



Shift work, increasingly common in industrialised societies, poses significant challenges to human health(Reference Hulsegge, Proper and Loef1). It is defined as a labor practice that includes a wide range of schedules such as evening or night shifts, irregular or rotating shifts, weekend work or on-call duties(Reference Rivera, Akanbi and O’Dwyer2). According to the Sixth European Working Conditions Survey, approximately 21 % of workers engage in permanent or rotating shift work, and 19 % perform shifts that include night work(Reference Parent-Thirion, Biletta and Cabrita3). This irregularity often results in circadian misalignment, which contributes to metabolic, cardiovascular and psychological disorders, with type 2 diabetes (T2D) being among the most frequently reported metabolic disorders associated with circadian misalignment(Reference Xie, Hu and Fu4–Reference Reutrakul and Van Cauter6).
Disruption of the circadian system, commonly referred to as chronodisruption, has been identified as a key mediator of the health effects associated with shift work. Irregular light exposure, sleep deprivation and misalignment between endogenous biological rhythms and behavioural cycles (e.g. feeding and activity) contribute significantly to metabolic dysregulation in shift workers, especially in those who work night shifts(Reference Khan, Duan and Yao7–Reference Pandi-Perumal, Cardinali and Zaki9). Furthermore, shift workers often exhibit poorer dietary habits, including increased intake of energy-dense snacks, irregular meal timing and reduced consumption of fresh, balanced meals. These patterns are driven by fatigue, lack of structured mealtimes, stress and limited access to healthy food during night shifts. Social isolation during meals and skipping family meals may further compromise diet quality(Reference Hulsegge, Proper and Loef1,Reference Pepłońska, Nowak and Trafalska10) . Altogether, these lifestyle disruptions exacerbate the physiological consequences of circadian misalignment, including impaired glucose metabolism, increased insulin resistance and elevated risk of weight gain and T2D(Reference Bass and Takahashi11,Reference Stenvers12) . These findings highlight the urgent need for dietary strategies tailored to shift-working populations that may reduce the adverse health impacts of circadian misalignment by addressing irregular meal timing and inappropriate or mis-timed distribution of nutrients.
Among dietary strategies targeting metabolic improvement in this population, hypoenergetic diets have been shown to promote weight loss and improve glycaemic outcomes in adults with overweight/obesity and type 2 diabetes(Reference Lin, Cienfuegos and Ezpeleta13,Reference Churuangsuk, Hall and Reynolds14) . However, intervention evidence specifically in shift workers remains limited, although recent trials suggest beneficial effects on body composition and metabolic parameters(Reference Sooriyaarachchi, Jayawardena and Pavey15). High-protein diets, particularly within energy-restricted interventions, have been associated with improvements in glycaemic control and other cardiometabolic parameters in individuals with T2D(Reference Szczerba, Barbaresko and Schiemann16,Reference Clina, Sayer and Pan17) . These findings are consistent with the evidence-based recommendations of the European Association for the Study of Diabetes, which indicate that higher protein intakes may be recommended in the short term within energy-restricted weight-loss diets in individuals with T2D and overweight/obesity, provided that renal function is preserved(Reference Aas, Axelsen and Churuangsuk18).
The mechanisms underlying the metabolic benefits of high-protein diets are not yet fully elucidated, but they may involve the insulinotropic effect of amino acids, better maintenance of muscle mass after weight loss and enhanced satiety, among others(Reference Guarneiri, Kirkpatrick and Maki19). Essential amino acids (especially branched chain amino acids) stimulate mammalian target of rapamycin complex, which is a key regulator of muscle growth and protein synthesis. Besides, proteins stimulate incretin secretion (glucagon-like peptide-1 and glucose-dependent insulinotropic polypeptide), which are essential in glucose homoeostasis by enhancing insulin secretion and suppressing glucagon release(Reference Dandona, Ghanim and Chaudhuri20,Reference Soenen, Martens and Hochstenbach-waelen21) . In shift workers, evidence from one controlled trial indicates that high-protein diets may reduce glucose and insulin levels and improve psychometric performance, while high-carbohydrate diets have been associated with increased fatigue and suboptimal glycaemic control(Reference Paz and Berry22).
