


Ramadan, the ninth month of the Islamic lunar calendar, is observed by Muslims worldwide through daily fasting from sunrise to sunset. During this period, healthy adults abstain from food, drink, smoking, sexual activity and other behaviours during daylight hours. Although Islamic law exempts pregnant and breast-feeding women from fasting, many choose to fast, often motivated by religious conviction, cultural norms or social expectations. Previous studies estimate that the majority of pregnant Muslim women fast during Ramadan, at least partially. For example, Ramadan fasting during pregnancy has been reported as 55 % in Iraq(Reference Safari, Piro and Ahmad1), 90 % in West Africa(Reference Prentice, Prentice and Lamb2), 80 % in Indonesia(Reference van Bilsen, Savitri and Amelia3), 87·5 % in Pakistan(Reference Mubeen, Mansoor and Hussain4), 87 % in Singapore(Reference Joosoph, Abu and Yu5) and 99 % in Bangladesh(Reference Seiermann, Al-Mufti and Waid6). Fasting during pregnancy alters the timing, frequency and nutritional composition of food intake, which may have implications for fetal growth and development. Theoretical frameworks such as Barker’s hypothesis (later expanded into the Developmental Origins of Health and Disease (DOHaD) theory) suggest that prenatal nutritional exposures can influence long-term health outcomes in offspring(Reference Barker7–Reference Paneth and Susser9). Animal studies have shown that prolonged fasting during pregnancy may increase PG levels(Reference Silver and Fowden10) and stimulate uterine contractions(Reference Binienda, Massmann and Mitchell11), potentially contributing to preterm birth. In humans, extended fasting during pregnancy has been linked to elevated maternal corticotropin-releasing hormone levels and a higher risk of preterm delivery(Reference Herrmann, Siega-Riz and Hobel12). Placental corticotropin-releasing hormone plays a key role in regulating fetal growth and the timing of parturition(Reference Wadhwa, Garite and Porto13,Reference Challis14) . Conversely, Ramadan fasting has also been associated with reductions in blood glucose and insulin resistance, metabolic changes that may lower the risk of preterm birth, even among non-diabetic women(Reference Metzger, Lowe and Dyer15,Reference Kenyon and Shnnan16) . These contrasting pathways reflect the complexity of Ramadan fasting’s effects in pregnancy and point to the need for high-quality evidence.
Despite theoretical plausibility and biological mechanisms linking fasting to pregnancy outcomes, studies examining the impact of Ramadan fasting during pregnancy on outcomes such as preterm birth, low birth weight and delivery by cesarean section have shown inconsistent and controversial findings(Reference Chen, Loy and Chen17–Reference Mahanani, Abderbwih and Wendt23). In a recent comprehensive umbrella review(Reference Al-Taiar, Rahman and Salama24), there was no conclusive evidence linking Ramadan fasting during pregnancy to adverse pregnancy or birth outcomes. However, a major limitation of most existing studies is inadequate control for confounding factors. Women who choose to fast during pregnancy often differ systematically from those who do not in characteristics that are strongly associated with birth outcomes. For instance, previous studies have shown that pregnant women who perceive themselves to be physically capable(Reference Alaeddine, Schreiber and Amin25) and those with higher pre-pregnancy BMI(Reference van Bilsen, Savitri and Amelia3) are more likely to fast, both of which are important predictors of pregnancy and birth outcomes. Moreover, the effect of Ramadan fasting may differ depending on maternal pre-pregnancy BMI, making BMI both a potential confounder and an effect modifier. The absence of a robust conceptual framework and the limited understanding of fasting-related behavioural and biological factors further complicate the analysis of observational studies in this area. While a randomised controlled trial could address these methodological challenges, assigning pregnant women to fast or not fast would be unethical(Reference Al-Taiar, Rahman and Salama24). Identifying the characteristics of women who fast during pregnancy is therefore essential to guide future research.
The Kuwait Birth Cohort (KBC) study, which was launched in 2017, provides a unique opportunity to explore the characteristics of women who fast during pregnancy in a Muslim-majority setting. The overwhelming majority of Kuwaiti citizens are Muslim, and expatriate populations include other religious groups, primarily Christians and Hindus. This study has two distinct aims. The first aim is to examine differences in nutritional biomarkers between women who fast during pregnancy and those who do not. Understanding these differences is essential for informing the design of future studies, guiding appropriate adjustment for confounders and explaining inconsistencies in the literature regarding the impact of fasting during pregnancy on adverse birth outcomes, including low birth weight and preterm birth. Specifically, this aim may help researchers identify relevant confounders, develop a robust conceptual framework and interpret findings more accurately. The second aim is to identify sociodemographic, clinical and behavioural factors associated with fasting during pregnancy. Identifying these factors is important for enabling healthcare providers and policymakers to recognise women who are more likely to fast and provide culturally sensitive counselling about fasting.
