


Nurturing family environments that promote health, nutrition and early learning opportunities, nested in emotionally supportive and safe relationships are fundamental to provide children with an optimal start in life(Reference Black, Walker and Fernald1). When established during early childhood, these opportunities can mitigate the risk of poor outcomes arising from inequalities, poverty and other contextual and environmental threats(Reference Belsky, Vandell and Burchinal2,Reference Black, Walker and Attanasio3) . Opportunities for early childhood development (ECD) are influenced by the child’s immediate surroundings (e.g. parents, siblings and caregivers), immediate settings (e.g. home and community environments) and external systems (e.g. early childhood services and policies)(Reference Britto and Ulkuer4,Reference Goldfeld, Woolcock and Katz5) .
There is a growing body of evidence supporting the implementation of holistic ECD interventions integrated into and delivered through existing, cross-sectoral platforms(Reference Jervis, Coore-Hall and Pitchik6,Reference Jeong, Franchett and Ramos de Oliveira7) . Evidence from low- and middle-income countries indicates that services combining caregiving and nutrition interventions provide greater benefits for improving children’s cognitive, language and motor development, compared with single-component interventions(Reference Dulal, Prost and Karki8). Further, multi-sectoral interventions are well understood as essential for making progress to reduce undernutrition(Reference Heidkamp, Piwoz and Gillespie9). In this context, the Nurturing Care (NC) framework, globally promoted by the WHO, United Nations Children’s Fund, World Bank Group and partners(10), recommends the deployment of integrated interventions that target systems, communities, caregivers and children to promote children’s health, growth and development during infancy and early childhood. Multi-sectoral interventions delivering multiple inputs have been recognised to improve child growth and development in low- and middle-income countries (LMIC), being preferred to interventions providing only individual inputs(11). Evidence suggests that interventions combining responsive care and enhanced nutrition can leverage mechanisms from both nutrition and mother–child interactions and are likely to be more effective at improving child outcomes than interventions promoting only one of the mechanisms(Reference Bliznashka, McCoy and Siyal12,Reference Brown, Finch and Obradović13) . However, findings around improved growth outcomes are mixed in both integrated programmes, as well as single-component nutrition programmes for young children that focus only on the promotion of infant and young child feeding practices(Reference Dulal, Prost and Karki8,Reference Keats, Das and Salam14) . In other words, mother–child interactions are an important mediator of the effect of responsive stimulation and nutrition interventions. Furthermore, more attention needs to be paid to the resources caregivers require – including their health and well-being – to provide nurturing care that supports optimal growth and development (Reference Martin, Zongrone and Craig15).
While there is strong evidence based on integrated approaches, research has shown mixed results in LMIC often due to implementation challenges(Reference Kirkwood, Sikander and Roy16,Reference Galasso, Weber and Stewart17) . Implementing evidence-based ECD programmes is complex and involves substantive adaptations to local contexts(Reference Grantham-McGregor and Walker18) with varying effects on child development outcomes, even when the same curriculum is followed(Reference Jervis, Coore-Hall and Pitchik6). With the growing endorsement and demand for integrated programmes to improve ECD, evidence is needed on how to deliver them effectively through existing platforms and systems. More understanding is needed on the benefits and feasibility of leveraging the touchpoints of existing services, including maternal and child health and nutrition services, with caregivers and children during the first 1000 d.
In this study, we report whether and how the integration of additional NC activities into an existing community-based nutrition platform in Mozambique has changed caregiver practices and ECD outcomes. There is a strong rationale to promote NC interventions in the country, where 72 % of young children are at risk of poor development(Reference Lu, Black and Richter19), with a large proportion experiencing chronic undernutrition, poor early nutritional practices and lack of stimulating learning environments(20). Mozambique’s fragile health and nutritional situation has been aggravated by recent events, including conflicts in the north of the country, climate shocks (cyclones and tropical storms in the centre and north and drought in the south), residual impacts of the COVID-19 pandemic and the impact of global prices of food and essential nutritional products due in part to the war in Ukraine(21).
Building on the government’s momentum in promoting NC to improve ECD through health and nutrition services, we implemented a structured caregiving intervention in Nampula Province in northern Mozambique. Nampula is the most populated province in the country, with close to 6·5 million inhabitants, two-thirds of whom live in rural areas. There are close to one million children under 5 years of age in Nampula, comprising approximately 15 % of the province’s population(22). Children in Nampula experience some of the worst living conditions in the country. More than half of the households do not have access to a safe water source; the prevalence of stunting among children under the age of five is 46·7 %, and seven out of every 100 children born alive die before reaching the age of five(21). Our intervention complemented the existing community-based nutrition programme, which was delivered through the USAID-funded Transform Nutrition Activity to support the Government of Mozambique’s nutrition intervention package (Pacote de Intervenções de Nutrição) and Multi-sectoral Plan of Action for the Reduction of Stunting (Plano de Acção Multissectorial para a Redução da Desnutrição Crónica em Moçambique), with a package to promote holistic NC. The objective of this study was to examine the impact of the holistic NC package delivered through frontline community-based workers and volunteers on children’s developmental status, as the study’s primary outcome. The study also examined the quality of early learning at home, infant and young child feeding practices and caregiver psychosocial well-being, as secondary outcomes.
Methods
Population and study settings
We conducted a quasi-experimental study with a non-equivalent comparison group across twelve districts in Nampula.
We assigned districts to the intervention or comparison group following a feasibility approach, with smaller districts allocated to the intervention by the local implementing partner for ease of programmatic logistics alongside other implementation research activities. Six comparison districts (Mecubure, Memba, Murrupula, Mongicual, Angoche and Mogovolas) received a community-based package of nutrition, sanitation and hygiene (SH) interventions. Six intervention districts (Nacala-Porto, Larde, Lalaua, Rapale, Mossuril and Meconta) received the same nutrition and SH intervention complemented by responsive care, early learning and monitoring children’s development to improve ECD outcomes, referred to as the NC package. (Figure 1)
Intervention and comparison districts.

