As Japan is one of the fastest-aging countries, there is significant interest in the prevention and management of age-related health issues(1). A notable phenomenon associated with aging is the decline in muscle strength, which is estimated to decrease by approximately 1·5 % per year(Reference Rolland, Czerwinski and Abellan Van Kan2), and muscle weakness is regarded as a key factor contributing to poor health(Reference Ji, Xia and Tong3,Reference Kim and Kwon4) . The age-related decline in muscle strength is reflected in common measures of physical performance, such as grip strength(Reference Vaishya, Misra and Vaish5). Grip strength is widely recognised as a simple and practical method for evaluating overall muscle strength(Reference Vaishya, Misra and Vaish5). Recently, it has attracted significant attention as a key biomarker of health due to its associations with sarcopenia and various chronic conditions including CVD, type 2 diabetes, metabolic syndrome, stroke, chronic kidney and liver diseases, certain cancers, fragility fractures and overall mortality(Reference Vaishya, Misra and Vaish5). Notably, grip strength typically peaks in the 30s and begins to decline more rapidly after the age of 40(Reference Dodds, Syddall and Cooper6–Reference Steiber9). This suggests the importance of early interventions to mitigate grip strength decline.
Grip strength is influenced by a range of factors, including ethnicity, age, sex, height, weight, abdominal obesity, nutritional status, education level, socioeconomic status and physical activity(Reference Vaishya, Misra and Vaish5). Among these, nutrition plays a pivotal role in muscle health, and dietary protein intake has received particular attention for its critical role in muscle protein synthesis(Reference Vaishya, Misra and Vaish5,Reference Kim, Jeon and Jeong10) . Protein intake has been positively associated with grip strength in several cross-sectional(Reference Pikosky, Cifelli and Agarwal11–Reference Suga and Hashimoto13) and longitudinal(Reference Robinson, Jameson and Batelaan14–Reference McLean, Mangano and Hannan17) studies, but not in all(Reference Gregorio, Brindisi and Kleppinger18,Reference Mulla, Cooper and Mishra19) previous studies. However, most of these studies were conducted in Western countries(Reference Pikosky, Cifelli and Agarwal11,Reference Baumgartner, Waters and Gallagher12,Reference Robinson, Jameson and Batelaan14–Reference McLean, Mangano and Hannan17) , which have different protein intakes and protein sources from those in Japan. Total protein intake, especially animal protein, is lower in Japan than in Western countries(Reference Pasiakos, Agarwal and Lieberman20–22). Moreover, despite age and sex differences in grip strength, limited research has explored the relationship between dietary factors and grip strength among Japanese adults, particularly by sex(Reference Suga and Hashimoto13). In addition, most studies have focused on the elderly(Reference Baumgartner, Waters and Gallagher12–Reference Granic, Mendonça and Sayer16,Reference Gregorio, Brindisi and Kleppinger18) , and little attention has been paid to adults.
Studies of the association between dietary protein intake and grip strength should consider not only the intake quantity but also the source. Dietary protein quality, which is influenced by factors such as amino acid composition and digestibility, differs between protein sources, with animal-derived proteins generally providing higher quality in terms of supporting muscle protein synthesis(Reference Boye, Wijesinha-Bettoni and Burlingame23–Reference Morgan, Harris and Marshall25). Among epidemiological studies, a cross-sectional study found an association between both animal and plant protein intake and grip strength in adults aged 19 and older(Reference Pikosky, Cifelli and Agarwal11), whereas a longitudinal study observed that higher intake of animal protein, but not plant protein, was linked to a slower decline in grip strength among adults aged 60 and older(Reference McLean, Mangano and Hannan17). Thus, few studies have examined the relationship between protein source and grip strength as an indicator of muscle strength, and their results are inconsistent.
Our study aimed to examine the association between dietary protein intake and grip strength, including the effect of protein source (total, animal and plant), among Japanese workers. We hypothesised that the relationship would be positive and would be influenced by both protein intake and source.