Methods
Study design and study participants
The KBC is a prospective study that enrolled pregnant women during their second or third trimester while attending routine antenatal care services in the period between 2017 and 2021. Eligible participants were those in their second or third trimester who could communicate in either Arabic or English and provided written consent. The details of the cohort have been described in previous publications(Reference Al-Sabah, Al-Taiar and Ziyab26,Reference Al-Taiar, Ziyab and Hammoud27) .
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Ethics Committee of the Kuwait Ministry of Health (reference: 173/2014; approved February 14, 2017) and the Institutional Review Board at Old Dominion University (reference: 1517949). All participants provided written informed consent before enrolment. The primary objective of the cohort was to investigate the influence of various prenatal exposures, such as maternal stress and vitamin D levels, on birth outcomes. The data collection included information on Ramadan fasting during pregnancy (including trimester and duration), maternal sociodemographic characteristics, pre-pregnancy BMI, physical activity, smoking, dietary intake, depression, stressful life events and laboratory measures such as Hb, serum levels of vitamin D, RBC folate, and vitamin B12.
Data collection
Dependent variable
Data on fasting during pregnancy were obtained through face-to-face interviews by a trained data collector. Participants were first asked ‘Since you became pregnant, have you fasted any day(s)?’ with response options of ‘yes’ or ‘no’. Women who responded affirmatively were then asked to report the number of days they fasted during each trimester of pregnancy.
Independent variables
Data on sociodemographic characteristics and lifestyle factors were collected through structured, face-to-face interviews conducted by a trained data collector using a standardised questionnaire. The questionnaire was developed and underwent pilot testing among thirty pregnant women who were not part of the final cohort. Physical activity during pregnancy was assessed using the Pregnancy Physical Activity Questionnaire(Reference Chasan-Taber, Schmidt and Roberts28), a validated instrument previously validated in a similar population(Reference Papazian, El Osta and Hout29). Dietary data were collected either using selected items from the Kuwait Nutritional Surveillance System or the WHO STEPwise approach to Noncommunicable Disease Risk Factor Surveillance(30). Pre-pregnancy weight and height were self-reported by participants, whereas current weight and height were measured at the time of interview using standardised procedures. Clinical data, including pregnancy-related complications, were extracted from medical records by trained clinical staff.
Laboratory methods
Blood samples were analysed at Al Sabah Maternity Hospital, where all assays were conducted under strict quality control procedures as part of routine clinical diagnostics. Complete blood count was performed using the Beckman Coulter haematology analyser (Beckman Coulter Inc.). Serum iron and ferritin concentrations were measured using the AU DxI 700 analyser (Beckman Coulter) with commercial kits specific to each analyte (Fe: Cat. no. 6502022361861; ferritin: Cat. no. 3737551190). Levels of vitamin B12, RBC folate and 25-hydroxyvitamin D were determined using the Cobas e601 analyser (Roche Diagnostics GmbH). Vitamin B12 was measured using the Roche commercial kit (Cat. no. 7212771190), total folate in haemolysed whole blood was measured using the Roche kit (Cat. no. 7559992190) and serum 25-hydroxyvitamin D was analysed with the Roche kit (Cat. no. 9038078190).
Statistical methods
To address the first aim, we tested the differences in nutritional biomarkers between women who fasted during pregnancy and those who did not using either an independent-samples t test or a Mann–Whitney U test, depending on the distribution of the data. When nutritional biomarkers were categorised, we compared fasting groups using the Pearson χ 2 test of independence. To address the second aim, we used univariable logistic regression to examine factors associated with fasting during pregnancy. To reduce dimensionality and identify the most predictive covariates, we applied the Least Absolute Shrinkage and Selection Operator (LASSO) logistic regression with 5-fold cross-validation using the ‘cvlassologit’ command in Stata. In this approach, categorical variables were introduced as grouped terms to ensure that all levels were retained or excluded together. Variables selected at the optimal penalty parameter (lambda at lopt) were then used in multivariable analysis. Because fasting was a common outcome, relative risks and 95 % CI were estimated using Poisson regression with robust standard error rather than multiple logistic regression, as recommended for binary outcome with high prevalence(Reference Zou31). Model fit was assessed using global Wald tests, and model discrimination was evaluated by calculating the area under the receiver operating characteristic curve. Statistical significance was determined at a two-sided P-value threshold of < 0·05.
