


Introduction
Mental disorder is one of the strongest suicide risk factors [Reference Ongeri, Theuri, Nyawira, Penninx, Tijdink and Kariuki1–Reference Fu, Qian, Jin, Yu, Wu and Du9] and registry-based studies leveraging healthcare data can identify those mental disorders most strongly associated with suicide [Reference Too, Spittal, Bugeja, Reifels, Butterworth and Pirkis10]. Studies from Denmark [Reference Plana-Ripoll, Pedersen, Agerbo, Holtz, Erlangsen and Canudas-Romo3], Sweden [Reference Holmstrand, Bogren, Mattisson and Brådvik11], and Taiwan [Reference Pan, Yeh, Chan and Chang12] found relative risks 9.5–14.3 and absolute risks 6.3–6.9% for schizophrenia, mood, and substance use disorders. Existing research often focused on severe disorders such as schizophrenia or bipolar disorder [Reference Melo, Dippenaar, Johnson, Weaver, de Assis Acurcio and Malta13–Reference Jayatilleke, Hayes, Dutta, Shetty, Hotopf and Chang15], a narrow subset of mental disorders [Reference Pan, Yeh, Chan and Chang12, Reference Jayatilleke, Hayes, Dutta, Shetty, Hotopf and Chang15–Reference Olaya, Moneta, Plana-Ripoll and Haro17], or broad diagnostic categories [Reference Plana-Ripoll, Pedersen, Agerbo, Holtz, Erlangsen and Canudas-Romo3]. They often rely on inpatient data, excluding milder cases treated in outpatient or primary care settings [Reference Melo, Dippenaar, Johnson, Weaver, de Assis Acurcio and Malta13, Reference Nordentoft, Wahlbeck, Hällgren, Westman, Osby and Alinaghizadeh14, Reference Thiruvalluru, Edgcomb, Brooks and Pathak18], potentially overestimating risk [Reference Ongeri, Theuri, Nyawira, Penninx, Tijdink and Kariuki1, Reference Hubers, Moaddine, Peersmann, Stijnen, van Duijn and van der Mast19]. A critical limitation is the scarcity of studies that also include non-lethal intentional self-harm (NLISH) as primary outcome [Reference Chai, Luo, Wong, Tang, Lam and Wong20, Reference Hawton, Saunders, Topiwala and Haw21]. NLISH is highly associated with personality disorders, especially borderline personality disorder (BPD) [Reference Ose, Tveit and Mehlum22], and functions as an important warning sign for future suicide. Another gap is limited research on population-level impact of mental disorders on self-harm [Reference Hung, Liao, Chang, Chang, Yang and Chien23, Reference Mortensen, Agerbo, Erikson, Qin and Westergaard-Nielsen24]. While conventional measures of association (e.g., hazard ratios [HRs]) describe relative differences in individual-level risk, complementary population-weighted summaries (e.g., population attributable fractions [PAFs]) that jointly consider disorder prevalence and individual-level association strength may better contextualize the representation of specific mental disorders within the population distribution of non-lethal and lethal self-harm for surveillance, service planning, and suicide prevention policy.
We conducted a population-based retrospective cohort study representative of the general population of Catalonia (Spain) to examine sex- and age-specific individual- and population-level associations of mental disorders with subsequent NLISH and suicide. We included 32 mental disorders, encompassing both broad diagnostic groups and more specific disorders typically classified within broader categories.
Methods
Study population and cohort sampling design
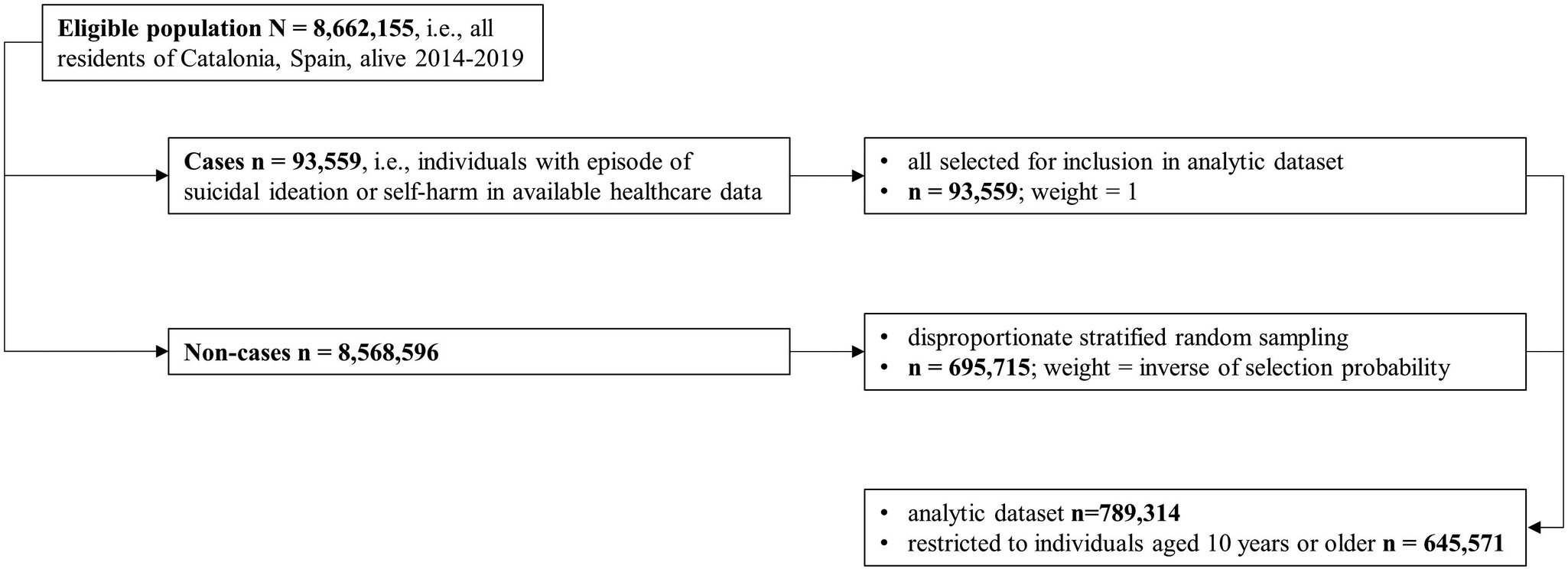
We used the Catalan Health Service’s central population register to identify all residents of Catalonia (Spain) who were alive at any point between January 1, 2014 and December 31, 2019 (n = 8,662,155). A random stratified sampling design disproportionately sampling for outcome and exposure status (enrichment), similar in principle to a case-cohort design [Reference Wimberley, Plana-Ripoll, Pedersen, Pedersen, Dreier and Christensen25, Reference O’Brien, Lawrence and Keil26], was applied to enhance computational efficiency in the analysis of rare outcomes and exposures while preserving population representativeness. See Figure 1 for a flow chart diagram of the sampling and weighting design of the study population. We selected all individuals with recorded suicidal ideation or self-harm events and a random subsample of non-cases. Among non-cases, we oversampled individuals with indicators of mental disorder history available in the central population register using disproportionate stratified random sampling. Inverse selection probability weights corrected for unequal selection probabilities, enabling population-representative inference. Suicide deaths were not used as a sampling criterion because mortality data were not available at the time of sample construction. Consequently, suicide deaths could occur among both sampled cases and non-cases and were incorporated analytically through inverse probability weighting. A detailed description of the sampling and weighting procedure is provided in the Supplementary Methods. All analyses were restricted to individuals aged ≥10 years in 2014. Follow-up for NLISH and suicide extended through December 31, 2019, with residents emigrating censored at date of emigration. The study protocol was approved by the Parc de Salut Mar Clinical Research Ethics Committee (2022/10325/I).
