


According to one parent report, attention-deficit hyperactivity disorder (ADHD) affects up to 11.3% of children in the USA. Reference Reuben1 Symptoms of ADHD include inattention, hyperactivity and impulsivity Reference Faraone, Bellgrove, Brikell, Cortese, Hartman and Hollis2 and result in functional challenges across multiple settings. 3 These challenges are amplified by inequities in access to diagnosis and treatment based on gender, Reference Hinshaw, Nguyen, O’Grady and Rosenthal4,Reference Kok, Groen, Fuermaier and Tucha5 race, Reference Morgan, Hillemeier, Farkas and Maczuga6–Reference Cénat, Blais-Rochette, Morse, Vandette, Noorishad and Kogan8 ethnicity Reference Morgan, Hillemeier, Farkas and Maczuga6,Reference Kamimura-Nishimura, Bush, Amaya de Lopez, Crosby, Jacquez and Modi7 and social determinants of health (SDOH). Reference Choi, Shin, Cho and Park9–Reference Torvik, Eilertsen, McAdams, Gustavson, Zachrisson and Brandlistuen13
Medication and functional outcomes
ADHD symptoms result in disruptions to the child’s functioning in multiple settings, including at home, with peers or at school. Reference Faraone, Bellgrove, Brikell, Cortese, Hartman and Hollis2 These disruptions can manifest as increased family conflict, Reference Shattell, Bartlett and Rowe14 impaired pro-social behaviour (i.e. behaviours of caring and helping) Reference Arango-Tobón, Guevara Solórzano, Orejarena Serrano and Olivera-La Rosa15 and difficulties in school. Reference Shattell, Bartlett and Rowe14 Previous studies have modelled latent trajectories of symptoms and functional outcomes in children with ADHD. Reference Bussing, Mason, Bell, Porter and Garvan16–Reference Murray, Hall, Speyer, Carter, Mirman and Caye18 In one UK cohort, Murray et al identified distinct symptom-trajectory classes across 11 years. Reference Murray, Hall, Speyer, Carter, Mirman and Caye18 In US samples, DuPaul et al modelled trajectories of inattentive and hyperactive symptoms alongside social skills and maths/reading performance over 8 years, Reference DuPaul, Morgan, Farkas, Hillemeier and Maczuga17 and Bussing et al examined long-term functional and mental health outcomes in a large cohort. Reference Bussing, Mason, Bell, Porter and Garvan16 Collectively, these studies clarify the developmental course of ADHD and identify risk factors for greater impairment. Nevertheless, updated longitudinal analyses are warranted: the US cohorts underpinning much of this literature were initiated between 1994 19 and 2003, Reference Bussing, Zima, Gary and Garvan20 and conceptualisations of ADHD and its treatments have advanced substantially since then. Reference Connolly, Glessner, Kao, Elia and Hakonarson21
Treatment of ADHD can include stimulant and/or non-stimulant medications, which are highly effective at reducing symptoms. Reference Wolraich, Hagan, Allan, Chan, Davison and Earls22 Diagnosis of ADHD early in childhood is hypothesised to result in earlier treatment (with medications or non-pharmacologic therapies), thus decreasing the risk of negative outcomes. Reference Zahmacioglu and Kilic23 Additionally, adults who received ADHD medication during their childhood have improved functional and health outcomes when compared with those who did not. Reference Shaw, Hodgkins, Caci, Young, Kahle and Woods24 Nevertheless, the impact of medication use over time throughout childhood remains understudied, and existing studies regarding the long-term effects of ADHD medication most often examine participants without prior medication use alongside those with a history of stimulant use. Reference Shaw, Hodgkins, Caci, Young, Kahle and Woods24 This approach does not consider the influence of differing patterns of medication use over time, including age at initiation, type of medication and consistency of use, which, despite the idea that earlier diagnosis and treatment of ADHD should lead to fewer adverse outcomes, have seldom been studied, except in the context of substance use disorders. Reference McCabe, Dickinson, West and Wilens25 Numerous studies have documented substantial heterogeneity in ADHD medication use over time, reflecting both barriers to initial treatment access and challenges in sustaining engagement once treatment has begun. Reported barriers to treatment access include stigma, logistical obstacles and socioeconomic disadvantage, with barriers to medication continuity including adverse effects, perceived lack of effectiveness, older child age and weaker therapeutic alliance with the prescribing clinician. Reference Kamimura-Nishimura, Brinkman, Epstein, Zhang, Altaye and Simon26,Reference Brinkman, Simon and Epstein27 Factors such as male gender, earlier follow-up and medication management, parent-perceived need for ongoing treatment, greater knowledge about medication and observable symptom improvement have been linked to greater treatment initiation and continuity. Reference Kamimura-Nishimura, Brinkman, Epstein, Zhang, Altaye and Simon26,Reference Brinkman, Sucharew, Majcher and Epstein28,Reference Brinkman, Baum, Kelleher, Peugh, Gardner and Lichtenstein29 Characterisation of these nuanced patterns of medication use within a large, contemporary cohort of children with ADHD, alongside trajectories of functional outcomes, can help identify modifiable targets for intervention, with the goal of enhanced access to earlier treatment and improved continuity and treatment engagement.
