


Introduction
Across the life course individuals will spend around 10 % of their time at work(1). While employment promotes physical and mental health and supports social and economic stability(2), the workplace is a key contributor to determinants of health. A UK economic and public health priority is to increase healthy working life span(3). The workplace is a key environment for public health nutritional interventions, with research demonstrating that promotion of nutritional health is of benefit to businesses and employees(Reference Grimani, Aboagye and Kwak4). In 2023, The Nutrition Society Workplace Diet and Health Special Interest Group Round Table Meeting identified a research priority to understand how to engage hard-to-reach employee groups (e.g. low paid, male, shift workers, ethnic minorities)(Reference Gibson, Lewis and Hilberink5) with nutrition and well-being interventions. Food and beverage is the largest manufacturing industry in the UK(6) employing ∼400 000 staff(Reference Dodds7) and is essential to sustaining UK food supply. Many of these employees have atypical working hours (e.g. outside 7 a.m. to 7 p.m., weekends, long hours and zero-hour contracts) and tend to be in low-paid occupational groups. Strong evidence supports the association between poor cardiometabolic health with shift work(Reference Moreno, Marqueze and Sargent8) and long working hours(Reference Kivimäki, Virtanen and Kawachi9), potentially mediated by poor dietary choices(Reference Lowden, Moreno and Holmbäck10). An extensive systematic review showed that workplace interventions with a nutrition component can improve dietary intake and cardiometabolic health but highlighted a need to understand how to tailor workplace programmes across different socio-economic contexts(Reference Penalvo, Sagastume and Mertens11). This may be of particular importance to UK food manufacturing staff, as shift workers have been shown to have limited engagement with workplace health programmes,(Reference Nabe-Nielsen, Jørgensen and Garde12) and the wider manufacturing sector has been shown to have low investment in staff well-being programmes(13).
Interventions to promote improved workforce health need to be of a complex design (e.g. targeting multiple levels – from individuals to society and/or comprising of multiple components). The UK guidance for developing complex interventions recommends that interventions should target key identified behaviours(Reference Skivington, Matthews and Simpson14). The Behaviour Change Wheel is an established toolbox recommended to inform UK public health intervention development, from selection of target behaviours to mapping behaviours to interventions that are under pinned by behaviour changes techniques(Reference West, Michie and Atkins15). An important development stage is to understand the types of behavioural interventions that are currently implemented or have been previously evaluated as well as to also understand implementation barriers and enablers.
Despite the size and economic importance of the UK food and beverage manufacturing sector, little is known about how employers support the nutritional health of their workforce, particularly those in low-paid or shift-based roles. Occupational challenges that are likely to contribute to nutritional health and well-being include working in highly controlled environments (e.g. protective clothing, temperature-controlled), manual and repetitive tasks and sensory exposure to food aromas. Evidence on the types of interventions implemented and the practical barriers to delivery remains limited. To address this gap, a scoping review and industry survey were conducted to: (i) characterise the nature and content of workplace diet and well-being interventions in food manufacturing settings; (ii) map intervention components to the Behaviour Change Techniques (BCTs) Taxonomy and (iii) identify perceived barriers and enablers to implementation. Findings will inform the development of more effective, context-specific interventions to promote food and beverage manufacturing employees’ health in this hard-to-reach UK workforce.
Methods
This project combined a systematic scoping literature review (Open Science Framework registration https://osf.io/3pxku/overview) and a UK food and beverage manufacturing industry survey to characterise the key elements of programmes that have been tested or implemented. A scoping review methodology was selected as the aim was to characterise the types of research conducted within this field and to identify knowledge gaps(Reference Munn, Peters and Stern16).
Scoping review
A systematic scoping review was conducted following JBI guidelines(Reference Peters, Marnie and Tricco17). The search strategy aimed to identify published and unpublished sources of evidence. An electronic database search was conducted in the following databases: MEDLINE, EMBASE, APA PsycINFO and Web of Science. The search strategy was constructed using the Population, Concept and Context framework. The search strategy, including all identified keywords and index terms, was adapted for each database and/or information source. Reference lists of systematic reviews and included articles were hand screened for additional studies. Unpublished (‘grey literature’) sources were searched and included trial registers (US National Institute of Health (clinicaltrials.gov), ISRCTN and WHO (ISCTRP registry)), PhD theses (UK repositories), preprints, organisational websites and key conference papers were searched for relevant studies, for full details of the search see Supplementary material – search strategy.
Peer reviewed studies and grey literature publications were included if they reported exposure to a workplace nutrition, health and well-being intervention set in a high-income country (defined by The World Bank Classification), among food or beverage manufacturing sector employees. The aim of the overall project is to develop strategies for UK organisations. However, as the pilot search identified a limited number (n 6), consensus agreement of the research team was to include studies in any high-income country to capture a wide number of examples that may have applicability to the UK. The food and beverage manufacturing sector was defined in consultation with the UK Food and Drink Federation as ‘companies that are primarily engaged in producing and/or processing and packaging final goods for human consumption from raw and/or processed food materials’. Manufacturing employees were defined as having a job role related to production operations in food or beverage manufacturing, covering roles such as production operatives, lab technicians to engineers. Where there was uncertainty over definitions, experts from the project steering group were consulted. There was no exclusion criteria applied to participant characteristics such as age, health status or ethnicity. Searches were limited to English language publications from January 2000 January 2025. Low- and middle-income settings were excluded as were those conducted in agriculture, food retail, catering and food service. Studies with no diet or nutrition component to the intervention were also excluded.
Study selection
All identified citations were collated and uploaded into Covidence literature review software (https://www.covidence.org/) and duplicates removed. Following a pilot, titles and abstracts were screened by two independent reviewers (GR, HA) against the inclusion and exclusion criteria. Any disagreements between reviewers were resolved by a third reviewer (RG). Potentially relevant citations were retrieved in full, and full text assessed for inclusion by two independent reviewers (RG, HA). Reasons for exclusion at full text stage were recorded and presented in a Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for Scoping Reviews(Reference Tricco, Lillie and Zarin18). Any disagreements arising between reviewers were resolved by a third reviewer (RG). See reporting checklist in Supplementary material.
Industry case studies
An extensive internet search was performed to identify publicly available case studies where an employee nutrition, health or well-being intervention had been implemented within the food or beverage manufacturing industry. An industry case study was defined by the research team as a publicly available published description or evaluation of a health and well-being programme in a food manufacturing company. All case studies identified were collated into a Microsoft Excel spreadsheet and screened by two independent reviewers (GR, HA) against the above inclusion criteria. Any disagreements were resolved by a third reviewer (RG), Supplementary material.
Data extraction and Behaviour Change Technique coding
Data were extracted in duplicate (GR and HA) using a data extraction template developed through consensus of the research team members (RG, BRH, WH, EP, LD and HT). The extraction tool was piloted by GR and HA prior to data extraction. The following information was extracted: Study design, industry setting, number of employees, participant characteristics, method of programme delivery (e.g. in person and by whom), type of nutrition intervention(s) employed, any non-nutrition intervention components, intervention duration, the method and measures of evaluation used, available information on levels of employee engagement, reported barriers or enablers to implementation, funding source. The characteristics of the nutrition programme or intervention elements describe in each study were extracted and coded (e.g. provision of healthier canteen options was coded as physical food environment change) and then mapped to one of sixteen groups of BCTs listed in The BCTs Taxonomy (BCTTv1)(Reference Michie, Richardson and Johnston19). Each BCT is defined as ‘an active component of an intervention designed to change behaviour’ (Reference Michie, Atkins and West20). For example, a change in the physical food environment (e.g. addition of healthy menu items in a canteen) was mapped to Group 12 ‘Antecedents’ – a stimulus that triggers a behaviour. Some intervention characteristics were mapped to two BCT groups, e.g. free fruit delivery was mapped to Group 7 ‘Associations’ – a stimulus with the purpose of prompting or cueing the behaviour and Group 12 ‘Antecedents’ as the provision of fruit also add a healthy food into the environment. Coding and mapping were conducted by two independent reviewers (GR, HA). Any disagreements arising in coding were resolved by a third reviewer (RG).
Results reporting and synthesis
Characteristics of the studies included are described using descriptive statistics. A narrative synthesis was conducted to identity behavioural techniques applied across all data sources. The reported barriers and enablers to intervention implementation were collated and mapped to the social ecological model based on the level they referred to: macro-wider society, community level, organisational level and employee level.
Industry survey
The industry survey was a self-administered online open survey (Supplementary material) and reported in-line with the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) guidelines(Reference Eysenbach21), Supplementary material CHERRIES checklist. Informed consent was obtained from all subjects at the start of the survey.
The web-based survey was built using Qualtrics, version 2025 (https://www.qualtrics.com) and divided into the following seven sections, reflecting the same domains of interest as the scoping review: organisational setting, nutrition, health and well-being provision, worksite food provision, nutrition support, staff participation, evaluation and feedback and, barriers and enablers to implementation. Before survey distribution, the survey was piloted among five people (researchers, dietitians and steering group members). Feedback was gained on the survey’s layout, clarity, content, ease and logic. Adaptive questioning was applied throughout to reduce complexity of questions, and forced responses were set to prevent incomplete responses. A non-response option, such as ‘prefer not to say’ or ‘I’m not sure’, was provided for all questions, no back button was provided. The order of questions was not randomised. The final survey contained thirty-three questions over thirteen pages, with a combination of multiple-choice questions and free text. The survey collected responses from individuals involved in staff nutrition, health and well-being across the UK food and beverage manufacturing industry. The survey ran between 27 March and 5 May 2025.