Materials and methods
Study design and participants
A survey was conducted during periodic health examinations in November 2019 among workers of a municipal office in Fukuoka Prefecture, Japan. All full-time workers (n 515), except those on long sick leave or maternity leave and foreign nationals, were invited to participate. Prior to the health check-up, we asked all workers to participate in a survey and complete two kinds of questionnaires on diet and health behaviour. On the day of the health check-up, research staff checked the answers and supported participants in completing any missing responses and measured grip strength. Additionally, we obtained health check-up data, including the results of anthropometric and biochemical measurements. We also obtained information on medical history from participants’ self-reports in the medical questionnaire administered during the health check-up.
Survey participants meeting any of the following criteria were excluded: (1) self-reported history of cancer, CVD, chronic hepatitis, chronic kidney disease including nephritis and pancreatitis in the health questionnaire, as these conditions may affect dietary habits and grip strength; (2) missing data on outcomes or covariates; and (3) extremely high or low energy intake (beyond the mean (3 sd)).
Dietary assessment
Dietary habits in the previous month were evaluated using the validated brief self-administered diet history questionnaire (BDHQ)(Reference Kobayashi, Honda and Murakami26), which consists of five sections: (1) frequency of intake of forty-six foods and non-alcoholic beverages; (2) daily frequency of rice and miso soup intake; (3) frequency of alcoholic drinking and amount of consumption for five alcoholic beverages per typical drinking occasion; (4) usual cooking methods; and (5) dietary behaviour. Energy and selected nutrient intake were then estimated based on the intake of food items obtained with the BDHQ and the corresponding food composition list in the Standard Tables of Food Composition in Japan(27). The validation study of the BDHQ, which used 16-d weighed dietary records as the gold standard, reported Pearson correlation coefficients for energy-adjusted intake of protein in ninety-two men and ninety-two women aged 31–76 years of 0·41 and 0·38(Reference Kobayashi, Honda and Murakami26).
Grip strength
We used a Smedley-style handheld dynamometer (No. T.K.K.5001; Takei Scientific Instruments Co., Ltd, Niigata, Japan) to measure the grip strength (kg) of each hand. The participants were instructed to grip the dynamometer as firmly as possible. Two trials were attempted on each hand for a total of up to four trials, and the maximum value among all trials regardless of side (left v. right) was used(Reference Visser, Harris and Langlois28). Grip strength is strongly correlated with lower limb muscle strength, which in turn reflects whole-body muscle strength, and can therefore be used as an indicator of whole-body muscle strength(Reference Strandkvist, Larsson and Pauelsen29).
Other variables
Data on the following variables were obtained from the questionnaire: job description; sedentary time during work, housework and commuting; smoking status; alcohol consumption; and total daily time spent in moderate-to-vigorous physical activity (MVPA) during leisure time.
Data on the following variables were obtained from the health check-up: body weight; height; and participants’ self-reported physician-diagnosed history of diabetes, hypertension and dyslipidaemia. Information on diabetes did not distinguish between type 1 and type 2 diabetes. BMI was calculated as the body weight in kilograms divided by the square of body height in metres.
Statistical analyses
Protein intake was adjusted for energy intake by the residual method(Reference Willett, Howe and Kushi30). We explored the continuous relationship between exposure and grip strength using locally estimated scatterplot smoothing to assess potential non-linear associations. As no clear non-linear trend was observed, tertile categorisation was used for further analyses. Characteristics of participants according to the tertile of total protein intake were expressed as means and standard deviations (sd) for continuous variables and percentages for categorical variables. Trend associations between protein intake and confounding factors were evaluated using linear regression analysis for continuous variables, treating the median of each tertile of total protein intake as a continuous variable, and the Cochran–Armitage χ 2 test for categorical variables.
