


Introduction
Healthy aging is the process of maintaining functional ability that enables wellness in older age, and as the population ages, concerns around healthy aging are of increased priority for many Canadians. Older adults are increasingly expressing interest in remaining in their home community and maintaining independence as they age, a phenomenon known as aging in place. Healthy aging can be a challenge for many older adults, which can impact their ability to age in place (Bacsu et al., Reference Bacsu, Jeffery, Abonyi and Johnson2014; Forum of Federal/Provincial/Territorial Ministers Responsible for Seniors, 2015; Yarker et al., Reference Yarker, Doran and Buffel2024). However, to successfully age in place, an individual requires support and resources at multiple different levels (Choi, Reference Choi2022; Vanleerberghe et al., Reference Vanleerberghe, De Witte, Claes, Schalock and Verte2017; Wiles et al., Reference Wiles, Leibing, Guberman, Reeve and Allen2011). While there is research on aging in place in Canada, much of the literature focuses on aging in place in urban environments. However, nearly a quarter of Canadian older adults live in rural areas (Forum of Federal/Provincial/Territorial Ministers Responsible for Seniors, 2006). There are a variety of definitions for the term rural, including qualitative and quantitative definitions. Quantitative definitions are often based on population size, population density, developed land cover, or distance to urban areas (Nelson et al., Reference Nelson, Nguyen, Brownstein, Garcia, Walker, Watson and Xin2021). An example of a commonly used quantitative definition is that in Canada, an area is considered rural if it is outside census agglomerations of 10,000 or more (Asad et al., Reference Asad, Nur, Morris and Bobiak2021). Qualitative definitions typically focus on the subjective experiences of those who live rurally. These definitions emphasise that the term rural can be flexible depending on different contexts or perspectives of rural residents (Nelson et al., Reference Nelson, Nguyen, Brownstein, Garcia, Walker, Watson and Xin2021). Moreover, rural-dwelling older adults experience unique factors that influence their ability to age in place. For example, rural areas typically have fewer health services available locally, which could be a barrier to healthy aging (Wilson et al., Reference Wilson, Rourke, Oandasan and Bosco2020). Conversely, rural older Canadians report higher levels of social support and social participation, which could improve the experience of aging in place (Bacsu et al., Reference Bacsu, Jeffery, Abonyi and Johnson2014). The socio-ecological model examines health behaviours and