



Background
Breastfeeding is an evidence-based and cost-effective public health strategy with numerous short- and long-term benefits for the nutrition, health and overall wellbeing of mothers, children and families(Reference Victora, Bahl, Barros, França, Horton and Krasevec1). Breastfeeding is associated with reduced risk of breast and ovarian cancers, type 2 diabetes, high blood pressure(Reference Chowdhury, Sinha, Sankar, Taneja, Bhandari and Rollins2,3) , post-partum weight retention and obesity in mothers(Reference Baker, Gamborg, Heitmann, Lissner, Sørensen and Rasmussen4,Reference Østbye, Krause, Swamy and Lovelady5) . It is also documented in the literature as an evidence-based strategy for reducing the risk of infections, asthma, sudden infant death syndrome, diabetes and obesity in infants and children(Reference Victora, Bahl, Barros, França, Horton and Krasevec1,3,Reference Horta, Loret De Mola and Victora6) . In addition, breastfeeding is associated with improved cognitive development and higher learning and education attainment among children(Reference Victora, Bahl, Barros, França, Horton and Krasevec1,Reference Anderson, Johnstone and Remley7) . Overall, breastfeeding plays a critical role in providing children with the nutrients and immunological advantage needed for optimal growth, development and disease prevention(Reference Victora, Bahl, Barros, França, Horton and Krasevec1,Reference Rollins and Doherty8) .
The World Health Organization and American Academy of Pediatrics both recommend early initiation of breastfeeding within the first hour after birth, exclusive breastfeeding (EBF) for the first 6 months of life, and continued breastfeeding for 24 months or more, as mutually desired by mother and child(9,Reference Meek and Noble10) . Despite increasing efforts to promote and support the practice in the United States, the progress in EBF rates has been slow. Data from the Centers for Disease Control and Prevention indicate that EBF rates in the United States increased by 6 percentage points (22·3% to 27·9%) between 2016 and 2025(11,12) , and the United States continues to have some of the lowest rates of EBF and sustained breastfeeding rates globally(13–Reference Gupta and Suri15). Also, racial and ethnic disparities in breastfeeding outcomes persist(Reference Li, Perrine, Anstey, Chen, Macgowan and Elam-Evans16–18).
Foreign-born immigrants and refugees are a group that are reported to have high breastfeeding initiation but low EBF rates(Reference Celi, Rich-Edwards, Richardson, Kleinman and Gillman19–Reference Rosenthal, Oliveira, Madubuko, Tanuos, Schwab and Monteiro21), even though breastfeeding has been identified as an important line of defence for children of immigrants who are at greater risk for food insecurity(Reference Neault, Frank, Merewood, Philipp, Levenson and Cook22). There are also mixed findings on the duration of breastfeeding for various immigrant groups, with reports indicating shorter duration of any and exclusive breastfeeding with increasing acculturation(Reference Hamner, Beauregard, Li, Nelson and Perrine23–Reference Harley, Stamm and Eskenazi26). In fact, one study reported a 3% decrease in the odds of (any) breastfeeding at 6 months with each additional year of living in the United States(Reference Gibson-Davis and Brooks-Gunn27). Challenges related to socioeconomic status, migration status, lack of social support and greater acculturation were also associated with decreased rates of EBF among immigrants(Reference Celi, Rich-Edwards, Richardson, Kleinman and Gillman19,Reference Ahluwalia, D’Angelo, Morrow and McDonald24,Reference Gorman, Madlensky, Jackson, Ganiats and Boies25,Reference Izumi, Trigg and Stephens28,Reference Anderson, Damio, Himmelgreen, Peng, Segura-Pérez and Pérez-Escamilla29) . For example, previous studies have reported that immigrant women were more likely to exclusively breastfeed in their home country than the United States(Reference Victora, Bahl, Barros, França, Horton and Krasevec1,Reference Vaughn, Ireton, Geraghty, Diers, Niño and Falciglia30–Reference Pineros-Leano, Pérez-Flores, Damian, Piñeros-Leaño, Yao and Rodrigues32) due to beliefs that formula feeding is more ‘American’ or that formula is beneficial or at least a harmless alternative to breastfeeding, especially since government agencies such as the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) supply it for free and teach them how to prepare it(Reference Jones, Reller, Knowles, Lin and Lohr33–Reference Fisher, Patel, Wouk, Neupane, Alkhalifah and Bartholmae36). Moreover, other research has indicated that refugee mothers, who often breastfeed amid the economic and health disadvantages common in emergency settings, tend to show a decrease in breastfeeding over time following their immigration to Western countries(Reference Bader, Ward, Fouts and Jaekel34).
Recent migration reports indicate that immigrants are a growing segment of the US population(37,38) , and that more than half of all immigrants in the United States as of 2022 were female(37,39) , mostly of childbearing age(Reference Dennis, Shiri, Brown, Santos, Schmied and Falah-Hassani20). Therefore, it is important to consider how to maintain the breastfeeding advantage that immigrant and refugee women have when they move to the United States and create a culture of support that allows them to sustain this positive health behaviour as they become increasingly acculturated(Reference Celi, Rich-Edwards, Richardson, Kleinman and Gillman19,Reference Rosenthal, Oliveira, Madubuko, Tanuos, Schwab and Monteiro21,Reference Harley, Stamm and Eskenazi26) . Understanding how immigrants could be better supported to exclusively breastfeed could be a key contributor to increasing the rates and promoting the culture of exclusive breastfeeding in the United States.
Although there are numerous ongoing national- and state-level breastfeeding support and education efforts – such as WIC, the Baby-Friendly Hospital Initiative and La Leche League International, and state- and community-level breastfeeding coalitions and peer support groups – in the United States(40,41) , less is known about the effectiveness of these strategies for immigrant mothers. Previous studies have highlighted the need for breastfeeding promotion programmes and efforts that target immigrant mothers to understand and consider the unique needs and cultures of immigrant families(Reference Celi, Rich-Edwards, Richardson, Kleinman and Gillman19,Reference Dennis, Shiri, Brown, Santos, Schmied and Falah-Hassani20,Reference Neault, Frank, Merewood, Philipp, Levenson and Cook22,Reference Hamner, Beauregard, Li, Nelson and Perrine23) . While some studies have looked at breastfeeding support interventions among minority populations(Reference Chapman and Pérez-Escamilla42), there were no reviews that looked at interventions specifically targeted at immigrant groups in the United States. We therefore planned to conduct a scoping review of the existing peer-reviewed literature to explore what is currently known about strategies to support breastfeeding of foreign-born women (including immigrants and refugees) in the United States. Specifically, the objectives are to: (i) identify the types of support that have been provided, (ii) document the strategies and methods used in delivering support, and (iii) understand which groups of immigrants have been studied.
Methods
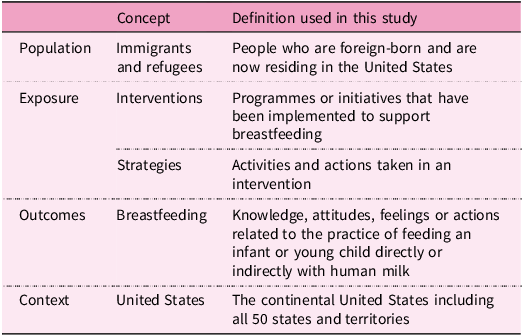
The review process was consistent with the Arksey & O’Malley framework(Reference Arksey and O’Malley43), and the PRISMA guidelines for scoping reviews were used in documenting our process and reporting the findings(Reference Tricco, Lillie, Zarin, O’Brien, Colquhoun and Levac44). The search terms were developed using the four key concepts in the research question stated above. Table 1 outlines the concepts included in the search terms and the definition used for each category.
Key concepts and definitions

Search strategy
PubMed, Scopus, Web of Science, Embase, ProQuest and all EBSCO Host databases were searched using a comprehensive search strategy that was developed with assistance from a research librarian (S.P). The search query incorporated synonyms of the population (immigrants and refugees), the outcome of interest (breastfeeding) and database-specific field tags and MeSH terms. This decision was made to ensure that the initial search was broad enough to capture as much data as possible, but also specific enough to eliminate articles that are completely unrelated to the research question. The exposure terms were used later in the screening process (see details in ‘Study screening, selection and data extraction’ section). The search strategy included all peer-reviewed publications prior to 18 January 2025. The search query included:
-
(Immigra* OR Foreign-born OR refugee*) AND (Breastfeed* OR Breast feed* OR breastmilk OR ‘human milk’ OR lactation OR lactating OR ‘Breast Feeding’[Mesh])
-
Field Tags: Title/Abstract
The search results were limited to peer-reviewed texts (original research and reviews) that were in English and US based, and the final results were exported from each database and uploaded into Covidence(45) for the study screening and selection process. The date range was kept open because this study is exploratory, and we aimed to see what has been documented in the literature regarding breastfeeding interventions for immigrant and refugee mothers in the United States.
