


Highlights
-
• People living with young-onset dementia are often unrepresented in studies exploring health system use.
-
• This study describes health system utilization for community-dwelling people living with young-onset dementia in Ontario.
-
• People living with young-onset dementia had similar comorbidity profiles to matched comparators but higher previous health system use.
Introduction
According to the World Health Organization, 1 over 55 million people are estimated to be living with dementia worldwide. In Canada specifically, there are approximately 730,000 people living with dementia, though with regional variations owing to the size and age of the population across provinces and territories. 2 The Alzheimer Society of Canada reports that in 2020, 250,300 people in Ontario were living with dementia. Both nationally and globally, this number is projected to continue to rise due to population aging.
Although the leading cause of dementia is Alzheimer’s disease, primarily affecting an older population and the leading symptom being memory loss, rarer forms of dementia are more commonly diagnosed in people under the age of 65 years. Reference Withall, Draper, Seeher and Brodaty3 The imprecise term “rare dementia” (i.e. rarer pathology), sometimes referred to as early- or young-onset dementia, includes diseases and conditions such as familial Alzheimer’s disease, young-onset Alzheimer’s disease, behavioral variant frontotemporal dementia, posterior cortical atrophy and primary progressive aphasia. Reference Harvey, Skelton-Robinson and Rossor4–Reference Kvello-Alme, Bråthen, White and Sando8 While prevalence rates of young-onset dementia are often argued to be much higher owing to challenges obtaining an accurate diagnosis, Hendriks and colleagues Reference Hendriks, Peetoom and Bakker9 estimate an overall age-standardized prevalence of 119.0 per 100,000 people between the ages of 30 and 64 years live with young-onset dementia. This translates to approximately 3.9 million people globally. More recently, Hendriks et al. Reference Hendriks, Peetoom and Bakker10 determined a global age-standardized incident rate of 11.0 per 100,000 people in the same age range corresponding to 310,000 new cases each year.
The economic, health and social costs of an increasing number of people living with dementia are of concern worldwide. Reference Long, Benoist and Weidner11 Literature documenting health utilization rates for older people living with dementia, for example, reinforces the potential strain on health and long-term care services. Reference Bronskill, Maclagan and Walker12,Reference Jones, Aigbogun, Pike, Berry, Houle and Husbands13 Unfortunately, even for the more common types of dementia, care systems are often limited or even nonexistent. Reference Giebel14 Set alongside are national contexts with fiscally constrained health and social service systems, and yet in contrast, still promoting costly initiatives that envision growing old at home, families living well with dementia, dementia-friendly communities and a rights-based emphasis on high-quality continuous care. Reference Sullivan, Camic and Harding15 And while dementia in younger people is less common, by virtue of the age of onset, its consequences have an extended impact on employment, family roles and transitions, childcare and even parental care responsibilities. Reference Stamou, Oyebode, La Fontaine, O’Malley, Parkes and Carter16–Reference Millenaar, Bakker, Koopmans, Verhey, Kurz and de Vugt18
People living with young-onset dementia are typically underrepresented in studies exploring health and social service needs. We do know that for younger people with atypical symptom presentation, their dementia diagnosis is often delayed Reference Loi, Cations and Velakoulis19 including receiving an incorrect psychiatric diagnosis. Reference Woolley, Khan, Murthy, Miller and Rankin20 Best practice assessment guidelines to promote diagnostic accuracy for younger people with atypical symptoms are also absent in many jurisdictions. Reference O’Malley, Parkes, Stamou, LaFontaine, Oyebode and Carter21 The transition to post-diagnostic care and support, if available, is not timely and often unsuitable. Reference O’Malley, Parkes, Stamou, LaFontaine, Oyebode and Carter21 Overall utilization rates of other community-based support services are largely unknown. Reference Cations, Withall and Horsfall22 While comorbidities in people with a young-onset dementia are less common than for people with a late-onset dementia diagnosis, the literature suggests that at least a third of people with a young-onset dementia diagnosis have at least one comorbidity, which likely affects their functional and cognitive decline Reference Carcaillon-Bentata, Quintin, Boussac-Zarebska and Elbaz23,Reference Gerritsen, Bakker and Verhey24 and thus impacts demands on service provision.
A growing body of research is beginning to provide insights into the barriers faced by families affected by young-onset dementia in relation to accessing health services and community support. Reference Wong, Kirk, Perlett, Karunanayake, Morgan and O’Connell25 While we have well-documented accounts of families struggling to access healthcare pre- and post-diagnosis, we have yet to quantitatively explore this further in terms of documented system utilization, regional variations given the availability of specialist diagnostic or support services or health system utilization rates as the disease progresses and the related care transitions over time.