Results
A detailed description of the study participants has been published previously(Reference Al-Sabah, Al-Taiar and Ziyab26,Reference Al-Taiar, Ziyab and Hammoud27) . Of the 1108 enrolled participants, 1087 (98·1 %) responded to questions regarding fasting during pregnancy. Among them, 581 women (53·5 %; 95 % CI 50·4 %, 56·4 %) reported fasting during their current pregnancy. Specifically, 212 women (19·5 %) fasted during the first trimester, 273 (25·1 %) during the second trimester and 110 (10·1 %) during the third trimester.
Differences in nutritional biomarkers by fasting during pregnancy
Differences in nutritional biomarkers between women who fasted during pregnancy and those who did not are presented in Table 1. Compared with non-fasting women, fasting women had significantly lower levels of ferritin (P = 0·048), vitamin B12 (P = 0·001), RBC folate (P < 0·001), 25-hydroxyvitamin D (P = 0·002) and vitamin D binding protein (P = 0·011), but higher levels of parathyroid hormone (P = 0·011). These differences remained evident when biomarkers were categorised using established cut-off points (online Supplementary Table S1).
Distribution of nutritional biomarkers by fasting during pregnancy in Kuwait (n 1087)

Q1–Q3: first quartile–third quartile.
Sociodemographic, clinical and behavioural factors associated with fasting during pregnancy
Online Supplementary Tables S2–S5 present associations between various maternal characteristics and fasting during pregnancy in univariable analysis. Factors significantly associated with fasting included husband’s income (P = 0·010), age at first pregnancy (P = 0·014), number of male children (P = 0·046), interpregnancy interval (P = 0·004), use of assisted reproductive treatment (P = 0·003) and consumption of carbonated drinks (P = 0·001).
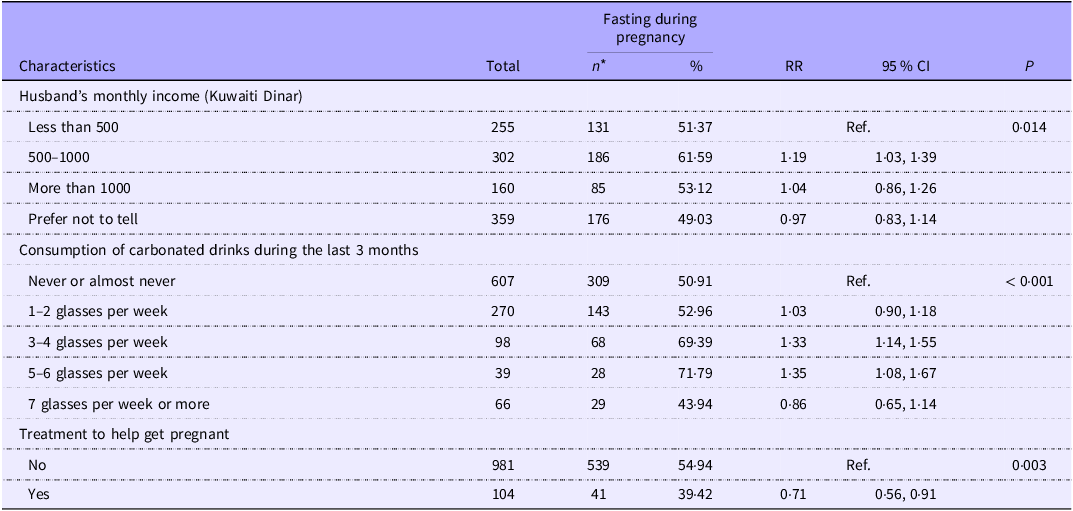
Table 2 presents factors associated with fasting during pregnancy based on a multivariable model selected using the LASSO approach. Women who fasted were more likely to fall into specific income categories and to consume carbonated drinks during the last 3 months. Additionally, women who reported receiving fertility treatment prior to conception were less likely to fast during pregnancy. However, the model demonstrated limited predictive ability, with an area under the receiver operating characteristic curve of 0·60. An alternative multivariable model was developed manually, including variables that were associated with fasting at a 20 % significance level in univariable analyses. Although this model included a larger number of variables, its predictive performance remained modest (AUC = 0·66). In this model, only the husband’s income remained statistically significant.
Factors significantly associated with fasting during pregnancy in the Kuwait Birth Cohort using multivariable analysis (n 1087)

RR, relative risk.
* Numbers in some variables do not add up to 1087 because of a few missing values.