Study screening, selection and data extraction
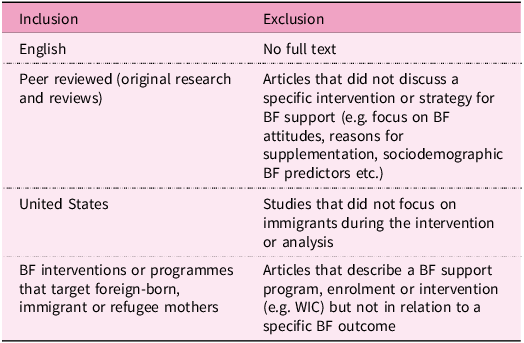
Once the search results were imported into Covidence, all duplicate articles were removed. The articles then underwent a title and abstract screening process by the first author (A.G.), where only articles that were US based, focused on foreign-born women or mothers, and focused on breastfeeding were included for full-text reviews. Next, the full-text articles of the included abstracts were sourced, uploaded and reviewed in Covidence by the first author (A.G.). All articles that met the exclusion criteria were removed, leaving only articles that were consistent with the full eligibility criteria outlined in Table 2. Articles that were unclear were discussed by A.G. and M.Y. until a decision was reached about their inclusion.
Inclusion and exclusion criteria for the scoping review
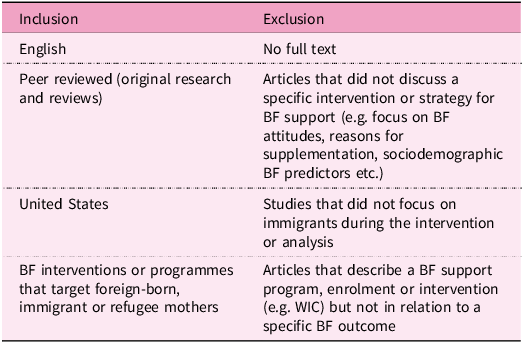
BF, breastfeeding; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
All papers that described, implemented or evaluated specific breastfeeding support interventions or strategies among a foreign-born population were included, regardless of their impact or study design. We excluded articles that recruited mixed populations, including immigrants, but did not focus on immigration status in their design or analysis. Studies that targeted minority populations, stratified their analysis by foreign-birth, reported data on foreign-born participants and made it a focal point of their study were included even if native-born women also participated. Each article was reviewed in detail, and relevant data were extracted by the first author using a pre-designed data extraction sheet (Supplementary Table S1). Using the extracted information, data mapping and percentage calculations were done systematically in Excel and key findings about the types of breastfeeding support that have been implemented, strategies utilised, key BF outcomes and the immigrant groups that have been studied are summarised in the results. The main breastfeeding behaviours that were targeted and persisting breastfeeding support gaps are summarised in subsequent sections.
Summary of strategies implemented to improve breastfeeding among foreign-born mothers

+The articles in this table are organised by the timeframe/duration of the intervention and the year of publication.
PP, postpartum; PCs, peer counsellors; WIC, Special Supplemental Nutrition Program for Women, Infants and Children; BF, Breastfeeding; LLLI, La Leche League International; FHCHC, Fair Haven Community Health Center; HHC, Hispanic Heritage Council.
* Interventions that reported meeting at least one but not all their targeted BF outcomes.
** Articles that discussed a strategy in relation to specific BF outcomes, but did not report the findings; interventions may be described in the context of a commentary, community based participatory research study or literature review.
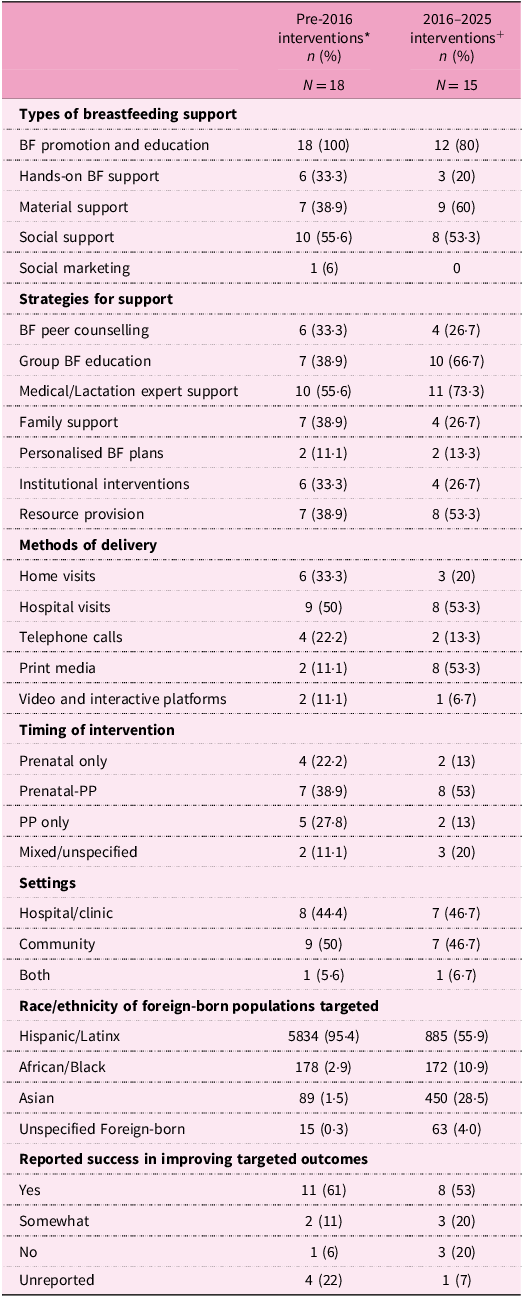
Furthermore, the publications were split into two time periods – articles published before 2016 and articles published within the last decade (2016–2025) – to observe how the types of BF support provided, strategies employed in interventions, timing/methods of delivery and settings varied across the time periods. Findings from this time-based analysis are presented in the results. The charted data were summarised as counts and percentages where applicable.
Differences in breastfeeding interventions over time
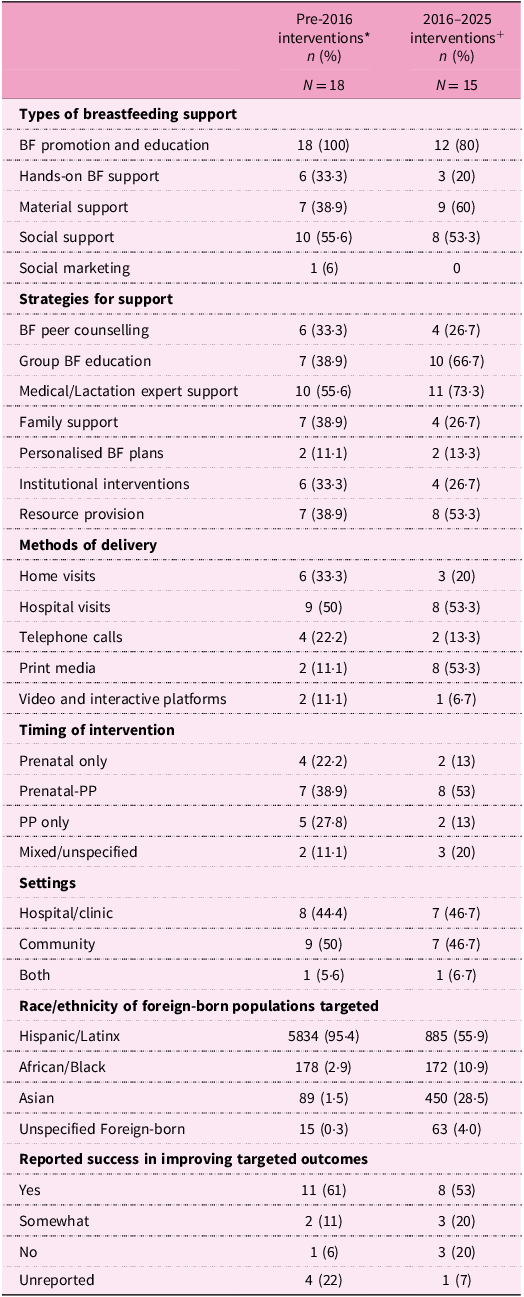
BF, breastfeeding; PP, postpartum.