Intervention description
We integrated the holistic NC package into an existing programme platform for nutrition and SH activities delivered through the USAID-funded activity Transform Nutrition(23). In the nutrition and SH intervention, frontline community-based staff, including community health workers, health promoters and supported volunteer nutrition group leaders, delivered nutrition services and promoted social and behavioural change interventions organised around nutrition groups. Nutrition group leaders who facilitated the groups and conducted home visits were volunteers who were recruited from the same community and were expected to have basic literacy and numeracy skills. Using a Portuguese language manual appropriate for caregiver group interventions, nutrition groups learn and exchange knowledge and skills while following a structured programme that emphasised interactive activities, direct practice, feedback and reflection. The groups were facilitated by nutrition group leaders on a weekly basis (1·5–2 h each) over the course of about 7–8 months for groups of 10 caregivers with their children ages 0–2 years, primarily mothers, with about five community influencers including male caregivers, local leaders and others. The nutrition group leaders also conducted monthly home visits for follow-up with caregivers who participated in the community group, focusing on those who needed additional support. Community radio and video messaging, in the local language of Makhuwa, are also used to broadcast additional content at this scale.
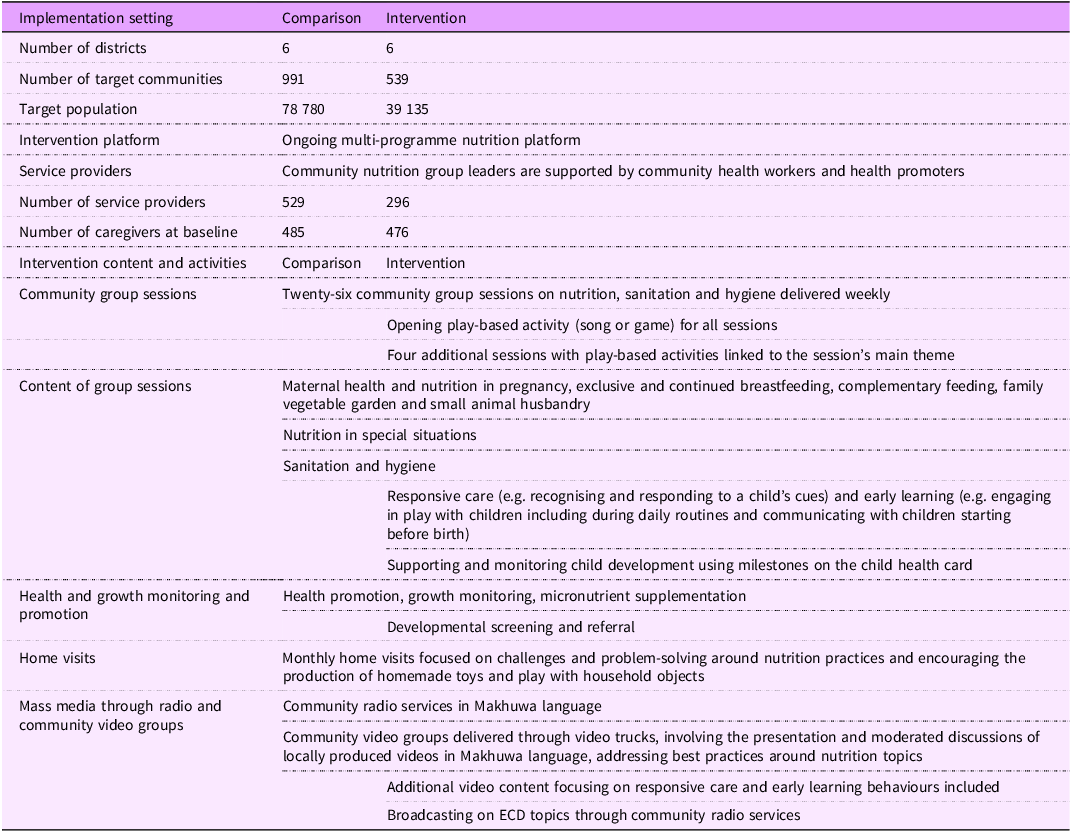
We embedded our NC activities into each of the nutrition and SH streams of activities described above and included promoting responsive care, early learning and development monitoring through community nutrition groups, home visits and radio/video spots, as detailed in Table 1. The additional components were adapted from previous studies on promoting ECD through primary healthcare in Mozambique(Reference Jeong, Bliznashka and Ahun24). We used a cascade training approach, guided by principles of adult learning, with follow-up supervision to strengthen the capacity of community-based workers to deliver the expanded NC content and support the workers to be able to successfully deliver the integrated approach. The initial training of trainers was conducted in Portuguese for district-level staff and area leaders who oversaw a cluster of community health workers and their associated nutrition group leaders. Trainees were evaluated using pre–post knowledge assessments and supervision checklists to assess the application of core skills during group sessions. Data from these tools were published elsewhere(25). The local implementing partner’s mentors supervised the nutrition group leaders and supplemented them with routine visits from the USAID Advancing Nutrition Team.
Description of intervention and comparison groups and of the intervention contents and activities
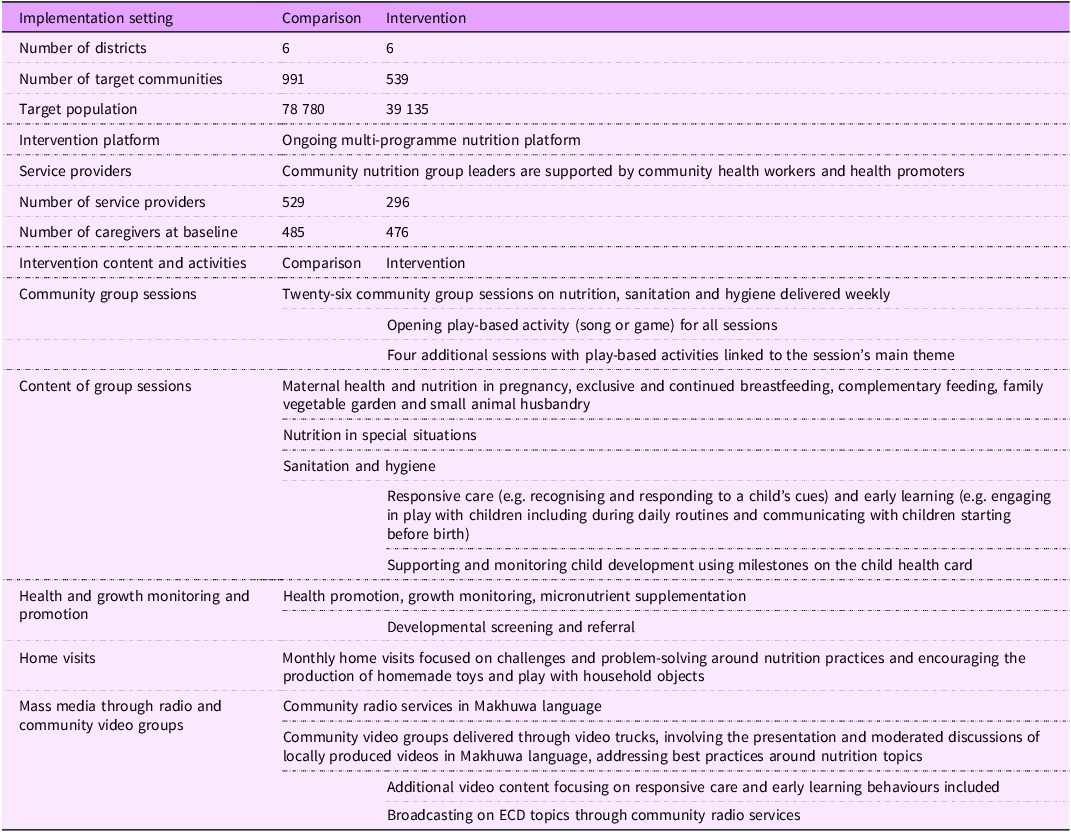
The materials for nutrition group volunteers and community health workers were provided in Portuguese, which is consistent with the approach of the Ministry of Health. Mass media radio and video spots were developed in the local language, most predominantly spoken in Nampula Province, Makhuwa.