Discussion
This study aimed to compare nutritional biomarkers between women who fasted during pregnancy and those who did not and to identify predictors of fasting in a cohort of pregnant women in Kuwait. More than half of the participants reported fasting during pregnancy. We observed several significant differences in nutritional biomarkers between the two groups. Specifically, women who fasted had significantly lower concentrations of ferritin, RBC folate, vitamin B12 and vitamin D, all of which are essential nutrients for healthy progression of pregnancy. Although these differences cannot be attributed directly to fasting, our findings highlight the need to consider maternal nutritional status when evaluating the potential effects of fasting during pregnancy on birth outcomes such as low birth weight and preterm birth.
Differences in nutritional biomarkers by fasting during pregnancy
Our results showed that women who fasted had significantly lower ferritin levels, a sensitive and specific marker of Fe stores and Fe deficiency. This is important, even in the absence of anaemia, given the limitations of using Hb thresholds alone to define anaemia during pregnancy(Reference Al-Naseem, Sallam and Choudhury32). Although the overall prevalence of anaemia in our cohort was approximately 28 %(Reference Al-Taiar, Ziyab and Hammoud27), we found no significant difference in anaemia prevalence between women who fasted and those who did not (P = 0·418). Fe deficiency is a leading cause of anaemia in pregnancy; however, Fe deficiency without anaemia reflected by reduced ferritin concentrations also poses important health risks. Previous studies have linked depleted Fe stores without anaemia to adverse outcomes such as low birth weight(Reference Ribot, Aranda and Viteri33) and other short- and long-term effects on child development(Reference Georgieff34). Although our findings do not establish a causal relationship between fasting and reduced Fe stores, they highlight the importance of considering Fe depletion as a potential confounder in future studies investigating the effects of fasting during pregnancy.
Another key difference between women who fasted during pregnancy and those who did not was folate status. Folate deficiency is a well-established risk factor for neural tube defects and other congenital anomalies(Reference Crider, Devine and Hao35,Reference Wald, Hackshaw and Stone36) . Evidence from clinical trials and community-based intervention programmes has consistently demonstrated that adequate maternal folate intake during early pregnancy significantly reduces the risk of such anomalies(Reference Berry, Li and Erickson37–Reference Czeizel and Dudás39). Similarly, vitamin B12 levels were significantly lower among women who reported fasting during pregnancy. The role of vitamin B12 in preventing neural tube defects is increasingly recognised(Reference Wald, Hackshaw and Stone36,Reference Nie, Liu and Li40) , and its deficiency, especially when combined with low folate, may further increase the risk of adverse fetal outcomes. In addition, women who fasted had significantly lower levels of vitamin D, which was accompanied by elevated levels of parathyroid hormone, suggesting a compensatory physiological response to vitamin D insufficiency. Low vitamin D levels during pregnancy have been associated with various adverse pregnancy and birth outcomes(Reference Mohamed, El Andaloussi and Al-Hendy41–Reference Papalia, Samonini and Buffat43); however, findings from randomised controlled trials assessing the benefits of vitamin D supplementation have been inconsistent(Reference Palacios, Kostiuk and Cuthbert44–Reference Moghib, Ghanm and Abunamoos51). As noted earlier, our findings do not establish a causal link between fasting and the observed differences in nutrient levels. Rather, they highlight the importance of considering these nutritional factors when evaluating the potential impact of fasting during pregnancy on maternal and birth outcomes. Additional biological markers may also warrant investigation. For instance, although data in pregnant women are limited, fasting has been associated with reductions in inflammatory markers such as IL-6 and C-reactive protein(Reference Aksungar, Topkaya and Akyildiz52). These markers have been implicated in adverse pregnancy outcomes, including pre-eclampsia(Reference Puttaiah, Kirthan and Sadanandan53,Reference Guan, Fu and Liu54) .
Sociodemographic, clinical and behavioural factors associated with fasting during pregnancy
More than half of pregnant women in our study reported fasting during pregnancy, a proportion comparable to findings from other countries such as Iran(Reference Ziaee, Kihanidoost and Younesian55) and Iraq(Reference Safari, Piro and Ahmad1) as well as Muslim women in Germany(Reference Leimer, Pradella and Fruth56) and the Netherlands(Reference Savitri, Yadegari and Bakker57). However, our estimate is lower than that reported in other settings such as the Gambia(Reference Prentice, Prentice and Lamb2), Indonesia(Reference Savitri, Amelia and Painter58) and Pakistan(Reference Mubeen, Mansoor and Hussain4).