To determine the association of protein intake with grip strength, multivariable linear regression was used with adjusted means and 95 % CI of grip strength by tertiles of protein intake. The first model was adjusted for age (years, continuous). The second model was additionally adjusted for BMI (< 18·5 kg/m2, 18·5–25 kg/m2 or ≥ 25 kg/m2); alcohol drinking (non-drinker or drinker consuming 1–3 times/month, consuming < 23 g, 23–< 46 g or ≥ 46 g of ethanol/d); smoking (never-smoker, ex-smoker, current smoker consuming < 20 cigarettes/d or current smoker consuming ≥ 20 cigarettes/d); MVPA in leisure time (min/d, quartile); sedentary time during work and housework or on commuting to work (h/d, quartile); job description (administrative or clerical work or fieldwork); history of diabetes, hypertension or dyslipidaemia (yes or no); and total energy intake (kcal/d, continuous). One go of sake (a traditional Japanese unit, 180 ml) contains approximately 23 g of ethanol, and the intake categories in the analysis corresponded to these amounts. Diabetes, hypertension and dyslipidaemia were adjusted for because these metabolic conditions have been reported to be associated with muscle strength, including grip strength(Reference Vaishya, Misra and Vaish5). The third model was additionally adjusted for intakes of carbohydrate (g/d, continuous), PUFA (g/d, continuous), dietary fibre (g/d, continuous), vitamin C (mg/d, continuous), vitamin D (µg/d, continuous) and Ca (mg/d, continuous), which have been reported to be associated with grip strength(Reference Kim, Jeon and Jeong31–Reference Isanejad, Mursu and Sirola33). These nutrient intakes were adjusted for energy intake by the residual method(Reference Willett, Howe and Kushi30). Examination for multicollinearity among the covariates confirmed that all variance inflation factors were below 10. Trend associations between protein intake and grip strength were evaluated using linear regression analysis for continuous variables. We also separately analysed protein intake by food sources (animal and plant protein). Animal and plant protein intakes were adjusted for each other in the third model. Since physical activity and age are associated with grip strength(Reference Vianna, Oliveira and Araujo7,Reference Mendonça, Hengeveld and Presse34) and may modify the association between protein intake and grip strength, we conducted analyses stratified by MVPA in leisure time (< median or ≥ median) and by age (< median or ≥ median). Interaction terms were created by multiplying protein intake with MVPA in leisure time and with age, and these were added to the model to assess statistical interactions. All analyses were conducted using JMP Pro 17.2.0 (JMP Statistical Discovery LCC.), with a nominal two-sided alpha level of 0·05 considered to indicate statistical significance.
Results
Of the 494 individuals who underwent a health check-up, 395 agreed to participate in the study (response rate 80 %). We excluded twenty-two who self-reported a history of cancer, cerebrovascular disease, chronic hepatitis, chronic kidney disease including nephritis and pancreatitis. We further excluded twenty-two with missing data on outcomes and covariates and two with extremely high or low energy intake (exceeding the mean (3 sd)). Finally, 349 participants (175 men and 174 women; mean age, 42·9 years; age range 19–71 years) were included in the analysis.