The survey was emailed to a list of 650 industry contacts via gatekeepers, and it was also advertised on social media (LinkedIn) through The Nutrition Society, British Dietetic Association and Nutritionists in Industry (professional networking and continuous professional development group for nutritionists working in industry). Respondent eligibility was self-reported; working directly or indirectly in nutritional health and well-being of UK food manufacturing employees. This was a convenience sample with no a priori sample size because of the exploratory and descriptive nature of the study. Participants were advised of the survey length, data storage procedures, lead investigator and the purpose of the survey on the landing page. Informed consent was obtained at this point. Participants were advised that survey completion was voluntary, and they could stop at any point during the survey; however, once submitted, participants were advised that they would be unable to withdraw their responses. As an incentive to participate, respondents were invited to enter a prize draw to win one of two £50 shopping vouchers following completion of the survey. To participate in the prize draw, participants were directed to a separate Qualtrics link for them to enter their email address and consent to the prize draw. It was not possible to link the email addresses to the participant responses, and all email addresses were deleted after the prizes had been claimed. Before analysis, all incomplete responses were excluded. Narrative synthesis was performed and the results triangulated with scoping review findings.
Results
Scoping review
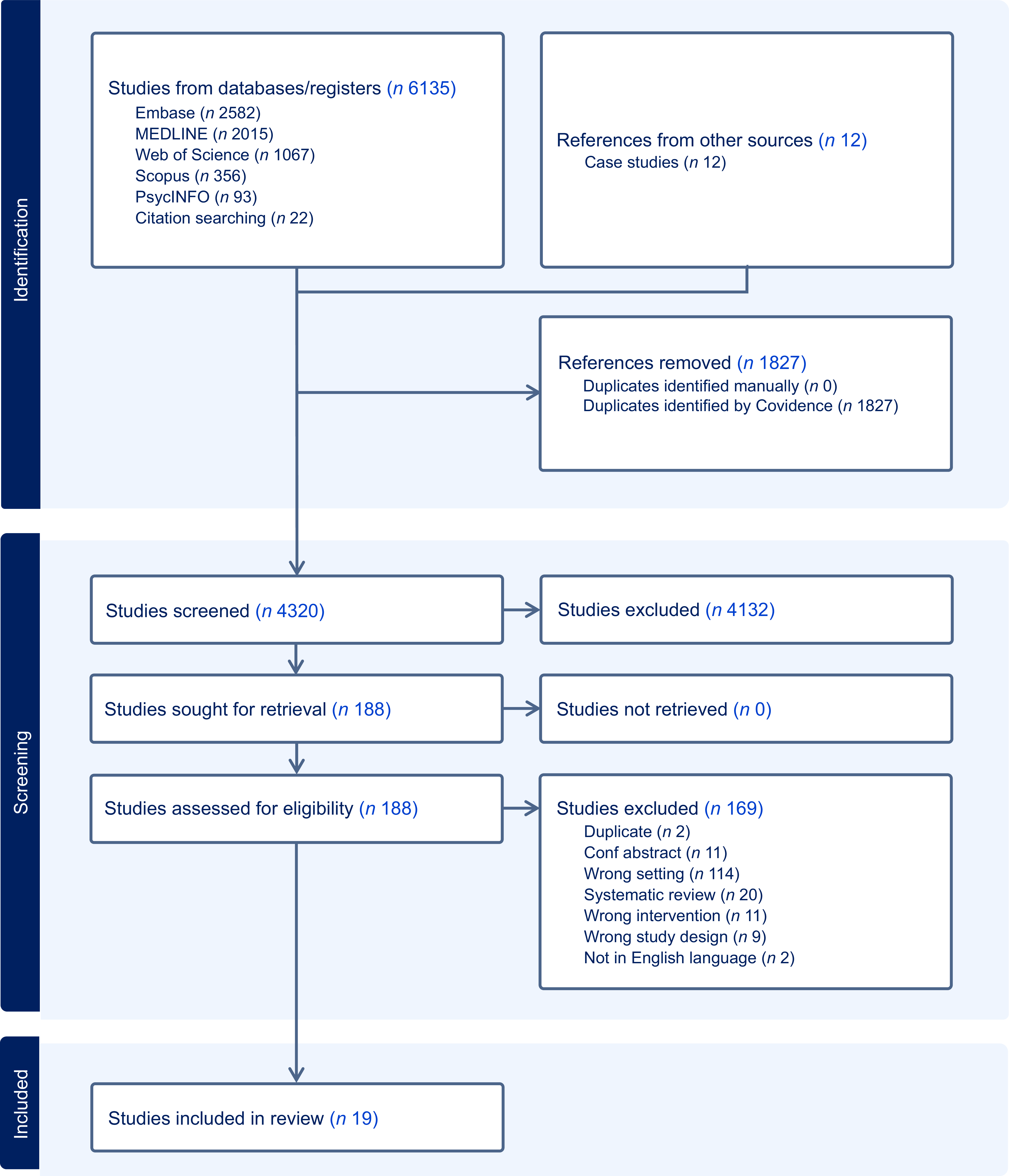
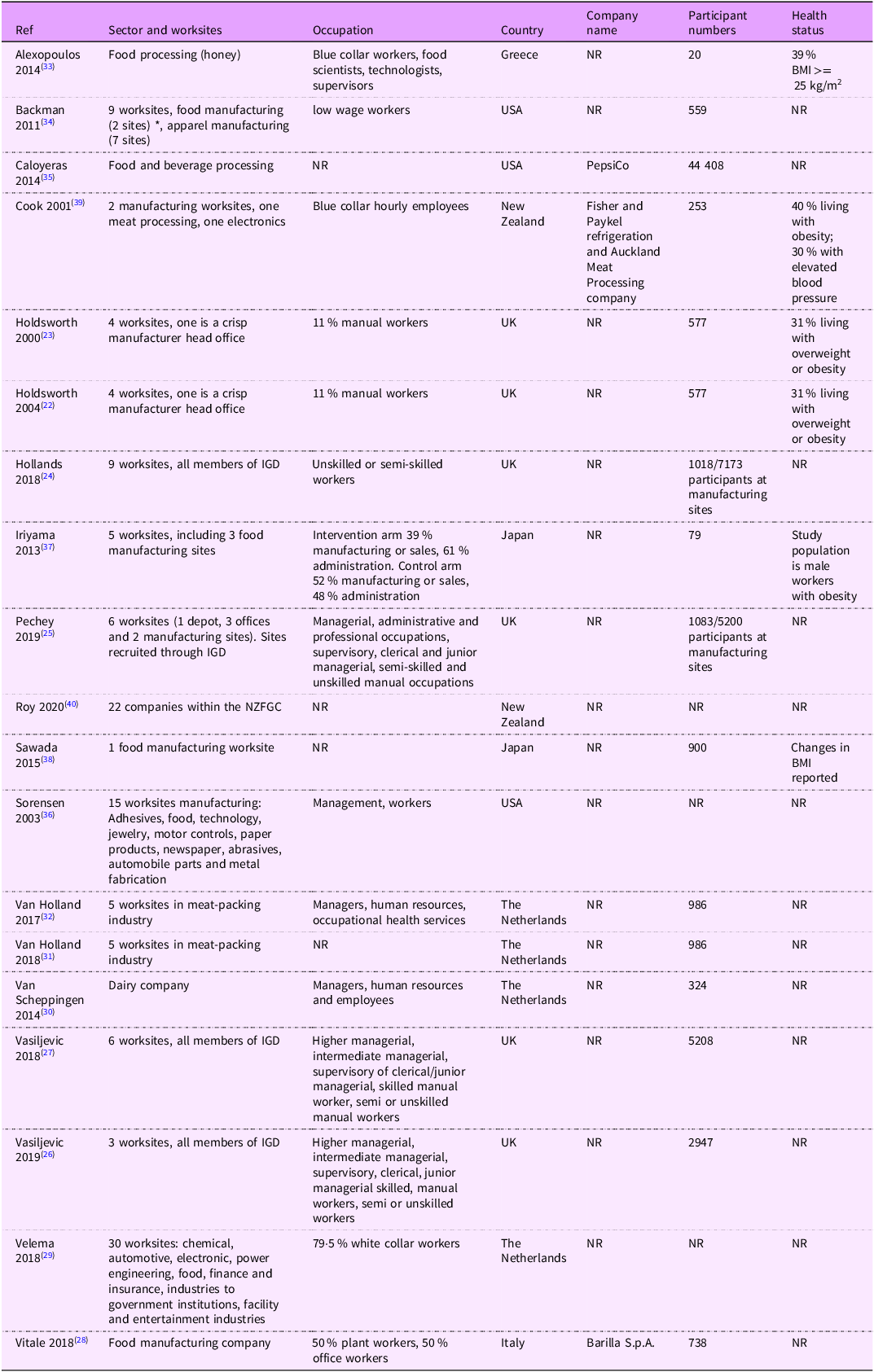
Of the 6147 studies screened, nineteen published studies met the inclusion criteria and are included in this review, as shown in Figure 1. Six studies were conducted in a UK setting(Reference Holdsworth, Raymond and Haslam22–Reference Vasiljevic, Cartwright and Pilling27), six in Europe,(Reference Vitale, Bianchi and Rapetti28–Reference Alexopoulos, Tanagra and Panidis33), three in the USA(Reference Backman, Gonzaga and Sugerman34–Reference Sorensen, Stoddard and LaMontagne36), two in Asia(Reference Iriyama and Murayama37,Reference Sawada, Murayama and Takemi38) and two in Australasia(Reference Cook, Swinburn and Stewart39,Reference Roy, Styles and Braakhuis40) . Except in three studies(Reference Vitale, Bianchi and Rapetti28,Reference Caloyeras, Liu and Exum35,Reference Cook, Swinburn and Stewart39) , the company name was not reported. Five studies reported the baseline health status of employees, with overweight/obesity prevalence ranging 30 %–100 %, the latter in a study focused on male workers living with obesity(Reference Iriyama and Murayama37) from characteristics of published studies are shown in Table 1.
