


In the last century, there has been a decrease in infectious diseases, while the increase in smoking, sedentary lifestyle and unhealthy eating habits has led to an increase in chronic diseases such as obesity, type 2 diabetes, hypertension, lipid profile changes, CVD, neurodegenerative diseases and cancer(Reference Dominguez, Di Bella and Veronese1). Although inadequate nutrition and dietary habits are risk factors for non-communicable diseases, healthy dietary habits protect against chronic diseases(Reference Di Renzo, Gualtieri and De Lorenzo2). According to the Global Burden of Disease Study-2017, dietary intake accounts for 22 % of total deaths (11 million) and 15 % of disability-adjusted life years (255 million) in adults(Reference Afshin, Sur and Fay3). Sustainable healthy dietary habits are important for the prevention of chronic diseases in the long term and for a healthy life(Reference Durmus, Gökler and Havlioglu4,Reference Maroto-Rodriguez, Ortolá and Cabanas-Sanchez5) .
Today’s global food systems make it easier to access and consume energy-dense and low-nutrient foods but also cause difficulties in reaching dietary intake recommendations(Reference Baker, Machado and Santos6). Assessing both the quality and quantity of dietary intake, including energy and nutrients, provides a more comprehensive examination of an individual’s diet(Reference Camhi, Whitney Evans and Hayman7). Validated tools such as the Healthy Eating Index (HEI), Dietary Approaches to Stop Hypertension, Dietary Inflammatory Index and Mediterranean diet are used to assess diet quality; the most widely used is the HEI(Reference Brlek and Gregorič8). The HEI, which reflects the US Department of Agriculture Food Models in determining diet quality, evaluates the quality of food independent of its quantity(Reference Guenther, Casavale and Reedy9).
Individuals’ demographic characteristics, such as age, sex, education level and nutrition-related knowledge and skills, are shaped by environmental factors and can significantly influence food choices(Reference Spronk, Kullen and Burdon10). Knowledge, skills and behaviours that enable individuals to select and consume foods that meet their body’s needs lead to healthy dietary choices(Reference Gréa Krause, Beer-Borst and Sommerhalder11). Food literacy is defined as the sum of processes, including the adequacy of food-related knowledge and skills and the stages of deciding on the food to be consumed, preparing it and consuming it(Reference Palumbo12). Vidgen and Gallegos defined food literacy as ‘the knowledge, skills and behaviours required to achieve diet quality’ and emphasised the relationship between food literacy and diet quality, which determines the degree to which dietary recommendations are met(Reference Vidgen and Gallegos13). An increase in food literacy has been associated with greater compliance with the Mediterranean diet and improved diet quality(Reference Sánchez-Sánchez, García-Vigara and Hidalgo-Mora14–Reference Uzdil, Macit Çelebi and Ertaş Öztürk16). How to prepare healthy foods, access accurate information and develop skills and knowledge about nutrition that lead to healthy food preferences are associated with higher diet quality(Reference Sklar, Radtke and Steinberg17). Furthermore, studies conducted on adolescents and adults indicate that increased knowledge of food preparation and healthy snacking practices is associated with a higher diet quality(Reference Murakami, Shinozaki and Okuhara18).
Understanding the factors that determine individuals’ food choices, eating behaviours and diet quality is important. The relationship between food literacy, different demographic characteristics and diet quality has been the subject of scientific studies in recent years(Reference Ashoori, Soltani and T-Clark19). However, most existing studies have primarily focused on specific population groups such as students(Reference Gökler, Durmuş and Havlioğlu20), healthcare workers(Reference El Sherbiny, Bellisario and Lenta21) or individuals with chronic illnesses(Reference Murakami, Shinozaki and Livingstone22), and there is limited evidence available for adults representing the general population. Furthermore, while many studies have assessed the relationship between food literacy and overall diet quality scores, very few have simultaneously examined how food literacy relates to dietary intake and diet quality index.
Therefore, this study aims to fill the existing knowledge gap by examining the relationship between food literacy, dietary intake and diet quality in adults. The study focuses on the following research questions:
RQ1: Does the level of food literacy in adults differ according to demographic characteristics?
RQ2: Do different levels of food literacy correspond to differences in dietary intake and overall diet quality?
RQ3: How is the food literacy level associated with overall diet quality and diet quality components?
The study aims to make a valuable contribution to existing literature by answering these questions and comprehensively evaluating the interaction between food literacy, nutritional behaviours and diet quality index in adults. Moreover, this study provides evidence in a Turkish adult population, thereby contributing to the limited data on food literacy and diet quality.
Materials and methods
Study design and population
This cross-sectional study was conducted among 639 adults between November 2024 and February 2025 at Ondokuz Mayıs University in Samsun, Türkiye. Before starting the study, ethical approval was obtained from the Ondokuz Mayıs University Clinical Research Ethics Committee (decision number: 2024/454, dated 30 October 2024). All procedures in this study were performed in accordance with the Declaration of Helsinki. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were used for reporting in this study. All participants were informed about the study, and informed consent was obtained.
