


Introduction
Equitable access to health care is a fundamental principle of the Canadian healthcare system. 1 However, persistent inequity in healthcare delivery exists, particularly in Northern communities where remote geography is one contributing factor. Reference Nguyen, Subhan, Williams and Chan2
Weeneebayko Area Health Authority (WAHA) provides health services to approximately 12,000 predominantly Indigenous people, along the James Bay and Hudson Bay coastal regions, one of the most remote areas within Ontario, with none of the communities having road access. 3 Weeneebayko General Hospital (WGH) has access to CT and ultrasound imaging onsite, however there is no MR imaging available. Currently, patients requiring MRI are transported via daily charter flights bringing patients 841 km (522 miles) from WGH to Kingston Health Sciences Centre (KHSC) in Kingston, Ontario (Fig. 1).
Map of Ontario, Canada, showing the six coastal communities comprising Weeneebayko Area Health Authority, the island of Moose Factory (where Weeneebayko General Hospital is located) and distance (841 km) patients must be transported for MRI imaging in Kingston, Ontario.

Transportation of patients from a remote setting is complex and is associated with a substantial increase in risk. Reference Fanara, Manzon, Barbot, Desmettre and Capellier4,Reference Holodinsky, Williamson and Demchuk5 The ability to perform cerebral imaging locally would reduce such risks. An additional consideration is the financial implications of patient transport within the framework of limited healthcare resources.
Up until recently, the technology for portable MRI has not existed. Reference Sheth, Cahn and Salehi6 Health Canada has recently provided licensing for a portable, POC low field (0.064T) MRI that is capable of producing images for a number of neurological indications. Reference Sheth, Cahn and Salehi6 The portable MRI has been used in academic centers throughout the United States as of 2019 and in COVID intensive care units for cerebral imaging. Reference Sheth, Mazurek and Yuen7–Reference Kuoy, Glavis-Bloom and Hovis9 In 2021, portable MRI has also been successfully deployed to a low resource setting in Malawi. Reference Chetcuti, Chilingulo and Goyal10
The use of this technology in a remote setting offers the potential advantages of reduced transportation of patients, improved triaging, as well as the ability to perform frequent re-imaging, without radiation exposure. However, there are no data to date on the feasibility of using portable MRI in a remote setting, such as in Canada’s North. Although a systematic review has been conducted comparing mobile versus fixed MRI, Reference Mohammadshahi, Alipouri Sakha, Esfandiari, Shirvani and Akbari Sari11 a cost analysis from the perspective of a Canadian context in a remote setting has also not been previously performed.
In this study, we sought to a) evaluate the feasibility, and b) the cost analysis of deploying portable MRI in a remote setting in comparison to transporting patients to a larger center.
We define feasibility as:
-
1. The local capacity to perform imaging in a remote setting.
-
2. The ability to capture images of patients that are of sufficient quality to be interpreted by KHSC staff neuroradiologists.
-
3. The ability to transfer and report images of patients in a timeframe meeting or exceeding that of Department practice for urgent and emergent scans.
Methods
This preliminary analysis of a single center cohort study was performed at WGH. After receiving Investigational Testing Authorization – Class II by Health Canada on September 14, 2021, an FDA approved portable MRI scanner [Swoop Portable MR Imaging System, RC8 software; ultra-low field (0.064 T), Hyperfine] was delivered via rail and then by barge to the island of Moose Factory, Ontario. The portable MRI was kept in the CT suite which allowed for patients to receive an MRI as part of this study directly after receiving the standard of care head CT.
Research Ethics Board approval was received (TRAQ #: 6034296), following WAHA Ethics Committee approval. The study was conducted in alignment with the OCAP Principles for governance of Indigenous Health Data. Reference Schnarch12
All portable MRI scans were performed by physicians, nurses, and x-ray technologists who were trained on portable MRI operation. The manufacturer’s standard protocol, consisting of axial T1-weighted fast spin echo, T2-weighted fast spin echo, T2-weighted fluid-attenuated inversion recovery (FLAIR) and diffusion-weighted imaging with apparent diffusion coefficient sequences was used for all examinations. No intravenous contrast or oral sedation was used. Informed consent for study inclusion was obtained in either English or Cree.
Inclusion Criteria
Patients were eligible if they were 18 years of age or older and presenting to WGH emergency department, inpatient services, or outpatient family medicine clinic with any indication for neuroimaging, if their treating team had ordered non-contrast head imaging (CT or MRI), and if neuroimaging was indicated necessary by the treating physician.