PRISMA-SCR flow diagram.

Figure 1. Long description
The flowchart illustrates the process of identifying, screening, and including studies in a review. It begins with the identification phase, where studies are sourced from databases/ registers and other references. Studies from databases/ registers include Embase (n = 2582), MEDLINE (n = 2015), Web of Science (n = 1067), Scopus (n = 356), PsycINFO (n = 93), and citation searching (n = 22), totaling 6135 studies. References from other sources include case studies, totaling 12 studies. In the next step, 1827 references are removed due to duplicates identified by Covidence. The screening phase involves 4320 studies, of which 4132 are excluded. 188 studies are sought for retrieval, with none not retrieved. These 188 studies are assessed for eligibility, resulting in 169 studies being excluded for various reasons such as being duplicates, conference abstracts, wrong setting, systematic reviews, wrong intervention, wrong study design, and not being in English. Finally, 19 studies are included in the review.
Characteristics of studies included in the systematic scoping review

* Food manufacturing sites were allocated to control condition. IGD, The Institute of Grocery Distribution; NZFGC, New Zealand Food and Grocery Council, NR, not reported.
Published studies – intervention components and outcome measures
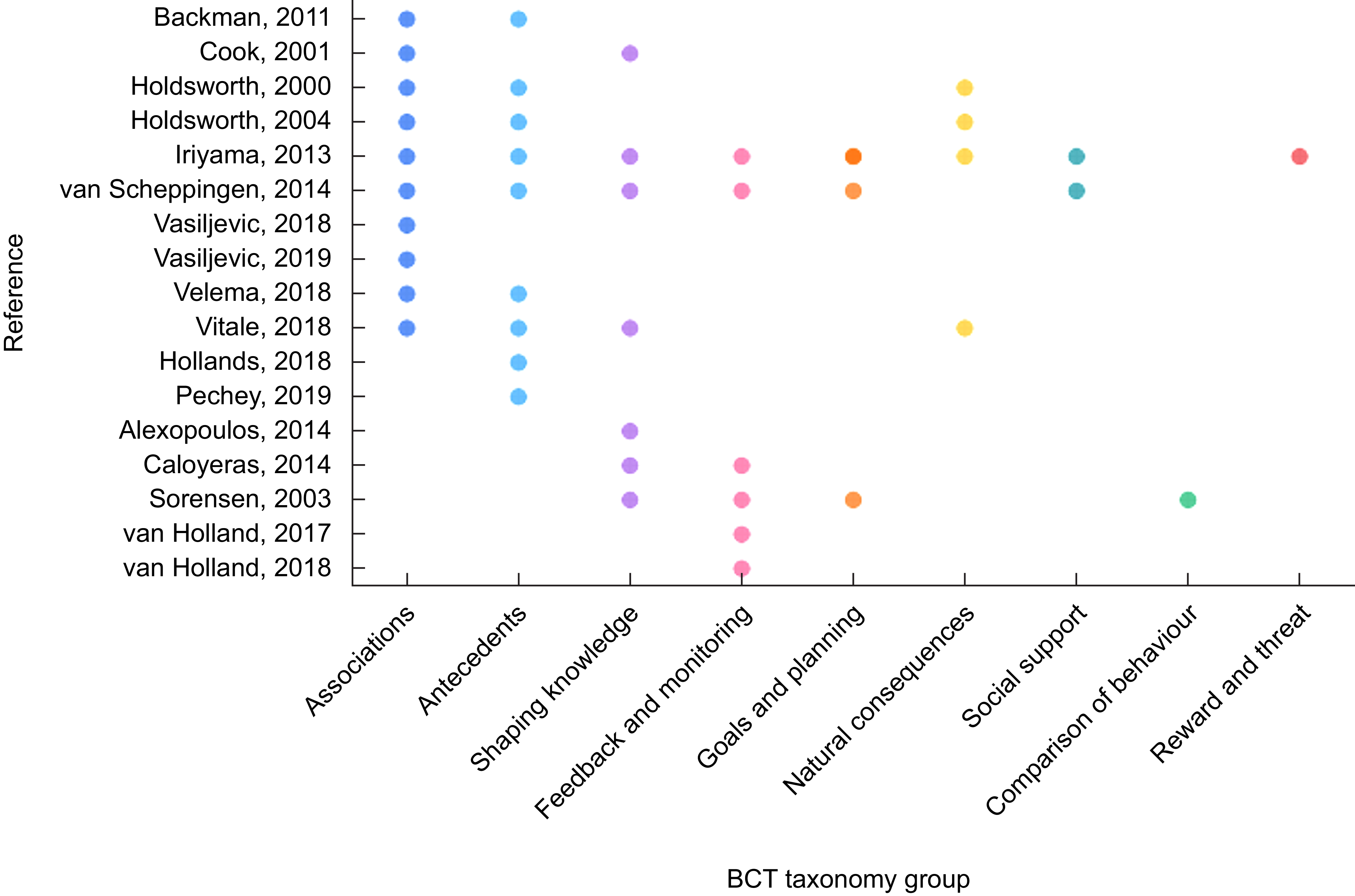
From the sixteen groups of BCT in the taxonomy(Reference Michie, Richardson and Johnston19), elements of the nutritional interventions identified were mapped to nine of them, in ten studies interventions were mapped to more than one BCT group – the most common combination being ‘Associations’ and ‘Antecedents’ in seven studies, Figure 2, supplementary Table S1. The most frequently mapped was Group 7 ‘Associations’ with ten studies (53 %) having intervention elements mapped(Reference Holdsworth, Raymond and Haslam22,Reference Holdsworth, Raymond and Haslam22,Reference Vasiljevic, Fuller and Pilling26–Reference van Scheppingen, de Vroome and Ten Have30,Reference Backman, Gonzaga and Sugerman34,Reference Iriyama and Murayama37,Reference Cook, Swinburn and Stewart39) , intervention elements mainly included the provision of cue and prompts through provision of fruit(Reference van Scheppingen, de Vroome and Ten Have30,Reference Backman, Gonzaga and Sugerman34) , canteen labels(Reference Vasiljevic, Fuller and Pilling26,Reference Vasiljevic, Cartwright and Pilling27) and material highlighting healthier choices(Reference Holdsworth, Raymond and Haslam22,Reference Holdsworth, Haslam and Raymond23,Reference Vitale, Bianchi and Rapetti28,Reference Velema, Vyth and Hoekstra29,Reference Iriyama and Murayama37,Reference Cook, Swinburn and Stewart39) . Nine studies (47 %) had intervention elements mapped to Group 12 ‘Antecedents’ (Reference Holdsworth, Raymond and Haslam22–Reference Pechey, Cartwright and Pilling25,Reference Vitale, Bianchi and Rapetti28–Reference van Scheppingen, de Vroome and Ten Have30,Reference Backman, Gonzaga and Sugerman34,Reference Iriyama and Murayama37) , these were mainly around restructuring the physical or social environment – for example, providing free fruit and altering canteen menu availability to focus on healthy options. Seven studies (37 %) were mapped to Group 4 ‘Shaping knowledge’ (Reference Vitale, Bianchi and Rapetti28,Reference van Scheppingen, de Vroome and Ten Have30,Reference Alexopoulos, Tanagra and Panidis33,Reference Caloyeras, Liu and Exum35–Reference Iriyama and Murayama37,Reference Cook, Swinburn and Stewart39) intervention elements included education and workshop sessions(Reference Vitale, Bianchi and Rapetti28,Reference van Scheppingen, de Vroome and Ten Have30,Reference Alexopoulos, Tanagra and Panidis33,Reference Caloyeras, Liu and Exum35–Reference Iriyama and Murayama37,Reference Cook, Swinburn and Stewart39) and provision of educational materials(Reference Holdsworth, Raymond and Haslam22,Reference Holdsworth, Haslam and Raymond23,Reference Vitale, Bianchi and Rapetti28,Reference Alexopoulos, Tanagra and Panidis33,Reference Iriyama and Murayama37,Reference Cook, Swinburn and Stewart39) . Six studies (32 %) were mapped to Group 2 ‘Feedback and monitoring’ (Reference van Scheppingen, de Vroome and Ten Have30–Reference van Holland, Brouwer and de Boer32,Reference Caloyeras, Liu and Exum35–Reference Iriyama and Murayama37) with elements mainly including health assessments that included feedback to staff. Four studies (21 %) mapped to Group 5 ‘Natural consequences’ (Reference Holdsworth, Raymond and Haslam22,Reference Holdsworth, Haslam and Raymond23,Reference Vitale, Bianchi and Rapetti28,Reference Iriyama and Murayama37) , three studies (16 %) to Group 1 ‘Goals and planning’ (Reference van Scheppingen, de Vroome and Ten Have30,Reference Sorensen, Stoddard and LaMontagne36,Reference Iriyama and Murayama37) , two studies (11 %) from group 3 ‘Social support‘ (Reference van Scheppingen, de Vroome and Ten Have30,Reference Iriyama and Murayama37) , one study (5 %) from Group 6 ‘Comparison of behaviour’ (Reference Sorensen, Stoddard and LaMontagne36) and one study (5 %) from Group 10 ‘Reward and threat’(Reference Iriyama and Murayama37). Non-nutrition intervention components were also reported, these included alcohol awareness, counselling, food hygiene advice, fitness or physical activities, smoking cessation and provision of no smoking areas. Characteristics of interventions implemented, mapped BCT and findings are shown in Table 2.