Recent evidence suggests that adding protein to carbohydrate-containing meals may modulate postprandial glucose responses(Reference Wolever, Zurbau and Koecher23,Reference Davis, Bonham and Nguo24) . Diurnal variation in glucose homoeostasis has been well documented; oral glucose tolerance and insulin sensitivity are higher in the morning, so carbohydrate consumption early in the day is likely to elicit a more favourable postprandial glycaemic response. Thus, within the broader framework of chrononutrition, the alignment of food intake with circadian physiology may be relevant for metabolic regulation(Reference Katsi, Papakonstantinou and Soulaidopoulos25,Reference Johnston, Ordovás and Scheer26) . Shift workers often exhibit higher postprandial glucose levels during night shifts(Reference Sharma, Laurenti and Dalla Man27), and some evidence suggests a high-protein meal consumed at evening/night-time may lead to more favourable postprandial responses than a standard meal(Reference Davis, Bonham and Nguo24). Accordingly, allocating a greater proportion of protein to the evening/night-time period may be a relevant strategy to explore in shift workers. Despite these insights, previous studies on shift workers are limited by small sample sizes, short intervention periods and a lack of focus on individuals with T2D. Moreover, the potential role of the distribution of protein intake across the day, particularly the proportion consumed during the evening/night-time meal window, remains insufficiently studied in this population. Therefore, further research is needed to explore whether different patterns of protein distribution within a hypoenergetic diet may influence glycaemic control and body composition in this population. We hypothesise that within hypoenergetic high-protein diets, allocating a greater proportion of daily protein intake to the evening/night-time period may lead to greater improvements in glycaemic control and body composition than allocating a smaller proportion of protein to that period in shift workers with impaired glucose metabolism and overweight or obesity.
This study protocol describes a three-arm, randomised controlled trial in shift workers with overweight or obesity and prediabetes or T2D, comparing the effects of three distinct hypoenergetic diets with varying macronutrient composition and protein distribution across the day on metabolic outcomes. The findings may contribute to the development of more tailored nutritional strategies for shift-working populations.
Therefore, this protocol describes a three-arm, randomised controlled trial designed to evaluate the effects of three distinct hypoenergetic diets – differing in macronutrient composition and distribution of protein intake across the day – on metabolic outcomes in shift workers with prediabetes or T2D and overweight or obesity. The primary objective is to assess changes in glycaemic parameters — mainly HbA1c concentration — and body composition. Secondary objectives include evaluating the impact of the interventions on lipid profile, adipokine concentration, sleep quality and health-related quality of life. The study will also assess chronotype, physical activity, sedentary behaviour and dietary intake as additional variables relevant to the interpretation of the study results. All outcomes will be measured over a 12-week intervention period.
Materials and methods
Study design
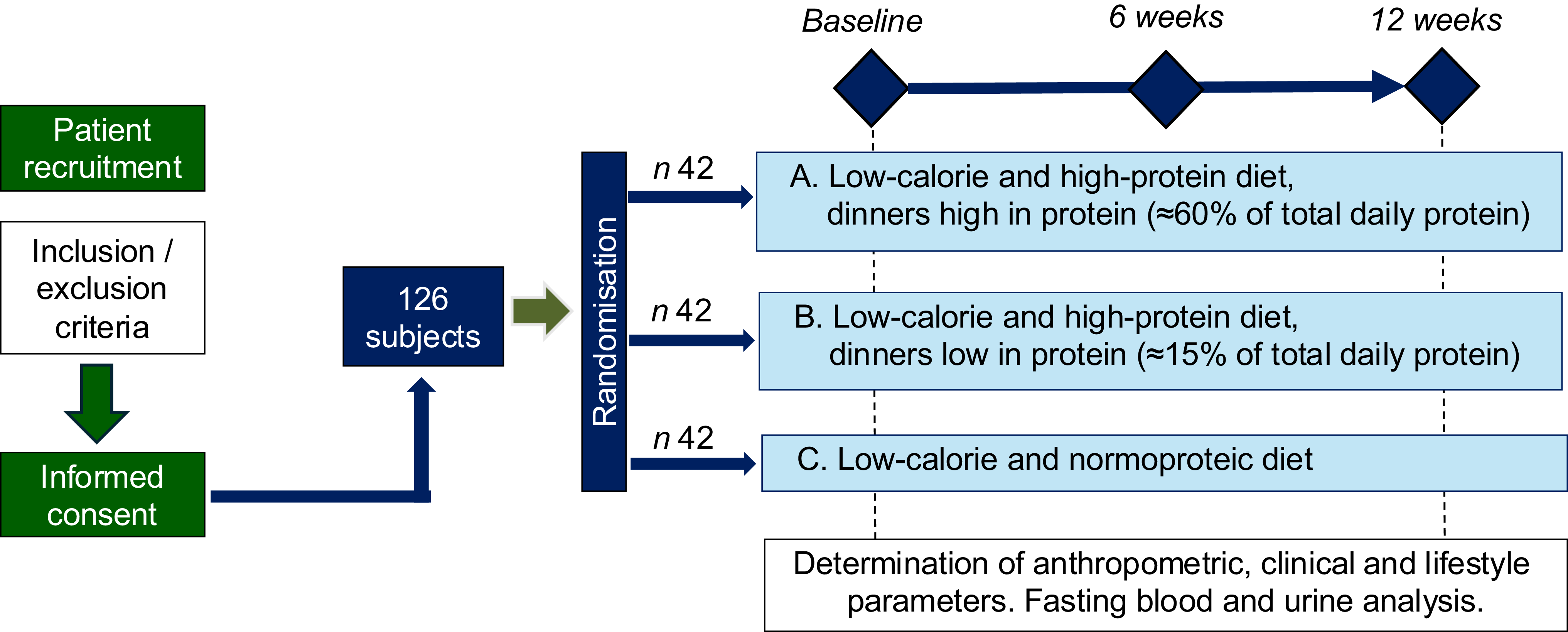
This study is a 12-week, three-arm, parallel-group, single-blind randomised controlled trial conducted in adult shift workers with prediabetes or T2D and overweight or obesity. The study started in September 2024 and is expected to be completed in December 2025. Eligible participants must be engaged in shift work that includes, on average, at least one night shift per month, either as part of a rotating schedule or as fixed night work. Participants are individually randomised in a 1:1:1 ratio to one of three dietary interventions: (A) high-protein with protein-enriched dinner (50–60 % of daily protein); (B) high-protein with protein-restricted dinner (10–20 % of daily protein) or (C) normoproteic control diet with usual protein distribution. The study comprises four visits: a prescreening visit, a baseline visit and follow-up assessments at 6 and 12 weeks post-randomisation, during which all study data are collected. A visual summary of the study design is provided in Figure 1.