ECD, early childhood development.
Sample design and recruitment
We identified participants in the twelve districts through Transform Nutrition programme documents on nutrition and SH interventions. Our sampling frame comprised all caregivers and their children under 24 months of age who had been identified for community-based activities from among all communities in each district. We considered primary caregivers, defined as the person providing daily care for the child, for inclusion if they were enrolled in the community groups of the nutrition and water, sanitation and hygiene intervention platform and were aged 18 years or older.
Following a cluster sample two-stage design, we first selected a sample of forty-seven communities in each district using a probability proportional to size. In the second stage, we randomly selected ten caregiver–child dyads from a list for each selected community stratified by child’s age at baseline. We aimed to obtain an equal distribution of children across six age brackets at baseline (0–2, 3–5, 6–8, 9–11, 12–17 and 18–23 months).
For each community, we followed a consistent process for informing the intervention community health workers about the selected households and seeking consent from the household prior to the completion of the interviews and assessments.
Sample size, power and detectable difference
Our sample size targets the detection of a change of 0·3 sd in overall child development, in line with a medium effect size from several systematic reviews of parenting interventions(Reference Jeong, Franchett and Ramos de Oliveira7,Reference Prado, Larson and Cox26) and assumes a design effect of 2 to adjust for clustering of caregivers in the nutrition groups (i.e. some of the caregiver–child dyads will come from the same nutrition groups), alpha of 0·05, power of 80 % and a 25 % loss to follow-up between the baseline and endline assessments.
Thus defined, we calculated that a sample of 930 caregiver–child dyads, 465 in each of the intervention and comparison groups, was required to detect differences in child development outcomes between the two groups.
Baseline and endline data collection
We collected baseline data from February to March 2022, and endline data collection took place 1 year later, from February to March 2023. Data were collected across one or two days per participating household using tablet-based data collection software. All supervisors and enumerators received standardised training on the content and intent of the survey questions, data collection software, approach to ensure ethical, secure and private data collection, as well as the process and requirements of informed consent. A validation process was completed for administration of the direct observation Global Scales for Early Development (GSED) tool. Additional details on enumerator training and evaluation are published elsewhere(27). We monitored the fieldwork progress and data quality indicators throughout the duration of data collection. Neither the data collectors nor the supervisors were blinded to the intervention assignments
Study outcomes and data collection tools
We administered eight tools to primary caregivers to collect data on the socio-demographic characteristics of the caregiver and the child, household assets and wealth, overall child development, early learning environment at home, infant and young child feeding practices and caregiver’s mental health.
Developmental status
Our primary outcome of interest was measured by the caregiver reported on the Ages and Stages Questionnaire(Reference Squires, Bricker and Twombly28) (ASQ-3), previously used in Mozambique(Reference Martinez, Naudeau and Pereira29). ASQ-3 consists of age-specific forms, each with thirty questions that capture development across five domains: fine motor, gross motor, communication, problem-solving and personal–social skills. In this study, we used 12 different ASQ-3 forms at baseline (the 2-month, 4-month, 6-month, 8-month, 10-month, 12-month, 14-month, 16-month, 18-month, 20-month, 22-month and 24-month forms) and four additional ASQ-3 forms at the end line (the 27-month, 30-month, 33-month and 36-month forms). We analysed ASQ-3 as a continuous score, standardised to in-sample sd units, using the standardised residuals from a linear regression of ASQ-3 on age, sex and the data collector. This approach is analogous to the length-for-age z-score, in that it represents deviations from the mean score given a participant’s age, sex and data collector. The GSED was included as a secondary measure of child development as part of global efforts to validate the GSED in different settings. The GSED combines direct observation and caregiver report on developmental milestones (‘combined form’) and is a global tool for measuring children’s developmental outcomes for ages 0–3 years which has been validated in diverse settings(Reference Cavallera, Lancaster and Gladstone30,Reference McCray, McCoy and Kariger31) . The GSED is analysed using the GSED Development Score (D-Score) which is converted to the development-for-age z-score (DAZ) for comparison of children’s development across ages(Reference Weber, Rubio-Codina and Walker32).
Infant and young child feeding practices
We measured infant and young child feeding practices using a 24-hour dietary recall(33) and scored the following standard guidelines(34). The minimum acceptable diet was defined as the percentage of children aged 6–23 months who had at least the minimum dietary diversity and minimum meal frequency during the previous day. Minimum dietary diversity was defined as a child aged 6–23 months who consumed at least five out of eight food groups during the previous day. Minimum meal frequency was defined as the percentage of children aged 6–23 months who received solid, semi-solid and soft foods (plus milk feeds for non-breastfed children) a minimum number of times or more during the previous day as appropriate (e.g. two feedings for breastfed children aged 6–8 months, three for breastfed children aged 9–23 months and four times for non-breastfed children aged 6–23 months).