Health disparities in ADHD
Disparities in access to effective ADHD medication treatment exist regarding gender, race, ethnicity and SDOH. Females often display subtle ADHD symptoms and are underdiagnosed and undertreated compared with males. Reference Hinshaw, Nguyen, O’Grady and Rosenthal4 Children from minoritised racial and ethnic groups are less likely to obtain a diagnosis, Reference Reuben1,Reference Shi, Hunter Guevara, Dykhoff, Sangaralingham, Phelan and Zaccariello30 or to fill a prescription for ADHD medication, Reference Yang, Flores, Carson and Cook31 and their caregivers have identified discrimination as a barrier to care and family well-being. Reference Emmanuel, Knafl, Hodges, Docherty, O’Shea and Santos10 SDOH are environmental factors that can influence functioning and health outcomes, and include five representative domains: (a) economic stability, (b) education access and quality, (c) health care access and quality, (d) neighbourhood and built environment and (e) social and community context. 32 In addition, SDOH are associated with differences in ADHD prevalence, symptom burden and treatment. Reference Reuben1,Reference Choi, Shin, Cho and Park9–Reference Carroll, Klump and Burt12,Reference Nfonoyim, Griffis and Guevara33
Study aims
This observational study will be a secondary analysis of longitudinal data from the Adolescent Brain and Cognitive Development (ABCD) Study®. Reference Volkow, Koob, Croyle, Bianchi, Gordon and Koroshetz34 We will examine a diverse cohort of children living in the USA with ADHD (aged 9–10 years at study enrolment; N = 1585), and identify unique typologies based on their medication use and functional outcomes (i.e. family conflict, pro-social behaviour and school experiences) across 6 annual time points. We will use latent class growth analysis, a model-based statistical method that clusters individuals into distinct typologies based on shared trajectories of change over time (i.e. slope and intercept). Reference Woo, Jebb, Tay and Parrigon35 The advantage of this child-centred approach is that it allows for the detection of unobserved heterogeneity within the sample rather than a variable-centred approach, which can account for only clustering of trajectories based on observable characteristics (e.g. demographics). Reference Woo, Jebb, Tay and Parrigon35 This sample of US children provides ample statistical power to complete the following aims.
Aim 1
Identify typologies of children with distinct trajectories of medication use using multivariate latent class growth analysis.
Aim 2
Identify typologies of children with distinct trajectories of child-reported functional outcomes using latent class growth analysis.
Aim 3
Examine the relationships of gender, race, ethnicity, SDOH and medication use trajectory typologies with trajectories of child-reported functional outcomes using multinomial logistic regression.
Therefore, this study seeks to understand the impact of longitudinal trajectories of ADHD medication use on longitudinal trajectories of child-reported functional outcomes in a diverse group of children with ADHD, in the context of disparities based on gender, race, ethnicity and SDOH. Characterisation of typologies of children with similar trajectories of child-reported functional outcomes, along with trajectories of medication use, will identify risk factors that can inform interventions that improve access to effective ADHD treatment.
Method
Theoretical framework
The profound impact of health disparities on child well-being necessitates a holistic approach. Thus, a biopsychosocial model, as described in Fig. 1, will provide the framework to guide this study. Reference Engel36
Theoretical framework, adapted from Engel’s biopsychosocial model (Engel, 1977). ADHD, attention-deficit hyperactivity disorder; SDOH, social determinants of health.

Biological factors include the core symptoms of ADHD (i.e. inattention, hyperactivity and impulsivity), which result from neurophysiological differences in the brains of children with ADHD, as well as from the effects of ADHD medications. Reference Wolraich, Hagan, Allan, Chan, Davison and Earls22 The psychological factor includes the diagnosis of ADHD which, in this study, will be based on past and/or current parent-reported symptoms and functional impairments. Social factors include gender assigned at birth, race, ethnicity and SDOH. Although biological differences between genders may influence ADHD symptom expression, the measured variable in this study is gender assigned at birth, which is conceptualised as a social factor given that disparities in ADHD diagnosis and treatment are driven by lack of understanding surrounding ADHD presentation in female children. Specifically, ADHD is under-recognised in girls, whose presentations are often more subtle and predominantly inattentive. Reference Hinshaw, Nguyen, O’Grady and Rosenthal4 Similarly, racial and ethnic disparities reflect systemic and structural racism rather than biological differences. SDOH include income, insurance status, parental education level, neighbourhood deprivation, perceived racial and ethnic discrimination and parent partnership and employment status. Functional outcomes reflect the combined influence of biological, psychological and social factors and, in this study, include family conflict, pro-social behaviour and school experiences, which are domains commonly affected among children with ADHD.
