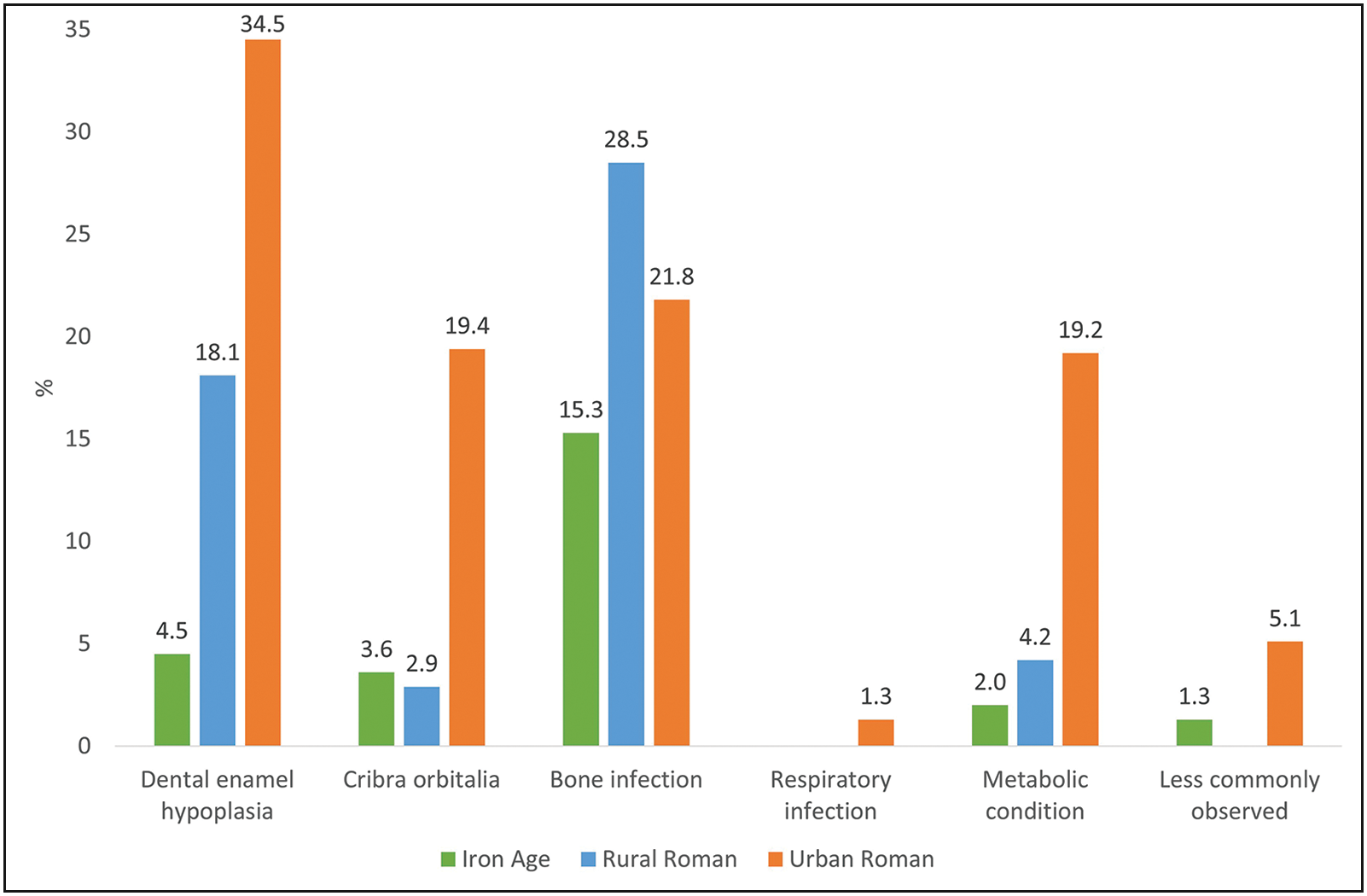
Percentage prevalence rates of palaeopathological changes in the non-adult skeletons (total individuals = 146/372) (figure by author).

