

Introduction
Through patient-centred care, healthcare teams deliver high-quality care to address the needs and preferences of each patient (Institute of Medicine (US) Committee on Quality of Health Care in America, 2001). Embedded within patient-centred care is the allied relations with a person or people identified by the patient as their family (Healthcare Excellence Canada, 2021). This has improved the design, delivery, and evaluation of healthcare through a valuable partnership between healthcare providers, patients, and the patients’ families (Healthcare Excellence Canada, 2021). Hospitals often form patient and family engagement committees and appoint a Patient Advocate who ensures that the voices of patients and their families are included in all aspects of care planning and delivery (Oehrlein et al., Reference Oehrlein, Harris, Balch, Furlong, Hargis, Woolley and Perfetto2021; Ontario Hospital Association, n.d a).
Some Ontario (Canada) healthcare centres have accommodating visitation policies (e.g., a Family Presence Policy), which are associated with improved patient and family member satisfaction (Canadian Foundation for Healthcare Improvement, 2015; Canadian Foundation for Healthcare Improvement, n.d; Correia et al., Reference Correia, Martins and Barroso2021; Ontario Hospital Association, n.d b; The Change Foundation and Ontario Hospital Association, 2019). However, there are limited guidelines on how to operationalize these policies in such a way that empowers families to become care partners (Bélanger et al., Reference Bélanger, Desmartis and Coulombe2018; Correia et al., Reference Correia, Martins and Barroso2021; Markwell & Godkin, Reference Markwell and Godkin2004; Palubiski et al., Reference Palubiski, Tulsieram, Archibald, Conklin, Elliott, Hsu, Stolee, Sveistrup and Kothari2022). In the event when family members do become care partners, there is a lack of procedures that guide healthcare providers on how they can incorporate family into the care circle and provide education to assist, support, and participate in the care of the individual hospitalized (Bélanger et al., Reference Bélanger, Desmartis and Coulombe2018; Correia et al., Reference Correia, Martins and Barroso2021; Saarinen et al., Reference Saarinen, Mishina, Soikkeli‐Jalonen and Haavisto2021). Although there is a paucity of evidence that illustrates the understanding of and the value of the DCP role among patients, families, and healthcare providers, a published report that guides the implementation process of a DCP program is vital.
To control the spread of infections in healthcare settings at the start of the COVID-19 pandemic, in-person visitation and family presence were suspended (Canadian Foundation for Healthcare Improvement, n.d). Although there was a need to implement precautions, consequently the increased patient isolation that resulted from this decision resulted in negative physical and mental impacts that led to increased pain, fall rates, and depressive symptoms accompanied by decreases in nutrition intake, activities of daily life, cognitive ability, and overall satisfaction (Hugelius et al., Reference Hugelius, Harada and Marutani2021; Lebrasseur et al., Reference Lebrasseur, Fortin-Bédard, Lettre, Raymond, Bussières, Lapierre and Routhier2021; Palubiski et al., Reference Palubiski, Tulsieram, Archibald, Conklin, Elliott, Hsu, Stolee, Sveistrup and Kothari2022; Silvera et al., Reference Silvera, Wolf, Stanowski and Studer2021). It has been illustrated that the pandemic has had a disproportionately negative impact on older adults, a cohort recognized as being among the most vulnerable due to underlying health conditions, within Canada and other countries worldwide (Beauchamp et al., Reference Beauchamp, Vrkljan, Kirkwood, Vesnaver, Macedo, Keller and Scott2021; Wister et al., Reference Wister, Li, Cosco, McMillan and Griffith2022). The negative impacts on older adult patients in particular have included reduced overall quality of life (Lebrasseur et al., Reference Lebrasseur, Fortin-Bédard, Lettre, Raymond, Bussières, Lapierre and Routhier2021). Without incorporating the compounded risks associated with COVID-19, more than one-third of older adults hospitalized within Canada are at increased frailty risks (CIHI, 2023). Furthermore, these older adults are characterized as being three times more likely to (i) be high users of hospital beds, and (ii) experience hospital days longer than 30 days, and, are twice as likely to be (i) readmitted within 30 days of discharge and (ii) deceased within 1 year of discharge (CIHI, 2023).