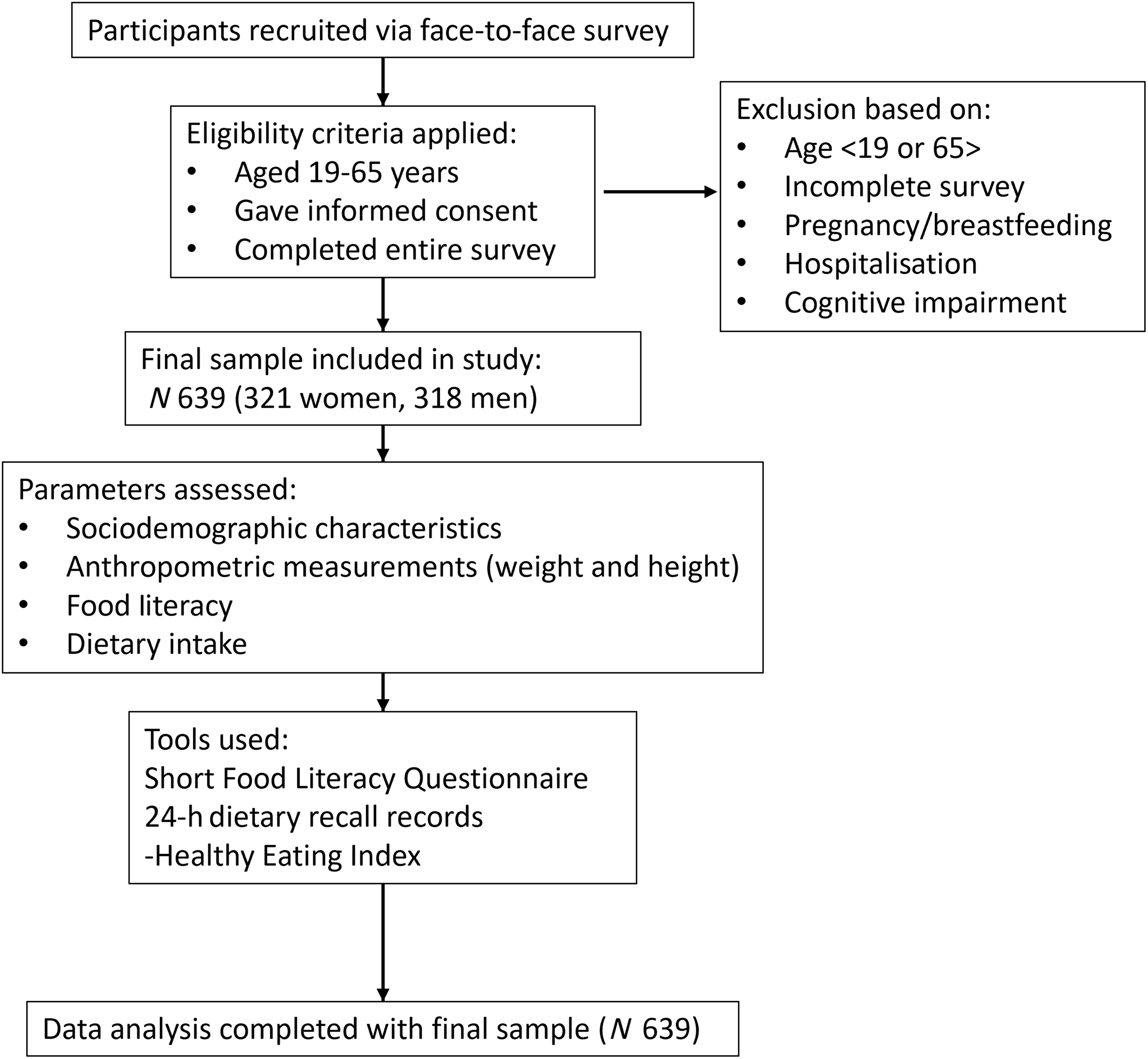
The sample size calculation was performed using the G*power programme (version 3.1) based on the study by Yiga et al. (Reference Yiga, Mokaya and Kiyimba23). A power analysis indicated that a sample of 570 individuals would be sufficient, with a 95 % confidence level and a 5 % sampling error (Power: 0·9501747 and effect size: 0·2760525). The study included 639 adults aged 19–65 years who spoke Turkish. Participants were recruited through convenience sampling of adults on the university campus and in the surrounding community. No formal advertisements were used. The exclusion criteria were pregnancy, breastfeeding, hospitalisation and cognitive impairment (Figure 1).
Participants flow chart.