Overall, 26.0% of Iron Age non-adults (n = 39) exhibit pathology, compared to 41.0% of rural Roman (n = 59) and 61.5% of urban Roman (n = 48) individuals (Figure 3). This demonstrates a statistically significant increase in pathological conditions from the Iron Age to the Roman period (Χ2 = 27.5, p<0.01, df = 2), and a statistically significant difference between rural and urban Roman non-adults (X2 = 8.6, p<0.01, df = 1). The most common lesion identified is bone infection (n = 81, 21.7%), which is significantly more prevalent in rural Roman non-adults (n = 41, 28.5%) than Iron Age non-adults (n = 23, 15.3%; X2 = 7.4, p<0.01, df = 1), but intermediate in the urban Roman cohort (n = 17, 21.8%). Urban Roman non-adults exhibit significantly higher rates of metabolic conditions (n = 15, 19.2%; X2 = 27.3, p<0.01, df = 2) and cribra orbitalia (n = 7; 19.4%; X2 = 12.9, p<0.01, df = 2) when compared to the other communities. A rise in non-specific stress indicators for Roman non-adults was also identified, with dental enamel hypoplasia present in 34.5% (n = 19) of urban Roman and 18.1% (n = 13) of rural Roman individuals compared to only 4.5% (n = 4) of Iron Age non-adults (X2 = 22.3, p<0.01, df = 2). No significant variation was identified regarding respiratory infections and less commonly observed lesions.
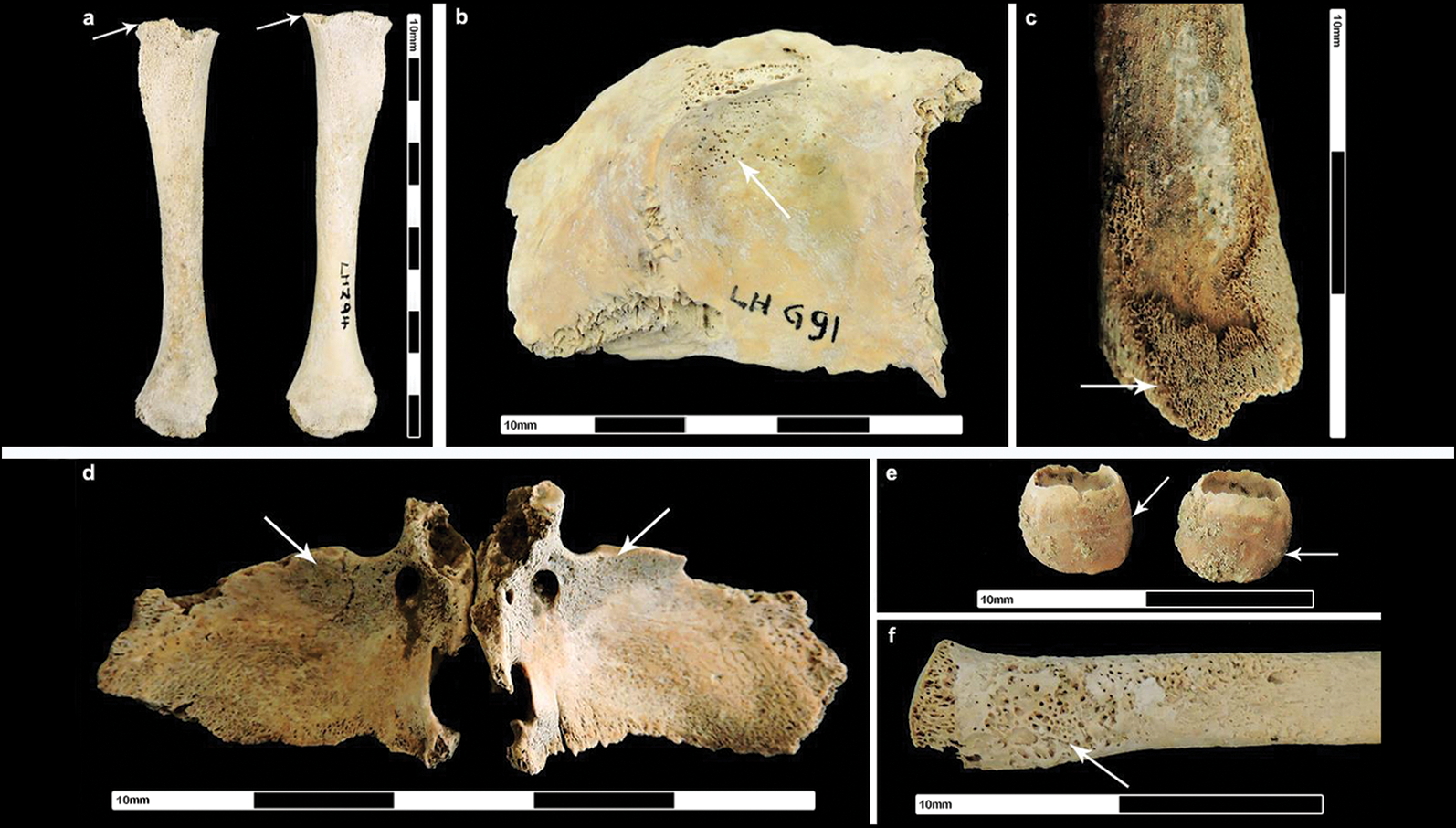