Design
This study is a secondary analysis of data from the ABCD Study®. Participants were 9–10 years old at the time of study enrolment, and follow-up visits occurred at 1-year intervals. The most recent complete data-set is from the 5-year follow-up visit, when participants were 14–15 years old. Therefore, 6 years of data will be analysed (time points 0–5). Latent class analysis will be used, which is an advanced, innovative statistical method that accounts for unobserved heterogeneity due to individual differences, allowing for a child-centred focus. Reference Woo, Jebb, Tay and Parrigon35 This novel approach will identify typologies of children based on trajectories of medication use and child-reported functional outcomes, and distinguish important predictors of functional outcomes in a diverse cohort of children with ADHD.
Sample
The ABCD Study® is a nationwide, National Institutes of Health (NIH)-funded longitudinal cohort study on environmental and biological factors influencing neurological development and long-term outcomes for children. The study consists of 21 research sites across the USA and shares data through an open science framework. Data collected and shared and specific to this study include medical history and participant survey data. Reference Volkow, Koob, Croyle, Bianchi, Gordon and Koroshetz34
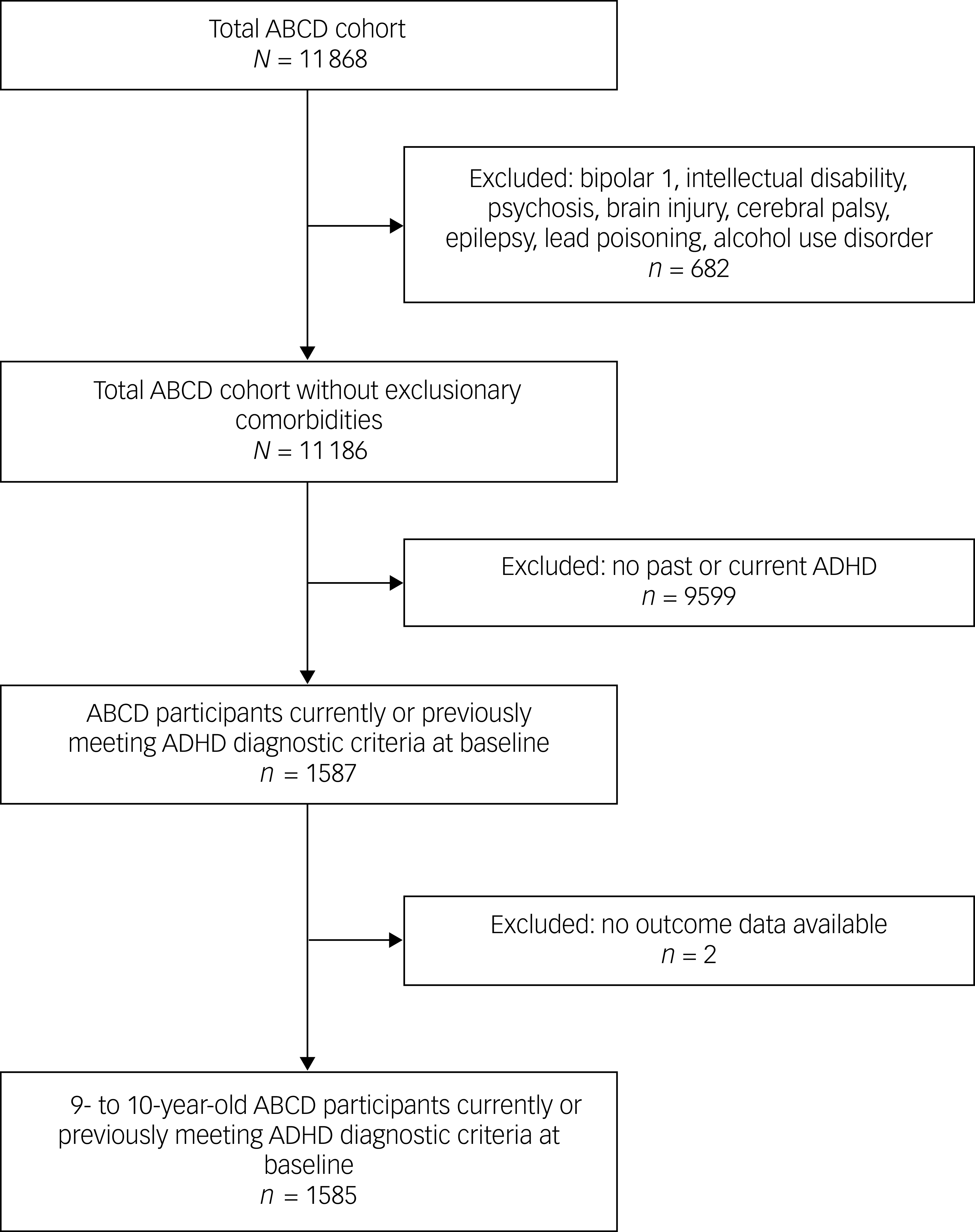
The ABCD Study® recruited 11 868 children aged 9–10 years at the time of study enrolment from selected schools, from 2016 to 2018. Reference Garavan, Bartsch, Conway, Decastro, Goldstein and Heeringa37 Parental informed consent was obtained for study participation. Reference Garavan, Bartsch, Conway, Decastro, Goldstein and Heeringa37 Children from minoritised racial and ethnic groups were recruited to ensure adequate representation of the US population, and children with signs of mental health disorders were over-sampled to provide data on mental health problems. The ABCD Study® required children to be fluent in English, attend school and be medically eligible to undergo magnetic resonance imaging (e.g. no exclusionary metal, no claustrophobia). Participants meeting DSM-5 diagnostic criteria for current or past ADHD at the initial study visit will be included in this study, and participants with serious neurological conditions or history of diagnosed mental disorders that mimic ADHD will be excluded (Fig. 2). Because ADHD is often persistent across development, and symptom expression may fluctuate over time in response to environmental demands and treatment, eligibility criteria were intentionally broad. Reference Faraone, Bellgrove, Brikell, Cortese, Hartman and Hollis2,Reference Sibley, Arnold, Swanson, Hechtman, Kennedy and Owens38,Reference Leopold, Christopher, Olson, Petrill and Willcutt39 This operationalisation is consistent with prior ABCD Study® work estimating ADHD prevalence. Reference Cordova, Antovich, Ryabinin, Neighbor, Mooney and Dieckmann40 Autism spectrum disorder was not adequately assessed in the ABCD Study® cohort, and thus children with co-occurring autism could not be excluded. Two participants were excluded due to missing outcome data. Therefore, 1585 children with ADHD were included in this study (Table 1).
Flowchart of sample selection. ABCD, Adolescent Brain and Cognitive Development Study®; ADHD, attention-deficit hyperactivity disorder.

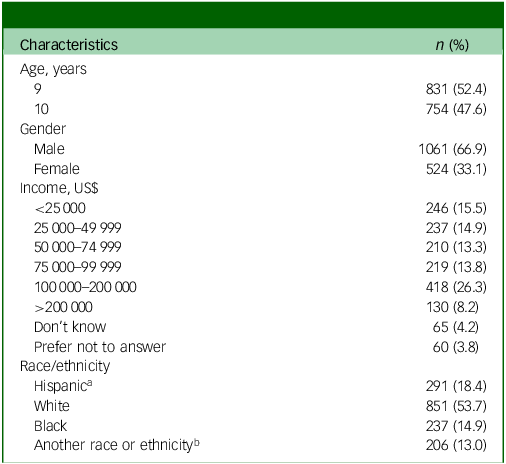
Demographic characteristics (N = 1585)

a. Puerto Rican, Dominican, Mexican, Mexican American, Chicano, Cuban, Cuban American, Central or South American, other Latin American, other Hispanic, Alaska Native, American Indian/Native American, Black, Chinese, Filipino, Vietnamese, White.