Data collection
The study data were obtained through face-to-face interviews conducted using a questionnaire prepared by the researchers. This method was chosen to enhance data accuracy and ensure participants’ full understanding of the questions, particularly during the 24-h dietary recall. The questionnaire included items on demographic characteristics (sex, age, education level, employment status, marital status, residence, chronic disease and smoking status), self-reported anthropometric measurements (body weight and height), the Short Food Literacy Questionnaire and 24-h dietary recall records.
Anthropometric measurements
The height and body weight were self-reported. The BMI was calculated by dividing the body weight by the square of the height. The values obtained were evaluated according to the WHO obesity classification for adults(24).
Evaluation of food literacy
The Short Food Literacy Questionnaire (SFLQ), developed by Gréa Krause et al. (Reference Gréa Krause, Beer-Borst and Sommerhalder11), was designed to measure the food literacy levels of adults. Durmus et al. (Reference Durmus, Gökler and Havlioglu4) conducted the Turkish adaptation, validation and reliability study of the scale. The SFLQ consists of twelve items. Responses to four items on the scale (items 2, 3, 7 and 8) are scored between 0 and 5, whereas responses to the remaining items are scored between 0 and 4. The highest score on this scale is 52. Scores of less than 31 were categorised as inadequate–limited food literacy level, and scores of 31 and above were categorised as adequate–excellent food literacy level(Reference Gökler, Durmuş and Havlioğlu20). In this study, the Cronbach’s alpha coefficient for the SFLQ was 0·877.
The 24-h dietary recall records
Dietary intake was assessed by the researchers using a single 24-h dietary recall, covering all foods and beverages consumed in the previous day. Portion sizes were estimated using standard household measures and common food models. Dietary supplement intake was not assessed in this study. Dietary data obtained from this recall were analysed using the Nutrition Information System (BeBiS version 8.2, Pacific Company) to estimate the total daily intake of energy, macronutrients and micronutrients.
The Healthy Eating Index (HEI-2015)
The HEI is an index developed by the US Department of Agriculture to assess diet quality. In accordance with the methodological guidance provided for the HEI(25), person-level HEI-2015 scores were calculated to enable the examination of associations between diet quality and other study variables. Dietary components were expressed as energy-adjusted densities (e.g. intake per 1000 kcal or percentage of total energy intake), and each was scored according to HEI-2015 standards. HEI-2015 comprises thirteen components; nine of these are nutrients that should be adequately consumed in the diet (total fruit (5 points), whole fruit (5 points), total vegetables (5 points), greens and beans (5 points), whole grains (10 points), dairy products (10 points), total protein foods (5 points), seafood and plant proteins (5 points) and fatty acids (10 points)); the remaining four components are foods that should be limited (refined grains (10 points), Na (10 points), added sugars (10 points) and saturated fats (10 points)). The total score that can be obtained from the HEI varies from 0 to 100. The scores of the thirteen components were summed to obtain a total score(Reference Krebs-Smith, Pannucci and Subar26).
Statistical analysis
IBM SPSS (version 27.0; IBM Corp.) was used to analyse all data. Data normality was assessed using skewness and kurtosis tests. Descriptive values are presented as mean (sd). Categorical variables are presented as numbers (n) and percentages (%). The SFLQ scores were categorised based on the established cut-off: scores less than 31 were classified as inadequate–limited food literacy and scores of 31 and above as adequate–excellent food literacy(Reference Gökler, Durmuş and Havlioğlu20). The Independent-sample t test, used for two independent groups, and the one-way ANOVA test, used for more than two groups, were used to evaluate the differences in SFLQ scores across participant characteristics. The Independent-samples Mann–Whitney U test was used to compare HEI-2015 score, daily energy intake and macronutrient and micronutrient intake according to food literacy level. Linear regression analysis was performed to estimate the associations between SFLQ and HEI-2015. The SFLQ total score ranges from 10·8 to 52·0 points. In regression analyses, coefficients β represent the expected change in diet quality (HEI-2015 score) per 1-point increase in SFLQ. Statistical significance was set at P < 0·05.