Exclusion Criteria
These include patients under 18 years of age, body size exceeding the portable MRI scanners 30 cm vertical opening or the presence of any contraindication for conventional MR imaging.
Scanning Protocol and Image Data Transfer
All clinical indications for portable MRI were documented. Following each scan, an acceptability checklist was administered to the WGH staff performing the scan to assess local capacity to perform imaging and document any adverse events.
A secure PACS link was established between WAHA and KHSC for transfer and storage of DICOM images from the portable MRI to KHSC PACS. All imaging was reported by board-certified Neuroradiologists at KHSC, providing 24/7 coverage. Prior to study start, all Neuroradiologists received training on portable MRI through online seminars provided by the vendor. All pathologies observed on imaging were documented in standardized reports, stored on KHSC servers. Report turnaround time was determined by the time from image acquisition to radiology report generation.
As per ethics requirement, the device could not be used to inform clinical decision-making. Therefore, the portable MRI taken as part of this research study did not interfere with the patient disposition pathway (discharging home, remaining at WGH as an inpatient, or transferring for further imaging).
Scan results were not disclosed to the referring physician, unless there was a significant pathology (stroke, large bleed, hydrocephalus, or herniation), that which required immediate surgical or medical intervention and for which confirmation with conventional imaging would be sought.
Technology Adoption
To determine the potential impact of portable MRI implementation on referral pattern for MRI studies, the volume, and indications for MRI head examinations from the year prior to the study period were retrospectively analyzed.
Cost Analysis
A cost analysis Reference Drummond, Sculpher, Claxton and Stoddart13 was conducted from the healthcare system’s perspective in 2022 Canadian dollars (CAN) (http://www.statcan.gc.ca). It only included costs borne out of the healthcare system and excluded any patient related costs, such as out-of-pocket costs (parking, local travel, childcare), or lost income. The Canadian healthcare system is universal and decentralized, funded primarily publicly through taxation. Provinces and territories have different health plans that fund charter flights for diagnostic imaging, as required in the case of necessary imaging.
The cost analysis conducted here is only applicable to locations that already have an existing radiology infrastructure (e.g., ultrasound, CT) connected with fiberoptic communication, as well as existing nursing stations, ER and inpatient beds, resources and physicians. Resource utilization, procedure related costs and patient and nurse direct travel costs were examined. A budget impact analysis Reference Sullivan, Mauskopf and Augustovski14 was conducted over 5 years between 2022 and 2026, using Microsoft Excel, examining difference in costs of gradually adopting portable MRI in a remote community in Canada compared with fixed MRI only as standard of care (a valid assumption). For the cost data collection, feasibility study staff completed cost forms to record time and resources allocated to the fixed and portable MRI. The forms contained information on a) transportation, b) personnel time to the nearest quarter of an hour, c) personnel compensation, and d) round trip patient and staff travel. One-way sensitivity analysis was conducted. Any costs related to evaluation research were excluded.
Results
Feasibility
Portable MRI was successfully delivered and implemented at WAHA (Fig. 2). From unboxing to testing, the total time for device setup was 3 hours. 14 staff members received training on operation (8 physicians, 3 nurses, and 3 x-ray technologists). Training sessions were on average 45 minutes and included demonstration for moving the patient into the scanner, performing the scan, troubleshooting, an introduction to low field versus conventional MRI, study overview and study document review (informed consent form, indications/contraindications for imaging). Trainees were provided practice time to become familiar with the scanner iPad interface.
Portable MRI at Weeneebayko General Hospital. The scanner is situated in the same room as the hospital’s CT scanner.

Investigational Testing Authorization – Class II approval was received from Health Canada for up to 50 patients. All patients who received a portable MRI from November 14, 2021, to September 7, 2022, approximately a 10-month period, were included in the study. No patients were excluded. The preliminary results are presented for the first 25 patients who underwent portable MRI examination. Specific demographic characteristics of these patients are not included in alignment with the OCAP principles, that of ownership, control, access and possession governing the use of indigenous health data. Reference Schnarch12 No patients were excluded from study analysis.