Sampling and weighting design of the study population. Note: See Supplementary Methods for a detailed description of the sampling and weighting procedure. Suicide deaths were not used as a sampling criterion because mortality data were not available at the time of sampling. The resulting analytic dataset is an outcome- and exposure-enriched sub-sample of the source population; inverse probability weights are therefore applied in all analyses to recover population-representative estimates for suicide, NLISH, and all other variables and associations examined.

Sources of registry data
Registry data came from the Agency for Health Quality and Assessment of Catalonia, which oversees the Public Data Analysis for Health Research and Innovation Programme [27, Reference Mas, Clougher, Anmella, Valenzuela-Pascual, De Prisco and Oliva28]. Using personal healthcare identification numbers, we linked registry data from four sources: (1) mortality data from Spain’s National Statistics Institute (2014–2019), including suicide coded by the International Classification of Diseases, Tenth Revision (ICD-10); (2) routinely collected electronic health record (EHR) data representing the entire Catalan public healthcare system, provided by the Catalan Health Service, including psychiatric hospitalizations (2008–2019), outpatient mental healthcare visits (2008–2019), emergency department visits (2014–2019), general hospitalizations (2007–2019), and primary care visits (2010–2019), with diagnoses coded by ICD-9-CM, ICD-10, and ICD-10-CM. EHR quality is monitored through systematic checks by health documentalists [Reference Dalmau-Bueno, García-Altés, Vela, Clèries, Pérez and Argimon29]; (3) clinically confirmed self-harm episodes (2014–2019) from the Catalonia Suicide Risk Code (CSRC) programme [Reference Pérez, Elices, Prat, Vieta, Blanch and Alonso30], which mandates psychiatric evaluation after self-harm; and (4) administrative data from the Catalan Health Service’s central population register (2014–2019), including sex, age, socioeconomic group, and nationality.
Outcome variables
To address undercoding, NLISH was defined using two sources: (1) healthcare visits coded with ICD self-harm external cause codes (ICD-9-CM E950*–E958*, ICD-10 X60*–X84*, or ICD-10-CM T14.91*, X71*–X83*, and T36*–T65*/T71* [if the fifth or sixth character equaled 2]) in routine EHR; and (2) clinically confirmed self-harm episodes from the CSRC programme. The first NLISH event recorded in either source was coded as the outcome event. Suicide was defined as death from intentional self-harm (ICD-10 X60–X84).
Explanatory variables and covariates
Explanatory variables included 32 mental disorder categories, created by grouping ICD-coded diagnoses from healthcare visits using the ten-level subchapter structure of ICD-10 Chapter V (F00–F99), with five categories subdivided to enhance granularity (Supplementary Table 1). Covariates were (1) sex; (2) age group (10–19, 20–44, 45–64, ≥65); (3) socioeconomic status, classified as employed or retired with contributory income above/below €18,000, or vulnerable (e.g., disability support, non-contributory pensions, minimum living income, or unemployed without benefits); and (4) nationality, grouped by country income level (high, upper-middle, lower-middle, low).
Statistical analysis
Descriptive statistics were used to characterize the study cohort by the covariates, and sex-specific point prevalence and 95% confidence intervals were estimated for each mental disorder category. Associations of mental disorders with NLISH and suicide were examined using cause-specific Cox proportional hazards models, run separately for each of the 32 disorders, stratified by sex, and adjusted for age, socioeconomic status, and nationality (by income level). Additional models were stratified by age group. In suicide models, non-suicide deaths were competing events; in NLISH models, all-cause deaths were competing events. To establish a temporal relationship between mental disorder diagnosis and NLISH, individuals with any NLISH diagnosis prior to January 1, 2014, were excluded through a washout procedure [Reference Chai, Luo, Wong, Tang, Lam and Wong20], based on available pre-2014 EHR data from primary care (from 2010) and hospitalization records (general from 2007; psychiatric from 2008). Because emergency department data were unavailable before 2014, the effective washout period varied by data source and was incomplete for NLISH events recorded exclusively in emergency departments.
Mental disorders were modeled as time-varying exposures. Individuals with no mental disorder diagnosis recorded in EHR before or during follow-up (2014–2019) were considered unexposed throughout. Prevalent cases, i.e., those diagnosed before January 1, 2014, were considered exposed from the start of follow-up. Incident cases diagnosed during the follow-up period were considered unexposed until the date of first healthcare contact for the mental disorder, and exposed afterwards. Because outpatient mental healthcare visit dates were only available by calendar year, January 1 was assigned as the diagnosis date.
Mental disorders were not mutually exclusive. Individuals could be classified into more than one disorder category and could therefore contribute to multiple disorder-specific models. Each Cox model compared individuals with the disorder of interest to all other individuals in the analytic cohort, irrespective of the presence of other mental disorders. As a result, disorder-specific estimates reflect the total association of each disorder category with the outcome and are not mutually adjusted for psychiatric comorbidity. In addition, we analyzed a composite category of “any mental disorder,” defined as the presence of at least one of the 32 mental disorder categories at any point during the observation window.
To evaluate population-level associations of mental disorders with the outcomes, we calculated PAFs [Reference Levin31] using Miettinen’s case-based formulation [Reference Lee, Moon, Kim, Sung, Hong and Lim32, Reference Rockhill, Newman and Weinberg33], combining the weighted prevalence of each mental disorder among cases with adjusted HRs from cause-specific Cox models. PAFs summarize the proportion of observed cases statistically attributable to an exposure under the specified model assumptions and over the observed follow-up period [Reference Rockhill, Newman and Weinberg33]. Although this formulation does not explicitly incorporate time or competing risks in the PAF calculation itself, it is commonly used as a summary measure in cohort studies; competing risks are addressed at the level of HR estimation [Reference Laaksonen, Knekt, Harkanen, Virtala and Oja34]. Accordingly, PAFs are interpreted here as descriptive, model-based measures averaged over follow-up rather than as time-specific or causal estimands of preventable risk.
Finally, we estimated a lethality index (LI) [Reference Tong, Yin, Lan and Conner35] of self-harm associated with each mental disorder by dividing the suicide incidence rate by the sum of the suicide and NLISH incidence rates among individuals diagnosed with the disorder, multiplied by 100.
Statistical analysis was performed using R, version 4.4.2 (R Project for Statistical Computing), primarily using the survey (version 4.4-2) and survival (version 3.7-0) packages. All analyses were conducted within the survey design framework, accounting for inverse probability sampling weights and stratification. Point estimates, including measures of association, prevalence, incidence rates, and HRs, were accompanied by standard errors and 95% confidence intervals derived using design-based variance estimation based on Taylor series linearization (robust sandwich estimators), as implemented in the survey package. For time-to-event analyses, cause-specific Cox proportional hazards models were fitted using survey-weighted partial likelihood (survey::svycoxph), yielding design-consistent HR estimates with inference based on robust, design-based variance estimation. Confidence intervals for PAFs were derived using an analytic variance estimator combining uncertainty from both the log-HR and the weighted exposure prevalence among cases, with interval construction based on a log(1−PAF) transformation [Reference Rothman36]. Two-sided P < .05 was considered significant. Analyses were conducted between October 14, 2024 and January 29, 2026.