Early learning in the home environment
We assessed home environment using the Family Care Indicators as used in the UNICEF Multiple Indicator Cluster Surveys(Reference Kariger, Frongillo and Engle35,Reference Frongillo, Basnet and Halpin36) . Early learning is defined as the percentage of children engaged in four or more activities to support learning in the last 3 days, with any adult household member, father or mother out of a maximum of six potential activities. The availability of children’s books is defined as the percentage of children who have one or more children’s books. The availability of playthings was defined as the percentage of children who played with two or more types of playthings out of three possible categories of playthings (manufactured toys or those purchased from a shop, homemade toys or household objects). Inadequate supervision was defined as the percentage of children left alone or under the supervision of another child younger than 10 years of age for more than 1 hour at least once in the last week. A total sum score for the family care indicators was calculated with the aforementioned items, with a maximum possible score of 30. We measured opportunities for early stimulation using a newly developed tool for measuring early learning for the NC Framework(Reference Hentschel, Siyal and Al Sager37) and scored it as a sum score out of a maximum of fourteen opportunities for early stimulation in the prior 24 h.
We also collected information on caregivers’ mental health using the Patient Health Questionnaire(Reference Kroenke, Spitzer and Williams38), a brief valid measure of depressive symptoms that allows screening for moderate and severe depression using predefined cut-off scores. Several studies in the region, including the validation of the tool in Mozambique(Reference Cumbe, Muanido and Manaca39), indicate that cut scores between 8 and 11 can be used, depending on the context and measurement needs. In the current study, we used a cut-off score of 9 as a cut-off for elevated symptoms of depression to have high specificity based on the validation study in Mozambique(Reference Cumbe, Muanido and Manaca39).
Statistical analysis
We used 95 % CI and P-values less than 0·05 to identify statistically significant results, unless otherwise indicated. To account for the dependence among observations within a community, we used cluster-robust standard errors, with the community as the independent unit of randomisation. To address the quasi-experimental study design and potential imbalance between the two intervention groups, we used the inverse probability of the treatment weight/propensity score weighting approach. Propensity scores were estimated using a logit model, in which the dependent variable was an indicator of whether the participant was in the ECD intervention arm or not. We selected baseline variables contributing to propensity score estimation based on their relationship to both intervention status and outcomes of interest and a background literature review and knowledge of study implementation guided us. To assess balance, we tested for variable equality across the intervention arms, as well as equality of the predicted propensity score across intervals of the predicted propensity score distribution. Common support was assessed by using standard common support graphs.
To estimate the intervention effect on continuous outcomes, we used multivariable linear models controlling for baseline outcome measurement and baseline variables potentially associated with the outcome based on theoretical background knowledge. To estimate the intervention effect on dichotomous outcomes, we used a multivariable modified Poisson model controlling for baseline outcome measurement as well as baseline variables potentially associated with the outcome based on theoretical background knowledge.
We checked assumptions for normality and homoscedasticity of residuals using Shapiro–Wilk and Breusch–Pagan tests and inspected and corrected for outliers following standard approaches. Analyses were conducted using the Stata software (version 16).
Results
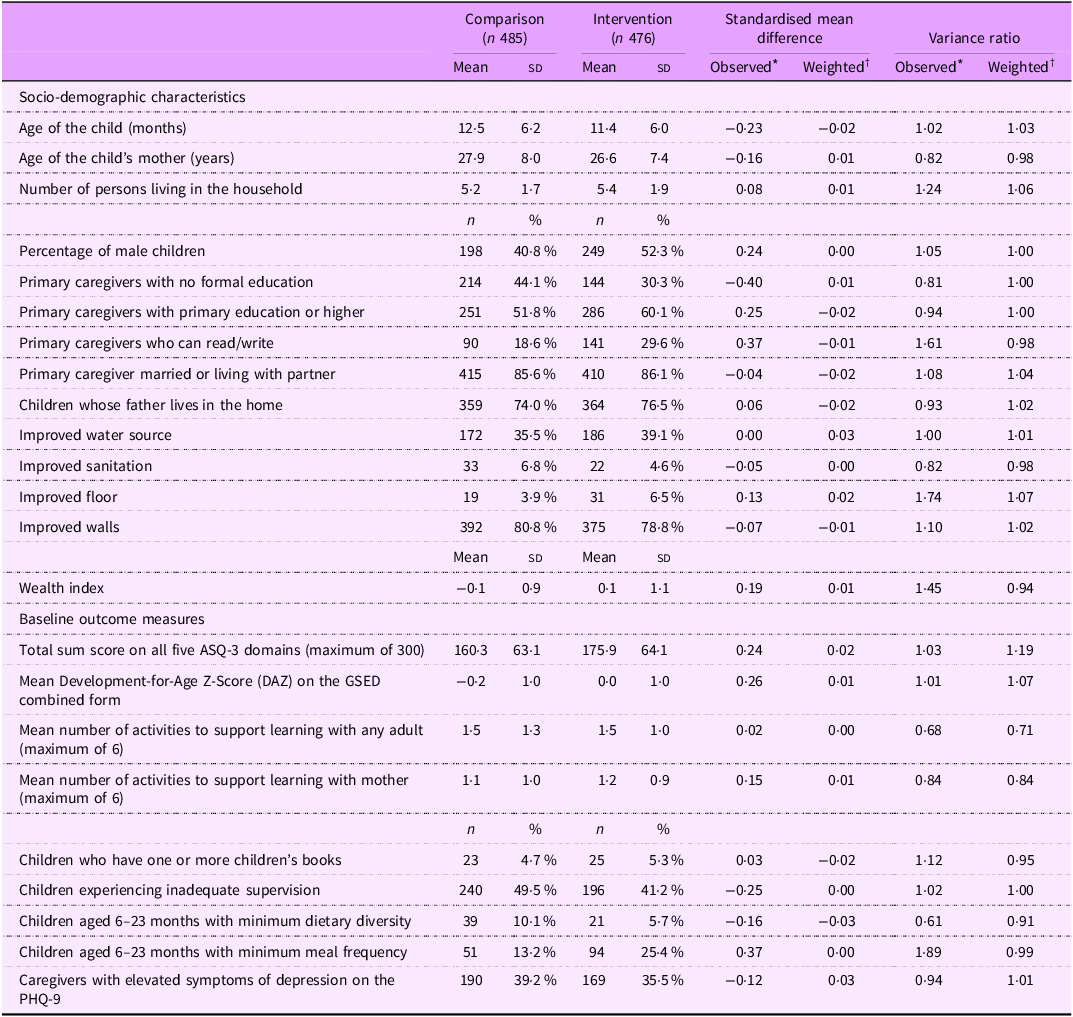
Of the 962 children included in the baseline evaluation, 875 (90·95 %) had complete matched information at the endline. Losses to follow-up were similar between the intervention and comparison groups (9·87 % and 8·04 %, respectively). Table 2 presents the characteristics of the children, caregivers and households in the intervention and comparison groups. The baseline indicators reflected the overall vulnerability of the target population, with slightly worse results for participants in the comparison group. A larger proportion of caregivers in the comparison group had no formal education than those in the intervention group (44·1 % v. 30·3 %). Children in the comparison group were more likely to be girls (58 % v. 48 %), to have participated in early stimulation activities (5·8 % v. 2·5 %), to have been left alone or under the care of another child (49·5 % v. 41·2 %) and to have higher proportions with minimum acceptable dietary diversity (10·1 % v. 5·7 %) but fewer achieving less likely to have minimum acceptable meal frequency (13·2 % v. 25·4 %). All other characteristics were generally similar, and propensity score weighting achieved a balance between the two groups (Table 2). We also confirmed balance via an overidentification test for covariate balance, P = 0·749 (indicating that the null hypothesis that covariates are balanced was not rejected).