the factors that influence them at the intrapersonal, interpersonal, institutional, community, and policy levels (McLeroy et al., Reference McLeroy, Bibeau, Steckler and Glanz1988). To better understand the factors that influence an older adult’s ability to age in place in rural Canada, the socio-ecological model will be suggested as a framework to examine the relationships between the older adult and their physical and sociocultural environment.
The socio-ecological model
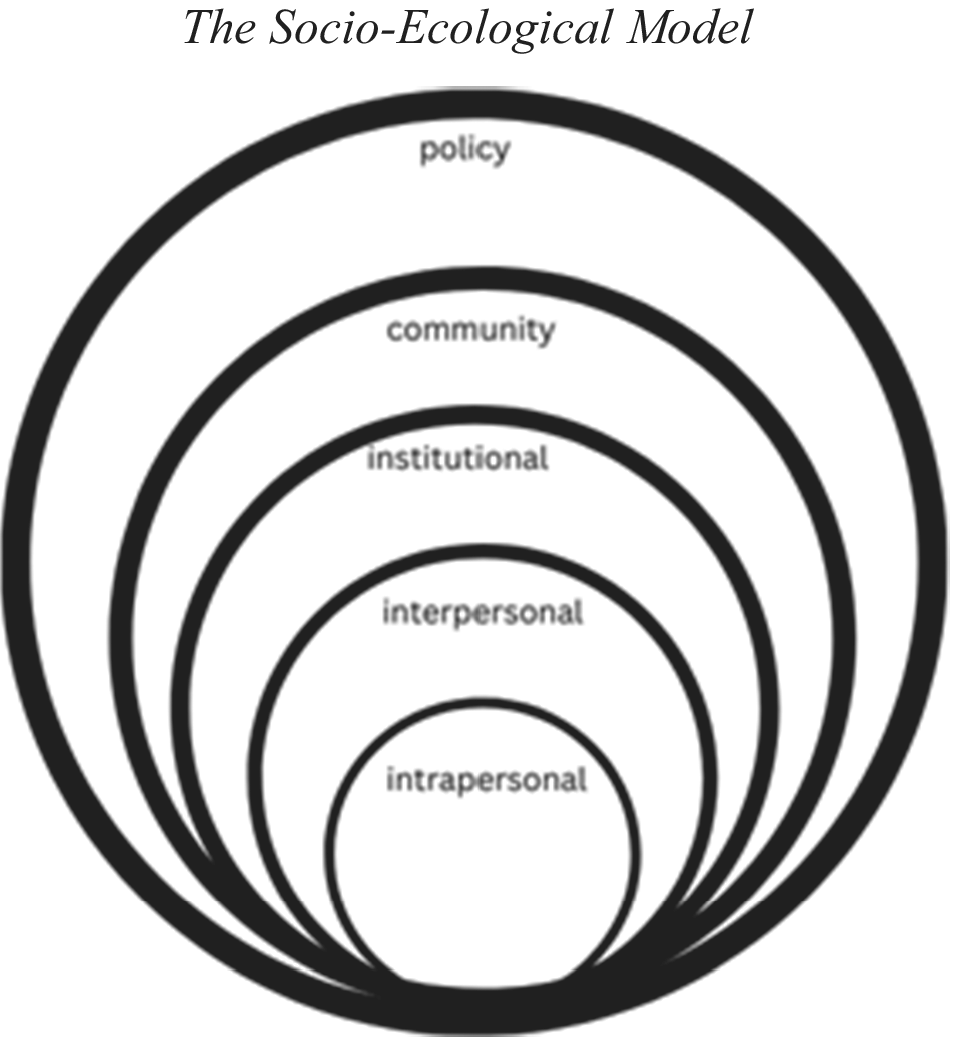
The socio-ecological model is commonly used in the field of health promotion to understand the factors that influence health behaviours. There are five levels of the socio-ecological model: intrapersonal, interpersonal, institutional, community, and policy (McLeroy et al., Reference McLeroy, Bibeau, Steckler and Glanz1988). These levels are interrelated and are outlined in Figure 1. The intrapersonal level examines the characteristics of the individual, including their attitudes, beliefs, skills, and personal history. The interpersonal level examines the relationships of the individual, including their family, close friends, and colleagues. The institutional level looks at the role of organisations or institutions, such as healthcare institutions, schools, or workplaces. The community level examines the community or town in which the individual resides. This could mean looking at the safety of the community, the resources available in the community, or the general demographics of the area. Finally, the policy level examines relevant federal, provincial, or municipal legislation and how it impacts the health behaviour of interest (McLeroy et al., Reference McLeroy, Bibeau, Steckler and Glanz1988).
The socio-ecological model.

The socio-ecological model is based on the ecological systems theory, which was published in 1977 by psychologist Urie Bronfenbrenner. The ecological systems theory suggests that human development and overall health are influenced by social and environmental factors (Brofenbrenner, Reference Brofenbrenner1977). This theory was later refined to create the socio-ecological model to focus attention on individual, social, and environmental factors that influence human health (McLeroy et al., Reference McLeroy, Bibeau, Steckler and Glanz1988). Additionally, the socio-ecological model considers the cumulative impact of individual, social, and environmental factors, and how these factors may be interrelated. The socio-ecological model can be used to better understand how environmental factors may affect people differently, depending on their individual and social factors (McLeroy et al., Reference McLeroy, Bibeau, Steckler and Glanz1988).