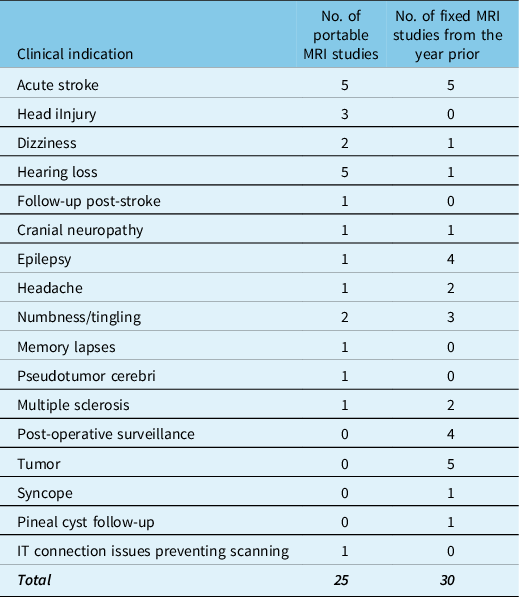
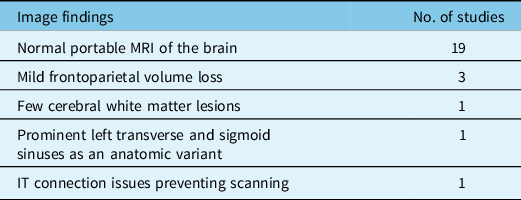
The most common clinical indication for imaging was acute stroke (n = 5) (Table 1). The studies were reported by 4 staff neuroradiologists at KHSC (O.I. = 10, I.S. = 8, D.T. = 3, J.O.J = 2). No acute infarction, hydrocephalus, herniation, or clinically significant pathologies were identified in any of the studies (Table 2). 19 of the studies were reported as normal. The typical quality of the portable MRI images acquired is shown in Figure 3. Comments on non-optimal study quality were reported for 5 of the studies. Quality comments included motion artifact (n = 1), zipper artifact (n = 3), and patient’s head not centered in coil (n = 1). None of the portable MRI studies were deemed non-diagnostic. A consistent finding on portable MRI that interpreters must be aware of is the high signal intensity in dural venous sinuses on FLAIR imaging (Fig. 4).
Clinical indications for ordering portable MRI during the study period (November 14, 2021–September 7, 2022) compared to fixed MRI the year prior (November 14, 2020–September 7, 2021)

Portable MRI image findings

Portable MRI of a patient presenting with two weeks of sudden intermittent dizziness with left ear tinnitus and left eye decreased vision. Select T2 images (a-d) through the brainstem show normal appearance of the midbrain and pons. There is no mass in the cerebellopontine angle cisterns. Images from portable MRI are of sufficient quality for diagnostic interpretation. This case also depicts a zipper artifact on image b (arrows). The zipper artifact is commonly observed in portable MRI examinations and is defined as a linear band of abnormal alternating black and white signal. This is an artifact where spurious bands of electronic noise extend across the image. This is likely a shielding issue with portable MRI, likely arising from spurious radio frequency signals contaminating received imaging data. It is displayed in the phase encoding direction, in this case in the antero-posterior direction.

Portable MRI of a patient presenting with left-sided hearing loss, dizziness, and nausea. Axial FLAIR (a) and axial T1 (b) demonstrate mild frontal and parietal volume loss. Note the bright signal in the posterior aspect of the superior sagittal sinus on FLAIR imaging (arrow) with no corresponding bright signal abnormality on T1. This is a normal finding on portable MRI and does not equate to venous sinus thrombosis.

Based on the indication for imaging and the results of the portable MRI, if the portable MRI was available for routine clinical use, 14 patients (56%) would not require transfer to a center with MRI imaging due to the availability of portable MRI onsite. Representative cases of patients who would and would not require transfer if portable MRI were available are shown in Figure 5 and Figure 6 respectively. For example, from the diffusion-weighted sequence in Figure 5c. acute infarction can be confidently ruled out as the cause of the patient’s presentation of left arm paresthesia. Contrastingly, for a patient presenting with query multiple sclerosis, the portable MRI images in Figure 6 are of sufficient quality to confidently exclude medium to large-sized plaques, however the resolution is not sufficient for confident identification of small plaques. Therefore, further imaging on fixed MRI would be required for complete evaluation in this situation.