Results
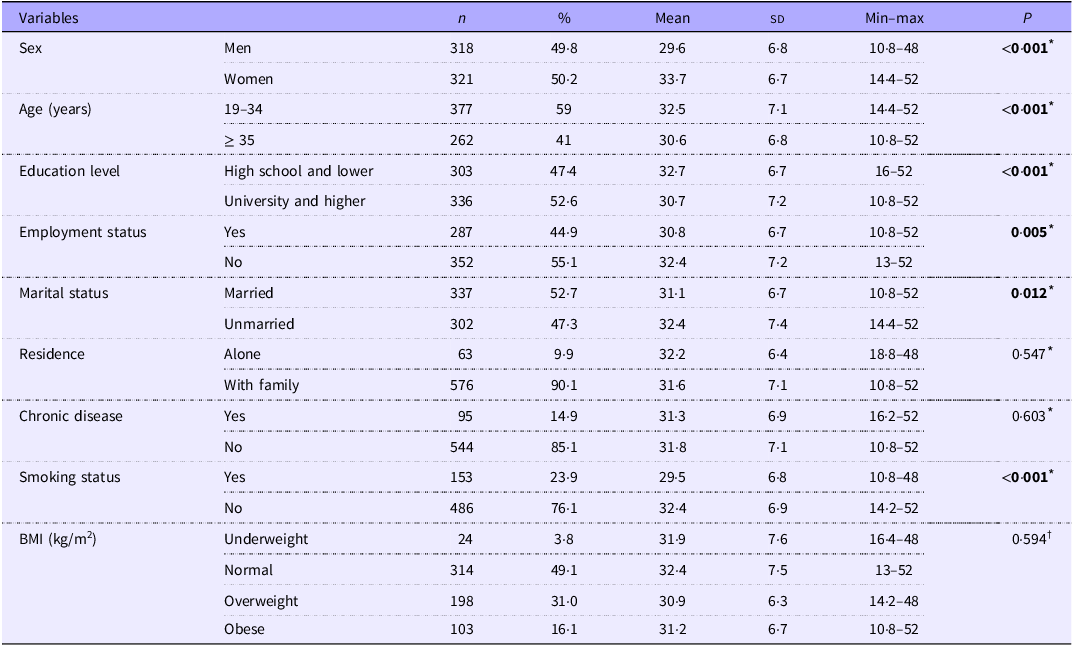
Table 1 presents the participants’ characteristics. Participants were aged 19–65 years; 49·8 % of the study sample were men (n 318), and 50·2 % were women (n 321). There were 377 participants between the ages of 19 and 34 and 262 participants aged 35 and over. While 47·4 % of the participants had a high school education or lower, 52·6 % had a university education or higher, 44·9 % of the participants were employed and 52·7 % were married. The majority of participants lived with their families (90·1 %), had no chronic diseases (85·1 %) and did not smoke (76·1 %). In terms of BMI, 31·0 % of the participants were overweight, and 16·1 % were obese. The SFLQ score was lower in men, those who were 35 years of age or older, had a university or higher level of education, were employed, were married and were smokers. In addition, the SFLQ scores were similar between the BMI groups.
Mean score of the SFLQ according to characteristics of the participants

SFLQ, Short Food Literacy Questionnaire; n, number; %, percent.
Boldface values indicate statistically significant differences (P < 0.05).
* Independent-sample t test.
† One-way ANOVA test.
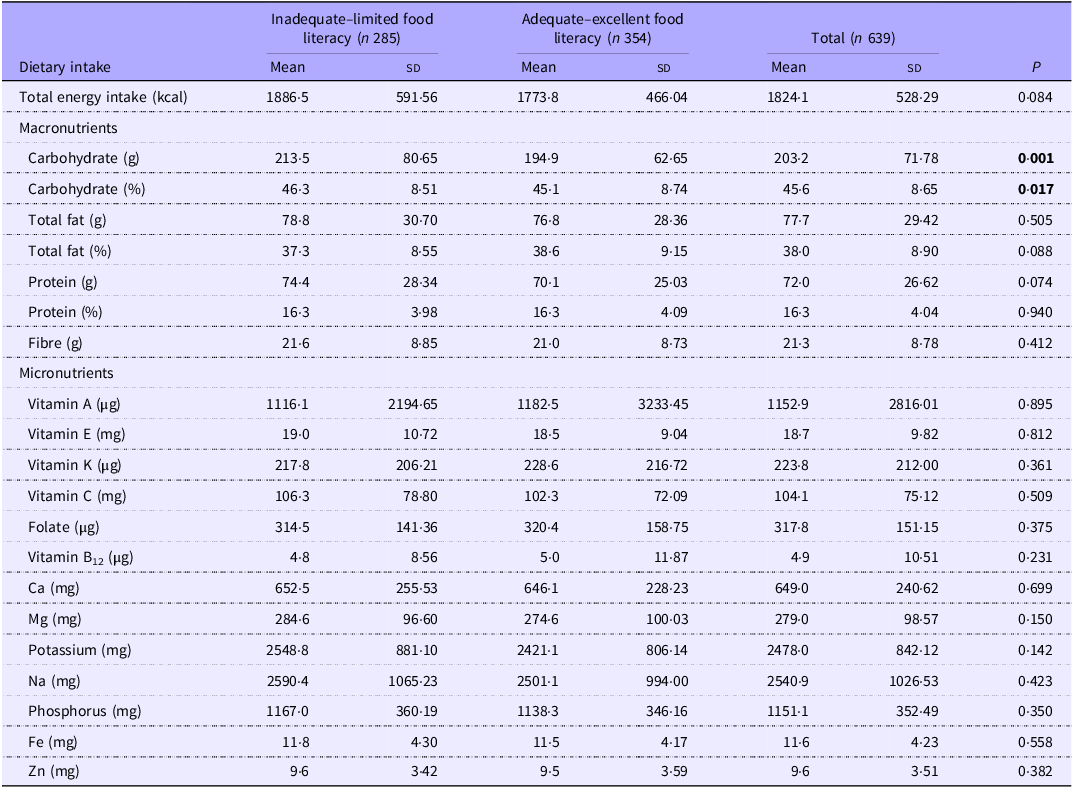
Table 2 shows the dietary energy and nutrient intakes of the participants according to their food literacy level. No differences were observed in the daily intakes of energy, fat, protein, fibre and micronutrients (vitamin A, vitamin E, vitamin K, vitamin C, folate, vitamin B12, Ca, Mg, potassium, Na, phosphorus, Fe and zinc) between participants with inadequate–limited and adequate–excellent food literacy. However, the mean daily carbohydrate intake (g) (213·5 (sd 80·65), P = 0·001) and the mean percentage of energy from carbohydrate (46·3 (sd 8·51), P = 0·017) were higher in the group with inadequate–limited food literacy.