Baseline characteristics of the intervention and comparison participants as observed and after propensity score weighting
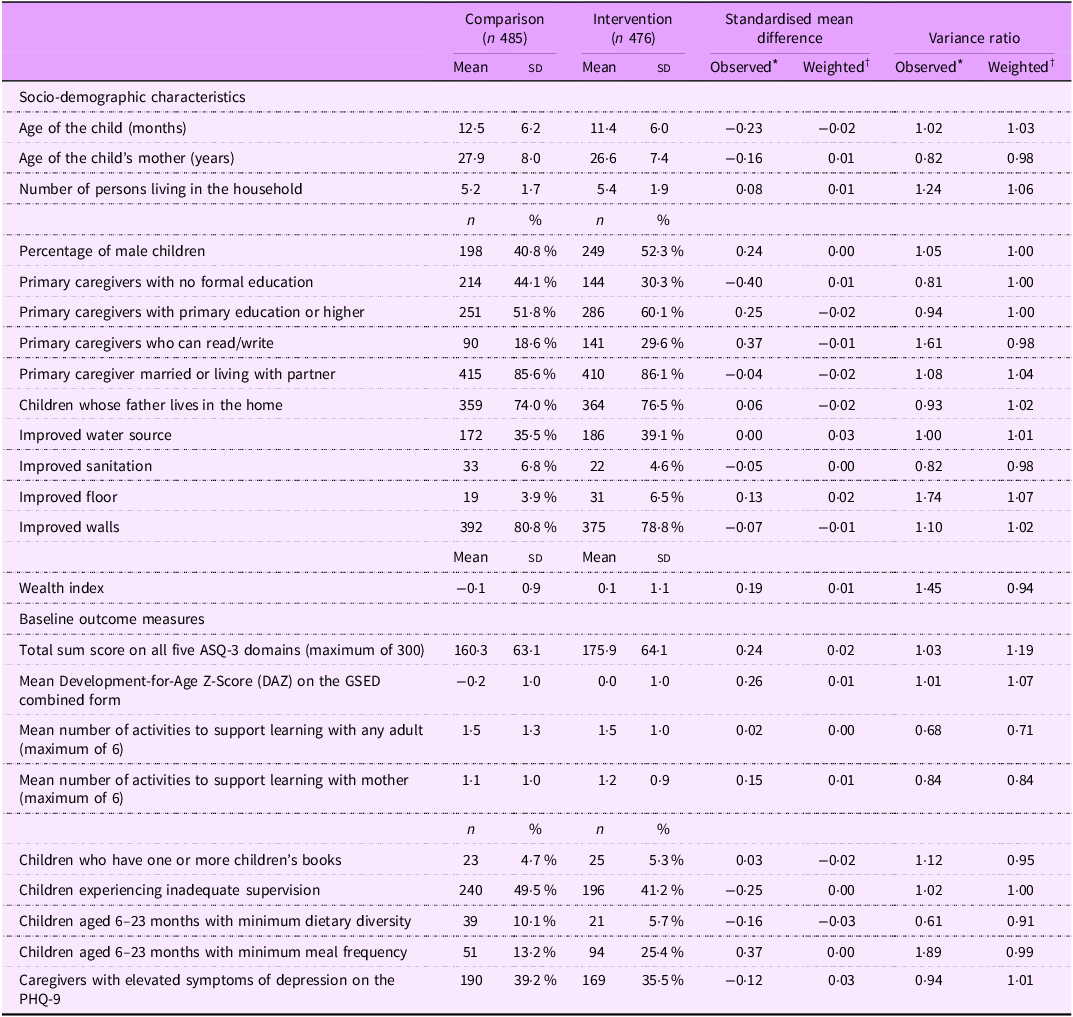
ASQ, Ages and Stages Questionnaire; GSED, Global Scales for Early Development; PHQ, Patient Health Questionnaire.
* Comparisons as observed in the unweighted data.
† Comparison adjusted by propensity score weights derived from child age and sex, baseline development assessment scores, caregiver education, literacy, household water source, sanitation, building material quality, wealth index and number of people in the household to balance the intervention arms across baseline characteristics.