The impact of older adult hospitalization during COVID-19 on family members was equally difficult, as they endured worry and anxiety about the well-being of the patients (Dennis et al., Reference Dennis, Vanstone, Swinton, Vegas, Dionne, Cheung, Clarke, Hoad, Boyle, Huynh, Toledo, Soth, Neville, Fiest and Cook2022; Hugelius et al., Reference Hugelius, Harada and Marutani2021). The detrimental effects of ‘no-visitor rules’ on patients and their family emphasizes the importance of in-person visitation to ensure the well-being of both members of the care circle as much as possible during a patient’s journey (Dennis et al., Reference Dennis, Vanstone, Swinton, Vegas, Dionne, Cheung, Clarke, Hoad, Boyle, Huynh, Toledo, Soth, Neville, Fiest and Cook2022; Nuss et al., Reference Nuss, Kelly, Campbell, Pierce, Entzminger, Blair, Wissinger, Bryant and Walker2014; Hugelius et al., Reference Hugelius, Harada and Marutani2021; Sudai, Reference Sudai2021). It is important that family members remain a consistent part of the care circle to prevent patient isolation, while ensuring the care they do receive is acceptable (Hugelius et al., Reference Hugelius, Harada and Marutani2021; Nuss et al., Reference Nuss, Kelly, Campbell, Pierce, Entzminger, Blair, Wissinger, Bryant and Walker2014; Silvera et al., Reference Silvera, Wolf, Stanowski and Studer2021; Sudai, Reference Sudai2021).
To address these consequences, hospitals and long-term care homes developed designated and essential caregiver/care partner programs to allow family members onsite access to their loved one (Montesanti et al., Reference Montesanti, MacKean, Fitzpatrick and Fancott2023). These programs stemmed from the successful concept in children’s hospitals, in which family members are not seen as visitors, but rather considered members of the healthcare team (Mackean et al., Reference Mackean, Thurston and Scott2005; Montesanti et al., Reference Montesanti, MacKean, Fitzpatrick and Fancott2023). Additionally, similar programs with older adults who have reduced cognitive function have been documented (Montesanti et al., Reference Montesanti, MacKean, Fitzpatrick and Fancott2023; Provincial Geriatrics Leadership Ontario and the Rehabilitative Care Alliance, 2021). Family members can recognize slight changes in cognitive function over hospital staff and can provide the bridge for communication; therefore, a co-designed person-centred rehabilitative care plan is vital (Montesanti et al., Reference Montesanti, MacKean, Fitzpatrick and Fancott2023; Provincial Geriatrics Leadership Ontario and the Rehabilitative Care Alliance, 2021).
A Designated Care Partner (DCP) program was implemented at a specialty community hospital in Southwestern Ontario, Canada. This program provided the opportunity for family members (i.e., any individual that the patient identified as important to their care) to support patients safely and actively during their hospital stay. By becoming DCPs, family members participated in decisions about care, mealtime, personal hygiene, and emotional support. This paper describes the development, implementation, and evaluation of the DCP program as a quality improvement initiative. The discussion aims to define the role of family members as care partners and guide their integration in healthcare settings.
Program planning
The DCP program was primarily implemented to establish a standardized procedure to promote and maintain family presence in the hospital setting. The planning for this program began in 2019 through informal discussions with patient and family advisory members. The onset of the COVID-19 pandemic quickly mobilized planning for the DCP Program to allow monitored family presence to be re-instated in hospitals as a strategy to offset the potential for emotional harm associated with severe visitor restrictions.
An Advisory Group was first developed by the Patient Advocate to ensure that the DCP program would be co-designed with individuals who have lived and clinical experience. This group comprised of approximately 12 experts with various perspectives, including family members of loved ones who were hospitalized at the site; the Patient Advocate; the Risk and Privacy Officer; and leaders of infection control and prevention, quality, restorative care, and communications. Together, this Advisory Group developed a Coordinated Care Policy and Procedure (CCP), which enables educated DCPs to provide specific aspects of the care plan as defined by the patient and care team in a carefully planned and coordinated approach (more information on this policy is available upon request). Ethical considerations, as described by Markwell and Godkin (Reference Markwell and Godkin2004) and Dokken et al. (Reference Dokken, Johnson and Markwell2021), underpinned the policy development process, which then acted as a guide to operationalize and implement the DCP Program on inpatient units. The policy marked a significant expansion of the existing Family Presence and Visiting Policy and Procedures at the hospital by formalizing the recognition of family members as part of the care circle, including a detailed approach to training and education requirements, as well as roles and responsibilities related to care planning and delivery of care. The patient, their family, and clinical staff were together recognized as key members of the care circle for program success.