* There were sixteen articles (eighteen interventions) published before 2016(Reference Faraz46,Reference Hopkinson and Konefal Gallagher47,Reference Noble, Rivera-Todaro, Hand and Noble50–Reference Watkins, Larson, Harlan and Young52,Reference Tuttle and Dewey55,Reference Moreland, Lloyd, Braun and Heins58–Reference de Bocanegra62,Reference Langellier, Chaparro, Wang, Koleilat and Whaley65,Reference Bonuck, Trombley, Freeman and McKee67,Reference Gill, Reifsnider and Lucke69–Reference Thompson, Joshi, Hernandez, Bair-Merritt, Arora and Luna71) .
+ Fifteen articles/interventions were published between 2016 and 2025(Reference Bader, Ward, Fouts and Jaekel34,Reference Fisher, Patel, Wouk, Neupane, Alkhalifah and Bartholmae36,Reference Linares, Cartagena and Rayens48,Reference Mosley, Pratt, Besera, Clarke, Miller and Noland49,Reference Lutenbacher, Elkins, Dietrich and Riggs53,Reference Lutenbacher, Elkins and Dietrich54,Reference Little, Motohara, Plegue, Medaugh, Sen and Ruffin56,Reference Madeira, Rangen and Avery57,Reference Gross, Mendelsohn, Gross, Scheinmann and Messito63,Reference Lawal, Owen, Brown and Effland64,Reference Linares, Wambach, Rayens, Wiggins, Coleman and Dignan66,Reference Cook, Kimball, Zittleman and Huntington68,Reference Van Zandt, Kim and Erickson72–Reference Duh-Leong, Au, Chang, Feldman, Pierce and Mendelsohn74) .
Results
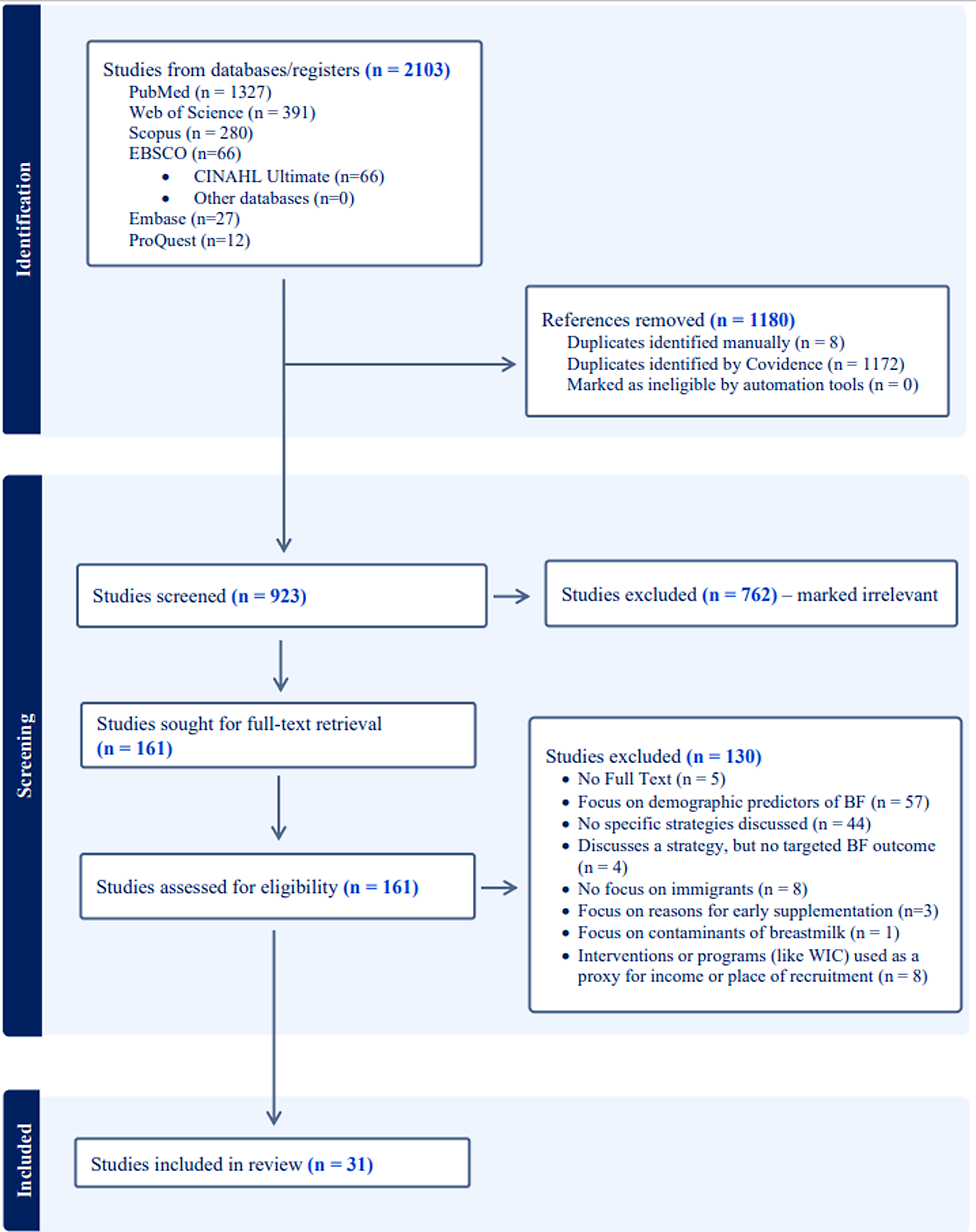
The database searches produced 2103 papers (Fig. 1). Once imported into Covidence, 1172 duplicates were removed. Preliminary title and abstract screening were then conducted, which resulted in the exclusion of 762 irrelevant papers and manual removal of 8 duplicates (Fig. 1). For example, studies conducted in non-humans (mice, pigs, birds, cows), outside of the United States, or focused on topics like breast cancer or biological components of human milk or topics unrelated to breastfeeding were removed. After this initial screening, 161 articles were imported for full-text reviews and assessed for full eligibility. Of these, 130 articles were excluded, leaving a total of 31 articles that were included for final review, data extraction and analysis (Fig. 1). All the included papers described at least one intervention or programme that supports or promotes breastfeeding in relation to foreign-born populations in the United States.
PRISMA flow diagram for the scoping review process.

Overview of included studies
The papers included in this review were published between 1988 and 2024 (n = 31), with 48% published within the past decade (n = 15). Strategies for BF support among immigrants have been implemented across all the major regions of the United States, including the northeast (26%, n = 8), the west coast (23%, n = 7), Midwest (10%, n = 3), southeast (26%, n = 8) and southwest (10%, n = 3). Two articles were literature reviews that discussed a range of strategies employed throughout the United States.
A little more than half the articles (58%, n = 18) used an experimental design and involved an intervention that was evaluated. The observational articles (42%, n = 13) included clinical and programme record review, cross-sectional studies, quality improvement, qualitative and literature review methods in relation to at least one programme or intervention. Hospital or clinic (n = 15) and community settings (n = 16) were similarly popular settings for the interventions, and 10% of the papers described interventions that used both community and hospital settings (n = 3). One of the included articles(Reference Faraz46) discussed three different immigrant BF support programmes which we describe individually going forward. This means that strategies from thirty-three total interventions described in thirty-one papers will be presented and discussed in this review.
The interventions targeted a variety of breastfeeding-related outcomes, namely exclusive BF (49%, n = 16), BF initiation (30%, n = 10), duration of BF (15%, n = 5), BF intentions (18%, n = 6), BF self-efficacy (12%, n = 4), BF knowledge (21%, n = 7) and general (or any) BF rates at various timepoints (21%, n = 7). Other breastfeeding outcomes of interest were perceptions of BF recommendations, willingness to BF, volume of formula given by mixed feeders, incidence of BF problems, delayed complementary feeding, delayed introduction of artificial nipples, delayed formula supplementation, BF decision-making, BF communication and support, and improved provider knowledge about community BF needs. Nearly two-thirds of the studies (64%, n = 21) began in the prenatal period, of which 71% (n = 15) extended into postpartum. The duration of postpartum follow-up of these studies varied from delivery to 3 years, and 40% engaged participants for up to 6 months postpartum (n = 6).
