


Pregnancy is a crucial period with short and long-term health consequences for both mother and infant(Reference Goldstein, Abell and Ranasinha1–Reference Voerman, Santos and Golab3). To date, a considerable proportion of European (37 %) and North American women (47 %) have pre-pregnancy overweight or obesity, which increases the risk of adverse pregnancy outcomes such as gestational diabetes mellitus (GDM), hypertension, pre-eclampsia, large-for-gestational-age infants, caesarean delivery and stillbirth(Reference Vats, Saxena and Sachdeva2,Reference Daly, Kipping and Tinner4) . Additionally, approximately 50 % of women have excessive gestational weight gain (GWG)(Reference Goldstein, Abell and Ranasinha1) which further increases the risk of adverse outcomes for both mother and child(Reference Voerman, Santos and Inskip5). Especially, GWG in fat mass seems to be a driver for adverse maternal metabolic profile and could influence infant adiposity and growth(Reference Balani, Hyer and Johnson6,Reference Lindsay, Most and Buehler7) , highlighting the need to also consider body composition, i.e. fat and fat-free mass, in pregnancy research(Reference Bijlholt, Ameye and van Uytsel8).
Diet is a modifiable behaviour with influence on maternal outcomes such as GWG and cardiometabolic health(Reference Ferreira, Lobo and Miranda9,Reference Flor-Alemany, Acosta and Marín-Jiménez10) . Promoting better dietary habits has also been shown to be a key component in interventions aimed at supporting a healthy GWG(Reference Muktabhant, Lawrie and Lumbiganon11–Reference Yu, Li and Qian13). One way to assess diet quality is by using dietary indices, which measure adherence to nutritional recommendations(Reference Dalwood, Marshall and Burrows14,Reference Wirt and Collins15) . Examples include the Healthy Eating Index (HEI)(16) and the Swedish Healthy Eating Index (SHEI)(Reference Moraeus, Lindroos and Lemming17,Reference Söderström, Sandborg and Nilsson18) which both assess adherence to recommendations in the USA and Sweden, respectively. Although these indices are based on country-specific nutritional guidelines, they share common components of healthy food patterns categorised by high intakes of fruit and vegetables, wholegrain, fish and low intakes of red meat(Reference Panagiotakos, Pitsavos and Arvaniti19). The advantages of using diet indices are that they can provide a more comprehensive view of dietary habits as well as adherence to national recommendations rather than focusing solely on individual dietary components. Previous research has indicated that better diet quality may have beneficial impact on health outcomes in pregnancy such as lower risk of hypertensive disorder(Reference Chen, Zhao and Mao20–Reference Xu, Wang and Bian23), improved cardiometabolic health(Reference Flor-Alemany, Acosta and Marín-Jiménez10,Reference van der Pligt, Kuswara and McNaughton24) and lower risk of developing GDM(Reference Xu, Wang and Bian23,Reference Gao, Zheng and Jiang25) . However, studies investigating the association of diet quality and combined metabolic risk (i.e. through a metabolic syndrome score (MetS)) in pregnancy are insufficient as most studies have focused on individual single cardiometabolic risk factors such as lipid profiles(Reference van der Pligt, Kuswara and McNaughton24) and hypertension in pregnancy(Reference Jarman, Mathe and Ramazani21–Reference Xu, Wang and Bian23). Moreover, the evidence on the impact of diet quality on GWG and body composition in pregnancy is scarce and inconclusive. For instance, healthy eating patterns have been associated with lower GWG(Reference Ferreira, Lobo and Miranda9,Reference Hirko, Comstock and Strakovsky26–Reference Ancira-Moreno, Vadillo-Ortega and Rivera-Dommarco28) and more favourable body composition(Reference Pellonperä, Koivuniemi and Vahlberg29), while other studies have not found an association between diet and GWG(Reference Fulay, Rifas-Shiman and Oken30,Reference Shin, Bianchi and Chung31) . Moreover, only one previous study has investigated the association between diet quality and body composition in pregnancy in women with overweight and obesity(Reference Pellonperä, Koivuniemi and Vahlberg29). Thus, more studies investigating associations between diet quality and body composition in pregnancy are warranted.
Aim
The aims of this study were to investigate the associations of diet quality (SHEI) with body composition (BMI, body fatness and fat mass index (FMI)), cardiometabolic health (MetS score, homeostatic model assessment for insulin resistance (HOMA-IR) and glycaemia) in early and late pregnancy (gestation weeks 14 and 37) and GWG.
Methods
Study design
This study used observational data from the HealthyMoms randomised controlled trial(Reference Henriksson, Sandborg and Blomberg32,Reference Sandborg, Söderström and Henriksson33) and is reported in accordance with the Strengthening The Reporting of OBservational Studies in Epidemiology – Nutritional Epidemiology checklist(Reference von Elm, Altman and Egger34,Reference Lachat, Hawwash and Ocké35) . The HealthyMoms trial (clinicaltrials.gov; NCT03298555) (n 305) examined the effectiveness of a 6-month intervention (the HealthyMoms app) on GWG, physical activity and diet compared with standard maternity care. The design and rationale of the study have been described in detail previously(Reference Henriksson, Sandborg and Blomberg32,Reference Sandborg, Söderström and Henriksson33) . Assessments were performed at baseline in early pregnancy (gestational week 14 (13·9 ± 0·7 weeks)) and follow-up in late pregnancy (gestational week 37 (36·4 ± 0·4 weeks)). This manuscript focuses on diet quality (SHEI), body composition (air-displacement plethysmography) and cardiometabolic health (glycaemia, insulin resistance and metabolic risk). In total, 305 women completed baseline assessment before randomisation in the trial. The intervention group received the HealthyMoms app, with support for health behaviours in terms of diet and physical activity, and since the intervention had an effect on diet quality(Reference Sandborg, Söderström and Henriksson33), we only included the control group in the analyses covering the follow-up measurement in the study. In total, 302 women had data on exposure in early pregnancy and 134 women in late pregnancy and were included in the analyses. The 134 women had comparable mean values for BMI, GWG, physical activity and similar distributions for parity and educational attainment compared with the whole study sample (data not shown). All but three women in early and late pregnancy, respectively, had dietary data and SHEI could be assessed. All participants reported age, parity (0 v. ≥ 1), pre-pregnancy weight and educational attainment (university degree v. no university degree). Moderate-to-vigorous physical activity was objectively measured using an accelerometer as previously reported(Reference Sandborg, Söderström and Henriksson33).