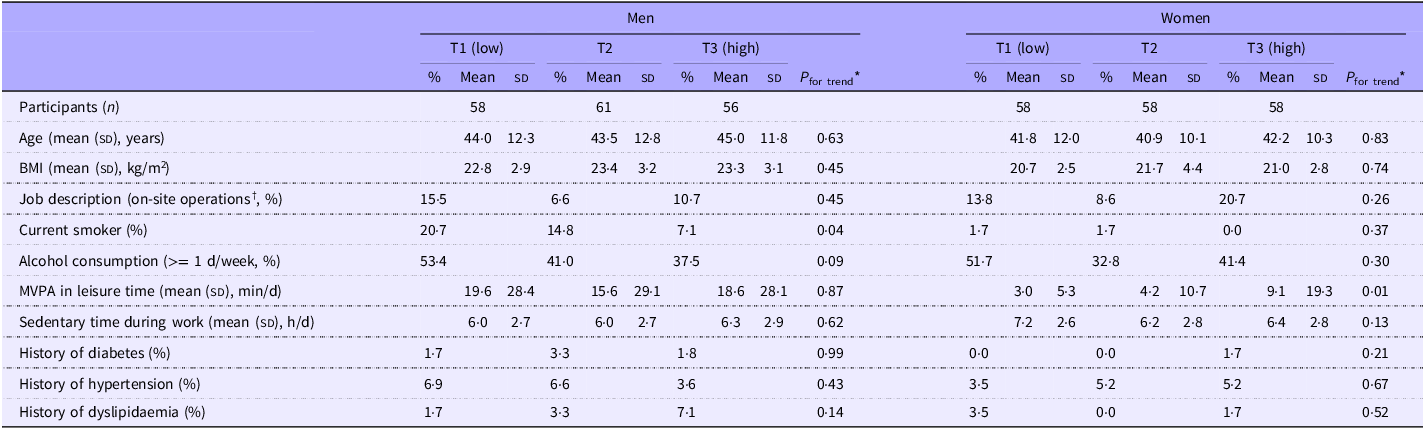
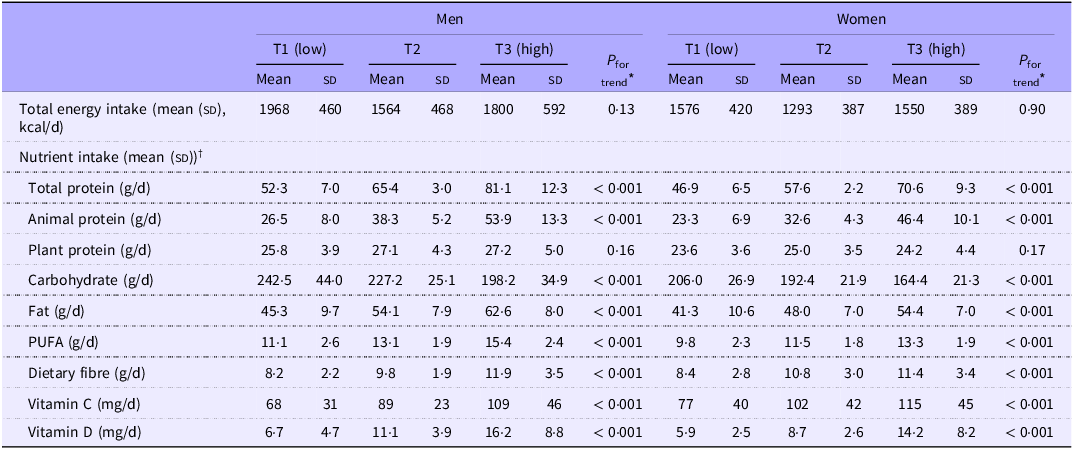
The means (sd) of grip strength were 43·4 (6·5) kg for men and 26·4 (4·4) kg for women. The mean (sd) of total protein intake was 66·1 (14·2) g/d for men and 58·7 g/d (11·7) for women, of which animal and plant proteins accounted for 58·3 and 41·7 % for men and 56·9 and 43·1 % for women, respectively. Participant characteristics by tertile of total protein intake for men and women are shown in Table 1. Men with a higher intake of total protein were slightly less likely to be current smokers and alcohol drinkers (P for trend = 0·038 for current smoker and 0·09 for alcohol drinker). Women with a higher intake of total protein had a higher of MVPA in leisure time (P for trend = 0·012). Energy and nutrition intakes of participants by tertile of total protein intake for men and women are shown in Table 2. Both men and women with higher intake of total protein had a lower intake of carbohydrate and higher intake of fat, PUFA, dietary fibre, vitamin C, vitamin D and Ca compared with participants with lower intake (all; P for trend < 0·001).