Program description
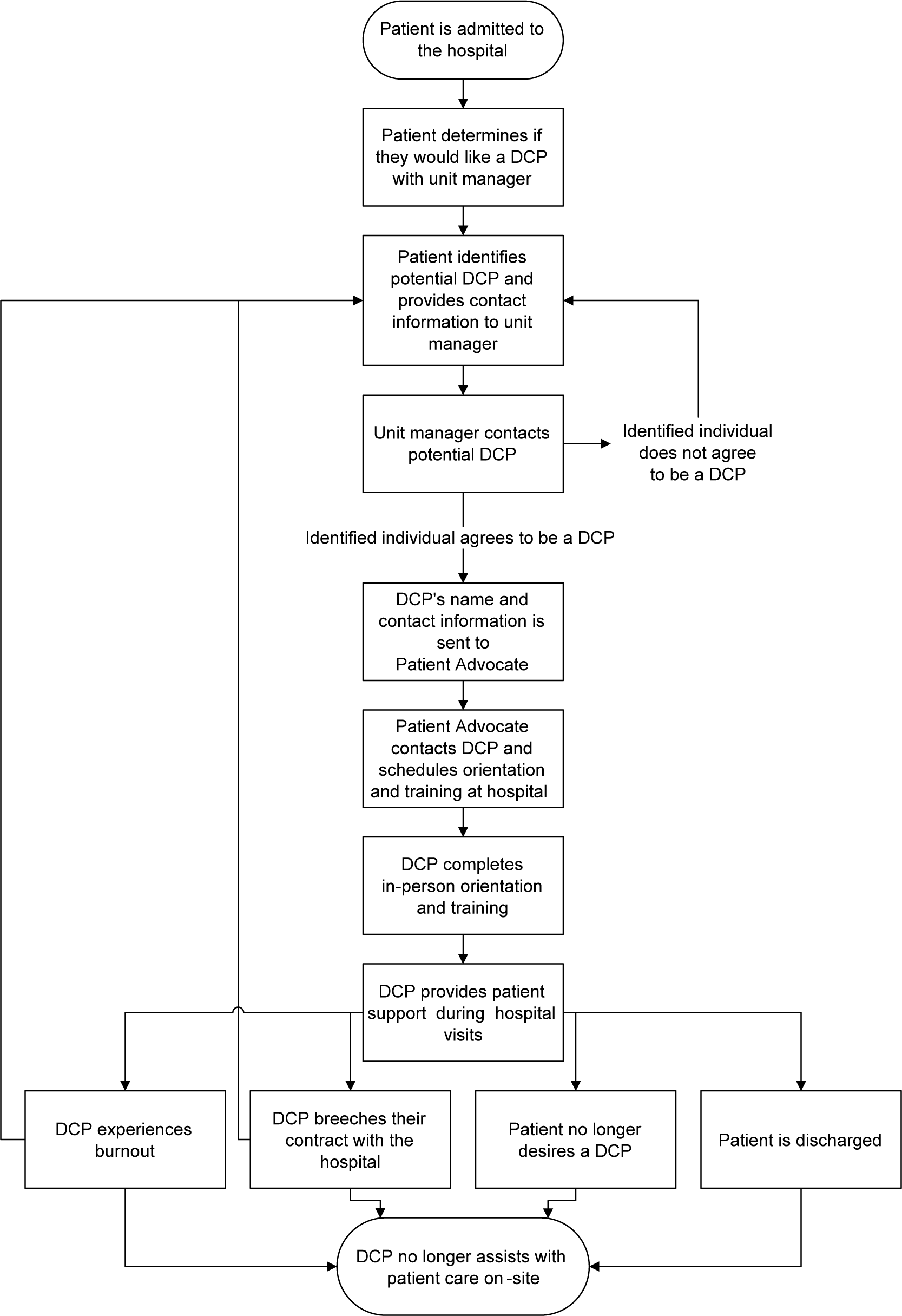
The DCP Program allowed admitted patients to have the opportunity to identify individuals (denoted as ‘family member(s)’) who may serve as their DCP (Figure 1). The term, DCP, has been used interchangeably with Essential Care Partner. However, with advice from a bioethicist, it was decided to incorporate the term ‘designated’ to signify that the patient chose the person, which deemed the individual unarguably essential to the care of the patient. Importantly, a DCP was not synonymous with or an alternative for a visitor or a staff member but rather a support person purposefully involved in the emotional well-being and recovery journey of the patient. For example, having a DCP was beneficial for patients who: (a) required assistance with communication, (b) needed social or emotional support, (c) were experiencing life-altering events, (d) required end-of-life care, and/or (e) were undergoing a transition in care.