The aim of this study was to document the range of health system use among community-dwelling people living with young-onset dementia leading to and following diagnosis at a population level in Ontario, Canada. The cohort under examination included a comparator group who did not live with young-onset dementia. We anticipate this investigation will stimulate further robust enquiry into the current barriers faced by younger people and their families as they access systems of care and social support and promote reasoned planning for dementia services in all localities.
Methods
Study design
Using a matched design, we conducted a retrospective cohort study with routinely collected population-based administrative healthcare data from Ontario, Canada. Canada provides a publicly funded healthcare system where administration and delivery are decentralized to each of the 10 provinces and 3 territories. Ontario, located in central Canada, is the country’s most populous province with the majority of its approximately 16 million multi-ethnic residents residing in the southern area. A move from hospital-centric healthcare delivery to clinically coordinated and fiscally integrated healthcare resulted in the development of Ontario Health Teams (OHT) in 2019. Reference Embuldeniya, Gutberg, Sibbald and Wodchis26 The 58 OHT group together healthcare providers to coordinate primary, acute, long-term, homecare, mental health and social and community care to a defined population. 27
The cohort comprised community-dwelling adults aged 30 to 64 years who were alive, residing in Ontario, and newly ascertained with young-onset dementia between January 2006 and March 2021 who were matched to comparator individuals without dementia. While young-onset dementia is typically defined as dementia onset prior to the age of 65 years (etiology unspecified), for the purpose of our study we used age limits and previously validated dementia algorithms Reference Jaakkimainen, Duchen and Lix28,Reference Jaakkimainen, Bronskill and Tierney29 to define our young-onset population. The algorithms use physician claims, hospitalization, and dispensed medication data to identify people with new dementia (case ascertainment date). For our cohort, we were unable to include dispensations for cholinesterase inhibitors as drug therapies for individuals younger than 65 years because they are not universally covered in Ontario. Nonresidents of Ontario, those not eligible for provincial health insurance or those residing in long-term care facilities not living within the community 60 days prior to and including the case ascertainment date were excluded from the study.
People living with new young-onset dementia were matched 1:1 to an individual who was alive on the ascertainment date with no documented history of young-onset dementia. To ensure comparability between the comparison groups, the individuals were matched based on age (±1 year), sex and number of ACG® System Aggregated Diagnosis Groups (ADGs) comorbidities (±2). Comorbidities were ascertained via The Johns Hopkins ACG® System Version 10 Reference Reid, MacWilliam, Verhulst, Roos and Atkinson30 from diagnoses recorded in hospitalization, emergency department and physician claims data in the 3 years immediately preceding the ascertainment date. This matching was done to 17,215 people with young-onset dementia.
Data sources
Ontario provides universal healthcare coverage of essential services for its residents. Daily encounters with healthcare services (e.g., physician visit, diagnostic procedure and hospital admission) are captured in health administrative databases and used for administrative or billing purposes. Datasets for this study (Supplementary Table S1) were linked using unique encoded identifiers and analyzed at ICES, an independent and non-profit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. The use of data in this project was authorized under section 45 of Ontario’s Personal Health Information Protection Act, which does not require review by a Research Ethics Board. This study is reported according to STROBE (STrengthening the Reporting of OBservational studies in Epidemiology). Reference von Elm, Altman, Egger, Pocock, Gøtzsche and Vandenbroucke31
Baseline characteristics
On the ascertainment date, we identified age, sex, neighborhood income quintile, rurality, remoteness index, northern residency and primary care provider roster status of all study participants. Neighborhood income quintile was determined by linking to census data using postal codes. Rurality was defined as living in a community with population size ≤ 10,000. Remoteness index was determined by the distance from residence to areas with population size ≥ 1,000 and population density of ≥ 400 persons per square kilometer. 32 Primary care provider status for each patient was determined using primary care enrollment model data and primary care physician renumeration codes. Specific comorbidities were identified using validated diagnostic algorithms, including diabetes, Reference Hux, Ivis, Flintoft and Bica33 congestive heart failure, Reference Schultz, Rothwell, Chen and Tu34 hypertension, Reference Tu, Campbell, Chen, Cauch-Dudek and McAlister35 asthma, Reference Gershon, Wang, Guan, Vasilevska-Ristovska, Cicutto and To36 rheumatoid arthritis Reference Widdifield, Bernatsky and Paterson37 and chronic obstructive pulmonary disease. Reference Gershon, Wang, Guan, Vasilevska-Ristovska, Cicutto and To38 We used physician and other claims data to identify a history of investigations including MRI, CT, electroencephalogram (EEG), consultations with medical specialties including family medicine, geriatrics, neurology and psychiatry, and number of admissions to the emergency department in the 3 years preceding ascertainment date.