Overview of the study design. Eligible participants (n 126) are randomised into one of three hypoenergetic dietary intervention arms (A, B or C) differing in total protein content and its distribution across meals. The intervention lasts 12 weeks, with assessments at baseline, week 6 and week 12. All participants undergo anthropometric, clinical and lifestyle evaluations, as well as fasting blood and urine analyses.

Figure 1. Long description
The flowchart begins with patient recruitment, followed by inclusion and exclusion criteria, and informed consent. 126 subjects are randomized into three groups of 42 each. Group A follows a low-calorie and high-protein diet with dinners high in protein. Group B follows a low-calorie and high-protein diet with dinners low in protein. Group C follows a low-calorie and normoproteic diet. Assessments occur at baseline, 6 weeks, and 12 weeks, including anthropometric, clinical, and lifestyle parameters, as well as fasting blood and urine analysis.
The randomisation sequence is generated using R statistical software by an investigator not involved in participant recruitment or outcome assessment, ensuring allocation concealment. To minimise assessment bias, investigators involved in dual-energy X-ray absorptiometry (DXA) measurements and laboratory analyses will be different from those delivering the dietary intervention and will remain unaware of participants’ group allocation. Randomisation is stratified by sex and by type of shift pattern, categorised as either high-frequency rotating shifts within the same week or fixed night shifts and weekly rotational blocks.
The intervention period lasts 12 weeks. Participants attend three in-person visits: one at baseline (week 0), one at week 6 (midpoint follow-up) and one at week 12 (end of intervention). In addition, a pre-screening visit is conducted prior to enrollment to verify eligibility and obtain informed consent. Participants also have access to the study dietitian throughout the trial via phone, WhatsApp or email to resolve questions and reinforce dietary guidance.
The study is conducted at the Clinical Research Unit of the Institute for Health Research Aragón, located within the Miguel Servet University Hospital in Zaragoza (Spain). All assessments are standardised and performed under controlled conditions. The trial is registered at ClinicalTrials.gov (identifier: NCT06912555) and has been approved by the institutional ethics committee (Research Ethics Committee of the Autonomous Community of Aragon; PI23-558). Written informed consent will be obtained from all participants prior to enrollment. In addition, at the first visit – together with the study explanation and the participant information sheet and prior to signing the informed consent – participants are clearly informed that they could withdraw from the study at any time, whether for personal or medical reasons, because the dietary intervention is not suitable for them, or for any other reason they consider appropriate. All withdrawals and their reasons are recorded throughout the study. The study protocol has been developed in accordance with the principles of the Declaration of Helsinki and adheres to the Standard Protocol Items: Recommendations for Interventional Trials guidelines(Reference Chan, Tetzlaff and Gotzsche28).
Study population
Recruitment will be carried out through a coordinated, multi-step process designed to ensure transparency and voluntary participation. Participant recruitment will be achieved by publicising the study through local media and displaying information posters in healthcare facilities and large companies with substantial shift-working staff. The study announcement will include a dedicated telephone number and email address through which interested individuals may contact the research team. Upon initial contact, potential participants will receive detailed information regarding the study’s objectives, procedures and eligibility criteria. Those expressing interest and meeting the basic requirements will be invited to a pre-screening visit at the Clinical Research Unit to confirm eligibility.