Designated care partner program process.
Note: DCP indicates Designated Care Partner.

Due to the ongoing COVID-19 pandemic, the initial goal was for each patient to have only one DCP participating to minimize the number of people on-site at any given time to abide by restrictions around physical distancing and illness screening. However, as outlined in the CCP, the care team determined the maximum number of DCPs permitted on the unit at a time, and, therefore, several exceptions were made when appropriate. For example, if a patient required support from a family member onsite at all times due to their condition, then multiple DCPs may be engaged to allow for each to take different shifts to cover the full day and reduce any potential for caregiver burnout. In some circumstances, the individual identified by the patient as a potential DCP would not be able to participate in the program due to personal- or employment-related reasons. In these cases, the patient would have the opportunity to identify other possible DCPs to ensure that each patient who wanted a DCP had a loved one on-site to support them.
All DCPs participated in a two hour in-person orientation and training session led by the Patient Advocate, members of the Patient and Family Advisory Council, the Volunteer Coordinator and representatives from infection prevention and control. Sessions were offered two days per week during the day and evening to accommodate DCPs’ schedules. The content of the orientation and training included a description of the DCP role and responsibilities, which would later be refined once the DCP was on the unit working with the clinical care team and a care plan is established, an explanation of the CCP in plain language, the range of support DCPs may be comfortable with providing their loved one during their hospital stay (e.g., emotional support, assistance with meal times, acting as a translator), how to navigate the facility, and infection, prevention, and control training. At the orientation, DCPs were also introduced to the Patient Advocate so they knew who to contact if they had questions, they signed a contract stating that they would follow infection, prevention, and control practices, and received a picture identification badge which was required to be displayed for the duration of their time in the hospital. Finally, DCPs were also trained by the Volunteer Coordinator on how to login into an existing volunteer management software program, which was accessible on a computer kiosk at the main entrance of the hospital. During orientation, the Volunteer Coordinator walked each DCP through the software program, helped them register with an account, and then taught them how to sign in and out at the beginning and end of their visit to the hospital. The purpose of using the volunteer software program was two-fold. First, it enabled hospital administrators to monitor the number of individuals physically onsite given the physical distancing and other restrictions that were in place during the pandemic, and second, using this software enabled tracking the number of visits performed by DCPs over time, which was a key process measure to evaluate the implementation of the program.
After orientation, DCPs were introduced to the unit leader (unit manager or charge nurse), with whom they discussed the patient’s care plan and how to support the patient alongside the patient when possible. Communication between DCPs and unit staff predominantly occurred through informal, unscheduled interactions during regular DCP visits. However, communication may have also occurred outside of visits over the phone. The care and support DCPs provided to their loved one during on-site visits was entirely voluntary and varied depending on the patient’s need and the preference and comfort level of both the patient and DCP. DCPs provided emotional, cognitive, communicative, and decision-making support as well as physical care (i.e., assistance with mealtimes, grooming, and personal hygiene). As a health and safety measure, DCPs signed into the volunteer management software each time they visited the hospital to track their time onsite. Although the hospital had no set tasks for each DCP to complete during their visits, DCPs were expected to adhere to infection control practices, wear their identification badge, be screened for COVID-19 infection upon site entry, and provide support only to their assigned patient during their stay. As outlined in the CCP and shared with DCPs during the orientation, DCPs who were unable to adhere to infection, prevention, and control practices as stated in the DCP contract were provided at least three verbal and written warnings prior to being considered ‘in breach’ of their contract and no longer able to assist with their loved one’s care onsite as a DCP.
Program implementation
A Implementation Working Group was formed to oversee the implementation of the DCP Program as a quality improvement initiative. This group included the Patient Advocate; members of the Patient and Family Advisory Council; several operational unit managers; and senior leaders in quality improvement, infection control and prevention, and restorative care. The program processes were mapped and integrated into the existing workflow on the unit. A program logic model was collaboratively developed to link program activities with key outputs, short-term, and long-term outcomes to monitor success of the initiative (Table 1).