Portable MRI of a patient presenting with headache and left arm paresthesia. The patient’s CT taken 24 hours prior was negative, and they were started on dual antiplatelet therapy. Axial T2 (a), Axial T1 (b), Axial DWI (b = 900 s/mm2) (c), and Axial FLAIR (d) at the level of the lateral ventricles show normal appearance of the cerebrum, apart from mild volume loss affecting the frontal and parietal lobes. The diffusion-weighted sequence (c) shows no acute infarction. It is postulated that this patient would not require transfer to a facility with MR imaging based on the results from the portable MRI.

Portable MRI of a patient presenting with left and right upper extremity numbness. The portable MRI study is normal, with no signs of large demyelinating plaques. Sagittal FLAIR (a) and (b) demonstrate normal appearance of the corpus callosum (white arrows) and provide an example of the multiplanar capability of portable MRI. Axial T2 (c), axial T1 (d), axial FLAIR (e), and axial DWI (b = 900 s/mm2) (f) demonstrate normal cerebral white matter at the level of the lateral ventricles and corona radiata. The image quality is sufficient to confidently exclude medium to large-sized plaques; however, the resolution is not sufficient for confident identification of small plaques. As such, this patient would require transfer for neuroimaging on fixed MRI for complete evaluation.

The median time from scan completion to the time reported by a neuroradiologist for non-urgent indications was 8.1 hours (IQR, 1.5–22.2 hours). During the 6-month study period, there were 2 instances of connection issues between the portable MRI scanner and Weeneebayko General Hospitals internet network which resulted in a delay in reporting time. Both cases were resolved within 24 hours and related to instability of the Wi-Fi connection. No image transfer issues occurred after switching to an ethernet connection. For emergent cases such as suspected acute stroke, there was telephone communication between the referring physician and reporting radiologist to allow for immediate communication of results, prior to a report being generated.
Technology Adoption
There was not a substantial change in MRI referral volumes or clinical indications with the implementation of portable MRI (Table 1). For the same 10-month period a year prior to portable MRI implementation (November 14, 2020–September 7, 2021) there were 31 MRI head studies performed. Of the 30 studies, 12 were done in Kingston, Ontario and 18 in Timmins, Ontario.
Costs
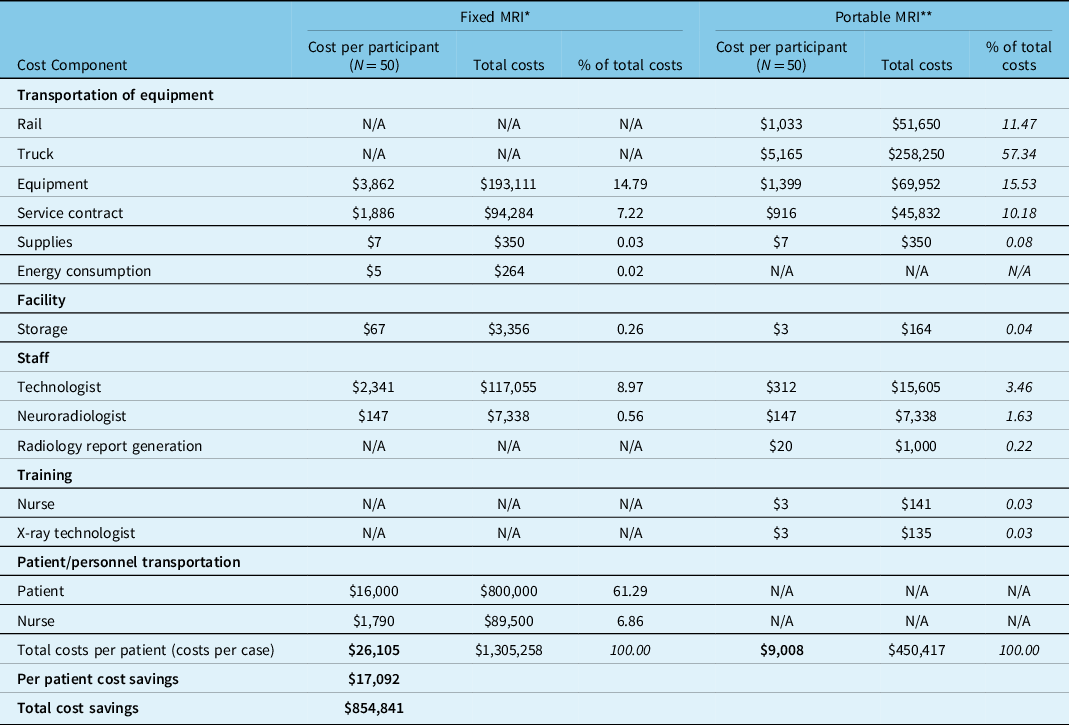
Fixed MRI costs were compared to portable MRI at WGH for 50 patients (expected patient capacity) over the first year. Fixed MRI was purchased from Germany (Siemens) in 2018 (CAN$2.2-2.5 million, including transportation and installation), comparable to the literature (US 2018 dollars $992,400–$1,984,800). Reference Mohammadshahi, Alipouri Sakha, Esfandiari, Shirvani and Akbari Sari11 Portable MRI cost was CAN$682,000 in 2021 from the US (Hyperfine), including 3 hours set up. Equipment costs were adjusted using purchasing power parity and depreciation (1.5% rate; 15 years lifetime for fixed MRI and 11 years for portable MRI). 15 Service contracts for both fixed and portable MRI were calculated as yearly estimates (including maintenance): $110,000 for years 2–7 for the fixed MRI and $55,000 for years 2–6 for portable MRI (first contract year included in purchase price).