Energy and nutrient intakes by food literacy level

Independent-samples Mann–Whitney U test.
Boldface values indicate statistically significant differences (P < 0.05).
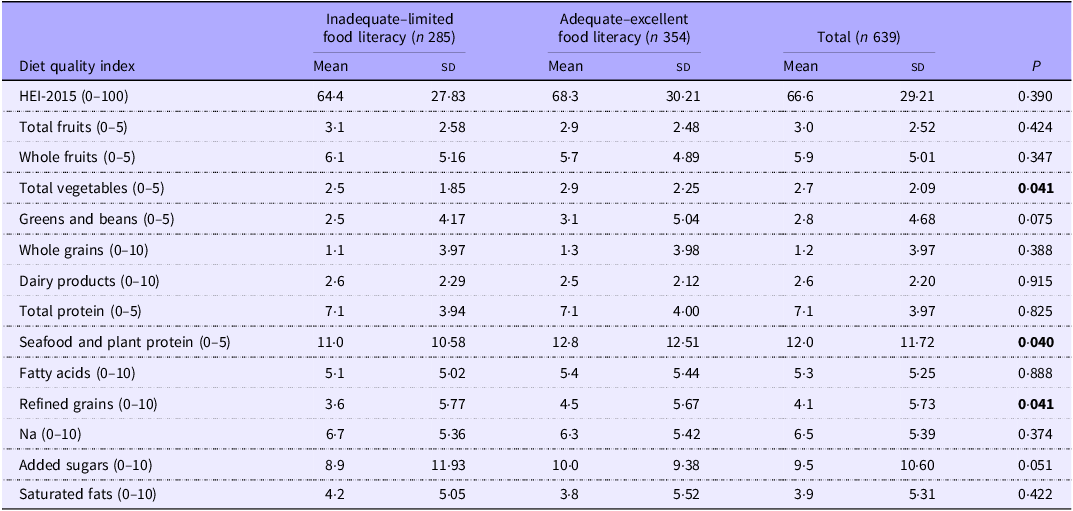
Table 3 shows differences in participants’ diet quality according to their food literacy levels. Although no difference was observed between the food literacy groups in terms of the HEI-2015 score, the total vegetable, seafood and plant protein scores were higher in the adequate–excellent food literacy group (P = 0·041 and P = 0·040, respectively). Conversely, the refined grain scores were higher in the inadequate–limited food literacy group (P = 0·041).
Diet quality index by food literacy level

HEI-2015, Healthy Eating Index-2015.
Independent-samples Mann–Whitney U test.
Boldface values indicate statistically significant differences (P < 0.05).
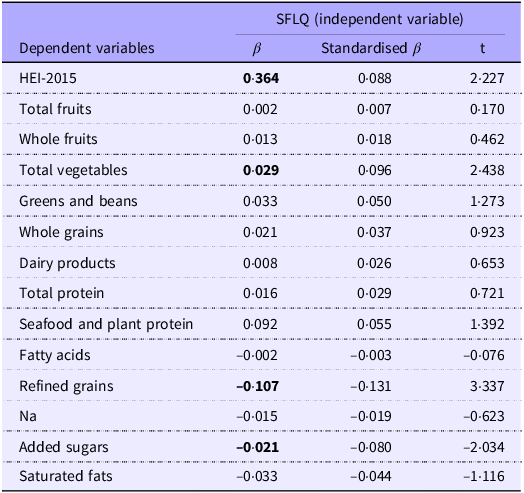
The linear regression model for HEI-2015 is presented in Table 4. The results of the analysis showed that SFLQ scores were positively associated with HEI-2015 scores (β = 0·364, P = 0·026) and total vegetable consumption scores (β = 0·029, P = 0·015). For each 1-point increase in the SFLQ score, the HEI-2015 score increased by 0·364 points on average (β = 0·364, P = 0·026). A negative association was found between the SFLQ score and both refined grain (β = −0·107, P = 0·001) and added sugar (β = −0·021, P = 0·042) scores.