Participants
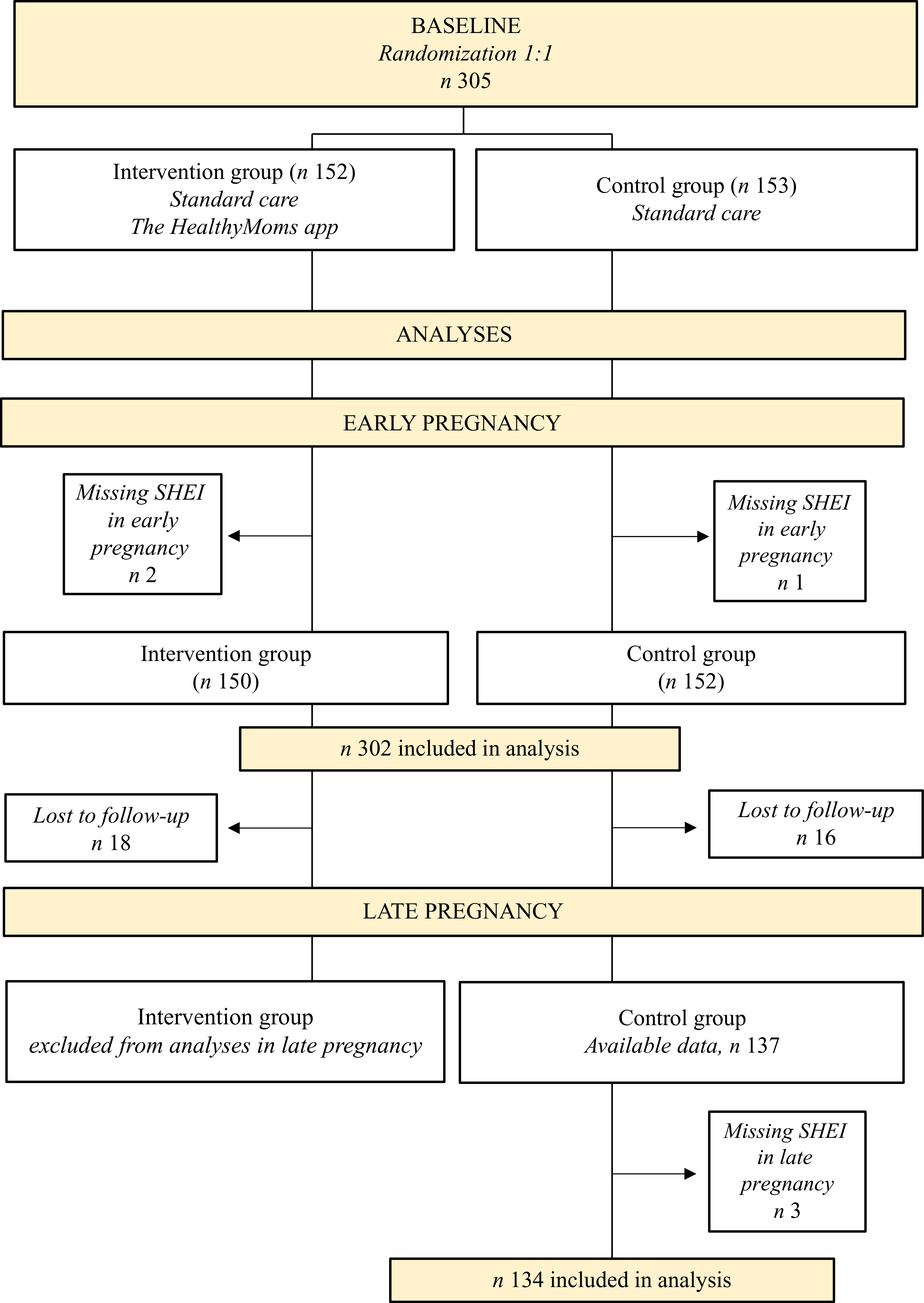
In short, women attending maternity clinics in the County of Östergötland, Sweden, were recruited during routine visits in the first trimester (between October 2017 and March 2020). Inclusion criteria were a singleton pregnancy, being ≥ 18 years and literate in Swedish in order to understand the content of the HealthyMoms app. Women previously diagnosed with an eating disorder, diabetes or other medical conditions with possible influence on body weight were excluded. As described elsewhere(Reference Sandborg, Söderström and Henriksson33), approximately 4000 eligible women entered maternity care during the recruitment period, of which 399 reported interests in participating and ninety-four women were later excluded due to not meeting inclusion criteria, declined to participate, had a miscarriage or were not able to get a hold off. A total of 305 women were enrolled and conducted the baseline assessment(Reference Sandborg, Söderström and Henriksson33). A detailed flowchart of participants at each stage of the present study is presented in Figure 1. All women received written and verbal information before entering the trial and provided their written informed consents.
Flowchart of participant inclusion and analyses in early and late pregnancy using data from the HealthyMoms trial.

Figure 1. Long description
The flowchart shows participant inclusion from the HealthyMoms trial. At baseline, 305 women were randomized to the intervention group (n 152) or control group (n 153). In early pregnancy, three participants had missing SHEI data, resulting in 302 women included in the analyses. In late pregnancy, the intervention group was excluded, and within the control group 16 participants were lost to follow-up and 3 had missing late pregnancy SHEI data, resulting in 134 women included in the analyses.