Inclusion criteria include (a) women and men aged ≥ 18 years; (b) body mass index (BMI) between 27·5 and 40 kg/m2; (c) diagnosis of prediabetes (fasting glucose 100–125 mg/dl and/or HbA1c 5·7–6·4 %) or T2D (fasting glucose ≥ 126 mg/dl and/or HbA1c ≥ 6·5 % and/or currently taking metformin), according to the American Diabetes Association criteria(29); (d) current employment in shift work that includes, on average, at least one night shift per month, either as part of a rotating schedule or as fixed night work, and expected to continue throughout the study period; (e) provision of written informed consent after having read the participant information sheet and clarified any doubts. Participants who meet any of the following criteria will be excluded: (a) treatment with any antidiabetic agents (oral or injectable), including insulin, within the past 2 months, except for metformin or dipeptidyl peptidase-4 inhibitors, which must have been taken at a stable dose for at least 6 months prior to enrollment; (b) use of lipid-lowering or glucose-modifying medications or functional foods (e.g. phytosterols, red yeast rice) unless taken in a stable regimen for a minimum of 6 months prior to enrollment and expected to remain unchanged throughout the study; (c) presence of uncontrolled chronic or endocrine diseases (e.g. cardiovascular, renal, hepatic or thyroid disorders) that could interfere with study outcomes, in the judgement of the investigators; (d) body weight variation of ≥ 5 % during the 3 months preceding enrollment; (e) unstable use of vitamin or nutritional supplements within the 6 months prior to the study; (f) regular alcohol consumption exceeding 30 g of ethanol per day; (g) pregnancy or intention to become pregnant during the study period; (h) any other circumstance that, in the opinion of the investigators, may compromise adherence to the nutritional intervention (e.g. frequent travel, inability to attend scheduled visits) or interfere with study results (e.g. any serious medical condition).
Randomisation and blinding
Participants will be randomly assigned in a 1:1:1 ratio to one of the three dietary intervention arms using computer-generated block randomisation. Stratification will be performed based on sex (male/female) and type of shift pattern (high-frequency rotating shifts within the same week v. weekly rotating or fixed night shifts), in order to ensure balanced allocation across key variables. The randomisation sequence will be generated using the block_ra() function from the randomizr package in R, with a fixed seed to ensure reproducibility.
The study follows a single-blind design. Participants will be unaware of the specific dietary group to which they are assigned, including the caloric prescription. Although investigators will withhold information on energy content, protein amount and specific diet allocation, complete blinding cannot be ensured because participants may infer their assignment from the menus provided. Investigators responsible for statistical analysis and outcome assessment will remain blinded to group allocation throughout the trial. The dietitians responsible for delivering the nutritional intervention will not be blinded, due to the practical and methodological requirements of dietary counseling and adherence monitoring. Group allocation will be concealed at the time of enrollment. Randomisation will be managed by a researcher not involved in recruitment, data collection or outcome evaluation, and assignment will be recorded in a masked database to maintain allocation concealment.
Dietary intervention
All participants receive an individually tailored hypoenergetic diet designed to induce a moderate caloric restriction of approximately 30 % of their estimated total energy expenditure, equivalent to a reduction of 400–600 kcal/d. Total energy expenditure is calculated individually for each participant based on validated predictive equations and clinical assessment. Caloric intake is never prescribed below 1200 kcal/d, in order to ensure that all nutritional requirements are met.
Participants are randomised to one of three dietary intervention arms, which differ in both total protein intake and the proportion of protein allocated to the evening/night-time period:
-
• HP Diet A (High-protein, protein-dominant dinner): A hypoenergetic diet providing 1·3–1·5 g of protein per kilogram of body weight per day, with approximately 60 % of the total daily protein allocated to the evening meal (consumed between 20.00 and 03.00).
-
• HP Diet B (High-protein, protein-restricted dinner): A hypoenergetic diet also providing 1·3–1·5 g protein/kg/d, but with only ∼15 % of total daily protein intake assigned to the evening meal (20·00–03·00).
-
• NP Diet C (Normoproteic control diet): A hypoenergetic diet providing 0·8 g of protein per kilogram of body weight per day, with protein intake distributed according to the participant’s usual habits and preferences, aiming for a relatively homogeneous intake across the day.
A predefined evening/night-time window (20·00–03·00) was established to standardise the intervention across participants with heterogeneous shift schedules and eating habits and to capture the main intake occurring during the latter part of the day/night. The trial was designed to compare protein allocation within this standardised evening/night-time window rather than the effects of specific clock times within that interval. The exact timing of intake will be recorded, although the study was not designed to compare narrower time points.
Macronutrient distribution remains consistent across groups (30 % of fat and the rest of calories coming from carbohydrates), aside from the variations in protein content and evening/night-time protein allocation. Each participant receives a detailed dietary prescription that includes structured meal plans specifying recommended food groups and quantities, sample menus with specific dishes to facilitate adherence and individualised nutritional counseling. A sample daily menu for each diet is provided in S1 Appendix.