Results
Study cohort descriptive statistics
The final cohort included 645,571 individuals aged ≥10 years (from 6,623,221 eligible residents). A total of 18,045 emigrated before December 31, 2019 and were lost to follow-up. During follow-up, 36,549 had one or more episodes of NLISH, and 1,118 died by suicide.
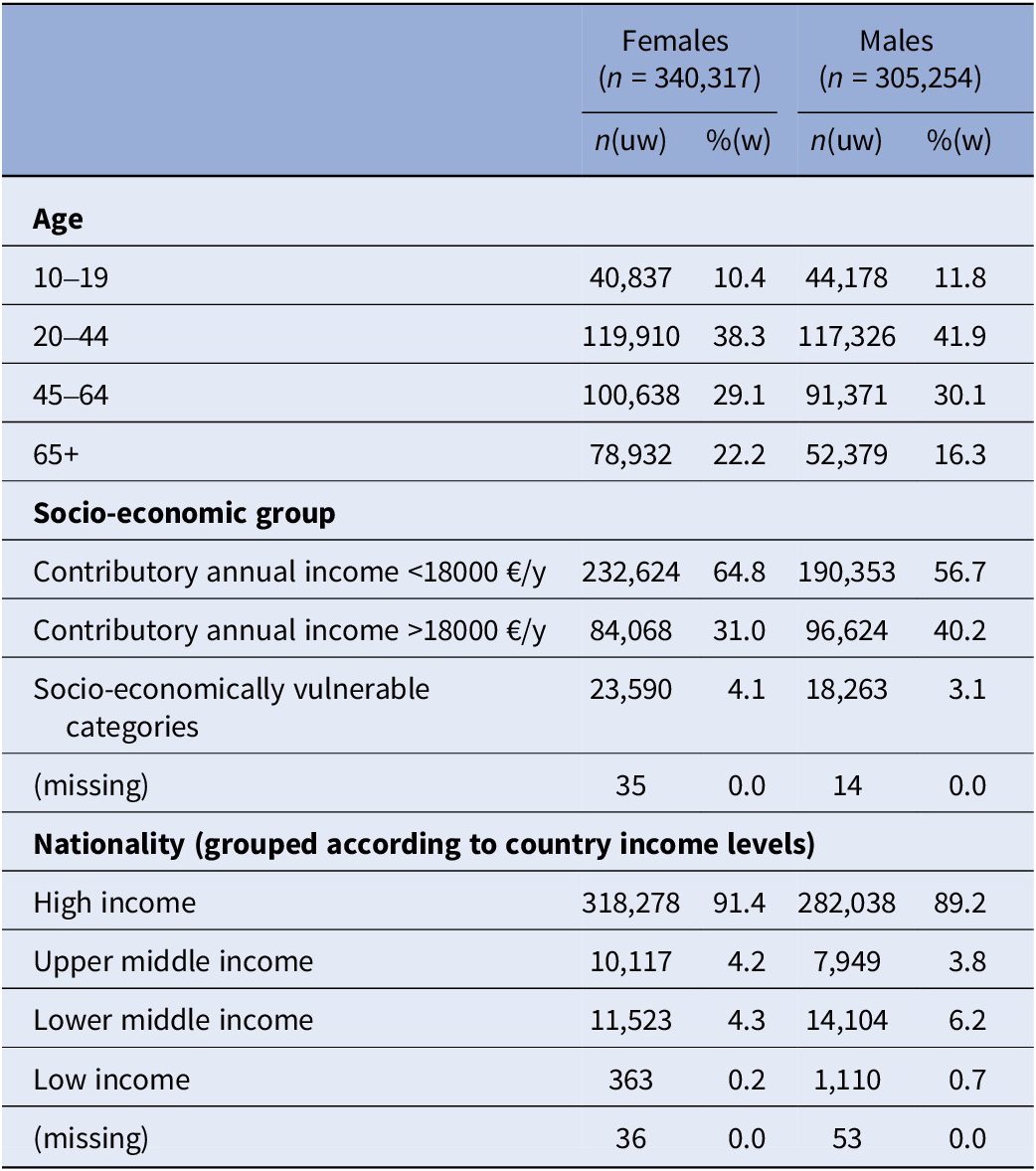
The cohort comprised 340,317 females (50.9%) and 305,254 males (49.1%). As shown in Table 1, most were aged 20–44 (38.3% in females; 41.9% in males) or 45–64 (29.1% in females; 30.1% in males), had annual contributory incomes <€18,000 (64.8% in females; 56.7% in males), and were of nationalities from high-income countries (91.4% in females; 89.2% in males).
Cohort descriptive statistics (n = 645,571)

Note: Weighted percentages were calculated applying inverse probability weights upon the cohort data and are representative for all individuals living in the autonomous region of Catalonia (Spain) between January 1, 2014 and December 31, 2019, aged 10 or older (n = 6,623,221).
Abbreviations: uw, unweighted; w, weighted.
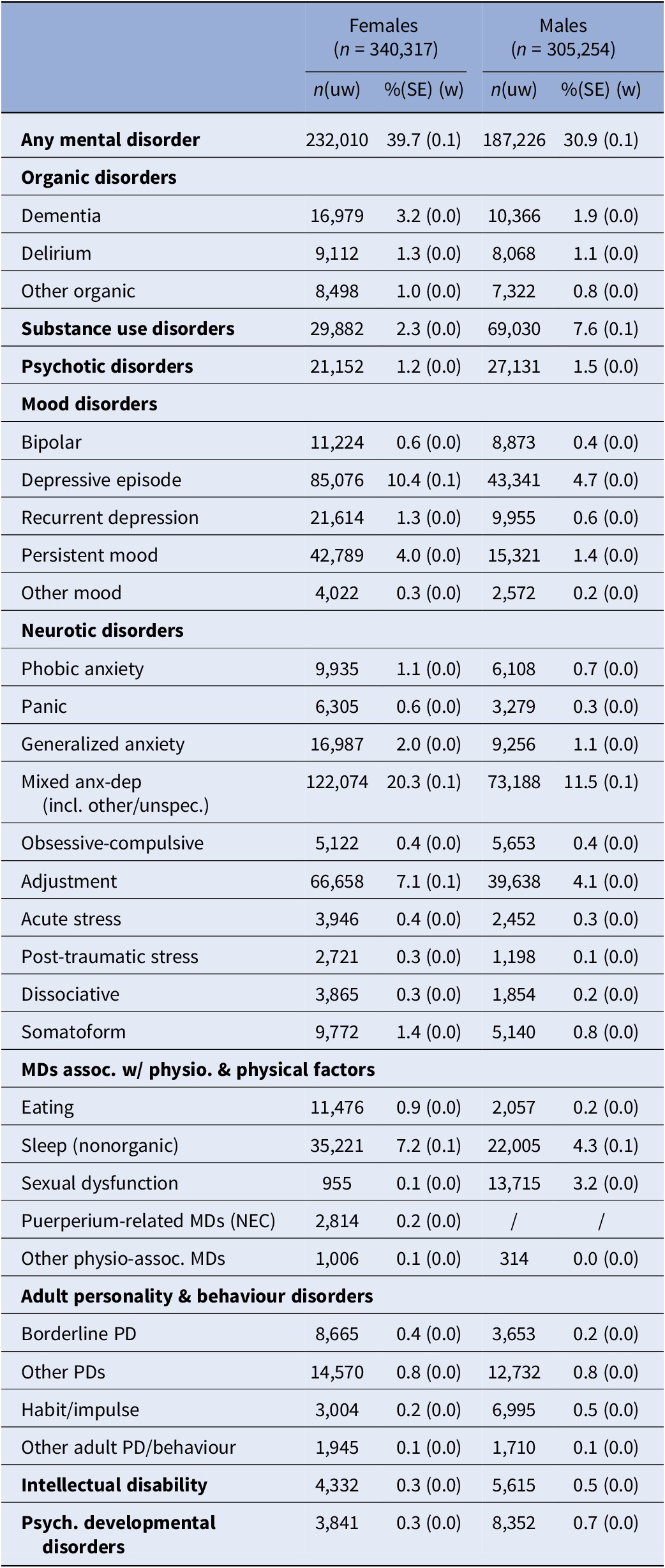
The prevalence of any recorded mental disorder was higher among females than males (39.7% vs 30.9%, respectively; Table 2). Mixed anxiety and depressive disorders were the most common diagnosis in both sexes, affecting 20.3% of females and 11.5% of males. Females showed higher prevalence of depressive episodes (10.4% vs 4.7%), adjustment disorders (7.1% vs 4.1%), and non-organic sleep disorders (7.2% vs 4.3%). In contrast, substance use disorders were more prevalent among males (7.6% vs 2.3%).