Study variables
Diet quality
A web-based dietary assessment method (RiksmatenFlex) developed by the Swedish Food Agency(Reference Lindroos, Sipinen and Axelsson36) was used to collect data on dietary intake. The method has previously been validated in pregnant women in terms of energy intake, macronutrients and key healthy and unhealthy foods(Reference Söderström, Sandborg and Nilsson18). In short, RiksmatenFlex is based on online 24-hour dietary recalls where participants register their dietary intake for three days(Reference Lindroos, Sipinen and Axelsson36). The first two days are registered consecutive, whereas the third day is randomly assigned to ensure that both weekdays and weekend days are covered. Participants were instructed to log in on a specific date, after which the days were assigned by the system. Participants were not informed in advance that they would report dietary intake for the previous day upon logging in. RiksmatenFlex provides food items, pre-specified dishes as well as photos demonstrating portion sizes to assist participants in their registration of dietary intake and support data quality. Registered intakes were automatically linked with the Swedish Food Agency’s Food composition database, which provides intake of energy, macro- and micronutrients(37), and summaries of participants’ dietary intakes were retrieved. As previously reported(Reference Sandborg, Söderström and Henriksson33) and in accordance with Moraeus et al. (Reference Moraeus, Lemming and Hursti38), energy intakes below 800 kcal/24 h were reviewed in detail by the research group, resulting in 4 d (< 800 kcal/24 h) deemed as implausible and removed from the analyses (1 in early pregnancy and 3 in late pregnancy). Dietary intake was calculated as averages of the registered days and were summarised according to a dietary index, SHEI(Reference Moraeus, Lindroos and Lemming17), which is based on key advice from national dietary recommendations provided by the Swedish Food Agency(39) and the Nordic Nutrition Recommendations(40). The SHEI consists of nine components including fruits and vegetables (g/d), fish and shellfish (g/d), red meat (g/week), fibre (g/MJ), wholegrain (g/10 MJ), polyunsaturated fat (energy percent (E%)), monounsaturated fat (E%), saturated fat (E%) and sucrose (E%)(Reference Moraeus, Lindroos and Lemming17). Individual scores for each SHEI component were calculated as a ratio between actual intake and recommended intake. Components associated with lower diet quality (i.e. intake of sucrose, saturated fat and red meat) were inverted, meaning a high intake resulted in a low score for these components. The final score for each component ranged between 0 and 1, where any scores below 0 or above 1 were recoded into 0 or 1, respectively, as previously described(Reference Moraeus, Lindroos and Lemming17). The individual scores where then summed into a total score ranging from 0 to 9, with a higher SHEI indicating better compliance with dietary recommendations and better diet quality(Reference Moraeus, Lindroos and Lemming17).
Body composition and gestational weight gain
Participant height was measured without shoes using a wall-stadiometer (Tillquist, Spånga, Sweden), and body weight was assessed through Bod Pod (COSMED) wearing only underwear. Pre-pregnancy BMI was calculated as weight prior to pregnancy (kg, self-reported) divided by squared height (m2). Body composition was measured using air-displacement plethysmography via the Bod Pod (COSMED, software version 5.2.0). The Bod Pod utilises a dual-chamber model that is based on Boyle’s law to measure body volume(Reference Most, Marlatt and Altazan41). Density is then derived by dividing body weight with body volume, followed by calculating fat and fat-free mass based on gestational week-specific density values(Reference van Raaij, Peek and Vermaat-Miedema42). FMI was calculated as fat mass (kg) divided by height squared (m2). GWG was calculated as the difference between the measured body weight in gestational week 37 and 14.
Cardiometabolic health
A fasting blood sample was taken to analyse levels of glucose, insulin, TAG, LDL, and HDL cholesterol. All analyses were performed at the Department of Clinical Chemistry, Linköping University, Linköping, Sweden, as previously described(Reference Henriksson, Sandborg and Söderström43). To measure insulin sensitivity, HOMA-IR was used. HOMA-IR was calculated as (fasting insulin (μU/l) × fasting glucose (mmol/l)/22·5)(Reference Matthews, Hosker and Rudenski44). Due to its skewness, HOMA-IR was transformed with the natural logarithm (ln), and standardisation of the HOMA-IR values was computed and used in the statistical analysis. Systemic blood pressure was measured twice using an electric sphygmomanometer (ProBP 3400 series, WelchAllyn, NY, USA) after a five-minute rest in a sitting position. If either systolic or diastolic blood pressure differed more than 10 mmHg between the two measurements, a third measurement was performed. Cardiometabolic health was assessed by means of MetS core, calculated as the sum of z-scores for TAG, inverted HDL cholesterol, glucose, the mean value of average systolic and diastolic blood pressure and FMI. The use of FMI replaced waist circumference in the score(Reference Henriksson, Sandborg and Söderström43), as waist circumference is not a suitable measure during pregnancy and since body fatness is one of the main outcomes in this study. Further, a standardisation of the MetS score was conducted and used in the analyses.
Statistical analyses
All statistical analyses were performed in R version 4.4.1 (R Foundation for Statistical Computing). A significance level of 5 % (two-sided) was considered statistically significant. Linear regression was used to investigate associations between the exposure (diet quality, SHEI) and outcomes (body fatness, BMI, FMI, glycaemia, HOMA-IR and MetS score) in early pregnancy (gestational week 14) and late pregnancy (gestational week 37), respectively. These analyses were conducted in separate models, each including one observation per participant. Prospective associations were examined by modelling SHEI in early pregnancy as a predictor of outcomes in late pregnancy. As each model included one outcome measurement per participant, no within-participant correlation across timepoints was present, and linear regression was considered appropriate. For each time point, unadjusted and adjusted models were fitted, where the adjusted models included adjustments for age, parity (0 v. ≥ 1) and educational level (university degree v. non-university degree). We also examined associations between change in exposure (dietary quality) and outcomes between early and late pregnancy, and these analyses were additionally adjusted for SHEI in early pregnancy to avoid regression towards the mean(Reference Vickers and Altman45). At last, we investigated associations between the individual SHEI components (i.e. calculated scores for fruit and vegetables, fish and shellfish, red meat, fibre, wholegrain, polyunsaturated fat, monounsaturated fat, saturated fat and sucrose) in early pregnancy with FMI and MetS score in early and late pregnancy. A higher value for scores that had been inverted, i.e. red meat, saturated fats and sucrose, corresponded to a lower intake. We chose FMI and Mets score as outcomes since FMI gives a more comprehensive view of body composition than BMI, and the MetS score includes multiple risk factors and comprises an overall indication for cardiometabolic health relevant in pregnancy.