Dietary adherence will be monitored using both dietary records and an objective biomarker. Participants will complete food records that include the timing of each eating occasion, allowing assessment of whether protein intake is consumed within the prescribed evening/night-time meal window and in the assigned proportion. In addition, urinary urea will be used as an objective marker of protein intake to evaluate whether participants are achieving the prescribed protein targets. Together, these measures will be used to assess adherence to both the amount and distribution of protein intake during the intervention.
Outcomes
The primary outcomes of this trial are glycaemic parameters – mainly HbA1c concentration – and body composition change after 12 weeks of intervention. HbA1c is a well-established marker of long-term glycaemic control and a reliable indicator of the risk of chronic diabetes-related complications; accordingly, it constitutes the principal therapeutic target in individuals with prediabetes and T2D. Additional glycaemic outcomes include fasting plasma glucose, fasting insulin and the homeostasis model assessment of insulin resistance. Body composition outcomes include total body fat, fat-free mass and visceral adipose tissue variation after 12 weeks post-randomisation.
Secondary outcomes comprise lipid profile (total cholesterol, triglycerides, HDL-cholesterol, LDL-cholesterol and non-HDL-cholesterol), adipokines concentration (asprosin, visfatin and apelin), sleep quality and health-related quality of life. Other clinical, biochemical and lifestyle parameters will be recorded to monitor health changes throughout the intervention in order to identify potential confounders. Clinical variables include blood pressure and chronotype; biochemical variables involve hepatic, renal or thyroid function assessment, among others and lifestyle parameters include dietary characteristics and objectively measured physical activity and sedentary behaviour.
Data collection and assessment procedures
Study visits
As outlined in Figure 1, participants will attend a pre-screening visit at which eligibility criteria will be verified and written informed consent obtained. If no laboratory analysis has been performed within the preceding 2 months, blood will be drawn and the relevant clinical and demographic variables recorded. During the randomisation visit, participants will also take part in a structured dietary interview with the study dietitian to assess individual food preferences and eating habits. This information will be used to tailor the dietary plan to improve adherence while maintaining the assigned macronutrient targets; the dietary plan will be delivered within 2–3 d of the randomisation visit. Clinical, anthropometric, biochemical and lifestyle data will be collected at baseline and at the end of the 12-week intervention. A mid-intervention visit at week 6 will include all assessments except for biochemical parameters and DXA. In addition, biweekly email or phone contact will be maintained to reinforce adherence, promote follow-up and minimise dropout.
Clinical data
Demographic and medical history data, including age, sex, smoking status, medication and supplement use and blood pressure, will be collected at all study visits. Blood pressure will be measured according to standardised procedures with an automated sphygmomanometer (Omron HEM-907-E, OMRON Healthcare Europe B.V.), following international standard procedures(Reference Stergiou, Alpert and Mieke30). Participants will be sitting quietly for ≥ 5 min in a temperature-controlled, silent room with back and arm supported, feet flat on the floor, legs uncrossed and the mid-cuff of the measured arm aligned with the heart. They will be asked to refrain from talking, moving or using electronic devices during the procedure and to abstain from caffeine, smoking and vigorous exercise for ≥ 60 min beforehand. Researchers will perform two different measurements obtained 1 min apart. If systolic or diastolic values differ by ≥ 5 mmHg, a third reading will be taken and the mean of the two closest values recorded for analysis(Reference Mancia, Kreutz and Brunström31).
Anthropometric and body composition data
Body composition will be measured via DXA (software version 8.1; Lunar Prodigy, General Electrics) in accordance with manufacturer instructions and international guidelines. Participants will be asked to wear loose, lightweight and non-metallic clothing and remove all jewellery or metal objects. During the scan, they will lie supine with arms extended alongside the torso, palms facing downwards and separated by 5–10 cm, legs slightly abducted and ankles secured with Velcro straps. If the patient’s body size exceeds the scan field, a validated hemi-body protocol will be applied(Reference Hangartner, Warner and Braillon32,Reference Rothney, Brychta and Schaefer33) . The DXA output will include total body weight, total and regional fat mass and fat-free mass, abdominal subcutaneous and visceral fat. Height will be measured to the nearest 0·1 cm using a calibrated wall-mounted stadiometer (Seca 813 and Seca 217, Seca Deutschland). BMI will be calculated by dividing body weight in kilograms by the square of height in metres (kg∙m⁻2). Waist circumference will be measured with anthropometric tape midway between the lowest rib and the iliac crest (Seca 201, Seca Deutschland).