Prevalence of recorded mental disorders (n = 645,571)

Note: Weighted percentages were calculated applying inverse probability weights upon the cohort data and are representative for all individuals living in the autonomous region of Catalonia (Spain) between January 1, 2014 and December 31, 2019, aged 10 or older (n = 6,623,221).
Abbreviations: MD, mental disorder; NEC, not elsewhere classified; PD, personality disorder; SE, standard error; uw, unweighted; w, weighted.
Associations of mental disorders with NLISH
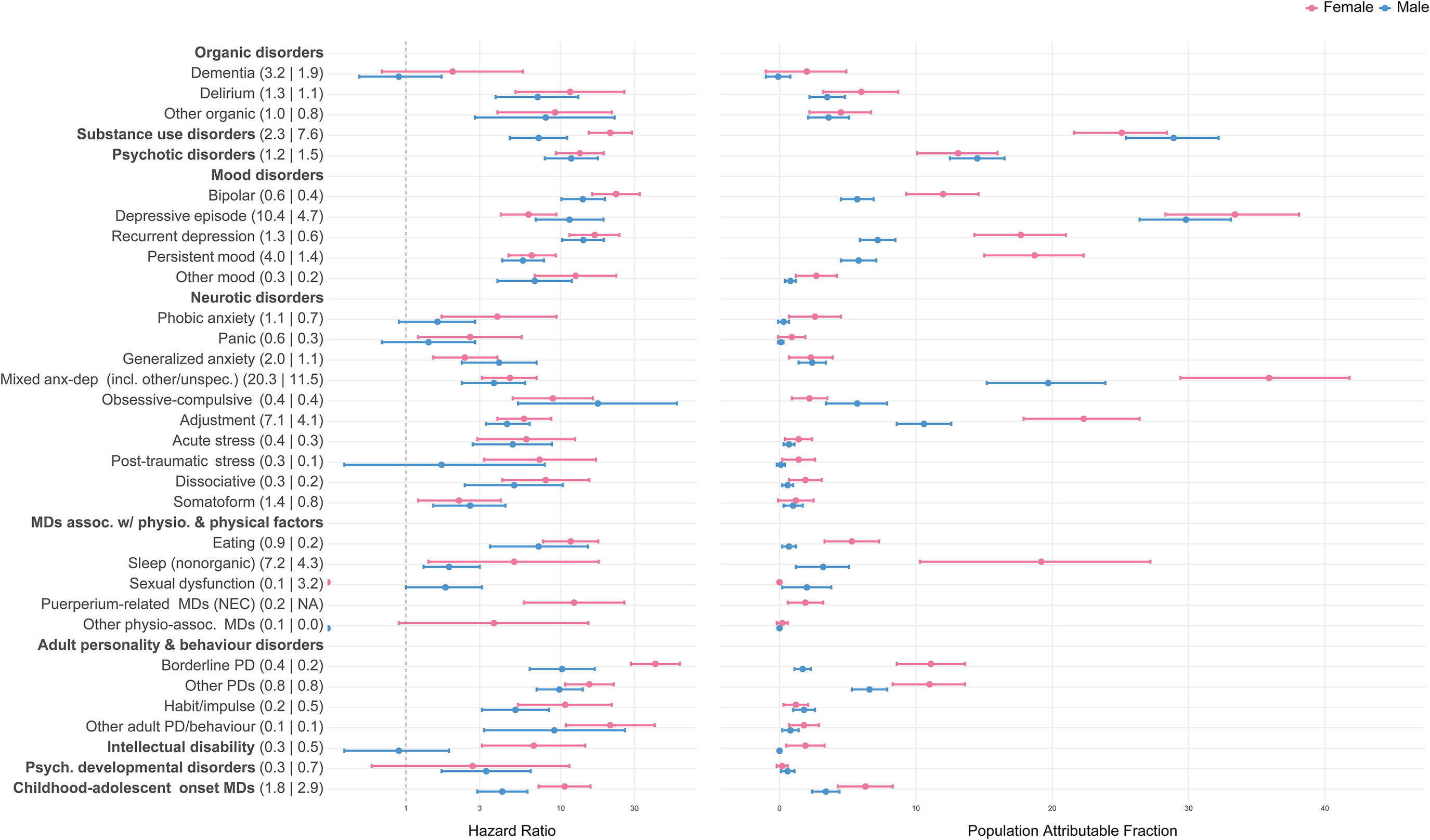
The individual-level association of any mental disorder (i.e., any of the 32 vs. none) with NLISH was strong in both sexes (HR = 20.5 [95%CI 19.4–21.7] in females; HR = 18.4 [95%CI 17.3–19.6] in males). Corresponding PAFs were 91.6% [95%CI 90.9–92.2] and 89.2% [95%CI 88.3–90.0]. The median HRs across the 32 disorders (i.e., comparing for each disorder to the group without the disorder) were 5.9 (interquartile range [IQR] = 4.1–9.6) in females and 6.6 (IQR = 4.8–9.7) in males; corresponding PAFs were 3.4% (IQR = 2.3–13.2) and 3.6% (IQR = 2.2–13.0).