Roman non-adult pathology: a) flattening of humeral heads, suggestive of vitamin D deficiency; b) cribra orbitalia; c) non-specific infection (distal femur); d) new bone on the greater wings of the sphenoid bone, suggestive of vitamin C deficiency; e) dental enamel hypoplasia on deciduous incisors, presenting as a grooved depression; f) lytic foci on the proximal head of a radius, suggestive of tuberculosis (figure by author).

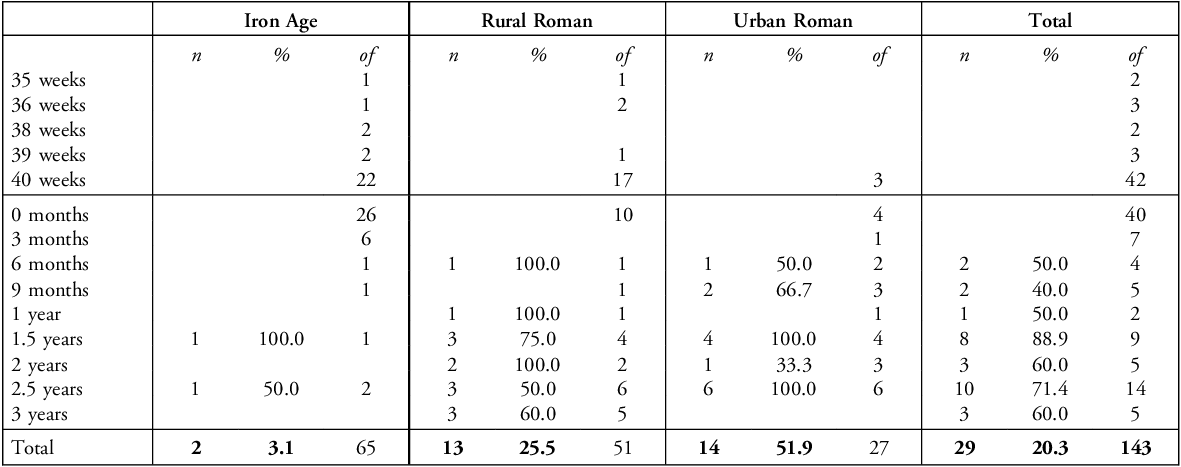
Z-scores could be calculated for 142 individuals: 53 perinates under approximately 40 weeks gestation and 90 non-adults aged over approximately 40 weeks (see Table 4 and Figure 4). Overall, a statistically significant increase in the number of individuals experiencing growth faltering was noted between Iron Age (n = 2, 3.1%) and both Roman cohorts (X2 = 29.4, p<0.01, df = 2), as well as between rural Roman (n = 13, 25.5%) and urban Roman non-adults (n = 14, 51.9%; X2 = 5.4, p<0.05, df = 1). Individuals aged to approximately six months old were the youngest to indicate growth faltering, suggesting post-utero experiences and the loss of a maternal buffer were more likely to impact growth and development.
Number of non-adults from each cohort by mean age that exhibit growth faltering (a Z-score below two standard deviations) when compared to clinical data; ‘of’ indicates the number of individuals with available Z-scores.