Types of breastfeeding support
The general forms of support provided were BF promotion and education (informational support) (91%, n = 30), hands-on BF support (27%, n = 9), material support (48%, n = 16), social support (55%, n = 18) and social marketing to promote community support for breastfeeding (3%, n = 1). Most of the interventions (n = 30) included an element of education to inform mothers about the benefits of breastfeeding, encourage them to practice breastfeeding postpartum, prepare them for potential challenges that may arise and/or increase their awareness of how to find additional help or support during breastfeeding. All five forms of support were delivered using the various strategies described in subsequent sections. Definitions for each type of support are provided in supplementary file S2.
Breastfeeding support strategies
Breastfeeding peer counselling
Twenty-one interventions used individualised/interpersonal education or counselling as a strategy to promote BF among immigrants. Of these, about half (48%, n = 10) used peer counselling as a mechanism for delivering breastfeeding education. Peer counsellors (PCs) were typically women from the target community, who had successfully breastfed and were trained to provide evidence-based BF support by most of the interventions described in the included studies(Reference Faraz46–Reference Tuttle and Dewey55). One peer counselling programme also required PCs to undergo a hands-on training process where they first shadow an International Board-Certified Lactation Counselor (IBCLC) or other lactation expert to observe hands-on BF management for some time before they were allowed to manage clients with supervision or independently(Reference Hopkinson and Konefal Gallagher47).
Peer counselling was often delivered prenatally, in the peripartum hospitalisation period, and postpartum. Prenatal peer counselling focused more on breastfeeding promotion via education about its benefits, correcting myths and common misinformation about breastfeeding, and providing anticipatory guidance about potential challenges and how to overcome them(Reference Linares, Cartagena and Rayens48,Reference Sandy, Anisfeld and Ramirez51,Reference Lutenbacher, Elkins, Dietrich and Riggs53–Reference Tuttle and Dewey55) . Postpartum visits by peer counsellors in the hospital or at home tended to focus more on practical support such as latching and positioning, breast examinations and providing encouragement and specialised counselling or referrals according to a mother’s needs(Reference Hopkinson and Konefal Gallagher47,Reference Noble, Rivera-Todaro, Hand and Noble50,Reference Sandy, Anisfeld and Ramirez51,Reference Tuttle and Dewey55) . Peer counselling was mostly utilised in interventions for primarily Hispanic mothers (n = 6), but a couple of interventions used peer counselling to promote breastfeeding among non-Hispanic mothers(Reference Mosley, Pratt, Besera, Clarke, Miller and Noland49,Reference Tuttle and Dewey55) and mixed immigrant populations(Reference Faraz46,Reference Noble, Rivera-Todaro, Hand and Noble50) . Where intervention results were reported, peer counselling interventions targeting both Hispanic and non-Hispanic populations tended to report success in meeting their targeted BF outcomes.
Group breastfeeding education
Another key strategy used to promote and support breastfeeding among immigrants in the United States is group breastfeeding education. Of the thirty-three interventions described in the included sources, about half (n = 17) described an element of group breastfeeding education and support. These commonly included group prenatal counselling classes(Reference Faraz46,Reference Mosley, Pratt, Besera, Clarke, Miller and Noland49,Reference Watkins, Larson, Harlan and Young52–Reference Torres, Smithwick, Luchok and Rodman-Rice61) , but also postpartum BF support groups(Reference Faraz46,Reference Mosley, Pratt, Besera, Clarke, Miller and Noland49,Reference Noble, Rivera-Todaro, Hand and Noble50,Reference Lutenbacher, Elkins, Dietrich and Riggs53,Reference Lutenbacher, Elkins and Dietrich54,Reference de Bocanegra62–Reference Lawal, Owen, Brown and Effland64) . The group prenatal classes were commonly facilitated by nurses, lactation, providers, health educators or peer counsellors in hospital, clinic settings or community settings(Reference Mosley, Pratt, Besera, Clarke, Miller and Noland49,Reference Lutenbacher, Elkins, Dietrich and Riggs53,Reference Lutenbacher, Elkins and Dietrich54,Reference Madeira, Rangen and Avery57,Reference Young and Kaufman60,Reference Torres, Smithwick, Luchok and Rodman-Rice61) . Group prenatal counselling sessions primarily involved breastfeeding promotion via education, providing information about BF resources and shared problem-solving (Reference Faraz46,Reference Lutenbacher, Elkins, Dietrich and Riggs53,Reference Lutenbacher, Elkins and Dietrich54,Reference Moreland, Lloyd, Braun and Heins58,Reference Young and Kaufman60,Reference Torres, Smithwick, Luchok and Rodman-Rice61) . Some articles also discussed group prenatal care provided by WIC(Reference Tuttle and Dewey55,Reference Moreland, Lloyd, Braun and Heins58) .
Postpartum BF support included peer support groups organised through clinics(Reference Noble, Rivera-Todaro, Hand and Noble50,Reference Lutenbacher, Elkins, Dietrich and Riggs53,Reference Lutenbacher, Elkins and Dietrich54,Reference de Bocanegra62–Reference Lawal, Owen, Brown and Effland64) or by more community-based programmes such as La Leche League(Reference Faraz46). The content and format used in postpartum BF support groups were not discussed.
Larger institutional interventions
Some breastfeeding support strategies identified through this review were implemented as part of larger interventions such as the Special Supplemental Nutrition Program for Women, Infants and Children (WIC)(Reference Bader, Ward, Fouts and Jaekel34,Reference Fisher, Patel, Wouk, Neupane, Alkhalifah and Bartholmae36,Reference Sandy, Anisfeld and Ramirez51,Reference Tuttle and Dewey55,Reference Moreland, Lloyd, Braun and Heins58,Reference Langellier, Chaparro, Wang, Koleilat and Whaley65) . A few articles also discussed hospital lactation or breastfeeding clinics(Reference Hopkinson and Konefal Gallagher47,Reference Noble, Rivera-Todaro, Hand and Noble50) or routine care practices(Reference Linares, Wambach, Rayens, Wiggins, Coleman and Dignan66) that were specific to certain hospitals or health systems.
The experimental studies that included WIC often used WIC BF support as the control or foundation for an additional intervention. For example, some studies assessed new methods of breastfeeding education for specific immigrant clients of WIC(Reference Tuttle and Dewey55,Reference Moreland, Lloyd, Braun and Heins58) such as the promotion of a personalised BF plan among Hispanic participants based on the ‘La Cuarentena del Bebe’ (baby-quarantine) curriculum, a model that builds on the Hispanic postpartum tradition of 40 d of rest and recovery for mother and baby, and champion 40 d of exclusive breastfeeding(Reference Moreland, Lloyd, Braun and Heins58). Other papers described the effectiveness of WIC programmes for BF support among immigrants(Reference Bader, Ward, Fouts and Jaekel34), participants’ perceptions of WIC’s BF support(Reference Fisher, Patel, Wouk, Neupane, Alkhalifah and Bartholmae36), the infant feeding intention and practices of WIC participants who had received WIC BF support(Reference Fisher, Patel, Wouk, Neupane, Alkhalifah and Bartholmae36), or evaluation of specific programme changes such as the WIC breastfeeding food package implemented in 2009(Reference Langellier, Chaparro, Wang, Koleilat and Whaley65).
Two studies discussed how postpartum referral to hospital-based lactation or breastfeeding clinics were used as a strategy to support immigrant breastfeeding. Assistance provided at these clinics included physical breast examinations, hand-on BF support, informational and skill-based counselling provided by peer counsellors, and access to medical providers in cases where more advanced lactation support is required(Reference Hopkinson and Konefal Gallagher47,Reference Noble, Rivera-Todaro, Hand and Noble50) . Another study evaluated the influence of early skin-to-skin contact on breastfeeding initiation and sustained exclusive breastfeeding among a group of women who gave birth in hospitals that routinely practiced skin-to-skin care(Reference Linares, Wambach, Rayens, Wiggins, Coleman and Dignan66). Practices such as postpartum lactation counsellor education and support were also discussed as institutional practices, but these were talked about as the control or standard of care where the intervention was set in a Baby-Friendly Hospital(Reference Linares, Cartagena and Rayens48).