Portable MRI transportation fees by rail were $1,033, and $5,165 by truck, and training costs of 3 nurses were $141 and $135 for 3 X-ray technologists (45 minutes on average, using Ontario wage rates 16,17 ). The cost of storage for the fixed MRI was $3,356 (512 square feet room). The cost of storage (25 square feet closet) for the portable MRI was calculated at $164 for safekeeping. Energy consumption for the fixed MRI was calculated based on the literature Reference Heye, Knoerl and Wehrle18: 19.9 kWh per exam, mean consumption per year: 82,174 kWh per MRI exam, 134,037 kWh total consumption), converted into mean energy costs: CAN$5.3 ± 1.4 (2022 dollars). For portable MRI, energy consumption and radiology report generation (plain films and fiber optic communication) were subsumed in the hospital’s existing infrastructure operation costs, except for one-time cost of $1000 for connection onto existing hospital networks. For the fixed MRI, patient and nurse related travel fees were on average $16,000 and $1,790, respectively, including the cost of each charter return flight from Weeneebayko to clinics in Kingston or Timmins (for routine and emergent MRI).
Total costs of fixed MRI were approximately triple compared to portable MRI (Table 3). Cost per patient (cost per case) for fixed versus portable MRI was $26,105 and $9,008, respectively. Overall, 1-year cost savings from adoption of the portable MRI, compared with fixed MRI, based on projected 50 patients were $854,841. Travel costs averted (savings from patient and nurse transportation from WGH) were $889,500 based on 50 patients over 1 year. These averted costs constituted 68.15% of total costs incurred by fixed MRI. The highest percentage costs attributable to portable MRI were equipment transportation (WGH 841 km from KHSC) (68.81%), followed by equipment costs (15.53%).
Fixed and portable MRI costs per participant and total costs per year for year 1

* The cost analysis conducted here is only applicable to locations that already have an existing radiology infrastructure (e.g., ultrasound, CT) connected with fiberoptic communication, and existing nursing stations, ER and inpatient beds, resources, and physicians. Therefore, installation and transportation costs and radiology report generation, as well as nurse and X-ray technologist training costs pertaining to fixed MRI, were not included in this cost calculation. Likewise, energy costs are already subsumed in regular hospital operations for portable MRI.
** Local travel costs for patients and nurses for portable MRI were not included in this cost analysis, since the cost calculations take into consideration only the healthcare system’s perspective.