Health system utilization
Health system use, while living in the community, was observed from ascertainment date to March 31, 2023. We examined home care visits, emergency department visits, hospitalizations, hospitalizations with discharge delay days, admissions to designated mental health beds, family physician visits, dementia specialist visits (composed of geriatric medicine, neurology or psychiatry visits), admissions to designated rehabilitation beds, placement in long-term care facilities and all-cause mortality. Publicly funded long-term and acute home care services may include homemaking, transportation, nursing care, personal care, end-of-life care, physiotherapy, occupational therapy or speech–language therapy. Discharge delays refer to a patient who has finished their medical stay in acute care but is unable to leave the hospital due to lack of capacity at the receiving facility (e.g., nursing home). Since our objective was to study health system use among community-dwelling residents over time, we censored observations for the cohort at the first occurrence of: transition to long-term care, all-cause mortality, loss of provincial health insurance eligibility or end of the follow-up period. People living without young-onset dementia were additionally censored if they met dementia case ascertainment criteria, as they were no longer eligible to serve as a comparator.
Statistical analysis
Descriptive statistics were used to compare baseline characteristics of people living with young-onset dementia to those without using the standardized difference (SD); a SD > 0.1 was considered statistically important. The association between young-onset dementia and the rate at which various health services were used was quantified using rate ratios (RRs) generated from Poisson regression models. Hazard ratios (HRs) for mortality and long-term care placement were generated from Cox regression models. All analyses were performed using SAS Enterprise Guide version 8.3.
Results
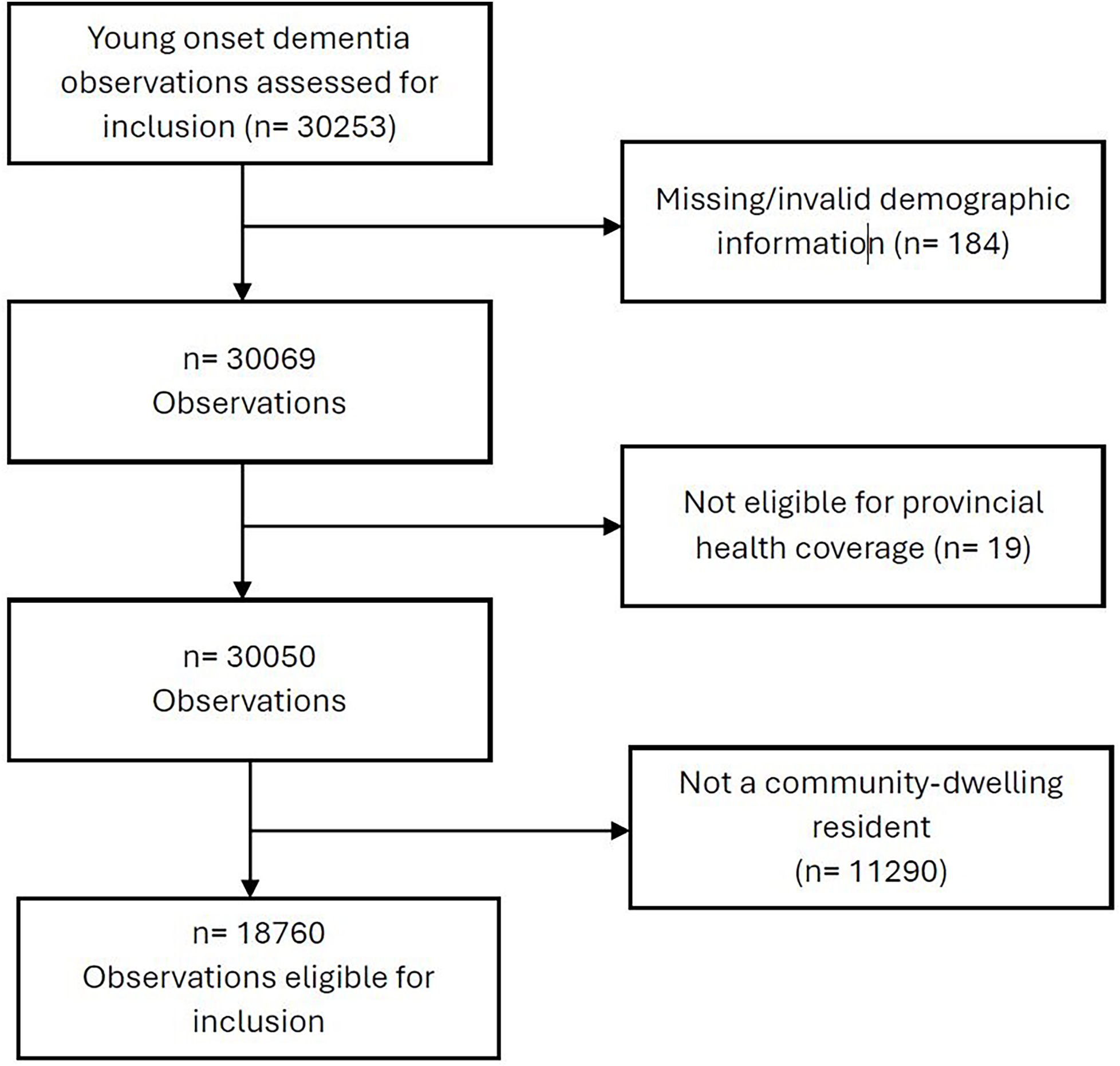
We successfully matched 17,215/18,760 (92%) of people living with young-onset dementia to a comparator group (Figure 1). The annual incidence rate of young-onset dementia for 2019 based on the cohort data was 11.5 per 100,000 person years (CI:11.0, 12.0). The data were age- and sex-standardized using the 2011 Canadian population estimates. 39
CONSORT diagram.