Biochemical analyses
Blood and urine samples will be obtained after an overnight fast (≥ 8 h) at baseline and at the end of the 12-week intervention. Analyses will be performed through the routine clinical laboratory services of the Miguel Servet University Hospital. Glucose concentrations will be quantified with the hexokinase method on a Beckman Coulter AU analyser (Beckman Coulter), while HbA1c will be measured by high-performance liquid chromatography (Tosoh). Insulin resistance will be estimated with the homeostasis model assessment of insulin resistance index, calculated as fasting glucose (mg/dl) × insulin (µU/ml)/405. Total cholesterol, TAG and HDL-cholesterol will be assessed by enzymatic colorimetry on the same Beckman platform; LDL-cholesterol will be derived with the Friedewald equation if TAG are < 400 mg/dl. Apolipoproteins A1 and B will be determined by kinetic nephelometry on the Beckman Coulter AU and high-sensitivity C-reactive protein by immunoturbidimetry. Fe, uric acid and albumin will be analysed colorimetrically, whereas vitamin B12 will be assayed by luminescence immunoassay. Serum and urinary creatinine will be obtained with the Jaffe’s reaction, and liver transaminases, together with urinary urea, will be quantified kinetically. Microalbuminuria will be measured by turbidimetry, while glomerular filtration rate will be estimated with the Chronic Kidney Disease Epidemiology Collaboration equation(Reference Levey, Stevens and Schmid34).
Moreover, two additional blood tubes will be collected at each time point to obtain anonymised serum aliquots, which will be stored at –80°C for batch analysis at study completion. The concentrations of adipokines will be determined in these samples using an enzyme-linked immunosorbent assay after study completion.
Dietary intake, physical activity, sedentary behaviour and sleep quality assessment
Participants will complete 5-d dietary records, including two days during morning or afternoon shifts, 2 days during night shifts and one weekend or holiday, at baseline, week 6 and week 12. Dietary data will be analysed using EasyDiet software (Biocentury, S.L.U, Barcelona, Spain), which is based on Spanish food composition tables.
Sleep quality assessment will be measured in two different ways: (1) the Pittsburgh Sleep Quality Index, a widely used self-report questionnaire that assesses sleep quality over a 1-month time interval, validated in Spanish(Reference Buysse, Reynolds and Monk35) and (2) using a three-axis accelerometer (ActiGraph wGT3X-BT, Pensacola, FL, USA), which participants will be instructed to wear on the non-dominant wrist using an adjustable Velcro strap(Reference Ward, Evenson and Vaughn36). The device will be worn continuously for eight consecutive days, removing it only for water-based activities (e.g. showering or swimming). Participants will be provided with a sleep and activity log, in which they will record their work shift schedule, bedtime and wake time, device removal times and any structured physical activity beyond routine walking. Each participant will receive oral instructions on how to wear the actigraph, keeping general recommendations and fulfilling the diary log, indicating the time of reference measurements (i.e. time to: wake up, get up, breakfast, lunch, nap, physical activity, dinner and asleep at night) and also to track all times when the device will be removed and replaced. On the eighth day, the actigraph will be returned to the investigators, and both the actigraph and the daily log will be collected. Accelerometer data will be downloaded, cleaned and analysed using the manufacturer’s software (Actilife 6 desktop). For the analysis of physical activity and sedentary behaviour, the triaxial accelerometer data will also be used. Participants will be asked to maintain their usual physical activity levels throughout the study. No specific exercise intervention or standardised exercise prescription will be provided. Physical activity will be considered in the statistical analyses where appropriate.
Chronotype assessment
The morningness–eveningness preference of each participant will be evaluated at baseline using the Horne & Östberg self-assessment questionnaire(Reference Horne and Ostberg37), a validated tool widely used to determine individual circadian typology.
Quality of life
Health-related quality of life will be assessed using the 12-Item Short-Form Health Survey (SF-12), a validated and widely used instrument that provides physical and mental health summary measures. The SF-12 has demonstrated good reliability and validity in both clinical and general populations(Reference Gandek, Ware and Aaronson38,Reference Jenkinson, Layte and Jenkinson39) . The Spanish version of the questionnaire has also been validated and shows appropriate psychometric properties, enabling accurate interpretation in this setting(Reference Monteagudo Piqueras, Hernando Arizaleta and Palomar Rodríguez40,Reference Vilagut, Valderas and Ferrer41) . Participants will complete the paper-based questionnaire during study visits, and responses will be processed using standardised scoring procedures.
Safety monitoring
Although adverse effects are not expected due to the nature of the dietary intervention, participants will be instructed to report any symptoms or concerns throughout the study, including symptoms or episodes compatible with hypoglycaemia, despite the low expected risk in this study population. All adverse events, regardless of suspected causality, will be documented and reviewed by the clinical team across the study.