Mapping behaviour change techniques (BCT) to identified elements of nutrition interventions in published studies. Two studies had insufficient detail to enable mapping.

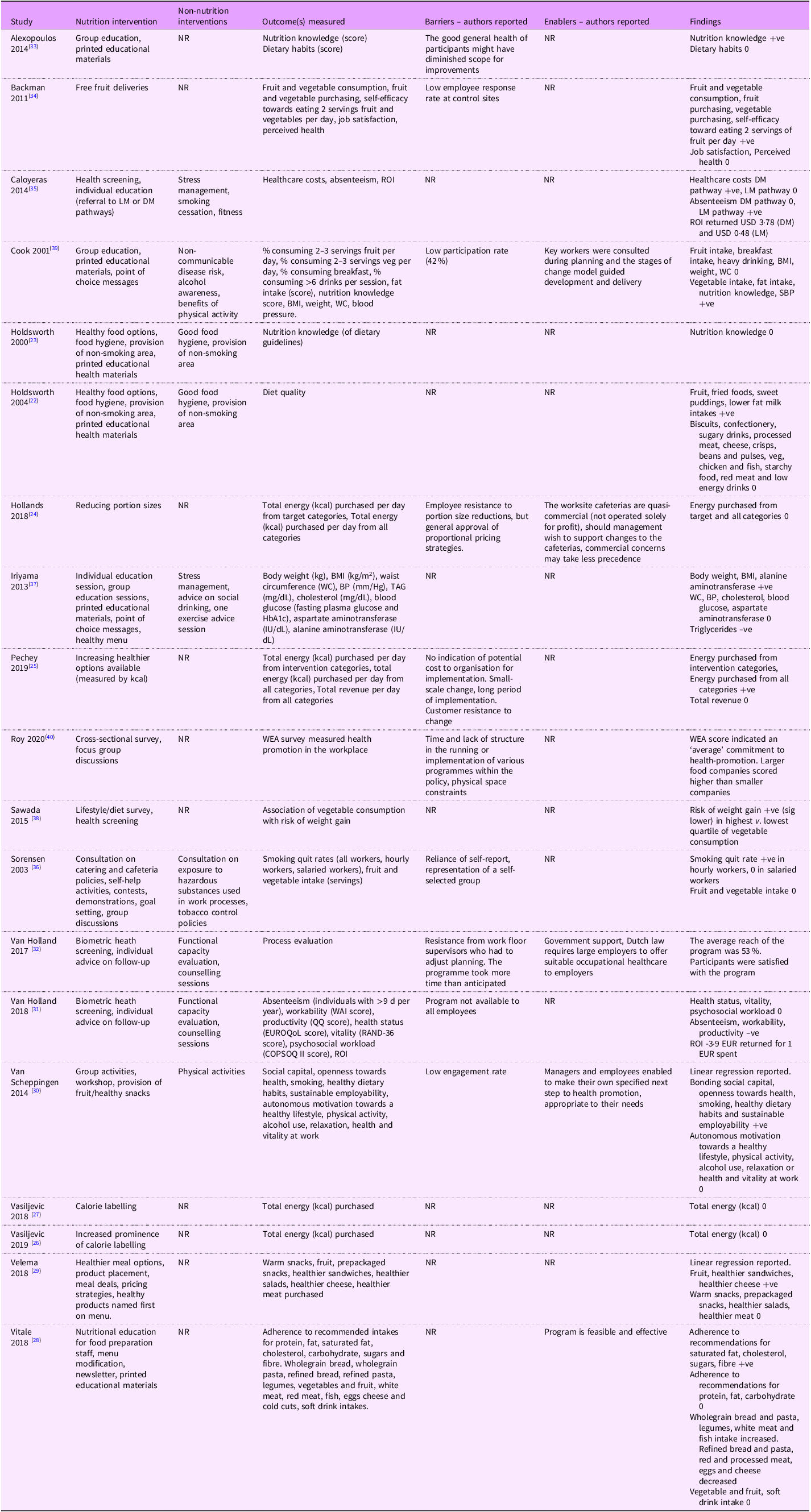
Nutrition, health and well-being interventions, reported barrier, enablers and summary results

Table 2. Long description
A table with 16 rows and 7 columns. The columns are labeled Study, Group, BCT, Intervention, Outcome, Barriers, and Enablers. The table lists various studies and their corresponding BCT groups, interventions, outcomes, barriers, and enablers. Each row provides detailed information about the specific study, the BCT group to which the intervention elements were mapped, the type of intervention, the outcome of the intervention, and the barriers and enablers reported. The table captures the diversity of interventions and their effects across different studies.
BCT, behaviour change technique taxonomy (17); LM, lifestyle management; DM, disease management; SBP, systolic blood pressure; ROI, return on investment; WC, waist circumference; WEA, workplace environment audit; NR, not reported. Legend: +ve Significant positive change, –ve significant negative change, 0 no significant change.
In total, ninety-five outcomes were reported in published studies. These were categorised into dietary outcomes (n 63), health outcomes (n 20) and organisational outcomes (n 12). These were wide ranging, including the following: Adherence to dietary recommendations, breakfast intake, dietary quality, energy purchased, fat intake, fruit and vegetable intake, intakes of healthy and unhealthy food items, nutrition knowledge, absenteeism, healthcare costs, job satisfaction, productivity, vitality and workability, blood glucose, blood pressure, BMI, body weight, cholesterol, perceived health, TAG and waist circumference. Of the sixty-three dietary outcomes, thirty-three (52 %) reported a positive change(Reference Holdsworth, Raymond and Haslam22,Reference Pechey, Cartwright and Pilling25,Reference Vitale, Bianchi and Rapetti28–Reference van Scheppingen, de Vroome and Ten Have30,Reference Alexopoulos, Tanagra and Panidis33,Reference Caloyeras, Liu and Exum35,Reference Cook, Swinburn and Stewart39) , thirty (48 %) reported no significant difference(Reference Holdsworth, Raymond and Haslam22–Reference Hollands, Cartwright and Pilling24,Reference Vasiljevic, Fuller and Pilling26–Reference Velema, Vyth and Hoekstra29,Reference Alexopoulos, Tanagra and Panidis33,Reference Sorensen, Stoddard and LaMontagne36,Reference Cook, Swinburn and Stewart39) . Of the 20 health outcomes, seven (35 %) reported a positive change(Reference van Scheppingen, de Vroome and Ten Have30,Reference Sorensen, Stoddard and LaMontagne36,Reference Iriyama and Murayama37,Reference Cook, Swinburn and Stewart39) , one (5 %) reported a negative change(Reference Iriyama and Murayama37) and, 12 (60 %) reported no significant difference(Reference van Scheppingen, de Vroome and Ten Have30,Reference Iriyama and Murayama37,Reference Cook, Swinburn and Stewart39) . Of the twelve organisational outcomes, five (42 %) reported a positive change(Reference van Scheppingen, de Vroome and Ten Have30,Reference Caloyeras, Liu and Exum35) , three (25 %) reported a negative change(Reference van Holland, Reneman and Soer31) and four (33 %) reported no significant difference(Reference van Scheppingen, de Vroome and Ten Have30,Reference van Holland, Reneman and Soer31) .