Characteristics of participants by tertile (T) of dietary total protein intake in men (n 175) and women (n 174)

MVPA, moderate-to-vigorous intensity physical activity.
* Median dietary total protein intake was assigned to each group as a continuous variable and regression analysis or the Cochran–Armitage χ 2 test was used.
† Fieldwork included childcare, food service, environmental and water and sewerage services.
Energy and nutrition intake of participants by tertile (T) of dietary total protein intake in men (n 175) and women (n 174)

* Median dietary total protein intake was assigned to each group as a continuous variable and regression analysis or the Cochran–Armitage χ 2 test was used.
† Nutrient intakes were adjusted for energy intake by the residual method.
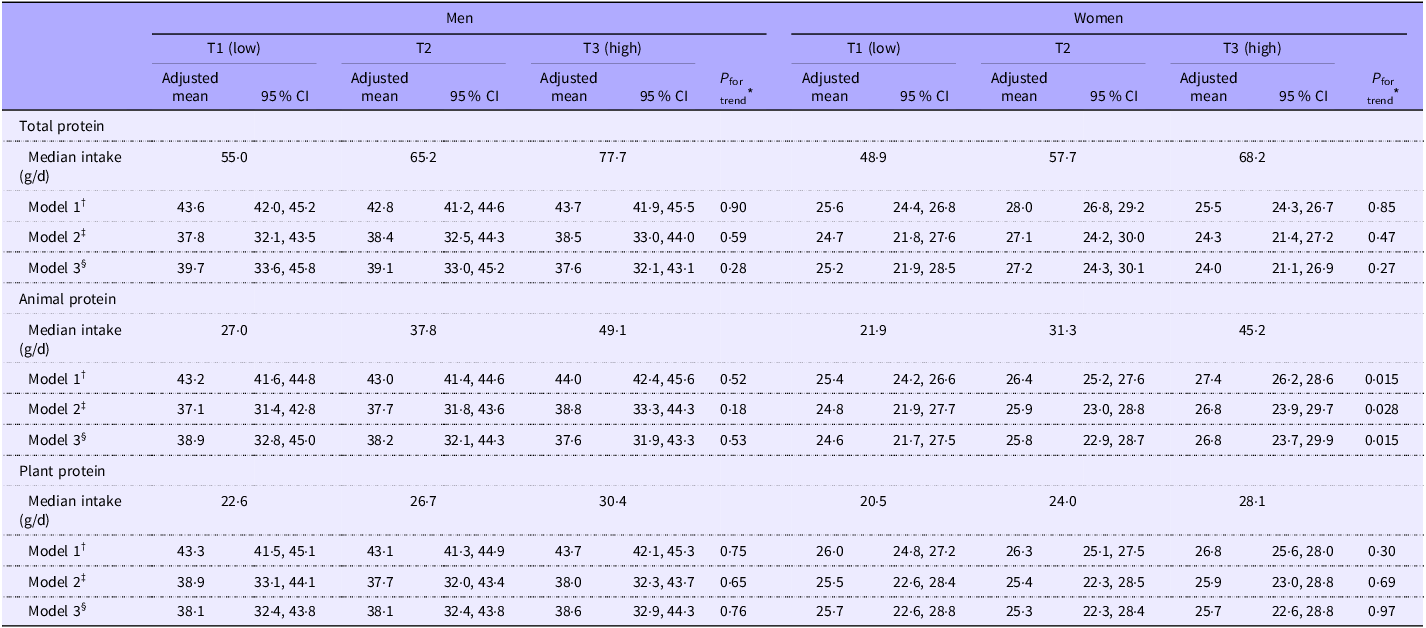
Adjusted means of grip strength by tertile of dietary protein intake for men and women are shown in Table 3. In men, total protein intake was not associated with grip strength after adjustment for age. The association did not materially change after additional adjustment for covariates. Adjusted means (95 % CI) of grip strength for the lowest through highest tertile of total protein intake were 39·7 (33·6, 45·8) kg, 39·1 (33·0, 45·2) kg and 37·6 (32·1, 43·1) kg (P for trend = 0·28). When analysed by protein source, neither animal nor plant protein intake was associated with grip strength in any model. In women, a higher intake of animal protein was associated with higher grip strength. In the age-adjusted model 1, the adjusted means (95 % CI) of grip strength for the lowest through highest tertiles of animal protein intake were 25·4 (24·2, 26·6) kg, 26·4 (25·2, 27·6) kg and 27·4 (26·2, 28·6) kg (P for trend = 0·015). The results remained largely unchanged in model 2, which adjusted for lifestyle factors, and model 3, which additionally adjusted for dietary factors. The least squares-adjusted means (95 % CI) of grip strength for the lowest through highest tertile of animal protein intake after adjustment for all covariates were 24·6 (21·7, 27·5) kg, 25·8 (22·9, 28·7) kg and 26·8 (23·7, 29·9) kg (P for trend = 0·015). Total and plant protein intake showed no statistically significant trend with grip strength, even after adjusting for covariates.