Expert support
More than half of the interventions (64%, n = 21) described the involvement of medical lactation experts such as International Board-Certified Lactation Consultants (IBCLCs) and Certified Lactation Consultants (CLCs) or trained maternity nurses and other medical providers as a strategy for immigrant BF support(Reference Hopkinson and Konefal Gallagher47–Reference Watkins, Larson, Harlan and Young52,Reference Little, Motohara, Plegue, Medaugh, Sen and Ruffin56,Reference Madeira, Rangen and Avery57,Reference Roby and Woodson59,Reference Young and Kaufman60,Reference Gross, Mendelsohn, Gross, Scheinmann and Messito63,Reference Lawal, Owen, Brown and Effland64,Reference Linares, Wambach, Rayens, Wiggins, Coleman and Dignan66–Reference Duh-Leong, Au, Chang, Feldman, Pierce and Mendelsohn74) .
IBCLCs acted in a variety of roles such as BF support programme coordinator(Reference Hopkinson and Konefal Gallagher47,Reference Linares, Cartagena and Rayens48) , direct breastfeeding counsellor(Reference Linares, Cartagena and Rayens48,Reference Gill, Reifsnider and Lucke69) , peer counsellor trainer and supervisor,(Reference Hopkinson and Konefal Gallagher47) or as a resource to provide support to mothers with serious BF problems(Reference Hopkinson and Konefal Gallagher47,Reference Gill, Reifsnider and Lucke69) . Nurses also took on various roles in these interventions. Nurses were the primary providers of the standard hospital BF support used as the control for the various immigrant-centred strategies included in this review(Reference Gross, Mendelsohn, Gross, Scheinmann and Messito63,Reference Gill75) , and they were also involved as project coordinators(Reference Watkins, Larson, Harlan and Young52), recruiters(Reference Gill, Reifsnider and Lucke69), data collectors(Reference Mosley, Pratt, Besera, Clarke, Miller and Noland49) or the primary breastfeeding counsellors who educated and provided direct lactation support to participants(Reference Noble, Rivera-Todaro, Hand and Noble50,Reference Watkins, Larson, Harlan and Young52,Reference Little, Motohara, Plegue, Medaugh, Sen and Ruffin56,Reference Schlickau and Wilson70) , sometimes with support from lactation consultants(Reference Gross, Mendelsohn, Gross, Scheinmann and Messito63). Lactation consultants were directly involved in delivering the BF support intervention(Reference Noble, Rivera-Todaro, Hand and Noble50,Reference Roby and Woodson59,Reference Lawal, Owen, Brown and Effland64,Reference Bonuck, Trombley, Freeman and McKee67,Reference Gill, Reifsnider and Lucke69) or acted in a more supportive role to peer counsellors and maternity nurses(Reference Linares, Cartagena and Rayens48,Reference Gross, Mendelsohn, Gross, Scheinmann and Messito63) . Other providers described as providing some form of expertise or BF support include physicians(Reference Noble, Rivera-Todaro, Hand and Noble50,Reference Sandy, Anisfeld and Ramirez51,Reference Linares, Wambach, Rayens, Wiggins, Coleman and Dignan66,Reference Cook, Kimball, Zittleman and Huntington68,Reference Thompson, Joshi, Hernandez, Bair-Merritt, Arora and Luna71) , nursing student doulas(Reference Van Zandt, Kim and Erickson72), social workers(Reference Watkins, Larson, Harlan and Young52,Reference Lawal, Owen, Brown and Effland64) , midwives and doulas(Reference Madeira, Rangen and Avery57,Reference Lawal, Owen, Brown and Effland64,Reference Zaidi, Fantasia, Penders, Koren and Enah73) .
Some studies (n = 6) also described the role of community expert support(Reference Mosley, Pratt, Besera, Clarke, Miller and Noland49,Reference Lutenbacher, Elkins and Dietrich54,Reference Madeira, Rangen and Avery57,Reference Roby and Woodson59,Reference Torres, Smithwick, Luchok and Rodman-Rice61,Reference Zaidi, Fantasia, Penders, Koren and Enah73) . Health educators, social workers and public health nutritionists are additional experts that were used to deliver BF support to immigrants in community and clinical settings(Reference Watkins, Larson, Harlan and Young52,Reference Young and Kaufman60–Reference Lawal, Owen, Brown and Effland64) . Madeira et al. (Reference Madeira, Rangen and Avery57) used an educational approach that was delivered by a variety of community experts, including religious and community leaders, doulas and educators. For example, the breastfeeding components of the intervention were delivered by WIC peer counsellors even though it was not a peer support or WIC-based intervention. Four interventions involved training providers about the need for BF support to immigrant women facing BF challenges(Reference Zaidi, Fantasia, Penders, Koren and Enah73), improving their communication skills(Reference Torres, Smithwick, Luchok and Rodman-Rice61,Reference Duh-Leong, Au, Chang, Feldman, Pierce and Mendelsohn74) and providing tools such as flipcharts and other visual aids to manage language barriers and support providers in caring for immigrant women(Reference Young and Kaufman60).
Family support
Although most of the articles included a measure or assessment of maternal social support, only a third of all the interventions intentionally targeted families and other support persons in the breastfeeding dyad’s support network (33%, n = 11). The primary methods of fostering family and friend support for breastfeeding among immigrants were education-based and involved inviting family and friends to classes(Reference Faraz46,Reference Roby and Woodson59–Reference Torres, Smithwick, Luchok and Rodman-Rice61,Reference Gross, Mendelsohn, Gross, Scheinmann and Messito63) and encouraging the entire family or at least primary support person(s) to participate in home visits(Reference Sandy, Anisfeld and Ramirez51,Reference Bonuck, Trombley, Freeman and McKee67) or other counselling sessions(Reference Faraz46,Reference Cook, Kimball, Zittleman and Huntington68) . Some articles also described a strength-based approach to family engagement which involved helping the family to recognise their own strengths and how those strengths can be used to meet their needs or health goals(Reference Lutenbacher, Elkins, Dietrich and Riggs53,Reference Lutenbacher, Elkins and Dietrich54) . Family education included discussing the importance of BF and their role in supporting the mother–baby dyad to meet BF recommendations.
Breastfeeding plans
A few interventions (n = 4) also encouraged mothers to create personalised breastfeeding plans as a strategy to promote commitment to BF, increase self-efficacy and foster BF success(Reference Linares, Cartagena and Rayens48,Reference Moreland, Lloyd, Braun and Heins58,Reference Schlickau and Wilson70,Reference Van Zandt, Kim and Erickson72) . These plans were created as a means of boosting mothers’ confidence(Reference Moreland, Lloyd, Braun and Heins58), strengthening their commitment to BF(Reference Schlickau and Wilson70) and communicating their BF plans with their family members and birthing support persons(Reference Moreland, Lloyd, Braun and Heins58).
Resource provision and community linkages
Overall, fifteen studies (45%) reported providing some forms of material support to promote BF among immigrants. Material support was defined as the provision of breastfeeding supplies, cash or food incentives, and linkage to community resources to address other family needs. Some of the studies described giving BF supplies such as breast pumps, breastfeeding sling, nursing bras, breast pads, nipple creams and water bottles to reduce breast pain and facilitate breastfeeding, especially among immigrant mothers who may need to return to work or school(Reference Bader, Ward, Fouts and Jaekel34,Reference Fisher, Patel, Wouk, Neupane, Alkhalifah and Bartholmae36,Reference Linares, Cartagena and Rayens48,Reference Bonuck, Trombley, Freeman and McKee67,Reference Gill, Reifsnider and Lucke69) . Others described connecting mothers with other community resources for assistance with needs such as housing, food insecurity and other social determinants of health or barriers that may limit breastfeeding(Reference Sandy, Anisfeld and Ramirez51–Reference Lutenbacher, Elkins and Dietrich54,Reference Lawal, Owen, Brown and Effland64,Reference Van Zandt, Kim and Erickson72,Reference Zaidi, Fantasia, Penders, Koren and Enah73) . Food incentives were also provided through WIC(Reference Langellier, Chaparro, Wang, Koleilat and Whaley65), and one study provided training, communication tools and aids to enable providers deliver BF support to non-English-speaking mothers(Reference Young and Kaufman60).