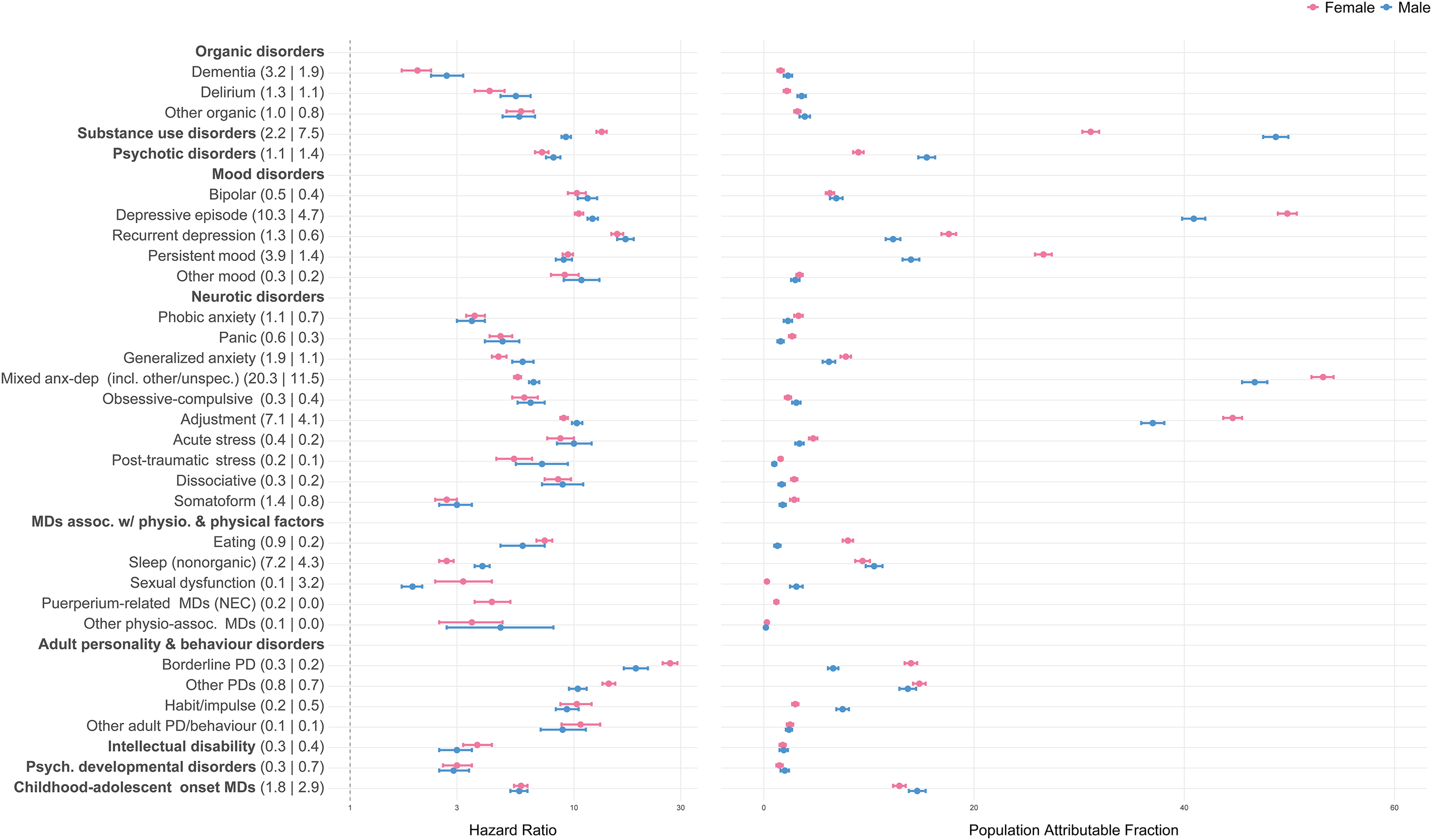
In both sexes, BPD showed the strongest individual-level associations with NLISH (HR = 26.9 in females; HR = 18.9 in males) followed by recurrent depression (HR = 15.6 in females; HR = 17.0 in males; Figure 2, Supplementary Table 2). Because these disorders were less prevalent, PAFs were modest (range 6.6–17.6%). In contrast, strong population-level associations with NLISH were found for depressive episodes, substance use disorders, mixed anxiety and depressive disorders (including other specified and unspecified types), and adjustment disorders, with PAFs ranging 31.1–53.2%, being highest in females with mixed anxiety and depressive disorders (PAF = 53.2%) and in males with substance use disorders (PAF = 48.7%). The individual-level associations with NLISH for depressive episodes, substance use disorders, and adjustment disorders were also considerable (HRs range 9.0–13.3 in females; 9.2–12.1 in males).
The associations of mental disorders with NLISH (n = 634,134). Note: Number in parentheses following mental disorder labels are mental disorder prevalence estimates, separate by sex (females | males). The HR and population attributable fractions are estimated for each mental disorder diagnosis separately (each time comparing to individuals without the diagnosis), using Cox proportional hazards models, adjusting for age, socio-economic status, and nationality (grouped according to country income levels). All estimates were calculated applying inverse probability weights upon the cohort data and are representative for all individuals living in the autonomous region of Catalonia (Spain) on January 1, 2014, aged 10 or older; to establish a temporal relationship between mental disorder diagnosis and NLISH, individuals with any recorded NLISH diagnosis prior to January 1, 2014, were excluded from analysis. See Supplementary Table 1 for detailed information on mental disorder diagnosis categories and corresponding ICD-9-CM, ICD-10, and ICD-10-CM diagnostic codes. Abbreviations: MD, mental disorder; NEC, not elsewhere classified; PD, personality disorder.

Seventeen disorders in females and 14 in males showed significant age-group variation in their associations with NLISH, most often stronger in ages 10–19 and 20–44, compared to older age groups (Supplementary Table 3). In both sexes, the overall pattern of associations was generally consistent across age groups, with the strongest associations observed for BPD (particularly in ages 10–19 [HR = 34.0 in females; HR = 28.9 in males]) and for recurrent depression (again, particularly in ages 10–19 [HR = 20.3 in females; HR = 27.7 in males]). In females, this was followed by other personality disorders (HRs range 12.3–17.2 across age groups) and substance use disorders (HRs range 9.0–17.7), and in males by bipolar disorder (HRs range 11.0–18.0) and depressive episodes (HRs range 9.0–17.1). Notably, in ages 10–19, psychotic disorders were strongly associated with NLISH in both sexes (HR = 17.4 in females; HR = 19.7 in males). In this age group, depressive episodes also showed a strong association in females (HR = 20.5) and dissociative disorders in males (HR = 17.7).
Associations of mental disorders with suicide
Both individual- and population-level associations of any mental disorder with suicide were stronger in females (HR = 35.6 [95%CI 13.4–94.5]; PAF = 92.0% [95%CI 87.2–95.0]) than males (HR = 12.2 [95%CI 5.9–25.3]; PAF = 73.3% [95%CI 67.1–78.3]). Median HRs and PAFs were 7.7 (IQR = 4.5–12.3) and 2.7% (IQR = 1.7–12.3) in females, and 5.0 (IQR = 2.3–8.6) and 2.0% (IQR = 0.7–5.8) in males.
In females, the strongest individual-level association was for BPD (HR = 40.9), followed by bipolar disorder, substance use disorders, and other disorders of adult personality and behaviour (HRs range 20.9–22.8), then recurrent depression and other personality disorders (HRs range 15.3–16.6), and psychotic disorders (HR = 13.3; Figure 3, Supplementary Table 4). In males, individual-level associations were strongest for obsessive-compulsive disorder (HR = 17.4) followed by recurrent depression and bipolar disorder (HR = 13.9–14.0), and by psychotic disorders, depressive episodes, and BPD (HRs range 10.2–11.7).