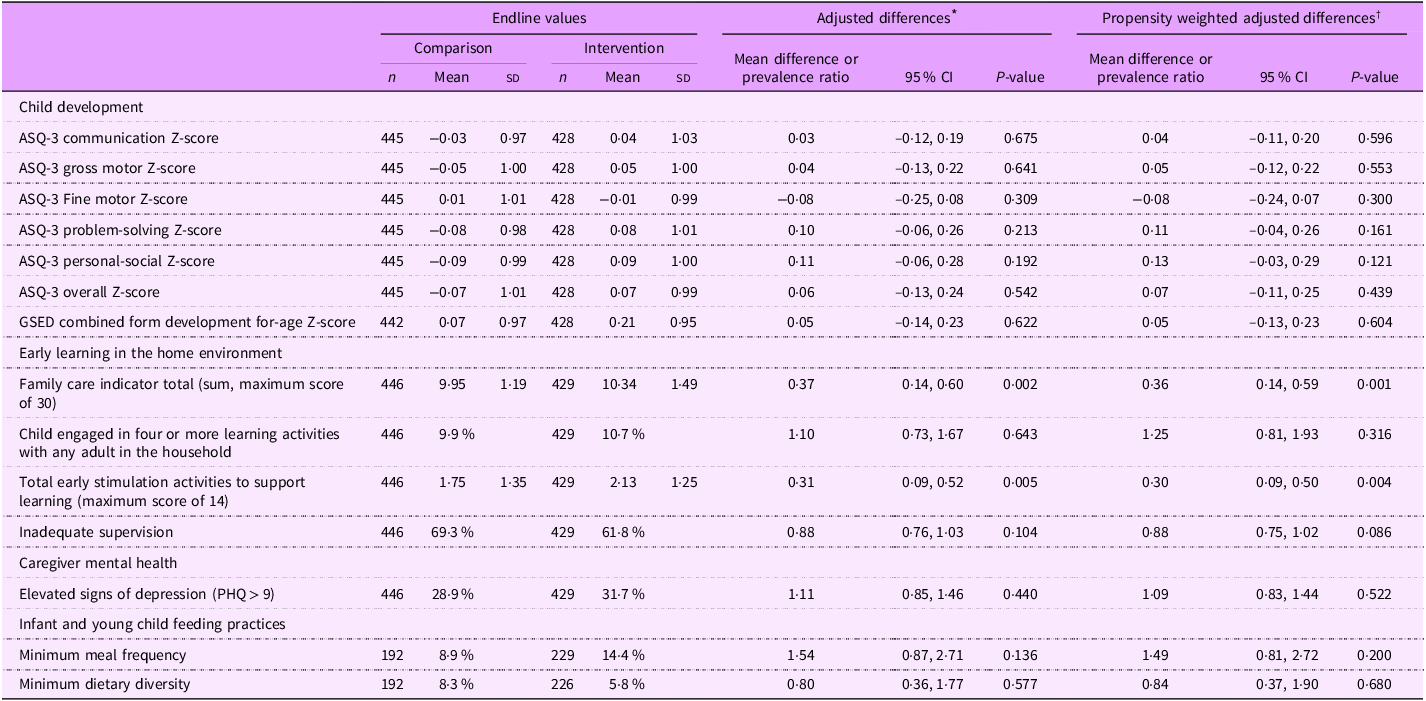
Table 3 presents the estimated intervention effect results as the endline difference in means between the groups for continuous outcomes or the prevalence ratio for binary outcomes. At the endline, we found a statistically significant mean difference between the intervention and control group total scores on opportunities for early stimulation as measured by the total score for the family care indicator (0·36 points; P ≤ 0·001) and similar differences for the total activities to support learning (0·30 activities sd; P ≤ 0·004).
Adjusted differences and propensity-weighted adjusted differences for primary outcomes at endline by group
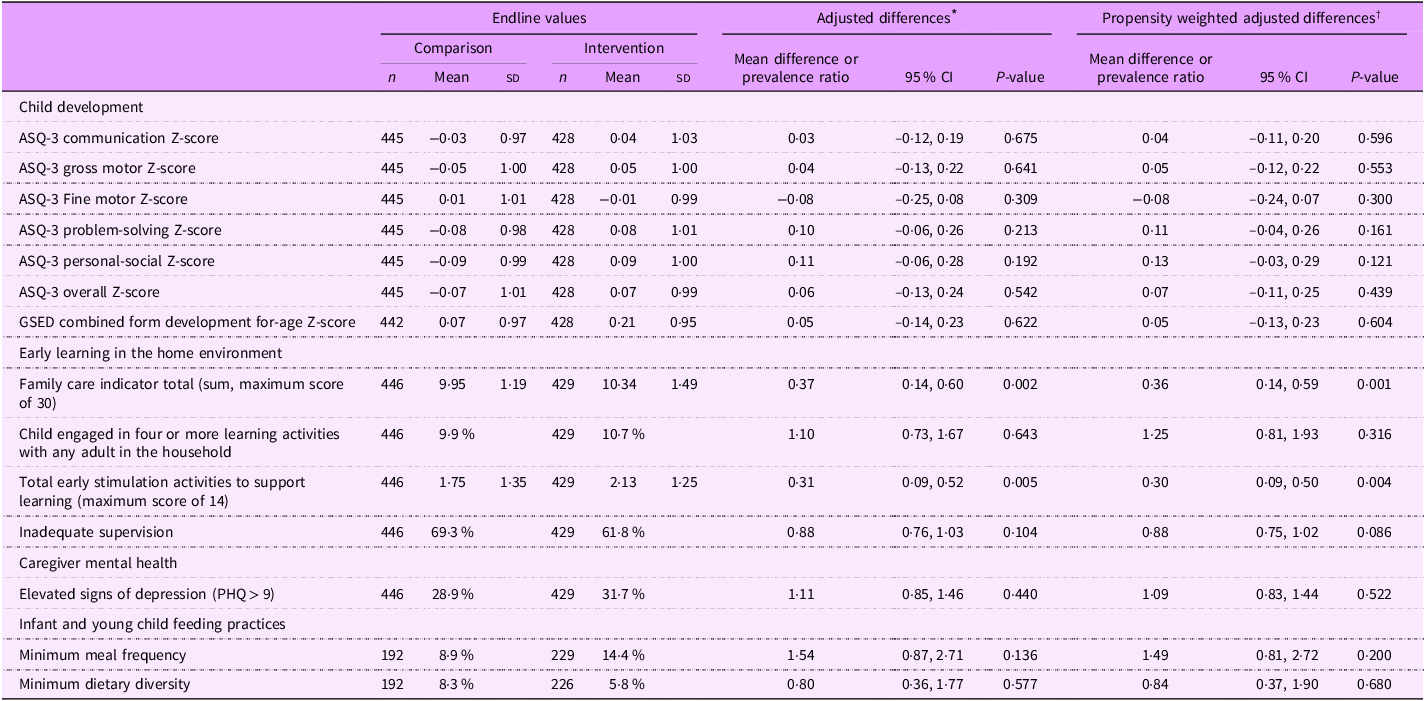
ASQ, Ages and Stages Questionnaire; GSED, Global Scales for Early Development; PHQ, Patient Health Questionnaire.
* We adjusted for differences in child age and sex, baseline development assessment scores, caregiver education, literacy, household water source, sanitation, building material quality, wealth index and the number of people in the household.