Methods of intervention delivery
The interventions described in this review were delivered primarily through home visits, hospital visits, telephone support and multimedia or technology-based campaigns. Home visits were conducted in 27% of the interventions (n = 9), and they occurred prenatally(Reference Watkins, Larson, Harlan and Young52), postnatally(Reference Noble, Rivera-Todaro, Hand and Noble50,Reference Tuttle and Dewey55,Reference Gill, Reifsnider and Lucke69) or both(Reference Linares, Cartagena and Rayens48,Reference Sandy, Anisfeld and Ramirez51,Reference Lutenbacher, Elkins, Dietrich and Riggs53,Reference Lutenbacher, Elkins and Dietrich54,Reference Bonuck, Trombley, Freeman and McKee67) . Home visits were often selected to make the interventions more accessible to participants, as a means of personalising the breastfeeding education and hands-on support, and to get a better picture of familial support and other circumstances that might affect an immigrant mother’s breastfeeding. Interventions that implemented home visits in both the prenatal and postpartum period did it to maintain a continuum of breastfeeding care throughout pregnancy and up to at least 6 months postpartum(Reference Linares, Cartagena and Rayens48,Reference Sandy, Anisfeld and Ramirez51,Reference Lutenbacher, Elkins, Dietrich and Riggs53,Reference Lutenbacher, Elkins and Dietrich54,Reference Bonuck, Trombley, Freeman and McKee67) .
Half of the interventions also involved some form of hospital visit (52%, n = 17). Seven interventions described counsellors visiting immigrant moms during perinatal hospitalisations (in the few days after birth) to support them with BF initiation and address any challenges that occur in the early stages of breastfeeding(Reference Hopkinson and Konefal Gallagher47,Reference Linares, Cartagena and Rayens48,Reference Sandy, Anisfeld and Ramirez51,Reference Tuttle and Dewey55,Reference Gross, Mendelsohn, Gross, Scheinmann and Messito63,Reference Bonuck, Trombley, Freeman and McKee67,Reference Van Zandt, Kim and Erickson72) . Other studies hosted prenatal class or individual visits with a lactation consultant or other professionals in the hospitals or clinic(Reference Faraz46,Reference Little, Motohara, Plegue, Medaugh, Sen and Ruffin56,Reference Madeira, Rangen and Avery57,Reference de Bocanegra62,Reference Gross, Mendelsohn, Gross, Scheinmann and Messito63,Reference Gill, Reifsnider and Lucke69,Reference Schlickau and Wilson70,Reference Van Zandt, Kim and Erickson72) , and a few studies described coordinating their postpartum follow-up BF support visits with routine well-child or paediatric hospital visits(Reference Gross, Mendelsohn, Gross, Scheinmann and Messito63,Reference Cook, Kimball, Zittleman and Huntington68,Reference Thompson, Joshi, Hernandez, Bair-Merritt, Arora and Luna71) .
Telephone calls(Reference Hopkinson and Konefal Gallagher47,Reference Linares, Cartagena and Rayens48,Reference Tuttle and Dewey55,Reference Little, Motohara, Plegue, Medaugh, Sen and Ruffin56,Reference Bonuck, Trombley, Freeman and McKee67,Reference Gill, Reifsnider and Lucke69) , print media (for example, informational pamphlets(Reference Fisher, Patel, Wouk, Neupane, Alkhalifah and Bartholmae36,Reference Linares, Cartagena and Rayens48,Reference Mosley, Pratt, Besera, Clarke, Miller and Noland49,Reference Lutenbacher, Elkins, Dietrich and Riggs53,Reference Lutenbacher, Elkins and Dietrich54,Reference Gross, Mendelsohn, Gross, Scheinmann and Messito63,Reference Cook, Kimball, Zittleman and Huntington68) , infant and young child feeding guides(Reference Faraz46,Reference Sandy, Anisfeld and Ramirez51,Reference Duh-Leong, Au, Chang, Feldman, Pierce and Mendelsohn74) , and bilingual ‘fotonovelas’ (photographic story booklets)(Reference Faraz46)), electronic media and other video materials on breastfeeding(Reference Roby and Woodson59,Reference Gross, Mendelsohn, Gross, Scheinmann and Messito63) , as well as interactive learning platforms(Reference Thompson, Joshi, Hernandez, Bair-Merritt, Arora and Luna71), were also utilised to deliver breastfeeding education and promote individual, interpersonal and community breastfeeding behaviour change among immigrants. Telephone visits were used for delivering BF education, follow-up or as a means of contacting nurses and PCs in case of a breastfeeding question or emergency(Reference Hopkinson and Konefal Gallagher47,Reference Linares, Cartagena and Rayens48,Reference Tuttle and Dewey55,Reference Little, Motohara, Plegue, Medaugh, Sen and Ruffin56,Reference Bonuck, Trombley, Freeman and McKee67,Reference Gill, Reifsnider and Lucke69) .
Immigrant populations studied
More than half of the papers in this review described BF support strategies or interventions that targeted immigrant Hispanic or Latina women and families (58%, n = 18). Six studies targeted specific non-Hispanic immigrant and refugee (NHIR) groups including women of African(Reference Bader, Ward, Fouts and Jaekel34,Reference Madeira, Rangen and Avery57,Reference Cook, Kimball, Zittleman and Huntington68) and Asian (Japanese, Chinese and Hmong) descent(Reference Tuttle and Dewey55,Reference Little, Motohara, Plegue, Medaugh, Sen and Ruffin56,Reference Duh-Leong, Au, Chang, Feldman, Pierce and Mendelsohn74) . The remaining seven papers included multiple (Hispanic and non-Hispanic) immigrant and refugee groups(Reference Mosley, Pratt, Besera, Clarke, Miller and Noland49,Reference Noble, Rivera-Todaro, Hand and Noble50,Reference Watkins, Larson, Harlan and Young52,Reference de Bocanegra62,Reference Lawal, Owen, Brown and Effland64,Reference Van Zandt, Kim and Erickson72,Reference Zaidi, Fantasia, Penders, Koren and Enah73) . Of the approximately 7700 immigrant women accounted for in the final papers, 87.3% (n = 6719) were Hispanic mothers, 4.5% were of African descent, 7.0% were of Asian descent and the rest were unspecified.
All interventions and key strategies that participants (or the intervention group in experimental studies) were exposed to are summarised in Table 3.
Differences in interventions over time
Compared with those published before 2016 (n = 18), a lower proportion of the interventions published in the past decade (n = 15) provided BF promotion and education (100% versus 80%) and hands-on breastfeeding support to foreign-born mothers (33% versus 20%). There were no social marketing campaigns for breastfeeding documented since 2010(Reference Faraz46), but more interventions in the past decade reported giving material (practical) support (39% versus 60%).
Compared with interventions published pre-2016, group BF education, support from medical/lactation experts and resource provision were more common in recent interventions, the proportion of interventions that promoted family support decreased, and other strategies such as peer counselling, creation of personalised breastfeeding plans, and leveraging existing programmes/institutions and resource provision were comparable across time periods (see details in Table 4). Home visits were less frequently reported in interventions published between 2016 and 2025, but the use of print media (for example, infant feeding guides, fotonovelas, pamphlets, brochures etc.) was more frequent. Hospital visits, telephone calls and video-based platforms were comparable across periods (see details in Table 4).
Furthermore, prenatal and postpartum breastfeeding interventions were less commonly reported in the past decade, while the proportion of interventions that cut across the prenatal and postpartum period increased (39% versus 53%). Recent interventions (2016–2025) had a more varied distribution in race/ethnicity of foreign-born mothers compared with the older interventions. The proportion of Hispanic mothers represented in the literature decreased (95% versus 56%), while the proportion of foreign-born mothers of African (3% versus 11%) and Asian (2% versus 29%) descent increased. Overall, interventions published pre-2016 reported more success in meeting their designated breastfeeding outcomes compared with interventions published within the past decade (61% versus 53%).