The associations of mental disorders with suicide (n = 645,571). Note: Number in parentheses following mental disorder labels are mental disorder prevalence estimates, separate by sex (females | males). The HR and population attributable fractions are estimated for each mental disorder diagnosis separately (each time comparing to individuals without the diagnosis), using Cox proportional hazards models, adjusting for age, socio-economic status, and nationality (grouped according to country income levels). All estimates were calculated applying inverse probability weights upon the cohort data and are representative for all individuals living in the autonomous region of Catalonia (Spain) on January 1, 2014, aged 10 or older. See Supplementary Table 1 for detailed information on mental disorder diagnosis categories and corresponding ICD-9-CM, ICD-10, and ICD-10-CM diagnostic codes. Abbreviations: MD, mental disorder; NEC, not elsewhere classified; PD, personality disorder.

Population-level associations were strongest for depressive episodes (PAFs range 29.8–33.4%), mixed anxiety and depressive disorders (including other specified and unspecified types), especially in females (PAF = 35.9% vs 19.7% in males), substance use disorders (PAFs range 25.1–28.9%), and adjustment disorders, especially in females (PAF = 22.3% vs 10.6% in males). In females, PAFs were also considerable for non-organic sleep disorders, persistent mood disorders, and recurrent depression (PAFs range 17.7–19.2%).
Twenty-five disorders in females and 18 in males showed significant age-group variation in their associations with suicide. In females, the strongest associations were typically observed in ages 10–19 or 20–44, whereas no consistent age-related pattern was identified in males (Supplementary Table 5). When examining the overall pattern of associations between mental disorders and suicide across age groups, no consistent pattern emerged in either sex. In females, BPD was strongly associated with suicide across all age groups, especially 10–19 and 20–44 (HRs range 64.1–64.9). In females aged 10–19, even stronger associations were observed for recurrent depression (HR = 146.0), substance use disorders (HR = 113.7), persistent and other mood disorders (HR = 91.3), and dissociative disorders (HR = 70.1). In males, the strongest associations across age groups were observed for obsessive-compulsive disorder but only in those aged 45 or older (HRs range 36.1–56.9). In males aged 10–19, associations were strongest for psychotic disorders (HR = 226.5), followed by bipolar disorder (HR = 75.9), substance use disorders (HR = 56.0), recurrent depression (HR = 50.3), and BPD (HR = 33.2). In males aged 20–44, associations were strongest for depressive episodes (HR = 15.5), bipolar disorder (HR = 15.4), psychotic disorders (HR = 14.4), and recurrent depression (HR = 14.3).
Lethality of self-harm associated with mental disorders
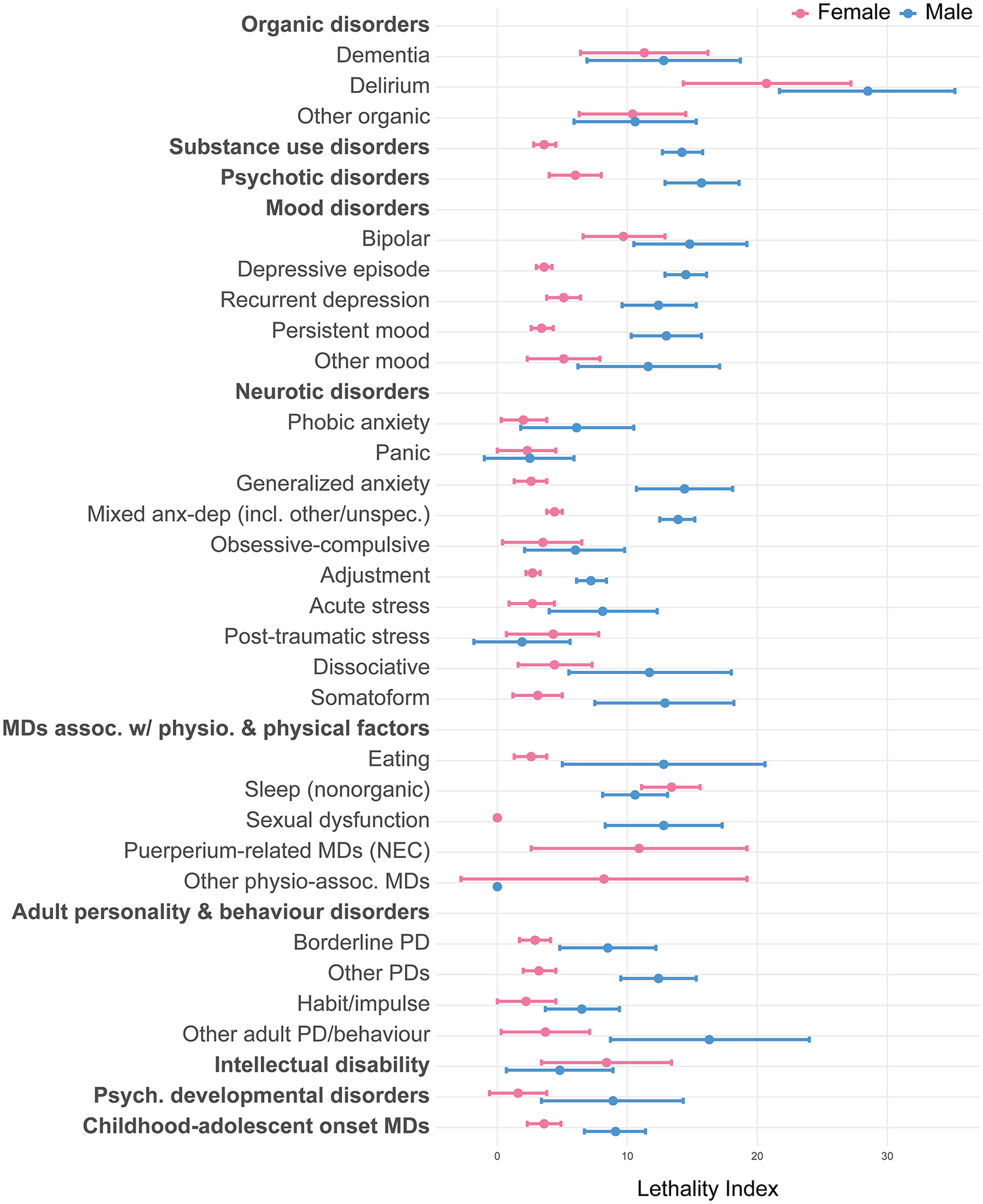
The median LI of self-harm associated with mental disorders in females was 3.6 (IQR = 2.7–6.6); in males this was substantially higher, i.e., 11.7 (IQR = 7.7–13.5; Figure 4 and Supplementary Table 6). Lethality was highest for organic disorders, especially delirium (LI = 20.7 females; LI = 28.5 males). In females, this was followed by non-organic sleep disorders (LI = 13.4), mental disorders associated with the puerperium not elsewhere classified, bipolar disorder, and intellectual disability (LIs range 8.4–10.9). In males, this was followed by other disorders of adult personality and behaviour (LI = 16.3), psychotic disorders (LI = 15.7), bipolar disorder (LI = 14.8), depressive episodes (LI = 14.5), generalized anxiety disorder (LI = 14.4), and mixed anxiety and depressive disorders (LI = 13.9).