The socio-ecological model has been used in numerous studies to investigate aging and older adults. In Australia, the National Ageing Research Institute used the socio-ecological model to assess the interpersonal, intrapersonal, institutional, community, and policy-level factors that contribute to elder abuse. These results were used to create priorities and guidelines for reducing instances of elder abuse (Dow et al., Reference Dow, Gaffy and Hwang2018). There have also been studies that use to socio-ecological model to investigate health behaviours related to aging in place. A study out of the United Kingdom used the socio-ecological model as a theoretical framework for investigating physical activity and sedentary behaviour in older adults. The authors specifically looked at how their home environments influenced older adults’ level of physical activity and sedentary behaviour and suggested that changes must be made at the policy level to improve physical activity and sedentary behaviours in older adults (Meghani et al., Reference Meghani, Hudson, Stratton and Mullins2023).
While there are many strengths of the socio-ecological model, it is not without limitations. As discussed, the socio-ecological model assesses individual, social, and environmental factors that influence human health and highlights the complexities of health behaviours (McLeroy et al., Reference McLeroy, Bibeau, Steckler and Glanz1988). As the barriers to health are often found to be quite complex by the socio-economic model, an interdisciplinary approach is needed to help rectify the issue. Interdisciplinary and multilevel interventions can be difficult to design and implement. There are various barriers that these multi-level and interdisciplinary interventions may face, including operational challenges. Multi-level and interdisciplinary interventions can be more logistically challenging and resource-intensive to design and implement than those that are single-level or discipline. Therefore, it can be difficult to put the results of an analysis using the socio-ecological model into practice (Schölmerich & Kawachi, Reference Schölmerich and Kawachi2016). Similarly, with the complexity of barriers to health, it can be difficult to discern which levels of the model need to be prioritised for an intervention. Public health interventions are typically single-level rather than multi-level (Schölmerich & Kawachi, Reference Schölmerich and Kawachi2016). Community-based participatory research can be used to allow community members to be a part of designing the intervention. This would allow the levels of the model that seem more pressing to the community to be addressed. Another critique of the socio-ecological model is that it does not account for power. Marginalisation can have negative health implications, including high levels of stress, mood and anxiety disorders, occupational injury, and limited healthcare access (Baah et al., Reference Baah, Teitelman and Riegel2020). The lack of emphasis on power in the socio-ecological model means that considerations for marginalisation and empowerment are not included in potential interventions.
Aging in place
Many Canadian older adults express interest in aging in place, or remaining in their homes or communities, rather than living in a long-term care facility (Forum of Federal/Provincial/Territorial Ministers Responsible for Seniors, 2015). Many older adults feel the decision to age in place has to do with maintaining their independence and ability to make choices for themselves and feel that moving into long-term care or another form of continuing care would mean they need to become more dependent on others (Wiles et al., Reference Wiles, Leibing, Guberman, Reeve and Allen2011). However, to successfully age in place, one needs a variety of supports such as transportation, housing, and social support (Choi, Reference Choi2022; Wiles et al., Reference Wiles, Leibing, Guberman, Reeve and Allen2011).
As noted by the socio-ecological model, the environment one resides in plays a key role in one’s health. The concept of ‘age-friendly cities’ has been introduced by the World Health Organization (2007) to help older adults remain active in their communities as they age. The elements of a community that contribute to the age-friendliness of a city include housing, transportation, social inclusion, and communication and information (World Health Organization, 2007). Additionally, the landscape and built environment of a community are known to affect the activity levels and overall health of older adults (Zheng & Yang, Reference Zheng and Yang2019). Furthermore, the presence of age-friendly community features, such as adequate housing, transportation, and opportunities for social participation, is associated with cities being perceived as age-friendly by older adults and aging in place, as well as with a high self-perceived quality of life (Choi, Reference Choi2022; Vanleerberghe et al., Reference Vanleerberghe, De Witte, Claes, Schalock and Verte2017).