b. Alaska Native, American Indian/Native American, Native Hawaiian, Samoan, Asian Indian, Chinese, Filipino, Japanese, Korean, Pacific Islander, Vietnamese.
There is no established procedure for calculation of the required sample size for achieving desired power in latent class analysis (LCA), because LCA is evaluated based on performance measures rather than significance testing. Reference Nylund-Gibson and Choi41 Nevertheless, based on the literature, the proposed sample size (N = 1585) is sufficient to address aims 1 and 2. Reference Nylund-Gibson and Choi41 Additionally, G*power was used to conduct power analysis for aim 3, and this study is sufficiently powered to detect a small estimated effect size (odds ratio 1.2) in multinomial logistic regression. Reference Faul, Erdfelder, Lang and Buchner42
Measures
This study will use data across the first 6 annual time points of the ABCD Study® (T0–5). Time-varying measures will use data from every time point, whereas time-fixed variables will use the first time point available.
ADHD diagnosis, symptoms and comorbid internalising and externalising disorders
To set the framework for this study, the computerised Kiddie Schedule for Affective Disorders and Schizophrenia (KSADS-5) – Parent Diagnostic Interview was used to assess diagnostic criteria at baseline for ADHD sample selection (past, present or partially remitted ADHD). KSADS-5 was also used to measure covariates of inattentive symptom counts (sum of inattentive symptoms, range 0–9) and hyperactive symptom counts (sum of hyperactive symptoms, range 0–9). Notably, in this ABCD Study® data release, because KSADS-5 ADHD data are missing at time point 5, symptom counts will be assessed at times 0–4. This computerised version of KSADS-5 is self-administered, and has high agreement with the widely used clinician-administered version of the instrument (76–94% agreement across diagnostic categories). Reference Townsend, Kobak, Kearney, Milham, Andreotti and Escalera43 The Child Behavior Checklist (CBCL) will be used to covary for parent-reported internalising and externalising symptoms. CBCL is a widely used parent-report measure that assesses children’s behaviours and emotional state; it yields standardised internalising and externalising composite scores. The internalising scale is a composite of the subscales anxiety/depression (13 items), withdrawal/depression (8 items) and somatic complaints (11 items); the externalising scale is a composite of the subscales oppositional/rule-breaking (17 items) and aggressive behaviours (18 items). Reference Achenbach, Ivanova, Rescorla, Turner and Althoff44
ADHD medication use
To address aim 1, we will use the ABCD Parent Medications Survey Inventory, in which parents reported their children’s 2-week medication use history at each time point. This instrument was adapted from the Phenotypes and Exposures (PhenX) toolkit, a web-based collection of standardised measurements Reference Hamilton, Strader, Pratt, Maiese, Hendershot and Kwok45 that has been used for decades in several large studies. Reference Bild46,Reference Psaty, Lee, Savage, Rutan, German and Lyles47 Stimulant and non-stimulant medications with U.S. Food and Drug Administration approval for the treatment of ADHD were selected and coded as two binary variables (i.e. stimulant, yes/no; non-stimulant, yes/no). 48 Data from time points 0–5 will be used to characterise the latent trajectory typologies of medication use.