Lethality index associated with mental disorders, by sex. Note: The lethality index of self-harm associated with each specific mental disorder is calculated by dividing the suicide incidence rate by the sum of the suicide and NLISH incidence rates among individuals diagnosed with the specific disorder, multiplied by 100. All estimates were calculated applying inverse probability weights upon the cohort data and are representative for all individuals living in the autonomous region of Catalonia (Spain) on January 1, 2014, aged 10 or older; for the estimation of NLISH and suicide incidence rates by mental disorder, we each time excluded all individuals with any recorded diagnosis of the specific mental disorder prior to January 1, 2014 from analysis. In addition, for the estimation of NLISH incidence, we also excluded all individuals with a recorded NLISH diagnosis prior to January 1, 2014 from analysis. See Supplementary Table 1 for detailed information on mental disorder diagnosis categories and corresponding ICD-9-CM, ICD-10, and ICD-10-CM diagnostic codes. Abbreviations: MD, mental disorder; NEC, not elsewhere classified; PD, personality disorder.

Discussion
Our study addressed an important lack of knowledge by quantifying the population-level associations between a wide range of mental disorders and non-lethal and lethal self-harm. By presenting individual-level association estimates alongside population-level summary measures, we provide a descriptive comparison of disorders that differ in prevalence and relative association strength. A novel and important finding was that not only depression and substance use disorders [Reference Ferrari, Norman, Freedman, Baxter, Pirkis and Harris4] but also mixed anxiety and depressive disorders and adjustment disorders were associated with high proportions of NLISH (PAFs range 37.0–53.2%) and suicide (PAFs range 10.6–35.9%). These large PAFs primarily reflect the high population prevalence of these disorders, rather than exceptionally strong individual-level risks.
According to ICD-10, mixed anxiety and depressive disorder involves subthreshold symptoms of both conditions that cause significant distress yet fall short of criteria for a syndromal diagnosis. These presentations are common in primary care [Reference Mas, Clougher, Anmella, Valenzuela-Pascual, De Prisco and Oliva28], functionally impairing, and frequently go unrecognized due to diagnostic ambiguity or somatic presentations [Reference Möller, Bandelow, Volz, Barnikol, Seifritz and Kasper37]. Adjustment disorders, though often considered less severe, have been shown to be strongly associated with non-lethal self-harm among stress-related disorders [Reference Street, Jiang, Horváth-Puhó, Rosellini, Lash and Sørensen38] and are highly prevalent among emergency department and psychiatric inpatients with self-harm [Reference Di Lorenzo, Scala, Reami, Rovesti and Ferri39, Reference Fegan and Doherty40]; however, research on self-harm risk in these populations remains limited. Taken together, these findings suggest that common and often under-recognized disorders represent a substantial share of the observed self-harm burden at the population level.
Importantly, the strong population-level associations observed in this study do not in themselves justify prioritizing these disorders as direct prevention targets [Reference Rockhill, Newman and Weinberg33, Reference Rowe, Powell and Flanders41]. PAFs should not be interpreted as the proportion of cases that could be prevented through elimination of mental disorders, but rather as descriptive, model-based summaries of population burden under the observed mental disorder exposure structure and specified model assumptions [Reference Rockhill, Newman and Weinberg33, Reference Rowe, Powell and Flanders41, Reference Benichou42]. Because several of these disorders are both common and highly comorbid, the estimated PAFs are not intended to represent mutually exclusive or independent effects. Approaches that explicitly adjust for psychiatric comorbidity would address a different, conditional estimand and were therefore not pursued in this analysis. Causality needs testing in robust prospective studies [Reference Hernán and Robins43] with careful control for somatic and psychiatric comorbidity [Reference Nock, Hwang, Sampson and Kessler44, Reference Qin, Hawton, Mortensen and Webb45], and other mediating and moderating factors between specific mental disorders and self-harm [Reference O’Connor and Kirtley46], which may all account for the associations observed in this study, and may represent more actionable targets. Even if indirect causal links are confirmed, prevention policy should ultimately be guided by the cost-effectiveness of available interventions [Reference Dunlap, Orme, Zarkin, Arias, Miller and Camargo47].
Our study also provides robust evidence on the relationship between BPD and self-harm [Reference Perea-González, De la Vega, Sanz-Gómez and Giner48, Reference McClelland, Cleare and O’Connor49], an area limited by small samples and heterogeneous study populations [Reference Lak, Shakiba, Dolatshahi, Saatchi, Shahrbaf and Jafarpour50]. Since self-harm is a common feature of BPD, it was perhaps unsurprising to find BPD to be the diagnosis most strongly associated with NLISH among both females (HR = 26.9) and males (HR = 18.9) and to find low lethality of self-harm in BPD, given the recurrent course of self-harm in BPD [Reference Reichl and Kaess51]. A notable finding from our study was the exceptionally high risk of death by suicide among females with BPD (HR = 40.9), particularly among young and early middle-aged females (10–44 years; HRs range 64.1–64.9). While individual-level risks were very high, the population-level burden of BPD remained modest because of its comparatively low prevalence, especially among males. This highlights the importance of targeted interventions for individuals with BPD, including access to evidence-based psychotherapies such as dialectical behaviour therapy, structured follow-up, and crisis response plans [Reference Lak, Shakiba, Dolatshahi, Saatchi, Shahrbaf and Jafarpour50].
Associations with NLISH in our study varied only modestly by sex or age, whereas associations with suicide were stronger among females, and were markedly stronger at ages 10–44 across mood, substance use, dissociative, borderline personality, and psychotic disorders, compared to older age groups. This age pattern is consistent with evidence that the suicide burden attributable to mental disorders peaks in early adulthood [Reference Ferrari, Norman, Freedman, Baxter, Pirkis and Harris4], and especially relevant given increasing rates of self-harm among young people in Spain [Reference López-Cuadrado, Mortier, Alonso and Martínez-Alés52]. The comparatively weaker associations in males may reflect more heterogeneous pathways less characterized by risk related to mental disorder (e.g., being single or unemployed [Reference Qin, Agerbo, Westergård-Nielsen, Eriksson and Mortensen53], social isolation [Reference Shaw, Cullen, Graham, Lyall, Mackay and Okolie54], legal problems [Reference Stone, Holland, Schiff and McIntosh55]), suicide in the absence of mental disorder [Reference Oquendo, Wall, Wang, Olfson and Blanco56], lower detection of mental disorder [Reference Snowdon57], or lower help-seeking behaviour [Reference Andrade, Alonso, Mneimneh, Wells, Al-Hamzawi and Borges58]. Notably, among males, risk for suicide was highest for obsessive-compulsive disorder (HR = 17.4), particularly in those aged ≥45 (HRs range 36.1–56.2). Although historically considered low risk, obsessive-compulsive disorder has recently been strongly linked to suicide in studies from Taiwan [Reference Chen, Pan, Cheng, Chang, Bai and Su59], Sweden [Reference de la Cruz, Rydell, Runeson, D’Onofrio, Brander and Rück60], and Denmark [Reference Meier, Mattheisen, Mors, Schendel, Mortensen and Plessen61], particularly in severe, chronic cases, likely reflecting the intense distress caused by core symptoms, independent of comorbidity [Reference Chen, Pan, Cheng, Chang, Bai and Su59].