However, while many factors may increase the likelihood, and improve the experience, of aging in place, some factors may make it more challenging for an individual to age in place. As mentioned, housing is an important factor for aging in place, and if someone’s home is physically unfit, it would make aging in place more challenging. Adequate housing must be affordable, accessible, secure, and habitable (Office of the United Nations High Commissioner for Human Rights, 2009). Another important factor for aging in place is transportation. As a quarter of Canadian older adults do not have a driver’s license, an area must have adequate public transportation and good walkability to allow older adults to remain independent as they age (World Health Organization, 2007; Yarker et al., Reference Yarker, Doran and Buffel2024). Finally, social participation is an important factor that predicts satisfaction with aging in place. Those who do not have the social support of family, friends, or other community members may find themselves feeling lonely or isolated. Additionally, those who do not have many social connections may have a lower perceived quality of life (Vanleerberghe et al., Reference Vanleerberghe, De Witte, Claes, Schalock and Verte2017; Wiles et al., Reference Wiles, Leibing, Guberman, Reeve and Allen2011; Yarker et al., Reference Yarker, Doran and Buffel2024). Additionally, as people age, they may rely on the support of their social network to act as informal caregivers, and those without social support would need to hire services to supplement their needs (Wiles et al., Reference Wiles, Leibing, Guberman, Reeve and Allen2011). An important note is that communities across Canada do not all face the same challenges, and therefore, older adults across Canada will require different supports depending on their needs (Government of Canada, 2023).
Since many older adults are left with unmet needs with the currently accepted concept of aging in place, it is not surprising that there are critiques. There are claims that the current concept of aging in place places too much emphasis on informal caregivers. Caregiving for an older friend or relative can be challenging, and informal caregivers can increasingly experience negative impacts from their role. This may even lead to poor health outcomes for the caregiver (Horner & Boldy, Reference Horner and Boldy2008; Ratayake et al., Reference Ratayake, Lukas, Brathwaite, Neave and Henry2022). Additionally, older adults who rely on informal caregivers may experience feelings of discomfort or guilt over the change in their relationship with their informal caregiver (Horner & Boldy, Reference Horner and Boldy2008). Some argue that the emphasis on aging in place in policy allows governments to avoid paying for structural support for older adults (Vanleerberghe et al., Reference Vanleerberghe, De Witte, Claes, Schalock and Verte2017). Another critique of aging in place is an overemphasis on housing. Naturally, housing is a very important part of aging in place; however, caring for a home can be a daunting task and can lead to a decrease in an older adult’s quality of life (Vanleerberghe et al., Reference Vanleerberghe, De Witte, Claes, Schalock and Verte2017). Additionally, while much of the literature and policy on aging in place focuses on housing, many do not have enough emphasis on issues such as transportation, opportunities for recreation and physical activity, social and cultural engagement, and ongoing education (Ratayake et al., Reference Ratayake, Lukas, Brathwaite, Neave and Henry2022; Wiles et al., Reference Wiles, Leibing, Guberman, Reeve and Allen2011; Yarker et al., Reference Yarker, Doran and Buffel2024). Finally, while many older adults do express interest in aging in place, they are often not consulted or asked for input on policy related to aging in place (Wiles et al., Reference Wiles, Leibing, Guberman, Reeve and Allen2011).
The socio-ecological model and aging in place in rural areas
An estimated 23% of Canada’s older adults live in rural areas, and this number is expected to increase as many older Canadians choose to move from cities to rural areas and small towns (Forum of Federal/Provincial/Territorial Ministers Responsible for Seniors, 2006). People who live in rural and remote areas may face unique challenges that could impact their ability to age in place. Additionally, rural older Canadians may lack support and resources that would allow them to remain independent, such as home care support or cleaning services (Forum of Federal/Provincial/Territorial Ministers Responsible for Seniors, 2006). The socio-ecological model would allow researchers to do a thorough analysis of the factors that influence a rural-dwelling older adult’s ability to age in place and identify any unique barriers that the older adult faces. The socio-ecological model allows the researcher to better understand the nuances of a given area. Recommendations could be made based on the analyses to better address the unique challenges faced by rural-dwelling older adults in their efforts to remain in place as they age.