Functional outcomes
To address aim 2, we will use measures of child-reported functional outcomes including family conflict, pro-social behaviour and school experiences, collected at each time point. Although parent-reported outcomes are often preferred in ADHD research due to concerns about children’s inflated self-perceptions, or ‘positive illusory bias’, Reference Bourchtein, Langberg, Owens, Evans and Perera49–Reference Sibley, Pelham, Molina, Gnagy, Waschbusch and Garefino51 emerging evidence supports the validity and importance of children’s perspectives. Studies have shown that not all children with ADHD demonstrate this bias and that they contribute meaningful insights distinct from parent or teacher reports. Reference Bourchtein, Langberg, Owens, Evans and Perera49,Reference Coghill and Hodgkins52,Reference Wanni Arachchige Dona, Badloe, Sciberras, Gold, Coghill and Le53 Therefore, this study will centre the perspectives of children with ADHD, addressing a gap in a literature that has largely been informed by parent perspectives. The ABCD Youth Family Environment Scale – Family Conflict Subscale Reference Zucker, Gonzalez, Feldstein Ewing, Paulus, Arroyo and Fuligni54–Reference Gonzalez, Thompson, Sanchez, Morris, Gonzalez and Feldstein Ewing56 (9 items, range 0–9) measures the level of conflict in the home as reported by the child, with higher scores indicating higher levels of family conflict. The Strengths and Difficulties Questionnaire – Prosocial Behavior Subscale Reference Zucker, Gonzalez, Feldstein Ewing, Paulus, Arroyo and Fuligni54,Reference Gonzalez, Thompson, Sanchez, Morris, Gonzalez and Feldstein Ewing56,Reference Goodman57 (3 items, range 0–6) measures child-reported levels of pro-social behaviour (e.g. being nice, helping). The ABCD Study® team opted to retain three of the five items on this subscale with the highest factor loadings. Reference Zucker, Gonzalez, Feldstein Ewing, Paulus, Arroyo and Fuligni54 The School Risk and Protective Factors survey was derived from two instruments, the School Social Environment section of the PhenX toolkit Reference Hamilton, Strader, Pratt, Maiese, Hendershot and Kwok45 and the Communities that Care Youth Survey, Reference Arthur, Briney, Hawkins, Abbott, Brooke-Weiss and Catalano58 the latter of which measures the child’s perception of their school experience and includes three subscales: school environment (6 items, range 6–24), school involvement (4 items, range 4–16) and school disengagement (2 items, range 2–8). Reference Zucker, Gonzalez, Feldstein Ewing, Paulus, Arroyo and Fuligni54,Reference Arthur, Hawkins, Pollard, Catalano and Baglioni59 Because a total score for this scale has not previously been tested for reliability or validity, we performed factor analysis to verify a single-factor structure across the three subscales, and to create a composite score to represent school experiences (Supplementary Materials, section 9).
To represent functional outcomes broadly, we will use a standardised composite score. To create this score, all outcome variables were coded so that higher scores indicate a higher level of functioning in the respective area (i.e. lower family conflict, higher pro-social behaviour and more positive school experiences), and z-scores were then calculated to produce equally weighted measures of each functional outcome. Reference Sinha, Calfee and Delucchi60 The mean composite z-score for functional outcomes was calculated for use in the latent class growth analysis, as described in the literature. Reference Sinha, Calfee and Delucchi60,Reference Weller, Bowen and Faubert61 Data from time points 0–5 will be used to characterise latent trajectory typologies of functional outcomes.