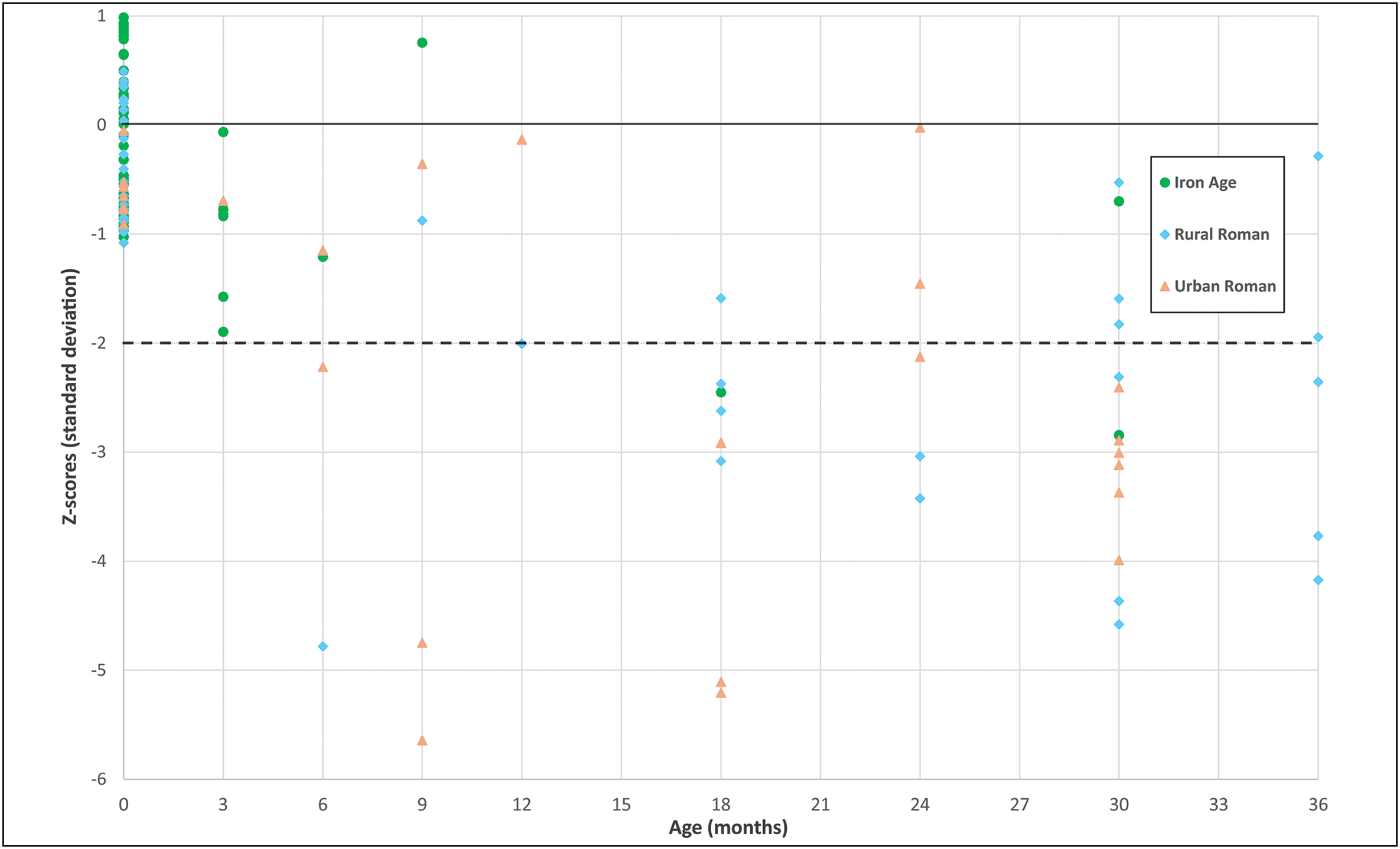
Non-adult Z-scores. Individuals above 0 standard deviation (0SD, solid line) exceeded expected growth rates. Those that fall below two standard deviations (-2SD, dotted line) experienced growth faltering and failed to reach expected growth rates (figure by author).