Linear regression for diet quality

SFLQ, Short Food Literacy Questionnaire; HEI-2015, Healthy Eating Index-2015.
Boldface values indicate statistically significant differences (P < 0·05).
Discussion
The present study revealed that food literacy differs according to the following sociodemographic characteristics: sex (higher among women), age (higher among the 19–34 age group than among those aged 35 and older), education level (higher among those with a high school education or lower than among those with a university education or higher), employment status (higher among unemployed individuals), marital status (higher among unmarried individuals) and smoking status (higher among non-smokers). In this study, the macronutrient and micronutrient intakes of individuals were investigated according to their food literacy levels; a difference was found only for carbohydrate intake (% and g). Specifically, those with an inadequate–limited food literacy group had higher amounts of daily carbohydrate intake and a higher percentage of energy from daily carbohydrates than those with an adequate–excellent food literacy group. Although statistically significant, the magnitude of this difference was relatively modest, suggesting a limited practical impact on the overall macronutrient distribution. When the HEI food groups were evaluated, the total vegetable, seafood and plant protein scores were higher in the adequate–excellent food literacy group. The food literacy scores were positively associated with HEI-2015 and with total vegetable consumption scores in regression models. Food literacy scores were negatively associated with refined grain and added sugar intake scores. Importantly, the effect size observed in the regression analysis (β = 0·364 for HEI-2015) indicates that each unit increase in food literacy is associated with a small but meaningful improvement in overall diet quality, suggesting that even incremental gains in food literacy may translate into measurable dietary improvements.
Many studies conducted in adults have reported that food and nutrition literacy is higher in women than in men(Reference Michou, Panagiotakos and Lionis27–Reference Zhixue, Ying and Zheng30). The present study confirmed these findings, reporting higher food literacy levels among women. This result can be considered an inevitable outcome of women’s social roles, as they are often responsible for tasks related to family nutrition, such as grocery shopping and cooking(Reference da Silva Oliveira, de Morais Sato and Arceño31,Reference Kozan Cikirikci and Esin32) . Although obesity rates are generally higher among women, they tend to experience greater body image dissatisfaction and a stronger desire to be thinner. Previous research suggests that food literacy may be associated with lower body-related concerns among women(Reference Arslan, Ayyıldız and Esin33). Therefore, women’s higher food literacy may partly reflect their efforts to manage or improve body-related issues.
According to this study, age appears to be another sociodemographic factor that may influence food literacy. In the present sample, participants aged 19–35 years had higher food literacy scores than those aged 36 years and above. Although the age range of the participants in this study did not include older adults, the grouping was based on the median age of the sample. Similar findings have been reported in previous studies. Studies from different populations similarly indicate that younger adults tend to have higher food literacy levels(Reference Michou, Panagiotakos and Lionis27,Reference Murakami, Shinozaki and Yuan28) . Greater exposure of younger individuals to topics related to healthy eating, diet and body weight concerns through traditional and social media may contribute to their higher levels of nutrition-related knowledge and skills(Reference Eşer Durmaz, Keser and Tunçer34–Reference Luo, Maafs-Rodríguez and Hatfield36).
The fact that nutrition-related diseases, such as obesity and other non-communicable conditions, have become significant global health problems with rapidly increasing prevalence in recent years(Reference Chooi, Ding and Magkos37) may be related to increased interest in food and nutrition literacy. This has spurred young individuals’ desire to increase their knowledge and understand the relationship between these diseases and nutrition. In a study conducted on adults in Iran, contrary to the results of the present study, it was reported that food literacy increased with age(Reference Moshtagh, Daneshvar and Ghaedamini Harouni38). Differences in the determinants of food literacy across populations may explain the variation in the relationship between age and food literacy. Investigating these determinants in each population will help identify target groups for food literacy interventions. Contrary to previous studies conducted by Banna et al. (Reference Banna, Hamiduzzaman and Kundu39), Martin et al. (Reference Martin, Wallace and Jacob40), Zhixue et al. (Reference Zhixue, Ying and Zheng30) and Moshtagh et al. (Reference Moshtagh, Daneshvar and Ghaedamini Harouni38), food literacy was found to be higher in those with lower levels of education in the study. Including basic education on health and nutrition in academic curricula or providing opportunities for university students to improve their health and nutrition may reverse this result. Another variable in which food literacy varies is employment status, as it is reported to be higher among those who are employed. Considering the higher food literacy levels among those with a high school education or lower, the high food literacy observed in unemployed individuals may reflect the characteristics of the study sample. This study found that food literacy was higher in unmarried individuals than in married individuals, which is inconsistent with the results of similar studies(Reference Zhixue, Ying and Zheng30,Reference Moshtagh, Daneshvar and Ghaedamini Harouni38) . Considering the increased responsibility for nutrition in the family environment, especially when children are involved, it was suggested that married individuals may be more inclined to improve their food knowledge and skills than single individuals. However, the finding that food literacy was higher among younger individuals in this study is consistent with its own results, considering that the likelihood of being married at these ages is also low. It is generally expected that individuals with greater health awareness are less likely to engage in behaviours harmful to health. Previous research has shown that smoking rates are lower among individuals with higher health literacy(Reference Tao, Xu and Zhu41). Similarly, the present study observed higher food literacy levels among non-smokers, consistent with previous findings.