Adjusted mean (95 % CI) grip strength (kg) by tertile (T) of dietary protein intake in men (n 175) and women (n 174)

* Based on multiple linear regression with assignment of median to categories of each dietary protein intake.
† Adjusted for age.
‡ Additionally adjusted for age, BMI, job description, smoking, alcohol consumption, moderate-to-vigorous intensity physical activity in leisure time, sedentary time during work and housework or on commuting to work, total energy intake, history of diabetes, hypertension or dyslipidaemia.
§ Additionally adjusted for carbohydrate, PUFA, dietary fibre, vitamin C, vitamin D and Ca. Animal and plant protein intakes adjusted for each other as a continuous, energy-adjusted variable.
In women, higher animal protein intake was consistently associated with higher mean grip strength across subgroups stratified by MVPA in leisure time or age. The adjusted mean (95 % CI) grip strength for the lowest through highest tertile of animal protein intake was 24·6 (20·7, 28·5) kg, 25·2 (21·5, 28·9) kg and 26·6 (22·7, 30·5) kg for those with low MVPA in leisure time (P for trend = 0·23) and 25·4 (18·5, 32·3) kg, 28·2 (21·1, 35·3) kg and 28·6 (21·7, 35·5) kg for those with high MVPA in leisure time (P for trend = 0·15; P for interaction = 0·71). The corresponding values were 26·2 (22·5, 29·9) kg, 28·2 (24·9, 31·5) kg and 29·3 (25·4, 33·2) kg for the younger age group (P for trend = 0·022) and 26·1 (22·2, 30·0) kg, 27·8 (23·7, 31·9) kg and 29·0 (24·9, 33·1) kg for the older age group (P for trend = 0·023; P for interaction = 0·90). In contrast, total, animal and plant protein intake in men and total and plant protein intake in women were not associated with grip strength across MVPA in leisure time or age subgroups (data not shown).
Discussion
In this cross-sectional study of local government workers in Japan, total protein intake was not associated with grip strength in either men or women. However, in the analysis by source of protein, animal protein intake was significantly and positively associated with grip strength among women. To the best of our knowledge, this study is the first in Asia to examine the association between protein intake and grip strength in adults.