Adult females
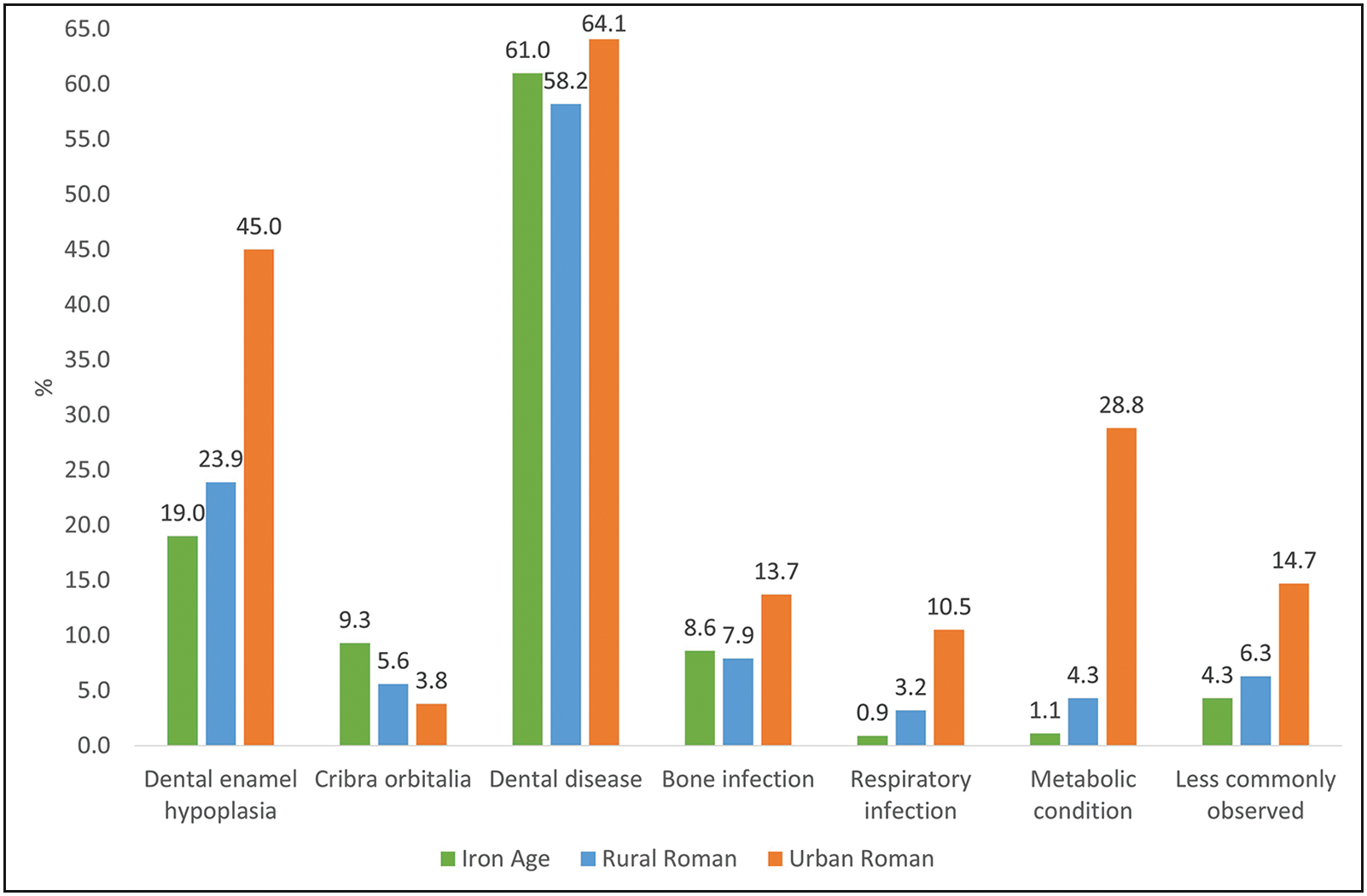
A total of 189 out of 274 adult females (69.0%) exhibit one or more lesion associated with negative health changes (see Table 5 and Figure 5). In general, dental pathologies are the most commonly observed lesions. Here, the ‘less commonly observed’ category is used to describe palaeopathological lesions with complex aetiologies, including congenital changes, osteochondroma, button osteomas and hyperostosis frontalis interna.
Number (n) and percentage prevalence (%) of adults with palaeopathological changes; ‘of’ indicates the number of individuals with relevant skeletal elements for examination.