Logic model for a designated care partner program in a specialty community hospital

Note: DCP indicates designated care partner.
Before the program was introduced on all rehabilitation and restorative care units, an initial 2-week pilot was conducted. The pilot commenced with thoroughly describing the program to unit staff through team huddles. Then, a small group of 12 DCPs were provided with training and orientation, as described above. After the training and orientation, DCPs spent two weeks onsite with their family member during designated program hours. Feedback surveys, completed by both DCPs and staff involved in the pilot, were collected on the content and quality of the orientation material and experience of either being a DCP or working with DCPs on the unit. Findings from the feedback surveys suggested that the program was positively received by both DCPs and staff and provided sufficient evidence to spread the program to the other rehabilitation and restorative care units.
Program evaluation
Upon the success of the initial DCP pilot, the program was spread to other inpatient units within the hospital, and further evaluation was conducted. To capture program outcomes, DCPs, patients, and staff anonymously completed evaluation surveys at various time points during program implementation. These evaluations were conducted by the hospital’s internal research department staff, who were also responsible for data management and storage. An initial paper-based evaluation survey of the orientation and training was administered to each DCP at the end of their orientation session and collected by research staff. At 1-month post-orientation, research staff would email each DCP a link to complete an electronic experience survey, which captured demographic information, frequency of onsite visits, perceptions surrounding the type of care they provided to their patient, how well they were integrated into the care circle, how frequently staff offered support, and overall satisfaction with the program. To gather patient perspectives, each patient was called within three days of hospital discharge to complete a telephone survey that asked five questions about their DCP experience, including the type of care their DCP provided and their overall program satisfaction. After the DCP Program had been operating for six months, frontline unit staff were emailed an electronic post-implementation survey to capture their feedback on the DCP training, the type of care activities provided by DCPs, and the effectiveness of DCPs being integrated into the care circle. Other key performance measures recorded by the research team for monitoring program implementation included the total number of DCPs trained, the number of patients assigned a DCP, and on-site visit hours logged by DCPs through the volunteer management system.
Results from the evaluation were summarized monthly and shared at the Advisory Group meetings for discussion and program refinement. For example, members of the Advisory Group (i.e., family members with loved ones who were hospitalized at the site) joined orientation sessions to provide examples of how they cared for their loved ones on-site to clarify the responsibilities of DCPs. The secondary use of evaluation data for the purposes of this paper was cleared by an institutional research ethics board (REB # 22-096).
Evaluation findings
Data collection spanned from July 2020 to August 2021, during which time 958 DCPs completed orientation and training, 937 inpatients were assigned at least one DCP, and DCPs logged 26,200 hours on-site. The training and orientation evaluation survey was completed by 692 DCPs, and program experience data was collected from 119 DCPs, 72 discharged patients, and 146 staff members. DCP survey respondents were, on average, 61 years of age and identified mostly as female (69%). Survey respondents’ relationship with patients included being the adult child of the patient (42%), spouse/partner (28%), other family member/friend (19%), or sibling (8%). Close to half of DCPs (49%) came on-site daily to provide care, and 45 per cent provided care at least three times per week.
Following orientation and training, nearly all DCPs (99%) who completed the survey indicated that they gained knowledge and skills, understood their role and responsibilities, and reported they were confident and prepared to act as a DCP. Comparatively, 88 per cent of staff who completed the survey reported that the DCP training was adequate. In terms of care activities, both DCPs and staff reported that DCPs predominantly supported patients’ emotional care, such as providing social support and companionship (stated by 67% of DCPs and 83% of staff), emotional support (78% and 79%), and assistance with decisions about care (51% and 62%). Aspects of physical care were more infrequently performed by DCPs as reported by both DCPs and staff; for example, assisting patients with mealtimes (stated by 35% of DCPs and 50% of staff), personal care (40% and 25%), and mobility (40% and 19%). On the other hand, patients suggested that the most common aspect of their care provided by DCPs was assisting them with decisions about their care (38%) and providing social support/companionship (39%). In general, all members of the care circle reported that DCPs more frequently supported a patient’s overall emotional care rather than physical (Figure 2).