Case studies – intervention components
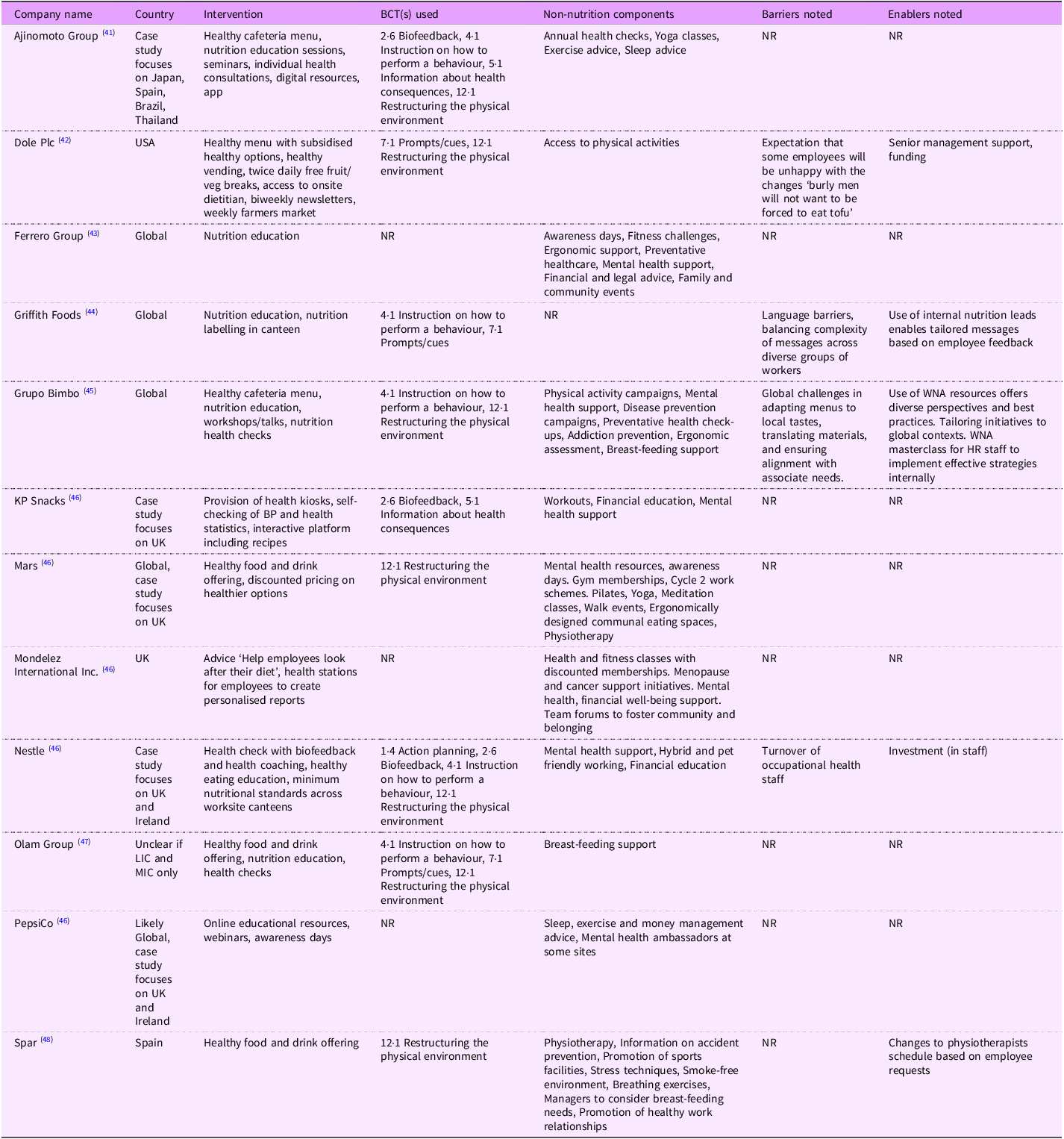
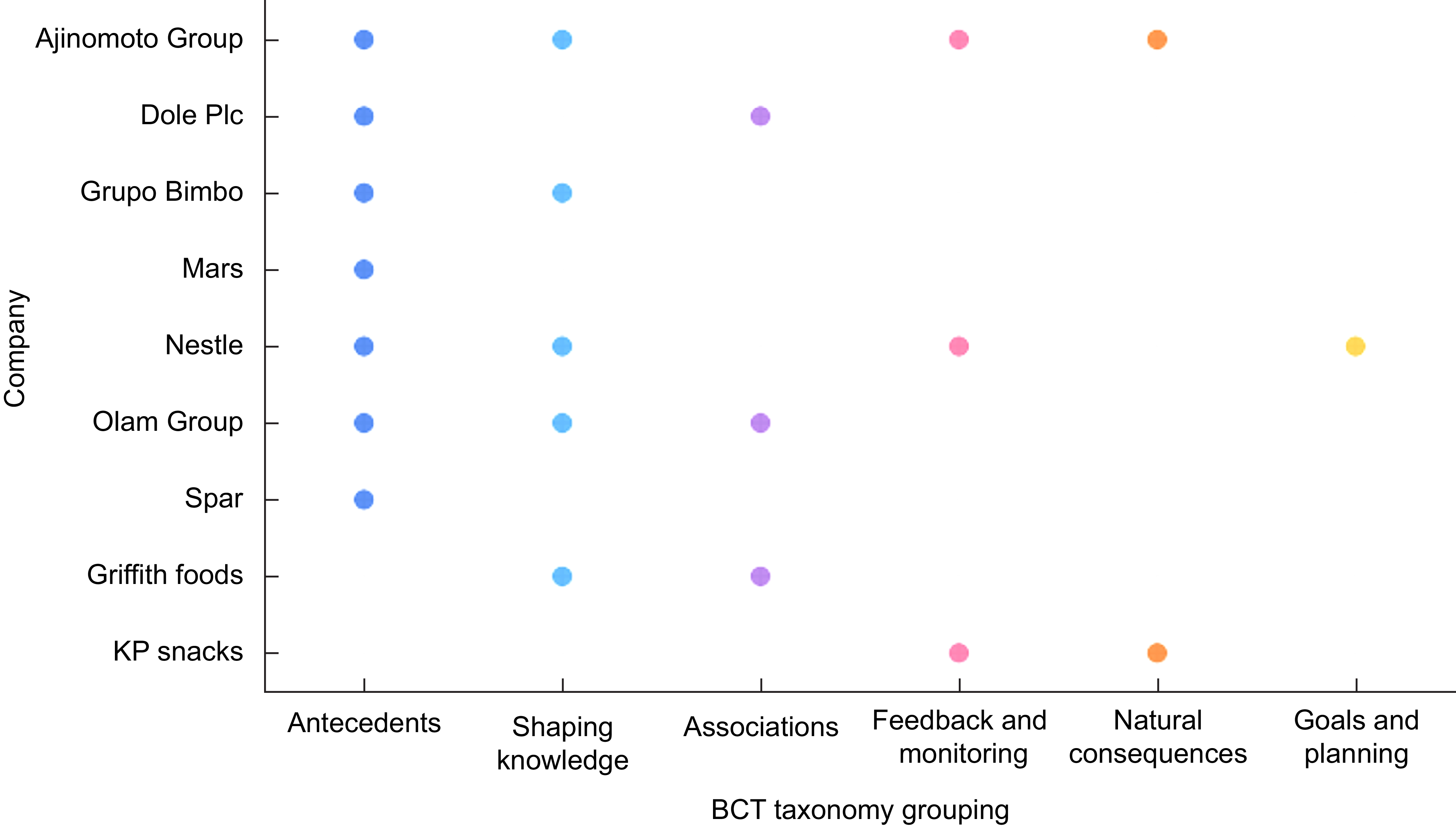
Twelve case studies met the inclusion criteria(41–48). These were predominantly conducted across company sites globally, five were focused primarily on UK and Republic of Ireland locations. Characteristics of case studies are shown in Table 3. A range of nutrition interventions were reported, and elements were mapped to seven of the sixteen BCT groups, as shown in Figure 3. Seven companies were identified as using BCT elements from Group 12 ‘Antecedents’, for example restructuring the physical food environment through healthy canteen options and vending. Five companies had elements mapped to Group 4 ‘Shaping knowledge’, including nutrition education sessions (one-one, webinars and workshops), provision of educational materials. Three companies had elements mapped to Group 2 ‘Feedback and monitoring’ e.g. health screenings, three companies from Group 7 ‘Associations’, two companies from Group 5 ‘Natural consequences’ one company from Group 1 ‘Goals and planning’. Non-nutrition intervention components were reported in all case studies, these included addiction prevention, breastfeeding support, breathing exercises, cycle to work schemes, ergonomic support, family and community events, financial and legal advice, fitness or physical activities, food hygiene advice, mental health support, physiotherapy, sleep advice, smoking cessation and provision of a smoke-free environment. None of the case studies reported the outcomes measured as part any evaluation of the programmes.
Characteristics of case studies identified

BCT, behaviour change technique taxonomy; LIC, low-income country; MIC, middle-income country; NR, not reported; WNA, Workforce Nutrition Alliance.
Mapping behaviour change techniques (BCT) to identified elements of nutrition interventions in case studies. Three studies had insufficient detail to enable mapping.

Fewer BCT were attributed to interventions reported in case studies compared with published studies (seven v. nine BCT coded), with higher frequency of physical environment modifications coded from case studies (30 % case studies v. 19 % published papers).