Data management
All study data will be pseudonymised using a unique participant identification code. The correspondence between personal identifiers and study codes will be kept separately and will only be accessible to authorised members of the research team. Paper documents will be stored in locked cabinets within restricted-access research facilities, accessible only to researchers with authorised card access. Biological samples will be labelled with the participant study code only and stored at –80°C in restricted-access laboratory facilities. Electronic files and study databases will be managed from a password-protected computer connected to the hospital’s internal network and will be accessible only to authorised study personnel. All data and samples will be handled in accordance with the study protocol approved by the corresponding Research Ethics Committee.
Sample size
The sample size was determined based on the expected change in HbA1c, one of the study’s primary outcomes. HbA1c reflects average glycaemia over approximately 2–3 months(Reference ElSayed, Aleppo and Bannuru42), and higher levels are strongly associated with an increased risk of diabetes-related (particularly microvascular) complications(Reference Kim, Choi and Bae43). Current American Diabetes Association Standards of Care emphasise individualised HbA1c targets as a central goal of glycaemic management in populations with both prediabetic and T2D(Reference Elsayed, Aleppo and Aroda44). Based on previous dietary intervention studies in adults with T2D, the sd of HbA1c was estimated at approximately 1 percentage point(Reference Clina, Sayer and Pan17,Reference Dong, Zhang and Wang45) . Because no directly comparable long-term intervention studies are available in shift workers, the expected between-group difference was estimated conservatively based on the comparison between the two most contrasted interventions (group A v. group C), rather than on evening protein allocation alone. A difference of 0·5 percentage points in HbA1c was considered clinically relevant and biologically plausible in light of prior evidence showing improved glycaemic control with higher-protein diets in T2D and more favourable nocturnal postprandial responses after high-protein meals(Reference Clina, Sayer and Pan17,Reference Davis, Bonham and Nguo24,Reference Dong, Zhang and Wang45) . The sample size calculation was therefore based on the hypothesis that the reduction in HbA1c in intervention group A would be at least 0·5 percentage points greater than that observed in group C. Assuming a one-sided test, with a 90 % confidence level (Zₐ = 1·645) and 80 % statistical power (Zᵦ = 0·842), the required sample size was estimated at thirty-six participants per group. To account for an anticipated 15 % dropout rate, the final sample size was set at forty-two participants per group, resulting in a total of 126 participants across the three study arms.
Statistical analysis
All participants who complete the study will be included in the data analysis, independent of reported dietary compliance or weight loss, according to intention-to-treat analysis. Data will be expressed as mean (standard deviation) or median (25th–75th percentile), depending on whether the variables follow a normal or non-normal distribution, respectively. The normality of data distribution will be assessed using the Shapiro–Wilk test. Differences that occur during the study within each diet group will be evaluated by the Friedman or repeated measures ANOVA test, when analysing non-parametric and parametric variables, respectively. We will calculate differences between diet groups (group × time interaction) using a generalised linear model including log-transformed data, if applicable. Other statistical analyses will be performed using conventional methods appropriate to the distribution of each variable. All analyses will be conducted using R software (version 3.5.0), with a significance level set at P < 0·05. Any change in glucose-lowering medication during the 12-week intervention will be recorded and considered in the analyses. Participants with medication changes during follow-up will be retained in the intention-to-treat analysis, and additional sensitivity analyses excluding these cases will be performed where appropriate.
Discussion
To our knowledge, this protocol describes the first randomised controlled trial designed to evaluate the effects of three hypoenergetic dietary interventions, varying in overall macronutrient distribution and protein distribution across the day, on glycemic control, body composition and metabolic health in shift workers with prediabetes or T2D and overweight or obesity. This population faces significant metabolic risks due to chronic circadian misalignment and irregular eating patterns, for which chrononutrition has emerged as a promising but underutilised intervention strategy(Reference Raji, Kyeremah and Sears46), particularly given the observed disruptions in eating windows and macronutrient intake during night shift(Reference Pereira Marot, Tibiletti Balieiro and do Vale Cardoso Lopes47), and the broader impact on metabolic and psychosocial health(Reference Azmi, Juliana and Teng48). A review conducted by Henry CJ et al. emphasises that while intermittent fasting and macronutrient variation have been studied individually, their integration with chronobiological principles in shift workers remains an emerging field(Reference Henry, Kaur and Quek49). Furthermore, although recent tools have been developed to assess temporal eating patterns in shift-working populations, clinical trials incorporating nutrient-specific timing based on chronotype, particularly protein, are still lacking(Reference Raji, Kyeremah and Sears46,Reference Phoi, Bonham and Rogers50) . By combining nutrient composition with evening/night-time protein allocation strategies, our trial seeks to fill this gap in the evidence.