In the present study, we investigated the associations between food literacy and food consumption and between food literacy adequacy and total energy, macronutrients and some micronutrients. Unlike a similar study conducted among Japanese university students, which showed a positive correlation between healthy eating literacy levels and energy intake(Reference Kawasaki, Akamatsu and Fujiwara42), this study did not show a difference in energy intake between food literacy groups. This difference may stem from cultural dietary habits, food access and measurement methods.
When we evaluated the percentage of macronutrients according to the Türkiye Dietary Guidelines and their food literacy levels, the percentage of protein intake (16 % in both groups) was within the recommended limits (10–20 %)(43). No difference was observed between the groups. A previous study in female university students reported a positive correlation between healthy eating literacy and protein intake (as a % of energy)(Reference Kawasaki, Akamatsu and Fujiwara42), in contrast to the present study. In another study conducted on Turkish adolescents, the percentage of total energy from protein was higher in those with high nutrition literacy than in those with low and moderate nutrition literacy(Reference Yurtdas Depboylu, Kaner and Suer44). The present study demonstrated that fat intake percentages (36 % in the inadequate–limited group and 38 % in the adequate–excellent group) were higher than the recommended limits (20–35 %)(43) and did not differ between the groups, replicating the results of previous studies(Reference Kawasaki, Akamatsu and Fujiwara42,Reference Yurtdas Depboylu, Kaner and Suer44) . However, carbohydrate intake percentages (47 % in the inadequate–limited group and 46 % in the adequate–excellent group) were within the recommended limits (45–60 %)(43). However, there was still a difference between the groups, which is contrary to the results of previous studies(Reference Kawasaki, Akamatsu and Fujiwara42,Reference Yurtdas Depboylu, Kaner and Suer44) . Although making a recommendation is inappropriate because the type of carbohydrates was not specified in the present study, it may be inferred that the percentage of energy derived from carbohydrates is positively associated with food literacy within the recommended intake limits.
In this study, micronutrient intake was compared between individuals with inadequate–limited and adequate–excellent levels of food literacy. No differences were observed between the groups. The lack of significant differences in micronutrient intake, despite improvements in certain diet quality components, may indicate that changes in food literacy are insufficient to influence micronutrient adequacy or that food choices affecting micronutrient intake are more context-dependent and influenced by availability and cultural dietary habits. According to the Turkish Dietary Guidelines, intakes of vitamins A, E and K were adequate in both groups, whereas intakes of vitamin C, vitamin B12, folate, Ca, Mg and potassium were insufficient. Fe and Zn intakes were at borderline levels(43). Previous studies in different populations have reported positive associations between food literacy and micronutrient intake(Reference Ashoori, Soltani and T-Clark19,Reference Kawasaki, Akamatsu and Fujiwara42,Reference Yurtdas Depboylu, Kaner and Suer44,Reference Tacon45) . Although the association between food literacy and overall diet quality is well known(Reference Murakami, Shinozaki and Yuan28,Reference Doustmohammadian, Omidvar and Keshavarz-Mohammadi46) , further studies are needed to evaluate its effect on macronutrient and micronutrient levels.
In the present study, we found that total vegetable, seafood and plant protein component scores of HEI-2015 were higher in the adequate–excellent food literacy group. Furthermore, the refined grain scores were higher in the inadequate–limited food literacy group. Regression analysis revealed that food literacy scores were positively associated with the HEI-2015 scores and total vegetable consumption scores in both crude and adjusted models. Refined grain and added sugar scores of HEI-2015 were negatively associated with food literacy. However, the absence of a significant association between food literacy and the total HEI-2015 score in group comparisons, despite significant associations in regression models and specific subcomponents, suggests that food literacy may influence particular aspects of diet quality rather than uniformly across the overall index. This discordance may be explained by the composite structure of HEI-2015, in which improvements in some components (e.g. vegetables) may be offset by non-significant changes in others. Additionally, variability in dietary patterns and measurement sensitivity of different indices may contribute to these mixed findings. Food literacy is a concept considered a subset of health literacy that is essential for the development and maintenance of healthy eating habits(Reference Yuen, Thomson and Gardiner47). Previous studies consistently show that higher food literacy is associated with better diet quality, including higher consumption of fruits, vegetables and healthier dietary patterns(Reference Poelman, Dijkstra and Sponselee48–Reference Lee, Park and Kim50). Higher food literacy is also associated with increased Mediterranean diet assessment tool scores(Reference Uzdil, Macit Çelebi and Ertaş Öztürk16). In addition, food literacy was positively associated with healthy and sustainable nutrition scores and factor scores(Reference Ertas Öztürk, Kabalı and Acar51).