Gender, race, ethnicity and SDOH
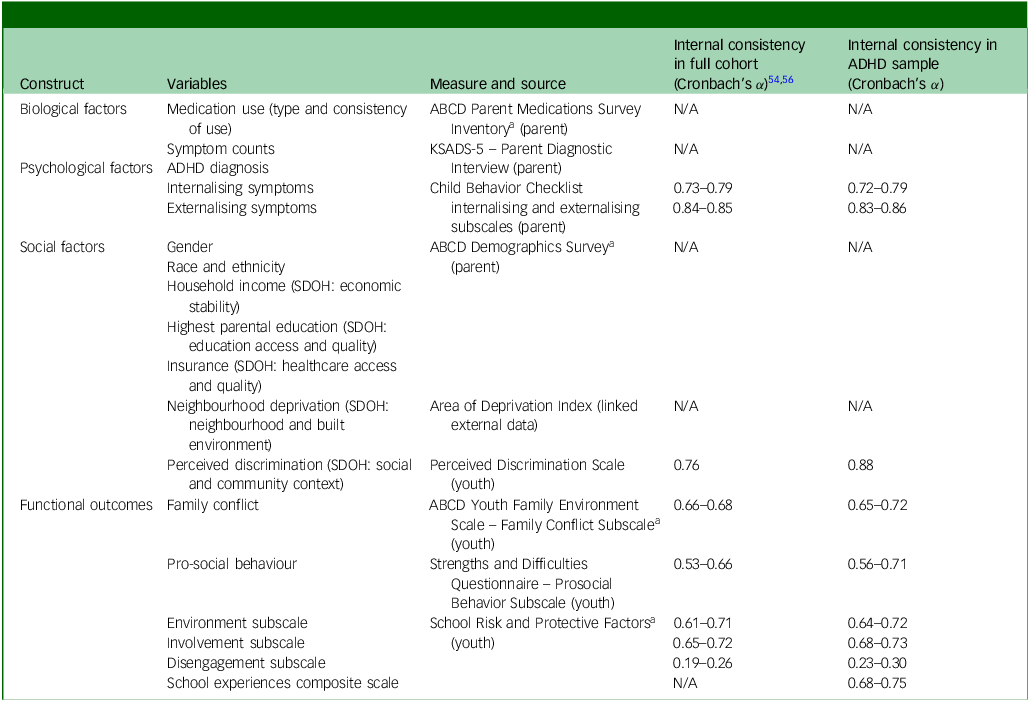
To address aim 3, baseline demographic characteristics will be used, as measured by the ABCD Demographics Survey. Additionally, five SDOH domains will include the following: (a) economic stability, (b) education access and quality, (c) health care access and quality, (d) neighbourhood and built environment and (e) social and community context. Demographic variables will include gender assigned at birth (male, female, and ethno-racial identity (White, Black, Hispanic and another race or ethnicity)). SDOH variables will include economic stability (household income (6 categories, US$25 000 increments)); education access and quality (highest parental education (5 categories, ranging from less than high school to graduate or professional degrees)); and healthcare access and quality (insurance status (private denotes employer, purchased, TRICARE or other military; public denotes Medicare, Medicaid, VA; or uninsured denotes no insurance, Indian Health Service only)). Reference Bureau62 Neighbourhood and built environment will be measured using the Area Deprivation Index (continuous sum score, range 2.6–124.6), Reference Singh63 a composite score of socioeconomic disadvantage that uses participant zip codes and census tract data and takes into consideration the education, employment, income and housing quality in a given area. Reference Kind, Jencks, Brock, Yu, Bartels and Ehlenbach64 Social and community context will use the Perceived Discrimination Scale (7 items, range 7–35), which measures experiences of racial or ethnic discrimination and has been a significant predictor of adverse outcomes in several studies using ABCD Study® data. Reference Oshri, Reck, Carter, Uddin, Geier and Beach65,Reference Karcher and Barch66 Of note, data from time point 2 will be used for insurance status and perceived discrimination, whereas all other time-fixed variables will use baseline values (time point 0). Details of each variable are described in Table 2.
Measures analysed

ADHD, attention-deficit hyperactivity disorder; N/A, not applicable; not available; KSADS-5, Kiddie Schedule for Affective Disorders and Schizophrenia; ABCD, Adolescent Brain and Cognitive Development Study®; SDOH, social determinants of health.
a. Modified from the toolkit Phenotypes and Exposures. Reference Oshri, Reck, Carter, Uddin, Geier and Beach65
Data management and preparation
Access to de-identified ABCD Study® data (release 6.0) was granted, and data-sets were downloaded on 4 August 2025 through the NIH Brain Development Cohorts Data Hub. Reference Jernigan, Brown, Dale, Tapert, Sowell and Herting67 Ongoing data use agreement and Institutional Review Board approval are in place (no. Pro00113309). The data are stored on a secure research compute cluster in compliance with NIST SP 800-171 standards for NIH controlled-access data, Reference Jernigan, Brown, Dale, Tapert, Sowell and Herting67 and are accessed only by approved study personnel. No personal identifying information is contained in these data or accessible to the authors. SAS version 9.4 for Windows (SAS Institute Inc., Cary, North Carolina, USA; https://www.sas.com) and R version 4.2.2 on a Linux-based compute environment (R Foundation for Statistical Computing, Vienna, Austria; https://www.r-project.org) will be used for data management and analysis. Descriptive statistics will be generated to examine the distribution and variability of each variable and check for missing data. Outliers representing invalid values will be identified and deleted if accounting for <5% of the data, or recoded to 4 standard deviations above or below the mean if accounting for >5% of the data. Imputation will be performed, when appropriate, for missing baseline demographic data. Maximum-likelihood estimation methods within the statistical models will account for missing longitudinal data. A detailed description of all data management activities completed to date is provided in the Supplementary Materials.