We observed no association between total protein intake and grip strength. Several but not all of the epidemiological studies of the relationship between protein intake and grip strength reported to date have found a positive association. Specifically, prospective studies, including the Hertfordshire Cohort Study, the Women’s Health Initiative, the Framingham Offspring Cohort and the Newcastle 85+ Study, have observed that higher protein intake was associated with slower declines in grip strength(Reference Robinson, Jameson and Batelaan14–Reference McLean, Mangano and Hannan17). Similarly, some cross-sectional studies have also reported a positive association between protein intake and grip strength(Reference Pikosky, Cifelli and Agarwal11–Reference Suga and Hashimoto13). Conversely, however, the Medical Research Council National Survey of Health and Development in the UK and a US cross-sectional study found no significant link between protein intake and grip strength(Reference Gregorio, Brindisi and Kleppinger18,Reference Mulla, Cooper and Mishra19) . Our findings of no association might be partly explained by the age of study participants: while our present participants were 19–71 years old (average 44·5 years for men and 42·1 years for women), most of these previous studies focused on individuals aged 50 years and older (average over 50 years)(Reference Pikosky, Cifelli and Agarwal11–Reference Gregorio, Brindisi and Kleppinger18). The Framingham Offspring Cohort found an association between total protein and grip strength in participants over age 60, but not in those under age 60(Reference McLean, Mangano and Hannan17). Older adults are at a higher risk of insufficient protein intake because of age-related malnutrition and anabolic resistance in aging muscles(Reference Landi, Calvani and Tosato35). This may be attributable to an increase in the thresholds for essential amino acids, higher overall dietary protein requirements and reduced energy intake and needs with aging(Reference Wall, Gorissen and Pennings36,Reference Moore, Churchward-Venne and Witard37) . Given these findings, dietary protein quantity may be more important in the older than in the young. In addition, the lack of association with grip strength in the present study might be attributable to the fact that participants had already achieved an adequate protein intake. Specifically, the mean protein intakes estimated by the BDHQ in this study of 66·1 g/d for men and 58·4 g/d for women are comparable to the Japanese Dietary Reference Intakes of 65 g/d for adult men and 50 g/d for adult women(38). In addition to quantity, the source of protein (ratio of animal:plant protein) may also contribute to the association between protein intake and grip strength. In the present study, the proportion of animal protein to total protein intake was 58·3 % in men and 56·9 % in women, which is comparable to the national average in Japan (56·0 %)(39) and lower than that reported in the USA (64·8 %)(Reference Shan, Rehm and Rogers40). Our findings suggest that dietary strategies focused solely on increasing protein intake may not be effective for preventing muscle strength decline in Japanese individuals.
In this study, we observed a positive association between animal protein intake and grip strength in women. Systematic reviews have reported that animal protein, which is of higher quality than plant protein, enhances muscle protein synthesis in both young and older populations(Reference van Vliet, Burd and van Loon24,Reference Morgan, Harris and Marshall25) . In epidemiological studies of the association between dietary protein source and grip strength, animal protein was more strongly associated with strength than plant protein(Reference Pikosky, Cifelli and Agarwal11,Reference McLean, Mangano and Hannan17) . Moreover, animal protein appears to be more advantageous for preserving muscle mass and strength in women. Some observational studies support this perspective(Reference Beasley, Wertheim and LaCroix15,Reference Pannemans, Wagenmakers and Westerterp41–Reference Murakami, Livingstone and Fujiwara43) , consistent with our results for women. However, while most of these on dietary protein sources(Reference Beasley, Wertheim and LaCroix15,Reference Shan, Rehm and Rogers40,Reference Lord, Chaput and Aubertin-Leheudre42) concentrated on elderly women, our present findings indicate that animal protein may play a crucial role in maintaining muscle strength among women.