To assess the robustness of our findings, we extended the adjusted models to also include moderate-to-vigorous physical activity (objectively measured using a wrist-worn ActiGraph wGT3x-BT accelerometer for seven consecutive 24-h periods) assessed simultaneously with the dietary assessment(Reference Sandborg, Söderström and Henriksson33), as well as total daily energy intake (kJ), and no major differences were observed (data not shown). We further investigated whether pre-pregnancy BMI had any interaction effect on SHEI and the study outcomes. However, no significant interaction effects were observed (data not shown). Finally, sensitivity analyses were conducted to account for possible energy misreporting. Basal metabolic rate (BMR) was estimated using the Henry equation in accordance with the Nordic Nutrition Recommendations(Reference Blomhoff, Andersen and Arnesen46), and the ratio of reported energy intake to basal metabolic rate (EI/BMR) was calculated. Participants with a ratio< 1·2 were considered potential underreporters and excluded from the analyses(Reference Black47,Reference Gibson48) . In total, thirty-nine participants in early pregnancy, nineteen in prospective analyses and twenty in late pregnancy were excluded from the analysis. The results showed similar associations, suggesting that energy misreporting did not materially influence the results (results not shown).
Results
Participant characteristics
In early pregnancy, participants were on average 31·3 (sd 4·1) years old, 77·4 % (233/301) had a university degree, and 57·8 % (174/301) were expecting their first child. The mean BMI was 24·2 (sd 3·8) kg/m2, and the mean level of moderate-to-vigorous physical activity was 39·0 (sd 23·6) min/d. Pre-pregnancy, the proportion of women with underweight was 2·0 % (6/302); normal weight, 69·2 % (209/302); overweight, 21·9 % (67/302); and obesity, 6·6 % (20/302).
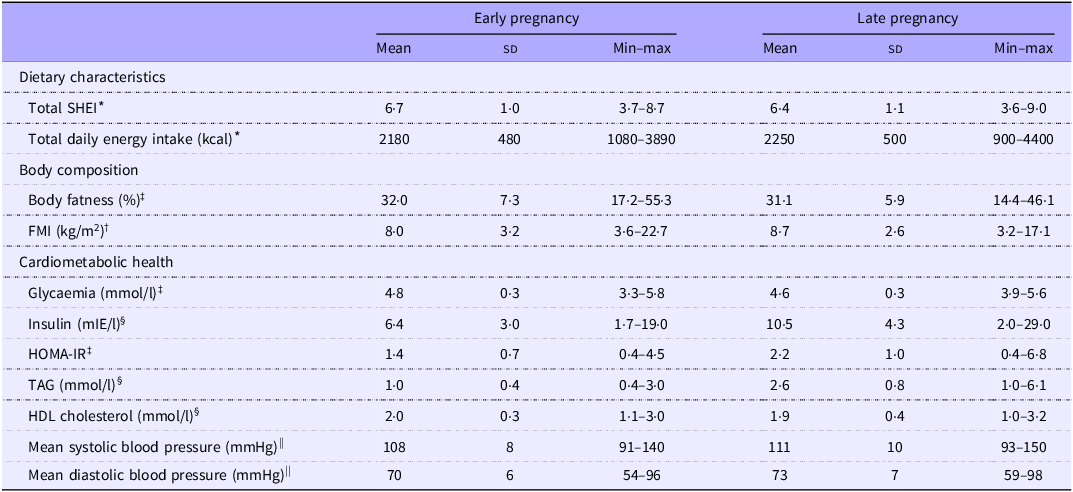
In early pregnancy, participants completed on average 2·9 (sd 0·3) days of dietary registration (n 302) and in late pregnancy 2·9 (sd 0·4) days (n 134). Scores for SHEI, energy intake, body composition and cardiometabolic health in early and late pregnancy are presented in Table 1. The average SHEI was 6·7 (sd 1·0) and 6·4 (sd 1·1) in early and late pregnancy, respectively. Body fatness and cardiometabolic outcomes including insulin and TAG were in general higher in late pregnancy.
Descriptive statistics of study sample in early (gestational week 14) and late pregnancy (gestational week 37)

Table 1. Long description
Table 1 summarizes participant characteristics in early pregnancy (gestational week 14) and late pregnancy (gestational week 37). Mean SHEI score was 6.7 (SD 1.0) in early pregnancy and 6.4 (SD 1.1) in late pregnancy. Mean daily energy intake was similar across the time points. Fat mass index was higher in late pregnancy. Cardiometabolic measures generally indicated a less favourable metabolic profile in late pregnancy, including higher insulin, HOMA-IR, triglycerides, and blood pressure, while HDL-cholesterol was slightly lower.
FMI, fat mass index; HOMA-IR, homeostatic model assessment for insulin resistance; MVPA, moderate-to-vigorous physical activity; SHEI, Swedish Healthy Eating Index.
* Early pregnancy (n 302), late pregnancy (n 134).
† Early pregnancy (n 302), late pregnancy (n 132).
SHEI, Swedish Healthy Eating Index; FMI, fat mass index; HOMA-IR, homeostatic model assessment for insulin resistance.
‡ Early pregnancy (n 301), late pregnancy (n 130).