Characteristics of people living with young-onset dementia
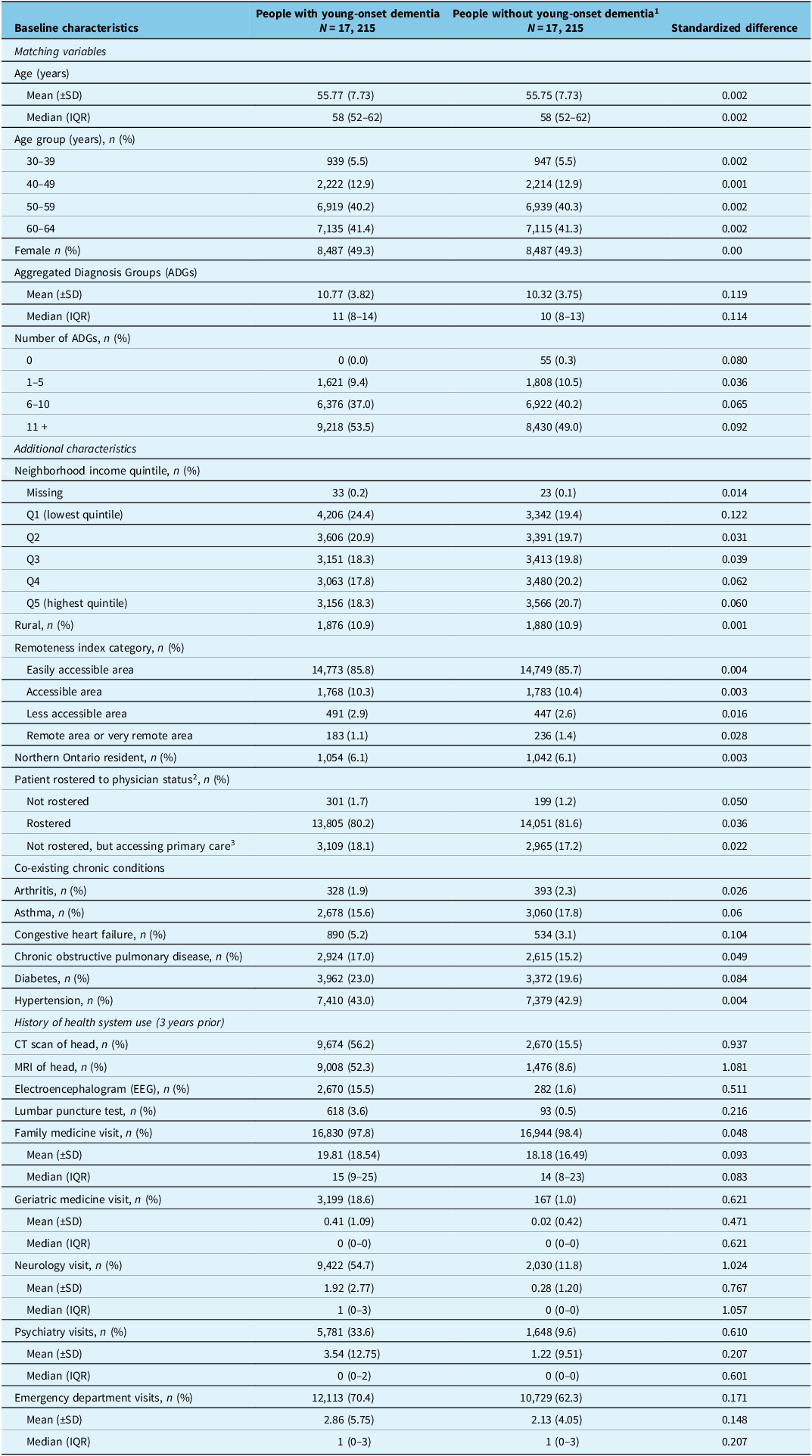
The 17,215 matched pairs had a mean age of 55.75 years (SD: 7.73), and 49.3% were women (Table 1). The comorbidity burden measured by ADGs was similar between groups; 90.5% of people with young-onset dementia (vs 89.2%) had 6 or more ADGs, indicating a high level of comorbidity. Other comorbidities were also similar across individuals, with the exception of congestive heart failure, with observed prevalence of 5.2% in persons with young-onset dementia (vs 3.1%).