† We adjusted propensity-weighted adjusted differences for the same set of variables and additionally incorporated propensity score weighting to balance the intervention arms across baseline characteristics.
There were no measurable impacts of the intervention on the primary outcomes of ASQ-3 developmental scores (ASQ-3 or GSED), maternal mental health, infant and child feeding practices, availability of playthings in the household, number of activities carried out by the father or inadequate supervision.
Discussion
In this study, the integrated NC package building upon an ongoing platform of nutrition, sanitation and hygiene community group sessions with caregivers in Nampula, Mozambique, showed some positive results in improving engagement in certain early learning and stimulation activities in the household. Caregiver and child engagement in activities outside the home increased as a result of the intervention. Furthermore, the intervention did not yield any measurable improvements in ECD outcomes. We found no effect of the intervention on improving or worsening meal frequency and dietary diversity, the two measured outcomes for infant and young child feeding practices. This indicates that the integration of ECD content into the nutrition and SH packages did not negatively affect these nutritional outcomes but did not contribute to their improvement. These results are likely driven by challenges both in the design of the integrated programme (e.g. complexity of family needs in the context and limited duration of the intervention) as well as implementation factors (e.g. gaps in training and workforce capacity).
Design challenges
Delivering evidence-based ECD interventions at scale requires careful adaptation and consideration of entry points, adequate resources and a phased approach for testing and learning(Reference Heidkamp, Piwoz and Gillespie9). Research studies about integrating additional components of nurturing care into existing programmes at the community level have shown mixed results in terms of improvements in ECD outcomes(Reference Jervis, Coore-Hall and Pitchik6,Reference Ahun, Aboud and Wamboldt40) . In our intervention, we adapted a set of activities previously tested in the Mozambican context(Reference Jeong, Bliznashka and Ahun24) to integrate into an existing community-based platform addressing nutrition, sanitation and hygiene, with the overall objective of promoting caregivers’ knowledge and skills regarding early stimulation and responsive caregiving. However, embedding these activities into an existing intervention with several other priority behaviours to change (e.g. feeding and hygiene) could have lessened the overall effectiveness of the intervention, especially in a population with so many vulnerabilities. In addition, our NC intervention involved multiple components, including training the facilitators, delivery of caregiver group sessions, home visits, mass media and existing nutrition, sanitation and hygiene activities. A possible explanation for the limited effect on caregiving practices and the lack of improvements in ECD outcomes is the complexity of the multi-component behaviour change-focused intervention itself in a context such as Nampula, where many unaddressed needs prevail such as the high rates of maternal depression, poverty and limited caregiver education as observed in our study sample that can affect a caregiver’s ability to provide nurturing care(Reference Martin, Zongrone and Craig15). Another bundled nutrition and stimulation intervention demonstrated greater improvements in ECD outcomes with greater father involvement, which could have been strengthened in this design(Reference Jeong, Ahun and Gunaratna41). Recent evidence further emphasised the implementation challenges of multi-component interventions often resulting in lower impact compared to single-component interventions(Reference Nores, Vazquez and Gustafsson-Wright42), necessitating greater attention to implementation processes and quality supports.
The timing, intensity and duration of parenting interventions are known to contribute to the impact of these interventions(Reference Aboud, Yousafzai and Nores43). The relatively short duration of our implementation period (one year) may not have allowed sufficient time to produce measurable changes in ECD outcomes, particularly in a setting like Nampula, where families and children experience many adversities, including poverty, neighbouring conflict and climate emergencies. A similar study in Jordan found no effect of a light-touch remote adaptation of the Reach Up and Learn programme integrated with health and nutrition on children’s development(44) and implementation constraints with the community health workforce in India(Reference Kirkwood, Sikander and Roy16) and Madagascar(Reference Galasso, Weber and Stewart17) were attributed to the null results of home-visiting programmes. A home-visiting programme in Rwanda demonstrated improvements in child development among families experiencing adversities using a home-visiting approach with two structured booster visits up to six months following an initial 12-week intervention(Reference Jensen, Placencio-Castro and Murray45). With only four out of twenty-six group sessions focusing on NC spread across several months and challenges in implementing additional play-based activities that were designed to occur in every session(46), we believe that exposure to ECD-specific content may have been insufficient to bring about the desired behavioural changes. Recent evidence also highlights that programmes that have a very strong emphasis on responsive care are more effective(Reference Keats, Das and Salam14), and we explicitly covered this practice in only one session and qualitative findings highlighted how this concept in particular was not well understood by the frontline workers delivering this intervention(46).
Implementation challenges
The implementation and synchronisation of all components involved in a holistic NC intervention require significant coordination and resources, and challenges in maintaining programme fidelity have been reported, even for standardised interventions(Reference Jervis, Coore-Hall and Pitchik6). Our integrated package was delivered through technical assistance to a local non-governmental organisation. We put mechanisms in place for monitoring programme delivery, fidelity and quality throughout implementation and provided technical assistance through ongoing mentorship and support based on learning. These strategies for programme monitoring showed improvements over time based on observation checklists completed during supervision(25) and informed programmatic adjustments over time, such as expanding the training on ECD to a wider range of actors that provided support to the nutrition group leaders to reinforce this programme content. In our study, we were not able to track the actual uptake of the intervention in terms of caregiver exposure to the group sessions specifically targeting the expanded nurturing care practices. However, we cannot discard quality issues, inconsistencies in the frequency of receiving the intervention and other implementation and contextual challenges. Qualitative research alongside this study, published elsewhere, highlighted some quality issues including a reliance on nutrition group leaders lecturing from the manual rather than conducting the interactive activities as intended, which are important for effective behaviour change(46). While the implementation drew from experiences in the Mozambican context(Reference Jeong, Bliznashka and Ahun24), additional time for piloting at a smaller scale and refining the implementation approach could have been beneficial.