Intrapersonal factors that influence aging in place in rural areas
Intrapersonal factors that influence one’s ability to age in place would not differ significantly depending on where an individual lives. An intrapersonal factor that influences one’s ability to age in place is the individual’s perception of themselves. Those with positive beliefs about their ability to remain independent were more likely to be able to do so. Rural communities often have a culture of self-reliance and self-sufficiency, and rural residents tend to value independence and resiliency (Bacsu et al., Reference Bacsu, Jeffery, Abonyi and Johnson2014). Another intrapersonal factor that would influence one’s ability to age in place is their health status. Those with complex medical needs may require additional support and would be better suited to a long-term care facility (Horner & Boldy, Reference Horner and Boldy2008). In a review of the variations in health between rural and urban areas, it was found that residents of rural areas had higher self-perceived levels of health status. Rural older adults have also reported recognising the importance of maintaining their health and report engaging in physical activity and cognitive exercises to support this goal (Bacsu et al., Reference Bacsu, Jeffery, Abonyi and Johnson2014). The high levels of health behaviours and outcomes in rural areas may help rural older adults successfully age in place.
Interpersonal factors that influence aging in place in rural areas
An interpersonal factor that influences one to age in place is their social network. Social interaction is considered essential for aging in place, and in a study on rural aging, Canadian older adults identified social interaction as a key facilitator to positive perceptions of aging in place (Bacsu et al., Reference Bacsu, Jeffery, Abonyi and Johnson2014). Many rural residents reported intentionally engaging with their social circles and noted the importance of friendships and close family relationships (Bacsu et al., Reference Bacsu, Jeffery, Abonyi and Johnson2014). Rural residents often have a strong sense of belonging to their community and are more likely to know all or most of their neighbours compared to urban residents (Turcotte, Reference Turcotte2005). In a study comparing Canadian older adults in rural and urban environments, it was found that rural older adults tend to report higher levels of social support than those who live in urban areas (Iverson et al., Reference Iverson, Schulze, Gill, Switkowski, Kelly and Ashe2025). Additionally, rural residents, including older adults, were more likely to volunteer their time with service clubs or organisations. Rural older adults participated in social activities associated their neighbourhoods with a sense of belonging and trustworthiness (Turcotte, Reference Turcotte2005). The higher levels of social support experienced by rural older adults help to improve their aging in place experience (Iverson et al., Reference Iverson, Schulze, Gill, Switkowski, Kelly and Ashe2025).
Institutional factors that influence aging in place in rural areas
An institutional factor that influences one’s ability to age in place in a rural area is access to health care. Rural communities face challenges in recruiting and retaining primary care physicians and other health care practitioners. Nearly 20% of Canadians and 25% of Canadian older adults live in rural areas, but only 8% of Canadian physicians work in rural areas. As a result, many residents of rural areas do not have a family doctor and have poor continuity of care for chronic conditions (Forum of Federal/Provincial/Territorial Ministers Responsible for Seniors, 2006; Wilson et al., Reference Wilson, Rourke, Oandasan and Bosco2020). Many rural Canadians are forced to travel long distances to access health care, which can be time-consuming and difficult, especially for those without access to transportation (Iverson et al., Reference Iverson, Schulze, Gill, Switkowski, Kelly and Ashe2025; Hansen et al., Reference Hansen, Newbold, Scott, Vrkljan and Grenier2020; Skinner & Winterton, Reference Skinner and Winterton2018). Virtual health care has recently become more prevalent in Canada, which allows rural residents who have access to a phone or internet to access health care without the need to travel (Canadian Institute for Health Information, 2022). However, many older adults lack experience using technology and may struggle to use technology to access health care (Canadian Institute for Health Information, 2022; Elliot et al., Reference Elliot, Kosteniuk, O’Connell, Cameron and Morgan2024). Additionally, the recent COVID-19 pandemic led to more reliance on virtual services in the health care system, which has further isolated older adults who may struggle to use such services (Canadian Institute for Health Information, 2022; Elliot et al., Reference Elliot, Kosteniuk, O’Connell, Cameron and Morgan2024). Moreover, access to health care is a common concern expressed by older Canadians when it comes to aging in place, and many older adults report a preference for health care to be received close to their homes (Elliot et al., Reference Elliot, Kosteniuk, O’Connell, Cameron and Morgan2024).