Characteristics of people living with new young-onset dementia between January 2006 and March 2021 compared to those without dementia

1Matched comparison group with no documented history of dementia on case diagnosis date, matched 1:1 on sex, birthyear and Aggregated Diagnosis Groups (±2 ADGS).
2Patients are formally registered with a physician or physician practice where comprehensive care is provided, and patients only seek care from their rostered physician unless it is an emergency or while traveling.
3Patients are not formally registered with a family practice but can access core primary care services.
The neighborhood income distribution (with exception of lowest quintile) and proportion living in rural and northern settings were similar across the matched pairs. Among those with young-onset dementia, 98.3% were rostered to a physician, including not rostered but accessing primary care (18.1%), and 98.8% of matched controls of which 17.2% were not rostered but accessing primary care.
As expected, health system use prior to ascertainment date appeared consistent with investigations towards a dementia diagnosis, and treatment differed between groups. For people living with young-onset dementia, prior visits were significantly higher for geriatric medicine (18.6% vs 1%), neurology (54.7% vs 11.8%) and psychiatry (33.6% vs 9.6%). People living with new young-onset dementia also had more CT head scans (56.2% vs 15.5%), MRI head scans (52.3% vs 8.6%), EEG tests (15.5% vs 1.6%) and lumbar puncture tests (3.6% vs 0.5%). Emergency department visits were only moderately higher for those with a dementia diagnosis (70.4% vs 62.3%). For people under the age of 60 years, there was a slight increase in diagnostic testing and dementia specialist visits (Supplementary Table S2).
Rates of health system use
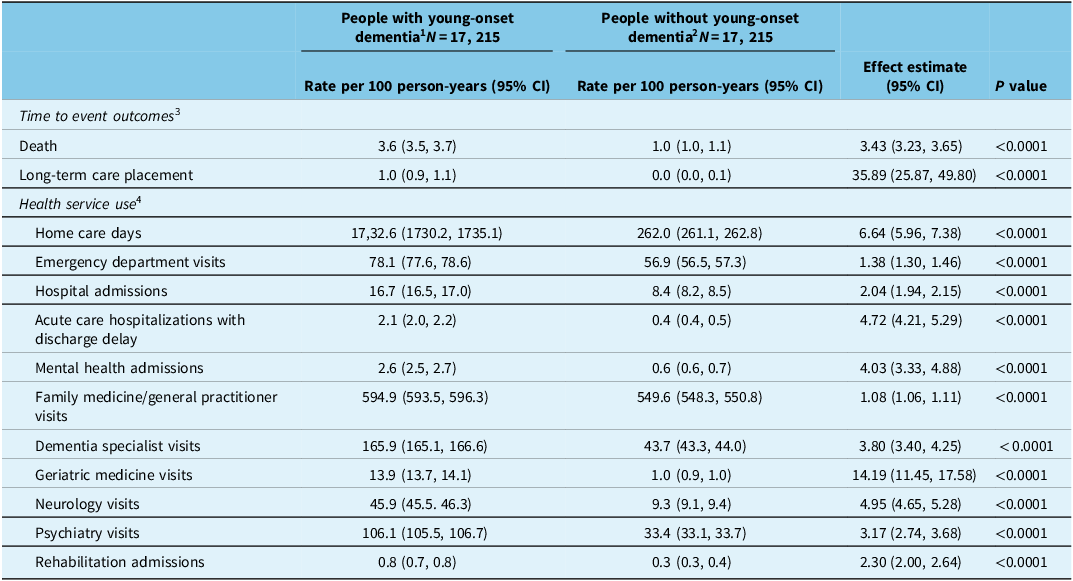
People living with new young-onset dementia had marginally higher family medicine visit rates; however, there was significantly greater use of other health services (Table 2). Compared to people without dementia, there was a twofold higher rate of hospital admission (RR = 2.04, 95% CI 1.94 to 2.15), a fourfold increase in mental health admissions (RR = 4.03, 95% CI 3.33 to 4.88) and a 38% increased rate of emergency department visits (RR = 1.38, 95% CI 1.30 to 1.46) during the follow-up period. The rate of acute care hospitalizations with discharge delays was 4.72 times higher (95% CI 4.21 to 5.29), and home care days were 6.64 times higher (95% CI 5.96 to 7.38). Dementia specialist visits, including geriatric medicine (RR = 14.19, 95% CI 11.45 to 17.58), neurology (RR = 4.95, 95% CI 4.65 to 5.28) and psychiatry (RR = 3.17, 95% CI 2.74 to 3.68) were 3.80 times higher (95% CI 3.40 to 4.25).