Data analysis
This study will use latent class growth analysis to characterise trajectory typologies for ADHD medication use and child-reported functional outcomes. This model-based approach considers group membership as an unobserved categorical variable based on the slope and intercept of a given individual, and trajectories within typologies are constrained to be equal. Reference Woo, Jebb, Tay and Parrigon35 Descriptive statistics will be generated to describe the sample and key variables of interest. Non-directional inferential statistical tests will be conducted with a significance level of 0.05. Effect sizes and 95% confidence intervals will be reported to address clinical significance.
Aims 1 and 2: latent class growth analyses
Multivariate latent class growth analysis will be used to identify distinct latent classes (typologies) of children with ADHD, based on similar trajectories of stimulant and non-stimulant medication use over time, with the coefficient representing the probability of either medication use at a given time point (aim 1). A separate latent class growth analysis will be used to identify distinct latent typologies of children with ADHD based on similar trajectories of functional outcomes (i.e. composite score of family conflict, pro-social behaviour and school experiences; aim 2). If correlations between functional outcomes are found to be too low to justify the use of a composite score, a multivariate latent class growth analysis will be used. Model selection will be determined by best-practice guidelines, including lower Akaike information criterion and Bayesian information criterion (BIC), with BIC being the preferred index for class enumeration due to its performance in simulation studies, as well as entropy ≥0.8 indicating clear class separation. Reference Jung and Wickrama68 Final selection of latent typologies will be determined by both optimal model fit and theory.
Because functional outcomes are highly related to symptom severity, Reference Meyer, Alaie, Ramklint and Isaksson69 functional outcome trajectories are hypothesised to reflect four previously described symptom trajectories, Reference Murray, Hall, Speyer, Carter, Mirman and Caye18 with one group sustaining positive outcomes, one sustaining negative outcomes, one improving over time and one declining over time (Fig. 3). Because the coronavirus disease (COVID-19) pandemic occurred at the time of ABCD Study® data collection and the potential confounding influence of this event on functional outcomes cannot be ignored, a variable representing COVID-19-related school disruptions was created to reflect the impact of the pandemic on children’s day-to-day lives during 2020 and 2021. Data from both the ABCD Study® annual COVID-19 questionnaire and the COVID-19 substudy included items regarding current schooling compared with January of 2020, school closures and schooling at home, which were all considered to be school disruptions (Supplementary Materials, section 8). COVID-19-related school disruptions will be treated as a covariate in the latent class growth model for functional outcomes (aim 2). Additionally, a shortage of stimulant medications occurred in the USA, beginning 12 October 2022. Sensitivity analysis showed no difference in stimulant medication use before and after this date, and therefore this will not be included in the model (aim 1).
Hypothesised functional outcome trajectories.

Aim 3: multinomial logistic regression
Multinomial logistic regression will be used to examine the relationships of gender, race, ethnicity, SDOH and medication use trajectory typologies (independent variables) with functional outcome trajectory typologies (dependent variable), controlling for symptom counts and comorbid internalising and externalising symptoms. Interactions between independent variables will be tested to detect the moderation effects of significant demographic and SDOH variables on the relationship between medication use and functional outcomes. Sensitivity analysis will be conducted using baseline ADHD type (past, present or both) and, if a significant effect is found, this will be included in the model as a covariate. Independent variables will be checked for multicollinearity. The model will be estimated using maximum-likelihood estimation; significant likelihood ratio tests, higher pseudo-R 2 and area under the receiver operating characteristic will indicate better-fitting models. The Wald χ 2 test will be used to assess individual parameter estimates, with odds ratios and 95% confidence intervals reported as effect sizes. Reference Nagelkerke70–Reference Hosmer, Lemeshow and Sturdivant72 Figure 4 details the analytic plan across all aims.
Analytic plan. SDOH, social determinants of health; ADHD, attention-deficit hyperactivity disorder.