This study has several limitations. First, EHR data from emergency departments, often the only point of contact for non-lethal self-harm, were only available from 2014 onwards; although a washout procedure was applied using available primary care and hospitalization registries, NLISH events occurring exclusively in emergency departments prior to 2014 could not be identified. As a result, some NLISH cases classified as incident may in fact have been prevalent. Future studies utilizing registry data spanning a larger time period will address this limitation, and will also explore whether NLISH serves as a mediator or moderator in the association of mental disorders with eventual suicide. Second, outpatient mental healthcare visit dates were only available at the year level, introducing potential immortal time bias [Reference Lévesque, Hanley, Kezouh and Suissa62] that may have led to an underestimation of associations in the Cox models. Third, the identification of mental disorders and NLISH relied on recorded diagnoses from healthcare contacts, which may be subject to underdiagnosis and misclassification, and exclude individuals who did not seek care. These limitations may have influenced prevalence estimates and, consequently, population-level measures such as PAFs. It is worth mentioning that, since public healthcare in Spain is free and highly accessible, the proportion of individuals with mental disorders who do not seek care may be relatively low [Reference Aznar-Lou, Serrano-Blanco, Fernández, Luciano and Rubio-Valera63]. Fourth, we did not investigate associations of mental disorders with repetition of NLISH, which requires specific analytic approaches [Reference Bøe, Mehlum, Melle and Qin64] and was beyond the scope of this study. Lastly, while our analysis included a broad range of mental disorders, some categories were not disaggregated into specific diagnoses (e.g., substance use, psychotic, or childhood-onset disorders). Future studies will address this, and will also adjust for psychiatric and somatic comorbidity.
Our findings reinforce calls to reduce suicide mortality associated with mental disorders [Reference O’Connor, Worthman, Abanga, Athanassopoulou, Boyce and Chan65], particularly among young people. The strong population-level associations of common disorders such as depressive episodes and substance use disorders with self-harm underscore the importance of routine screening and timely referral in primary care [Reference O’Connor, Perdue, Coppola, Henninger, Thomas and Gaynes66, Reference Mann, Michel and Auerbach67] and tailored prevention strategies in individuals with substance use disorders [Reference Padmanathan, Hall, Moran, Jones, Gunnell and Carlisle68]. Moreover, our results emphasize the need to investigate the potential contribution of adjustment disorders and subsyndromal anxiety-depressive presentations to self-harm risk. The finding that common disorders are strongly associated with self-harm at both the individual and population level suggests that healthcare systems must be equipped to recognize and manage these conditions. Integrated collaborative care models [Reference Ko, Jeong, Yim and Lee69, Reference Reist, Petiwala, Latimer, Raffaelli, Chiang and Eisenberg70] coordinating efforts across primary, emergency, and mental health services offer a scalable solution. Their impact could be enhanced by data-driven risk stratification tools and clinical decision support systems [Reference Mortier, Amigo, Bhargav, Conde, Ferrer and Flygare71], enabling more efficient allocation of resources. Finally, clinical strategies must also be complemented by broader policy initiatives addressing the social determinants of mental health [Reference Pirkis, Dandona, Silverman, Khan and Hawton72].
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1192/j.eurpsy.2026.10182.
Data availability statement
The primary data, including healthcare, mortality, and administrative records, were provided by a third party, the Agency for Quality and Assessment of Catalonia (Agència de Qualitat i Avaluació Sanitàries de Catalunya; AQuAS), under the PADRIS (Programa d’Analítica de Dades per a la Recerca i la Innovació en Salut) framework. Access to these data is restricted, and must comply with PADRIS’s legal and ethical requirements. Interested parties can obtain access to the data, code, and documentation upon request, in accordance with the agreement’s provisions. The minimum dataset needed to replicate the analyses underlying this study, including the anonymized individual-level registry data, data dictionaries, and statistical code, is available upon reasonable request from the corresponding authors (Philippe Mortier: pmortier@researchmar.net; Gemma Vilagut: gvilagut@researchmar.net), provided (a) the purpose is to replicate our analysis and results without additional investigator support, (b) access is granted following approval of a brief proposal and the signing of a Data Access Agreement, and (c) the request aligns with the terms of our agreement with PADRIS/AQuAS and is approved by the PADRIS legal representative.
Acknowledgments
This study was conducted using anonymized data provided by the Agency for Quality and Assessment of Catalonia (Agència de Qualitat i Avaluació Sanitàries de Catalunya; AQuAS), within the framework of the Data Analytics Programme for Health Research and Innovation (Programa d’analítica de dades per a la recerca i la innovació en salut; PADRIS) Programme.
Author contribution
Conceptualization: P.M., M.F., O.P-R., G.V., and J.A.; Data Curation: I.A., P.M., M.F., and G.V.; Formal Analysis: P.M., M.F., O.P-R., and G.V.; Funding Acquisition: P.M.; Investigation: P.M., M.F., O.P-R., G.V., and J.A.; Methodology: P.M., M.F., O.P-R., G.V., and J.A.; Project Administration: P.M.; Visualization: P.M., M.F., O.P-R., and G.V.; Writing – Original Draft: P.M.; Writing – Review & Editing: All authors.
Financial support
P.M. is supported by Miguel Servet grant CP21/00078 co-financed by the Instituto de Salud Carlos III (ISCIII) and co-funded by the European Union; grant PI22/00107 funded by ISCIII and co-funded by the European Union; and grant 202220-30-31 from the Fundació la Marató de TV3. A.P.V.D. is supported by grant FI23/00004 funded by ISCIII and co-funded by the European Union. This work was further supported by ISCIII PI17/00521 (CODIRISC/CSRC-Epi) con fondos FEDER (J.A.); Spanish Ministry of Science and Innovation/ISCIII/FEDER PI21/01148 (D.P.); the Secretaria d’Universitats i Recerca del Departament d’Economia i Coneixement of the Generalitat de Catalunya AGAUR 2021 SGR 00624 (J.A.) and AGAUR 2021 SGR 01431 (D.P.); the CERCA programme of the I3PT (D.P.); Centro de Investigación Biomédica en Red de Salud Mental, Instituto de Salud Carlos III (CIBERSAM, ISCIII), and grant CB06/02/0046 from the Centro de Investigación Biomédica en Red de Epidemiología y Salud Pública (CIBERESP), ISCIII (J.A.). Funding agencies for this study had no role in study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
Competing interests
In the past 3 years, Dr. Kessler was a consultant for Cambridge Health Alliance, Child Mind Institute, Massachusetts General Hospital, RallyPoint LLC., Sage Therapeutics, University of Michigan, and University of North Carolina. He has stock options in Cerebral Inc., Mirah, PYM (Prepare Your Mind), and Verisense Health. He owns an interest in Menssano LLC. Diego Palao has received grants and also served as consultant or advisor for Rovi, Janssen, and Lundbeck with no financial or other relationship relevant to the subject of this article. The other authors have no conflicts of interest to declare.



 Open access
Open access
Comments
No Comments have been published for this article.