Health service use among people with young-onset dementia after diagnosis compared to those without dementia

1 Follow-up after case ascertainment date concluded upon first occurrence of death, loss of health insurance eligibility, dementia diagnosis (only for matched participants free of young-onset dementia) or March 31, 2023.
2 Matched comparison group with no documented history of dementia on case ascertainment date, matched 1:1 on sex, birth year and Aggregated Diagnosis Groups (±2 ADGs).
3 Hazard ratios generated using cox proportional hazards models.
4 Rate ratios generated using Poisson regression models; rates are expressed per 100 person-years.
The HR (35.89, 95% CI 25.87 to 49.80) of long-term care placement for people living with new young-onset dementia relative to those without was very high which may be explained by the rare incidence of placement among persons of similar age without a dementia diagnosis, so this estimate is likely primarily driven by the baseline rate of long-term care placement for this cohort. There was a twofold higher rate for rehabilitation services (i.e., designated inpatient beds), whether specialized units or general rehabilitation programs (RR = 2.30, 95% CI 2.0 to 2.64). Finally, the hazard of mortality rate was 3.43 times higher (95% CI 3.23 to 3.65) for people with new young-onset dementia.
Discussion
As far as we are aware, this study offers a first account of health system use for community-dwelling individuals living with new young-onset dementia at a population level in Canada. We observed high rates of comorbidity and higher rates of secondary and tertiary health system utilization among individuals with new young-onset dementia. Our study offers valuable preliminary insights on the range of health service use for a growing population that is typically overlooked in dementia-related research and health service planning. Our work also reinforces the need for further empirical investigation with respect to health system use over the trajectory of the illness for the different variants of young-onset dementia. This would include developing an understanding of interventions for both dementia and mental or physical comorbidities, variations among diverse populations, and expanding explanations for the utilization rates described.
At baseline, the characteristics of persons living with young-onset dementia were not unsurprising given the types of dementia associated with earlier onset are indeed rarer, and often either underdiagnosed or misdiagnosed. Reference Widdifield, Bernatsky and Paterson37 For those newly ascertained as living with dementia, the mean age was 55.75, plus a significant minority in younger age categories. This is important given we know that younger people may be living with symptoms for as long as 5 years before a formal diagnosis is obtained. Reference Kvello-Alme, Bråthen, White and Sando8,Reference van Vliet, de Vugt and Bakker40,Reference Rossor, Fox, Mummery, Schott and Warren41 In addition, people are likely to be living 10 or more years without benefiting from specialized geriatric services where ongoing dementia care is often located but normally targeted to individuals over the age of 65 years. This may or may not account for the relatively low number of geriatric medicine visits (18.6%), for example.