In addition to health care access, rural residents may experience limitations in access to community resources, such as physical activity facilities or financial institutions (Iverson et al., Reference Iverson, Schulze, Gill, Switkowski, Kelly and Ashe2025). However, churches and faith-based institutions are often prominent in rural communities, with many offering volunteer services that benefit older adults, such as meal delivery services or social events. These volunteer services, along with the opportunities for socialisation provided by churches, can positively influence the aging in place experience for rural dwelling older adults (Bacsu et al., Reference Bacsu, Jeffery, Abonyi and Johnson2014; Iverson et al., Reference Iverson, Schulze, Gill, Switkowski, Kelly and Ashe2025).
Community factors that influence aging in place in rural areas
A factor that influences one’s ability to age in place at the community level is housing. Rural Canadians face unique challenges when it comes to housing. Rural areas tend to have limited rental options, which makes housing inaccessible for those who cannot afford to purchase a house, including newcomers and people with low incomes. The housing market in rural areas is less dynamic than in urban areas, and there is less new development, leading to limited availability of housing (Government of Canada, 2023). Additionally, people with a lower income are also more likely to live in areas with poor landscaping and an inaccessible built environment (Choi, Reference Choi2022; Ratayake et al., Reference Ratayake, Lukas, Brathwaite, Neave and Henry2022; Vanleerberghe et al., Reference Vanleerberghe, De Witte, Claes, Schalock and Verte2017; Zheng & Yang, Reference Zheng and Yang2019). People with complex medical and physical needs may also struggle with housing, as they would need accessible housing to support their changing mobility needs. This would mean finding an accessible home in their community or modifying their existing home, which can be prohibitive for those with a lower income (Choi, Reference Choi2022; Vanleerberghe et al., Reference Vanleerberghe, De Witte, Claes, Schalock and Verte2017).
Another factor for aging in place at the community level is transportation. As people age, many restrict or cease driving, often due to health concerns. This is of increased concern in rural areas, which commonly have no public transportation and poor walkability. Rural older adults often report the desire to walk, bike, or use public transit for their daily transportation needs, but it is not practical or possible (Hansen et al., Reference Hansen, Newbold, Scott, Vrkljan and Grenier2020). In such areas, access to a vehicle and the ability to drive are required to meet one’s basic needs, such as grocery stores, pharmacies, and health care (Hansen et al., Reference Hansen, Newbold, Scott, Vrkljan and Grenier2020; Ratayake et al., Reference Ratayake, Lukas, Brathwaite, Neave and Henry2022; Skinner & Winterton, Reference Skinner and Winterton2018). A restriction or cessation of driving is linked to social isolation, loneliness, perceived loss of independence, and poor health status (Hansen et al., Reference Hansen, Newbold, Scott, Vrkljan and Grenier2020; Ratayake et al., Reference Ratayake, Lukas, Brathwaite, Neave and Henry2022). Many rural older adults report that if they could no longer drive, they would be forced to move, despite their desire to remain in their home communities (Hansen et al., Reference Hansen, Newbold, Scott, Vrkljan and Grenier2020).
Access to nutrient dense foods can be a challenge for older adults who live in rural areas (Govindaraju et al., Reference Govindaraju, Owen and Mccaffrey2022). As mentioned, many rural residents are forced to travel far distances to reach grocery stores and other necessities (Skinner & Winterton, Reference Skinner and Winterton2018). The groceries available in rural areas tend to be less varied and with fewer fruit and vegetable options (Govindaraju et al., Reference Govindaraju, Owen and Mccaffrey2022; Skinner et al., Reference Skinner, Burnett, Williams, Martin, Stothart, Leblanc, Veeraraghavan and Sheedy2016). The quality and freshness of foods available are often impacted by the fact that they need to travel far distances to reach rural and remote grocery stores, with some foods showing visible signs of expiration or mold in remote grocery stores (Skinner et al., Reference Skinner, Burnett, Williams, Martin, Stothart, Leblanc, Veeraraghavan and Sheedy2016). These factors limit the food security of rural residents. Food insecurity results from a lack of adequate and secure access to food (Gundersen & Seligman, Reference Gundersen and Seligman2017; Tarasuk & Mitchell, Reference Tarasuk and Mitchell2020). Older adults who live in rural areas may experience additional barriers to their food security as a result of their age, including financial barriers and health status changes associated with aging (Gundersen & Seligman, Reference Gundersen and Seligman2017; Tarasuk & Mitchell, Reference Tarasuk and Mitchell2020). Food insecurity is associated with negative health outcomes, including malnutrition, depression, and poor health status (Gundersen & Seligman, Reference Gundersen and Seligman2017).