Discussion
This review provides novel insight into existing breastfeeding support strategies and identifies critical gaps for intervention to promote optimal breastfeeding among foreign-born mothers in the United States. A variety of approaches have been documented in the literature for supporting breastfeeding among immigrants in the United States. The common types of support used in interventions to promote optimal breastfeeding among immigrants include education and informational support, hands-on support, social support, material support and social marketing to promote community support for breastfeeding. Specific strategies employed by immigrant BF programmes include peer counselling, group prenatal education and postpartum support, institutional interventions such as hospital lactation care and skin-to-skin care, expert support, family support promotion, encouraging breastfeeding plans, provider training, and providing material support in the form of breastfeeding supplies, food incentives or connecting immigrant mothers to other community resources necessary for them to achieve positive health states. These strategies are widely recognised as best practices and have all been demonstrated to improve breastfeeding rates(Reference Chapman and Pérez-Escamilla42,Reference Chapman, Morel, Anderson, Damio and Pérez-Escamilla76,Reference Shakya, Kunieda, Koyama, Rai, Miyaguchi and Dhakal77) . The main methods of delivering the interventions were through hospital and home visits, telephone calls, print and electronic media and interactive learning platforms.
The targeted immigrant populations in the included studies were primarily Hispanic/Latino women. African and Asian breastfeeding mothers were far less represented in the literature on immigrant BF support. Although representation has improved within the past decade, non-Hispanic foreign-born mothers, especially Africans, are still largely understudied. As the population of non-Hispanic immigrants and refugees increase in the United States(78,Reference Farivar79) , more studies are needed to unpack the nuances of BF and BF support among these populations of mothers.
Of the twenty-seven interventions that measured and reported specific BF outcomes, 70% (n = 19) reported success in meeting their targeted BF outcomes. Among the 50% of interventions (n = 16) that targeted EBF at various timepoints, about half (53%, n = 10) reported success in meeting their outcomes. This is useful considering that previous research has identified high initiation but low EBF rates among immigrant populations in the United States(Reference Celi, Rich-Edwards, Richardson, Kleinman and Gillman19–Reference Rosenthal, Oliveira, Madubuko, Tanuos, Schwab and Monteiro21) Also, most of the interventions that reported success used a combination of strategies and delivery methods, which is consistent with what has previously been reported in the literature(Reference Gill75,Reference Renfrew, McCormick, Wade, Quinn and Dowswell80,Reference de Oliveira, Camacho and Tedstone81) . Specifically, combining strategies for BF promotion and education with strategies for social support and/or material support seemed to be a common theme in this review. There were two articles that reported being successful in meeting their targeted BF outcomes despite being focused only on BF promotion and education strategies(Reference Linares, Cartagena and Rayens48,Reference Schlickau and Wilson70) . However, both articles encouraged immigrant mothers to create some sort of commitment to action plan, which may have increased their self-efficacy and prepared them to breastfeed.
In total, 84.2% of the nineteen interventions (n = 16) that reported success in this review also recruited immigrant mothers prenatally, and more than half (58%, n = 11) followed participants through the postpartum period. Previous studies have found that delivering BF interventions postnatally was more effective than when delivered only antenatally(Reference McFadden, Siebelt, Marshall, Gavine, Girard and Symon82,Reference Skouteris, Bailey, Nagle, Hauck, Bruce and Morris83) , which is consistent with the findings of this review. Starting in the prenatal period to help mothers form the intention to exclusively breastfeed, providing in-hospital support to initiate breastfeeding after birth and then following them through the postpartum period is best practice, as highlighted by standards of care such as the World Health Organization’s Ten Steps to Successful Breastfeeding(84). The stratified analysis of interventions across time indicates that a higher proportion of the recent interventions (2016–2025) followed participants from the prenatal to postpartum period, which is consistent with the recommended best practices for BF support.
Another key aspect of all the strategies for support utilised in this review was that the education and informational materials were made accessible to the target population. Counselling was often delivered by bilingual and bicultural professionals, handouts were translated into the primary language and matched the literacy levels apparent in the target population, and the one study that used an interactive learning platform also ensured that all content, imagery and voice over were appropriate for the targeted immigrant audience(Reference Thompson, Joshi, Hernandez, Bair-Merritt, Arora and Luna71). The time-based analyses also indicated a much higher use of handouts and printed informational material in more recent interventions, which could be due to increased accessibility, affordability, quality and advancements in print technology over time. However, details on the format of these print media and how they are delivered to participants are unclear. For example, the studies do not discuss how text-based approaches or the use of QR codes and web-based resource hubs might impact participant access to the resources, and there is limited information on the effectiveness of print media for improving BF knowledge and self-efficacy among various populations of foreign-born mothers.
Furthermore, fewer interventions published in the past decade reported BF promotion and education, while more of them provided material support for participants. Group breastfeeding education and resource provision – including the provision of breastfeeding supplies and referral to community support resources – seem to have become more popular strategies for immigrant breastfeeding support. This is consistent with the shift in public health from purely education-based approaches towards approaches that combine community-strengthening and practical approaches and address social and structural determinants, to promote positive health behaviour(Reference Nichols85–88).
Many of the experimental studies involved some level of formative work to inform the intervention design in a way that would be culturally respectful, specific and acceptable. A good example of this is the use of ‘La Cuarentena del Bebe’ as a concept to promote breastfeeding in Latina populations. This concept draws directly from the target population’s home culture of avoiding vaginal penetration for 40 d after birth and was adapted to promote 40 d of exclusive breastfeeding where nothing but a mother’s milk enters a baby’s mouth(Reference Moreland, Lloyd, Braun and Heins58,Reference Schlickau and Wilson70) . Another article highlighted the importance of cultural sensitivity in BF interventions for immigrants by describing how inviting female friends and relatives was beneficial because participants had expressed discomfort with discussing breastfeeding in front of men(Reference Young and Kaufman60).
Previous research has demonstrated mixed findings on WIC’s effectiveness for BF support among immigrants(Reference Bader, Ward, Fouts and Jaekel34,Reference Reeves Tuttle and Dewey35,Reference Chapman and Pérez-Escamilla42,Reference Tuttle and Dewey55) . Although WIC is not targeted at immigrants, it tends to include a substantial number of immigrants in certain areas(Reference Fisher, Patel, Wouk, Neupane, Alkhalifah and Bartholmae36,89) , yet few studies have evaluated key aspects of WIC’s BF support strategies in immigrant populations. Most of the WIC studies reviewed during the screening process used WIC as a marker of low income or a convenient means of recruiting pregnant immigrant mothers(Reference Roess, Robert, Kuehn, Ume, Ericson and Woody90,Reference Gross, Mendelsohn, Arana and Messito91) , or focused on barriers to enrolment in WIC(Reference Pelto, Ocampo, Garduño-Ortega, Barraza López, Macaluso and Ramirez92). Many of the WIC-related studies in this review met the inclusion criteria because they either used WIC support as a foundation or usual care (control) for their intervention(Reference Sandy, Anisfeld and Ramirez51,Reference Tuttle and Dewey55,Reference Madeira, Rangen and Avery57,Reference Moreland, Lloyd, Braun and Heins58) or discussed WIC services in general with respect to BF(Reference Bader, Ward, Fouts and Jaekel34,Reference Fisher, Patel, Wouk, Neupane, Alkhalifah and Bartholmae36) . This highlights a need for more studies that evaluate the effectiveness of all aspects of WIC BF support (peer counselling, BF food package, BF education materials etc.) among various immigrant groups, and studies that explore how WIC counsellors can incorporate the cultural values of their immigrant clients into their routine education/classes to emphasise breastfeeding as a strength. A couple of studies tested cultural adaptations to standard WIC classes, but they did not discuss the various aspects of WIC’s breastfeeding support in detail(Reference Fisher, Patel, Wouk, Neupane, Alkhalifah and Bartholmae36,Reference Langellier, Chaparro, Wang, Koleilat and Whaley65) or describe how they plan to integrate the successful and culturally specific trainings into routine WIC programming(Reference Moreland, Lloyd, Braun and Heins58).