Given the lack of specificity in the diagnostic coding within the health administrative databases, differential dementia diagnoses are unknown. An even distribution among males versus females in this sample is consistent with Reference van Vliet, de Vugt and Bakker40 who identified similar young-onset dementia incidence rates between males and females. Knowledge of ethnocultural differences was also not available. A minority of our sample resided in rural or remote locations, and while this was not unexpected, this number may not have captured those who have not had a dementia diagnosis due to more limited access to regular primary care and specialist diagnostic services in these regions of the province. Specialist neurological services and memory clinics are more often only available in large urban centers such as Toronto, Ottawa or London. For example, in northwestern Ontario, people residing in rural communities may have to travel up to 6 hours by car to access these services in the only tertiary care center located in Thunder Bay. Geographic distances and reduced access to family physician visits, specialist visits and all type prescription drug dispensations for people living with dementia in rural areas was recently reported on by Kosteniuk and colleagues. Reference Kosteniuk, Osman and Osman42
Positively, almost the entire sample was rostered to a primary care physician, meaning they had access to a family physician. In Ontario, family physicians often provide a referral pathway to additional health services such as physician specialists and subspecialists. Although most of the cohort living with young-onset dementia also lived in a remote index classified as “easily accessible area,” geriatric medicine, neurology, psychiatry visits and imaging tests (CT, MRI and EEG) were few considering existing recommendations for systematic assessment to accurately diagnosis dementia, particularly when young in onset. Reference O’Malley, Parkes, Stamou, LaFontaine, Oyebode and Carter21 For example, only about half the sample had a prior neurology or psychiatry visit, and/or CT scan or MRI. Although there is a lack of consensus on factors contributing to specialist referral rates Reference Chan and Austin43,Reference Hussey and Butler44 and the diagnosis pathway for young-onset dementia is variable (e.g., neurology vs memory clinic), Reference Carter, Oyebode and Koopmans45,Reference Belder, Schott and Fox46 we do know that timely diagnosis is a critical factor for new therapies and stress management and adaptation once the diagnosis is confirmed. Reference Bronskill, Maclagan and Walker12,Reference Jones, Maclagan and Watt47
In terms of primary healthcare service utilization, the data demonstrate significant differences between those living with young-onset dementia versus the comparator group over time. Hospital admissions, emergency department visits, mental health admissions and delayed discharge from acute care for people living with young-onset dementia were each significantly higher, similar to prior studies in older ages Reference Damsgaard, Janbek and Laursen48 and recent young-onset dementia study cohorts elsewhere. Reference Damsgaard, Janbek and Laursen48 Interestingly though, family physician visits remained relatively similar for both cohorts. Multiple explanations may account for this complex pattern of health system use including both a consideration of the precipitating health condition(s) and its acuity, and other contextual factors. For example, utilization rates may reflect access barriers to primary care providers, Reference Webster49 difficulties obtaining community health supports or other specialist services, Reference Duong and Vogel50 absence of specialist knowledge to effectively understand and implement supportive strategies for behavioral symptoms, Reference Trivedi, Braun and Dickinson51 higher incidence rates of physical and psychiatric comorbidities Reference Webster49 or simply a lack of understanding on how best to treat and manage medical comorbidities when someone also lives with a dementia diagnosis. Reference Bergman, Borson and Jessen52
In addition to hospital admissions and emergency department visits, people living with young-onset dementia also had high rates of home care visits and long-term care placements. It appears that despite the availability of home and community-based care, this did not lessen or sufficiently supplement the demand for acute healthcare services. This situation may be further understood by home care’s capacity to support and focus on physical health, increasing resource rationing, or by the absence of tailored dementia support for younger people and their families. Reference Bronskill, Maclagan and Walker12,Reference Sullivan, Camic and Harding15 Similarly, a higher hazard of long-term care placements, often premature and unsuitable for younger people living with dementia, Reference Trivedi, Braun and Dickinson51 might also reflect the absence of adequate or age-appropriate community-based supports to enable individuals to live at home to maintain their quality of life. Reference Mayrhofer, Mathie, McKeown, Bunn and Goodman17,Reference Giebel, Eastham, Cannon, Wilson, Wilson and Pearson53
The increased use of rehabilitation services, although low, and possible precipitating factors are not understood given there are few organized specialist rehabilitation services for people living with young-onset dementia. Given that recent evidence suggests that individuals diagnosed with a young-onset dementia have higher incidence rates of injuries due to falls, Reference Giebel, Eastham, Cannon, Wilson, Wilson and Pearson53 we hypothesize that service use here might be accounted for by falls and related fractures, possible rehabilitation following surgical procedures or possibly inpatient behavior support therapies.
The data also draw attention to significant differences in mortality between the two matched cohorts. The higher hazard of mortality for people living with young-onset dementia was not unexpected; however, further knowledge pertaining to cause(s) of death in the administrative data is unknown. Although cause of death is complex, various studies point to a shortened life expectancy following a diagnosis of dementia earlier in life. For example, Gerritsen and colleagues (2019) suggest that life expectancy after a diagnosis of young-onset dementia was reduced by 51% for males and 59% for females compared to the general population of a similar age. Reference Gerritsen, Bakker and Verhey54 An exploration of dementia subtypes may provide additional data to facilitate support for advanced care and end-of-life care planning.
While we have begun to document health system utilization among community-dwelling people living with young-onset dementia, we are yet unable in the existing administrative data to articulate health needs and healthcare access according to the dementia subtypes that normally affect younger people. For example, mental health admissions or long-term care placements may be more likely for someone living with behavioral variant frontotemporal dementia owing to complex symptoms and delayed discharges associated with someone living with a memory-led dementia given the potential for safety issues considering forgetfulness (see for example Loi et al. Reference Loi, Cations and Velakoulis19 To develop further knowledge here would necessitate the health administrative data to specify the type of dementia alongside further exploration of primary care referral patterns including specialist and other health and allied health services delivered.