Policy factors that influence aging in place in rural areas
In a review of aging in place policies, it was found that many rural municipalities do not have policies in place that mention aging in place or adapting to an aging population (Russell et al., Reference Russell, Skinner and Colibaba2021). Of those that do, finances can be an issue. Funding is often critical to enacting age friendly programming and policy, but often funding from the government is insufficient. Typically, staff need to be hired to support age friendly programs and initiatives, and after paying a salary, there is little funding left for implementing and sustaining these programs (Russell et al., Reference Russell, Skinner and Colibaba2021). Additionally, rural communities may not have the population capacity to support age-friendly programs or initiatives (Russell et al., Reference Russell, Skinner and Colibaba2021; Skinner & Winterton, Reference Skinner and Winterton2018). Many rural areas are experiencing a decline in population in Canada, and this can have cascading effects on age friendly programming in rural areas, as they do not have a sufficient population to provide enough volunteers to participate in the program (Russell et al., Reference Russell, Skinner and Colibaba2021; Statistics Canada, 2022). Many communities report that community leaders may move away from the rural areas to access services, such as long-term care homes, and therefore, they cannot volunteer with these programs or initiatives. If there are no people available or willing to support these age friendly programs or initiatives, then the programming will not be able to sufficiently support older adults in aging in place in rural areas, regardless of policy (Skinner & Winterton, Reference Skinner and Winterton2018).
Much of the policy that impacts aging in place will differ depending on the provincial or territorial and municipal governments. Therefore, policy factors that influence an individual’s ability to age in place in a rural area will differ depending on the area in which they reside. Each of the provinces and territories has an age-friendly policy that is suited to the needs of older adults in each area, and most of these specifically address aging in place and developing age-friendly communities (Russell et al., Reference Russell, Skinner and Colibaba2021). Additionally, factors such as health care, which is critical for aging in place, are also controlled by the provincial government (Government of Canada, 2017). At the federal level, there is an intergovernmental forum of the Federal/Provincial/Territorial Ministers Responsible for Seniors, which discuss, research, and report on issues facing Canadian older adults. For example, the Forum of Federal, Provincial, and Territorial Ministers Responsible for Seniors created a guide for rural and remote communities to become more age-friendly. This group also shares resources for older adults and their caregivers, including a guide for aging in place (Forum of Federal/Provincial/Territorial Ministers Responsible for Seniors, 2006, 2015; Government of Canada, 2023). This allows for the resources and information available to Canadian older adults to be more standardised across the country since so much of policy around aging differs based on province or territory.
Implementation of the socio-ecological model
The socio-ecological model often demonstrates the complex nature of health behaviours, and therefore, addressing barriers to health behaviours can be challenging. Interventions based on the socio-ecological model tend to require an interdisciplinary effort. Implementing the findings of research done using the socio-ecological model can be challenging, as interdisciplinary or multi-level interventions can be resource-intensive. This includes financial, personal, and time resources (Schölmerich & Kawachi, Reference Schölmerich and Kawachi2016). However, the complex understanding of health behaviours that is provided by the ecological model allows for comprehensive and effective solutions (McLeroy et al., Reference McLeroy, Bibeau, Steckler and Glanz1988). A systematic review of interventions based on the socio-ecological model found that interventions that target multiple levels of the socio-ecological model were most effective (Paskett et al., Reference Paskett, Thompson, Ammerman, Ortega, Marsteller and Richardson2016). It has also been suggested that such multilevel interventions can have a broader impact on public health as the interventions may improve the health of those outside the target population (Paskett et al., Reference Paskett, Thompson, Ammerman, Ortega, Marsteller and Richardson2016). The effectiveness of interventions based on the socio-ecological model can be improved by utilising community-based participatory research. This research method involves community members in the research and gives them the power to influence the intervention (Paskett et al., Reference Paskett, Thompson, Ammerman, Ortega, Marsteller and Richardson2016). As mentioned, rural areas of Canada are not a monolith, and community-based participatory research would help to ensure that any aging in place interventions would be well suited to the needs of the community.