Percentage of stakeholders that perceived designated care partners supported emotional and physical care.
Note: DCP indicates Designated Care Partner.

Survey questions about the supportive role of the clinical team showed that 40 per cent of DCP reporting that they received ‘a lot’ of support from the clinical team while 34 per cent reported having received ‘a little’ support. Moreover, 37 per cent of DCP survey respondents ‘always’ or ‘often’ reported being involved in discussions about the patient’s care. More than a third (35%) of staff who completed their evaluation survey suggested that DCPs were ‘very effectively’ integrated into the care circle, and 24 per cent indicated that DCPs were ‘not at all’ integrated. Additionally, 57 per cent of staff reported that they used DCPs as a source of information regarding the patient’s health, whereas 10% reported that DCPs were ‘never/rarely’ used as a source of information. Regarding overall program satisfaction, 85 per cent of DCPs and 97 per cent of patient survey respondents reported being satisfied or very satisfied with the DCP program.
Summary and next steps
Based on the preliminary evaluation, the program resulted in high satisfaction ratings from both patients and their DCPs and demonstrated a promising approach to maintaining family involvement in patient care while balancing health and safety during pandemic visitation restrictions. The mandatory training provided to DCPs was found to be effective in preparing DCPs for their role and in performing infection control and prevention procedures to ensure safety while onsite. Notably, visitation restrictions may continue to occur annually with seasonal outbreaks of illnesses (e.g., influenza) in hospitals and other care settings.
Further development is needed in seamlessly integrating DCPs into the care circle and considering them as a key source of information about the patient. Next steps at the community hospital revolve around refining the knowledge and communication shared about the program with key members of the care circle, including staff, and developing further education to enhance and sustain the role of the DCP in the care circle. In the absence of visitor restrictions, it may be challenging to distinguish the role of the DCP from that of a visitor, and further research is warranted to better inform this distinction (Palubiski et al., Reference Palubiski, Tulsieram, Archibald, Conklin, Elliott, Hsu, Stolee, Sveistrup and Kothari2022). It is important for DCP Program representatives to consistently engage with patients and their families when patients are initially admitted to the hospital to ensure continued program success.
The process of supporting DCPs health literacy around their care transitions could begin at hospital admission (Allen et al., Reference Allen, Woolford, Livingston, Lobchuk, Muldowney and Hutchinson2023). Insufficient education on transitions from hospital to home has been a previously identified barrier for caregivers, especially when caring for older adults with multimorbidity (Allen et al., Reference Allen, Woolford, Livingston, Lobchuk, Muldowney and Hutchinson2023). Notably, improved health literacy around care transitions has the potential to reduce the likelihood of a patient being readmitted after discharge (Allen et al., Reference Allen, Woolford, Livingston, Lobchuk, Muldowney and Hutchinson2023; Rennke et al., Reference Rennke, Nguyen, Shoeb, Magan, Wachter and Ranji2013). Given that older adults are twice as likely to be readmitted within 30 days of discharge, developing care transition-specific education within the DCP programming is paramount (CIHI, 2023). This education could include topics such as caregiver burnout, activities of daily living, communication with healthcare providers, navigation of community supports, and managing specific health conditions (Cianfrocca et al., Reference Cianfrocca, Caponnetto, Donati, Lancia, Tartaglini and Di Stasio2018).
One of the primary concerns with restricting visitation was that patients’ emotional well-being may be compromised due to lack of in-person interaction with their family members. The current evaluation findings suggest that this concern was mitigated by the introduction of DCPs, who were perceived as providing primarily emotional support to their loved one during their stay. Although supporting the emotional well-being of their family member was of utmost importance during the COVID-19 pandemic, contributing to physical aspects of care (i.e., activities of daily living, including assisting with mobility, personal care, mealtimes, advocacy, and care coordination) and care planning may also be meaningful aspects of the DCP role, which, in turn, will contribute to the delivery of holistic patient care and support a seamless transition back to the community following hospital discharge (e.g., Dyrstand et al., Reference Dyrstad, Laugaland and Storm2015).