Percentage prevalence rates of palaeopathological changes in the adult female skeletons (total individuals = 189/274) (figure by author).

Overall, the urban Roman cohort exhibit statistically significantly higher rates of palaeopathological changes (Figure 6), with 81.1% (n = 77) of adult females affected compared to 62.1% (n = 72) of Iron Age (X2 = 26.5, p<0.01, df = 1) and 63.5% (n = 40) of rural Roman females (X2 = 27.1, p<0.01, df = 1). The Iron Age and rural Roman cohorts do not differ significantly. The most common palaeopathological change is dental disease (n = 155, 61.5%), but this does not significantly alter by cohort. The most significant variation is exhibited in metabolic conditions, with 28.8% (n = 23) of urban Roman females affected compared to only 1.1% (n = 1) of Iron Age (X2 = 26.7, p<0.01, df = 1) and 4.3% (n = 2) of rural Roman adults (X2 = 11.2, p<0.01, df = 1). The prevalence of cribra orbitalia does not differ by cohort. Respiratory infections also affected a significantly higher number of urban Roman individuals (n = 10, 10.5%) when compared to the Iron Age (n = 1, 0.9%; X2 = 9.9, p<0.01, df = 1), but no variation in bone infections could be noted. Dental enamel hypoplasia, suggestive of non-specific stress, are significantly more prevalent in urban Roman females (n = 36, 45.0%) compared to Iron Age (n = 16, 19.0%; X2 = 12.7, p<0.01, df = 1) and rural Roman cohorts (n = 11, 23.9%; X2 = 5.6, p<0.05, df = 1).
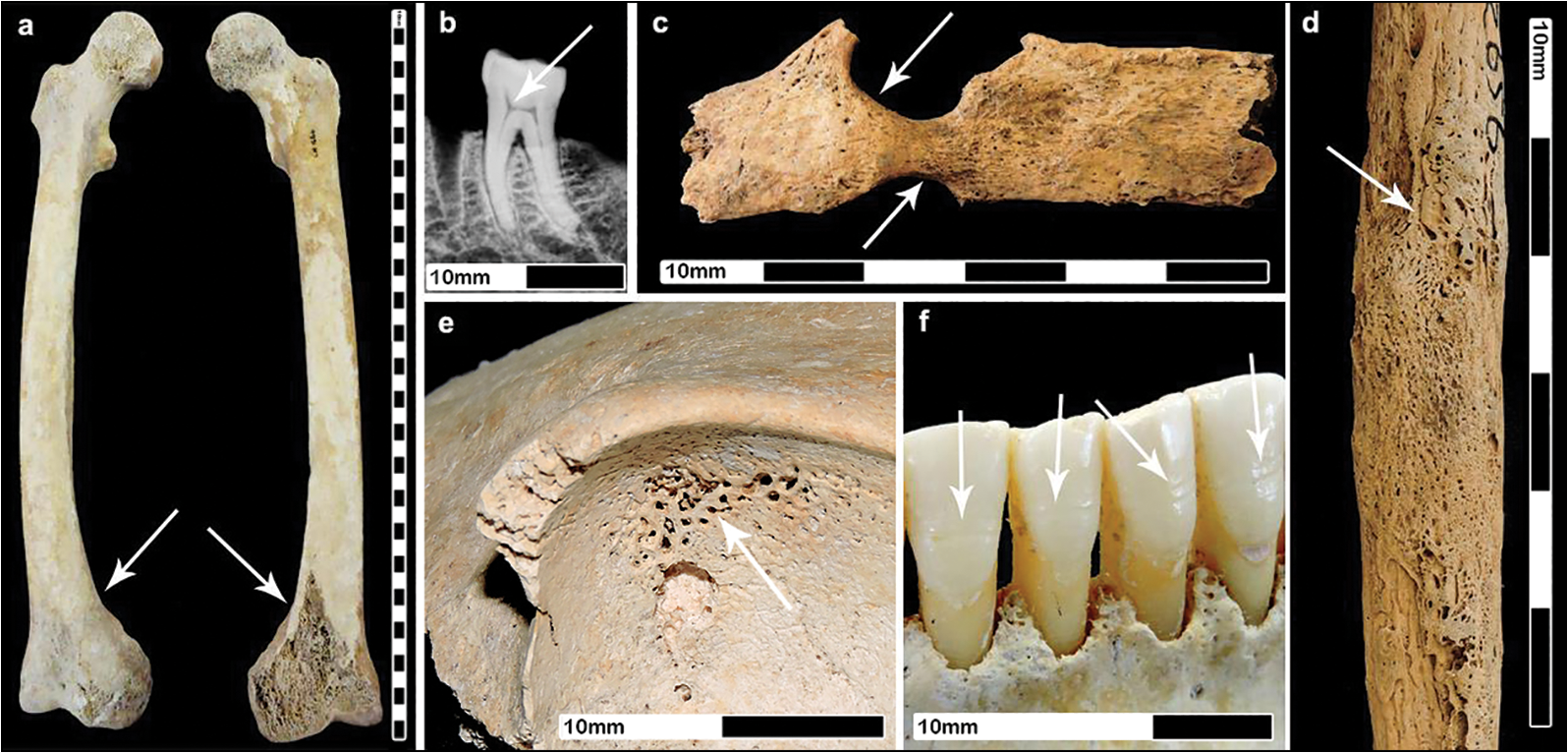
Roman adult female pathology: a) residual bilateral bowing of femora; b) ‘chair-shaped’ pulp chamber of a first molar, indicative of vitamin D deficiency; c) lytic lesions on a rib shaft, suggestive of tuberculosis; d) non-specific infection (shaft of fibula); e) cribra orbitalia; f) dental enamel hypoplasia on permanent incisors (figure by author).

Discussion
A rise in negative health markers affecting Roman individuals is identified, particularly within urban centres, suggesting life under Roman occupation was less conducive to long-term health. Archaeological evidence suggests strains on urban life fluctuated, prompting debate as to whether the fourth century marked a ‘golden age’ for Roman administration in England or a population decline that may have reduced overcrowding and nutritional stress (Gerrard Reference Gerrard2013). This study indicates that urban settlements dating to the fourth century AD exhibit higher rates of palaeopathology, including non-specific stress, respiratory conditions and metabolic disease, indicative of poor socioeconomic status and overcrowded, polluted living situations. Similar indicators of ill-health have been reported at other fourth-century towns including Poundbury Camp in Dorset (Rohnbogner & Lewis Reference Rohnbogner and Lewis2017) and Bath Gate Cemetery in Cirencester (Rohnbogner Reference Rohnbogner2022), which may signify the harsh impact of urbanisation on communities at this time.