Another key gap identified during this review is the need for broader implementation and better evaluation of social marketing campaigns to change BF culture at the community level. Previous studies have revealed prevalent beliefs in certain immigrant groups that mixed feeding is harmless(Reference de Bocanegra62), that formula is more nutrient-rich or healthier than breastmilk(Reference Bunik, Clark, Zimmer, Jimenez, O’Connor and Crane93,Reference Thomas and DeSantis94) or that BF is not ‘American’(Reference Bader, Ward, Fouts and Jaekel34). Although the evidence base has highlighted the crucial role of family and community support in successfully meeting BF recommendations(Reference Wood and Qureshi95–Reference Rhodes, Damio, LaPlant, Trymbulak, Crummett and Surprenant97), only a third of interventions in this review targeted family or other social support networks as a strategy for promoting BF. Also, family support was less frequently reported among recent interventions, and there have been no social marketing campaigns for BF reported in immigrant communities within the past decade. Since social marketing has been previously identified as an excellent tool for promoting positive health behaviours(98), it is important to assess the reach and effectiveness of social marketing campaigns like the one done by Stopka et al.(Reference Stopka, Segura-Perez, Chapman, Damio and Perez-Escamilla99) among foreign-born Hispanic women and to see if the success of such interventions can be replicated more broadly in other US immigrant communities, especially using social media and other modern technology.
Furthermore, the effectiveness of bilingual peer counsellor home visitation programmes for improving breastfeeding outcomes was observed in a series of studies on Hispanic women conducted by researchers in Connecticut and Massachusetts(Reference Anderson, Johnstone and Remley7,Reference Rhodes, Damio, LaPlant, Trymbulak, Crummett and Surprenant97,Reference Chapman, Morel, Bermúdez-Millán, Young, Damio and Pérez-Escamilla100) , but these studies were excluded from the review because it was unclear if the participants were immigrants or US-born Hispanic women. In this review, peer counselling was also utilised in interventions that primarily targeted Hispanic foreign-born mothers, many of which reported success in meeting their targeted breastfeeding outcomes(Reference Hopkinson and Konefal Gallagher47,Reference Linares, Cartagena and Rayens48,Reference Sandy, Anisfeld and Ramirez51–Reference Lutenbacher, Elkins and Dietrich54) . However, the couple of interventions where the strategy was used to improve breastfeeding outcomes among non-Hispanic immigrants also reported success(Reference Mosley, Pratt, Besera, Clarke, Miller and Noland49,Reference Tuttle and Dewey55) . This is consistent with previous research that has highlighted peer support as a broad and robust means of promoting positive health behaviours and outcomes among groups that are hardly reached through conventional approaches, such as immigrants with language barriers(Reference Sokol and Fisher101). More research is needed to understand the effectiveness of peer support approaches among various immigrant and refugee groups.
Also, national breastfeeding interventions such as the Baby Friendly Hospital Initiative need to incorporate more culturally sensitive approaches that target and are inclusive of various populations of immigrant mothers(Reference Ahluwalia, D’Angelo, Morrow and McDonald24). BFHI is a global programme that encourages the widescale adoption of the Ten Steps to Successful Breastfeeding and the International Code of Marketing Breast-Milk Substitutes as the standard of care in birthing facilities(102). The components of the Ten Steps include prenatal BF education, in-hospital lactation care and postpartum community lactation support. Despite many of the interventions utilising strategies such as skin-to-skin care(Reference Linares, Wambach, Rayens, Wiggins, Coleman and Dignan66) and other evidence-based BF enabling practices that are routinely implemented as part of the BFHI(84), we found only one recent article (published February 2025) that has assessed the delivery and implementation of Ten Steps for immigrant families(Reference Tucker, Arcoleo, DiTomasso, Oaks, Cabral and São-João103). The authors found disparities by racial and ethnic groups and concluded that mothers from various racial and ethnic minority groups (Black, Hispanic and Asian) were at lower odds of receiving 100% of key BFHI clinical practices, compared with white non-Hispanic mothers(Reference Tucker, Arcoleo, DiTomasso, Oaks, Cabral and São-João103). Other studies have also highlighted that language barriers may limit the quality of care, lactation counselling and breastfeeding support that immigrants, especially non-English-speaking mothers, receive in clinical settings(Reference Little, Motohara, Plegue, Medaugh, Sen and Ruffin56–Reference Moreland, Lloyd, Braun and Heins58). As the BFHI gains more popularity in the United States, it is important to ensure equitable access to its benefits. Therefore, we need more research to understand how the programme can be tailored to accommodate and support immigrant or refugee women who deliver at Baby-Friendly facilities.
Lastly, none of the included studies targeted workplace BF or discussed an effective strategy to address this crucial area of life, despite the return to work or school being commonly cited as a reason why many immigrant mothers stop exclusive or any breastfeeding(Reference Fisher, Patel, Wouk, Neupane, Alkhalifah and Bartholmae36,Reference Schlickau and Wilson70,Reference Lindsay, Wallington, Greaney, Hasselman, Tavares Machado and Mezzavilla104) . It could be important to understand how models and toolkits that are used more generally, like Mississippi WINS(105), can be adapted to promote workplace breastfeeding in predominantly immigrant workplaces and communities.
The main strength of this scoping review is that the methods were sufficient to address the research question and highlight key gaps in the literature. The authors searched multiple databases, carefully documented all decision-making processes and followed a systematic process that enabled consistency in selection and analysis. Also, the entire process from search to analysis was conducted twice with an interval of 6 months, which allowed the authors to re-review all the articles and double check all reported findings with a fresh perspective. The first two databases were searched in May 2024, and the updated search was conducted to include all articles published through January 2025. The limitations of the study include the focus on peer-reviewed articles and the fact that the literature review and analysis was conducted primarily by one author (A.G.), which indicates some risk of bias in study selection. We managed these issues by searching six databases (including PubMed) and using a thorough and well-documented systematic process for study selection, full text review and analysis. The other authors (M.Y. and U.R.) reviewed the paper and 20% of the articles to confirm that they were eligible for inclusion or exclusion.
Also, due to the exploratory nature of this review, critical appraisal of studies was not conducted, and some included papers may have been of poor quality or incomprehensive. The lack of a comprehensive quality appraisal means that we cannot draw conclusions about how well the different strategies work for various groups of immigrants, or the effectiveness of more modern information and communication strategies on the success of interventions. Further research is needed to understand these aspects and to inform future interventions.
Conclusions
This review provides a comprehensive overview of evidence on existing strategies for breastfeeding support and education among foreign-born women in the United States and highlights important gaps in the targeting and implementation of existing interventions. Strategies that have been documented in the literature include peer counselling, group prenatal and postpartum education or support, institutional interventions such as WIC classes and hospital lactation clinics, medical expert support for BF immigrants, educating family members to promote support, encouraging breastfeeding goal-setting and providing material support such as breastfeeding supplies, cash or food incentives, and connecting immigrant mothers to other community resources necessary for them to achieve positive health states. The main methods of delivering the interventions were through home and hospital visits, telephone calls, print and electronic media and interactive learning platforms. Interventions that reported success in meeting their targeted BF outcomes tended to combine BF promotion and education strategies with strategies that provided other forms of support.
Implications for research and practice
The key research gaps identified include limited implementation and evaluation of social marketing campaigns to promote a culture of exclusive breastfeeding, efforts to promote workplace breastfeeding support, and the need for national breastfeeding programmes like WIC and the Baby-Friendly Hospital Initiative to incorporate more culturally sensitive and inclusive approaches to breastfeeding education and support for various immigrant populations in the United States. Overall, the review presents opportunities for improving breastfeeding education and support for foreign-born mothers in the United States by addressing the identified gaps, and underscores a need for coordinated multisector approaches to promoting optimal breastfeeding practices, including EBF, throughout the continuum of pregnancy, birth and childcare(Reference Rethy, Gallo, Doig, Brady and Goodfriend106). Efforts should also be made to (i) understand how various breastfeeding education and support strategies might work differently among immigrant and refugee groups, and (ii) to adapt and replicate the success of interventions that have targeted pockets of predominantly Hispanic foreign-born mothers, for improving EBF more broadly among foreign-born families in the United States.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954422426100341.
Acknowledgements
The authors would like to thank Drs. Aryeh Stein, Jean Welsh and Mary Beth Weber, as well as Ms. Shenita Peterson for their guidance and support on this project.
Authorship
A.G. conceived and designed the scoping review with search strategy guidance from the librarian, Shenita Peterson. A.G. carried out the searches, screened manuscripts, analysed the research evidence, drafted and reviewed the manuscript. M.Y. assisted with record reviews, provided critical feedback and substantively revised the manuscript. U.R. provided critical feedback during the second round of the review and substantively revised the manuscript. All authors read and approved the final manuscript and agreed to be accountable for all aspects of the review.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The authors declare no competing interests.
Ethical standards
Not applicable.




 Open access
Open access