§ Early pregnancy (n 302), late pregnancy (n 130).
|| Early pregnancy (n 302), late pregnancy (n 133).
Cross-sectional associations of diet quality and outcomes in early and late pregnancy
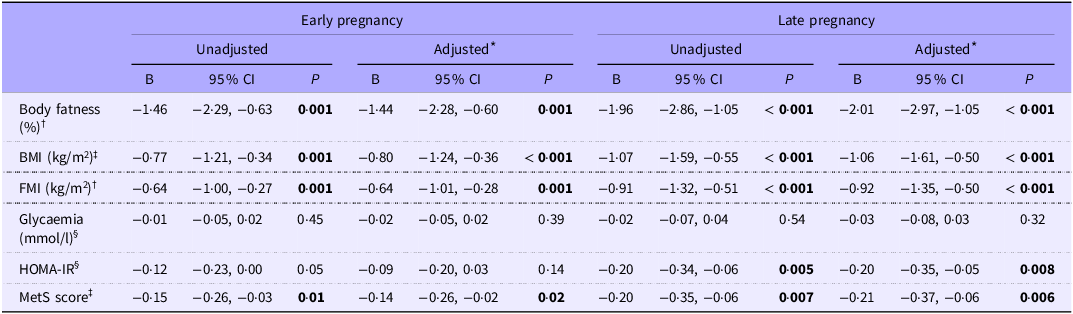
In early pregnancy, statistically significant associations were found between SHEI and body fatness, BMI, FMI and MetS score (all B ≤ −0·14, all P ≤ 0·02), but not with glycaemia and HOMA-IR (all P ≥ 0·05) (Table 2). In terms of the individual SHEI components (online Supplementary Table S1), higher intakes of the following components were associated with lower FMI in early pregnancy; fruit and vegetables, fibre, wholegrain and polyunsaturated fat (all B ≤ −1·83, all P ≤ 0·05), whereas a lower intake of red meat was associated with lower FMI (all B ≤ −1·13, all P ≤ 0·04). Moreover, for MetS score, lower intakes of red meat and higher intakes of fruit and vegetables were associated with a lower MetS score (all B ≤ −0·35, all P ≤ 0·05). No significant associations were observed between either FMI or MetS score and fish and shellfish, monounsaturated fat, saturated fat or sucrose (all P ≥ 0·14). In late pregnancy, a higher SHEI was associated with lower body fatness, BMI, FMI, HOMA-IR and MetS score (all B ≤ −0·20, all P ≤ 0·008), but not with glycaemia (all P ≥ 0·32) (Table 2).
Cross-sectional associations between diet quality (Swedish Healthy Eating Index) and body composition and cardiometabolic health in early (gestational week 14) and late pregnancy (gestational week 37) examined by linear regression

Table 2. Long description
The table presents unadjusted and adjusted linear regression analyses of the association between Swedish Healthy Eating Index (SHEI) score and body composition and cardiometabolic outcomes in early and late pregnancy. In early pregnancy, higher diet quality was associated with lower body fatness, BMI, fat mass index, and metabolic syndrome score, while no significant associations were observed for glycemia or HOMA-IR. In late pregnancy, higher diet quality was associated with lower body fatness, BMI, fat mass index, HOMA-IR, and metabolic syndrome score, whereas no significant association was observed for glycemia.
B, unstandardised regression coefficient; FMI, fat mass index; HOMA-IR, homeostatic model assessment for insulin resistance; MetS score, metabolic syndrome score. P values in bold indicate statistically significant associations (p < 0·05).
Due to missing data for some outcome variables, n varies slightly (see footnotes and numbers provided below).
* Analyses adjusted for age, parity (0 v. ≥ 1) and educational level (university degree v. non-university degree).
† Early pregnancy, n 302 in unadjusted model and n 301 in adjusted model. Late pregnancy, n 132 in unadjusted and adjusted model.
‡ Early pregnancy, n 302 in unadjusted model and n 301 in adjusted model. Late pregnancy, n 133 in unadjusted and adjusted model.
§ Early pregnancy, n 301 in unadjusted model and n 300 in adjusted model. Late pregnancy, n 130 in unadjusted and adjusted model.
Prospective associations of diet quality in early pregnancy with outcomes in late pregnancy
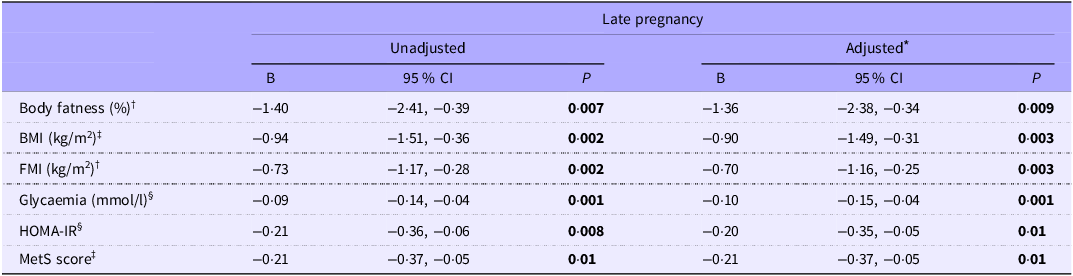
A high SHEI in early pregnancy was associated with lower body fatness, BMI, FMI, glycaemia, HOMA-IR and MetS score in late pregnancy (all B ≤ −0·09, all P ≤ 0·01) (Table 3). Among the individual SHEI components, higher intakes of fruit and vegetables, fibre, wholegrain, polyunsaturated fat and lower intake of sucrose were associated with lower FMI in late pregnancy (all B ≤ −1·75, all P ≤ 0·03). No associations were observed between FMI and intakes of fish and shellfish, red meat and saturated fat (all P ≥ 0·32). Moreover, a higher intake of polyunsaturated fat was associated with lower MetS score (all B ≤ −1·16, all P ≤ 0·02) (online Supplementary Table S2). No statistically significant associations were observed for the other SHEI components and MetS score (all P ≥ 0·06).