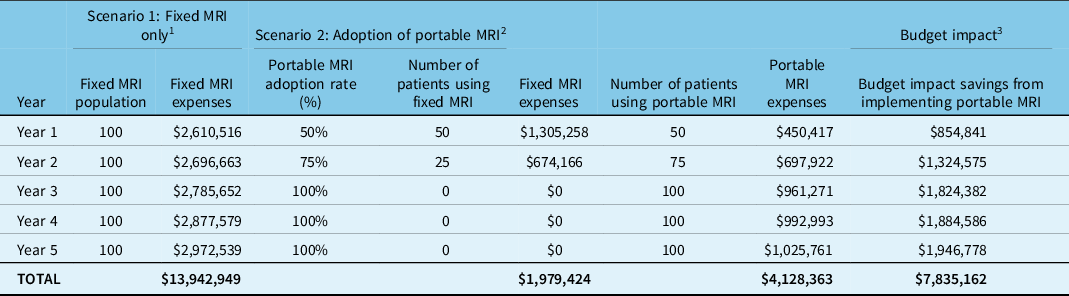
For the budget impact model over 5 years, in one scenario, it was assumed that 100 patients would be eligible for the fixed MRI only for 5 years, compared with a second scenario in which there would be a gradual adoption of portable MRI, starting with 50 patients in the first year, followed by 75 patients in the 2nd year and 100 patients in years 3 to 5. The model of future portable MRI examinations was based on late adopters. As comfort with using the new technology increased locally, we anticipate growth in the use of portable MRI. Savings were calculated: fixed MRI costs (scenario 1) minus cost of gradually implementing portable MRI (scenario 2). Total savings amounted to $7,835,162 (Table 4). An inflation rate of 3.3% was used (estimated from consumer price index increase between 2020 and 2021) in the base case analysis. For one-way sensitivity analysis, inflation rate for each of the years was varied (7.2% 4.6%, 2.3%, 2.0%, and 2.0%, respectively for years 1–5) 19 , resulting in 5-year savings of $7,731,882. Further, nurse and x-ray technologist training for the portable MRI was excluded in sensitivity analysis, in the scenario that it becomes part of training new hospital staff, resulting in 5-year savings of $7,837,688. An additional sensitivity analysis was conducted using low uptake rates of portable MRI (25% uptake in the first year, followed by 30%, 35%, 40%, and 45% in years 2–5, respectively), and showed cost savings of $3,225,669.
Budget impact analysis over a 5-year period

1 Scenario 1: costs associated with 100 patients with fixed MRI only.
2 Scenario 2: costs associated with gradual portable MRI adoption. In year 1, 50% of patients use portable MRI (50% fixed MRI); in year 2, 75% use portable MRI (25% fixed MRI). Complete adoption was assumed, years 3 to 5.
3 Budget impact savings:100% fixed MRI (scenario 1) minus gradual implementation of portable MRI (scenario 2). Over 5 years, savings: $13,942,949 – (4,128,363 + $1,979,424) = $7,835,162.
Discussion
Feasibility
Portable MRI can be successfully implemented in remote communities as it requires limited resources to meet the local capacity for imaging under the developed workflows, can be housed and operated in a low-cost environment, and has the ability to transfer images to radiologists who typically may be offsite.
The setup of the portable MRI at WGH was efficient, only taking 3 hours and not requiring changes to infrastructure, power supply, or magnetic safety considerations. A benefit of portable MRI observed was that it did not require extensive training to operate. 14 staff members at WGH received training, only taking an average of 45 minutes. Given the high rate of staff turnover, especially in Northern Canadian healthcare settings, the rapid training of new staff is important to the sustainability of a portable MRI program. As part of this study, we developed training documents and videos on the use of portable MRI that can be included in the standard onboarding for new hospital staff.
The indications for imaging in this preliminary analysis are limited due to study size. Acute stroke was the most common indication for imaging (n = 5). This is also perhaps the most clinically relevant indication, as traditional MRI DWI sequences offer a higher sensitivity in detecting acute blood compared to CT. Reference Lansberg, Albers, Beaulieu and Marks20 For example, Kuoy et al. found 13% of portable MRI examinations demonstrated acute infarctions that were not apparent on comparison CT scans. Reference Kuoy, Glavis-Bloom and Hovis9 Access to portable MRI may also be of benefit for other less urgent neurological indications, where patients may otherwise face substantial wait times for traditional MRI.
Image capture was of sufficient quality to be reported by staff Neuroradiologists, however due to the limitations of portable MRI, in some cases full diagnostic imaging may still be required. Based on clinical presentation and portable MRI findings, it was estimated that 11 of 25 patients would require transfer to a center with fixed MRI for further imaging workup. Comments on non-optimal study quality were reported for 5 of 25 studies. Motion artifact was able to be limited by stabilizing the patients’ head inside the head coil with inflatable pads and placing the patient in a 5–10 degree Trendelenburg position to keep the head centered in the coil. The median turnaround time from study completion to reported by a neuroradiologist was 8.1 hours (IQR, 1.5–22.2 hours). Ontario Ministry of Health’s standard of practice for report turn about time for priority one (urgent) scans is 24 hours, 48 hours for priority two (emergent) and several days for elective scans. Ensuring adequate phone communication between the referring physician and reporting neuroradiologist was particularly important early on during the study while workflow was being streamlined and for urgent indications such as acute stroke.