Training facilitators across the range of knowledge and skills required to effectively deliver NC group sessions can also be challenging. Aligned with the evidence base, our intention was to demonstrate active group practice and feedback; however, the cascade nature of the training may have made it less effective by the time it reached the level of volunteers as was indicated in the accompanying qualitative research.(46) This learning loss was evidenced by relatively lower changes in pre- and post-test scores at the lower level of the cascades, and only 43 % of trainees demonstrated mastery on pre-/post-tests overall(25). Similar challenges in cascade training models were identified during the scale-up of a nutrition programme in Madagascar(Reference Weber, Galasso and Fernald47). Techniques for stronger training at the community level or job aids that simplify the work of volunteers will need to be more carefully considered, along with alternative training models to strengthen this or other similar programmes. For instance, Abimpaye et al. found a facilitator for a group radio programme to be as effective as a more intensive programme requiring more in-person skill-building/supervision(Reference Abimpaye, Dusabe and Nzabonimpa48), Ferla et al. showed that looking at videos as part of capacity strengthening (with supervision and mentorship) improves the skills of community health workers(Reference Ferla, Gill and Komba49), and Bond et al. highlighted how effective and routine training, supervision and job aids can prepare non-specialist community workers to deliver ECD programmes(Reference Bond, Cheonga and Byansi50).
Another reason that may explain the limited impact of our intervention is the insufficient capacity of the community workers and volunteers who delivered the group sessions and other activities. Facilitators’ education level is known to directly influence the fidelity to the programme content and effectiveness of parenting and ECD interventions by shaping their understanding and ability to adequately deliver the programme’s contents(Reference Yousafzai, Rasheed and Daelmans51). Facilitators with lower education levels may have limited knowledge and may struggle to effectively communicate and implement the components of nurturing care and early stimulation interventions(Reference Pearson, Rao and Siraj52), exchange knowledge and skills with caregivers and employ appropriate instructional strategies, such as interactive sessions and hands-on activities, to enhance caregivers’ understanding and application of nurturing care and early stimulation practices(Reference Britto, Lye and Proulx53). Literacy rates in communities where our intervention took place are extremely low, and finding literate volunteers in this context will always be a barrier even when that is the recruitment criteria, which provides an additional reason to invest further in training and job aids that can mitigate the absence of some facilitators’ skills and workforce constraints(Reference Abimpaye, Dusabe and Nzabonimpa48,Reference Ferla, Gill and Komba49) . A better assessment of workforce capacity is also needed before the start of the programme, along with the alignment of tools and strategies to existing capacities(Reference Pearson, Rao and Siraj52). While we designed the programme with the intention of requiring all volunteers to be literate, this was a challenge in practice. Furthermore, we provided all the written tools in Portuguese and delivered the activities in the local language Makhuwa, which is predominantly used orally. This is important learning not only for our programme but broadly for NC interventions in Mozambique, as the current volunteer model is aligned with the government’s nutrition intervention package (Pacote de Intervenções de Nutrição) and is also primarily restricted to written implementation tools in Portuguese(54). This approach is unlikely to be successful without rethinking how to train and support facilitators through feasible and friendly implementation tools and resources, particularly in fragile settings like Mozambique and elsewhere(Reference Raven, Wurie and Idriss55). Ensuring adequate time for understanding workforce constraints and capacity to deliver an integrated package at the design and throughout implementation, with timely data for identifying challenges and employing quality improvement strategies, is essential in any NC programme.
This study had some methodological limitations that should be acknowledged. First, the impact evaluation was not a randomised study; we chose integration intervention districts based on convenience. There were some differences between the comparison districts and the intervention districts where we integrated the nurturing care package. While we attempted to adjust for potential socio-demographic differences in the analysis, we cannot fully eliminate potential bias. In addition, the lack of data on attendance and home visits limits our ability to understand the dose of the programme received. Another limitation of this study is the lack of a validated measure for child development outcomes in Mozambique, which may have resulted in a less sensitive measurement of the study’s main outcome. Likewise, while the Family Care Indicators are a valid measure of the quality of the early learning environment, they were designed in the context of global monitoring surveys(Reference Kariger, Frongillo and Engle35,Reference Frongillo, Basnet and Halpin36) and may not be sensitive enough to detect certain changes resulting from parenting interventions. Lastly, the research team was not blinded to the group assignments, which could have contributed to some bias in their assessments.
In conclusion, this study adds to the literature on the integration of additional components of nurturing care into existing programmes at the community level and highlights important challenges in achieving effective caregiver behavioural changes that can translate into improved ECD outcomes. Our NC intervention was effective in promoting the engagement of children in certain early stimulation and care practices; however, the overall exposure to early learning and responsive care opportunities remained extremely low in the targeted population. We detected no effects at the level of ECD outcomes, warranting the attention of future interventions, perhaps delivered with greater frequency, for a longer period of implementation, and with more robust mechanisms for quality improvement.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980025100554
Acknowledgements
We thank the caregivers and their children for participating in this study. We acknowledge the teams from the Government of Mozambique, USAID Advancing Nutrition and Transform Nutrition for their support in this work and collaboration throughout the study, especially Francisco Guivala, Romilla Karnati, Natacha dos Santos, Malia Uyehara, Elcio Naife, Tonecas Sunge and Leonor Voctor. We appreciate the technical assistance provided by PATH Mozambique in adapting and delivering the training package. The local research firm we collaborated with Maraxis made the study possible with key insights into the context and careful management of research activities to ensure quality data. We thank Jamie Gow, Erin Milner, Helio Penicela and Megan Thompson from the U.S. Agency for International Development, who provided guidance throughout programme implementation and study.
Authorship
F.d.C. and K.M. drafted the paper and contributed to the analysis and interpretation of the data. K.M. also supported the data collection. C.M.K. and J.Y. led the study conception and design, data collection, interpretation of the results and contributed to drafting the paper. C.D.A. contributed to the study design, led the analysis and contributed to drafting the manuscript. F.Z., A.M. and E.I. supported the data collection, interpretation of the results and critically reviewed the paper. All authors approved the final version of the manuscript for publication and are accountable for this work.
Financial support
The U. S. Agency for International Development provided financial support for this article through its flagship multi-sectoral nutrition project, USAID Advancing Nutrition. It was prepared under the terms of contract 7200AA18C00070 awarded to JSI Research & Training Institute, Inc. The contents are the responsibility of JSI and do not necessarily reflect the views of USAID or the U.S. Government.
Competing interests
C.M.K. is employed through the USAID-funded Global Solution Ventures mechanism by one of the implementers, ZemiTek LLC. The opinions herein are those of the authors and do not necessarily reflect the views of the US Agency for International Development (USAID), the U.S. Government, or ZemiTek, LLC.
Ethics of human subject participation
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by John Snow Inc. The Institutional Review Board (#21-25) was approved by the Universidade Lurio Institutional Review Board (01/Feb/CBISUL/23). Written informed consent was obtained from all subjects.




 Open access
Open access