Prospective associations between diet quality (Swedish Healthy Eating Index) in early pregnancy (gestational week 14) and body composition and cardiometabolic health in late pregnancy (gestational week 37) examined by linear regression

Table 3. Long description
The table shows unadjusted and adjusted linear regression analyses examining whether higher diet quality in early pregnancy was associated with more favourable outcomes in late pregnancy. In both unadjusted and adjusted analyses, higher SHEI in early pregnancy was associated with lower body fatness, BMI, fat mass index, glycemia, HOMA-IR, and metabolic syndrome score in late pregnancy. The direction of all associations indicated that better diet quality early in pregnancy was related to a more favourable body composition and cardiometabolic profile later in pregnancy.
B, unstandardised regression coefficient; FMI, fat mass index; HOMA-IR, homeostatic model assessment for insulin resistance; MetS score, metabolic syndrome score. P values in bold indicate statistically significant associations (p < 0.05).
Due to missing data for some outcome variables, n varies slightly (see footnotes and numbers provided below).
* Analyses adjusted for age, parity (0 v. ≥1) and educational level (university degree v. non-university degree).
† n 133 in unadjusted and adjusted model.
‡ n 135 in unadjusted and adjusted model.
§ n 131 in unadjusted model and adjusted model.
Changes in diet quality and outcomes throughout pregnancy
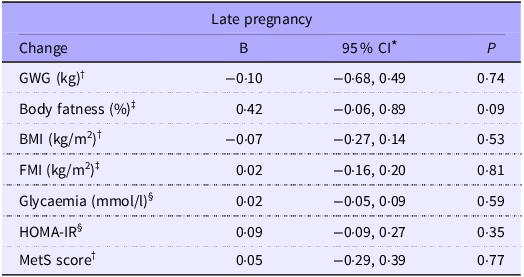
Changes in SHEI between early and late pregnancy and associations with changes in GWG, body fatness, BMI, FMI, glycaemia, HOMA-IR and MetS score are presented in Table 4. No associations were observed between change in SHEI and GWG (P = 0·74) or any other of the outcome variables (all P ≥ 0·09).
Associations between change in the Swedish Healthy Eating Index between early pregnancy (gestational week 14) and late pregnancy (gestational week 37) and change in body composition, cardiometabolic health variables and gestational weight gain between early and late pregnancy examined by linear regression

Table 4. Long description
The table presents adjusted regression analyses of associations between change in Swedish Healthy Eating Index (SHEI) score from early to late pregnancy and change in gestational weight gain, body composition, glycemia, HOMA-IR, and metabolic syndrome score. No statistically significant associations were observed between change in diet quality and gestational weight gain or any other outcome
B, unstandardised regression coefficient; FMI, fat mass index; GWG, gestational weight gain; HOMA-IR, homeostatic model assessment for insulin resistance; MetS score, metabolic syndrome score.
Due to missing data for some outcome variables, n varies slightly (see footnotes and numbers provided below).
* Analyses adjusted for age, parity (0 v. ≥ 1), educational level (university degree v. non-university degree) and Swedish Healthy Eating Index score in gestational week 14.
† n 131.
‡ n 130.
§ n 128.
Discussion
Main findings
This study is one of the first to investigate associations between diet quality and body composition in pregnancy including women from all BMI categories. Our findings suggest that better diet quality is associated with more favourable body composition and cardiometabolic health in both early and late pregnancy. A better diet quality in early pregnancy was also associated with better body composition, glycaemia and cardiometabolic health outcomes in late pregnancy. However, no association was observed between diet quality and GWG.
Comparison with previous studies
We did not observe any association between change in diet quality between early and late pregnancy and change in GWG. This finding is not surprising since dietary habits are likely to remain similar throughout pregnancy apart from an increased energy intake as a response to the higher energy demand in the last trimester(Reference Khammarnia, Ansari-Moghaddam and Kakhki49). This finding is also in line with previous studies where no associations between diet quality by means of HEI and GWG were observed(Reference Shin, Bianchi and Chung31,Reference Schlaff, Baruth and Deere50) . Moreover, a previous systematic review stated that there is limited evidence for the association of certain dietary patterns characterised by higher intakes of fruit and vegetables, legumes, nuts, fish and lower intakes of added sugars and red meat, and a lower risk of excessive GWG(Reference Donovan, Dewey and Novotny51). Individual studies have, however, reported associations between diet quality and GWG(Reference Ancira-Moreno, Vadillo-Ortega and Rivera-Dommarco28,Reference Almeida, Costa and Paganoti52,Reference Yang, Wang and Tobias53) . For instance, a study in Mexican women found that higher compliance to dietary guidelines was protective against excessive rates of GWG(Reference Ancira-Moreno, Vadillo-Ortega and Rivera-Dommarco28). Similarly, a Brazilian cohort found that a higher diet quality index was associated with lower frequency of excessive GWG in women with GDM(Reference de Almeida, da Costa and Paganoti27). In line with this, a recent population-based study reported that better adherence to healthy dietary patterns (HEI-2015, AHEI-2010 and DASH) was associated with a lower risk of excessive GWG(Reference Li, Zheng and Jiang54). In our study, we used objectively measured weight in early and late pregnancy to assess GWG, whereas other studies have relied on self-reported pre-pregnancy weight in their assessment of GWG(Reference de Almeida, da Costa and Paganoti27,Reference Shin, Bianchi and Chung31,Reference Schlaff, Baruth and Deere50,Reference Yang, Wang and Tobias53) , which could be a limitation due to the risk of under-reporting(Reference Gorber, Tremblay and Moher55) and might limit comparison across studies. Comparison might also be limited by the various methodologies used to assess dietary intakes (e.g. FFQ, self-administered and traditional 24-hour dietary recalls), categorise diet quality and the different timepoints during gestation for assessment of dietary intake and outcomes.