In particular, the evaluation results suggest that there is an opportunity for further training DCPs to actively support patients’ physical care if the care partner is both willing and able, which may build confidence in performing these tasks to further support better discharge planning and care transitions (Hahn-Goldberg et al., Reference Hahn-Goldberg, Jeffs, Troup, Kubba and Okrainec2018). In this case, three important aspects must be considered: (1) clear expectations around the type of physical care activities that DCPs can competently perform, (2) the provision of appropriate training to ensure DCPs can perform their roles safely and competently, and (3) the implementation of parameters to protect both DCPs and patients. To make informed changes, research is currently underway to engage members of the care circle, inclusive of DCPs, to better understand their expectations about the DCP role and to refine the training DCPs receive, while ensuring their responsibilities do not replace that of the paid clinical care team. Expectations for the DCP role may vary depending on both the patient’s needs and the caregiver capacity, as many DCPs may have their own limits to the support they can provide (Petry et al., Reference Petry, Lara and Boucher2024). This is especially important when older adults are caring for one another and they each have underlying health conditions (Petry et al., Reference Petry, Lara and Boucher2024). Therefore, capacity and other ethical considerations must always guide the development and policies of an organization’s DCP program to align with the needs of the organization, the patient, and the DCP (Dokken et al., Reference Dokken, Johnson and Markwell2021; Markwell & Godkin, Reference Markwell and Godkin2004).
Furthermore, improving the education, knowledge, and commitment of staff is essential to supporting the transition and sustainability of the DCP program beyond the COVID-19 pandemic. The success of care partnership between healthcare professionals, patients, and families is rooted in a culture of Patient- and Family- Centred Care (PFCC) (Dokken et al., Reference Dokken, Johnson and Markwell2021; Montesanti et al., Reference Montesanti, MacKean, Fitzpatrick and Fancott2023) and, therefore, revolves around developing a relationship between unit staff and family. Establishing this collaboration through the DCP program can contribute to all patients, including vulnerable groups with complex health challenges (e.g., older adults with multiple chronic conditions), and their DCPs, being supported by the healthcare system (Ploeg et al., Reference Ploeg, Matthew-Maich, Fraser, Dufour, McAiney, Kaasalainen, Markle-Reid, Upshur, Cleghorn and Emili2017). The success of the DCP program requires staff to understand the relevance and value of the program and the role of the DCP in care planning and the patient’s recovery. Therefore, training for staff should entail the significance of the DCP Program in delivering PFCC, clear information on the DCP role and assessing what DCPs are capable of performing, and how to effectively communicate and collaborate with DCPs during a patient’s hospital stay. With improved staff education and awareness, DCPs may feel more supported by the clinical team, resulting in members of the care circle working in synergy to provide the best patient care possible. Moreover, staff may better understand how to integrate DCPs into the care circle and utilize them as a source of knowledge. Improved education for members of the care circle will ensure that the absence of formalized program procedures does not become a barrier to incorporating family into the care circle (Bélanger et al., Reference Bélanger, Desmartis and Coulombe2018; Correia et al., Reference Correia, Martins and Barroso2021; Saarinen et al., Reference Saarinen, Mishina, Soikkeli‐Jalonen and Haavisto2021). Mitigating any barrier to the effective integration of family into care planning and care delivery practices is vital to ensure program stability and positive outcomes for patients, even during severe visitor restrictions (Correia et al., Reference Correia, Martins and Barroso2021; Hugelius et al., Reference Hugelius, Harada and Marutani2021; Silvera et al., Reference Silvera, Wolf, Stanowski and Studer2021).
This paper, including the logic model (Table 1), offers an approach to planning, implementation, and evaluation of the integration of family involvement into the care circle at community specialty hospitals. Notably, the logic model could be expanded and strengthened by using an evidence-based implementation science framework (e.g., Consolidated Framework for Implementation Research) that considers multilevel implementation contexts that influence effectiveness and sustainability (Damschroder et al., Reference Damschroder, Aron, Keith, Kirsh, Alexander and Lowery2009). Nonetheless, the significant message for healthcare providers and other specialty community hospitals is that offering education and training to staff, patients, and DCPs on the involvement of families in the care circle (roles and capacity) may potentially improve inpatient outcomes and help support discharge recovery (Hahn-Goldberg et al., Reference Hahn-Goldberg, Jeffs, Troup, Kubba and Okrainec2018). Future research is needed to determine if the early engagement of DCPs and their roles on the unit effectively support avenues within inpatient care and beyond.
Acknowledgement
The authors would like to thank Dr. Hazel Markwell for sharing her expertise and useful discussions on the topic.



 Open access
Open access