Technology Adoption
The local availability of a new imaging technology itself has the potential to change the threshold to order an imaging test, however we did not observe an increase in the number of MRI head studies performed with the implementation of portable MRI (25 portable MRI studies compared to 30 fixed MRI studies the same timeframe a year prior). It is thought this was largely due to being early adaptors and lack of familiarity with the technology. In our experience, training sessions for hospital staff and community information sessions were helpful in this regard.
One of the greatest challenges encountered implementing portable MRI in a remote setting has been staff availability and time required for scanner operation. The total scanning time for each patient was approximately 40 minutes. In situations where the staff physician was the person preforming the scan, this is 40 minutes where the physician must leave the ER or clinic for scanner operation. As a new technology, portable MRI operation is not covered under the scope of practice for Canadian X-ray technologists or nurses, which could present hesitancy of adoption. Further, the financial remuneration for such services has yet to be implemented. In remote settings where staff resources are already limited, staffing factors represent a barrier to the use of portable MRI. It is recommended that where possible, a designated staff member other than physicians or nurses is designated the scanning lead and financially compensated for their time.
Economic Discussion
The cost analysis showed savings of $7,835,162 over 5 years for the implementation of the portable MRI. The literature on costs for portable MRI is scant, with one systematic literature review Reference Mohammadshahi, Alipouri Sakha, Esfandiari, Shirvani and Akbari Sari11 deeming mobile and fixed CT and MRI cost-effective compared with fixed CT and MRI. Mobile MRI or CT were established in trailers at referring centers (up to 3) within 75 km, compared with our 841 km distance. Estimated annual total costs of mobile MRI were 2018 US$1,890,620, higher than our annual total costs at 2022 CAN$450,417. These appear to be attributable to the high costs of wagon, trailer and energy costs (2015 US$302,288) and equipment costs.
Study Limitations
As this is an initial feasibility study, the analysis is limited due to a small sample size. Health Canada approval was obtained for scanning 50 patients, of which the first 25 are presented here. Given that the study was initiated under Health Canada Investigational Testing Authorization and prior to Health Canada approval of portable MRI for clinical use, the portable MR images obtained as part of this study were not used in the clinical decision-making pathway. Therefore, we can only theorize, based on the imaging results obtained, if they were to be used in clinical decision-making which patients would require transfer to another center for fixed MRI vs. for which patient’s portable MRI alone would be of sufficient diagnostic use.
While this study focused on the feasibility of implementing portable MRI in a remote setting, a limitation is that in terms of clinical utility, there was no gold-standard imaging for comparison. Therefore, it is possible that significant diagnoses may have been missed due to limitations in the quality of portable MRI compared to gold-standard imaging.
Conclusion
This study may serve as a model to help democratize MRI access in remote areas where conventional MRI is unavailable. Portable MRI implementation is feasible; however, the clinical utility remains an active area of study. Future studies should be conducted to determine the influence of portable MRI on clinical management in remote settings. Currently, this technology cannot fully replace conventional MRI neuroimaging but may be useful in triaging patients and provide timely care. Projected cost savings are substantial, largely due to patient transportation costs averted. The preliminary study findings can guide the implementation of portable MRI at other Canadian and international sites, especially in remote communities.
Acknowledgements
The authors thank Hannah McGregor at Queen’s University for assisting with editing the economics portions of the manuscript.
Statement of authorship
The authors confirm their contribution to the paper as follows: study conception and design: OI, CD, EI, JGB; acquisition, analysis, and/or interpretation of data: OI, DT, JOJ, IS, BYMK, APJ, CD; draft manuscript: preparation: CD, OI, APJ, EBH; revising manuscript: JGB, OI, APJ. All authors reviewed the results and approved the final version of the manuscript.
Funding
This work was supported by the William H. Boyd Memorial Fund for Neurological Research, Faculty of Health Sciences, Queen’s University and the Academic Fund, Department of Diagnostic Radiology, Faculty of Health Sciences, Queen’s University. Hyperfine Inc. has supplied the portable MRI, training, and associated equipment. Author JGB receives honoraria from the Canadian Critical Care Forum to cover accommodation and travel costs for lectures at their annual meeting.
Competing interests
None.







 Open access
Open access