In addition to GWG, measures of body composition can provide more information, and one of our main findings was that higher SHEI was associated with more favourable body composition in both early and late pregnancy. Thus far, studies on the association between diet quality and body composition in pregnancy are scarce. A Finnish study by Pellonperä et al. (Reference Pellonperä, Koivuniemi and Vahlberg29) (n 110) investigated associations between diet quality and body composition in early and late pregnancy and found that better diet quality was associated with more favourable body composition, i.e. more fat-free mass in early and late pregnancy(Reference Pellonperä, Koivuniemi and Vahlberg29). Similar to our study, Pellonperä et al. (Reference Pellonperä, Koivuniemi and Vahlberg29) used air-displacement plethysmography to assess body composition; however, their study was restricted to women with overweight and obesity, and dietary intake was measured through FFQ, which may limit the comparability of results. Taken together, these findings suggest that better diet quality could be beneficial for body composition in pregnancy regardless of pre-pregnancy BMI; however, more research in this field is needed to corroborate these findings. Building on this, emerging research suggests that the maternal metabolic milieu may be more closely related to cardiometabolic health than GWG alone, particularly in populations at higher metabolic risk(Reference Niclou, Cabre and Flanagan56,Reference Söderström Shields, Kaegi-Braun and Sandborg57) . Moreover, greater fat mass gain during pregnancy has been associated with an adverse maternal metabolic profile and may also be linked to offspring adiposity and growth(Reference Balani, Hyer and Johnson6,Reference Lindsay, Most and Buehler7) . In contrast, GWG is heterogeneous and comprises fat mass, fat-free mass, extracellular fluid, as well as placental and fetal tissues(Reference Rasmussen and Yaktine58), thereby reflecting both physiological adaptations and metabolically relevant processes to varying extents. In this context, our finding that higher SHEI was associated with lower maternal body fatness and FMI, but not total GWG, suggests that diet quality may be more closely related to body composition than overall weight gain during pregnancy. However, these associations may partly reflect pre-pregnancy differences in body weight, fat mass and lifestyle behaviours, which are likely to persist into pregnancy. Future studies should explore these associations longitudinally, using repeated measures of diet, body composition and other lifestyle behaviours such as physical activity, to better understand how these factors collectively influence the quality, rather than merely the quantity, of weight gained during pregnancy.
We further found that better diet quality in early pregnancy was associated with lower glycaemia levels in late pregnancy, which is similar to recent systematic reviews and meta-analyses(Reference Xu, Wang and Bian23,Reference Gao, Zheng and Jiang25,Reference Raghavan, Dreibelbis and Kingshipp59) . In the review by Gao et al. (Reference Gao, Zheng and Jiang25), better diet quality (defined according to either Mediterranean diet, DASH, Alternate HEI, overall plant-based index or adherence to national guidelines) was associated with lower risk of developing GDM(Reference Gao, Zheng and Jiang25). Among these, adherence to national dietary guidelines was associated with the lowest risk (OR: 0·39; 95 % CI: 0·31, 0·48)(Reference Gao, Zheng and Jiang25), which is similar to the definition of diet quality in our study. Moreover, Gao et al. (Reference Gao, Zheng and Jiang25) found that better diet quality pre-pregnancy was associated with lower GDM risk, suggesting the important role of a healthy diet already before conception. It is also relevant to note that we used glycaemia as an outcome rather than GDM diagnosis, which could limit comparison between studies since thresholds for diagnosis varies(Reference Wang, Li and Chivese60). Moreover, we did not observe any associations between diet quality and glycaemia or HOMA-IR in early pregnancy, which could be explained by physiological mechanisms in pregnancy where insulin resistance tends to develop in the final trimester, resulting in higher values for glycaemia and HOMA-IR. Another main finding in this study was that better diet quality was associated with better cardiometabolic health, which is in line with previous studies looking at gestational hypertension(Reference Chen, Zhao and Mao20–Reference Xu, Wang and Bian23) and cardiometabolic risks(Reference Flor-Alemany, Acosta and Marín-Jiménez10).
In our study, a better diet quality was categorised according to adherence to national dietary guidelines, including higher intakes of fruit and vegetables, wholegrain, fibre, fish and healthy fats, and lower intakes of red and processed meat, added sugars and unhealthy fats. Indeed, this categorisation aligns with an overall healthy dietary pattern, similar to, e.g., a Mediterranean dietary pattern(Reference Panagiotakos, Pitsavos and Arvaniti19), and is comparable to dietary guidelines also in other countries(16). We found that higher intakes of fruit and vegetables, fibre, wholegrain and polyunsaturated fats and lower intake of red meat and sucrose were associated with a lower FMI, which aligns with previous findings in non-pregnant adults(Reference Boushey, Ard and Bazzano61). In addition, we observed that lower intakes of red meat and higher intakes of fruit and vegetables and polyunsaturated fat were associated with a lower MetS score. Similarly, intake of red meat has been associated with higher risk of MetS in adults(Reference Kim and Je62). Moreover, low intake of red meat, refined carbohydrates and greater intake of fruit, vegetables and fish have also been shown to have a cardioprotective effect in pregnancy(Reference Flor-Alemany, Acosta and Marín-Jiménez10). In summary, based on our findings and other existing evidence, it seems that a healthy diet may be beneficial in terms of body composition and for cardiometabolic health in pregnancy.