Industry survey
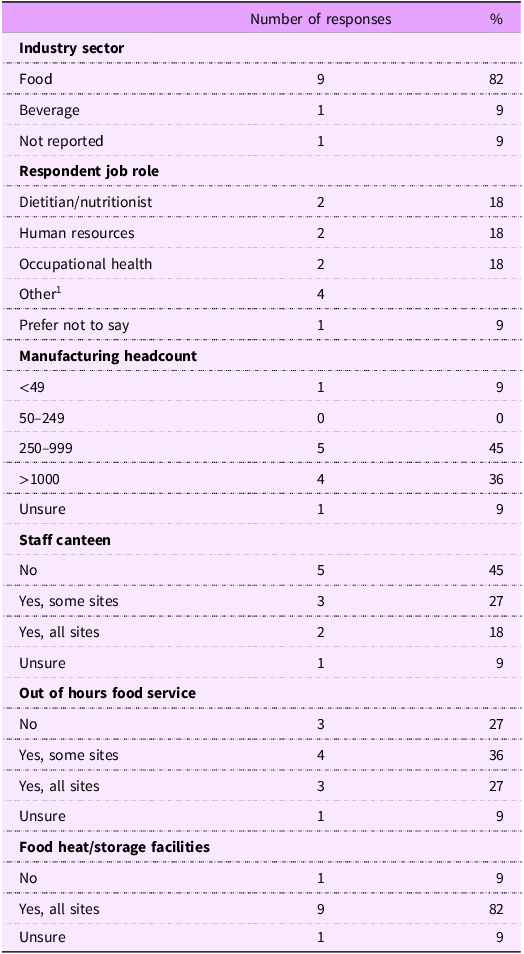
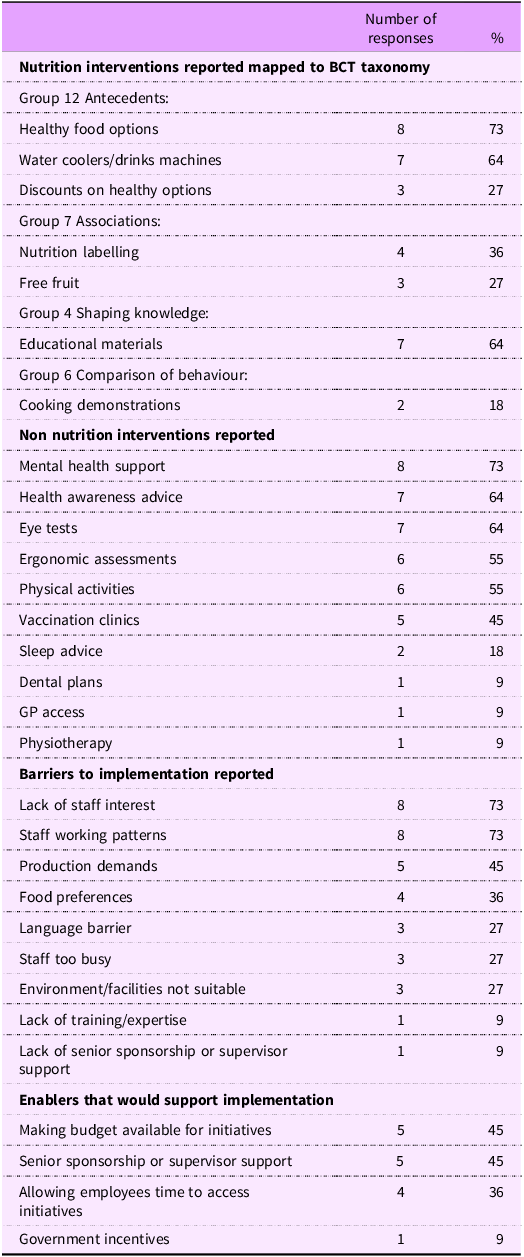
Despite a potential high survey reach, the response rate was low. In total, twenty-eight respondents started the survey, of these, 12 (43 %) completed all questions. One participant response was excluded in the final analysis due to ineligibility (not food and beverage manufacturing setting). One participant completed the survey in a paper copy format on request. Nine respondents reported working with the food manufacturing sector, one with beverage manufacturing and one did not state. Respondents included dietitians and nutritionists, human resources, occupational health, health and well-being managers, company directors, communications and business development officers. The majority (91 %) of respondents worked with large (>250 employees) sized companies, employing staff on permanent, fixed term and zero hours contracts. Five (45 %) respondents reported having no staff canteen providing hot meals at manufacturing sites, and three (27 %) made no food service provision for out of hours (weekend or night) working. Characteristics of survey respondents and settings are shown in Table 4. A range of nutrition interventions were reported, including provision of healthy cafeteria food (n 8, 73 %), educational materials (n 7, 64 %), water/drinks machines (n 7, 64 %), nutrition labelling (n 4, 36 %), free fruit deliveries (n 3, 27 %), discounts on healthier options (n 3, 27 %) and cooking demonstrations (n 2, 18 %). Non-nutrition intervention components were also reported, these included mental health support (n 8, 73 %), health awareness advice such as alcohol or smoking cessation (n 7, 64 %), eye tests (n 7, 64 %), ergonomic assessments (n 6, 55 %), fitness/physical activities (n 6, 55 %), vaccination clinics (n 5, 45 %), sleep advice (n 2, 18 %), dental plans (n 1, 9 %), remote GP access (n 1, 9 %) and physiotherapy (n 1, 9 %). Private health insurance provision was reported at five companies, although if this was offered to all staff or only those above a certain level was unclear.
Characteristics of stakeholders who responded to the UK food and drink manufacturing staff health and well-fbeing implementation survey

1 Health & Wellbeing Manager, Company Director, Communications Manager, Business Development Officer.
Identified behaviour change elements mapped to intervention function and Theoretical Domains Framework
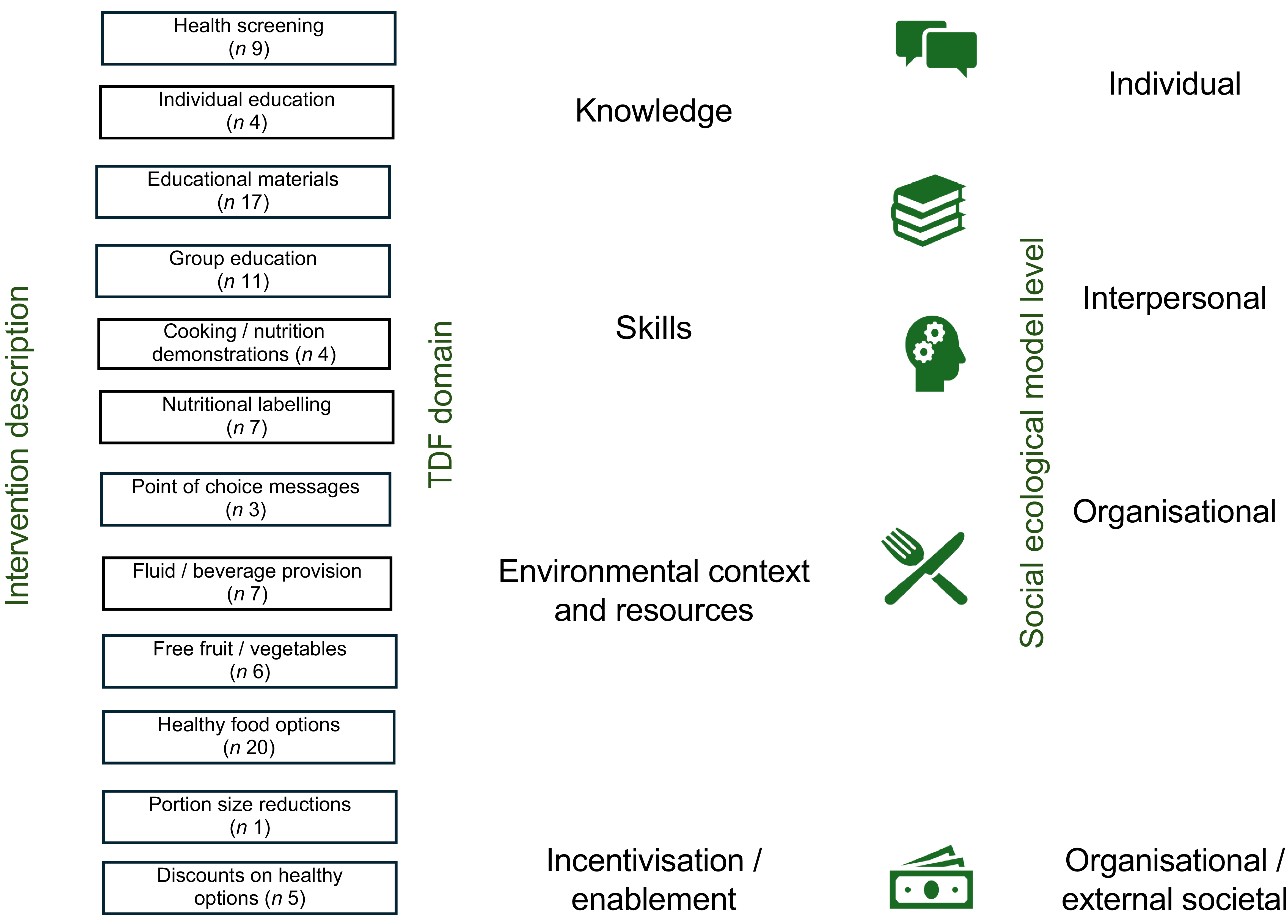
Most intervention elements identified from all data sources were focused at the individual level in the ‘knowledge’ domain – for example, health screening and individual education, as shown in Figure 4. Limited interventions were identified as being in the ‘skills’ domain; demonstrations along with group education are targeted at the ‘interpersonal’ level – as these activities are likely to occur with groups of colleagues. The second most frequent domain identified was ‘environmental context and resources’ – modifications in the food environment, for example – provision of water, fruit, vegetables and healthy choices. The only example of incentivisation was the provision of discounted healthy foods.