It is possible the rise in negative health markers in urban Roman communities may have been exacerbated by exposure to the poisonous metal lead. Lead was integral to the infrastructure of Roman towns, used in plumbing systems, everyday objects such as tableware, cookware and toys, and within consumables including wine and medicines (Moore et al. Reference Moore, Filipek, Kalenderian, Gowland, Hamilton, Evans and Montgomery2021a & Reference Moore, Filipek, Kalenderian, Gowland, Hamilton, Evans and Montgomeryb). Its use in water systems would have made its consumption almost inescapable in urban centres, with even the poorer margins of society unknowingly ingesting quantities of the metal (Scott et al. Reference Scott, Shafer, Smith, Overdier, Cunliffe, Stafford and Farrell2020). Lead poisoning can disrupt metabolic pathways and result in increased rates of nutritional deficiencies (Moore et al. Reference Moore, Filipek, Kalenderian, Gowland, Hamilton, Evans and Montgomery2021a), particularly in infants who can absorb up to double the lead concentrations of adults due to their rapid growth (Moore et al. Reference Moore, Williams-Ward, Filipek, Gowland, Montgomery, Kendall and Kendall2021b). Lead exposure could therefore contribute to the high rates of metabolic conditions observed within urban Roman individuals, demonstrating the detrimental effect of pollutants on health.
Previous research suggested that similar rates of metabolic conditions were present across rural and urban settlements (Rohnbogner Reference Rohnbogner2017); however, the current study demonstrates that the impact on rural health was less than expected for non-adult and adult female health. The prevalence of particular palaeopathological changes suggests that rural non-adults were experiencing higher rates of non-specific stress and increased exposure to pathogens, which may have disrupted normal growth and development, but significant variation between Iron Age and rural Roman adult female health is not identifiable in the study sample. It is possible that the perceived lack of significant variation in health markers could indicate the preservation of regional Iron Age traditions in rural communities, challenging preconceptions of drastic change under Roman administration. Continued occupation from the Iron Age to Roman period is evidenced at several of the sites included in this study; these may have upheld local traditions, leading to a limited health impact.