Neglected populations in rural aging in place research
Moving forward, the socio-ecological model could be used to assess aging in place for Indigenous Canadians, especially those who live on reserve, as this group has many unique challenges (Oosman et al., Reference Oosman, Nisbet, Smith and Abonyi2021). However, Indigenous peoples also have a unique relationship with research in Canada. Colonisation and its lasting impacts in Canada have led to the severe mistreatment of Indigenous peoples by researchers. Therefore, any researcher conducting research with Indigenous peoples must do so in an ethical and culturally sensitive manner (Government of Canada Panel on Research Ethics, 2022).
Another group that could benefit from further research when it comes to aging in place is those who have migrated, either from another country or internally within Canada. It has been suggested that the concept of aging in place is inadequate for assessing aging for this group, as their migration may have warped their sense of place. The desire to remain in place may not resonate with those who have experienced migration (Johansson et al., Reference Johansson, Laliberte Rudman, Mondaca, Park, Luborsky, Josephsson and Asaba2015). The socio-ecological model could be used to better understand the unique experiences of this group and help to modify the concept of aging in place to better suit their needs.
Similarly, the concept of aging in place may not resonate with unhoused older adults. While there is a lack of research on unhoused older adults, it is known that being unhoused can accelerate the aging process, which could impact their ability to experience healthy aging (Ontario Non-Profit Housing Association, 2016). To better understand aging in place for unhoused individuals or those in social housing, the socioeconomic model could provide a framework to analyse aging in place for unhoused individuals at multiple levels. This could aid in developing appropriate support for unhoused older adults.
Finally, rural Canada is changing. The population density of rural areas of Canada has been decreasing over time (Statistics Canada, 2022). Conversely, certain provinces and territories of Canada, namely Nunavut and Prince Edward Island, have actually experienced increases in their rural populations in recent years and therefore do not necessarily experience the same challenges associated with a decreasing population density as the rest of the country (Statistics Canada, 2022). Financial changes are also impacting rural Canada, as the economies of many rural areas are suffering. Climate change is having a direct effect on natural resources industries, such as fishing and forestry, which many rural communities rely on. This is impacting the employment opportunities of rural areas and, thus, influences young people to choose to move to urban areas (Government of Canada, 2023). These changes can greatly impact the aging experience of rural-dwelling older adults, as they may impact the resources available to them and their social network. Future research could focus on investigating how changes to Canada’s rural communities impact the older adults who live there.
Conclusion
Many older Canadians are expressing interest in remaining in their home communities and maintaining independence as they age (Forum of Federal/Provincial/Territorial Ministers Responsible for Seniors, 2015). Based on this discussion, it is evident that more research is needed on aging in place in rural Canada. The socio-ecological model assesses factors that influence health at the intrapersonal, interpersonal, institutional, community, and policy levels and could serve as the theoretical framework to further investigate aging in place in rural Canada (McLeroy et al., Reference McLeroy, Bibeau, Steckler and Glanz1988). This paper highlighted some of the unique factors that impact aging in place in rural Canada at each level of the socio-ecological model. However, different rural areas will need to be studied separately, as rural Canada is not a monolith, and each community will have unique factors that impact aging in place. A better understanding of the barriers that rural-dwelling older Canadians face will allow for multilevel and effective interventions to enhance the aging in place experience for Canadians.
Competing interests
The authors declare no conflicts of interest.

 Open access
Open access