Summary of identified nutritional behavioural change interventions across published studies, case studies and survey respondents mapped to the theoretical domains framework and social ecological model. TDF, theoretical domains framework.

Figure 4. Long description
A diagram mapping nutritional behavioral change interventions to the theoretical domains framework and social ecological model. The diagram is divided into two main sections: Intervention description and TDF domain on the left, and Social ecological model level on the right. The Intervention description section lists various interventions such as Health screening, Individual education, Educational materials, Group education, Cooking/nutrition demonstrations, Nutritional labelling, Point of choice messages, Fluid/beverage provision, Free fruit/vegetables, Healthy food options, Portion size reductions, and Discounts on healthy options. These interventions are categorized under Knowledge, Skills, Environmental context and resources, and Incentivisation/enablement. The Social ecological model level section categorizes these interventions into Individual, Interpersonal, Organizational, and Organizational/external societal levels. Each category is represented by different icons: speech bubbles for Individual, stacked books for Interpersonal, a head with gears for Organizational, a fork and knife for Organizational, and money for Organizational/external societal.
Barriers and enablers across published studies, case studies and survey respondents
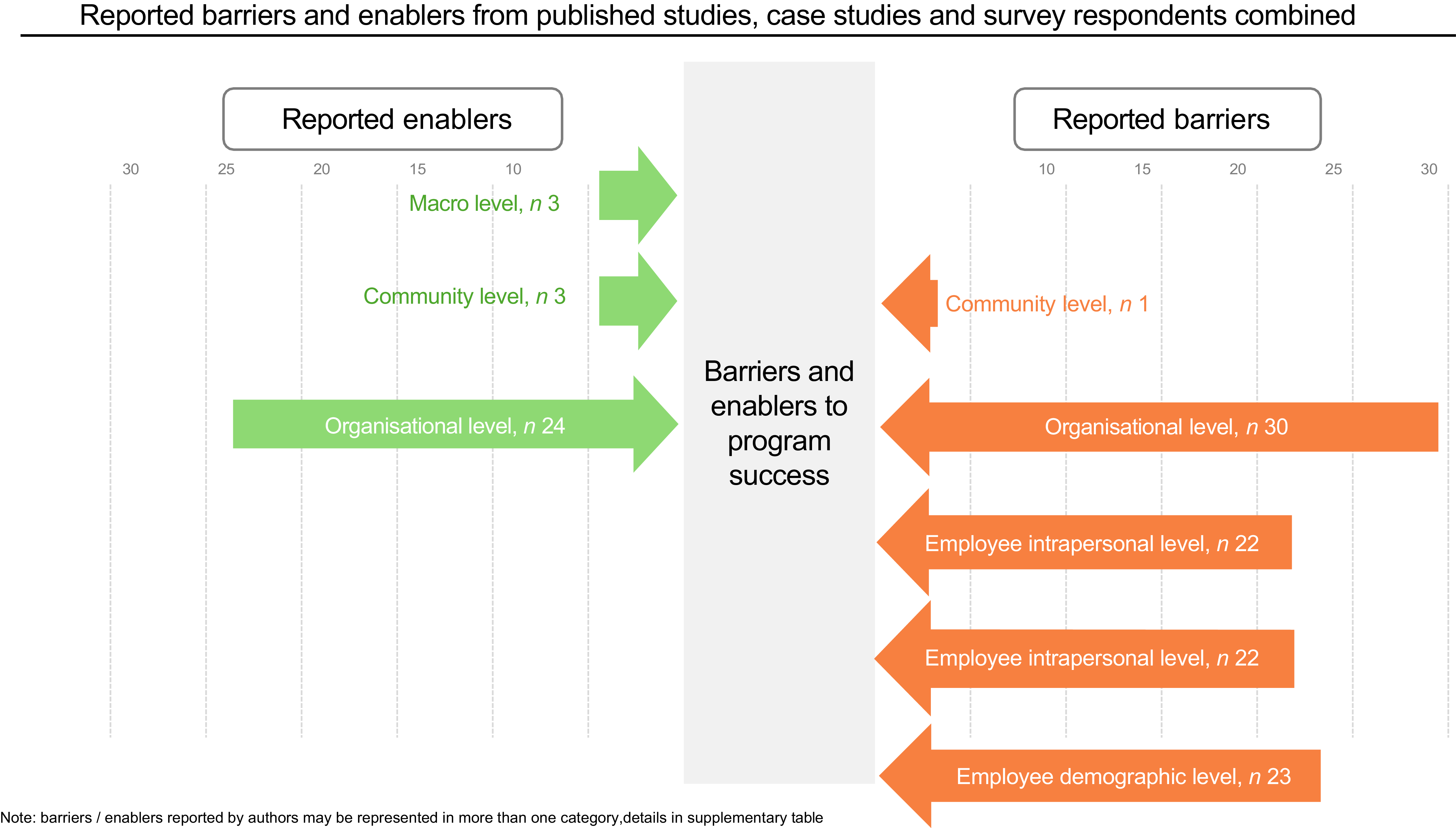
Ten published studies and four cased studies reported barriers to implementation or limitations to success. Common barriers to implementation of nutrition and well-being interventions were reported consistently across published studies, organisational case studies and survey responses. These were mapped to employee, organisational and macro-level factors drivers, as shown in Figure 5. At the employee level, low engagement, resistance to change, language barriers and food preferences were frequently cited. Published articles noted: employee resistance to change(Reference Hollands, Cartwright and Pilling24,Reference Pechey, Cartwright and Pilling25) and low employee engagement rate(Reference van Scheppingen, de Vroome and Ten Have30,Reference Backman, Gonzaga and Sugerman34,Reference Cook, Swinburn and Stewart39) – quantified in two studies as 28 % and 42 % uptake by eligible staff. The reasons noted in case studies included employee resistance to change (n 1), language barriers (n 1), global challenges adapting menus and messaging to local tastes (n 1) and turnover of occupational health staff (n 1). From interview responses, eight (73 %) respondents noted lack of staff interest and 27 % stated language barriers, Table 5. Organisational barriers included limited resources (time, space, staff or budget), unsupportive working patterns, lack of supervisor or senior management buy-in and practical constraints related to shift work or food service provision. From studies included in the scoping review, organisational-level barriers included that the programme was not available to all employees(Reference van Holland, Reneman and Soer31), lack of supervisor support(Reference van Holland, Brouwer and de Boer32), too lengthy/time consuming(Reference van Holland, Brouwer and de Boer32,Reference Roy, Styles and Braakhuis40) , reliance on self-reported information (36), lack of implementation structure and physical space constraints(Reference Roy, Styles and Braakhuis40). Production demands were noted by five (45 %) respondents to the survey, and employees being too busy (27 %), work environment/facilities not suitable (27 %), lack of training/expertise to deliver initiatives (9 %) and lack of senior-level sponsorship and supervisor support were also noted.
Reported barrier and enablers from published studies, case studies and survey respondents combined. Examples included at each level. Macro level, i.e. government incentives/legislation, community level, i.e. global challenges adapting to local tastes, links to local health provisions, organisational level, i.e. production demands, lack of senior sponsorship, employee interpersonal level, i.e. language barrier, employee resistance to change, employee intrapersonal level, i.e. food preferences, low engagement rate, employee demographic level, i.e. good health limiting scope for improvement, language barrier.

Intervention elements, barriers and enablers reported by stakeholders involved in UK workplace interventions in the food and beverage manufacturing sector

BCT, behaviour change technique.
Several enablers were also identified, including strong leadership support, employee involvement in programme design, flexible delivery models and internal capacity (e.g. in-house nutrition leads). Enabling factors stated in published studies included consultation with workers during planning stage(Reference Cook, Swinburn and Stewart39), stages of change model guided programme development and delivery(Reference Cook, Swinburn and Stewart39), not-for-profit cafeteria allowed commercial concerns to take less precedence(Reference Hollands, Cartwright and Pilling24), managers and employees enabled to make their own appropriate next steps toward health(Reference van Scheppingen, de Vroome and Ten Have30) and government legislation requiring employers to offer suitable occupational healthcare(Reference van Holland, Brouwer and de Boer32). Five case studies reported strengths or enablers to implementation including senior management support and funding (n 1), internal nutrition provider allows tailored messaging based on employee feedback (n 2), use of external resources allows for diverse perspectives and best practices (n 1), tailoring initiatives to global contexts (n 1), investment (n 1) and flexibility in providers schedule based on employee requests (n 1). From survey responses, budget available for initiatives was noted by five (45 %) as well as senior-level sponsorship and supervisor support (45 %) and allowing time for employees to access initiatives during work (36 %). Survey respondents also highlighted the potential role of external incentives such as government grants or community partnerships to improve uptake and sustainability of workplace health initiatives. Community partners and/or external support, government guidelines, supervisor training, and senior-level sponsorship were suggested as possible resources that would help to improve employee nutrition, health and well-being in the food manufacturing setting.