Discussion
Due to the high prevalence and chronic nature of ADHD, and the use of medications as first-line treatment for the disorder, trajectories of medication use are an important issue in trying to better understand it. Children and adults with ADHD are vulnerable to comorbidities and poorer functional outcomes Reference Faraone, Bellgrove, Brikell, Cortese, Hartman and Hollis2 and, even when the core symptoms of ADHD have resolved, individuals still endure increased healthcare costs related to multimorbidity. Reference Du Rietz, Jangmo, Kuja-Halkola, Chang, D.’Onofrio and Ahnemark73 Although clinical practice guidelines recommend stimulant medication as first-line treatment for ADHD starting at the age of 6 years, Reference Wolraich, Hagan, Allan, Chan, Davison and Earls22 it remains unknown what the role of timing and consistency of medication use during childhood plays in the prevention of these long-term outcomes. This study will provide insight into this issue, allowing for identification of targets for intervention to improve access to ADHD diagnosis and treatment, with the goal of improving long-term outcomes. For example, if children who start medication earlier have significantly improved outcome trajectories, independent of their type and consistency of medication use, interventions should be focused on facilitating treatment access through earlier screening and diagnosis, and on parent education regarding medication initiation. Alternatively, if consistent medication use is associated with improved outcome trajectories, regardless of age at initiation, an intervention focused on treatment engagement may be more successful. Additionally, SDOH associated with functional outcomes will allow identification of those populations with the greatest need for intervention.
Strengths of this study include the use of a large sample of children from multiple sites across the USA, allowing for robust analyses using advanced statistical methods. Additionally, the longitudinal nature of this study allows us to elucidate the trajectories of ADHD medication use and functional outcomes over several years and, as data for subsequent time points become available, future work can build upon this study to further examine outcomes associated with ADHD medication use.
Although these are substantial strengths, the data available have limitations regarding ADHD treatment (e.g. parent-reported medication use represents only those medications taken in the 2 weeks prior to data collection, with no data on non-pharmacological treatment). Generalisability is also limited to that of the ABCD Study® cohort. Despite having recruited a diverse sample, participants were required to be within the catchment area of 1 of the 21 ABCD Study® sites and to be fluent in English, and thus rural and primarily Spanish-speaking youth may be underrepresented in this cohort. Reference Garavan, Bartsch, Conway, Decastro, Goldstein and Heeringa37 Another limitation is the occurrence of the COVID-19 pandemic during data collection. We covary for COVID-19-related school disruptions in aim 2, but we acknowledge that individual experiences with COVID-19 vary and that the effects cannot be fully captured in the proposed study. Importantly, sample size considerations for the statistical methods used in this study preclude us from examining differences between racial and ethnic groups beyond the broad categories included in these analyses. This does not allow us to fully capture the nuances of racial and ethnic differences in access to ADHD medication and in functional outcomes. Fortunately, the ABCD Study® provides more detailed racial and ethnic data that will allow for more comprehensive analyses in the future.
Moreover, the use of child-reported measures in ADHD research is controversial. Although we believe that this offers insight into an under-studied perspective, the possibility remains that these outcomes may be positively biased. Future investigations using ABCD Study® data would benefit from comparison between child-reported and parent- or teacher-reported outcomes, to provide greater understanding of the positive illusory bias phenomenon. Despite these limitations, this is a robust, diverse sample and a novel approach, which will allow us to address the study aims and contribute valuable insight into the practice of ADHD medication treatment.
The present study addresses critical gaps in the literature regarding trajectories of ADHD medication use and functional outcomes in relation to disparities based on gender, race, ethnicity and SDOH. For transparency and reproducibility, findings will be reported in accordance with Strengthening the Reporting of Observational Studies in Epidemiology guidelines. Reference Von Elm, Altman, Egger, Pocock, Gøtzsche and Vandenbroucke74 These findings have the potential to inform future research developing targeted, nursing-led interventions addressing inequities in access to ADHD diagnosis and treatment, thus improving functional outcomes in children with ADHD.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjo.2026.10994
Data availability
The data used in this study were obtained from the National Institutes of Health Brain Development Cohorts (NBDC) Data Hub. Access is available upon request and approval through NBDC. ABCD Study® data are available upon request at https://www.nbdc-datahub.org/.
Acknowledgements
Data from ABCD Study® data release 6.0 were obtained from the NBDC Data Hub and used in this study. This manuscript reflects the views of the authors and may not reflect the opinions or views of the NIH or the ABCD Study®.
Author contributions
M.F. conceptualised and designed the study, acquired the data, conducted the analyses and interpreted the findings. She drafted and revised the manuscript, gave final approval for the version to be published and agrees to be accountable for all aspects of this work. W.P. was involved in the conceptualisation of all statistical aspects of the study design, guided the analyses and interpretation, provided extensive revisions of the manuscript, has given final approval for the version to be published and agrees to be accountable for all aspects of this work. R.D. was involved in the conceptualisation of this study, provided important revisions as a content expert, has given final approval for the version to be published and agrees to be accountable for all aspects of this work. P.J.D. was involved in the conceptualisation of this study, provided important revisions as a content expert, has given final approval for the version to be published and agrees to be accountable for all aspects of this work. K.R.-R. guided the conceptualisation of the study, participated in data acquisition, analysis and interpretation, provided extensive revisions, has given final approval for the version to be published and agrees to be accountable for all aspects of this work.
Funding
This project is supported by the Southern Nursing Research Society (grant no. 383003166).
Declaration of interest
None.






 Open access
Open access
eLetters
No eLetters have been published for this article.