Understanding the ‘everyday’ life of Roman communities is complicated by the comparative lack of surviving archaeological signatures, with the majority of written accounts and material culture available for analysis reflecting elite viewpoints (Gerrard Reference Gerrard2013). Iron Age communities are generally perceived to have been fairly regionalised, while a colonial system relying on local administrative centres highlighting individual power was introduced in the Roman period (Gerrard Reference Gerrard2013). Nevertheless, influence from Roman occupation ultimately varied regionally, depending on the adoption of practices (Champion Reference Champion, Millett, Revell and Moore2016). For example, differing attitudes to diet have been identified within southern Roman England: urban Londinium demonstrates a cereal-rich weaning diet (Redfern et al. Reference Redfern, Gowland, Millard, Powell and Gröcke2018), matching Roman recommendations by Sonarus (Gynecology 2.XXI [117–119]; Temkin Reference Temkin1991) that may have unwittingly restricted nutritional resources, while stable isotope signatures from rural Oxfordshire indicate a divergence from contemporary advice in a higher intake of freshwater protein (Nehlich et al. Reference Nehlich, Fuller, Jay, Mora, Nicholson, Smith and Richards2011). It is therefore difficult to ascertain how widespread the adoption of practices impacting health would have been; communities likely experienced varied resource strains and exposure to pathogens depending on their proximity to large urban centres or military camps. Despite variations, skeletal evidence is increasingly vital in understanding how life altered alongside Roman occupation.
Conclusion
The rise in prevalence of negative health markers within Roman populations when compared to their Iron Age counterparts suggests Roman individuals were more likely to be exposed to an increasingly negative external environment. Skeletal remains reflect increased indicators of stress, pathogens and limited nutritional resources, evidencing how increasingly stressful living environments—brought on by the establishment of polluted and overcrowded urban centres (Mattingly Reference Mattingly2006), exposure to lead infrastructure (Moore et al. Reference Moore, Filipek, Kalenderian, Gowland, Hamilton, Evans and Montgomery2021a & Reference Moore, Filipek, Kalenderian, Gowland, Hamilton, Evans and Montgomeryb) and restriction of access to resources prompting a reliance on cereals (Rohnbogner & Lewis Reference Rohnbogner and Lewis2017)—contributed to a long-term impact on health. Limited variation between Iron Age and rural Roman communities may indicate the continuation of cultural norms, challenging perspectives that England was widely affected by the imposition of Roman identity. Meanwhile, the significant rise in negative health indicators identified across urban Roman civitas capitals implies that individuals were more likely to be exposed to, and therefore develop markers of, a poor socioeconomic environment within the first 1000 days after conception, constricting health parameters for later life and subsequent generations. These findings emphasise how the Roman occupation affected generations of mothers and infants.
Acknowledgements
The author would like to thank the following individuals and institutions for access to skeletal collections: Ross Turle (Hampshire Cultural Trust), Angie Bolton (Oxfordshire Museums Service), Brett Thorn (Discover Bucks Museum), Ben Donnelly-Symes (Northamptonshire Archaeological Resource Centre), Louisa Sharman (Peterborough Museum), Caroline Morris (Corinium Museum), Elizabeth Selby (Dorchester Museum), Tabatha Barton (Milton Keynes Museum) and Jo Buckberry (Bradford University). Thanks are also due to Prof Mary Lewis and Prof Hella Eckardt (University of Reading) for valuable advice and input.
Funding statement
This research received no specific grant from any funding agency or from commercial and not-for-profit sectors.
Online supplementary material (OSM)
To view supplementary material for this article, please visit https://doi.org/10.15184/aqy.2025.10263 and select the supplementary materials tab.
Author contribution: CRediT Taxonomy
Rebecca Pitt: Conceptualization-Lead, Data curation-Lead, Formal analysis-Lead, Investigation-Lead, Methodology-Lead, Project administration-Lead, Resources-Lead, Software-Lead, Validation-Lead, Writing - original draft-Lead, Writing - review & editing-Lead.




 Open access
Open access