Discussion
Occupational health behaviours and longer‑term health outcomes are shaped by the interaction between workplace environments and wider social and structural determinants. In the UK food and beverage manufacturing sector, a workforce disproportionately employed in low‑paid roles, with a high representation of migrant workers(49) and exposure to shift work and physically demanding labour, may be particularly vulnerable to diet‑related health inequalities. Diet is a key modifiable behaviour, with diets that are low in fibre, fruit and vegetables and high in salt, sugar and saturated fat contributing significantly to morbidity and mortality in the UK population(Reference Rayner and Scarborough50). This scoping review demonstrates a limited and weakly evaluated UK evidence base for workplace nutrition interventions in manufacturing settings, with existing initiatives predominantly focused on environmental modification and education, and recurrently constrained by low employee engagement, organisational barriers and a lack of whole‑systems integration.
Health interventions in workplaces have the potential to engage with hard-to-reach population groups including ethnic minority groups and male employees. These population groups are overrepresented in manufacturing job roles that require atypical working schedules and are at the lower end of salary scales. The COVID pandemic and Brexit have made staff recruitment and retention a challenge across the UK food and beverage manufacturing sector(Reference Grimani, Aboagye and Kwak4). These roles are vital to the resilience of the UK food system. This scoping project aimed to understand current practice and the barriers and enablers to supporting the nutritional health of UK food and beverage manufacturing workers in the workplace. The results point to a lack of evaluation in UK settings with most interventions utilising knowledge enhancement and environmental cues; however, a lack of employee engagement and resistance to change were identified as the main barriers to successful implementation. Previous research has proposed reasons for poor engagement levels that may be the result of demographic, language, cultural barriers and lack of availability within working hours(Reference Fleming51). Effective behaviour change interventions should be tailored to the population and underpinned by behaviour change theory(Reference Michie, Atkins and West20). This project found that most interventions used BCT that target modification of the food environment – primarily the addition of healthier food options, often coupled with prompts and cues, that aim to ‘nudge’ individuals towards a specific behaviour. A combination of ‘nudge’ strategies in workplace food provision has been shown to improve whole grain purchasing, but not across other food categories(Reference Meeusen, van der Voorn and Berk52). However, studies tend to be short in duration; therefore, limited data exist on the sustainable dietary changes that are needed for improved health outcomes, for example, within a school setting health outcomes are anticipated after 5 years of a nutritional programme(Reference Macdiarmid, Loe and Douglas53). Within a manufacturing context, the timing of food availability is key – as many employees in the sector work outside of standard working hours. Survey results suggested that not all sites have out of hours food service provision that would limit the reach of any workplace canteen nudge strategies. Shaping knowledge – providing information through nutritional health education and promotion sessions – was a common element of interventions but rarely used in isolation. Previous studies have suggested that multi-component interventions are more likely to be effective than those addressing only one element(Reference Skivington, Matthews and Simpson14).
Behaviours around food choice and nutrition at work are influenced by several domains – interventions should target the behaviours identified as being key determinants. The identified barriers to implementation and success were similar across those reported by published articles, case studies and survey – with most citing individual staff-level barriers, e.g. employee resistance to change and lack of engagement, language barriers and individual food preferences. Future research needs to understand from an employee perspective how to develop interventions to address these barriers. Wider organisational barriers included higher management support and practical considerations such as space, capability and production demands. In terms of enablers, published sources included higher stakeholder support and recourses. Survey respondents stated that wider support was needed such as government incentives and engagement with community health partners. These observations point to the need for a whole systems approach to workforce nutritional health, integrating interventions at multiple levels across individual staff, team, organisation and policy. Rather than isolated initiatives, a whole systems approach aligns leadership, culture, environment and employee support systems to improve workforce health and organisational performance.
The purpose of a scoping review is not to determine the strength of the evidence, but to understand what has been published in this topic and the elements of interventions that have been implemented. The scoping review identified limitations of the current evidence base. There is a lack of studies conducted in a UK setting, this is important to address as the UK health system structure is different to many other countries, for example, in America where most organisations are mandated to provide health care and incentivised for health promotion. The population characteristics were poorly reported particularly ethnicity, job roles and contract type (e.g. permanent or agency staff). The setting of the intervention was not always clearly reported to determine the legibility. Other fields that were unclearly reported were the intervention lead and if other components were delivered alongside the nutrition intervention, e.g. physical activity. In addition, there was limited information regarding the health status of food manufacturing staff, this may be likely to lack of information available (e.g. would not be collected routinely in some organisations). Although the case studies provided information around interventions and programmes, they lacked outcome measures. There are several likely reasons for this including confidentiality and commercial sensitivity – this should be further explored to enable effective knowledge exchange.
Strengths and limitations
A key strength of the scoping review is the number of databases and grey literature searched and the addition of an industry survey. The scoping review followed the JBI methodology with independent reviewing and data extraction. An additional strength is the involvement of the steering committee comprising of expert stakeholders independent of the research, this ensured that the terms of reference were appropriate throughout the scoping project. The poor reporting of industry sector may mean that food and beverage manufacturing-based studies were missed due to not specifying the sector. The mapping of intervention elements to BCT is based on an element of subjectivity, and to strengthen the scoping review, the BCT were mapped independently, and disagreements resolved by the research team. The BCT mapping is based on the information reported in the published papers and case studies; some interventions may have used elements that were not reported. The industry survey was limited by the low response rate; there are several reasons that could have impacted this including sector pressures around time to complete, bias around not wanting to complete the survey unless positive interventions to report and lack of identifiable personnel who see themselves as responsible with nutritional well-being for this occupational group. This latter point may be a reason why most responses were from large organisations that are more likely to have a designated member of staff in this role. Based on our scoping review, a full systematic review is not indicated at this time due to the variability in sectors, interventions and measurements reported.
Implications and next steps
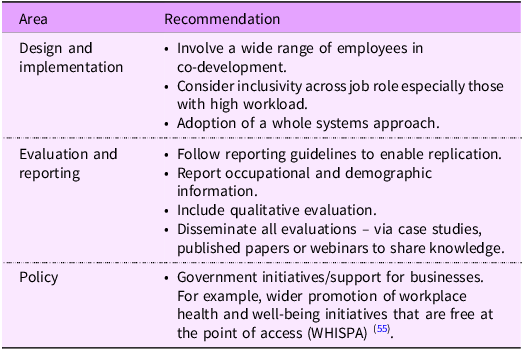
Future research in this area would benefit from fully reporting of intervention details, for example, application of Template for Intervention Description and Replication checklist,(Reference Hoffmann, Glasziou and Boutron54) this would support potential synthesis of data to fully understand intervention characteristics Table 6. While studies conducted outside of the UK can be useful, given the size of the UK food and manufacturing workforce, the paucity of studies limits UK-specific knowledge.
Supporting workplace nutrition and well-being in UK food and beverage manufacturing employees – recommendations for research and practice

The next stage of this project is to conduct a qualitative study with employees employed in the UK food manufacturing sector to understand their perceptions and view around workplace nutrition health and well-being from future research we can then consider the barriers and enablers from an employee perspective and how behavioural change techniques can be developed to support health of UK food and manufacturing employees. Given the number of studies identified in this scoping review, a full systematic review is indicated to determine the effectiveness of interventions.
Conclusion
Despite food and drink manufacturing being the largest UK manufacturing sector, the scoping review and industry survey highlight a notable lack of evaluated nutrition and well-being interventions. Those that exist predominantly focus on modifying the food environment, providing education and prompts/cues, with a limited use of a broader range of BCTs. Barriers to implementation, particularly low employee engagement, practical constraints of shift work and resource limitations, are consistently reported across evidence sources, meriting further exploration. To promote better workforce health in this sector, future research should prioritise co-development of interventions with a tailored, broader range of BCTs that are feasible and acceptable. Programmes should be evaluated across a range of metrics including levels of engagement across the whole workforce. This in turn may support investment and budget availability for sustained well-being programmes.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980026102833
Acknowledgements
The research team would like to thank the research project steering group members – Dr Kiu Sum, Lecturer in Dietetics and Human Nutrition, London Metropolitan University; Deborah David MSc RD, Registered Dietitian, Deborah David Nutrition; Amy Glass, Head of UK Diet and Health Policy, The Food and Drink Federation and Jumanah Alawfi, Lecturer, College of Applied Medical Science, Department of Clinical Nutrition, Imam Abdulrahman Bin Faisal University (IAU), Dammam, Saudi Arabia. We would also like to thank participants who took the time to answer the industry survey.
Financial support
This project is funded by a BBSRC Consumer Lab Business Interaction Voucher – 2024 in collaboration with Marlow Foods Limited.
Competing interests
R.G. hold the following unpaid roles: Research Lead, British Dietetic Association Work Ready Steering Group and Research Lead HercuWise Ltd. B.R-H. is a current employee of Marlow Foods Limited and has previously worked for United Biscuits; L.D. and H.T. were employed at Marlow Foods Limited at the time of the research design. W.H. is a Consultant for Zoe Limited.
Authorship
R.G., W.H., L.D., H.T. and E.P. derived the research question and overall study design. G.R. conducted the scoping review searches. G.R. and H.A. analysed the data from the scoping review and survey. R.G. and G.R. drafted the initial manuscript. All authors critically reviewed the manuscript and contributed to interpretation of the results. All authors reviewed the final version of the manuscript and approved for publication.
Ethical statement
This industry survey was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving research study participants were approved by the King’s College London Research Ethics Office [ref MRA-24/25-47251].



 Open access
Open access