Our findings underscore the importance of increasing food literacy among adults by demonstrating a positive association between diet quality and food literacy levels. This association may be related to various components of food literacy. These components focus on skills and behaviours, food/health choices, culture, knowledge, emotions and food systems(Reference Truman, Lane and Elliott52). In a study, food and nutrition knowledge, food skills and resilience were positively associated with healthy eating habits(Reference Lee, Kim and Jung53). Similarly, in a nationwide cross-sectional study in Japan, 2231 adults aged 19–80 years were assessed for food literacy, food choices and diet quality. The food choice values of health/weight control, nutrition knowledge and cooking skills were positively associated, and food fussiness was negatively associated with HEI-2015(Reference Murakami, Shinozaki and Livingstone54). Furthermore, in a cross-sectional study of 5998 adults in Japan, Murakami et al. showed a positive relationship between subjective food literacy and the diet quality index (HEI-2015). Each 1-point increase in subjective food literacy increased the HEI-2015 score by 4·8 points for general diet, 6·2 points for breakfast, 4·6 points for lunch and 3·6 points for dinner. In particular, subjective food literacy subscales, such as meal preparation skills, healthy snacking habits and healthy budgeting, were found to be associated with diet quality at all meals(Reference Murakami, Shinozaki and Okuhara18). The significance of food and nutrition literacy lies in its capacity to foster healthy eating behaviours and alleviate chronic illnesses, such as obesity, diabetes and CVD. Improving individuals’ capacity to make informed dietary choices can lower the prevalence of certain conditions and enhance overall health outcomes. It is crucial to enhance the knowledge of how food literacy affects the diet and plan further educational programmes and policies accordingly(Reference Silva55). However, nutrition education focuses only on nutrition knowledge, ignoring the positive development of attitudes towards food and nutrition, which may be insufficient to provide adequate dietary behaviour(Reference Jezewska-Zychowicz and Plichta56). In this study, the positive association between food literacy and diet quality underscores its significance since food literacy encompasses multiple components.
Given the cross-sectional design, the findings should be interpreted as associations rather than causal relationships. Future studies using longitudinal or experimental designs may help clarify the nature and direction of these associations. Another limitation is that dietary intake data were collected using a single 24-h dietary recall, which may not fully capture the habitual intake. Although 24-h dietary recalls are generally considered to reflect usual intake at the group level, a more relevant limitation is the potential for residual systematic error (bias) inherent in self-reported dietary assessment methods. In addition, BMI was calculated using self-reported height and weight, which may have introduced a reporting bias. The study sample was recruited using convenience sampling from a university-based setting within a single region. This may limit the representativeness of the sample and the generalisability of the findings. Although various food literacy assessment tools exist(Reference Yuen, Thomson and Gardiner47), the SFLQ was used, focusing on skills and abilities for healthy food choices(Reference Durmus, Gökler and Havlioglu4,Reference Gréa Krause, Beer-Borst and Sommerhalder11) ; however, subfactor analysis could not be performed because the SFLQ consists of a single factor. Despite these limitations, this study provides valuable insights into the interactions between food literacy, food consumption and diet quality in Turkish adults.
Conclusion
This study contributes to the existing literature by showing the variation in food literacy within this sample of Turkish adults according to different sociodemographic characteristics. In addition, this study identified differences in energy and nutrient intakes according to food literacy adequacy levels. Accordingly, carbohydrate intake was lower among those with better food literacy. In addition to its association with sociodemographic and dietary intakes, food literacy was associated with better diet quality including increased total vegetable intake and decreased intake of refined grains and added sugars. Enhancing nutrition knowledge, skills and attitudes related to food literacy may contribute to improved diet-related outcomes. Further studies with larger sample sizes are warranted.
Acknowledgements
N/A
The authors did not receive support from any organisation for the submitted work.
G. Ü, Y. E. Ö. and Z. U. designed the study. S. K., G. Ü., Y. E. Ö., Z. U. and Y. A. K. contributed to data acquisition. S. K. contributed to data analysis and interpretation. S. K. performed the statistical analysis. S. K., G. Ü., Y. E. Ö., Z. U. and Y. A. K. contributed to drafting and revising the manuscript critically for important intellectual content of the manuscript together. All authors read and approved the final manuscript.
The authors declare no conflicts of interest.
During the preparation of this manuscript, the authors used AI-assisted language editing tools, including DeepL, Paperpal Preflight and PoolText, solely for the purpose of improving grammar, clarity and readability. The authors take full responsibility for the content of the manuscript and confirm that all scientific ideas, interpretations and conclusions are their own.

 Open access
Open access