Strength and limitations
The strength of this study is that it is the first Canadian, population-based study to examine community-dwelling persons living with new young-onset dementia matched to persons without dementia in relation to health system utilization. The illustration of specific health system utilization effectively stimulates the need for further attention to the physical health needs of people living with young-onset dementia, their intersection with mental and social health needs, the current limitations of primary healthcare and the current gaps in other community-based supports. This is important for health and social services planners as Canada, like most other countries around the globe, continue to grapple with the dementia projections for the coming decades.
However, some important limitations that are inherent with this dataset should be noted. First, our administrative data definition of young-onset dementia, although validated in a primary care population sample, is not a clinical diagnosis of dementia and thus the potential for misclassification and undercounting. As previously mentioned, to identify our cohort we were unable to include dispensations for cholinesterase inhibitors as drug therapies for individuals younger than 65 years as they are only covered through private insurance and thus data are not available.
Additionally, we were not able to conduct an in-depth exploration of pathways to differential diagnoses including varied health visits and specific testing to determine the underlying pathology of the dementia symptoms. Second, administrative databases allow for documentation of health system use patterns at a population level but provide minimal information on the causal path. This poses challenges to understanding the interrelationship between individual, household and health system factors leading to the use of the varied healthcare services among people with dementia. There may have been, for example, confounding unmeasured variables such as family status and support, health behaviors, social isolation or performance on activities of daily living that impacted on health system use. Third, we were also unable to obtain information on perceived quality of care for people with dementia and their families to better understand, for example, the benefits of allied health or community-based services or the choices made to enter long-term care. Further mixed-methods investigations would provide additional quantitative detail of care and support transitions coupled with lived experience insights to understand the illness trajectory and impact on families and health systems. Finally, the data accessed did not include nurse practitioners as primary health providers. With an ever-increasing scope of practice, nurse practitioner-led clinics are relatively new in Ontario, with the first clinic only opening in 2007, 55 and this type of healthcare contact is not yet fully captured in the data accessed.
Conclusion
The impact of late-onset dementia on the global economy and healthcare is well documented, including ongoing calls for strategic health system planning. However, fewer studies have examined the healthcare needs and use of individuals living with young-onset dementia. Though the patterns of health system use among those living with late-onset and young-onset dementia may be comparable, as documented here, specialist health and community-based solutions to lessen system burden and improve the lives of those affected at a younger age may differ. Our study was a novel attempt to explore health system use among people living with young-onset dementia – recognizing that the picture would be a complex one. We observed higher rates of health system utilization and hazards of long-term care placement and mortality among community-dwelling persons with young-onset dementia compared with persons without dementia. However, further work is necessary to uncover the underlying reasons for varied patterns of health system utilization from pre-diagnosis to end-of-life care. This will enable planning for and the provision of timely, continuous and tailored high-quality care and support across a variety of settings.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/cjn.2026.10607.
Data availability statement
The dataset from this study is held securely in coded form at ICES. While data sharing agreements prohibit ICES from making the dataset publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at www.ices.on.ca/DAS. The full dataset creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Acknowledgments
This study was also supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation. Parts of this material are based on data and information compiled and/or provided by the Canadian Institute for Health Information (CIHI), MOH, and Ontario Health (OH). The analyses, conclusions, opinions, and statements expressed herein are those of the authors, and not necessarily those of funding or data sources; no endorsement is intended or should be inferred. Standardized rates were calculated using the 2011 intercensal and postcensal Canadian population estimates, adapted from Statistics Canada.
Author contributions
MPS, VW, DS and SB conceived the study. All authors contributed to the design. TL and JC conducted the data collection and analysis which was overseen by SB. MPS, VW, JC and TL wrote the manuscript. All authors provided critical appraisal and review and approved the final manuscript.
Funding statement
Funding for this work was received from The Hilary and Galen Weston Foundation.
Competing interests
MPS reports funding from the Canadian Institutes for Health Research and The Hilary and Galen Weston Foundation. VW reports funding from the Canadian Institutes for Health Research. DWS reports funding from the Canadian Institutes for Health Research and the Northern Ontario Academic Medical Association. TL and JOC report no disclosures. SEB reports funding from the Canadian Institutes for Health Research, Public Health Agency of Canada, the Alzheimer Society of Canada, Sunnybrook Research Institute and the Canadian Consortium on Neurodegeneration in Aging.



 Open access
Open access