This trial has several methodological strengths. First, the 12-week intervention period is based on extensive evidence showing that this duration is sufficient to produce significant improvements in HbA1c, fasting glucose and lipid profiles in patients with T2D undergoing dietary treatment(Reference Dong, Zhang and Wang45,Reference Binou, Stergiou and Kosta51) . Second, the randomised controlled design with stratified allocation by sex and shift type strengthens internal validity and ensures balanced group assignment. Third, the intervention arms are energy-matched, differing only in macronutrient composition and temporal protein distribution, enabling a clear assessment of these dietary factors.
Moreover, the study employs a wide range of validated assessment tools and gold-standard measurements. Body composition is assessed using DXA, which is considered the gold standard for quantifying fat and lean mass(Reference Messina, Albano and Gitto52). Physical activity and sedentary behaviour and sleep patterns are objectively measured using triaxial accelerometers, which are widely used and validated in clinical research(Reference Guediri, Robin and Lacroix53). Dietary intake is analysed using structured 5-d food records entered into the EasyDiet software, and chronotype is assessed using the Horne–Östberg questionnaire(Reference Horne and Ostberg37). Additional validated questionnaires, such as the Pittsburgh Sleep Quality Index(Reference Buysse, Reynolds and Monk35) and the SF-12 for health-related quality of life(Reference Gandek, Ware and Aaronson38), provide standardised, reliable measures of key lifestyle and psychosocial variables.
While the study is designed to be methodologically robust, certain limitations should be acknowledged. Recruitment may be slower than anticipated due to the relatively strict inclusion criteria and the need to engage a working population with irregular schedules. Although a 15 % dropout rate has been anticipated in the sample size estimation, the rotating nature of shift work, personal constraints and potential disruptions to routine may still pose challenges to study retention. Additionally, the 12-week intervention period, although supported by previous evidence for eliciting clinically relevant metabolic improvements, does not allow for evaluation of long-term outcomes or sustainability of dietary changes. Furthermore, because the expected between-group difference in HbA1c was estimated in the absence of directly comparable long-term trials in shift workers, the study may have limited power to detect smaller effects. Lastly, although dietary intake will be assessed through standardised 5-d food records, self-reporting remains subject to potential bias, even with the support of structured tools and investigator guidance.
Results from this trial will be disseminated through peer-reviewed publications, conference presentations and institutional communication channels, including collaboration with the hospital’s press office.
Any substantial protocol modifications, including changes to eligibility criteria, outcomes or analysis plans, will be documented and reported to the CEICA and updated in the trial registry (ClinicalTrials.gov: NCT06912555). The study may be terminated early only in the event of serious adverse events, funding discontinuation or other ethical concerns, in which case all relevant stakeholders and participants will be notified.
In summary, this trial will provide novel evidence on the effects of hypoenergetic diets with distinct macronutrient profiles and protein distribution patterns in a population at high metabolic risk: shift workers with prediabetes or T2D. By incorporating circadian-related considerations into established dietary strategies, the study addresses a significant gap in the current literature. The findings may inform future dietary recommendations tailored to circadian biology and work schedules, contributing to more effective and personalised nutritional approaches for managing metabolic disorders in shift-working populations.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114526107417
Acknowledgements
The authors would like to acknowledge the support received during the development of this study.
C. R-C. received a predoctoral grant from Aragon Government. The research group within authors developed the study received funding from CIBERCV (co-supported by the European Regional Development Fund (ERDF), which is allocated by the European Union; IIS16/0114) and Aragon Government (B-14).
R. M.-G., It. L.-M., and I. G.-R.: Conceptualisation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – original draft, and Writing – review & editing. C. R.-C.: Formal analysis, Investigation, Methodology, Resources, Writing – original draft, and Writing – review & editing. M. T.-E., S. P.-C., Is. L., Re. M.-G., and Á. L.-E.: Formal analysis, Investigation, Methodology, and Writing – review & editing.
The authors declare that they have no conflicts of interest to disclose.
This study will be conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and the guidelines of Good Clinical Practice. The protocol (Version 3, dated December 16, 2023) and the participant information and consent document (Version 3.0, dated December 15, 2023) were reviewed and approved by the Clinical Research Ethics Committee of Aragón (CEICA) on January 10, 2024 (Act No. 01/2024; Reference: PI23/558). A copy of the ethical approval is available in S1 Appendix. The committee deemed the study ethically acceptable, including the justification of foreseeable risks and burdens, the appropriateness of the informed consent procedures, the suitability of the research team and facilities and the adequacy of proposed data protection and compensation measures.
Written informed consent will be obtained from all participants prior to inclusion. Participants will be informed about the voluntary nature of the study, the right to withdraw at any time and the confidentiality of their data. The full informed consent materials are provided in S1 Appendix.
The trial is registered at ClinicalTrials.gov (Identifier: NCT06912555) and adheres to the SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) guidelines. The completed SPIRIT checklist is included in S1 Appendix.



 Open access
Open access