Strengths and limitations
This study has several strengths to acknowledge. Both cross-sectional and prospective data from the HealthyMoms trial were used and covered both early and late pregnancy(Reference Sandborg, Söderström and Henriksson33). We had a relatively large study sample and included data of pregnant women from all BMI categories. Nevertheless, it should be noted that we had a lower proportion of women with overweight and obesity (29 %) compared with the general pregnant population (47 % in 2024)(Reference Skogsdal, Conner and Elvander63), which might limit generalisability to populations with higher overweight/obesity prevalences. Moreover, all measurements were performed in a standardised manner using accurate and objective methodology to assess body composition, GWG and cardiometabolic health. Additionally, we used online 24-hour recalls (RiksmatenFlex) to assess dietary intake, and although the method is based on self-report, 24-hour recalls have to a less extent been associated with under-reporting compared with other methods (e.g. FFQ)(Reference Burrows, Ho and Rollo64). RiksmatenFlex has also previously been validated in pregnancy and showed that the method captured intakes of energy, key food groups and adherence to SHEI in a comparable way to the doubly labelled water method and 24-h dietary recalls(Reference Söderström, Sandborg and Nilsson18). Moreover, dietary intake was based on three days of data and did not include any statistical modelling (e.g. MSM or NCI) to estimate habitual intake. While this may not fully capture intake of foods consumed irregularly, the use of a dietary index reduces the influence of day-to-day variation in single food items since the score reflects overall dietary pattern rather than exact quantities of each component. For analyses of individual components of SHEI (online Supplementary material), estimates may be more affected by the limited number of intake days. Furthermore, this study is among the first to investigate the association between diet quality and body composition, which complements the measure of GWG in pregnant women of all BMI categories. Finally, we used MetS score as a measure of cardiometabolic health since the accumulation of more than one cardiometabolic outcome gives a more complete picture than only looking at a single outcome(Reference Lei, Niu and Lv65). This study also has limitations to acknowledge. First, most participants in our sample had a university degree (77 %) and the corresponding number in the female Swedish population is approximately 40 %(66). Also, participants had relatively high scores for SHEI, and these factors together might limit the generalisability of our results. However, it should be noted that the proportion of women gaining excessive weight was similar to that of Swedish women in general(Reference Henriksson, Sandborg and Blomberg67). Second, previous studies have shown that pre-pregnancy BMI may influence the association between diet and GWG(Reference Hirko, Comstock and Strakovsky68,Reference Yong, Mohd Shariff and Mohd Yusof69) and has been suggested as a stronger predictor of GWG than a healthy diet(Reference Yong, Mohd Shariff and Mohd Yusof69). Indeed, we extended our analyses to investigate any interaction effect between pre-pregnancy BMI and SHEI on outcomes but did not observe any such interaction. However, it should be noted that in this study, the sample size was rather small to investigate the influence of pre-pregnancy BMI on the association between diet and GWG, which should be further investigated in large-scale studies. On that note, it is likely that body composition and cardiovascular risk develop over time, and therefore, pre-pregnancy diet might have greater influence on these outcomes. We did not investigate dietary habits pre-pregnancy; however, this could be a topic for future research. Similarly, we only assessed dietary intake and outcomes at two timepoints, which limits the ability to capture within-individual changes over time and more complex trajectories. Future studies should therefore include more frequent measurements, potentially contributing to a more detailed understanding of how dietary patterns relate to changes in body composition and cardiometabolic health in pregnancy over time. Finally, it is relevant to note that, overall, the coefficients for the associations between SHEI and body composition outcomes and MetS score had relatively narrow CI, indicating precise estimates, even though this was a secondary analysis which was originally powered for the trial evaluation.
Public health relevance of research findings
Findings from this study could be of relevance for maternity healthcare. Although the observed associations were modest, our findings suggest that better adherence to dietary guidelines in early and late pregnancy was associated with a more favourable body composition and cardiometabolic health. For example, a one-point higher score in SHEI was associated with approximately 0·6–0·9 kg/m2 lower FMI and 1–2 % lower body fatness, corresponding to small but potentially meaningful differences at a population level. Moreover, one of our key findings suggests that dietary habits in early pregnancy were especially important and could be beneficial for maternal health also in late pregnancy. Thus, support for healthy dietary habits already upon the first contact with maternity healthcare could be warranted with additional support throughout gestation. The results also support the use of existing dietary guidelines, including the key advice captured in SHEI(Reference Moraeus, Lindroos and Lemming17). Focusing on this advice could be an accessible and straightforward strategy to use within maternity care to support healthy dietary habits among pregnant women and could be a potential target for future interventions in pregnancy.
Conclusion
Better diet quality was associated with a more favourable body composition and cardiometabolic health in early and late pregnancy, but not with GWG. These results indicate that a healthy diet in especially early pregnancy is advantageous, and focusing on key dietary advice could be a feasible and promising strategy to use within maternity care to improve body composition and cardiometabolic health in pregnancy.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114526107594
Acknowledgements
The authors would like to thank the participating women in the HealthyMoms trial and the midwives that assisted in recruitment. The authors would also like to thank Eva Flinke and Ellinor Nilsson for valuable help with data collection in the trial.
The HealthyMoms study was funded by the Swedish Research Council (2016-01147 to M.L.) and additionally supported by the Swedish Research Council for Health, Working Life and Welfare (Forte, 2017-00088 to P.H.; 2018-01410 to M.L.); Bo and Vera Ax:son Johnsons’ Foundation (to M.L.); the Strategic Research Area Health Care Science, Karolinska Institutet/Umeå University (to P.H.); the Swedish Society of Medicine (to P.H.); Karolinska Institutet (to P.H.); Lions Forskningsfond (to P.H.); and ALF Grants, Region Östergötland (M.L.). The funders had no role in study design, conduct, or reporting of this study.
M. L. is the principal investigator for the study and designed the HealthyMoms trial with P. H. E. S. S. and J. S. were responsible for participant recruitment and data collection in the trial. E. S. S. analysed the data and interpreted the data together with J. S., M. F-A., P. H. and M. L. E. S. S. drafted the manuscript, which was critically reviewed by J. S., M. F-A., P. H. and M. L. All authors reviewed and approved the final manuscript before submission.
The authors declare no conflict of interest.
The HealthyMoms trial was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Regional Ethical Review Board in Linköping, Sweden (reference numbers: 2017/112-31 and 2018/262-32).



 Open access
Open access