Identifying women who are more likely to fast during pregnancy using sociodemographic, clinical and behavioural data routinely collected in healthcare settings is important for providing culturally sensitive counselling regarding fasting. Muslim women, including those in the USA and Europe, often ask their clinicians about fasting during pregnancy, yet many clinicians may feel insufficiently prepared to address these questions. A recent study in Germany showed the importance of sensitising healthcare providers to Ramadan fasting during pregnancy and of routinely addressing this issue with Muslim families of reproductive age(Reference Witte, Pradella and van Ewijk59). In our study, predictive models demonstrated limited ability to accurately identify women likely to fast based on sociodemographic, clinical and behavioural characteristics, regardless of the modelling approach used. These findings suggest that the decision to fast may be influenced more strongly by individual beliefs and attitudes than by observable sociodemographic characteristics. For instance, one study found that the most important predictors of a woman’s intention to fast during pregnancy were her perception of Islamic encouragement to fast and her belief in her own physical ability to do so(Reference Alaeddine, Schreiber and Amin25). Similarly, in rural Bangladesh, women’s beliefs about whether pregnant women should fast were significantly associated with their fasting behaviour(Reference Seiermann, Al-Mufti and Waid6). Conversely, in Iraq, the main reasons cited for not fasting included the belief that fasting is not obligatory during pregnancy and the perception that fasting would be too physically difficult(Reference Safari, Piro and Ahmad1). In Pakistan, the encouragement of family members was reported as a major influence on the decision to fast(Reference Masood, Saeed and Lakho60), while in Lebanon, the views of the pregnant women’s mothers played a pivotal role, with most women who intended to fast believing their mothers would encourage them to do so, whereas those who did not plan to fast reported that their mothers would discourage it(Reference Alaeddine, Schreiber and Amin25). In Singapore, the majority of husbands and other family members supported and encouraged fasting during pregnancy(Reference Joosoph, Abu and Yu5). Likewise, in rural Bangladesh, the partner’s attitude towards fasting was found to significantly influence a woman’s decision(Reference Seiermann, Al-Mufti and Waid6). None of these factors was investigated in our cohort. Given all the above, this highlights the need for healthcare providers to provide culturally sensitive counselling when discussing fasting during pregnancy.
Strengths and limitations
This study has strengths and limitations. One of its key strengths is the large sample size of pregnant women, with data collected through face-to-face interviews using a structured and pretested questionnaire. Another notable strength is the inclusion of biochemical measurements for key nutrients such as folate, vitamin D and vitamin B12, which are essential for maternal and fetal health. However, the study also has limitations. Notably, we did not collect data on women’s beliefs about fasting or the influence of social and familial support, particularly from husbands, which may be important determinants of fasting behaviour during pregnancy. Additionally, we did not measure certain biological markers, such as inflammatory cytokines or metabolic indicators, that may also be affected by fasting. As mentioned above, our findings do not prove a causal relationship between fasting and lower levels of nutritional biomarker but rather highlight the systematic differences between women who fast during pregnancy and those who do not, which need to be considered in future studies investigating the impact of fasting on birth outcomes. Despite these limitations, the study offers valuable insights into the characteristics of women who choose to fast during pregnancy. These findings can inform future research and contribute to the development of a conceptual framework for understanding the determinants and potential consequences of fasting during pregnancy.
Conclusion
This study found that more than half of pregnant women in Kuwait chose to fast during Ramadan. Women who fasted had significantly lower levels of ferritin, RBC folate, vitamin B12 and vitamin D, all of which are essential for optimal maternal health and fetal development. These findings highlight the importance of accounting for nutrient status when evaluating the potential short- and long-term effects of fasting during pregnancy. Moreover, our results indicate that fasting behaviour cannot be reliably predicted based on sociodemographic characteristics alone. Instead, the decision to fast appears to be driven largely by personal beliefs, religious interpretations and social influences. This highlights the need for healthcare providers to provide culturally sensitive counselling when discussing fasting during pregnancy.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114526107028
Acknowledgements
The authors would like to thank Mrs Nadien Rushdi for efforts to support the daily activities of the project.
The Kuwait Birth Cohort study was supported by the Research Sector, Kuwait University, Project ID: MC01/15.
The authors declare that there are no conflicts of interest.
A. A.-T.: study design, data collection, data analysis and manuscript writing; A. H. Z.: data collection, data interpretation and critical revision of the manuscript; R. A.-S.: study design, data collection and critical revision of the manuscript; A. N. A.: data analysis and critical revision of the manuscript; J. B.: critical revision of the manuscript; M. S. H.: data collection, data interpretation and critical revision of the manuscript. All authors have read and approved the final version of the manuscript.




 Open access
Open access