Meanwhile, no significant association was observed between the protein source and grip strength in men. Sex differences in the association between protein intake and grip strength have been reported with inconsistent results. Like our study, the Hertfordshire Cohort Study and the Newcastle 85+ Study reported an association in women, but not in men(Reference Robinson, Jameson and Batelaan14,Reference Granic, Mendonça and Sayer16) . A cross-sectional study in Japan reported an association between protein intake and grip strength at different ages for men and women, namely, in men aged 75 and older and in women aged 65 and older(Reference Suga and Hashimoto13). In contrast, the National Health and Nutrition Examination Survey and New Mexico Aging Process Study reported associations in both men and women(Reference Pikosky, Cifelli and Agarwal11,Reference Baumgartner, Waters and Gallagher12) . Although the observed sex differences in the association with grip strength could be attributed to differences in protein intake, both men and women met the recommended protein intake levels, and their proportions of animal protein intake were similar. We propose some possible explanations for the sex difference. First, the sex difference might be partially explained by the role of sex hormones. Testosterone gradually declines from middle age, while oestrogen decreases sharply during menopause, which may result in differences in the timing of age-related muscle strength decline between men and women. Consequently, men might experience a delayed reduction in muscle strength compared with women(Reference Gheller, Riddle and Lem44,Reference Callahan, Bedrin and Subramanian45) . Second, men generally have a greater absolute muscle mass than women(Reference Janssen, Heymsfield and Wang46). Therefore, even if both sexes increase protein intake by the same amount, the relative improvement in muscle strength may appear smaller in men because they start from a higher baseline. Third, women have been reported to have higher fractional synthesis rates of muscle proteins and greater whole-body protein turnover than men, independent of age and BMI(Reference Henderson, Dhatariya and Ford47). Although women have smaller muscle mass, their higher muscle protein turnover may contribute to more efficient renewal of muscle proteins and maintenance of muscle quality, which could partly explain the stronger association between protein intake and grip strength observed in women. Future studies should explore the factors underlying these sex-specific differences.
Strengths of this study include its high participation rate, which minimises the impact of selection bias; adjustment for dietary factors associated with grip strength; and the minimisation of missing questionnaire data through careful checks by research staff. This study also has some limitations. First, cross-sectional studies can only demonstrate associations and do not establish causality. To reduce the risk of reverse causation, we excluded participants with a history of severe illness that could influence their diet and grip strength. Second, as the BDHQ is a self-administered, fixed-portion dietary questionnaire designed to estimate habitual intake over a short period, some misclassification due to measurement error cannot be ruled out. Moreover, since protein intake was assessed at a single time point, it may not reflect the long-term dietary intake. Third, we did not obtain information on protein intake from supplements. Men, particularly those who exercise regularly and young adult men, consume more health foods than women for the purpose of protein supplementation(22). Accordingly, protein intake evaluated using the BDHQ may underestimate actual intake. Future analyses should consider the intake from protein supplements. Finally, since the participants were local government workers in Japan, the findings may not be directly generalisable to other populations with different demographic or occupational backgrounds.
In conclusion, higher dietary intakes of animal protein, but not total and plant protein, were associated with higher grip strength in women. Meanwhile, protein intake or sources were not associated with grip strength in men. Our findings suggest that protein from animal sources is an important factor in muscle strength in women and that there are sex differences in the relationship between protein intake and grip strength. Future prospective studies should investigate dietary intake at multiple time points to confirm the association between animal protein intake and grip strength among women observed in this cross-sectional study and apply more comprehensive dietary assessment strategies, including the use of metabolomics data and protein quality metrics beyond protein source, and evaluation of the potential impact of protein supplementation. Additionally, mechanism-based research exploring the biological and physiological pathways underlying the observed sex differences and dietary changes over time would help clarify causal relationships between dietary protein intake and grip strength.
Acknowledgements
The authors would like to thank those who helped collect data for the nutritional epidemiology study. They are also grateful to the study participants for their cooperation and participation.
This work was supported by an FWU Research Grant from Fukuoka Women’s University. The funder had no role in the design, analysis or writing of this article.
Research conception and design: M. O. and A. N., conduct of the survey: M. O., M. N., Y. U. and A. N.: statistical analysis of the data: Y. Y. and A. N.: interpretation of the data: Y. Y. and A. N.: writing – original draft preparation: Y. Y.: writing – review and editing: A. N. All authors approved the final version of the manuscript.
There are no conflicts of interest.
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human participants were approved by the Ethics Committee of Fukuoka Women’s University, Japan (approval number: 2019-34). Written informed consent was obtained from all participants prior to the survey.